Comparison of prophylactic genotypic matching with ...
13
1 Comparison of prophylactic genotypic matching with phenotypic matching for reducing the rate of alloimmunization and hemolytic transfusion reactions in patients with Sickle Cell Disease (SCD) Ianca leal, Maria Rita M Miranda, Tamires D Santos, Simone Gilli, Lilian Castilho Date: 10/19/2021
Transcript of Comparison of prophylactic genotypic matching with ...
1
Comparison of prophylactic genotypic matchingwith phenotypic matching for reducing the rate of
alloimmunization and hemolytic transfusionreactions in patients with Sickle Cell Disease (SCD)
Ianca leal, Maria Rita M Miranda, Tamires D Santos, Simone Gilli, Lilian Castilho
Date: 10/19/2021
Faculty Disclosure
2
In compliance with ACCME policy,
AABB requires the following
disclosures to the session audience
I have no conflict of interest to declare
3
Red blood cell alloimmunization
Transfusion of patients with SCD represents a significant challenge in clinical transfusion medicine with RBC alloimmunization a primary and serious complication
The rates of RBC alloimmunization in patients with SCD (18-52%) are considerably higher than rates reported in general transfused population (0.2–2.8%)
Alloimmunization often makes finding compatible RBC products difficult and is also associated with:
Delayed hemolytic transfusion reactions (DHTRs)
Production of autoantibody
Decrease in red blood cell survival
Increased transfusion requirement
4
Red blood cell alloimmunization
Prophylactic serologic matching
Prophylactic genotypic matching
Transfusion strategies proposed to mitigate alloimmunization in SCD
Transfusion protocols with limited or extended RBC antigen matching reduces antibody formation
No consensus to the best practical approach
Cost effectiveness is controversial
Provision of RH genotype-matched RBCs
5
serologic matching x genotypic matching
Transfusion strategies proposed to mitigate alloimmunization in SCD
Evaluate the effect prophylactic genotypic matching and serologic
matching have on alloimmunization and hemolytic transfusion
reactions in patients with SCD receiving regular transfusions
Objective
6
Prospective study
March/2016-March/2021 (5 years)
29 patients with SCD
(HgbSS)
15 patients received prophylactic RBC transfusions serologicmatched for ABO, Rh, K, Fya/Fyb, Jka/Jkb and S/s antigens
Number of transfusions, RBC phenotype/genotype of the patient and received unit and presence of antibodies were registered for all patients
Antibodies were classified as allo-antibodies based on the
serologic testing, RBC phenotyping and RBC genotyping
The clinical significance of the antibody was accessed by
comparison of the hemoglobin (Hb) levels recorded before and
after transfusion at time of antibody detection
14 patients received prophylactic RBC transfusions genotypicmatched for ABO, Rh, K, Fya/Fyb, Jka/Jkb, S/s, Dia, Doa/Dob antigensand Rh variants
Patients and donors were from Hemocentro
Unicamp, Campinas, SP, Brazil
7
Methods
Serology
Phenotyping and antibody screening were performed by gel test
Adsorption onto autologous RBC was performed to aid the
differentiation of auto and alloantibodies
D C E Jkb sSc e K Fya Fyb Jka Dia
Molecular biology
Performed by LDTs, HEA BeadChip , RHD BeadChip, RHCE BeadChip
8
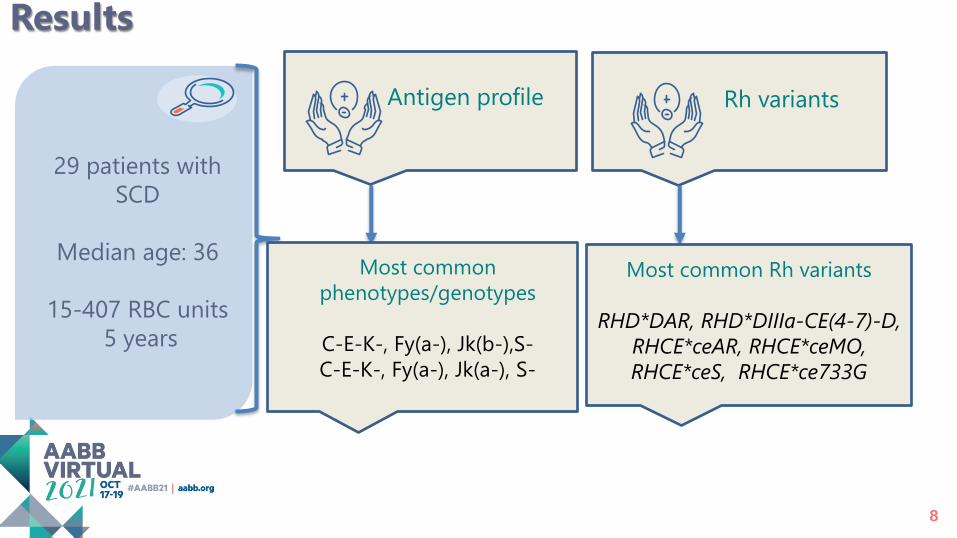
Results
29 patients with
SCD
Median age: 36
15-407 RBC units
5 years
Antigen profile Rh variants
Most common
phenotypes/genotypes
C-E-K-, Fy(a-), Jk(b-),S-
C-E-K-, Fy(a-), Jk(a-), S-
Most common Rh variants
RHD*DAR, RHD*DIIIa-CE(4-7)-D,
RHCE*ceAR, RHCE*ceMO,
RHCE*ceS, RHCE*ce733G
9
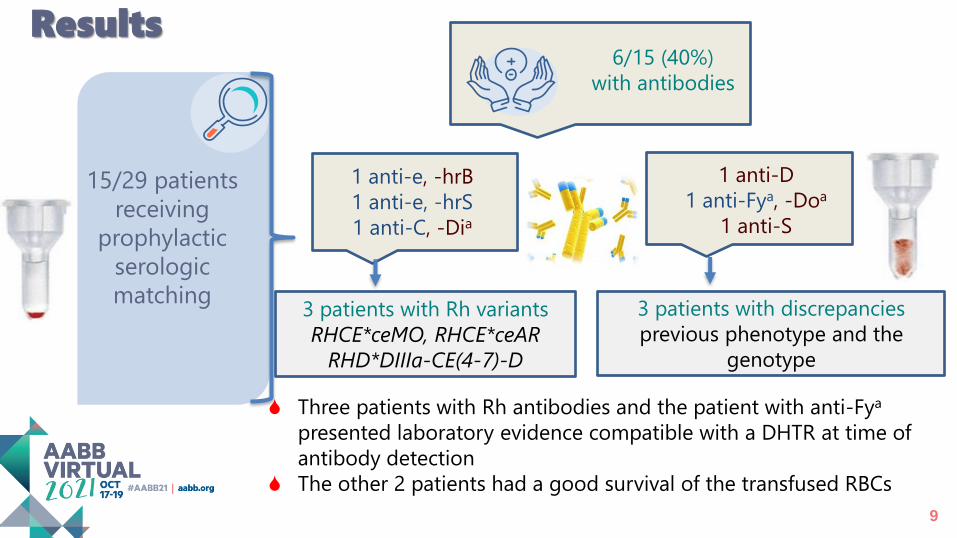
15/29 patients
receiving
prophylactic
serologic
matching
6/15 (40%)
with antibodies
1 anti-D
1 anti-Fya, -Doa
1 anti-S
1 anti-e, -hrB
1 anti-e, -hrS
1 anti-C, -Dia
3 patients with Rh variants
RHCE*ceMO, RHCE*ceAR
RHD*DIIIa-CE(4-7)-D
3 patients with discrepancies
previous phenotype and the
genotype
Results
Three patients with Rh antibodies and the patient with anti-Fya
presented laboratory evidence compatible with a DHTR at time of
antibody detection
The other 2 patients had a good survival of the transfused RBCs
10
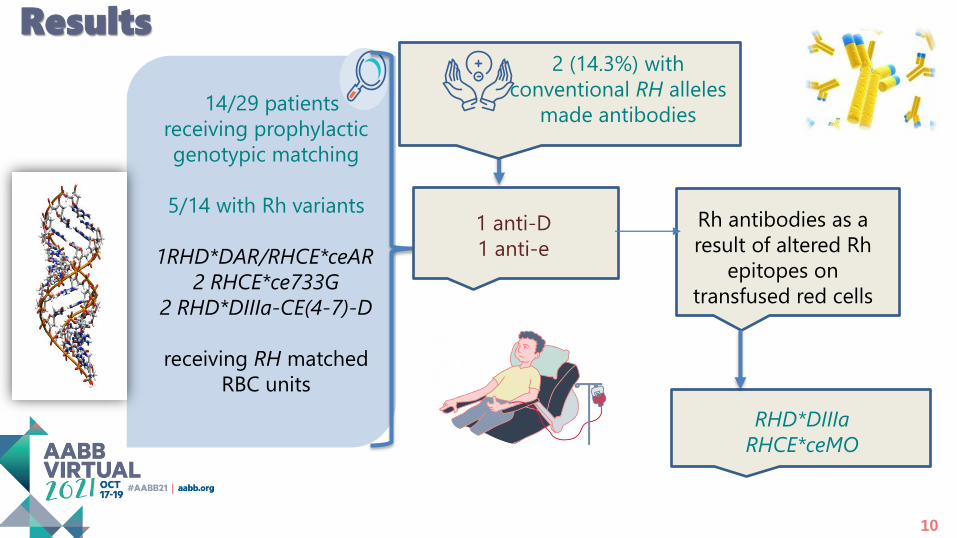
14/29 patients
receiving prophylactic
genotypic matching
5/14 with Rh variants
1RHD*DAR/RHCE*ceAR
2 RHCE*ce733G
2 RHD*DIIIa-CE(4-7)-D
receiving RH matched
RBC units
2 (14.3%) with
conventional RH alleles
made antibodies
Rh antibodies as a
result of altered Rh
epitopes on
transfused red cells
RHD*DIIIa
RHCE*ceMO
1 anti-D
1 anti-e
Results
11
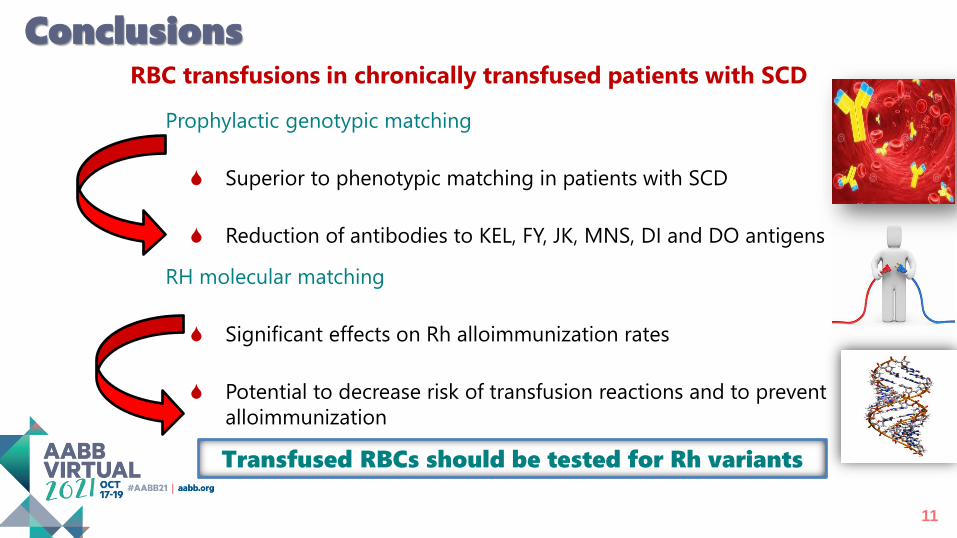
Conclusions
Prophylactic genotypic matching
Superior to phenotypic matching in patients with SCD
Reduction of antibodies to KEL, FY, JK, MNS, DI and DO antigens
RBC transfusions in chronically transfused patients with SCD
RH molecular matching
Significant effects on Rh alloimmunization rates
Potential to decrease risk of transfusion reactions and to prevent
alloimmunization
Transfused RBCs should be tested for Rh variants
12
IMPACT OF PROPHYLACTIC RBC TRANSFUSION WITH EXTENDED GENOTYPIC
MATCHING INCLUDING RH VARIANTS IN PATIENTS WITH SCD
Challenges
Transfusion of non-matched RBC units in another hospital
Presence of RH variant alleles in blood donors and risk of alloimmunization
Increased racial admixture of African and European genomes in blood donors
Antigenic differences in relation to patients with SCD
Finding good approaches for screening donors with homozygous
genotypes and RH variants