
Comparison of Magnetic Auriculotherapy, Laser ...
20
Research Article Comparison of Magnetic Auriculotherapy, Laser Auriculotherapy and Their Combination for Treatment of Insomnia in the Elderly: A Double-Blinded Randomised Trial Lorna K. P. Suen , 1 A. Molassiotis, 1 S. K. W. Yueng, 1 and C. H. Yeh 2 1 School of Nursing, e Hong Kong Polytechnic University, Hung Hom, Hong Kong 2 School of Nursing, Johns Hopkins University, 525 N. Wolfe St., Room 421, Baltimore, MD 21205, USA Correspondence should be addressed to Lorna K. P. Suen; [email protected] Received 2 April 2019; Accepted 7 May 2019; Published 21 May 2019 Academic Editor: Mario Ledda Copyright © 2019 Lorna K. P. Suen et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Insomnia is common amongst the elderly. With the adverse effects of prolonged use of hypnotics, the exploration of noninvasive and nonpharmacological complementary methods for insomnia is warranted. Auriculotherapy (AT) is a therapeutic approach where specific points on the auricle are stimulated to manage various physiological disorders. e purpose of this study is to determine the desirable treatment modality using AT to improve the sleep conditions of the elderly. Methods. A three- arm double-blinded randomised trial was conducted on 145 eligible subjects. is study investigated three minimally invasive procedures, namely, laser auriculotherapy (LAT), magneto-auriculotherapy (MAT), and their combination. Seven auricular points were used. Treatment was performed three times a week, for six weeks. Subjects were assessed at baseline, six weeks, and follow-up aſter six weeks, three months, and six months. Generalised estimating equations were used to evaluate interactions amongst the groups over time based on the Pittsburgh Sleep Quality Index (PSQI), sleep parameters using actigraphic monitoring, health-related quality of life (HRQOL) using SF-12, and PHQ-9 for depression status. Results. e treatment effects of the three procedures were comparable. Significant improvements were found in all of the subjective measures (PSQI, HRQOL, and PHQ-9) for individual groups over time. Improvements in the objective sleep parameters using actigraphic monitoring were detected in subjects who received MAT procedures but not in those who received LAT. e combined MAT and LAT approach did not show any advantage over MAT. Conclusions. e treatment effects of the three procedures were comparable in subjective parameters but not by objective measures using actigraphic monitoring. Longer therapeutic course and more frequent administration of LAT may be considered in future trials to achieve the optimal treatment effect. Trial Registration. is trial is registered with ClinicalTrials.gov: NCT02970695, registered May 2016. 1. Background Insomnia is common amongst the elderly, and in some countries, the reported prevalence rate is over 60% [1]. Elderly people have difficulty falling asleep and maintaining sleep due to frequent awakenings [1]. Sleep loss in the aging population is associated with depression, anxiety, increased suicidal risks, comorbid chronic conditions, and high fre- quency of accidents and falls [2–4]. Moreover, chronic sleep disturbance can seriously compromise the overall quality of life of those who suffer from it [5, 6]. Given the adverse effects of prolonged use of hypnotics, such as morning sedation, impaired balance, drug dependence, depression, and amnesia [1, 7], the exploration of noninvasive and nonpharmaco- logical complementary methods for insomnia amongst the elderly is warranted. Auriculotherapy (AT) is a traditional Chinese medicine (TCM) approach in which the ear is viewed as a microsystem of the body [8]. AT is a therapeutic method where specific points on the auricle are stimulated to treat various bodily disorders. Different materials, such as acupuncture needles, press tack needles, seeds, magnetic pellets, or low-energy laser, could be applied on auricular points (denoted as “acu- points” in this paper) located on the external ear for therapeu- tic effect [8–11]. However, auricular acupuncture may induce patients’ discomfort and cause infection and inflammation Hindawi Evidence-Based Complementary and Alternative Medicine Volume 2019, Article ID 3651268, 19 pages https://doi.org/10.1155/2019/3651268
Transcript of Comparison of Magnetic Auriculotherapy, Laser ...

Research ArticleComparison of Magnetic AuriculotherapyLaser Auriculotherapy and Their Combination for Treatment ofInsomnia in the Elderly A Double-Blinded Randomised Trial
Lorna K P Suen 1 A Molassiotis1 S K W Yueng1 and C H Yeh 2
1School of Nursing The Hong Kong Polytechnic University Hung Hom Hong Kong2School of Nursing Johns Hopkins University 525 N Wolfe St Room 421 Baltimore MD 21205 USA
Correspondence should be addressed to Lorna K P Suen lornasuenpolyueduhk
Received 2 April 2019 Accepted 7 May 2019 Published 21 May 2019
Academic Editor Mario Ledda
Copyright copy 2019 Lorna K P Suen et alThis is an open access article distributed under theCreative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Background Insomnia is common amongst the elderly With the adverse effects of prolonged use of hypnotics the exploration ofnoninvasive and nonpharmacological complementary methods for insomnia is warranted Auriculotherapy (AT) is a therapeuticapproach where specific points on the auricle are stimulated to manage various physiological disorders The purpose of this studyis to determine the desirable treatment modality using AT to improve the sleep conditions of the elderly Methods A three-arm double-blinded randomised trial was conducted on 145 eligible subjects This study investigated three minimally invasiveprocedures namely laser auriculotherapy (LAT) magneto-auriculotherapy (MAT) and their combination Seven auricular pointswere used Treatment was performed three times a week for six weeks Subjects were assessed at baseline six weeks and follow-upafter six weeks three months and six months Generalised estimating equations were used to evaluate interactions amongst thegroups over time based on the Pittsburgh SleepQuality Index (PSQI) sleep parameters using actigraphicmonitoring health-relatedquality of life (HRQOL) using SF-12 and PHQ-9 for depression status Results The treatment effects of the three procedures werecomparable Significant improvements were found in all of the subjective measures (PSQI HRQOL and PHQ-9) for individualgroups over time Improvements in the objective sleep parameters using actigraphic monitoring were detected in subjects whoreceived MAT procedures but not in those who received LATThe combined MAT and LAT approach did not show any advantageoverMATConclusionsThe treatment effects of the three procedures were comparable in subjective parameters but not by objectivemeasures using actigraphicmonitoring Longer therapeutic course andmore frequent administration of LATmay be considered infuture trials to achieve the optimal treatment effectTrial Registration This trial is registeredwith ClinicalTrialsgov NCT02970695registered May 2016
1 Background
Insomnia is common amongst the elderly and in somecountries the reported prevalence rate is over 60 [1] Elderlypeople have difficulty falling asleep and maintaining sleepdue to frequent awakenings [1] Sleep loss in the agingpopulation is associated with depression anxiety increasedsuicidal risks comorbid chronic conditions and high fre-quency of accidents and falls [2ndash4] Moreover chronic sleepdisturbance can seriously compromise the overall quality oflife of those who suffer from it [5 6] Given the adverse effectsof prolonged use of hypnotics such as morning sedationimpaired balance drug dependence depression and amnesia
[1 7] the exploration of noninvasive and nonpharmaco-logical complementary methods for insomnia amongst theelderly is warranted
Auriculotherapy (AT) is a traditional Chinese medicine(TCM) approach in which the ear is viewed as a microsystemof the body [8] AT is a therapeutic method where specificpoints on the auricle are stimulated to treat various bodilydisorders Different materials such as acupuncture needlespress tack needles seeds magnetic pellets or low-energylaser could be applied on auricular points (denoted as ldquoacu-pointsrdquo in this paper) located on the external ear for therapeu-tic effect [8ndash11] However auricular acupuncture may inducepatientsrsquo discomfort and cause infection and inflammation
HindawiEvidence-Based Complementary and Alternative MedicineVolume 2019 Article ID 3651268 19 pageshttpsdoiorg10115520193651268
2 Evidence-Based Complementary and Alternative Medicine
in the puncture sites Magneto-auriculotherapy (MAT) hasgradually emerged as a popular intervention for treatingmany chronic problems such as insomnia [12] low backpain [13] constipation [14] and hypertension [15] Theeffectiveness of magnetic pellets may be attributed to thefunctional changes caused by the interaction of magneticfields with biological tissues Such changes may be related tomoving ions in blood [16]
Laser auriculotherapy (LAT) has also been widely usedin different medical conditions including insomnia [17]pain relief [18] and weight reduction [19] The combinationof LAT and other treatments proposed in the literatureproduces a synergistic effect LAT has been combined withear point pressing to treat bed wetting in children [20] andwith auricular pressing therapy for alcoholic addiction [21]According to TCM the laser beam irradiates and stimulatesthe acupoint and activates the therapeutic effects of qi (energyflow) thereby regulating the functions of zang-fu (internalorgans) and restoring yin-yang (equilibrium) to produce atherapeutic effect [22]
Laser treatment is noninvasive painless and presentsno risk of infection or cross infection [22] As such thetherapeutic benefits of laser combined with MAT meritfurther investigation LAT followed by MAT optimises thetherapeutic effect because the latter allows continuous stim-ulation of acupoints after the laser treatment as long as themagnet pellets on the ears are in situ
In this study three minimally invasive proceduresnamely LAT MAT and their combination were investigatedto determine the desirable treatment modality using ATto improve the sleep conditions of the elderly Comparedwith the separate treatment procedures of MAT and LATtheir combined used is hypothesised to be more effective inimproving the sleep conditions and thereby the quality of lifeof the elderly with insomnia
2 Methods
21 Design This study employed a three-arm double-blindedrandomised trial Eligible subjects were randomly dividedinto three groups by using a computer-generated randomisedtable and the equal proportion rule (111)The randomcodingwas concealed from the subjects and evaluator by usingopaque envelopes
211 Settings and Participants Through convenience sam-pling subjects were recruited from elderly centres in HongKong A recruitment talk on AT was given to potentialsubjects in the targeted elderly centres The definition ofinsomnia is adapted from existing literature [23] After apreliminary screening volunteers aged 65 years or abovewere recruited if they have the following symptoms (1)difficulty falling or staying asleep andor frequent noctur-nal awakenings at least three nights per week (2) sleepdisturbance lasting for a minimum of 6 months and (3)poor quality of sleep as indicated by a PSQI score greaterthan five All the subjects fulfilled the criteria stipulated forthe diagnosis of insomnia in the lsquoDiagnostic and StatisticalManual of Mental Disordersrsquo fifth edition [24]The exclusion
criteria were as follows (1) presence of profound physicalillnesses such as stroke (2) diagnosis of obstructive sleepapnoea (3) wearing a hearing aid or pacemaker in situ(to prevent the magnetic pellets from interfering with thedevices) (4) received ATwithin the preceding sixmonths (5)suffering from aural injuries or infections and (6) inability tounderstand instructions or provide consent
22 Intervention and Procedures
221 Acupoints Selection Seven auricular points namelyldquoshenmenrdquo ldquoheartrdquo ldquoliverrdquo ldquospleenrdquo ldquokidneyrdquo ldquoocciputrdquoand ldquosubcortexrdquo (Figure 1) were selected because they pro-mote sleep as verified in a previous study by the first author[12] The selection was based on the nomenclature andlocation of acupoints published by the China StandardisationOrganising Committee (GBT 13734-2008) [25] Therapywas delivered by research personnel (SY) who had receivedintensive coaching from the first author (LS) Establishing theinterrater reliability and accuracy of the ear point identifica-tion scheme ensured the fidelity of the study
222 Groupings Group 1 (Placebo LAT and MAT) The laserdevice was switched to ldquopower offrdquo mode (ie deactivated)for acupoint lsquostimulationrsquo to achieve blinding and the placeboeffect before the MATThe subjects were asked to wear a pairof laser-protective goggles to lsquoblindrsquo them during treatmentMAT was then applied by placing magnetic pellets on theselected acupoints (Figure 2) Each magnetic pellet has anaverage gausspellet magnetic flux density of approximately200 Gs (20 mT) and a diameter of 176 mm
Group 2 (LAT and Placebo MAT) A laser device (PointerPulse) was used for LATThedevice has a wavelength of 650nm average output power of 25 mW energy density of 054Jcm2 for 1 minute and a pulse of 10Hz which is a commonlyacceptable dosage for clinical use [18 26] LAT used low-levellaser therapy (LLLT) in which the energy level emitted fromthe device is comparable with that of the teaching pointerThecontinuous mode of the device was used to directly treat theacupoints for one minute (Figure 3) A plaster centred with asmall dried stem of Junci medulla a soft perennial plant wasprovided to mimic MAT In a previous study J medulla wassuccessfully adopted as a placebo because it did not induceany physical pressure on the acupoints of the ear [12]
Group 3 (Combined AT) The subjects received the com-bined LAT and MAT The procedures for applying LAT andMAT were identical to the abovementioned descriptions
223 Procedures Therapies were administered at elderlycentres adjacent to the subjectsrsquo residences The followingprocedures were standardised across the three groups toenhance the blinding effect All therapies were administeredin a room assigned for research purposes Laser-protectivegoggles specific for the wavelengths of the laser device wereprovided to the subjects and researchers for eye protection
The auricle of every subject was cleaned with 75 iso-propyl alcohol before therapy Only one ear was treated at atimeThe treatment was applied alternately to the right ear inthe first visit and then to the left ear in the subsequent visit
Evidence-Based Complementary and Alternative Medicine 3
Shenmen
Spleen
Subcortex
Internal acupoint
Occiput
Heart
Liver
Kidney
Figure 1 Selected auricular points for insomnia
Figure 2 Administration of magneto-auriculotherapy
We replaced the experimental objects (ie magnetic pelletsfor true MAT or J medulla for placebo MAT) every otherday that is three times a week (except Sunday) to preventlocal irritation of acupoints The total treatment period wassix weeks
Participation in the study was voluntary Writteninformed consent was obtained from each subject uponexplaining the risks and benefits of their participationEthical approval was obtained from the Human ResearchEthics Review Committee of the Hong Kong PolytechnicUniversity The study was conducted in accordance with theDeclaration of Helsinki Given their multiple visits to thecentres to receive treatment the subjects were provided atravel subsidy in the form of supermarket coupons uponcompletion of the study
224 Treatment Effect Evaluation Thesubjectswere assessedat baseline at six weeks (postintervention) and duringfollow-up after six weeks three months and six months Toachieve evaluator blinding the assessment was conductedby a different researcher who was unaware of the treatmentmodality given to the subjects PSQI which was used tocollect data related to the sleep conditions of the subjectswas considered as the primary outcomeThis instrument wasscored from 0 to 21 and scores greater than five indicatedpoor sleep quality Chong andCheung [27] validated theCan-tonese PSQI and reported a high internal consistency of 075
The secondary outcomes considered are as follows(1) actigraphic monitoring was conducted to collect sleepparameters including sleep latency (minutes) waking aftersleep onset (minutes) total sleep time (hours) and sleep
4 Evidence-Based Complementary and Alternative Medicine
Figure 3 Administration of laser auriculotherapy
efficiency () An Actiwatchrsquo Spectrum Plus device with0025G ultra-high sensitivity and 32 Hz sampling rate wasused in actigraphic monitoring The subjects were requestedto wear the device on the wrist of their nondominant hand 24hours a day for 7 consecutive days to determine the overallsleep conditions within a certain period Data were collectedin epochs every 30 second These epoch-by-epoch data werestored in the internal memory of the device until theycould be downloaded to a computer Actiware 6 ActigraphAnalysis Software was used for sleep analysis (2)TheChinese(HK) SF-12 v2copy an abbreviated version of the SF36 healthquestionnaire was used to evaluate the health-related qualityof life (HRQOL) of the subjects This instrument covered 12items and the resultswere presented by a physical componentscore (PCS) and a mental component score (MCS) PCS andMCS ranged from 0 to 100 with higher scores indicatingbetter HRQOL [28] (3) Patient Health Questionnaire (PHQ-9) was also used This instrument was validated as a usefultool for assessing depression status The scores ranged from0 to 27 and high scores indicated severe depression status[29] The scale had a Cronbachrsquos alpha of 082 and therecommended cut-off score was 8 [30]
The subjectsrsquo expectations and satisfaction towards thetherapy were evaluated using a 10-point scale with highscores indicating high expectations or satisfaction [31] Datawere likewise collected on sociodemographic characteris-tics including age gender marital status educational levelreligion number of family members body mass indexsingleshared bed comorbid illnesses use of sleeping pillsor aids and current medications taken Similarly monitoredwere the recruitment rate compliance rate of the treatmentprotocol and adverse effects arising from the therapy
225 Data Analyses Descriptive statistics were determinedon the sociodemographic and clinical characteristics of the
subjects The estimated mean and standard error were com-puted for the outcome variables of each time point Associa-tion amongst categorical variables was estimated using x2 testor Fisherrsquos exact test where appropriate to identify significantvariables for inclusion in the generalised estimating equa-tions (GEE) for adjustment One-way analysis of variancewas used to examine group differences Primary analysiswas conducted using GEE model with an autoregressioncorrelation structure to evaluate interactions amongst thegroups over time (baseline to six months follow-up) on theprimary outcome (ie PSQI score) and secondary outcomes(sleep parameters using 24-hour actigraphic monitoringquality of life using SF-12 and PHQ-9) Missing data werehandled usingGEE and assumed to be random [32]Themainanalysis was repeated at postintervention and during thefollow-up sessions (up to six months) for sensitivity analysisSPSS version 250 (IBM Corporation USA) was used for allstatistical analyses All statistical tests were two sided withsignificance level set at 005
3 Results
The study was conducted from May 2016 to May 2018Data were collected from 11 centres for the elderly and therecruitment rate was 886 A total of 147 eligible subjectswere randomly divided into three groups (Group 1=50Group2=46 and Group 3=51)
31 Participantsrsquo Characteristics The recruited subjects hadan average age of 7529 yearsplusmn 699 with a mean durationof insomnia for 1012 plusmn 1067 years Majority of the subjects(700) did not take any medication to manage their sleepproblems The groups were essentially comparable and wellbalanced in terms of sociodemographic variables includ-ing gender distribution body mass index education level
Evidence-Based Complementary and Alternative Medicine 5
marital status comorbid illnesses and regular medicationstaken However age showed slight significant differencesamongst the groups and thus this variable was adjusted inthe GEE models in subsequent analyses According to the24-hour actigraphic recordings the subjects had an averageof poor sleep quality (PSQI 1263 plusmn324 sleep efficiency7233 plusmn1609) long sleep latency (2703 plusmn 2313 minutes)short total sleep time (376 plusmn 196 hours) and waking aftersleep onset (9031plusmn 8853minutes)The subjects also hadmilddepression (PHQ-9 947 plusmn 607) and low HRQOL in termsof physical component (4139 plusmn 851) and mental component(4668 plusmn 1234) (Table 1)
32 Compliance Expectation and Satisfaction towards theTreatment Compliance with the intervention protocol washigh at an average of 952 (n = 140) of the subjects contin-ued with postintervention and all follow-up measurementsuntil six months The recruitment flowchart is illustrated inFigure 4 Althoughmajority of the subjects (653) had nevertried complementary and alternative treatments they gener-ally exhibited strong confidence in the proposed therapy (782of 10) and had a relatively high expectation of its effectiveness(773 of 10) before the trial After the intervention the subjectsin Group 1 had the highest satisfaction from the therapy(786) followed by those in Group 3 (758) and Group 2 (702)A correlation analysis was conducted between expectationsof the treatment effect and sleep parameters (PSQI SE)However no significant relationship was detected (pgt005)Over 75 of the subjects (n = 109) indicated that they woulddefinitely recommend the therapy to others No specificadverse effects were observed arising from the therapyapart from 16 cases (109) who reported having mild skinirritation on the ears due to the adhesive tapes that were usedto hold the experimental tools in place and 20 cases (136)who felt tenderness on the acupoints (most of these subjectsreceived MAT) The number of subjects who believed thatthey might be receiving placebo treatment was higher inGroup 1 than in the other groups although majority of thesubjects (90) believed that they were not receiving placebo(Table 2)
33 Treatment Effect The differences in the primary andsecondary outcomes of the three groups across differenttime points were compared through GEE model analysiswith adjustment for age In general no significant differ-ences were detected in the outcomes (including PSQI sleepparameters measured by actigraphic monitoring SF-12 andPHQ-9) of the three groups (Table 3) However significantdifferences were found in all of the subjective measuresincluding PSQI (Figure 5) SF-12 (physical andor mentalcomponents) (Figures S1 and S2) and PHQ-9 (Figure 6) forindividual groups over time When the sleep conditions wereevaluated by actigraphic monitoring significant differencesin lsquowaking after sleep onsetrsquo (minutes) (Figure S3) and lsquosleepefficiencyrsquo () (Figure S4) were detected only in Groups 1and 3 (Table 4) The completersrsquo analysis showed consistentfindings on the primary and secondary outcomes of thetrial
4 Discussion
Numerous studies that used AT to manage sleep problemsin China encountered methodological flaws which renderedtheir findings unconvincingThe commonproblems includedlack of details on how randomisation and allocation conceal-ment were conducted absence of objective measurementsand a control or placebo group as well as failure to report theuse of blinding and selective reporting of findings [33ndash35]The present study was performed using a scientific approachto identify the optimum treatment protocol forAT in improv-ing the sleep conditions and quality of life of the elderlywith insomnia This meticulous randomised controlled trial(RCT) could provide scientific evidence regarding causalrelationships between interventions and outcomes
In general the treatment effect was comparable amongstthe three AT protocols However significant improvementswere observed in all of the subjective measures includingsleep conditions measured by PSQI HRQOL and depressionstatus for individual groups over time When the sleepconditions were evaluated by objective measures using acti-graphic monitoring significant differences in ldquowaking aftersleep onsetrdquo (minutes) and ldquosleep efficiencyrdquo () were onlynoted in Groups 1 and 3 The use of actigraphs has beenwidely recognised as an objective measurement that couldprovide longitudinal assessment of sleep patterns in a naturalenvironment [36 37]This technique could similarly providevalidmeasures thatmay not be influenced by subject bias Sig-nificant reduction in the awakening time after sleep onset andincrease in sleep efficiency were only detected in subjects whoreceived MAT protocols (ie Groups 1 and 3) but not in thosewho received only the LAT protocol Despite the improvedsleep efficiency of the subjects at postintervention and duringthe follow-up periods the evaluated indices remained below85 a common cut-off percentage that indicates the presenceof sleep disturbances [38] Sleep efficiency is calculated bydividing the total sleep time by total bedtime a higher sleepefficiency means better sleep quantity and quality A longtherapeutic course such as 10ndash12 weeks may be necessaryto further elevate sleep efficiency to a desirable level throughsustainable treatment effect
MAT could provide continuous stimulation of acupointsas long as the magnetic pellets on the ears are in situ and thesubjects could receive laser stimulation to the acupoints onthe day of treatment The synergistic effect of the combinedMAT and LAT was demonstrated in two previous trials[39 40] conducted by the research team In a double-blindRCT for osteoarthritic knee the subjects who received thecombined AT protocols exhibited stronger treatment effectsin terms of pain relief ambulation status and range of kneemovements compared with those treated with separate MATor LAT [39] whereas in another double-blinded RCT foraging males with lower urinary tract symptoms a combinedAT protocol exhibited a stronger therapeutic effect in reliev-ing voiding problems improving the urinary flow rate andminimizing the postvoid residual urine than the placebogroup or MAT alone [40] However the combined MAT andLAT approach did not show any advantage over the separateMAT protocol in current studyTherefore a greater frequency
6 Evidence-Based Complementary and Alternative Medicine
Table1So
ciod
emograph
icandbaselin
echaracteristicso
fthe
participantssample(
N=147)
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Age
(years)
j0025lowast
Mean(SD)
7529(699)
7602(702)
7680(616
)7320(729)
Gender
Male
197
57
permil0907
Female
128
4341
44Ed
ucationlevel
Prim
aryor
below
100
3235
330734
Second
ary
3915
915
Tertiary
orabove
83
23
Marita
lstatus
Sing
le5
21
20971
Marrie
d82
2926
27DivorcedWidow
ed60
1919
22Re
ligion
No
7526
2227
permil0895
Yes
7224
2424
Body
massind
ex(kgm2)
2229(373)
2285(348)
2150(357)
2246(404)
j0076
Shared
bed
No
109
3338
38permil0188
Yes
3817
813
Living
alon
eNo
6620
2719
permil0079
Yes
8130
1932
Evidence-Based Complementary and Alternative Medicine 7
Table1Con
tinued
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Sleeping
pills
taken
No
103
3433
360391
Previous
user
3214
711
Currentu
ser
122
64
Durationof
insomnia
(years)
Mean(SD)
1012
(1067)
923(
834)
1115
(1309)
1006(1040
)j
0678
Com
orbidillness
No
225
512
permil0488
Yes
125
4541
39Re
gulard
rugs
taken
No
3210
715
permil044
1Yes
11540
3936
PSQI(total)(0-21)
1263(324)
1267(315
)1289(413
)1235(234)
j0715
Sleeplatency(
min)
2703(2313)
2656(2376)
2868(2486)
2600(2119)
j0839
Totalsleep
time(
hours)
376
(196)
393
(193)
374
(186)
362
(210
)j
0734
Wakea
ftersleep
onset
(minutes)
9031
(8853)
9206(914
4)9003(995
6)8886(7595)
j0984
Sleepeffi
ciency
()
7233
(1609)
7244(1591)
7425(
1604)
7050(1642)
j0521
SF-12(PCS
)4139
(851)
4065(758)
4143(969)
4207(836)
j0707
SF-12(M
CS)
4668(1234)
4822(117
6)46
19(1349)
4562(118
9)j
0542
PHQ-9
947(607)
954(534)
952(669)
935(
626)
j0986
SDstand
arddeviation
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
njOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
8 Evidence-Based Complementary and Alternative Medicine
Table2Re
ported
adversee
ffectsexpectationsand
satisfactiontowards
thetherapy
yen
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Havey
ouused
complem
entary
therapiesinthep
ast
permil0423
No
96(653
)33
3330
Yes
51(347
)17
1321
How
muchfaith
doyouhave
incomplem
entary
therapiesin
general
(0to
10)
782(213
)840
(194)
748(218
)75
5(218
)j
0056
Expectationfortreatmenteffect
towards
MAT
(0to
10)
741(210)
796(211)
693
(203)
731(207)
j0051
Expectationfortreatmenteffect
towards
LAT
(0to
10)
741(213)
808
(200)
687
(209)
725(
215)
j0016lowast
Averagee
xpectatio
nfor
treatmenteffect
(0to
10)
773(213
)840
(203)
720(203)
757(218
)j
0016lowast
Earitchinessyen
16(109
)8lowast
(resolve
automatically)
2lowast(resolve
automatically)
6lowast(resolve
automatically)
---
Evidence-Based Complementary and Alternative Medicine 9
Table2Con
tinued
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Tend
ernesson
acup
ointsyen
20(136
)9lowast
(resolve
automatically)
1lowast(resolve
automatically)
10lowast
(resolve
automatically)
---
Satisfactiontowards
therapy(
0to
10)yen
758(237
)78
6(203)
702(268)
758(237
)j
0225
Thou
ghtthattheymight
bereceivingplacebotre
atmentyen
No
126(900
)39
4146
0011lowast
Yes
14(100
)10
31
Will
recommendthistherapyto
othersyen
0166
Definitelywill
109(757
)38
2942
Maybe
20(139
)5
96
No
15(104
)6
72
Mean(stand
arddeviation)
unlessotherw
iseno
ted
ΩAssociatio
nbetweenvaria
bles
was
determ
ined
bychi-s
quarea
nalyseso
rFish
errsquos-exacttestw
here
approp
riate
Evaluated
beforetheinterventio
nyenE
valuated
after
theinterventionhasb
eencompleted
lowastldquoC
ertainrdquoc
ausality
jOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
10 Evidence-Based Complementary and Alternative Medicine
Table3Outcomev
ariables
acrossthreeg
roup
satd
ifferenttim
epoints
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PSQI(total)(0-21)
Baselin
e1268(044)
1290(062)
1234(034)
Postinterventio
n94
6(052
)99
1(055)
848
(051)
023
(-14
418
9)-065(
-23610
6)087
(-055230)
6we
eksfollowup
907(053
)92
5(065)
926(054)
-050(-207197)
053
(-114219)
-058(-254138)
3mon
thsfollowup
912(079)
781(068)
906(058)
-154(-400
093)
027
(-18
8242)
-181(-399037)
6-mon
thfollo
wup
820
(062)
796(067)
846
(066)
-047(-268175)
059
(-13
8256)
-106(-316105)
Sleeplatency(minutes)
Baselin
e2682(333
)2916
(359)
2517
(286)
Postinterventio
n2529(297)
2500(332
)2617
(303)
(-1329802)
223
(-8111257)
-486(-1533
560)
6we
eksfollowup
1935(322)
2656(339
)2368(330)
487
(-77
31747)
567
(-589172
3)-080(-11771018
)3m
onthsfollowup
1799
(337
)2129(356)
2390(422)
096
(-11491341)
725(
-6932143)
-629(-2065807)
6-mon
thfollo
wup
1966(531
)2342(539
)1907(434)
143(-15791864)
076
(-15341686)
067
(-15851718)
Totalslee
ptim
e(hours)
Baselin
e393
(027)
375
(028)
361
(030)
Postinterventio
n393
(249)
405
(030)
396
(029)
031(-067128)
035
(-065136)
-005(
-117108)
6we
eksfollowup
381
(027)
390
(029)
385
(025)
027
(06812
3)036
(-059131
)-009(-116099)
3mon
thsfollowup
366
(044)
426
(049)
338
(024)
077
(-081236)
0034(-13
213
9)074
(-061209)
6-mon
thfollo
wup
392
(049)
442
(061)
371
(045)
068
(-10
3238)
0112(-14
516
8)057
(-114227)
Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

2 Evidence-Based Complementary and Alternative Medicine
in the puncture sites Magneto-auriculotherapy (MAT) hasgradually emerged as a popular intervention for treatingmany chronic problems such as insomnia [12] low backpain [13] constipation [14] and hypertension [15] Theeffectiveness of magnetic pellets may be attributed to thefunctional changes caused by the interaction of magneticfields with biological tissues Such changes may be related tomoving ions in blood [16]
Laser auriculotherapy (LAT) has also been widely usedin different medical conditions including insomnia [17]pain relief [18] and weight reduction [19] The combinationof LAT and other treatments proposed in the literatureproduces a synergistic effect LAT has been combined withear point pressing to treat bed wetting in children [20] andwith auricular pressing therapy for alcoholic addiction [21]According to TCM the laser beam irradiates and stimulatesthe acupoint and activates the therapeutic effects of qi (energyflow) thereby regulating the functions of zang-fu (internalorgans) and restoring yin-yang (equilibrium) to produce atherapeutic effect [22]
Laser treatment is noninvasive painless and presentsno risk of infection or cross infection [22] As such thetherapeutic benefits of laser combined with MAT meritfurther investigation LAT followed by MAT optimises thetherapeutic effect because the latter allows continuous stim-ulation of acupoints after the laser treatment as long as themagnet pellets on the ears are in situ
In this study three minimally invasive proceduresnamely LAT MAT and their combination were investigatedto determine the desirable treatment modality using ATto improve the sleep conditions of the elderly Comparedwith the separate treatment procedures of MAT and LATtheir combined used is hypothesised to be more effective inimproving the sleep conditions and thereby the quality of lifeof the elderly with insomnia
2 Methods
21 Design This study employed a three-arm double-blindedrandomised trial Eligible subjects were randomly dividedinto three groups by using a computer-generated randomisedtable and the equal proportion rule (111)The randomcodingwas concealed from the subjects and evaluator by usingopaque envelopes
211 Settings and Participants Through convenience sam-pling subjects were recruited from elderly centres in HongKong A recruitment talk on AT was given to potentialsubjects in the targeted elderly centres The definition ofinsomnia is adapted from existing literature [23] After apreliminary screening volunteers aged 65 years or abovewere recruited if they have the following symptoms (1)difficulty falling or staying asleep andor frequent noctur-nal awakenings at least three nights per week (2) sleepdisturbance lasting for a minimum of 6 months and (3)poor quality of sleep as indicated by a PSQI score greaterthan five All the subjects fulfilled the criteria stipulated forthe diagnosis of insomnia in the lsquoDiagnostic and StatisticalManual of Mental Disordersrsquo fifth edition [24]The exclusion
criteria were as follows (1) presence of profound physicalillnesses such as stroke (2) diagnosis of obstructive sleepapnoea (3) wearing a hearing aid or pacemaker in situ(to prevent the magnetic pellets from interfering with thedevices) (4) received ATwithin the preceding sixmonths (5)suffering from aural injuries or infections and (6) inability tounderstand instructions or provide consent
22 Intervention and Procedures
221 Acupoints Selection Seven auricular points namelyldquoshenmenrdquo ldquoheartrdquo ldquoliverrdquo ldquospleenrdquo ldquokidneyrdquo ldquoocciputrdquoand ldquosubcortexrdquo (Figure 1) were selected because they pro-mote sleep as verified in a previous study by the first author[12] The selection was based on the nomenclature andlocation of acupoints published by the China StandardisationOrganising Committee (GBT 13734-2008) [25] Therapywas delivered by research personnel (SY) who had receivedintensive coaching from the first author (LS) Establishing theinterrater reliability and accuracy of the ear point identifica-tion scheme ensured the fidelity of the study
222 Groupings Group 1 (Placebo LAT and MAT) The laserdevice was switched to ldquopower offrdquo mode (ie deactivated)for acupoint lsquostimulationrsquo to achieve blinding and the placeboeffect before the MATThe subjects were asked to wear a pairof laser-protective goggles to lsquoblindrsquo them during treatmentMAT was then applied by placing magnetic pellets on theselected acupoints (Figure 2) Each magnetic pellet has anaverage gausspellet magnetic flux density of approximately200 Gs (20 mT) and a diameter of 176 mm
Group 2 (LAT and Placebo MAT) A laser device (PointerPulse) was used for LATThedevice has a wavelength of 650nm average output power of 25 mW energy density of 054Jcm2 for 1 minute and a pulse of 10Hz which is a commonlyacceptable dosage for clinical use [18 26] LAT used low-levellaser therapy (LLLT) in which the energy level emitted fromthe device is comparable with that of the teaching pointerThecontinuous mode of the device was used to directly treat theacupoints for one minute (Figure 3) A plaster centred with asmall dried stem of Junci medulla a soft perennial plant wasprovided to mimic MAT In a previous study J medulla wassuccessfully adopted as a placebo because it did not induceany physical pressure on the acupoints of the ear [12]
Group 3 (Combined AT) The subjects received the com-bined LAT and MAT The procedures for applying LAT andMAT were identical to the abovementioned descriptions
223 Procedures Therapies were administered at elderlycentres adjacent to the subjectsrsquo residences The followingprocedures were standardised across the three groups toenhance the blinding effect All therapies were administeredin a room assigned for research purposes Laser-protectivegoggles specific for the wavelengths of the laser device wereprovided to the subjects and researchers for eye protection
The auricle of every subject was cleaned with 75 iso-propyl alcohol before therapy Only one ear was treated at atimeThe treatment was applied alternately to the right ear inthe first visit and then to the left ear in the subsequent visit
Evidence-Based Complementary and Alternative Medicine 3
Shenmen
Spleen
Subcortex
Internal acupoint
Occiput
Heart
Liver
Kidney
Figure 1 Selected auricular points for insomnia
Figure 2 Administration of magneto-auriculotherapy
We replaced the experimental objects (ie magnetic pelletsfor true MAT or J medulla for placebo MAT) every otherday that is three times a week (except Sunday) to preventlocal irritation of acupoints The total treatment period wassix weeks
Participation in the study was voluntary Writteninformed consent was obtained from each subject uponexplaining the risks and benefits of their participationEthical approval was obtained from the Human ResearchEthics Review Committee of the Hong Kong PolytechnicUniversity The study was conducted in accordance with theDeclaration of Helsinki Given their multiple visits to thecentres to receive treatment the subjects were provided atravel subsidy in the form of supermarket coupons uponcompletion of the study
224 Treatment Effect Evaluation Thesubjectswere assessedat baseline at six weeks (postintervention) and duringfollow-up after six weeks three months and six months Toachieve evaluator blinding the assessment was conductedby a different researcher who was unaware of the treatmentmodality given to the subjects PSQI which was used tocollect data related to the sleep conditions of the subjectswas considered as the primary outcomeThis instrument wasscored from 0 to 21 and scores greater than five indicatedpoor sleep quality Chong andCheung [27] validated theCan-tonese PSQI and reported a high internal consistency of 075
The secondary outcomes considered are as follows(1) actigraphic monitoring was conducted to collect sleepparameters including sleep latency (minutes) waking aftersleep onset (minutes) total sleep time (hours) and sleep
4 Evidence-Based Complementary and Alternative Medicine
Figure 3 Administration of laser auriculotherapy
efficiency () An Actiwatchrsquo Spectrum Plus device with0025G ultra-high sensitivity and 32 Hz sampling rate wasused in actigraphic monitoring The subjects were requestedto wear the device on the wrist of their nondominant hand 24hours a day for 7 consecutive days to determine the overallsleep conditions within a certain period Data were collectedin epochs every 30 second These epoch-by-epoch data werestored in the internal memory of the device until theycould be downloaded to a computer Actiware 6 ActigraphAnalysis Software was used for sleep analysis (2)TheChinese(HK) SF-12 v2copy an abbreviated version of the SF36 healthquestionnaire was used to evaluate the health-related qualityof life (HRQOL) of the subjects This instrument covered 12items and the resultswere presented by a physical componentscore (PCS) and a mental component score (MCS) PCS andMCS ranged from 0 to 100 with higher scores indicatingbetter HRQOL [28] (3) Patient Health Questionnaire (PHQ-9) was also used This instrument was validated as a usefultool for assessing depression status The scores ranged from0 to 27 and high scores indicated severe depression status[29] The scale had a Cronbachrsquos alpha of 082 and therecommended cut-off score was 8 [30]
The subjectsrsquo expectations and satisfaction towards thetherapy were evaluated using a 10-point scale with highscores indicating high expectations or satisfaction [31] Datawere likewise collected on sociodemographic characteris-tics including age gender marital status educational levelreligion number of family members body mass indexsingleshared bed comorbid illnesses use of sleeping pillsor aids and current medications taken Similarly monitoredwere the recruitment rate compliance rate of the treatmentprotocol and adverse effects arising from the therapy
225 Data Analyses Descriptive statistics were determinedon the sociodemographic and clinical characteristics of the
subjects The estimated mean and standard error were com-puted for the outcome variables of each time point Associa-tion amongst categorical variables was estimated using x2 testor Fisherrsquos exact test where appropriate to identify significantvariables for inclusion in the generalised estimating equa-tions (GEE) for adjustment One-way analysis of variancewas used to examine group differences Primary analysiswas conducted using GEE model with an autoregressioncorrelation structure to evaluate interactions amongst thegroups over time (baseline to six months follow-up) on theprimary outcome (ie PSQI score) and secondary outcomes(sleep parameters using 24-hour actigraphic monitoringquality of life using SF-12 and PHQ-9) Missing data werehandled usingGEE and assumed to be random [32]Themainanalysis was repeated at postintervention and during thefollow-up sessions (up to six months) for sensitivity analysisSPSS version 250 (IBM Corporation USA) was used for allstatistical analyses All statistical tests were two sided withsignificance level set at 005
3 Results
The study was conducted from May 2016 to May 2018Data were collected from 11 centres for the elderly and therecruitment rate was 886 A total of 147 eligible subjectswere randomly divided into three groups (Group 1=50Group2=46 and Group 3=51)
31 Participantsrsquo Characteristics The recruited subjects hadan average age of 7529 yearsplusmn 699 with a mean durationof insomnia for 1012 plusmn 1067 years Majority of the subjects(700) did not take any medication to manage their sleepproblems The groups were essentially comparable and wellbalanced in terms of sociodemographic variables includ-ing gender distribution body mass index education level
Evidence-Based Complementary and Alternative Medicine 5
marital status comorbid illnesses and regular medicationstaken However age showed slight significant differencesamongst the groups and thus this variable was adjusted inthe GEE models in subsequent analyses According to the24-hour actigraphic recordings the subjects had an averageof poor sleep quality (PSQI 1263 plusmn324 sleep efficiency7233 plusmn1609) long sleep latency (2703 plusmn 2313 minutes)short total sleep time (376 plusmn 196 hours) and waking aftersleep onset (9031plusmn 8853minutes)The subjects also hadmilddepression (PHQ-9 947 plusmn 607) and low HRQOL in termsof physical component (4139 plusmn 851) and mental component(4668 plusmn 1234) (Table 1)
32 Compliance Expectation and Satisfaction towards theTreatment Compliance with the intervention protocol washigh at an average of 952 (n = 140) of the subjects contin-ued with postintervention and all follow-up measurementsuntil six months The recruitment flowchart is illustrated inFigure 4 Althoughmajority of the subjects (653) had nevertried complementary and alternative treatments they gener-ally exhibited strong confidence in the proposed therapy (782of 10) and had a relatively high expectation of its effectiveness(773 of 10) before the trial After the intervention the subjectsin Group 1 had the highest satisfaction from the therapy(786) followed by those in Group 3 (758) and Group 2 (702)A correlation analysis was conducted between expectationsof the treatment effect and sleep parameters (PSQI SE)However no significant relationship was detected (pgt005)Over 75 of the subjects (n = 109) indicated that they woulddefinitely recommend the therapy to others No specificadverse effects were observed arising from the therapyapart from 16 cases (109) who reported having mild skinirritation on the ears due to the adhesive tapes that were usedto hold the experimental tools in place and 20 cases (136)who felt tenderness on the acupoints (most of these subjectsreceived MAT) The number of subjects who believed thatthey might be receiving placebo treatment was higher inGroup 1 than in the other groups although majority of thesubjects (90) believed that they were not receiving placebo(Table 2)
33 Treatment Effect The differences in the primary andsecondary outcomes of the three groups across differenttime points were compared through GEE model analysiswith adjustment for age In general no significant differ-ences were detected in the outcomes (including PSQI sleepparameters measured by actigraphic monitoring SF-12 andPHQ-9) of the three groups (Table 3) However significantdifferences were found in all of the subjective measuresincluding PSQI (Figure 5) SF-12 (physical andor mentalcomponents) (Figures S1 and S2) and PHQ-9 (Figure 6) forindividual groups over time When the sleep conditions wereevaluated by actigraphic monitoring significant differencesin lsquowaking after sleep onsetrsquo (minutes) (Figure S3) and lsquosleepefficiencyrsquo () (Figure S4) were detected only in Groups 1and 3 (Table 4) The completersrsquo analysis showed consistentfindings on the primary and secondary outcomes of thetrial
4 Discussion
Numerous studies that used AT to manage sleep problemsin China encountered methodological flaws which renderedtheir findings unconvincingThe commonproblems includedlack of details on how randomisation and allocation conceal-ment were conducted absence of objective measurementsand a control or placebo group as well as failure to report theuse of blinding and selective reporting of findings [33ndash35]The present study was performed using a scientific approachto identify the optimum treatment protocol forAT in improv-ing the sleep conditions and quality of life of the elderlywith insomnia This meticulous randomised controlled trial(RCT) could provide scientific evidence regarding causalrelationships between interventions and outcomes
In general the treatment effect was comparable amongstthe three AT protocols However significant improvementswere observed in all of the subjective measures includingsleep conditions measured by PSQI HRQOL and depressionstatus for individual groups over time When the sleepconditions were evaluated by objective measures using acti-graphic monitoring significant differences in ldquowaking aftersleep onsetrdquo (minutes) and ldquosleep efficiencyrdquo () were onlynoted in Groups 1 and 3 The use of actigraphs has beenwidely recognised as an objective measurement that couldprovide longitudinal assessment of sleep patterns in a naturalenvironment [36 37]This technique could similarly providevalidmeasures thatmay not be influenced by subject bias Sig-nificant reduction in the awakening time after sleep onset andincrease in sleep efficiency were only detected in subjects whoreceived MAT protocols (ie Groups 1 and 3) but not in thosewho received only the LAT protocol Despite the improvedsleep efficiency of the subjects at postintervention and duringthe follow-up periods the evaluated indices remained below85 a common cut-off percentage that indicates the presenceof sleep disturbances [38] Sleep efficiency is calculated bydividing the total sleep time by total bedtime a higher sleepefficiency means better sleep quantity and quality A longtherapeutic course such as 10ndash12 weeks may be necessaryto further elevate sleep efficiency to a desirable level throughsustainable treatment effect
MAT could provide continuous stimulation of acupointsas long as the magnetic pellets on the ears are in situ and thesubjects could receive laser stimulation to the acupoints onthe day of treatment The synergistic effect of the combinedMAT and LAT was demonstrated in two previous trials[39 40] conducted by the research team In a double-blindRCT for osteoarthritic knee the subjects who received thecombined AT protocols exhibited stronger treatment effectsin terms of pain relief ambulation status and range of kneemovements compared with those treated with separate MATor LAT [39] whereas in another double-blinded RCT foraging males with lower urinary tract symptoms a combinedAT protocol exhibited a stronger therapeutic effect in reliev-ing voiding problems improving the urinary flow rate andminimizing the postvoid residual urine than the placebogroup or MAT alone [40] However the combined MAT andLAT approach did not show any advantage over the separateMAT protocol in current studyTherefore a greater frequency
6 Evidence-Based Complementary and Alternative Medicine
Table1So
ciod
emograph
icandbaselin
echaracteristicso
fthe
participantssample(
N=147)
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Age
(years)
j0025lowast
Mean(SD)
7529(699)
7602(702)
7680(616
)7320(729)
Gender
Male
197
57
permil0907
Female
128
4341
44Ed
ucationlevel
Prim
aryor
below
100
3235
330734
Second
ary
3915
915
Tertiary
orabove
83
23
Marita
lstatus
Sing
le5
21
20971
Marrie
d82
2926
27DivorcedWidow
ed60
1919
22Re
ligion
No
7526
2227
permil0895
Yes
7224
2424
Body
massind
ex(kgm2)
2229(373)
2285(348)
2150(357)
2246(404)
j0076
Shared
bed
No
109
3338
38permil0188
Yes
3817
813
Living
alon
eNo
6620
2719
permil0079
Yes
8130
1932
Evidence-Based Complementary and Alternative Medicine 7
Table1Con
tinued
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Sleeping
pills
taken
No
103
3433
360391
Previous
user
3214
711
Currentu
ser
122
64
Durationof
insomnia
(years)
Mean(SD)
1012
(1067)
923(
834)
1115
(1309)
1006(1040
)j
0678
Com
orbidillness
No
225
512
permil0488
Yes
125
4541
39Re
gulard
rugs
taken
No
3210
715
permil044
1Yes
11540
3936
PSQI(total)(0-21)
1263(324)
1267(315
)1289(413
)1235(234)
j0715
Sleeplatency(
min)
2703(2313)
2656(2376)
2868(2486)
2600(2119)
j0839
Totalsleep
time(
hours)
376
(196)
393
(193)
374
(186)
362
(210
)j
0734
Wakea
ftersleep
onset
(minutes)
9031
(8853)
9206(914
4)9003(995
6)8886(7595)
j0984
Sleepeffi
ciency
()
7233
(1609)
7244(1591)
7425(
1604)
7050(1642)
j0521
SF-12(PCS
)4139
(851)
4065(758)
4143(969)
4207(836)
j0707
SF-12(M
CS)
4668(1234)
4822(117
6)46
19(1349)
4562(118
9)j
0542
PHQ-9
947(607)
954(534)
952(669)
935(
626)
j0986
SDstand
arddeviation
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
njOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
8 Evidence-Based Complementary and Alternative Medicine
Table2Re
ported
adversee
ffectsexpectationsand
satisfactiontowards
thetherapy
yen
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Havey
ouused
complem
entary
therapiesinthep
ast
permil0423
No
96(653
)33
3330
Yes
51(347
)17
1321
How
muchfaith
doyouhave
incomplem
entary
therapiesin
general
(0to
10)
782(213
)840
(194)
748(218
)75
5(218
)j
0056
Expectationfortreatmenteffect
towards
MAT
(0to
10)
741(210)
796(211)
693
(203)
731(207)
j0051
Expectationfortreatmenteffect
towards
LAT
(0to
10)
741(213)
808
(200)
687
(209)
725(
215)
j0016lowast
Averagee
xpectatio
nfor
treatmenteffect
(0to
10)
773(213
)840
(203)
720(203)
757(218
)j
0016lowast
Earitchinessyen
16(109
)8lowast
(resolve
automatically)
2lowast(resolve
automatically)
6lowast(resolve
automatically)
---
Evidence-Based Complementary and Alternative Medicine 9
Table2Con
tinued
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Tend
ernesson
acup
ointsyen
20(136
)9lowast
(resolve
automatically)
1lowast(resolve
automatically)
10lowast
(resolve
automatically)
---
Satisfactiontowards
therapy(
0to
10)yen
758(237
)78
6(203)
702(268)
758(237
)j
0225
Thou
ghtthattheymight
bereceivingplacebotre
atmentyen
No
126(900
)39
4146
0011lowast
Yes
14(100
)10
31
Will
recommendthistherapyto
othersyen
0166
Definitelywill
109(757
)38
2942
Maybe
20(139
)5
96
No
15(104
)6
72
Mean(stand
arddeviation)
unlessotherw
iseno
ted
ΩAssociatio
nbetweenvaria
bles
was
determ
ined
bychi-s
quarea
nalyseso
rFish
errsquos-exacttestw
here
approp
riate
Evaluated
beforetheinterventio
nyenE
valuated
after
theinterventionhasb
eencompleted
lowastldquoC
ertainrdquoc
ausality
jOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
10 Evidence-Based Complementary and Alternative Medicine
Table3Outcomev
ariables
acrossthreeg
roup
satd
ifferenttim
epoints
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PSQI(total)(0-21)
Baselin
e1268(044)
1290(062)
1234(034)
Postinterventio
n94
6(052
)99
1(055)
848
(051)
023
(-14
418
9)-065(
-23610
6)087
(-055230)
6we
eksfollowup
907(053
)92
5(065)
926(054)
-050(-207197)
053
(-114219)
-058(-254138)
3mon
thsfollowup
912(079)
781(068)
906(058)
-154(-400
093)
027
(-18
8242)
-181(-399037)
6-mon
thfollo
wup
820
(062)
796(067)
846
(066)
-047(-268175)
059
(-13
8256)
-106(-316105)
Sleeplatency(minutes)
Baselin
e2682(333
)2916
(359)
2517
(286)
Postinterventio
n2529(297)
2500(332
)2617
(303)
(-1329802)
223
(-8111257)
-486(-1533
560)
6we
eksfollowup
1935(322)
2656(339
)2368(330)
487
(-77
31747)
567
(-589172
3)-080(-11771018
)3m
onthsfollowup
1799
(337
)2129(356)
2390(422)
096
(-11491341)
725(
-6932143)
-629(-2065807)
6-mon
thfollo
wup
1966(531
)2342(539
)1907(434)
143(-15791864)
076
(-15341686)
067
(-15851718)
Totalslee
ptim
e(hours)
Baselin
e393
(027)
375
(028)
361
(030)
Postinterventio
n393
(249)
405
(030)
396
(029)
031(-067128)
035
(-065136)
-005(
-117108)
6we
eksfollowup
381
(027)
390
(029)
385
(025)
027
(06812
3)036
(-059131
)-009(-116099)
3mon
thsfollowup
366
(044)
426
(049)
338
(024)
077
(-081236)
0034(-13
213
9)074
(-061209)
6-mon
thfollo
wup
392
(049)
442
(061)
371
(045)
068
(-10
3238)
0112(-14
516
8)057
(-114227)
Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Evidence-Based Complementary and Alternative Medicine 3
Shenmen
Spleen
Subcortex
Internal acupoint
Occiput
Heart
Liver
Kidney
Figure 1 Selected auricular points for insomnia
Figure 2 Administration of magneto-auriculotherapy
We replaced the experimental objects (ie magnetic pelletsfor true MAT or J medulla for placebo MAT) every otherday that is three times a week (except Sunday) to preventlocal irritation of acupoints The total treatment period wassix weeks
Participation in the study was voluntary Writteninformed consent was obtained from each subject uponexplaining the risks and benefits of their participationEthical approval was obtained from the Human ResearchEthics Review Committee of the Hong Kong PolytechnicUniversity The study was conducted in accordance with theDeclaration of Helsinki Given their multiple visits to thecentres to receive treatment the subjects were provided atravel subsidy in the form of supermarket coupons uponcompletion of the study
224 Treatment Effect Evaluation Thesubjectswere assessedat baseline at six weeks (postintervention) and duringfollow-up after six weeks three months and six months Toachieve evaluator blinding the assessment was conductedby a different researcher who was unaware of the treatmentmodality given to the subjects PSQI which was used tocollect data related to the sleep conditions of the subjectswas considered as the primary outcomeThis instrument wasscored from 0 to 21 and scores greater than five indicatedpoor sleep quality Chong andCheung [27] validated theCan-tonese PSQI and reported a high internal consistency of 075
The secondary outcomes considered are as follows(1) actigraphic monitoring was conducted to collect sleepparameters including sleep latency (minutes) waking aftersleep onset (minutes) total sleep time (hours) and sleep
4 Evidence-Based Complementary and Alternative Medicine
Figure 3 Administration of laser auriculotherapy
efficiency () An Actiwatchrsquo Spectrum Plus device with0025G ultra-high sensitivity and 32 Hz sampling rate wasused in actigraphic monitoring The subjects were requestedto wear the device on the wrist of their nondominant hand 24hours a day for 7 consecutive days to determine the overallsleep conditions within a certain period Data were collectedin epochs every 30 second These epoch-by-epoch data werestored in the internal memory of the device until theycould be downloaded to a computer Actiware 6 ActigraphAnalysis Software was used for sleep analysis (2)TheChinese(HK) SF-12 v2copy an abbreviated version of the SF36 healthquestionnaire was used to evaluate the health-related qualityof life (HRQOL) of the subjects This instrument covered 12items and the resultswere presented by a physical componentscore (PCS) and a mental component score (MCS) PCS andMCS ranged from 0 to 100 with higher scores indicatingbetter HRQOL [28] (3) Patient Health Questionnaire (PHQ-9) was also used This instrument was validated as a usefultool for assessing depression status The scores ranged from0 to 27 and high scores indicated severe depression status[29] The scale had a Cronbachrsquos alpha of 082 and therecommended cut-off score was 8 [30]
The subjectsrsquo expectations and satisfaction towards thetherapy were evaluated using a 10-point scale with highscores indicating high expectations or satisfaction [31] Datawere likewise collected on sociodemographic characteris-tics including age gender marital status educational levelreligion number of family members body mass indexsingleshared bed comorbid illnesses use of sleeping pillsor aids and current medications taken Similarly monitoredwere the recruitment rate compliance rate of the treatmentprotocol and adverse effects arising from the therapy
225 Data Analyses Descriptive statistics were determinedon the sociodemographic and clinical characteristics of the
subjects The estimated mean and standard error were com-puted for the outcome variables of each time point Associa-tion amongst categorical variables was estimated using x2 testor Fisherrsquos exact test where appropriate to identify significantvariables for inclusion in the generalised estimating equa-tions (GEE) for adjustment One-way analysis of variancewas used to examine group differences Primary analysiswas conducted using GEE model with an autoregressioncorrelation structure to evaluate interactions amongst thegroups over time (baseline to six months follow-up) on theprimary outcome (ie PSQI score) and secondary outcomes(sleep parameters using 24-hour actigraphic monitoringquality of life using SF-12 and PHQ-9) Missing data werehandled usingGEE and assumed to be random [32]Themainanalysis was repeated at postintervention and during thefollow-up sessions (up to six months) for sensitivity analysisSPSS version 250 (IBM Corporation USA) was used for allstatistical analyses All statistical tests were two sided withsignificance level set at 005
3 Results
The study was conducted from May 2016 to May 2018Data were collected from 11 centres for the elderly and therecruitment rate was 886 A total of 147 eligible subjectswere randomly divided into three groups (Group 1=50Group2=46 and Group 3=51)
31 Participantsrsquo Characteristics The recruited subjects hadan average age of 7529 yearsplusmn 699 with a mean durationof insomnia for 1012 plusmn 1067 years Majority of the subjects(700) did not take any medication to manage their sleepproblems The groups were essentially comparable and wellbalanced in terms of sociodemographic variables includ-ing gender distribution body mass index education level
Evidence-Based Complementary and Alternative Medicine 5
marital status comorbid illnesses and regular medicationstaken However age showed slight significant differencesamongst the groups and thus this variable was adjusted inthe GEE models in subsequent analyses According to the24-hour actigraphic recordings the subjects had an averageof poor sleep quality (PSQI 1263 plusmn324 sleep efficiency7233 plusmn1609) long sleep latency (2703 plusmn 2313 minutes)short total sleep time (376 plusmn 196 hours) and waking aftersleep onset (9031plusmn 8853minutes)The subjects also hadmilddepression (PHQ-9 947 plusmn 607) and low HRQOL in termsof physical component (4139 plusmn 851) and mental component(4668 plusmn 1234) (Table 1)
32 Compliance Expectation and Satisfaction towards theTreatment Compliance with the intervention protocol washigh at an average of 952 (n = 140) of the subjects contin-ued with postintervention and all follow-up measurementsuntil six months The recruitment flowchart is illustrated inFigure 4 Althoughmajority of the subjects (653) had nevertried complementary and alternative treatments they gener-ally exhibited strong confidence in the proposed therapy (782of 10) and had a relatively high expectation of its effectiveness(773 of 10) before the trial After the intervention the subjectsin Group 1 had the highest satisfaction from the therapy(786) followed by those in Group 3 (758) and Group 2 (702)A correlation analysis was conducted between expectationsof the treatment effect and sleep parameters (PSQI SE)However no significant relationship was detected (pgt005)Over 75 of the subjects (n = 109) indicated that they woulddefinitely recommend the therapy to others No specificadverse effects were observed arising from the therapyapart from 16 cases (109) who reported having mild skinirritation on the ears due to the adhesive tapes that were usedto hold the experimental tools in place and 20 cases (136)who felt tenderness on the acupoints (most of these subjectsreceived MAT) The number of subjects who believed thatthey might be receiving placebo treatment was higher inGroup 1 than in the other groups although majority of thesubjects (90) believed that they were not receiving placebo(Table 2)
33 Treatment Effect The differences in the primary andsecondary outcomes of the three groups across differenttime points were compared through GEE model analysiswith adjustment for age In general no significant differ-ences were detected in the outcomes (including PSQI sleepparameters measured by actigraphic monitoring SF-12 andPHQ-9) of the three groups (Table 3) However significantdifferences were found in all of the subjective measuresincluding PSQI (Figure 5) SF-12 (physical andor mentalcomponents) (Figures S1 and S2) and PHQ-9 (Figure 6) forindividual groups over time When the sleep conditions wereevaluated by actigraphic monitoring significant differencesin lsquowaking after sleep onsetrsquo (minutes) (Figure S3) and lsquosleepefficiencyrsquo () (Figure S4) were detected only in Groups 1and 3 (Table 4) The completersrsquo analysis showed consistentfindings on the primary and secondary outcomes of thetrial
4 Discussion
Numerous studies that used AT to manage sleep problemsin China encountered methodological flaws which renderedtheir findings unconvincingThe commonproblems includedlack of details on how randomisation and allocation conceal-ment were conducted absence of objective measurementsand a control or placebo group as well as failure to report theuse of blinding and selective reporting of findings [33ndash35]The present study was performed using a scientific approachto identify the optimum treatment protocol forAT in improv-ing the sleep conditions and quality of life of the elderlywith insomnia This meticulous randomised controlled trial(RCT) could provide scientific evidence regarding causalrelationships between interventions and outcomes
In general the treatment effect was comparable amongstthe three AT protocols However significant improvementswere observed in all of the subjective measures includingsleep conditions measured by PSQI HRQOL and depressionstatus for individual groups over time When the sleepconditions were evaluated by objective measures using acti-graphic monitoring significant differences in ldquowaking aftersleep onsetrdquo (minutes) and ldquosleep efficiencyrdquo () were onlynoted in Groups 1 and 3 The use of actigraphs has beenwidely recognised as an objective measurement that couldprovide longitudinal assessment of sleep patterns in a naturalenvironment [36 37]This technique could similarly providevalidmeasures thatmay not be influenced by subject bias Sig-nificant reduction in the awakening time after sleep onset andincrease in sleep efficiency were only detected in subjects whoreceived MAT protocols (ie Groups 1 and 3) but not in thosewho received only the LAT protocol Despite the improvedsleep efficiency of the subjects at postintervention and duringthe follow-up periods the evaluated indices remained below85 a common cut-off percentage that indicates the presenceof sleep disturbances [38] Sleep efficiency is calculated bydividing the total sleep time by total bedtime a higher sleepefficiency means better sleep quantity and quality A longtherapeutic course such as 10ndash12 weeks may be necessaryto further elevate sleep efficiency to a desirable level throughsustainable treatment effect
MAT could provide continuous stimulation of acupointsas long as the magnetic pellets on the ears are in situ and thesubjects could receive laser stimulation to the acupoints onthe day of treatment The synergistic effect of the combinedMAT and LAT was demonstrated in two previous trials[39 40] conducted by the research team In a double-blindRCT for osteoarthritic knee the subjects who received thecombined AT protocols exhibited stronger treatment effectsin terms of pain relief ambulation status and range of kneemovements compared with those treated with separate MATor LAT [39] whereas in another double-blinded RCT foraging males with lower urinary tract symptoms a combinedAT protocol exhibited a stronger therapeutic effect in reliev-ing voiding problems improving the urinary flow rate andminimizing the postvoid residual urine than the placebogroup or MAT alone [40] However the combined MAT andLAT approach did not show any advantage over the separateMAT protocol in current studyTherefore a greater frequency
6 Evidence-Based Complementary and Alternative Medicine
Table1So
ciod
emograph
icandbaselin
echaracteristicso
fthe
participantssample(
N=147)
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Age
(years)
j0025lowast
Mean(SD)
7529(699)
7602(702)
7680(616
)7320(729)
Gender
Male
197
57
permil0907
Female
128
4341
44Ed
ucationlevel
Prim
aryor
below
100
3235
330734
Second
ary
3915
915
Tertiary
orabove
83
23
Marita
lstatus
Sing
le5
21
20971
Marrie
d82
2926
27DivorcedWidow
ed60
1919
22Re
ligion
No
7526
2227
permil0895
Yes
7224
2424
Body
massind
ex(kgm2)
2229(373)
2285(348)
2150(357)
2246(404)
j0076
Shared
bed
No
109
3338
38permil0188
Yes
3817
813
Living
alon
eNo
6620
2719
permil0079
Yes
8130
1932
Evidence-Based Complementary and Alternative Medicine 7
Table1Con
tinued
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Sleeping
pills
taken
No
103
3433
360391
Previous
user
3214
711
Currentu
ser
122
64
Durationof
insomnia
(years)
Mean(SD)
1012
(1067)
923(
834)
1115
(1309)
1006(1040
)j
0678
Com
orbidillness
No
225
512
permil0488
Yes
125
4541
39Re
gulard
rugs
taken
No
3210
715
permil044
1Yes
11540
3936
PSQI(total)(0-21)
1263(324)
1267(315
)1289(413
)1235(234)
j0715
Sleeplatency(
min)
2703(2313)
2656(2376)
2868(2486)
2600(2119)
j0839
Totalsleep
time(
hours)
376
(196)
393
(193)
374
(186)
362
(210
)j
0734
Wakea
ftersleep
onset
(minutes)
9031
(8853)
9206(914
4)9003(995
6)8886(7595)
j0984
Sleepeffi
ciency
()
7233
(1609)
7244(1591)
7425(
1604)
7050(1642)
j0521
SF-12(PCS
)4139
(851)
4065(758)
4143(969)
4207(836)
j0707
SF-12(M
CS)
4668(1234)
4822(117
6)46
19(1349)
4562(118
9)j
0542
PHQ-9
947(607)
954(534)
952(669)
935(
626)
j0986
SDstand
arddeviation
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
njOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
8 Evidence-Based Complementary and Alternative Medicine
Table2Re
ported
adversee
ffectsexpectationsand
satisfactiontowards
thetherapy
yen
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Havey
ouused
complem
entary
therapiesinthep
ast
permil0423
No
96(653
)33
3330
Yes
51(347
)17
1321
How
muchfaith
doyouhave
incomplem
entary
therapiesin
general
(0to
10)
782(213
)840
(194)
748(218
)75
5(218
)j
0056
Expectationfortreatmenteffect
towards
MAT
(0to
10)
741(210)
796(211)
693
(203)
731(207)
j0051
Expectationfortreatmenteffect
towards
LAT
(0to
10)
741(213)
808
(200)
687
(209)
725(
215)
j0016lowast
Averagee
xpectatio
nfor
treatmenteffect
(0to
10)
773(213
)840
(203)
720(203)
757(218
)j
0016lowast
Earitchinessyen
16(109
)8lowast
(resolve
automatically)
2lowast(resolve
automatically)
6lowast(resolve
automatically)
---
Evidence-Based Complementary and Alternative Medicine 9
Table2Con
tinued
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Tend
ernesson
acup
ointsyen
20(136
)9lowast
(resolve
automatically)
1lowast(resolve
automatically)
10lowast
(resolve
automatically)
---
Satisfactiontowards
therapy(
0to
10)yen
758(237
)78
6(203)
702(268)
758(237
)j
0225
Thou
ghtthattheymight
bereceivingplacebotre
atmentyen
No
126(900
)39
4146
0011lowast
Yes
14(100
)10
31
Will
recommendthistherapyto
othersyen
0166
Definitelywill
109(757
)38
2942
Maybe
20(139
)5
96
No
15(104
)6
72
Mean(stand
arddeviation)
unlessotherw
iseno
ted
ΩAssociatio
nbetweenvaria
bles
was
determ
ined
bychi-s
quarea
nalyseso
rFish
errsquos-exacttestw
here
approp
riate
Evaluated
beforetheinterventio
nyenE
valuated
after
theinterventionhasb
eencompleted
lowastldquoC
ertainrdquoc
ausality
jOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
10 Evidence-Based Complementary and Alternative Medicine
Table3Outcomev
ariables
acrossthreeg
roup
satd
ifferenttim
epoints
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PSQI(total)(0-21)
Baselin
e1268(044)
1290(062)
1234(034)
Postinterventio
n94
6(052
)99
1(055)
848
(051)
023
(-14
418
9)-065(
-23610
6)087
(-055230)
6we
eksfollowup
907(053
)92
5(065)
926(054)
-050(-207197)
053
(-114219)
-058(-254138)
3mon
thsfollowup
912(079)
781(068)
906(058)
-154(-400
093)
027
(-18
8242)
-181(-399037)
6-mon
thfollo
wup
820
(062)
796(067)
846
(066)
-047(-268175)
059
(-13
8256)
-106(-316105)
Sleeplatency(minutes)
Baselin
e2682(333
)2916
(359)
2517
(286)
Postinterventio
n2529(297)
2500(332
)2617
(303)
(-1329802)
223
(-8111257)
-486(-1533
560)
6we
eksfollowup
1935(322)
2656(339
)2368(330)
487
(-77
31747)
567
(-589172
3)-080(-11771018
)3m
onthsfollowup
1799
(337
)2129(356)
2390(422)
096
(-11491341)
725(
-6932143)
-629(-2065807)
6-mon
thfollo
wup
1966(531
)2342(539
)1907(434)
143(-15791864)
076
(-15341686)
067
(-15851718)
Totalslee
ptim
e(hours)
Baselin
e393
(027)
375
(028)
361
(030)
Postinterventio
n393
(249)
405
(030)
396
(029)
031(-067128)
035
(-065136)
-005(
-117108)
6we
eksfollowup
381
(027)
390
(029)
385
(025)
027
(06812
3)036
(-059131
)-009(-116099)
3mon
thsfollowup
366
(044)
426
(049)
338
(024)
077
(-081236)
0034(-13
213
9)074
(-061209)
6-mon
thfollo
wup
392
(049)
442
(061)
371
(045)
068
(-10
3238)
0112(-14
516
8)057
(-114227)
Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

4 Evidence-Based Complementary and Alternative Medicine
Figure 3 Administration of laser auriculotherapy
efficiency () An Actiwatchrsquo Spectrum Plus device with0025G ultra-high sensitivity and 32 Hz sampling rate wasused in actigraphic monitoring The subjects were requestedto wear the device on the wrist of their nondominant hand 24hours a day for 7 consecutive days to determine the overallsleep conditions within a certain period Data were collectedin epochs every 30 second These epoch-by-epoch data werestored in the internal memory of the device until theycould be downloaded to a computer Actiware 6 ActigraphAnalysis Software was used for sleep analysis (2)TheChinese(HK) SF-12 v2copy an abbreviated version of the SF36 healthquestionnaire was used to evaluate the health-related qualityof life (HRQOL) of the subjects This instrument covered 12items and the resultswere presented by a physical componentscore (PCS) and a mental component score (MCS) PCS andMCS ranged from 0 to 100 with higher scores indicatingbetter HRQOL [28] (3) Patient Health Questionnaire (PHQ-9) was also used This instrument was validated as a usefultool for assessing depression status The scores ranged from0 to 27 and high scores indicated severe depression status[29] The scale had a Cronbachrsquos alpha of 082 and therecommended cut-off score was 8 [30]
The subjectsrsquo expectations and satisfaction towards thetherapy were evaluated using a 10-point scale with highscores indicating high expectations or satisfaction [31] Datawere likewise collected on sociodemographic characteris-tics including age gender marital status educational levelreligion number of family members body mass indexsingleshared bed comorbid illnesses use of sleeping pillsor aids and current medications taken Similarly monitoredwere the recruitment rate compliance rate of the treatmentprotocol and adverse effects arising from the therapy
225 Data Analyses Descriptive statistics were determinedon the sociodemographic and clinical characteristics of the
subjects The estimated mean and standard error were com-puted for the outcome variables of each time point Associa-tion amongst categorical variables was estimated using x2 testor Fisherrsquos exact test where appropriate to identify significantvariables for inclusion in the generalised estimating equa-tions (GEE) for adjustment One-way analysis of variancewas used to examine group differences Primary analysiswas conducted using GEE model with an autoregressioncorrelation structure to evaluate interactions amongst thegroups over time (baseline to six months follow-up) on theprimary outcome (ie PSQI score) and secondary outcomes(sleep parameters using 24-hour actigraphic monitoringquality of life using SF-12 and PHQ-9) Missing data werehandled usingGEE and assumed to be random [32]Themainanalysis was repeated at postintervention and during thefollow-up sessions (up to six months) for sensitivity analysisSPSS version 250 (IBM Corporation USA) was used for allstatistical analyses All statistical tests were two sided withsignificance level set at 005
3 Results
The study was conducted from May 2016 to May 2018Data were collected from 11 centres for the elderly and therecruitment rate was 886 A total of 147 eligible subjectswere randomly divided into three groups (Group 1=50Group2=46 and Group 3=51)
31 Participantsrsquo Characteristics The recruited subjects hadan average age of 7529 yearsplusmn 699 with a mean durationof insomnia for 1012 plusmn 1067 years Majority of the subjects(700) did not take any medication to manage their sleepproblems The groups were essentially comparable and wellbalanced in terms of sociodemographic variables includ-ing gender distribution body mass index education level
Evidence-Based Complementary and Alternative Medicine 5
marital status comorbid illnesses and regular medicationstaken However age showed slight significant differencesamongst the groups and thus this variable was adjusted inthe GEE models in subsequent analyses According to the24-hour actigraphic recordings the subjects had an averageof poor sleep quality (PSQI 1263 plusmn324 sleep efficiency7233 plusmn1609) long sleep latency (2703 plusmn 2313 minutes)short total sleep time (376 plusmn 196 hours) and waking aftersleep onset (9031plusmn 8853minutes)The subjects also hadmilddepression (PHQ-9 947 plusmn 607) and low HRQOL in termsof physical component (4139 plusmn 851) and mental component(4668 plusmn 1234) (Table 1)
32 Compliance Expectation and Satisfaction towards theTreatment Compliance with the intervention protocol washigh at an average of 952 (n = 140) of the subjects contin-ued with postintervention and all follow-up measurementsuntil six months The recruitment flowchart is illustrated inFigure 4 Althoughmajority of the subjects (653) had nevertried complementary and alternative treatments they gener-ally exhibited strong confidence in the proposed therapy (782of 10) and had a relatively high expectation of its effectiveness(773 of 10) before the trial After the intervention the subjectsin Group 1 had the highest satisfaction from the therapy(786) followed by those in Group 3 (758) and Group 2 (702)A correlation analysis was conducted between expectationsof the treatment effect and sleep parameters (PSQI SE)However no significant relationship was detected (pgt005)Over 75 of the subjects (n = 109) indicated that they woulddefinitely recommend the therapy to others No specificadverse effects were observed arising from the therapyapart from 16 cases (109) who reported having mild skinirritation on the ears due to the adhesive tapes that were usedto hold the experimental tools in place and 20 cases (136)who felt tenderness on the acupoints (most of these subjectsreceived MAT) The number of subjects who believed thatthey might be receiving placebo treatment was higher inGroup 1 than in the other groups although majority of thesubjects (90) believed that they were not receiving placebo(Table 2)
33 Treatment Effect The differences in the primary andsecondary outcomes of the three groups across differenttime points were compared through GEE model analysiswith adjustment for age In general no significant differ-ences were detected in the outcomes (including PSQI sleepparameters measured by actigraphic monitoring SF-12 andPHQ-9) of the three groups (Table 3) However significantdifferences were found in all of the subjective measuresincluding PSQI (Figure 5) SF-12 (physical andor mentalcomponents) (Figures S1 and S2) and PHQ-9 (Figure 6) forindividual groups over time When the sleep conditions wereevaluated by actigraphic monitoring significant differencesin lsquowaking after sleep onsetrsquo (minutes) (Figure S3) and lsquosleepefficiencyrsquo () (Figure S4) were detected only in Groups 1and 3 (Table 4) The completersrsquo analysis showed consistentfindings on the primary and secondary outcomes of thetrial
4 Discussion
Numerous studies that used AT to manage sleep problemsin China encountered methodological flaws which renderedtheir findings unconvincingThe commonproblems includedlack of details on how randomisation and allocation conceal-ment were conducted absence of objective measurementsand a control or placebo group as well as failure to report theuse of blinding and selective reporting of findings [33ndash35]The present study was performed using a scientific approachto identify the optimum treatment protocol forAT in improv-ing the sleep conditions and quality of life of the elderlywith insomnia This meticulous randomised controlled trial(RCT) could provide scientific evidence regarding causalrelationships between interventions and outcomes
In general the treatment effect was comparable amongstthe three AT protocols However significant improvementswere observed in all of the subjective measures includingsleep conditions measured by PSQI HRQOL and depressionstatus for individual groups over time When the sleepconditions were evaluated by objective measures using acti-graphic monitoring significant differences in ldquowaking aftersleep onsetrdquo (minutes) and ldquosleep efficiencyrdquo () were onlynoted in Groups 1 and 3 The use of actigraphs has beenwidely recognised as an objective measurement that couldprovide longitudinal assessment of sleep patterns in a naturalenvironment [36 37]This technique could similarly providevalidmeasures thatmay not be influenced by subject bias Sig-nificant reduction in the awakening time after sleep onset andincrease in sleep efficiency were only detected in subjects whoreceived MAT protocols (ie Groups 1 and 3) but not in thosewho received only the LAT protocol Despite the improvedsleep efficiency of the subjects at postintervention and duringthe follow-up periods the evaluated indices remained below85 a common cut-off percentage that indicates the presenceof sleep disturbances [38] Sleep efficiency is calculated bydividing the total sleep time by total bedtime a higher sleepefficiency means better sleep quantity and quality A longtherapeutic course such as 10ndash12 weeks may be necessaryto further elevate sleep efficiency to a desirable level throughsustainable treatment effect
MAT could provide continuous stimulation of acupointsas long as the magnetic pellets on the ears are in situ and thesubjects could receive laser stimulation to the acupoints onthe day of treatment The synergistic effect of the combinedMAT and LAT was demonstrated in two previous trials[39 40] conducted by the research team In a double-blindRCT for osteoarthritic knee the subjects who received thecombined AT protocols exhibited stronger treatment effectsin terms of pain relief ambulation status and range of kneemovements compared with those treated with separate MATor LAT [39] whereas in another double-blinded RCT foraging males with lower urinary tract symptoms a combinedAT protocol exhibited a stronger therapeutic effect in reliev-ing voiding problems improving the urinary flow rate andminimizing the postvoid residual urine than the placebogroup or MAT alone [40] However the combined MAT andLAT approach did not show any advantage over the separateMAT protocol in current studyTherefore a greater frequency
6 Evidence-Based Complementary and Alternative Medicine
Table1So
ciod
emograph
icandbaselin
echaracteristicso
fthe
participantssample(
N=147)
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Age
(years)
j0025lowast
Mean(SD)
7529(699)
7602(702)
7680(616
)7320(729)
Gender
Male
197
57
permil0907
Female
128
4341
44Ed
ucationlevel
Prim
aryor
below
100
3235
330734
Second
ary
3915
915
Tertiary
orabove
83
23
Marita
lstatus
Sing
le5
21
20971
Marrie
d82
2926
27DivorcedWidow
ed60
1919
22Re
ligion
No
7526
2227
permil0895
Yes
7224
2424
Body
massind
ex(kgm2)
2229(373)
2285(348)
2150(357)
2246(404)
j0076
Shared
bed
No
109
3338
38permil0188
Yes
3817
813
Living
alon
eNo
6620
2719
permil0079
Yes
8130
1932
Evidence-Based Complementary and Alternative Medicine 7
Table1Con
tinued
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Sleeping
pills
taken
No
103
3433
360391
Previous
user
3214
711
Currentu
ser
122
64
Durationof
insomnia
(years)
Mean(SD)
1012
(1067)
923(
834)
1115
(1309)
1006(1040
)j
0678
Com
orbidillness
No
225
512
permil0488
Yes
125
4541
39Re
gulard
rugs
taken
No
3210
715
permil044
1Yes
11540
3936
PSQI(total)(0-21)
1263(324)
1267(315
)1289(413
)1235(234)
j0715
Sleeplatency(
min)
2703(2313)
2656(2376)
2868(2486)
2600(2119)
j0839
Totalsleep
time(
hours)
376
(196)
393
(193)
374
(186)
362
(210
)j
0734
Wakea
ftersleep
onset
(minutes)
9031
(8853)
9206(914
4)9003(995
6)8886(7595)
j0984
Sleepeffi
ciency
()
7233
(1609)
7244(1591)
7425(
1604)
7050(1642)
j0521
SF-12(PCS
)4139
(851)
4065(758)
4143(969)
4207(836)
j0707
SF-12(M
CS)
4668(1234)
4822(117
6)46
19(1349)
4562(118
9)j
0542
PHQ-9
947(607)
954(534)
952(669)
935(
626)
j0986
SDstand
arddeviation
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
njOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
8 Evidence-Based Complementary and Alternative Medicine
Table2Re
ported
adversee
ffectsexpectationsand
satisfactiontowards
thetherapy
yen
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Havey
ouused
complem
entary
therapiesinthep
ast
permil0423
No
96(653
)33
3330
Yes
51(347
)17
1321
How
muchfaith
doyouhave
incomplem
entary
therapiesin
general
(0to
10)
782(213
)840
(194)
748(218
)75
5(218
)j
0056
Expectationfortreatmenteffect
towards
MAT
(0to
10)
741(210)
796(211)
693
(203)
731(207)
j0051
Expectationfortreatmenteffect
towards
LAT
(0to
10)
741(213)
808
(200)
687
(209)
725(
215)
j0016lowast
Averagee
xpectatio
nfor
treatmenteffect
(0to
10)
773(213
)840
(203)
720(203)
757(218
)j
0016lowast
Earitchinessyen
16(109
)8lowast
(resolve
automatically)
2lowast(resolve
automatically)
6lowast(resolve
automatically)
---
Evidence-Based Complementary and Alternative Medicine 9
Table2Con
tinued
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Tend
ernesson
acup
ointsyen
20(136
)9lowast
(resolve
automatically)
1lowast(resolve
automatically)
10lowast
(resolve
automatically)
---
Satisfactiontowards
therapy(
0to
10)yen
758(237
)78
6(203)
702(268)
758(237
)j
0225
Thou
ghtthattheymight
bereceivingplacebotre
atmentyen
No
126(900
)39
4146
0011lowast
Yes
14(100
)10
31
Will
recommendthistherapyto
othersyen
0166
Definitelywill
109(757
)38
2942
Maybe
20(139
)5
96
No
15(104
)6
72
Mean(stand
arddeviation)
unlessotherw
iseno
ted
ΩAssociatio
nbetweenvaria
bles
was
determ
ined
bychi-s
quarea
nalyseso
rFish
errsquos-exacttestw
here
approp
riate
Evaluated
beforetheinterventio
nyenE
valuated
after
theinterventionhasb
eencompleted
lowastldquoC
ertainrdquoc
ausality
jOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
10 Evidence-Based Complementary and Alternative Medicine
Table3Outcomev
ariables
acrossthreeg
roup
satd
ifferenttim
epoints
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PSQI(total)(0-21)
Baselin
e1268(044)
1290(062)
1234(034)
Postinterventio
n94
6(052
)99
1(055)
848
(051)
023
(-14
418
9)-065(
-23610
6)087
(-055230)
6we
eksfollowup
907(053
)92
5(065)
926(054)
-050(-207197)
053
(-114219)
-058(-254138)
3mon
thsfollowup
912(079)
781(068)
906(058)
-154(-400
093)
027
(-18
8242)
-181(-399037)
6-mon
thfollo
wup
820
(062)
796(067)
846
(066)
-047(-268175)
059
(-13
8256)
-106(-316105)
Sleeplatency(minutes)
Baselin
e2682(333
)2916
(359)
2517
(286)
Postinterventio
n2529(297)
2500(332
)2617
(303)
(-1329802)
223
(-8111257)
-486(-1533
560)
6we
eksfollowup
1935(322)
2656(339
)2368(330)
487
(-77
31747)
567
(-589172
3)-080(-11771018
)3m
onthsfollowup
1799
(337
)2129(356)
2390(422)
096
(-11491341)
725(
-6932143)
-629(-2065807)
6-mon
thfollo
wup
1966(531
)2342(539
)1907(434)
143(-15791864)
076
(-15341686)
067
(-15851718)
Totalslee
ptim
e(hours)
Baselin
e393
(027)
375
(028)
361
(030)
Postinterventio
n393
(249)
405
(030)
396
(029)
031(-067128)
035
(-065136)
-005(
-117108)
6we
eksfollowup
381
(027)
390
(029)
385
(025)
027
(06812
3)036
(-059131
)-009(-116099)
3mon
thsfollowup
366
(044)
426
(049)
338
(024)
077
(-081236)
0034(-13
213
9)074
(-061209)
6-mon
thfollo
wup
392
(049)
442
(061)
371
(045)
068
(-10
3238)
0112(-14
516
8)057
(-114227)
Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Evidence-Based Complementary and Alternative Medicine 5
marital status comorbid illnesses and regular medicationstaken However age showed slight significant differencesamongst the groups and thus this variable was adjusted inthe GEE models in subsequent analyses According to the24-hour actigraphic recordings the subjects had an averageof poor sleep quality (PSQI 1263 plusmn324 sleep efficiency7233 plusmn1609) long sleep latency (2703 plusmn 2313 minutes)short total sleep time (376 plusmn 196 hours) and waking aftersleep onset (9031plusmn 8853minutes)The subjects also hadmilddepression (PHQ-9 947 plusmn 607) and low HRQOL in termsof physical component (4139 plusmn 851) and mental component(4668 plusmn 1234) (Table 1)
32 Compliance Expectation and Satisfaction towards theTreatment Compliance with the intervention protocol washigh at an average of 952 (n = 140) of the subjects contin-ued with postintervention and all follow-up measurementsuntil six months The recruitment flowchart is illustrated inFigure 4 Althoughmajority of the subjects (653) had nevertried complementary and alternative treatments they gener-ally exhibited strong confidence in the proposed therapy (782of 10) and had a relatively high expectation of its effectiveness(773 of 10) before the trial After the intervention the subjectsin Group 1 had the highest satisfaction from the therapy(786) followed by those in Group 3 (758) and Group 2 (702)A correlation analysis was conducted between expectationsof the treatment effect and sleep parameters (PSQI SE)However no significant relationship was detected (pgt005)Over 75 of the subjects (n = 109) indicated that they woulddefinitely recommend the therapy to others No specificadverse effects were observed arising from the therapyapart from 16 cases (109) who reported having mild skinirritation on the ears due to the adhesive tapes that were usedto hold the experimental tools in place and 20 cases (136)who felt tenderness on the acupoints (most of these subjectsreceived MAT) The number of subjects who believed thatthey might be receiving placebo treatment was higher inGroup 1 than in the other groups although majority of thesubjects (90) believed that they were not receiving placebo(Table 2)
33 Treatment Effect The differences in the primary andsecondary outcomes of the three groups across differenttime points were compared through GEE model analysiswith adjustment for age In general no significant differ-ences were detected in the outcomes (including PSQI sleepparameters measured by actigraphic monitoring SF-12 andPHQ-9) of the three groups (Table 3) However significantdifferences were found in all of the subjective measuresincluding PSQI (Figure 5) SF-12 (physical andor mentalcomponents) (Figures S1 and S2) and PHQ-9 (Figure 6) forindividual groups over time When the sleep conditions wereevaluated by actigraphic monitoring significant differencesin lsquowaking after sleep onsetrsquo (minutes) (Figure S3) and lsquosleepefficiencyrsquo () (Figure S4) were detected only in Groups 1and 3 (Table 4) The completersrsquo analysis showed consistentfindings on the primary and secondary outcomes of thetrial
4 Discussion
Numerous studies that used AT to manage sleep problemsin China encountered methodological flaws which renderedtheir findings unconvincingThe commonproblems includedlack of details on how randomisation and allocation conceal-ment were conducted absence of objective measurementsand a control or placebo group as well as failure to report theuse of blinding and selective reporting of findings [33ndash35]The present study was performed using a scientific approachto identify the optimum treatment protocol forAT in improv-ing the sleep conditions and quality of life of the elderlywith insomnia This meticulous randomised controlled trial(RCT) could provide scientific evidence regarding causalrelationships between interventions and outcomes
In general the treatment effect was comparable amongstthe three AT protocols However significant improvementswere observed in all of the subjective measures includingsleep conditions measured by PSQI HRQOL and depressionstatus for individual groups over time When the sleepconditions were evaluated by objective measures using acti-graphic monitoring significant differences in ldquowaking aftersleep onsetrdquo (minutes) and ldquosleep efficiencyrdquo () were onlynoted in Groups 1 and 3 The use of actigraphs has beenwidely recognised as an objective measurement that couldprovide longitudinal assessment of sleep patterns in a naturalenvironment [36 37]This technique could similarly providevalidmeasures thatmay not be influenced by subject bias Sig-nificant reduction in the awakening time after sleep onset andincrease in sleep efficiency were only detected in subjects whoreceived MAT protocols (ie Groups 1 and 3) but not in thosewho received only the LAT protocol Despite the improvedsleep efficiency of the subjects at postintervention and duringthe follow-up periods the evaluated indices remained below85 a common cut-off percentage that indicates the presenceof sleep disturbances [38] Sleep efficiency is calculated bydividing the total sleep time by total bedtime a higher sleepefficiency means better sleep quantity and quality A longtherapeutic course such as 10ndash12 weeks may be necessaryto further elevate sleep efficiency to a desirable level throughsustainable treatment effect
MAT could provide continuous stimulation of acupointsas long as the magnetic pellets on the ears are in situ and thesubjects could receive laser stimulation to the acupoints onthe day of treatment The synergistic effect of the combinedMAT and LAT was demonstrated in two previous trials[39 40] conducted by the research team In a double-blindRCT for osteoarthritic knee the subjects who received thecombined AT protocols exhibited stronger treatment effectsin terms of pain relief ambulation status and range of kneemovements compared with those treated with separate MATor LAT [39] whereas in another double-blinded RCT foraging males with lower urinary tract symptoms a combinedAT protocol exhibited a stronger therapeutic effect in reliev-ing voiding problems improving the urinary flow rate andminimizing the postvoid residual urine than the placebogroup or MAT alone [40] However the combined MAT andLAT approach did not show any advantage over the separateMAT protocol in current studyTherefore a greater frequency
6 Evidence-Based Complementary and Alternative Medicine
Table1So
ciod
emograph
icandbaselin
echaracteristicso
fthe
participantssample(
N=147)
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Age
(years)
j0025lowast
Mean(SD)
7529(699)
7602(702)
7680(616
)7320(729)
Gender
Male
197
57
permil0907
Female
128
4341
44Ed
ucationlevel
Prim
aryor
below
100
3235
330734
Second
ary
3915
915
Tertiary
orabove
83
23
Marita
lstatus
Sing
le5
21
20971
Marrie
d82
2926
27DivorcedWidow
ed60
1919
22Re
ligion
No
7526
2227
permil0895
Yes
7224
2424
Body
massind
ex(kgm2)
2229(373)
2285(348)
2150(357)
2246(404)
j0076
Shared
bed
No
109
3338
38permil0188
Yes
3817
813
Living
alon
eNo
6620
2719
permil0079
Yes
8130
1932
Evidence-Based Complementary and Alternative Medicine 7
Table1Con
tinued
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Sleeping
pills
taken
No
103
3433
360391
Previous
user
3214
711
Currentu
ser
122
64
Durationof
insomnia
(years)
Mean(SD)
1012
(1067)
923(
834)
1115
(1309)
1006(1040
)j
0678
Com
orbidillness
No
225
512
permil0488
Yes
125
4541
39Re
gulard
rugs
taken
No
3210
715
permil044
1Yes
11540
3936
PSQI(total)(0-21)
1263(324)
1267(315
)1289(413
)1235(234)
j0715
Sleeplatency(
min)
2703(2313)
2656(2376)
2868(2486)
2600(2119)
j0839
Totalsleep
time(
hours)
376
(196)
393
(193)
374
(186)
362
(210
)j
0734
Wakea
ftersleep
onset
(minutes)
9031
(8853)
9206(914
4)9003(995
6)8886(7595)
j0984
Sleepeffi
ciency
()
7233
(1609)
7244(1591)
7425(
1604)
7050(1642)
j0521
SF-12(PCS
)4139
(851)
4065(758)
4143(969)
4207(836)
j0707
SF-12(M
CS)
4668(1234)
4822(117
6)46
19(1349)
4562(118
9)j
0542
PHQ-9
947(607)
954(534)
952(669)
935(
626)
j0986
SDstand
arddeviation
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
njOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
8 Evidence-Based Complementary and Alternative Medicine
Table2Re
ported
adversee
ffectsexpectationsand
satisfactiontowards
thetherapy
yen
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Havey
ouused
complem
entary
therapiesinthep
ast
permil0423
No
96(653
)33
3330
Yes
51(347
)17
1321
How
muchfaith
doyouhave
incomplem
entary
therapiesin
general
(0to
10)
782(213
)840
(194)
748(218
)75
5(218
)j
0056
Expectationfortreatmenteffect
towards
MAT
(0to
10)
741(210)
796(211)
693
(203)
731(207)
j0051
Expectationfortreatmenteffect
towards
LAT
(0to
10)
741(213)
808
(200)
687
(209)
725(
215)
j0016lowast
Averagee
xpectatio
nfor
treatmenteffect
(0to
10)
773(213
)840
(203)
720(203)
757(218
)j
0016lowast
Earitchinessyen
16(109
)8lowast
(resolve
automatically)
2lowast(resolve
automatically)
6lowast(resolve
automatically)
---
Evidence-Based Complementary and Alternative Medicine 9
Table2Con
tinued
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Tend
ernesson
acup
ointsyen
20(136
)9lowast
(resolve
automatically)
1lowast(resolve
automatically)
10lowast
(resolve
automatically)
---
Satisfactiontowards
therapy(
0to
10)yen
758(237
)78
6(203)
702(268)
758(237
)j
0225
Thou
ghtthattheymight
bereceivingplacebotre
atmentyen
No
126(900
)39
4146
0011lowast
Yes
14(100
)10
31
Will
recommendthistherapyto
othersyen
0166
Definitelywill
109(757
)38
2942
Maybe
20(139
)5
96
No
15(104
)6
72
Mean(stand
arddeviation)
unlessotherw
iseno
ted
ΩAssociatio
nbetweenvaria
bles
was
determ
ined
bychi-s
quarea
nalyseso
rFish
errsquos-exacttestw
here
approp
riate
Evaluated
beforetheinterventio
nyenE
valuated
after
theinterventionhasb
eencompleted
lowastldquoC
ertainrdquoc
ausality
jOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
10 Evidence-Based Complementary and Alternative Medicine
Table3Outcomev
ariables
acrossthreeg
roup
satd
ifferenttim
epoints
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PSQI(total)(0-21)
Baselin
e1268(044)
1290(062)
1234(034)
Postinterventio
n94
6(052
)99
1(055)
848
(051)
023
(-14
418
9)-065(
-23610
6)087
(-055230)
6we
eksfollowup
907(053
)92
5(065)
926(054)
-050(-207197)
053
(-114219)
-058(-254138)
3mon
thsfollowup
912(079)
781(068)
906(058)
-154(-400
093)
027
(-18
8242)
-181(-399037)
6-mon
thfollo
wup
820
(062)
796(067)
846
(066)
-047(-268175)
059
(-13
8256)
-106(-316105)
Sleeplatency(minutes)
Baselin
e2682(333
)2916
(359)
2517
(286)
Postinterventio
n2529(297)
2500(332
)2617
(303)
(-1329802)
223
(-8111257)
-486(-1533
560)
6we
eksfollowup
1935(322)
2656(339
)2368(330)
487
(-77
31747)
567
(-589172
3)-080(-11771018
)3m
onthsfollowup
1799
(337
)2129(356)
2390(422)
096
(-11491341)
725(
-6932143)
-629(-2065807)
6-mon
thfollo
wup
1966(531
)2342(539
)1907(434)
143(-15791864)
076
(-15341686)
067
(-15851718)
Totalslee
ptim
e(hours)
Baselin
e393
(027)
375
(028)
361
(030)
Postinterventio
n393
(249)
405
(030)
396
(029)
031(-067128)
035
(-065136)
-005(
-117108)
6we
eksfollowup
381
(027)
390
(029)
385
(025)
027
(06812
3)036
(-059131
)-009(-116099)
3mon
thsfollowup
366
(044)
426
(049)
338
(024)
077
(-081236)
0034(-13
213
9)074
(-061209)
6-mon
thfollo
wup
392
(049)
442
(061)
371
(045)
068
(-10
3238)
0112(-14
516
8)057
(-114227)
Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

6 Evidence-Based Complementary and Alternative Medicine
Table1So
ciod
emograph
icandbaselin
echaracteristicso
fthe
participantssample(
N=147)
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Age
(years)
j0025lowast
Mean(SD)
7529(699)
7602(702)
7680(616
)7320(729)
Gender
Male
197
57
permil0907
Female
128
4341
44Ed
ucationlevel
Prim
aryor
below
100
3235
330734
Second
ary
3915
915
Tertiary
orabove
83
23
Marita
lstatus
Sing
le5
21
20971
Marrie
d82
2926
27DivorcedWidow
ed60
1919
22Re
ligion
No
7526
2227
permil0895
Yes
7224
2424
Body
massind
ex(kgm2)
2229(373)
2285(348)
2150(357)
2246(404)
j0076
Shared
bed
No
109
3338
38permil0188
Yes
3817
813
Living
alon
eNo
6620
2719
permil0079
Yes
8130
1932
Evidence-Based Complementary and Alternative Medicine 7
Table1Con
tinued
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Sleeping
pills
taken
No
103
3433
360391
Previous
user
3214
711
Currentu
ser
122
64
Durationof
insomnia
(years)
Mean(SD)
1012
(1067)
923(
834)
1115
(1309)
1006(1040
)j
0678
Com
orbidillness
No
225
512
permil0488
Yes
125
4541
39Re
gulard
rugs
taken
No
3210
715
permil044
1Yes
11540
3936
PSQI(total)(0-21)
1263(324)
1267(315
)1289(413
)1235(234)
j0715
Sleeplatency(
min)
2703(2313)
2656(2376)
2868(2486)
2600(2119)
j0839
Totalsleep
time(
hours)
376
(196)
393
(193)
374
(186)
362
(210
)j
0734
Wakea
ftersleep
onset
(minutes)
9031
(8853)
9206(914
4)9003(995
6)8886(7595)
j0984
Sleepeffi
ciency
()
7233
(1609)
7244(1591)
7425(
1604)
7050(1642)
j0521
SF-12(PCS
)4139
(851)
4065(758)
4143(969)
4207(836)
j0707
SF-12(M
CS)
4668(1234)
4822(117
6)46
19(1349)
4562(118
9)j
0542
PHQ-9
947(607)
954(534)
952(669)
935(
626)
j0986
SDstand
arddeviation
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
njOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
8 Evidence-Based Complementary and Alternative Medicine
Table2Re
ported
adversee
ffectsexpectationsand
satisfactiontowards
thetherapy
yen
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Havey
ouused
complem
entary
therapiesinthep
ast
permil0423
No
96(653
)33
3330
Yes
51(347
)17
1321
How
muchfaith
doyouhave
incomplem
entary
therapiesin
general
(0to
10)
782(213
)840
(194)
748(218
)75
5(218
)j
0056
Expectationfortreatmenteffect
towards
MAT
(0to
10)
741(210)
796(211)
693
(203)
731(207)
j0051
Expectationfortreatmenteffect
towards
LAT
(0to
10)
741(213)
808
(200)
687
(209)
725(
215)
j0016lowast
Averagee
xpectatio
nfor
treatmenteffect
(0to
10)
773(213
)840
(203)
720(203)
757(218
)j
0016lowast
Earitchinessyen
16(109
)8lowast
(resolve
automatically)
2lowast(resolve
automatically)
6lowast(resolve
automatically)
---
Evidence-Based Complementary and Alternative Medicine 9
Table2Con
tinued
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Tend
ernesson
acup
ointsyen
20(136
)9lowast
(resolve
automatically)
1lowast(resolve
automatically)
10lowast
(resolve
automatically)
---
Satisfactiontowards
therapy(
0to
10)yen
758(237
)78
6(203)
702(268)
758(237
)j
0225
Thou
ghtthattheymight
bereceivingplacebotre
atmentyen
No
126(900
)39
4146
0011lowast
Yes
14(100
)10
31
Will
recommendthistherapyto
othersyen
0166
Definitelywill
109(757
)38
2942
Maybe
20(139
)5
96
No
15(104
)6
72
Mean(stand
arddeviation)
unlessotherw
iseno
ted
ΩAssociatio
nbetweenvaria
bles
was
determ
ined
bychi-s
quarea
nalyseso
rFish
errsquos-exacttestw
here
approp
riate
Evaluated
beforetheinterventio
nyenE
valuated
after
theinterventionhasb
eencompleted
lowastldquoC
ertainrdquoc
ausality
jOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
10 Evidence-Based Complementary and Alternative Medicine
Table3Outcomev
ariables
acrossthreeg
roup
satd
ifferenttim
epoints
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PSQI(total)(0-21)
Baselin
e1268(044)
1290(062)
1234(034)
Postinterventio
n94
6(052
)99
1(055)
848
(051)
023
(-14
418
9)-065(
-23610
6)087
(-055230)
6we
eksfollowup
907(053
)92
5(065)
926(054)
-050(-207197)
053
(-114219)
-058(-254138)
3mon
thsfollowup
912(079)
781(068)
906(058)
-154(-400
093)
027
(-18
8242)
-181(-399037)
6-mon
thfollo
wup
820
(062)
796(067)
846
(066)
-047(-268175)
059
(-13
8256)
-106(-316105)
Sleeplatency(minutes)
Baselin
e2682(333
)2916
(359)
2517
(286)
Postinterventio
n2529(297)
2500(332
)2617
(303)
(-1329802)
223
(-8111257)
-486(-1533
560)
6we
eksfollowup
1935(322)
2656(339
)2368(330)
487
(-77
31747)
567
(-589172
3)-080(-11771018
)3m
onthsfollowup
1799
(337
)2129(356)
2390(422)
096
(-11491341)
725(
-6932143)
-629(-2065807)
6-mon
thfollo
wup
1966(531
)2342(539
)1907(434)
143(-15791864)
076
(-15341686)
067
(-15851718)
Totalslee
ptim
e(hours)
Baselin
e393
(027)
375
(028)
361
(030)
Postinterventio
n393
(249)
405
(030)
396
(029)
031(-067128)
035
(-065136)
-005(
-117108)
6we
eksfollowup
381
(027)
390
(029)
385
(025)
027
(06812
3)036
(-059131
)-009(-116099)
3mon
thsfollowup
366
(044)
426
(049)
338
(024)
077
(-081236)
0034(-13
213
9)074
(-061209)
6-mon
thfollo
wup
392
(049)
442
(061)
371
(045)
068
(-10
3238)
0112(-14
516
8)057
(-114227)
Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Evidence-Based Complementary and Alternative Medicine 7
Table1Con
tinued
All
(N=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Sleeping
pills
taken
No
103
3433
360391
Previous
user
3214
711
Currentu
ser
122
64
Durationof
insomnia
(years)
Mean(SD)
1012
(1067)
923(
834)
1115
(1309)
1006(1040
)j
0678
Com
orbidillness
No
225
512
permil0488
Yes
125
4541
39Re
gulard
rugs
taken
No
3210
715
permil044
1Yes
11540
3936
PSQI(total)(0-21)
1263(324)
1267(315
)1289(413
)1235(234)
j0715
Sleeplatency(
min)
2703(2313)
2656(2376)
2868(2486)
2600(2119)
j0839
Totalsleep
time(
hours)
376
(196)
393
(193)
374
(186)
362
(210
)j
0734
Wakea
ftersleep
onset
(minutes)
9031
(8853)
9206(914
4)9003(995
6)8886(7595)
j0984
Sleepeffi
ciency
()
7233
(1609)
7244(1591)
7425(
1604)
7050(1642)
j0521
SF-12(PCS
)4139
(851)
4065(758)
4143(969)
4207(836)
j0707
SF-12(M
CS)
4668(1234)
4822(117
6)46
19(1349)
4562(118
9)j
0542
PHQ-9
947(607)
954(534)
952(669)
935(
626)
j0986
SDstand
arddeviation
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
njOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
8 Evidence-Based Complementary and Alternative Medicine
Table2Re
ported
adversee
ffectsexpectationsand
satisfactiontowards
thetherapy
yen
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Havey
ouused
complem
entary
therapiesinthep
ast
permil0423
No
96(653
)33
3330
Yes
51(347
)17
1321
How
muchfaith
doyouhave
incomplem
entary
therapiesin
general
(0to
10)
782(213
)840
(194)
748(218
)75
5(218
)j
0056
Expectationfortreatmenteffect
towards
MAT
(0to
10)
741(210)
796(211)
693
(203)
731(207)
j0051
Expectationfortreatmenteffect
towards
LAT
(0to
10)
741(213)
808
(200)
687
(209)
725(
215)
j0016lowast
Averagee
xpectatio
nfor
treatmenteffect
(0to
10)
773(213
)840
(203)
720(203)
757(218
)j
0016lowast
Earitchinessyen
16(109
)8lowast
(resolve
automatically)
2lowast(resolve
automatically)
6lowast(resolve
automatically)
---
Evidence-Based Complementary and Alternative Medicine 9
Table2Con
tinued
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Tend
ernesson
acup
ointsyen
20(136
)9lowast
(resolve
automatically)
1lowast(resolve
automatically)
10lowast
(resolve
automatically)
---
Satisfactiontowards
therapy(
0to
10)yen
758(237
)78
6(203)
702(268)
758(237
)j
0225
Thou
ghtthattheymight
bereceivingplacebotre
atmentyen
No
126(900
)39
4146
0011lowast
Yes
14(100
)10
31
Will
recommendthistherapyto
othersyen
0166
Definitelywill
109(757
)38
2942
Maybe
20(139
)5
96
No
15(104
)6
72
Mean(stand
arddeviation)
unlessotherw
iseno
ted
ΩAssociatio
nbetweenvaria
bles
was
determ
ined
bychi-s
quarea
nalyseso
rFish
errsquos-exacttestw
here
approp
riate
Evaluated
beforetheinterventio
nyenE
valuated
after
theinterventionhasb
eencompleted
lowastldquoC
ertainrdquoc
ausality
jOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
10 Evidence-Based Complementary and Alternative Medicine
Table3Outcomev
ariables
acrossthreeg
roup
satd
ifferenttim
epoints
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PSQI(total)(0-21)
Baselin
e1268(044)
1290(062)
1234(034)
Postinterventio
n94
6(052
)99
1(055)
848
(051)
023
(-14
418
9)-065(
-23610
6)087
(-055230)
6we
eksfollowup
907(053
)92
5(065)
926(054)
-050(-207197)
053
(-114219)
-058(-254138)
3mon
thsfollowup
912(079)
781(068)
906(058)
-154(-400
093)
027
(-18
8242)
-181(-399037)
6-mon
thfollo
wup
820
(062)
796(067)
846
(066)
-047(-268175)
059
(-13
8256)
-106(-316105)
Sleeplatency(minutes)
Baselin
e2682(333
)2916
(359)
2517
(286)
Postinterventio
n2529(297)
2500(332
)2617
(303)
(-1329802)
223
(-8111257)
-486(-1533
560)
6we
eksfollowup
1935(322)
2656(339
)2368(330)
487
(-77
31747)
567
(-589172
3)-080(-11771018
)3m
onthsfollowup
1799
(337
)2129(356)
2390(422)
096
(-11491341)
725(
-6932143)
-629(-2065807)
6-mon
thfollo
wup
1966(531
)2342(539
)1907(434)
143(-15791864)
076
(-15341686)
067
(-15851718)
Totalslee
ptim
e(hours)
Baselin
e393
(027)
375
(028)
361
(030)
Postinterventio
n393
(249)
405
(030)
396
(029)
031(-067128)
035
(-065136)
-005(
-117108)
6we
eksfollowup
381
(027)
390
(029)
385
(025)
027
(06812
3)036
(-059131
)-009(-116099)
3mon
thsfollowup
366
(044)
426
(049)
338
(024)
077
(-081236)
0034(-13
213
9)074
(-061209)
6-mon
thfollo
wup
392
(049)
442
(061)
371
(045)
068
(-10
3238)
0112(-14
516
8)057
(-114227)
Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

8 Evidence-Based Complementary and Alternative Medicine
Table2Re
ported
adversee
ffectsexpectationsand
satisfactiontowards
thetherapy
yen
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Havey
ouused
complem
entary
therapiesinthep
ast
permil0423
No
96(653
)33
3330
Yes
51(347
)17
1321
How
muchfaith
doyouhave
incomplem
entary
therapiesin
general
(0to
10)
782(213
)840
(194)
748(218
)75
5(218
)j
0056
Expectationfortreatmenteffect
towards
MAT
(0to
10)
741(210)
796(211)
693
(203)
731(207)
j0051
Expectationfortreatmenteffect
towards
LAT
(0to
10)
741(213)
808
(200)
687
(209)
725(
215)
j0016lowast
Averagee
xpectatio
nfor
treatmenteffect
(0to
10)
773(213
)840
(203)
720(203)
757(218
)j
0016lowast
Earitchinessyen
16(109
)8lowast
(resolve
automatically)
2lowast(resolve
automatically)
6lowast(resolve
automatically)
---
Evidence-Based Complementary and Alternative Medicine 9
Table2Con
tinued
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Tend
ernesson
acup
ointsyen
20(136
)9lowast
(resolve
automatically)
1lowast(resolve
automatically)
10lowast
(resolve
automatically)
---
Satisfactiontowards
therapy(
0to
10)yen
758(237
)78
6(203)
702(268)
758(237
)j
0225
Thou
ghtthattheymight
bereceivingplacebotre
atmentyen
No
126(900
)39
4146
0011lowast
Yes
14(100
)10
31
Will
recommendthistherapyto
othersyen
0166
Definitelywill
109(757
)38
2942
Maybe
20(139
)5
96
No
15(104
)6
72
Mean(stand
arddeviation)
unlessotherw
iseno
ted
ΩAssociatio
nbetweenvaria
bles
was
determ
ined
bychi-s
quarea
nalyseso
rFish
errsquos-exacttestw
here
approp
riate
Evaluated
beforetheinterventio
nyenE
valuated
after
theinterventionhasb
eencompleted
lowastldquoC
ertainrdquoc
ausality
jOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
10 Evidence-Based Complementary and Alternative Medicine
Table3Outcomev
ariables
acrossthreeg
roup
satd
ifferenttim
epoints
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PSQI(total)(0-21)
Baselin
e1268(044)
1290(062)
1234(034)
Postinterventio
n94
6(052
)99
1(055)
848
(051)
023
(-14
418
9)-065(
-23610
6)087
(-055230)
6we
eksfollowup
907(053
)92
5(065)
926(054)
-050(-207197)
053
(-114219)
-058(-254138)
3mon
thsfollowup
912(079)
781(068)
906(058)
-154(-400
093)
027
(-18
8242)
-181(-399037)
6-mon
thfollo
wup
820
(062)
796(067)
846
(066)
-047(-268175)
059
(-13
8256)
-106(-316105)
Sleeplatency(minutes)
Baselin
e2682(333
)2916
(359)
2517
(286)
Postinterventio
n2529(297)
2500(332
)2617
(303)
(-1329802)
223
(-8111257)
-486(-1533
560)
6we
eksfollowup
1935(322)
2656(339
)2368(330)
487
(-77
31747)
567
(-589172
3)-080(-11771018
)3m
onthsfollowup
1799
(337
)2129(356)
2390(422)
096
(-11491341)
725(
-6932143)
-629(-2065807)
6-mon
thfollo
wup
1966(531
)2342(539
)1907(434)
143(-15791864)
076
(-15341686)
067
(-15851718)
Totalslee
ptim
e(hours)
Baselin
e393
(027)
375
(028)
361
(030)
Postinterventio
n393
(249)
405
(030)
396
(029)
031(-067128)
035
(-065136)
-005(
-117108)
6we
eksfollowup
381
(027)
390
(029)
385
(025)
027
(06812
3)036
(-059131
)-009(-116099)
3mon
thsfollowup
366
(044)
426
(049)
338
(024)
077
(-081236)
0034(-13
213
9)074
(-061209)
6-mon
thfollo
wup
392
(049)
442
(061)
371
(045)
068
(-10
3238)
0112(-14
516
8)057
(-114227)
Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Evidence-Based Complementary and Alternative Medicine 9
Table2Con
tinued
All
(n=147)
Group
1PlaceboLA
TampMAT
(n=5
0)
Group
2LA
TampplaceboMAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)P-value
Tend
ernesson
acup
ointsyen
20(136
)9lowast
(resolve
automatically)
1lowast(resolve
automatically)
10lowast
(resolve
automatically)
---
Satisfactiontowards
therapy(
0to
10)yen
758(237
)78
6(203)
702(268)
758(237
)j
0225
Thou
ghtthattheymight
bereceivingplacebotre
atmentyen
No
126(900
)39
4146
0011lowast
Yes
14(100
)10
31
Will
recommendthistherapyto
othersyen
0166
Definitelywill
109(757
)38
2942
Maybe
20(139
)5
96
No
15(104
)6
72
Mean(stand
arddeviation)
unlessotherw
iseno
ted
ΩAssociatio
nbetweenvaria
bles
was
determ
ined
bychi-s
quarea
nalyseso
rFish
errsquos-exacttestw
here
approp
riate
Evaluated
beforetheinterventio
nyenE
valuated
after
theinterventionhasb
eencompleted
lowastldquoC
ertainrdquoc
ausality
jOne-w
ayanalysisof
varia
nce
Fisherrsquosexacttest
permilCh
i-squ
aretest
lowastStatisticallysig
nificantatPlt005
10 Evidence-Based Complementary and Alternative Medicine
Table3Outcomev
ariables
acrossthreeg
roup
satd
ifferenttim
epoints
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PSQI(total)(0-21)
Baselin
e1268(044)
1290(062)
1234(034)
Postinterventio
n94
6(052
)99
1(055)
848
(051)
023
(-14
418
9)-065(
-23610
6)087
(-055230)
6we
eksfollowup
907(053
)92
5(065)
926(054)
-050(-207197)
053
(-114219)
-058(-254138)
3mon
thsfollowup
912(079)
781(068)
906(058)
-154(-400
093)
027
(-18
8242)
-181(-399037)
6-mon
thfollo
wup
820
(062)
796(067)
846
(066)
-047(-268175)
059
(-13
8256)
-106(-316105)
Sleeplatency(minutes)
Baselin
e2682(333
)2916
(359)
2517
(286)
Postinterventio
n2529(297)
2500(332
)2617
(303)
(-1329802)
223
(-8111257)
-486(-1533
560)
6we
eksfollowup
1935(322)
2656(339
)2368(330)
487
(-77
31747)
567
(-589172
3)-080(-11771018
)3m
onthsfollowup
1799
(337
)2129(356)
2390(422)
096
(-11491341)
725(
-6932143)
-629(-2065807)
6-mon
thfollo
wup
1966(531
)2342(539
)1907(434)
143(-15791864)
076
(-15341686)
067
(-15851718)
Totalslee
ptim
e(hours)
Baselin
e393
(027)
375
(028)
361
(030)
Postinterventio
n393
(249)
405
(030)
396
(029)
031(-067128)
035
(-065136)
-005(
-117108)
6we
eksfollowup
381
(027)
390
(029)
385
(025)
027
(06812
3)036
(-059131
)-009(-116099)
3mon
thsfollowup
366
(044)
426
(049)
338
(024)
077
(-081236)
0034(-13
213
9)074
(-061209)
6-mon
thfollo
wup
392
(049)
442
(061)
371
(045)
068
(-10
3238)
0112(-14
516
8)057
(-114227)
Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

10 Evidence-Based Complementary and Alternative Medicine
Table3Outcomev
ariables
acrossthreeg
roup
satd
ifferenttim
epoints
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PSQI(total)(0-21)
Baselin
e1268(044)
1290(062)
1234(034)
Postinterventio
n94
6(052
)99
1(055)
848
(051)
023
(-14
418
9)-065(
-23610
6)087
(-055230)
6we
eksfollowup
907(053
)92
5(065)
926(054)
-050(-207197)
053
(-114219)
-058(-254138)
3mon
thsfollowup
912(079)
781(068)
906(058)
-154(-400
093)
027
(-18
8242)
-181(-399037)
6-mon
thfollo
wup
820
(062)
796(067)
846
(066)
-047(-268175)
059
(-13
8256)
-106(-316105)
Sleeplatency(minutes)
Baselin
e2682(333
)2916
(359)
2517
(286)
Postinterventio
n2529(297)
2500(332
)2617
(303)
(-1329802)
223
(-8111257)
-486(-1533
560)
6we
eksfollowup
1935(322)
2656(339
)2368(330)
487
(-77
31747)
567
(-589172
3)-080(-11771018
)3m
onthsfollowup
1799
(337
)2129(356)
2390(422)
096
(-11491341)
725(
-6932143)
-629(-2065807)
6-mon
thfollo
wup
1966(531
)2342(539
)1907(434)
143(-15791864)
076
(-15341686)
067
(-15851718)
Totalslee
ptim
e(hours)
Baselin
e393
(027)
375
(028)
361
(030)
Postinterventio
n393
(249)
405
(030)
396
(029)
031(-067128)
035
(-065136)
-005(
-117108)
6we
eksfollowup
381
(027)
390
(029)
385
(025)
027
(06812
3)036
(-059131
)-009(-116099)
3mon
thsfollowup
366
(044)
426
(049)
338
(024)
077
(-081236)
0034(-13
213
9)074
(-061209)
6-mon
thfollo
wup
392
(049)
442
(061)
371
(045)
068
(-10
3238)
0112(-14
516
8)057
(-114227)
Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Evidence-Based Complementary and Alternative Medicine 11
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
Wakea
fterslee
ponset
(minutes)
Baselin
e9232
(1283)
9051(1464)
8833
(1031)
Postinterventio
n6944(1041)
7160(949)
6584(886)
397
(-22032996)
038
(-23412418
)358
(-24423159)
6we
eksfollowup
5145(510
)6140(860)
6234(707)
1176
(-24444795)
1488(-1749472
5)-313
(-39793354)
3mon
thsfollowup
5082(913
)7474
(2096)
6390(1200
)2573(
-3806
895
1)1706
(-304364
55)
867
(-55727306)
6-mon
thfollo
wup
4881(96
6)8087(2646
)6159(110
4)3387(-385710630)
1677(-307164
24)
1710
(-55558975)
Sleepeffi
ciency()
Baselin
e7234(223)
7406(238)
7070(223)
Postinterventio
n7828(190)
7694(193)
7886(164)
-306(-852240)
222
(-406
850)
-528(-116110
5)6we
eksfollowup
7757(180)
7614
(249)
7457(221)
-314
(-93
1303)
-136(-77
1500
)-178(-875518
)12-w
eekfollo
wup
8132
(198)
7802(356)
7882(234)
-503(
-1544
539
)-087(-1027854)
-416
(-1543710)
6-mon
thfollo
wup
7602(
484)
7737
(464)
8019
(220)
-037
(-14641390)
581
(-618178
0)-618
(-1897662)
SF-12
(PCS
)Ba
selin
e40
87(109)
4184(137
)4164(119
)-
Postinterventio
n44
46(123)
4312
(138)
4296(122)
231
(-600
139
)-227(-569114
)-0035
(-362355)
6-we
eksfollowup
4504(134)
4258(144)
4033
(151)
-342(-75
1066
)-547(-98
9-106)lowast
205
(-206
615
)3m
onthsfollowup
4555(
134)
4621(14
2)4130(166)
-031
(-469407)
-502(
-953
-052)lowast
472
(013
930)lowast
6-mon
thfollo
wup
4626(136)
4596(141)
4199(229)
-126(-563311)
-503(
-1055048)
377
(-206
960)
SF-12
(MCS
)Ba
selin
e4799(163)
4577(195)
4605(163)
Postinterventio
n5184(164)
4735(
178)
5058(137
)-226(-710257)
0675(-402537
)-294(-74
215
4)6we
eksfollowup
5097(161)
5089(184)
5315
(165)
214
(-262690)
412
(-095918
)-198(-673277)
3mon
thsfollowup
4805(231
)5131
(227)
5055(
176)
548
(-15
21247)
444
(-18
01067)
104(-538747)
6-mon
thfollo
wup
5164(200)
5224(205)
5105(220)
282
(-383947)
135(-524794)
147(-541836)
12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

12 Evidence-Based Complementary and Alternative Medicine
Table3Con
tinued
Pairw
isecomparis
onsb
etwe
engrou
ps998787
Group
1PlaceboLA
Tamp
MAT
(n=5
0)
Group
2LA
Tampplacebo
MAT
(n=4
6)
Group
3Com
binedAT
(n=5
1)Group
1vsG
roup
2Group
1vsG
roup
3Group
3vs
Group
2
Estim
ated
mean
(SE)
nEstim
ated
mean
(SE)
nEstim
ated
mean
(SE)
n120573(95
CI)
120573(95
CI)
120573(95
CI)
PHQ-9
(0-27)
Baselin
e95
2(074
)94
8(096)
940(086)
Postinterventio
n630
(071)
677
(095)
646
(079)
0504(-15
2252)
028
(-17
8235)
022
(-17
2217)
6we
eksfollowup
687
(100)
649
(111)
500
(071)
-035(
-273204
)-175(-429078)
141(-064345)
3mon
thsfollowup
658
(120)
568
(129)
655
(119
)ndash0
87(-393221)
009
(-308326)
-096(-405214
)6-mon
thfollo
wup
477
(097)
582
(130)
568
(105)
110(-18
8401)
104(-18
7395)
006
(-307318
)nE
stimated
meanandsta
ndarderror(SE
)from
generalized
estim
atingequatio
ns
PSQIPittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
for
depressio
n998787Ad
juste
dfora
ge
lowastStatisticallysig
nificantatPlt005
Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Evidence-Based Complementary and Alternative Medicine 13
Table4Ch
ange
indifferent
outcom
evariables
over
timefor
individu
algrou
psusinggeneralized
estim
atingequatio
ns
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
1PlaceboLA
TampMAT
(119899=5
0)PS
QI(0-21total)
-321(-456-187)
000
0lowastlowastlowast
-361(-483-238)
000
0lowastlowastlowast
-356(-528-18
3)000
0lowastlowastlowast
-447(-595-300
)000
0lowastlowastlowast
Sleeplatency(
minutes)
-153
(-897592)
0688
-747(-1674
181)
0115
-883(-1748-018)
004
5lowast-716
(-1908475)
0239
Totalsleep
time(
hours)
-001(-059058)
0989
-012
(-069045)
0681
-027(-13
9086)
064
2-001(-112
109)
0985
Wakea
ftersleep
onset
(minutes)
-2287
(-3801-774
)0003lowastlowast
-4087
(-6338
-1836)
000
0lowastlowastlowast
-414
9(-7447-852
)0014lowast
-4351
(-7726-976
)0012lowast
Sleepeffi
ciency
()
594
(212
976
)0002lowastlowast
522
(13690
9)000
8lowastlowast
898
(3071490)
0003lowastlowast
368
(-5991335)
0455
SF12
(PCS
)359
(109609)
000
5lowastlowast
416
(10672
7)000
9lowastlowast
468
(16477
2)0003lowastlowast
538
(258819)
000
0lowastlowastlowast
SF12
(MCS
)385
(02974
1)0034lowast
298
(061657)
0103
006
(-476488)
0980
365
(-083812
)0110
PHQ-9
(0-27)
-322(-473-17
1)000
0lowastlowastlowast
-265(-463-066
)000
9lowastlowast
-294(-517-071)
0010lowast
-475(
-669-282)
000
0lowastlowastlowast
Group
2LA
TampplaceboMAT
(n=4
6)PS
QI(0-21total)
-299(-396-202)
000
0lowastlowastlowast
-366(-526-205)
000
0lowastlowastlowast
-509(-685-333)
000
0lowastlowastlowast
-494(-660
-328)
000
0lowastlowastlowast
Sleeplatency(
minutes)
-416
(-1178346)
0284
-259(-1115596)
0552
-787(-168210
8)0085
-574
(-1818
671)
0366
Totalsleep
time(
hours)
030
(-047108)
044
4015
(-061092)
0695
051
(-061162)
0375
067
(-064
197)
0316
Wakea
ftersleep
onset
(minutes)
-1891
(-40
04223)
0080
-291
1(-574
9-072)
004
4lowast-1576
(-70403888)
0572
-964(-74215494)
0770
Sleepeffi
ciency
()
288
(-10
3678)
0148
208
(-272689)
0396
396
(-4621253)
0366
331
(-7321395)
0542
SF12
(PCS
)12
8(-14
4400
)0357
074
(-19
1339)
0585
437
(121753)
000
7lowastlowast
412
(07574
9)0017lowast
SF12
(MCS
)15
8(-16
8485)
0341
512
(199825)
000
1lowastlowast
554
(0481061)
0032lowast
647
(1551139)
0010lowast
PHQ-9
(0-27)
-272(
-406-138)
000
0lowastlowastlowast
-299(-431-16
7)000
0lowastlowastlowast
-380(-592-16
9)000
0lowastlowastlowast
-366(-591-14
1)000
1lowastlowast
14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

14 Evidence-Based Complementary and Alternative Medicine
Table4Con
tinued
Post-
hoca
nalyses998787
(1)v
s(2)
(1)v
s(3)
(1)v
s(4)
(1)v
s(5)
120573(95
CI)
p-value
120573(95
CI)
119901-value
120573(95
CI)
p-value
120573(95
CI)
p-value
Group
3Com
binedAT
(n=5
1)PS
QI(0-21total)
-386(-491-282)
000
0lowastlowastlowast
-308(-420-19
5)000
0lowastlowastlowast
-328(-457-200
)000
0lowastlowastlowast
-388(-518258)
000
0lowastlowastlowast
Sleeplatency(
minutes)
070
(-647788)
0848
-180(-870510
)0610
-158(-128296
7)0784
-640(-1734454)
0251
Totalsleep
time(
hours)
035
(-046
116
)0399
024
(-052100)
0535
-023(
-099052)
0543
010
(-10
012
1)0858
Wakea
ftersleep
onset
(minutes)
-2249
(-40
86-412
)0016lowast
-2598
(-4925-272)
0029lowast
-2443
(-586297
6)0161
-2674
(-60
4970
1)0120
Sleepeffi
ciency
()
816
(118
1314)
000
1lowastlowast
387
(-118891)
0133
812
(0801544)
0030lowast
949(231
1668)
0010lowast
SF12
(PCS
)13
2(-10
1364
)0268
-131
(-445182)
0413
-035(
-367298)
0839
035
(-440
510
)0886
SF12
(MCS
)452
(146759)
000
4lowastlowast
710(352
1067)
000
0lowastlowastlowast
450
(055845)
0026lowast
500
(018
982)
004
2lowastPH
Q-9
(0-27)
-294(-435-15
3)000
0lowastlowastlowast
-440(-597-283)
000
0lowastlowastlowast
-285(
-510
-059)
0013lowast
-371(-589-154)
000
1lowastlowast
SEstand
arderrorCI
con
fidence
interval
Timepoints(1)=
baselin
e(2)=
postintervention
(3)=
6-we
ekfollo
wup
(4)
=3-mon
thfollo
wup
and
(5)=
6-mon
thfollo
w-up
998787Ad
juste
dfora
ge
PSQI=
Pittsbu
rghsle
epqu
ality
index
SF-12(PCS
)ph
ysicalcompo
nent
score
SF-12(M
CS)mentalcom
ponent
score
PHQ-9P
atient
Health
Question
naire
lowastStatisticallysig
nificantatPlt005
lowastlowastStatisticallysig
nificantatPlt001
lowastlowastlowastStatisticallysig
nificantatPlt000
1
Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Evidence-Based Complementary and Alternative Medicine 15
Randomised (n=147)
44 completed (957)Lost to follow-up (n=1)
Trip (n=1)
49 completed (980)Lost to follow-up (n=0)
47 completed (922)Lost to follow-up (n=1)
Sickness (n=1)
Three-Month Follow-Up
49 completed (980)Lost to follow-up (n=0)
48 completed (941)Lost to follow-up (n=1)
Trip (n=1)
45 completed (980)Lost to follow-up (n=0)
Six-Week Follow-Up
Assessed for eligibility (n=166)
Excluded (n=19)
Not meeting inclusion criteria (n=9)Declined to participate (n=3)Poor cognitive functions (n=7)
Enrollment
Group 1Placebo LAT + MAT
(n=50)
Group 3Combined intervention
(LAT + MAT)(n=51)
Allocation
Group 2LAT+ placebo MAT
(n=46)
49 completed (961)Loss to follow-up (n=2)
Hospitalization (n=2)
49 completed (980)Loss to follow-up (n=1)
Hospitalization (n=1)
45 completed (980)Loss to follow-up (n=1)
Mobility restriction (n=1)
Post-Intervention
Figure 4 Flowchart of recruitment
for LAT administration such as daily application adoptedin previous studies [41ndash44] may be considered in futurestudies to enhance the treatment effect and possibly improveits synergistic effect when combined with MAT
Numerous clinical trials reported the use of MAT ondifferent disorders including but not limited to sleep dis-turbances [12 45 46] low back pain [13] constipation [14]and obesity [47] The effectiveness of MAT may relate to the
interaction of magnetic fields with blood flow and calciumchannel proteins in the cell membrane Such interactionsmay elicit functional body changes [16 48 49] MeanwhileLAT is a noninvasive alternative to needle acupuncture [22]and has been adopted to increase pain threshold [50] aswell as relieve musculoskeletal pain [18] and insomnia [17]The laser beam not only irradiates and stimulates acupointsbut also triggers the energy flow (qi) and regulates the
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom
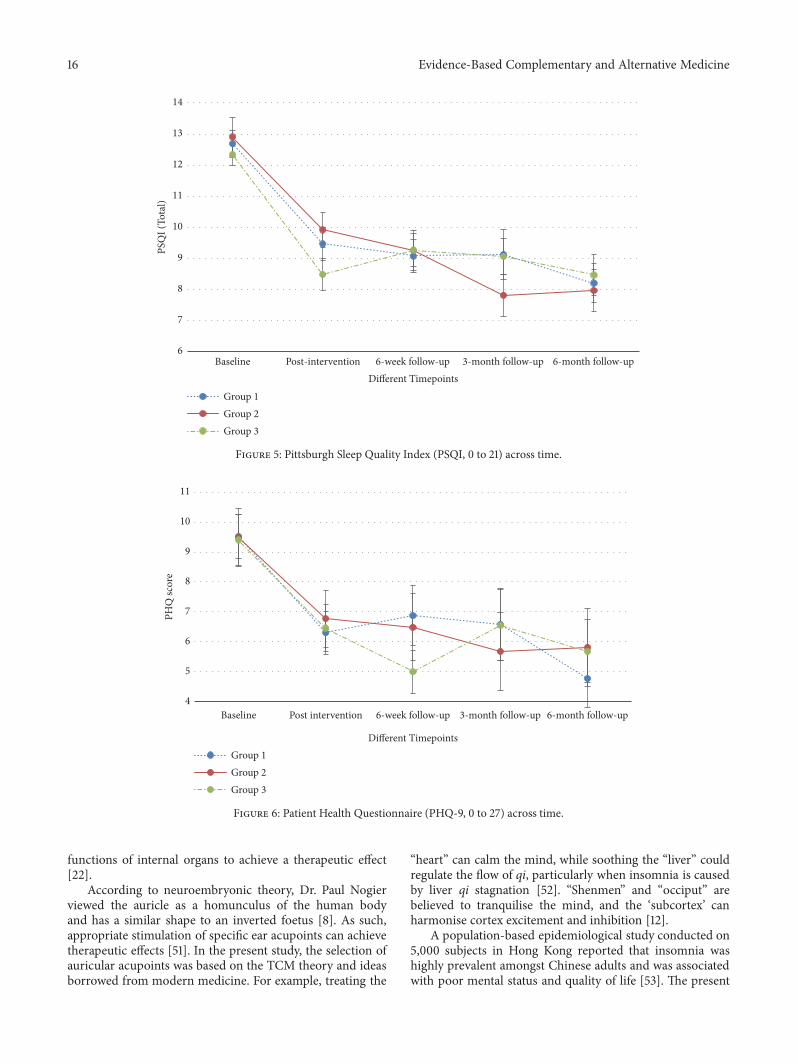
16 Evidence-Based Complementary and Alternative Medicine
Baseline Post-intervention 6-week follow-up 3-month follow-up 6-month follow-upDifferent Timepoints
Group 1Group 2Group 3
6
7
8
9
10
11
12
13
14
PSQ
I (To
tal)
Figure 5 Pittsburgh Sleep Quality Index (PSQI 0 to 21) across time
Group 1Group 2Group 3
Baseline Post intervention 6-week follow-up 3-month follow-up 6-month follow-up
Different Timepoints
4
5
6
7
8
9
10
11
PHQ
scor
e
Figure 6 Patient Health Questionnaire (PHQ-9 0 to 27) across time
functions of internal organs to achieve a therapeutic effect[22]
According to neuroembryonic theory Dr Paul Nogierviewed the auricle as a homunculus of the human bodyand has a similar shape to an inverted foetus [8] As suchappropriate stimulation of specific ear acupoints can achievetherapeutic effects [51] In the present study the selection ofauricular acupoints was based on the TCM theory and ideasborrowed from modern medicine For example treating the
ldquoheartrdquo can calm the mind while soothing the ldquoliverrdquo couldregulate the flow of qi particularly when insomnia is causedby liver qi stagnation [52] ldquoShenmenrdquo and ldquoocciputrdquo arebelieved to tranquilise the mind and the lsquosubcortexrsquo canharmonise cortex excitement and inhibition [12]
A population-based epidemiological study conducted on5000 subjects in Hong Kong reported that insomnia washighly prevalent amongst Chinese adults and was associatedwith poor mental status and quality of life [53] The present
Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Evidence-Based Complementary and Alternative Medicine 17
study reported PCS scores of the subjects comparable withthose of Hong Kong people with insomnia (4321 in ourstudy versus 4139 population norm) but stated a slightlyhigherMCS (4668 versus 3636)HRQOL (in PCS andMCS)improved and depression declined over time in subjectstreated with AT Thus quality of life and emotional statusof the subjects may be positively associated with sleepimprovement after the therapy
No specific adverse effectswere observed to arise from thetherapy apart from a small number of reported cases (109)having mild skin irritation on the ears from the adhesivetapes used to hold the experimental tools in place Moreover20 cases (136) reported tenderness on the acupoints andmost of these subjects received MAT According to theauricular diagnosis system the areas of the auricle withheightened tenderness upon touching correspond to specificareas of the body where pathological conditions exist [5455] Applying magnetic pellets may induce physical pressureon the ear acupoints and cause tenderness especially incases with disequilibrium of bodily functions (eg insomnia)corresponding to specific acupoints The tenderness on thereflective acupoints experienced by the subjects may beconsidered part of the treatment process rather than adverseeffects of AT
The high compliance rate (952) and positive impres-sion of the therapy indirectly indicated that blinding wassuccessful because of the successful placebo applicationin the trial Over 75 of the participants expressed thatthey would definitely recommend the therapy to othersThe findings of this trial can provide valuable informationand increase understanding of the therapeutic effect of ATwhether separate or combinedMATandLAT Longer therapyduration may be considered in future trials to determinefurther improvements in the outcome variables The pro-posed treatment approach can be considered as a noninvasivestrategy for managing insomnia amongst the elderly
Although actigraphic monitoring is a reliable objectivemeasure in sleep study changes in different sleep stagescaused by the therapy cannot be ascertained The recruitedelders generally obtained low education levels and had amean age of over 75 and therefore using a sleep log toverify the actigraphic data was not feasible Night-to-nightvariability in the sleeping patterns of subjects may also beaffected by physical psychological andor environmentalfactors Due to the above limitations the actigraphic datamust be interpreted with caution The exact mechanismsremain unknown regarding the interaction of magnetic fieldswith biological tissues which results in functional changesFurther studies from the biomedical perspective are requiredto elucidate the biological pathway of the treatment and effectsuch as to examine the impact of the treatment protocolson the changes in sleep biomarkers when sleep prosperity isachieved
5 Implications
This study provides valuable findings regarding the therapeu-tic effect of different protocols usingMAT LAT or their com-bination In general the AT protocols under testing may be
considered as a noninvasive approach with minimal adverseeffects for managing sleep problems amongst the elderlyThe findings of this study provide important implications toguide future research and apply evidence-based practice inthe community via service provision tomanage this commonproblem
6 Conclusion
The treatment effects of the three protocols were comparablein terms of self-reported sleep conditions HRQOL anddepression status In several parameters such therapeuticeffects may be sustained at six-month follow-up Significantimprovement in the objective sleep parameters could beobserved in subjects who received MAT protocols but notin those who received LAT The combined MAT and LATapproach did not show any advantage over MAT Longertherapeutic course and more frequent administration of LATmay be considered in future trials to achieve the optimaltreatment effect In general the proposed AT protocolswere demonstrated to be a well-received treatment modalitywith minimal adverse effects and effectively improved sleepconditions of the elderly with insomnia
Data Availability
The datasets used andor analysed during the current studyare available from the corresponding author on reasonablerequest
Ethical Approval
Ethical approval from the Human Research Ethics ReviewCommittee of the Hong Kong Polytechnic University wasgranted [Reference no HSEARS20151129001] Participationin the study was on a voluntary basis All potential par-ticipants were assured that they could withdraw from thestudy at any time Personal information and data remainedconfidential and anonymous
Consent
Written informed consent was obtained from each partici-pant upon recruitment
Conflicts of Interest
The authors declare that they have no conflicts of interest
Authorsrsquo Contributions
Lorna K P Suen was the principal investigator Lorna KP Suen A Molassiotis and C H Yeh were involved inconception and design of the study S K W Yueng collectedthe data Lorna K P Suen was responsible for data analysisLorna K P Suen drafted the manuscript with the supportof all authors All authors read and approved the finalmanuscript
18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

18 Evidence-Based Complementary and Alternative Medicine
Acknowledgments
The authors extend their appreciation to the elderly centresand participants for their sincere support for this studyThis project was supported by the Health and MedicalResearch Fund Food and Health Bureau Hong Kong SARGovernment (13144061)
Supplementary Materials
Figure S1 wake after sleep onset (minutes) across timeFigure S2 sleep efficiency () across time Figure S3 SF-12(physical component) across time Figure S4 SF-12 (mentalcomponent) across time (Supplementary Materials)
References
[1] K K Gulia and V M Kumar ldquoSleep disorders in the elderly agrowing challengerdquo Psychogeriatrics vol 18 no 3 pp 155ndash1652018
[2] V Sagayadevan E Abdin S Binte Shafie et al ldquoPrevalenceand correlates of sleep problems among elderly SingaporeansrdquoPsychogeriatrics vol 17 no 1 pp 43ndash51 2017
[3] J Yu I Rawtaer J Fam et al ldquoSleep correlates of depression andanxiety in an elderly Asian populationrdquo Psychogeriatrics vol 16no 3 pp 191ndash195 2016
[4] Y Zhang M Cifuentes X Gao G Amaral and K L TuckerldquoAge- and gender-specific associations between insomnia andfalls in Boston Puerto Rican adultsrdquo Quality of Life Researchvol 26 no 1 pp 25ndash34 2017
[5] M van de Laar D Pevernagie P van Mierlo and S OvereemldquoCorrelates of general quality of life are different in patientswithprimary insomnia as compared to patients with insomnia andpsychiatric comorbidityrdquoPsychology HealthampMedicine vol 22no 2 pp 172ndash183 2017
[6] M R Rosekind and K B Gregory ldquoInsomnia risks and costshealth safety and quality of liferdquo The American Journal ofManaged Care vol 16 no 8 pp 617ndash626 2010
[7] D J Buysse ldquoInsomniardquo The Journal of the American MedicalAssociation vol 309 no 7 pp 706ndash716 2013
[8] T OlesonAuriculotherapyManual Churchill Livingstone Else-vier Edinburgh Scotland 4th edition 2014
[9] S AbbateChinese Auricular Acupuncture CRC Press Taylor ampFrancis Group Boca Raton Fla USA 2nd edition 2015
[10] N Soliman Solimanrsquos Auricular Therapy Textbook New Local-izations And Evidence Based Therapeutic Approaches Author-House Bloomington Indiana 2008
[11] L K P Suen T K SWong andAWN Leung ldquoIs there a placefor auricular therapy in the realm of nursingrdquo ComplementaryTherapies in Nursing and Midwifery vol 7 no 3 pp 132ndash1392001
[12] L K P Suen T K S Wong and A W N Leung ldquoEffectivenessof auricular therapy using magnetic pearls on sleep promotionin the elderlyrdquo The American Journal of Chinese Medicine vol30 no 4 pp 429ndash499 2002
[13] L K P Suen and E M C Wong ldquoLongitudinal changes in thedisability level of the elders with low back pain after auriculo-therapyrdquo Complementary Therapies in Medicine vol 16 no 1pp 28ndash35 2008
[14] M K Li T F D Lee and K P L Suen ldquoComplementary effectsof auricular acupressure in relieving constipation symptoms
and promoting disease-specific health-related quality of life arandomized placebo-controlled trialrdquo Complementary Thera-pies in Medicine vol 22 no 2 pp 266ndash277 2014
[15] L K P Suen S Y Chair D R Thompson et al ldquoTraditionalauriculotherapy for hypertension a pilot randomized trialrdquoJournal of Cardiovascular Disease vol 2 pp 19ndash24 2014
[16] DWRamey ldquoMagnetic and electromagnetic therapyrdquo ScientificReview of Alternative Medicine vol 2 no 1 pp 13ndash19 1998
[17] S Y Yao ldquo46 cases of insomnia treated by semiconductor laserirradiation on auricular pointsrdquo Journal of Traditional ChineseMedicine vol 19 no 4 pp 298-299 1999
[18] W J Kneebone ldquoLaser acupuncture as a pain relief modalityrdquoPractical Pain Management pp 64ndash68 2008
[19] W-L Hu C-H Chang and Y-C Hung ldquoClinical observationson laser acupuncture in simple obesity therapyrdquo AmericanJournal of Chinese Medicine vol 38 no 5 pp 861ndash867 2010
[20] C X Zhao ldquoLaser acupuncture combined with ear-pointpressing for bed-wettingrdquo International Journal of ClinicalAcupuncture vol 6 no 1 pp 69ndash71 1995
[21] Q Xia ldquoLaser auriculotherapy combined with auricular press-ing therapy in 30 cases with alcoholic addictionrdquo ChineseJournal of Information on Traditional Chinese Medicine vol 13no 2 p 56 2006 (Chinese)
[22] D Z Tian ldquoLaser acupuncture andTCM (Part I)rdquo InternationalJournal of Clinical Acupuncture vol 7 no 4 pp 397ndash399 1996
[23] T Roth ldquoInsomnia Definition prevalence etiology and con-sequencesrdquo Journal of Clinical Sleep Medicine vol 3 no 5 ppS7ndashS10 2007
[24] Diagnostic and Statistical Manual of Mental Disorders TheDiagnosis of Insomnia (DSM-5) American Psychiatric Associ-ation Arlington VA USA 5th edition 2013
[25] China Standardization Organizing Committee Nomenclatureand Location of Auricular Points (GBT 13734-2008) ZhijianPublishingHouse and Standards Press of China Beijing China2008
[26] R Round G Litscher and F Bahr ldquoAuricular acupuncturewith laserrdquo Evidence-Based Complementary and AlternativeMedicine vol 2013 Article ID 984763 22 pages 2013
[27] A M L Chong and C-K Cheung ldquoFactor structure of aCantonese-version pittsburgh sleep quality indexrdquo Sleep andBiological Rhythms vol 10 no 2 pp 118ndash125 2012
[28] C L K Lam E Y Y Tse and B Gandek ldquoIs the standard SF-12Health Survey valid and equivalent for a Chinese populationrdquoQuality of Life Research vol 14 no 2 pp 539ndash547 2005
[29] AMartinW Rief A Klaiberg and E Braehler ldquoValidity of thebrief Patient Health Questionnaire Mood Scale (PHQ-9) in thegeneral populationrdquo General Hospital Psychiatry vol 28 no 1pp 71ndash77 2006
[30] Z Liu Y Yu M Hu et al ldquoPHQ-9 and PHQ-2 for screeningdepression in chinese rural elderlyrdquo PLoS ONE vol 11 no 3Article ID e0151042 2016
[31] D Kalauokalani D C Cherkin K J Sherman T D Koepselland R A Deyo ldquoLessons from a trial of acupuncture andmassage for low back pain patient expectations and treatmenteffectsrdquoThe Spine Journal vol 26 no 13 pp 1418ndash1424 2001
[32] M L Bell N J Horton H M Dhillon V J Bray and JVardy ldquoUsing generalized estimating equations and extensionsin randomized trials with missing longitudinal patient reportedoutcome datardquo Psycho-Oncology vol 27 no 9 pp 2125ndash21312018
Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom

Evidence-Based Complementary and Alternative Medicine 19
[33] Y Q Chen and Y Shao ldquoThe combined use of acupuncture andauriculotherapy for patients with insomnia of yin deficiencysyndromerdquo Guangdong Medical Journal vol 34 no 6 pp 966-967 2013
[34] C X Ma ldquoThe combined use of foot bathing and auricular seedpressing for improving sleep quality of the eldersrdquo Journal ofQilu Nursing vol 19 no 21 pp 90-91 2013
[35] Y Wang and X Z Zhu ldquoInfluence of acupoint sticking com-bined with ear pressure beans therapy on sleep quality of elderlypatientswith different syndromes of insomniardquoChineseNursingResearch vol 29 no 7A p 2394 2015
[36] J H Chen LWaite LMKurina R AThistedMMcClintockand D S Lauderdale ldquoInsomnia symptoms and actigraph-estimated sleep characteristics in a nationally representativesample of older adultsrdquoThe Journals of Gerontology vol 70 no2 pp 185ndash192 2015
[37] C M Moore S J Schmiege and E E Matthews ldquoActigraphyand sleep diary measurements in breast cancer survivors dis-crepancy in selected sleep parametersrdquo Behavioral Sleep Medi-cine vol 13 no 6 pp 472ndash490 2015
[38] KM Blytt B Bjorvatn B Husebo and E Flo ldquoClinically signi-ficant discrepancies between sleep problems assessed by stan-dard clinical tools and actigraphyrdquo BMC Geriatrics vol 17 no1 Article ID 253 2017
[39] L K Suen C H Yeh and S K Yeung ldquoUsing auriculotherapyfor osteoarthritic knee among elders a double-blinded ran-domised feasibility studyrdquoBMCComplementary andAlternativeMedicine vol 16 no 1 article no 257 p 9 2016
[40] L K Suen C H Yeh S K Yeung and J W Yeung ldquoIs thecombined auriculotherapy approach superior tomagneto-auri-culotherapy alone in aging males with lower urinary tractsymptoms A randomized controlled trialrdquoThe Aging Male pp1ndash12 2019
[41] Y F Li ldquoLaser auriculotherapy for30 cases of coronary heartdiseasesrdquo Journal of Community Health vol 2 no 1 p 89 2004(Chinese)
[42] G Y Liang ldquoThe use of laser auriculotherapy for insomnia in30 cancer patientsrdquoClinicalMedical Practical Journal vol 5 no6 2006 (Chinese)
[43] L H Sun ldquoHe-Ne laser irradiation plus acupuncture for acnevulgaris in 36 casesrdquo Shanghai Journal of Traditional ChineseMedicine vol 38 no 9 pp 43-44 2004 (Chinese)
[44] G-Y Zhou ldquoModerate and severe sudden deafness treated withlow-energy laser irradiation combined with auricular acupointstickingrdquoChinese Acupuncture ampMoxibustion vol 32 no 5 pp413ndash416 2012 (Chinese)
[45] C Lo W C Liao J J Liaw et al ldquoThe stimulation effect ofauricular magnetic press pellets on older female adults withsleep disturbance undergoing polysomnographic evaluationrdquoEvidence-Based Complementary and Alternative Medicine vol2013 Article ID 530438 8 pages 2013
[46] L K P Suen T K S Wong A W N Leung andW C Ip ldquoThelong-term effects of auricular therapy using magnetic pearls onelderly with insomniardquo Complementary Therapies in Medicinevol 11 no 2 pp 85ndash92 2003
[47] C H Hsieh T-J Su Y-W Fang and P-H Chou ldquoEfficacy oftwo different materials used in auricular acupressure on weightreduction and abdominal obesityrdquo American Journal of ChineseMedicine vol 40 no 4 pp 713ndash720 2012
[48] S L Henry M J Concannon and G J Yee ldquoThe effect of mag-netic fields on wound healingrdquo Journal of Plastic Surgery vol 8pp 393ndash399 2008
[49] C L M Koch M Sommarin B R R Persson L G Salfordand J L Eberhardt ldquoInteraction between weak low frequencymagnetic fields and cell membranesrdquo Bioelectromagnetics vol24 no 6 pp 395ndash402 2003
[50] H Sampaio-Filho S K Bussadori M L Goncalves et al ldquoLow-level laser treatment applied at auriculotherapypoints to reducepostoperative pain in third molar surgery A randomizedcontrolled single-blinded studyrdquo PLoS ONE vol 13 no 6Article ID e0197989 2018
[51] P W Hou H C Hsu Y W Lin et al ldquoThe history mechanismand clinical application of auricular therapyrdquo Evid Based Com-plement Alternat Med Article ID 495684 13 pages 2015
[52] C X Feng X H Bai and Y Du Chinese Auricular TherapyScientific and Technical Documents Publishing House BeijingChina 1994
[53] W S Wong and R Fielding ldquoPrevalence of insomnia amongChinese adults in Hong Kong a population-based studyrdquoJournal of Sleep Research vol 20 no 1 pp 117ndash126 2011
[54] L K P Suen C H Yeh J Y M Kwan et al ldquoAssociation ofauricular reflective points and status of Type 2 diabetesmellitusa matched case-control studyrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 981563 11 pages2015
[55] L Suen C Yeh S Yeung et al ldquoAssociation between auricularsignals and the risk factors of metabolic syndromerdquoMedicinesvol 4 no 3 p 45 2017
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom
Stem Cells International
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Disease Markers
Hindawiwwwhindawicom Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwwwhindawicom Volume 2013
Hindawiwwwhindawicom Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwwwhindawicom Volume 2018
PPAR Research
Hindawi Publishing Corporation httpwwwhindawicom Volume 2013Hindawiwwwhindawicom
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwwwhindawicom Volume 2018
Journal of
ObesityJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwwwhindawicom Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwwwhindawicom Volume 2018
Diabetes ResearchJournal of
Hindawiwwwhindawicom Volume 2018
Hindawiwwwhindawicom Volume 2018
Research and TreatmentAIDS
Hindawiwwwhindawicom Volume 2018
Gastroenterology Research and Practice
Hindawiwwwhindawicom Volume 2018
Parkinsonrsquos Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwwwhindawicom
Submit your manuscripts atwwwhindawicom


















