Comparison of INSTI vs EFV STARTMRK GS-US-236-0102 SINGLE.
12
Comparison of INSTI vs EFV STARTMRK GS-US-236-0102 SINGLE
-
Upload
claude-brooks -
Category
Documents
-
view
213 -
download
0
Transcript of Comparison of INSTI vs EFV STARTMRK GS-US-236-0102 SINGLE.

Comparison of INSTI vs EFV
STARTMRK GS-US-236-0102 SINGLE

Lennox JL. Lancet 2009;374:796-806STARTMRKSTARTMRK
Design
Objective– Non inferiority of RAL vs EFV: % HIV RNA < 50 c/mL by per protocol, non-
completer = failure analysis (lower margin of the 2-sided 95% CI for the difference = - 12%, 90% power)
RAL 400 mg BID + EFV placebo
TDF/FTC fdc QD
EFV 600 mg QD + RAL placebo
TDF/FTC fdc QD
> 18 yearsARV-naïve
HIV RNA > 5,000 c/mLAny CD4 cell count
No resistance toEFV, TDF or FTC
> 18 yearsARV-naïve
HIV RNA > 5,000 c/mLAny CD4 cell count
No resistance toEFV, TDF or FTC
*Randomisation was stratified by baseline HIV RNA (< or > 50,000 c/mL)and viral hepatitis co-infection status
STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC
Randomisation*1 : 1
Double-blind
Randomisation*1 : 1
Double-blind
N = 284
N = 282
W240W240W48W48

STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC
RAL EFVRandomized, N 282 284
Treated eligible patients, N 281 282
Median age, years 37 36
Female 19% 18%
White/Black/Other 41% / 12% / 47% 44% / 8% / 48%
HIV RNA (log10 c/mL), median 5.1 5.0
HIV RNA > 100,000 c/mL 55% 51%
HIV RNA > 50,000 c/mL 72% 70%
CD4 cell count (/mm3), median 212 204
CD4 < 50 per mm3 10% 11%
HBsAg+ or HCV Ab+ 6% 6%
Discontinuation by W48 24 (8.5%) 35 (12.4%)
For lack of efficacy N = 4 N = 2
For adverse event N = 8 N = 17
RAL was administered with or without food, EFV on an empty stomach at bedtime,TDF/FTC in the morning with food
STARTMRKSTARTMRK Lennox JL. Lancet 2009;374:796-806
Baseline characteristics and patient disposition

Baseline RAL EFV
RNA < 5 log10 c/mL
RNA > 5 log10 c/mL
92.5%
90.9%
89.1%
89.2%
CD4 > 200/mm3
CD4 < 200/mm3
94.4%
88.3%
92.4%
85.6%
HIV-1 B subtype
Non-B subtype
90.3%
96.3%
88.5%
90.9%
Response to treatment at week 48
* Exclusion of discontinuations due to intolerability or reasons unrelated to treatment
STARTMRKSTARTMRK
STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC
Lennox JL. Lancet 2009;374:796-806
HIV RNA < 50 c/mL at W48(observed-failure analysis)
by baseline factors
Mean CD4/mm3 increase at W48 (observed-failure analysis): 189 (RAL) vs 163 (EFV)(P = 0.0184)
HIV RNA < 50 c/mL
86.181.9
95% CI for the difference
= - 1.9; 10.3
91.6 89.1
Per protocol,observed-failure *
95% CI for the difference
= - 2.6; 7.7
281 282 263 258
25
50
100
75
% Primaryanalysis
RAL EFV
PP, NC = F
N =

RAL EFV PClinical adverse events
Drug-related AE 44.1% 77.0% < 0.0001
Serious drug-related AE 1.4% 1.8% NS
Treatment discontinuation due to AE 3.2% 6.0% NS
Laboratory adverse events
Drug-related AE 5.0% 8.5% NS
Treatment discontinuation due to AE 0 0.4% NS
Clinical drug-related AE of moderate to severe intensity 16% 32% < 0.0001
Headache 4% 5%
Dizziness 1% 6%
Insomnia 4% 3%
Fatigue 1% 3%
Diarrhoea 1% 3%
No difference in incidence in other AE occurring in > 2% of patients
Grade 3 or 4 laboratory abnormality
Fasting LDL-cholesterol > 4.92 mmol/L (190 mg/dl) 1% 4%
Incidence of other abnormalities < 2% and not different between arms
STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC Safety at W48
STARTMRKSTARTMRK Lennox JL. Lancet 2009;374:796-806

STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC Safety: neuropsychiatric symptoms
– At Week 8• CNS-related adverse events had occurred in 10% of RAL patients vs 18%
of EFV patients (P = 0.0149)
• Retrospective sensitivity analysis (additional symptoms): > 1 CNS-related adverse event: 20% vs 52% (P < 0.0001)
• Most symptoms were self-limited
– At Week 48• Cumulative incidence of CNS-related adverse event was significantly
lower in patients on RAL: 14% vs 23% in the main analysis (P = 0.0044); 26% vs 59% in the sensitivity analysis (P < 0.0001)
• These events were generally mild: 62% of RAL vs 79% of EFV
• Only 1 patient, on EFV, discontinued the trial because of CNS-related adverse event
STARTMRKSTARTMRK Lennox JL. Lancet 2009;374:796-806

RALN = 281
EFVN = 282
HIV RNA level < 50 c/mL 71.0% 61.3%
Mean CD4/mm3 change from baseline 374 312
Virologic failure (confirmed HIV RNA > 50 c/mL) 19.6% 20.9%
Non response 3.6% 8.5%
Rebound 16.0% 12.4%
Death 5 (1.8%) 5 (1.8%)
Discontinuation 71 (25.2% 98 (34.5%)
Due to lack of efficacy 6 10
Due to clinical AE 14 25
Due to laboratory AE 0 3
Due to other reasons 51 60
Drug-related clinical adverse events 52.0% 80.1%
Cumulative treatment outcome for the entire 5 years study
STARTMRKSTARTMRK
STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC
Rockstroh JK, JAIDS 2013;63:77-85

STARTMRKSTARTMRK
STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC
Rockstroh JK, JAIDS 2013;63:77-85
Cumulative Discontinuation Rate due to AE (%)
0
2
4
Log rank P-value = 0,023
6
8
10
12
14
16
18
20
0 16 32 48 60 72 84 96 120 140 168 192 216 240
Weeks
281 272 265 262 255 246 236 231 227 223 217 190
282 272 257 254 245 235 221 213 203 200 196 183
Number at risk
RAL EFV
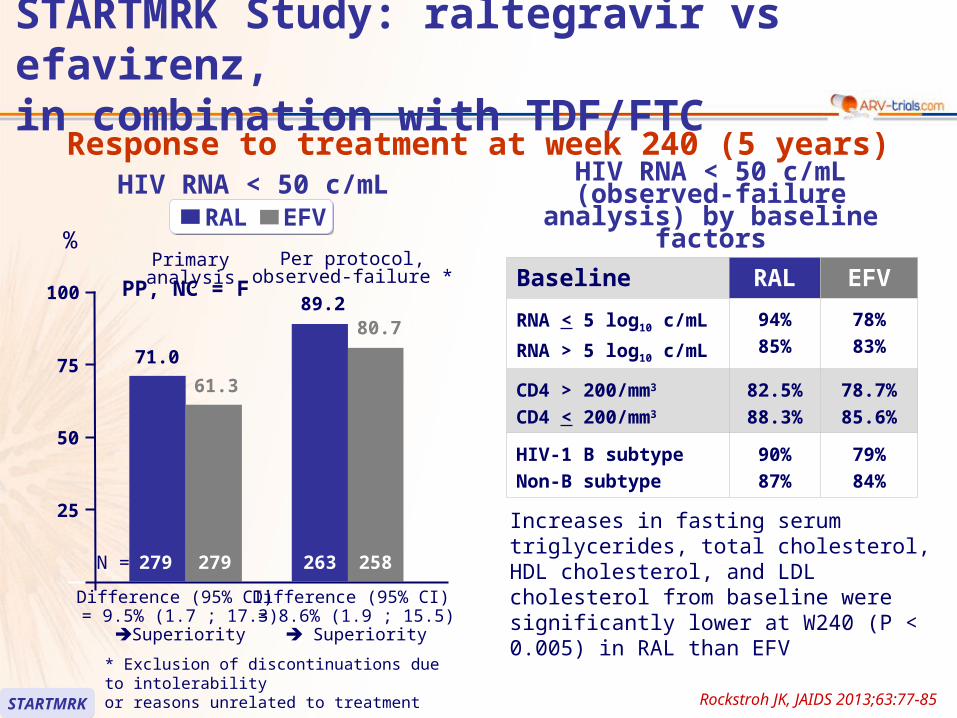
Baseline RAL EFV
RNA < 5 log10 c/mL
RNA > 5 log10 c/mL
94%
85%
78%
83%
CD4 > 200/mm3
CD4 < 200/mm3
82.5%
88.3%
78.7%
85.6%
HIV-1 B subtype
Non-B subtype
90%
87%
79%
84%
Response to treatment at week 240 (5 years)
* Exclusion of discontinuations due to intolerability or reasons unrelated to treatment
STARTMRKSTARTMRK
STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC
HIV RNA < 50 c/mL (observed-failure analysis) by baseline factors
HIV RNA < 50 c/mL
71.0
61.3
Difference (95% CI) = 9.5% (1.7 ; 17.3)
Superiority
89.280.7
Per protocol,observed-failure *
279 279 263 258
25
50
100
75
%Primary analysis
RAL EFV
PP, NC = F
N =
Difference (95% CI) = 8.6% (1.9 ; 15.5)
Superiority
Increases in fasting serum triglycerides, total cholesterol, HDL cholesterol, and LDL cholesterol from baseline were significantly lower at W240 (P < 0.005) in RAL than EFV
Rockstroh JK, JAIDS 2013;63:77-85

RALN = 281
EFVN = 282
Protocol-defined virologic failure confirmed (HIV RNA > 50 c/mL) 55 (19.6%) 59 (20.9%)
Resistance data available (HIV RNA > 400 c/mL) 23* 20
RAL or EFV resistance alone 1 7
RAL or EFV resistance, and NRTI resistance 3 3
NRTI resistance alone 3 2
Cumulative summary of genotypicresistance data for patients with RNA > 400 c/mL at the time of virologic failure out to week 240
* Integrase gene could not be amplified in 5 cases
STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC
Rockstroh JK, JAIDS 2013;63:77-85STARTMRKSTARTMRK
Emergence of RAL resistance in 4 patients (1.4%)Sequencing data of the 4 patients with emergence of RAL-associated mutations
– Q148H + G140S,
– Q148R + G140S,
– Y143Y/H + L74L/M + E92Q +T97A,
– Y143R

RAL EFVGastrointestinal disorders
Diarrhea 5.3% 9.9%
Flatulence 3.6% 5.0%
Nausea 8.9% 11.0%
General disorders
Fatigue 4.3% 8.9%
Nervous system disorders
Dizziness 7.8% 35.1%
Headache 9.3% 14.2%
Somnolence 1.1% 7.4%
Psychiatric disorders
Abnormal dreams 6.8% 13.1%
Insomnia 7.5% 8.2%
Nightmare 2.8% 5.3%
Skin and subcutaneous tissue disorders
Rash 1.1% 8.2%
Drug-related adverse events in > 5% in either group over 5 years
STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC
Rockstroh JK, JAIDS 2013;63:77-85STARTMRKSTARTMRK

STARTMRK Study: raltegravir vs efavirenz,in combination with TDF/FTC Summary – Conclusion
– At 48 weeks of treatment, RAL was non-inferior to EFV, in combination with TDF/FTC. Virologic non-inferiority of RAL was confirmed through W24. RAL was superior to EFV for virologic outcome at week 240
– RAL + TDF/FTC led to more rapid viral load decline (significantly more patients with HIV RNA < 50 c/mL for weeks 2 to 16)
– Greater increase in CD4 was observed in the RAL group. It was significant from W156
– Upon virologic failure, resistance mutations to RAL was found in few cases
– RAL was associated with significantly fewer overall and drug-related clinical adverse events, and CNS-related adverse events than was EFV
– Mean changes in lipid parameters were smaller for RAL than for EFV– RAL + TDF/FTC is an alternative to EFV + TDF/FTC as a first-line
combination regimen in treatment-naïve HIV-infected patients
STARTMRKSTARTMRK Lennox JL. Lancet 2009;374:796-806; Rockstroh JK, JAIDS 2013;63:77-85