Comparison of a Chromogenic Factor X Assay to International Normalized Ratio for Monitoring Oral...
23
Comparison of a Chromogenic Factor X Assay to International Normalized Ratio for Monitoring Oral Anticoagulation Therapy David L. McGlasson; Major Benjamin G. Romick † , † , Bernard J. Rubal ‡ † Wilford Hall US Air Force Medical Center, Lackland Air Force Base, TX ‡ Brooke Army Medical Center, Fort Sam Houston, TX
-
Upload
georgia-peters -
Category
Documents
-
view
221 -
download
1
Transcript of Comparison of a Chromogenic Factor X Assay to International Normalized Ratio for Monitoring Oral...

Comparison of a Chromogenic Factor X Assay to International Normalized
Ratio for Monitoring Oral Anticoagulation Therapy
David L. McGlasson; Major Benjamin G. Romick†, †, Bernard J. Rubal‡
†Wilford Hall US Air Force Medical Center, Lackland Air Force Base, TX
‡ Brooke Army Medical Center, Fort Sam Houston, TX

Background
• The International Normalized Ratio (INR) is the primary method for monitoring patients on oral anticoagulation therapy (OAT).
• Numerous confounding variables limit monitoring of INR in patients on OAT– Lupus Anticoagulant (LA)– Converting direct thrombin inhibitors to OAT

Background
• Chromogenic Assay for Factor X (CFX) has been validated for use in monitoring patients with LA who are on OAT
• CFX is not affected by presence of LA and other variables that affect INR

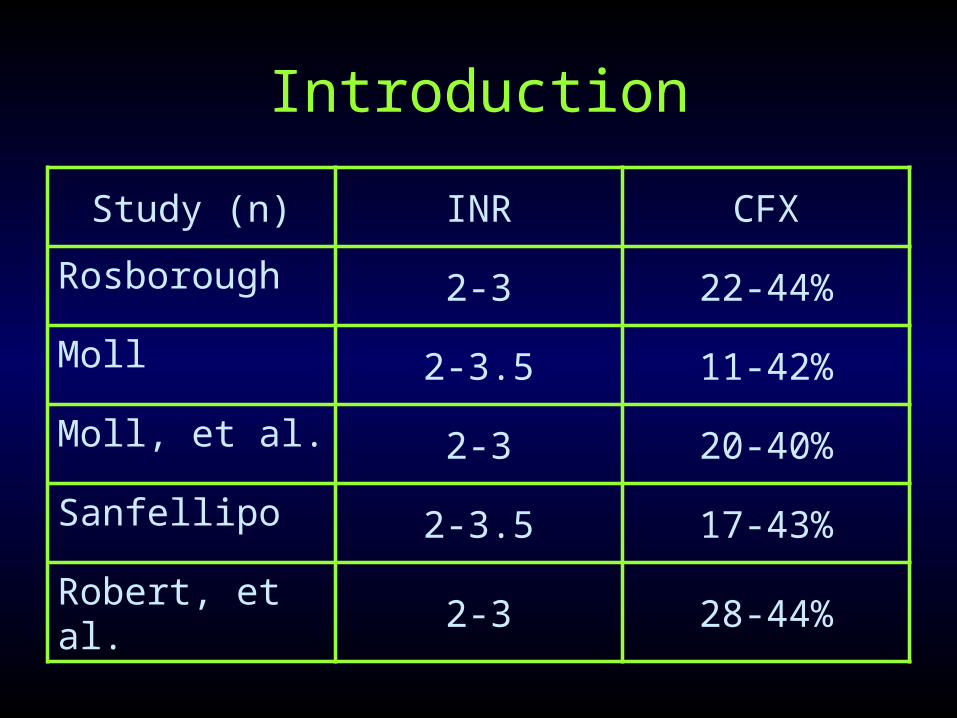
Introduction
• CFX has not been compared to INR in monitoring a broad population of patients on OAT
• No universally defined range of values of CFX for:– Therapeutic anticoagulation– Supratherapeutic anticoagulation– Subtherapeutic anticoagulation
Introduction
Study (n) INR CFX
Rosborough 2-3 22-44%
Moll 2-3.5 11-42%
Moll, et al. 2-3 20-40%
Sanfellipo 2-3.5 17-43%
Robert, et al. 2-3 28-44%

Introduction
• Objectives of the present study:
1. Define the therapeutic range for CFX in this population
2. Assess the relationship between CFX and INR values in an outpatient “Coumadin Clinic” setting

Methods
• INR and CFX levels were evaluated in randomly selected excess specimens from the coumadin clinic and normal subjects not receiving anticoagulant therapy
• INR values were correlated to CFX for determining the following ranges for OAT patients:– Normal or Subtherapeutic INR < 2.0– Therapeutic INR 2.0-3.0– Supratherapeutic INR > 3.0

Methods
• Instrumentation:– STA-R Evolution automated coagulation
analyzer (Diagnostica-Stago, Inc.®, Parsippany, NJ)
– Chromogenic Factor X assay (Diapharma, Inc.®, Westchester, OH)
– INR performed with PT method using Neoplastine Cl+ with ISI of 1.28 and geometric mean of 13.8 seconds
Data Analysis
• Overall correlation of INR to CFX assessed with inverse square method (Sigmaplot version 9.01; Systat Software, Inc, San Jose, Ca)– Goodness of fit expressed as the coefficient of
determination: R2
• Receiver Operator Characteristic (ROC) curves used to discriminate therapeutic ranges (SPSS version 11.5, SPSS, Inc. Chicago, IL) – ROC area > 0.900 → highly discriminative– ROC area > 0.800 → good discrimination

Data Analysis
• CFX ranges consistent with INR therapeutic ranges defined by plots of sensitivity and specificity versus CFX
• Kolmogorov-Smirnov test employed to assess normality of CFX distributions among therapeutic subsets
• Non-normally distributed data presented as median and 25th and 75th percentiles

Data Analysis
• One-way Analysis of Variance on Ranks (Sigmastat version 3.11; Systat Software, Inc., San Jose, CA) used to assess differences in CFX among INR therapeutic ranges
• Differences between groups assess used Dunn’s post hoc test
• P values < 0.05 are considered significant
Results
• 309 randomly selected OAT patients were tested
• 30 normal subjects not on anticoagulants tested for comparison
• Range of INR & CFX in OAT patients:– INR 0.92 – 12.76– CFX 9 – 132%

Results
INRCFX Range
(Mean)N
< 2.032 - 132%
(53%)70
2.0 – 3.018 – 48%
(28%)135
> 3.09 – 46%
(21%)104
Normals72 – 131%
96%30

Figure 1. Good model fit between INR and CFX when expressed as a second order inverse function (N = 339, r2 = 0.929; P<0.001). Open circles represent samples from normal control group (CFXn), closed circles represent patients receiving Coumadin therapy (CFXc).

Figure 2A. ROC curve using INR ≥ 2.0 as criteria for the threshold of therapeutic anticoagulation. Figure 2B (arrow) is a plot of sensitivity and specificity over the range of CFX values tested (N = 339). The arrow indicates the CFX value ≤ 35.5% that has maximum combined sensitivity and specificity for the INR therapeutic threshold (INR ≥ 2.0).

Figure 3A is a ROC curve for the patients with INR ≥ 2.0 (N = 240) using an INR value >3.0 for discriminating therapeutic form surpratherapeutic ranges of CFX. Figure 3B is a plot of sensitivityand specificity vs CFX values. Arrow indicates that CFX ≤ 23.5% is consistent with an INR >3.0.

Figure 4 depicts box plots (median: solid line, mean: dotted line, whiskers: 10th and 90th percentile) for CFX values categorized by INR therapeutic ranges. Significant differences were noted between all groups. Dashed lines indicate the CFX range (23.5%-35.5%) is equivalent to the INR therapeutic range (INR 2.0-3.0).

Conclusion
• CFX correlates well with INR in a randomly selected group of OAT patients at varying levels of anticoagulation– R = 0.964 by inverse square function
• CFX is highly discriminative for patients in therapeutic and subtherapeutic INR ranges– ROC curve area 0.948, p < 0.0001, n = 339
• CFX has good discrimination for patients in therapeutic and supratherapeutic INR range– ROC curve area 0.864, p < 0.0001, n = 240
Conclusion
• CFX < 35.5% appears to be equivalent to INR > 2.0– Sensitivity 91.7%– Specificity 91.9%
• CFX < 23.5% suggests supratherapeutic anticoagulation equivalent to INR > 3.0– Sensitivity 78.2%– Specificity 84.6%

Conclusion
• Current findings suggest usefulness of CFX for monitoring oral anticoagulation in broad groups of patients seen in a coumadin clinic

Conclusion
• Further study warranted to compare outcomes in OAT patients monitored with CFX and conventional INR methods– Bleeding events– Thromboembolism– Cost– Convenience– Availability

References• 1. Delate T, Witt DM, Jones JR, Bhardwaja B, Senser M. Falsely elevated international
normalized• ratio values in patients undergoing anticoagulation therapy: a descriptive evaluation. Chest• 2007;131(3):816-822.• 2. Newman DH, Zhitomirsky I. The prevalence of nontherapeutic and dangerous international• normalized ratios among patients receiving warfarin in the emergency department. Ann Emerg• Med 2006;48(2):182-189.• 3. van den Besselaar AMHP, Hoekstra MMCL, Witteveen E, Didden JH, van der Meer FJM.• Influence of blood collection systems on the prothrombin time and international sensitivity index• determined with human and rabbit thromboplastin reagents. Am J Clin Pathol 2007;127(5):724-• 729.• 4. McGlasson DL. A comparison of INRs after local calibration of thromboplastin international• sensitivity indexes. Clin Lab Sci 2002;15(2):91-95.• 5. McGlasson DL. Laboratory variables that may affect test results in prothrombin times• (PT)/international sensitivity indexes. Clin Lab Sci 2003;34:124-128.• 6. McGlasson DL, Shaklee PN. A multi-instrument evaluation of a commercial chromogenic factor• X assay to monitor oral anticoagulation therapy. Blood 2004;104(11):4059.• 7. Shaklee PN, McGlasson DL. A multi-instrument evaluation of a chromogenic factor X assay for• monitoring oral anticoagulation therapy. Clin Chem 2005;51(Suppl 1):20112.• 8. Ortel TL, Moll S. Monitoring oral anticoagulant therapy in patients with lupus• anticoagulants.[comment]. Br J Haematol 1998;101(2):390-392.

References• 9. Robert A, Le Querrec A, Delahousse B, Caron C, Houbouyan L, Boutiere B, et al. Control of oral• anticoagulation in patients with the antiphospholipid syndrome--influence of the lupus• anticoagulant on International Normalized Ratio. Groupe Methodologie en Hemostase du Groupe• d'Etudes sur l'Hemostases et la Thrombose. Thromb Haemostasis 1998;80(1):99-103.• 10. Rosborough TK, Shepherd MF. Unreliability of international normalized ratio for monitoring• warfarin therapy in patients with lupus anticoagulant. Pharmacotherapy 2004; 24(7):838-842. • 11. Thom J, Ivey L, Gilmore G, Eikelboom JW. Evaluation of the phospholipid-rich dilute Russell's• viper venom assay to monitor oral anticoagulation in patients with lupus anticoagulant. Blood• Coagul Fibrinolysis 2004;15(4):353-357.• 12. Arpino PA, Demirjian Z, Van Cott EM. Use of the chromogenic factor X assay to predict the• international normalized ratio in patients transitioning from argatroban to warfarin.• Pharmacotherapy 2005;25(2):157-164.• 13. Perry SL, Samsa GP, Ortel TL. Point-of-care testing of the international normalized ratio in• patients with antiphospholipid antibodies. Thromb Haemostasis 2005: 94(6):1196-1202.• 14. Khamashta MA, Cuadrado MJ, Mujic F, Taub NA, Hunt BJ, Hughes GR. The management of• thrombosis in the antiphospholipid-antibody syndrome.[see comment]. N Engl J Med• 1995;332(15):993-997.• 15. Levine JS, Branch DW, Rauch J. The antiphospholipid syndrome.[see comment]. N Engl J• Med 2002;346(10):752-763.• 16. Sanfelippo MJ, Sennet J, McMahon EJ. Falsely elevated INRs in warfarin-treated patients with• the lupus anticoagulant. WMJ 2000 Jun;99(3):62-64.• 17. Trask AS, Gosselin RC, Diaz JA, Dager WE. Warfarin initiation and monitoring with clotting• factors II, VII, and X. Ann of Pharmacotherapy 2004 Feb;38:251-256.


















