
Quantifying The Effects Of Nicotine And Nitroglycerin On ...

Comparison of Intravenous Nitroglycerin and SodiumNitroprusside for Treatment of Acute HypertensionDeveloping after Coronary Artery Bypass SurgeryJOHN T. FLAHERTY, M.D., PATRICK A. MAGEE, M.B., TIMOTHY L. GARDNER, M.D.,
ALAN POTTER, B.A., AND NIAL P. MACALLISTER, M.D.
SUMMARY The present study was designed to test the hypothesis that i.v. nitroglycerin is as effective as
sodium nitroprusside for managing acute hypertension early after coronary artery bypass surgery. Seventeenpatients received both nitroglycerin and nitroprusside in a randomized crossover protocol. Infusion rates were
increased stepwise to lower mean arterial pressures comparably with each drug. In 14 of 17 patients, similarinfusion rates of the two vasodilators resulted in equal lowering of both blood pressure and systemic vascularresistance. In the remaining three patients, very high infusion rates of nitroglycerin were required and achievedonly 20-50% of nitroprusside's response in two of three. Hemodynamic responses to the two vasodilators were
similar, except that nitroglycerin increased cardiac output more than nitroprusside did. In contrast, pul-monary gas exchange responses differed in that nitroglycerin improved intrapulmonary shunting, whilenitroprusside worsened it. Similarly, nitroglycerin resulted in a significantly smaller increase in the alveolar-arterial oxygen gradient than did nitroprusside. These results suggest that in the majority of patients, i.v. nitro-glycerin was as effective as nitroprusside in controlling acute hypertension after coronary artery bypass sur-
gery. In addition, nitroglycerin appeared to have more favorable effects on pulmonary gas exchange. Becausenitroglycerin has more beneficial effects on intercoronary collateral blood flow in the setting of regionalischemia, it may be preferable to nitroprusside in patients with ischemic heart disease.
ARTERIAL HYPERTENSION requiring i.v. vaso-dilator therapy occurred early after coronary arterybypass surgery in approximately two out of three pa-tients in an earlier study from this institution.' Al-though nitroglycerin is often viewed predominantly as avenodilator, our clinical studies of i.v. nitroglycerin inpatients with acute myocardial infarction clearly indi-cate that, at higher infusion rates, nitroglycerin is alsoa potent arterial dilator. Nitroglycerin reduced bothleft ventricular filling pressure and mean arterial pres-sure, while stroke volume remained constant or in-creased.2' s Lowering of peripheral vascular resistancewas greatest in patients who had hemodynamic evi-dence of severe left ventricular failure.
In the present study, we used a randomized cross-over protocol to determine whether i.v. nitroglycerincould be as effective as sodium nitroprusside in reduc-ing arterial pressure in patients who were acutelyhypertensive after coronary bypass. Previous studieshave shown that nitroglycerin and nitroprusside canhave opposite effects on the severity of regional ische-mia.' 6 In these studies, nitroglycerin improved re-gional ischemia by increasing intercoronary collat-eral flow, while nitroprusside appeared to worsenischemia by decreasing coronary perfusion pressurewithout improving collateral flow. Thus, if i.v. nitro-glycerin is equally effective for treating acute hyper-
From the Departments of Medicine, Surgery and Anesthesiology,The Johns Hopkins Medical Institutions, Baltimore, Maryland.
Supported by NIH grant P 50 HL-17655 (SCOR for IschemicHeart Disease).
Dr. Flaherty is the recipient of NHLBI Research CareerDevelopment Award 1 KO 4-0019.
Address for correspondence: John T. Flaherty, M.D., CardiologyDivision, The Johns Hopkins Medical Institutions, 600 NorthWolfe Street, Baltimore, Maryland 21205.
Received April 7, 1981; revision accepted August 31, 1981.Circulation 65, No. 6, 1982.
tension in patients with coronary artery disease, itmight be preferable to sodium nitroprusside.
MethodsThe study population consisted of 17 patients un-
dergoing coronary artery bypass surgery at The JohnsHopkins Hospital. Patients with a history of hyperten-sion requiring drug therapy were excluded, but thestudy group was otherwise unselected. Written, in-formed consent was obtained from all patients beforesurgery. Premedication included morphine anddiazepam. Pancuromium bromide was used during in-tubation and the patients were mechanically ventilatedthroughout the study period. Anesthesia during thecardiac surgery was induced with i.v. diazepam,morphine, or thiamylol sodium. Anesthesia was sub-sequently maintained with i.v. morphine in 11 pa-tients and fentanyl in six patients. Standard cardio-pulmonary bypass with nonpulsatile flow rates of2-2.5 1/min/M2 was used. Systemic hypothermia(27-29° C), topical myocardial hypothermia andhyperkalemic cardioplegia were used. The aortic rootwas cross-clamped for periods of 10-60 minutes. Allpatients received heparin, 4 mg/kg; anticoagulationwas reversed by protamine.
Before induction of anesthesia, a Swan-Ganz ther-modilution catheter was placed in all patients to allowcontinuous monitoring of right atrial and pulmonaryartery pressures. Cardiac output was serially mea-sured by the thermodilution technique using 10-ml in-jections of 5% dextrose in water. Arterial pressure wasmonitored by a radial artery catheter and a StathamP23Db transducer. After surgery, all patients weretransferred to the surgical intensive care unit andmechanical ventilation was continued. Significantpostoperative hypertension was defined as the oc-currence of a sudden and persistent (> 15 minutes) in-
1072
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

I.V. NITROGLYCERIN IN POSTOP HYPERTENSION/Flaherty et al.
crease in mean arterial pressure of at least 20 mm Hg(to mean arterial pressures of 95-150 mm Hg) duringthe first 3 hours after weaning from cardiopulmonarybypass. All patients were normotensive (mean arte-rial pressure 75-94 mm Hg) before the hypertensiveepisode. None were receiving vasopressor or vaso-dilator drugs before the study.Hemodynamic variables at the time hypertension
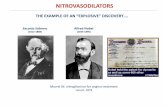
developed were recorded in all 17 patients before theinitiation of vasodilator therapy. These variables in-cluded heart rate, cardiac output, mean arterial pres-sure, pulmonary capillary wedge pressure (or pulmo-nary artery diastolic pressure) and mean pulmonaryartery pressure, as well as cardiac index, stroke workindex, systemic vascular resistance index, pulmonaryvascular resistance index and stroke volume index.After control measurements were obtained, patientswere randomly assigned to one of two experimentalprotocols, depending on the last digit of their medicalhistory number (fig. 1). Seven patients with evennumbers received an infusion of sodium nitroprussidefirst and then crossed over to i.v. nitroglycerin. Tenpatients with an odd number received i.v. nitroglycerinfirst and then crossed over to nitroprusside. The nitro-glycerin solution, supplied by the Johns Hopkins Hos-pital Pharmacy, contained nitroglycerin, 250 ,g/ml, in50-ml glass ampules. Nitroprusside was prepared in a500-,ug/ml concentration and infusion lines from thesyringe containing nitroprusside to the patient werecovered with aluminum foil. The nitroglycerin solu-tion was refrigerated in the dark during long-termstorage, but did not require protection from light dur-ing short-term infusion.
Infusion of each drug was begun at 5-10 Ag/minand increased stepwise every 3-5 minutes until meanarterial pressure was lowered 10-33% (10-40 mm Hg),depending on the starting value. Then, the hemo-dynamic effects were allowed to stabilize from ap-proximately 20 minutes and cardiac output wasremeasured to define a hemodynamic profile for thefirst vasodilator drug. The first vasodilator was thendiscontinued and infusion of the second drug begun.As the vasodilating effects of the initial agent began todecrease, the infusion rate of the second agent was in-creased in a stepwise fashion in an attempt to main-
tain mean arterial pressure at the same level reachedwith the first drug. When a stable infusion rate of thesecond vasodilator had been obtained, the hemo-dynamic effects were again allowed to stabilize for 20minutes and cardiac output was remeasured to obtaina hemodynamic profile for the second vasodilatordrug. Because all patients had significant drainagefrom their mediastinal tubes during the study, volumein the form of whole blood was administered simul-taneously to replace surgical blood loss.
In eight of the 17 patients, pulmonary and tissue gasexchange were assessed by temporarily switching to aninspired oxygen concentration (Fio2) of 100% for 10minutes during the control and each subsequent inter-vention period. Arterial oxygen tension (Pao2), mixedvenous oxygen tension (Pvo2), alveolar-arterial oxy-gen gradient (AaDo2), intrapulmonary shunting(Qs/Qt) and tissue oxygen use (MVo2) could therebybe measured or calculated during each of theseperiods.7
All results are expressed as mean ± SD. Statisticalanalysis was by two-way analysis of variance-re-peated measures test, and individual comparisonswere made only when analysis of variance revealedsignificant (p < 0.05) differences.
ResultsThe mean infusion rate of sodium nitroprusside re-
quired in all 17 patients to obtain the desired loweringof mean arterial pressure was 95 ± 116 ,ug/min. Themean infusion rate of nitroglycerin required to obtaina comparable lowering of arterial pressure was 304 i440 ug/min. Fourteen patients responded to nitro-glycerin infusions of less than 300 ,ug/min (range8-292 jsg/ min). Of the remaining three patients, onerequired 1125 ,tg/min to obtain a comparable bloodpressure lowering, the second received 1245 ,ug/minand yet obtained only 50% of the mean arterial pres-sure reduction obtained with nitroprusside (167 tg/min), and the third received 1245 ,g/min andobtained only 20% of the reduction in blood pressureobtained with nitroprusside (250 'g/min). In the 14patients who obtained comparable blood pressurelowering with infusion rates less than 300 Ag/min, themean infusion rate of nitroglycerin was I ± 116
HYPERTENSIONCONTINUOUS MONITORING
OF AP AND PAP
IV NITROGLYCERIN
V NITROPRUSSIDE
130min t--30mmn-+- 30mmn-jFIGURE 1. The experimental protocol. Allpatients received both i. v. nitroglycerin andi. v. nitroprusside in a randomized crossoverfashion. Arterial pressure (AP) and pulmo-nary artery pressure (PAP) were con-tinuously monitored and cardiac output wasmeasured by the thermodilution techniqueusing Swan-Ganz balloon flotation cathe-ters.
THERMODI LUTI ONCARDIAC OUTPUT
1
1073
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 65, No 6, JUNE 1982
Ag/min. This mean infusion rate of nitroglycerin wasnot significantly different from the average infusionrate of nitroprusside in these same patients.
After initiation of vasodilator therapy, arterial pres-sure decreased rapidly from a mean of 115 ± 18 mmHg to 90 ± 9 mm Hg with nitroprusside and 90 ± 10mm Hg with nitroglycerin (both p < 0.001 vs control)(fig. 2A). Systemic vascular resistance index decreasedfrom an initially elevated level of 44 ± 9 units to nor-mal levels of 31 ± 10 units with nitroglycerin and 31 ±7 units with nitroprusside (both p < 0.001 vs control).Cardiac output increased from a control level of 2.4 ±0.5 1/min/M2 to 2.7 ± 0.7 1/min/M2 with nitroprus-side and to 2.9 ± 0.9 1/min/M2 with i.v. nitroglycerin.Only the increase in cardiac output obtained with i.v.nitroglycerin was statistically significant (p < 0.025 vscontrol). The heart rate increased from 85 ± 14 beats/min during control to 93 ± 18 beats/min during nitro-prusside and 93 ± 20 beats/min during nitroglycerin(both p < 0.025 vs control).
Because volume expanders were administeredsimultaneously with the vasodilator therapy, thepreload-lowering effect of both agents was largely
L ControlTNP
:1 TNG
counteracted (fig. 2B). Left ventricular filling pressure(pulmonary capillary wedge pressure or pulmonaryartery diastolic pressure), which was 11 ± 4 mm Hgbefore vasodilator therapy, was 10 ± 4 mm Hg duringnitroprusside and 9 ± 3 mm Hg during i.v. nitroglyc-erin (NS). The control stroke work index was 38 ± 10g-m/m2 and did not change significantly with eitherdrug (32 ± 7 g-m/m2 during nitroprusside and 35 ±12 g-m/m2 during nitroglycerin). Stroke volume in-creased slightly with both vasodilators, from a controlvalue of 54 ± 11 ml to 59 i 19 ml during nitroglycerinand 56 ± 12 ml during nitroprusside (NS).The mean pulmonary artery pressure decreased
from a control value of 17 ± 5 mm Hg to 15 i 5 mmHg with nitroglycerin and 16 ± 6 mm Hg withnitroprusside (NS) (fig. 2B). Control pulmonaryvascular resistances were normal (< 4 units); conse-quently, small decreases in pulmonary vascular resis-tance index, from 2.8 ± 1.9 units to 2.2 ± 1.4 unitsduring nitroglycerin and 2.4 ± 1.3 units duringnitroprusside, were not expected to reach significance.
Nitroglycerin and nitroprusside had differentialeffects on pulmonary gas exchange (fig. 3). Mean Pao2
***= p <.OO vs Control* = p <.05 vs Control+ = p < 05 NP vs TNG
Mean Arterial Systemic Vascular Cardiac IndexPressure(mm Hg) Resistance Index (units) (L/min/m2)
Heart Ratem(min. )
LV Filling Stroke WorkPressure (mm Hg) Index (Gm-M/M2)
30[
2.6 F
22 F
1.8F
1.4h
I.0
I
O ControaE NP
EJ TNG
Stroke Mean Pulmonary Pulmonary VascularVolume (ml) Artery Pressure Resistance Index
(mm Hg) (units)
FIGURE 2. Hemodynamic variables (mean± SD) measured during the control state andafter a stable response to each drug had beenobtained. Statistical significance of paireddata is indicated only when the overallanalysis of variance showed p < 0.05. NP =nitroprusside; TNG = nitroglycerin; L V =left ventricular.
1074 CIRCULATION
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

I.V. NITROGLYCERIN IN POSTOP HYPERTENSION/Flaherty et al.
n Control
E NP
[ TNG
Pv02 Mv02(mm Hg) (ml /min)
* = P<.05 vs Control+= p<.OI NPvsTNG++- p <.001 NP vs TNG
AoDO2 °s/Qt(mm Hg) FIGURE 3. Pulmonary and tissue gas ex-
change variables measured at an inspiredoxygen concentration of 100% during thecontrol period and during the last 10minutes ofeach intervention period in a sub-group of eight patients. NP = nitroprus-side; TNG = nitroglycerin; Pao2 = arterialoxygen tension; Pvo2 = mixed venous
oxygen tension; Mvo,2 = tissue oxygen use;
AaDo2 = alveolar-arterial oxygen gradient;Qs/Qt = intrapulmonary shunting.
decreased from 397 ± 49 mm Hg during the controlperiod to 363 ± 33 mm Hg during nitroprusside and384 ± 27 mm Hg during nitroglycerin (NS). Pvo2 in-creased during nitroprusside and decreased duringnitroglycerin. From a control level of 44 ± 10 mm Hg,Pvo2 decreased to 41 ± 6 mm Hg during nitro-glycerin and increased to 46 ± 6 mm Hg during nitro-prusside (NS). MVo2 calculated by the Fick equationalso increased with nitroglycerin and decreased withnitroprusside. Control MVo2 was 101 ± 66 ml/min/m2, compared with 111i± 38 ml/min/m2 during nitro-glycerin and 84 ± 24 ml/min/M2 during nitroprusside(NS).AaDo2 increased significantly with both vasodila-
tors. However, the magnitude of the rise was greaterwith nitroprusside than with nitroglycerin (p < 0.025).AaDo2 increased from a control level of 266 ± 26 mmHg to 292 ± 27 mm Hg with nitroglycerin and to 331± 52 mm Hg with nitroprusside (both p < 0.025 vs
control). Qs/Qt as calculated by the method of Berg-gren7 also showed directionally opposite responses toi.v. nitroglycerin and nitroprusside. The shunt de-creased from 22 ± 9% to 18 ± 2% with nitroglycerinand increased to 25 ± 5% with nitroprusside (p <0.01).The mean body temperature in all 17 patients dur-
ing the control period was 35.7 ± 0.9°C. The meanbody temperature was significantly higher during bothnitroglycerin (36.2 ± 0.8°C) and nitroprusside infu-sion (36.0 ± 0.8°C) because the patients weregradually rewarming. However, because of the ran-domized crossover study design, mean temperatureswere not different during nitroprusside and nitroglyc-erin periods.The study patients had various hemodynamic pro-
files. Six patients had elevated filling pressures (13-18mm Hg) and 11 patients had normal filling pressures(5-11 mm Hg). Three of the six patients with elevatedleft ventricular filling pressures had a depressed car-diac index (1.8-2.0 I/min/M2) and three had a normalcardiac index (2 2.5 1/min/M2). Ten of the 11 patientswith normal filling pressures had a normal cardiac in-
dex.In the six patients with elevated left ventricular fill-
ing pressures, pulmonary capillary wedge pressure
decreased from 15 ± 2 mm Hg to 9 2 mm Hg (p <0.001) with nitroglycerin and to 13 i 4 mm Hg withnitroprusside (p < 0.05). Patients with normal fillingpressures showed no decrease in filling pressure witheither vasodilator. Similarly, nitroglycerin reducedmean pulmonary artery pressure more than did nitro-prusside in patients with initially elevated filling pres-sures. From a control of 22 ± 4 mm Hg, the meanpulmonary artery pressure decreased to 20 ± 6 mmHg with nitroprusside (NS) and to 14 ± 5 mm Hg (p< 0.02 vs control) with nitroglycerin. There were noother significant differences in the hemodynamiceffects of the two vasodilators ih patients in eitherhemodynamic subgroup.No complications occurred during the study. Mean
arterial pressure remained greater than 80 mm Hg andreduction of the infusion rate after the desired bloodpressure lowering had been obtained was not required.Mild sinus tachycardia (< 120 beats/min) occurredduring nitroprusside infusion in four patients and dur-ing nitroglycerin infusion in four patients, withouthemodynamic or electrocardiographic (standard 12-lead ECG) evidence of regional ischemia. Neithersinus bradycardia nor vomiting was encountered. Be-cause the patients remained intubated and at least par-tially anesthetized throughout the study, subjectivesymptoms of headache or nausea could not be elicited.
DiscussionThe present study demonstrates that i.v. nitroglyc-
erin can, in the majority of cases, be as effective assodium nitroprusside for the treatment of hyperten-sion after coronary bypass surgery. Both vasodilatorscorrected the elevated systemic vascular resistanceand the elevated mean arterial pressure.
Previous investigators have suggested that nitro-glycerin was predominantly a venodilator, obtainingits beneficial effects in angina pectoris by increasedvenous pooling.8 In an initial study of i.v. nitro-glycerin in patients with acute myocardial infarction,lower infusion rates (mean 37 ug/min) of nitro-glycerin reduced left ventricular filling pressure whileminimally lowering mean arterial pressure (meandecrease 7 mm Hg).2 This lowering of left ventricularfilling pressure was most likely the result of a change
P02
(mm Hg)
1075
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 65, No 6, JUNE 1982
in the diastolic pressure-volume relationship of the leftventricle or an increase in contractility secondary to areduction in ischemia. If peripheral venodilation alonewere the mechanism, then venous return and therebycardiac output should have decreased. In subsequentclinical studies, i.v. nitroglycerin at higher infusionrates (mean 57 ,ug/min) was a potent arterial dilatorwith a variable effect on stroke volume that dependedon the presence or absence of left ventricular failure.2Patients without left ventricular failure had a decreasein stroke volume as if they were moving leftward downthe same Starling curve. This might be expected toresult from venodilation and the associated reductionin venous return. Patients with mild-to-moderate leftventricular failure maintained or increased theirstroke volume despite a significant reduction in theirfilling pressures, appearing to move leftward along thesame flattened Starling curve or to shift upward and tothe left to a more favorable Starling curve. Thus,patients with the greatest elevations of left ventricularfilling pressure and the lowest stroke work obtained, inaddition to the beneficial antiischemic effects demon-strated in all hemodynamic subgroups, the optimalhemodynamic effects as well.We recently found that the incidence of acute
hypertension during the first 5 hours after coronaryartery bypass surgery was 61% (131 of 215 patients).1We investigated the possible roles of renin-angio-tensin and catecholamines in the pathogensis of thissyndrome. At peak hypertension, plasma catechola-mine levels were highest and renin and angiotensinlevels were low. Plasma catecholamine levels werecomparably elevated in both hypertensive and non-hypertensive patients. The patients with postoperativehypertension were statistically more likely to havebeen receiving chronic propranolol therapy and athigher doses than patients without hypertension. Therole of prior propranolol therapy in the pathogenesisof postoperative hypertension is uncertain.By design, mean arterial pressure was lowered
equally by the two drugs in the majority of patients;systemic vascular resistance was comparably lowered.At the time patients developed hypertension, systemicvascular resistance was markedly increased, associ-ated with decreased cardiac output. One might haveexpected an increase in cardiac output and heart rateif excess 3-adrenergic stimulation had been the cause.Instead, peripheral arterial constriction appeared tobe the primary response with a secondary decrease incardiac output. The mechanism responsible for thissudden increase in vascular resistance is unclear. Al-though we found that both renin and angiotensin weresuppressed when hypertension developed, other inves-tigators have reported elevated renin and angiotensinII levels. In our patients, renin and angiotensin levelsappeared to decrease rapidly after the development ofhypertension; slight differences in the timing of bloodsamples could explain this apparent contradiction. Allpatients were hypothermic (35-36°C) at the time oftheir hypertensive episode, but patients who developedhypertension were no more hypothermic than those
of administration of the two vasodilators should haveneutralized differences directly related to this gradualpostoperative rewarming.
Administration of nitroprusside to anesthetized pa-tients has been shown to result in a decrease in Pao2.In older patients and in patients with low preoperativePao2 values, Pao2 decreased markedly, suggesting aworsening of ventilation-perfusion mismatch.9 Seltzeret al.'0 found a similar decrease in Pao2 in pa-tients receiving nitroprusside for treatment of intra-operative hypertension.10 Several investigators havesuggested that the mechanism by which nitroprussideworsens intrapulmonary shunting is inhibition ofhypoxic vasoconstriction in the pulmonary vascula-ture, resulting in increased perfusion of poorly ven-tilated regions of the lung."14 Sublingual nitroglyc-erin caused only a small decrease in Pao2 in a group ofpatients with chronic obstructive pulmonary disease(COPD).15 Similarly, in patients undergoing coro-nary artery bypass surgery, nitroglycerin may havemore favorable effects on the alveolar-arterial oxygengradient and, in turn, on intrapulmonary shuntingthan does nitroprusside. In addition, the increase inPvo2 with nitroprusside could be explained by inhibi-tion of electron transport within mitochondria bycyanide, a metabolite of sodium nitroprusside.
Several investigators have compared the effects ofnitroglycerin and nitroprusside on the severity ofregional myocardial ischemia. Chiarello and co-workers4 administered both nitroglycerin and nitro-prusside to patients with acute myocardial infarctionand found directionally opposite effects on the severityof ischemia. The magnitude and extent of ST-segmentelevation recorded by precordial ST-segment mappingworsened when they infused i.v. sodium nitroprusside.When they administered sublingual nitroglycerin tothe same patients, ST-segment elevation was reduced.Chiarello et al. also performed a similar study in ananimal model using radioactive microspheres to quan-tify regional myocardial blood flow. When they in-fused sodium nitroprusside, epicardial ST segments inthe region of myocardium distal to the coronary liga-tion became more elevated and regional myocardialblood flow decreased. When they infused nitroglyc-erin and obtained comparable hemodynamic effects,ST-segment elevation in the ischemic region wasreduced and myocardial blood flow in that region in-creased. Thus, nitroprusside appeared to worsenregional ischemia by reducing coronary perfusionpressure without augmenting collateral flow. In con-trast, nitroglycerin appeared to improve ischemia byincreasing flow through preexisting intercoronary col-lateral channels, out of proportion to its effect on per-fusion pressure.
Subsequent studies have confirmed these differingeffects of nitroglycerin and nitroprusside on regionalmyocardial blood flow. In dogs with well-developedcollaterals induced by placement of an ameroid con-strictor, Capurro et al." showed that i.v. nitroglycerincauses a greater reduction in intercoronary collateralresistance than does nitroprusside. In patients with
who did not. Furthermore, the randomized sequence
1076 CIRCULATION
coronary disease and angiographically demonstrable
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

I.V. NITROGLYCERIN IN POSTOP HYPERTENSION/Flaherty et al.
collaterals, Mann et al." used the xenon washout tech-nique to show that regional blood flow distal to asevere coronary stenosis increased after infusion ofnitroglycerin but decreased after sodium nitroprus-side. Using an animal model of regional ischemiainduced by atrial pacing in the presence of a fixed cor-onary stenosis, we confirmed the ability of i.v. nitro-glycerin to dilate intercoronary collateral channels."6An increase in collateral blood flow became the domi-nant antiischemic effect when preload- and afterload-lowering effects of nitroglycerin were reversed by re-turning arterial pressure to control levels.
In conclusion, i.v. nitroglycerin and nitroprussideare effective for the management of acute hyper-tension after coronary artery surgery. Nitroglycerinand nitroprusside reduced arterial pressure andsystemic vascular resistance equally in the majority ofpatients. Nitroglycerin appears to have morefavorable effects on pulmonary gas exchange and in-trapulmonary shunting, which may be important inmanaging postoperative patients with pulmonaryhypertension or those with intrinsic lung disease andlarge intrapulmonary shunts. In view of the direction-ally opposite effects of nitroglycerin and nitroprussideon the severity of regional ischemia, nitroglycerin ap-pears to be preferable for use in patients with ischemicheart disease.
References1. Whelton PK, Flaherty JT, MacAllister NP, Watkins L, Potter
A, Johnson D, Russell RP, Walker WG: Hypertension follow-ing coronary artery bypass surgery: role of pre-operativepropranolol therapy. Hypertension 2: 291, 1980
2. Flaherty JT, Reid PR, Kelly KT, Taylor DR, Weisfeldt ML,Pitt B: Intravenous nitroglycerin in acute myocardial infarc-tion. Circulation 51: 132, 1975
3. Flaherty JT, Come PC, Baird MF, Rouleau J, Taylor DR,Weisfeldt ML, Greene HL, Becker LC, Pitt B: Effects of in-travenous nitroglycerin on left ventricular function and ST seg-ment changes in myocardial infarction. Br Heart J 38: 612,1976
4. Chiarello M, Gold HK, Leinbach RC, Davis MA, Maroko PR:Comparison between the effects of nitroprusside andnitroglycerin on ischemic injury during acute myocardial in-farction. Circulation 54: 766, 1976
5. Capurro NL, Kent KM, Epstein SE: Comparison of nitroglyc-erin, nitroprusside, and phentolamine induced changes in coro-nary collateral function in dogs. J Clin Invest 60: 295, 1977
6. Mann T, Cohn PF, Holman BL, Green LH, Markis JE,Phillips DA: Effect of nitroprusside on regional myocardialblood flow in coronary disease. Results in 25 patients and com-parison with nitroglycerin. Circulation 57: 732, 1978
7. Berggren SM: The oxygen deficit in arterial blood caused bynonventilating parts of the lung. Acta Physiol Scand 4: 11, 1942
8. Mason DT, Braunwald E: The effects of nitroglycerin onarteriolar and venous tone in the human forearm. Circulation32: 755, 1965
9. Wildsmith JAW, Drummond GB, MacRae WR: Blood-gaschanges during induced hypotension with sodium nitroprusside.Br J Anaesth 47: 1205, 1975
10. Seltzer JL, Doto JB, Jacoby J: Decreased arterial oxygenationduring sodium nitroprusside administration for intraoperativehypertension. Anesth Analg 55: 880, 1976
11. Colley PS, Cheney FW: Sodium nitroprusside increases Qs/Qtin dogs with regional atelectasis. Anesthesiology 47: 338, 1977
12. Hill AB, Sykes MK, Reyes A: A hypoxic pulmonary vasocon-strictor response in dogs during and after infusion of sodiumnitroprusside. Anesthesiology 50: 484, 1979
13. Colley PS, Cheney FW, Hlastala MP: Ventilation-perfusionand gas exchange effects of sodium nitroprusside in dogs withnormal and edematous lungs. Anesthesiology 50: 489, 1979
14. Benumof JL: Hypoxic pulmonary vasoconstriction and infusionof sodium nitroprusside. Editorial views. Anesthesiology 50:481, 1979
15. Kochukoshy KN, Chick TW, Jenne JW: Effect of nitroglycerinon gas exchange in chronic obstructive pulmonary disease. AmRev Respir Dis 111: 177, 1975
16. Gerry JL, Schaff HV, Kallman CH, Flaherty JT: Effects ofnitroglycerin on regional myocardial ischemia induced by atrialpacing in dogs. Circ Res 48: 569, 1981
1077
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

J T Flaherty, P A Magee, T L Gardner, A Potter and N P MacAllisteracute hypertension developing after coronary artery bypass surgery.
Comparison of intravenous nitroglycerin and sodium nitroprusside for treatment of
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1982 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.65.6.1072
1982;65:1072-1077Circulation.
http://circ.ahajournals.org/content/65/6/1072the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from









![[Biochemistry 1] nitroprusside reaction](https://static.fdocuments.in/doc/165x107/558c113ad8b42adf758b45be/biochemistry-1-nitroprusside-reaction.jpg)






