“COMPARATIVE STUDY OF VAGINAL DELIVERY AND CAESAREAN ...
130
I “COMPARATIVE STUDY OF VAGINAL DELIVERY AND CAESAREAN SECTION IN ANTEPARTUM ECLAMPSIA IN PRIMIGRAVIDA AFTER 32 WEEKS OF GESTATION” BY DR. SUDHARANI. C. N M.B.B.S., DGO, Dissertation submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore. In partial fulfillment of the requirements for the degree of MASTER OF SURGERY IN OBSTETRICS & GYNAECOLOGY Under the guidance of Dr. MUMTAZ BENDIGERI MD, Professor DEPARTMENT OF OBG VIJAYANAGAR INSTITUTE OF MEDICAL SCIENCES CANTONMENT BELLARY-583104. 2012
Transcript of “COMPARATIVE STUDY OF VAGINAL DELIVERY AND CAESAREAN ...

I
“COMPARATIVE STUDY OF VAGINAL DELIVERY AND
CAESAREAN SECTION IN ANTEPARTUM ECLAMPSIA IN
PRIMIGRAVIDA AFTER 32 WEEKS OF GESTATION”
BY
DR. SUDHARANI. C. N M.B.B.S., DGO,
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore.
In partial fulfillment of the requirements for the degree of
MASTER OF SURGERY
IN
OBSTETRICS & GYNAECOLOGY
Under the guidance of
Dr. MUMTAZ BENDIGERI MD, Professor
DEPARTMENT OF OBG
VIJAYANAGAR INSTITUTE OF MEDICAL SCIENCES
CANTONMENT BELLARY-583104.
2012

II
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,
KARNATAKA
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation / thesis entitled “COMPARATIVE STUDY OF
VAGINAL DELIVERY AND CAESAREAN SECTION IN ANTEPARTUM ECLAMPSIA
IN PRIMIGRAVIDA AFTER 32 WEEKS OF GESTATION” a bonafide and genuine
research work carried out by me under the guidance of DR. MUMTAZ BENDIGERI MD,
Professor OBG, Department of OBG, VIMS, Bellary.
Date: Signature of the Candidate Place: Bellary Name: Dr. SUDHARANI C.N

III
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA
CERTIFICATE BY THE GUIDE
This is to certify that this dissertation entitled “COMPARATIVE STUDY OF VAGINAL
DELIVERY AND CAESAREAN SECTION IN ANTEPARTUM ECLAMPSIA IN
PRIMIGRAVIDA AFTER 32 WEEKS OF GESTATION” is a bonafide research work done
by Dr. SUDHARANI. C. N, in partial fulfillment of the requirement for the degree of M.S
(OBG).
Date : Dr. MUMTAZ BENDEGERI. M.D Place: Bellary Professor, Dept. of OBG, Vijayanagar Institute of Medical Sciences, Bellary.

IV
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA
ENDORSEMENT BY THE HOD, PRINCIPAL/ HEAD OF THE INSTITUTION
This is to certify that this dissertation entitled “COMPARATIVE STUDY OF
VAGINAL DELIVERY AND CAESAREAN SECTION IN ANTEPARTUM ECLAMPSIA
IN PRIMIGRAVIDA AFTER 32 WEEKS OF GESTATION” is a bonafide research work
done by Dr. SUDHARANI. C.N under the guidance of
Dr. Mumtaz Bendegeri, M.D, Professor, Department of OBG, VIMS Bellary.
Dr. A.A. KHAZI, M.D., DGO, Dr. A.SRINIVASA MURTHY MD Professor & HOD PRINCIPAL Department of OBG, Vijayanagar Institute of Medical Sciences, Vijayanagar Institute of Medical Sciences, Bellary. Bellary. Date : Place : Bellary

V
COPYRIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka shall
have the rights to preserve, use and disseminate this dissertation / Thesis in print or electronic
format for academic / research purpose.
Date: Signature of the Candidate Place: Bellary. Name: Dr. SUDHARANI. C.N
© Rajiv Gandhi University of Health Sciences, Karnataka

VI
ACKNOWLEDGEMENT
My sincere thanks to my guide Dr. Mumtaz Bendigeri M.D, Professor, Department of
OBG for her constant guidance and valuable suggestions.
I also express my heartfelt gratitude to Dr. Khazi. A. A., Professor and Head, all
Professors, Associate Professors & Assistant Professors for their valuable suggestions.
My sincere thanks to the Dr. Srinivasa Murthy Principal, V.I.M.S., Dr. B. Devanand
Director, V.I.M.S., and Dr. Vidyadhar Kinhal Medical Superintendent V.I.M.S., Bellary for
their unconditional help and support during my post-graduation and dissertation.
My also express my heartfelt gratitude to All- dept. of Anaesthesiology i.e., Prof. &
HOD, Dr. Devanand. B., Professors, Dr. Srinivasmurthy. A., Dr. Srinivasulu, Associate
Professors, Assistant Professors and postgraduates for their full co-operation during the study
period.
I am thankful to my Parents & Brother, & co postgraduate students for their full support
during this work.
I also acknowledge with gratitude, All the Patients who have co-operated for this study.
Finally I acknowledge the almighty.
Date: Signature of the Candidate Place: Bellary. Name: DR. SUDHARANI. C.N

VII
LIST OF ABBREVIATIONS USED
C.D. group....... Caesarean Delivery group
CPD................. Cephalopelvic Disproportion
DIC.................. Disseminated Intravascular Coagulation
IUD................. Intrauterine Death
IUGR............... Intrauterine Growth Restriction
MMR............... Maternal Mortality Rate
NICU............... Neonatal Intensive Care Unit
PND................. Post Natal Day
PNM................ Perinatal Mortality
PMR................ Perinatal Mortality Rate
PPH................. Postpartum Hemorrhage
V.D. group...... Vaginal Delivery group
HIE…………. Hypoxic Ischemic Encephalopathy
MAS………... Meconium Aspiration Syndrome
RDS………… Respiratory Distress Syndrome
NND………... Neonatal Death

VIII
ABSTRACT
Objective: To compare maternal and fetal outcome in pregnancies of primigravidae with more
than 32 weeks gestation complicated by antepartum eclampsia when terminated by caesarean
section and when terminated by vaginal delivery.
Material and Methods: 100 primigravidae with more than 32 weeks of gestation with
antepartum eclampsia were studied from admission to discharge or death.
Depending upon the mode of delivery, they were divided into two groups: C.D. group, where
caesarean section was performed and V.D. group, where vaginal delivery was carried out.
Maternal and perinatal outcomes were studied in the two groups and compared.
Results: Of the 100 cases, caesarean section was done in 41% of the cases, while vaginal
delivery was carried out in 59%. Maternal complications were seen in 13.4% of the cases in the
C.D. group and 29.2% of the cases in the V.D. group. Maternal deaths occurred in none of the
cases in the C.D. group and in 1.7% of the cases in the V.D. group.
The incidence of live births, still births and neonatal deaths was 92.3%, nil and 7.3% respectively
in the C.D. group, while it was 78%, 11.8% and 8.4% in the V.D. group. Apgar score less than 5
at 1 minute was seen in 9.7% cases in the C.D. group and 25.5% cases in the V.D. group. 21.9%
of the cases in the C.D. group and 32.2% of the cases in the V.D. group required NICU
admission.
IX
Conclusion: Timely caesarean section reduces maternal and perinatal mortality and improves
their outcome in antepartum eclampsia, especially in primigravidas with more than 32 weeks of
pregnancy.
Keywords: Primigravida; Antepartum eclampsia; Caesarean section.
X
TABLE OF CONTENTS
1. Introduction........................................................................... 01
2. Objectives ............................................................................. 03
3. Review of Literature ............................................................. 04
4. Methodology......................................................................... 35
5. Results................................................................................... 41
6. Discussion............................................................................. 65
7. Summary ............................................................................ 77
8. Conclusion............................................................................. 80
9. Bibliography ......................................................................... 82
10. Annexures
Proforma ............................................................................... 93
Master Chart.......................................................................... 96

XI
LIST OF TABLES
SL.
NO.
TITLE PAGE PAGE
NO.
1. Incidence of Eclampsia in Primis 14
2. Incidence of Unbooked Cases 14
3. Incidence of Different types of Eclampsia in Different Studies 18
4. Maternal Mortality figures in different Studies using different
Regimes
23
5. Perinatal Mortality in Different Studies 26
6. Age-wise distribution of study subjects 41
7. Religion-wise distribution of study subjects 42
8. Relation between number of convulsions and mode of delivery 43
9. Relation between consciousness b/w convulsions and mode of
delivery
44
10. Relation between ante natal checkup and mode of delivery 45
11. Relation between patient general condition and mode of delivery 45
12. Relation between conjunctiva status and mode of delivery 46
13. Relation between tongue condition and mode of delivery 46
14. Mode of delivery 47
15. Relation between gestational age and mode of delivery 48

XII
16. Indications for caesarean section 49
17. Incidence of IUD’S on admission 50
18. Relation between Modified bishop score finding and mode of
delivery
50
19. Bishop’s Preinduction Cervical Scoring System 51
20. Convulsion- delivery interval 52
21. Induction-delivery interval 52
22. Perinatal Morbidity 53
23. Comparison of birth weight, APGAR score and NICU stay 54
24. Perinatal Mortality 55
25. Analysis of causes of perinatal mortality with gestational age
>32 weeks
56
26. Comparison of pnm with respect to GA (excluding IUDS) 57
27. Comparison of pnm with respect to birth weight 58
28. Relation of pnm to total no convulsion 59
29. Maternal complications 60
30. Relation maternal complications to convulsion delivery interval 61
31. Relation maternal complications to induction delivery interval 62
32. Relation between cessation of proteinuria and mode of delivery 62
33. Maternal Mortality 63

XIII
34. Comparison of time between events 63
35. Comparison Blood Pressure 63
36. Comparison blood pressure during admission and delivery 64
37. Comparative incidence of caesarean section in eclampsia 66
38. Comparative incidence of PNM to mode of delivery 70
39. Comparative study of PNM to Convulsion-Delivery Interval
in Lopezllera Series
73
40. Comparative Incidence of Maternal Mortality to Mode of
Delivery
75
41. Relation of maternal Mortality to First Convulsion-Delivery
Interval
76

XIV
LIST OF FIGURES Sl.
No.
Figure Page No.
1. Age wise distribution 41
2. Religion wise distribution 42
3. Relation b/w no. of convulsions and mode of delivery 43
4. Relation b/w consciousness and mode of delivery 44
5. General condition and mode of delivery 45
6. Distribution of study subjects based on tongue status 46
7. Mode of delivery 47
8. Gestational age and mode of delivery 48
9. Indications for caesarean section 49
10. Perinatal morbidity 53
11. Birth weight of babies 54
12. APGAR score 54
13. Perinatal outcome 55
14. Causes of perinatal mortality with gestational age > 32 weeks 56
15. Comparison of PNM with respect to gestational age 57
16. Comparison of PNM with respect to birth weight 58
17. Relation between PNM and Convulsions 59
18. Maternal complications 60
19. Relation between maternal complications and convulsion delivery
interval
61

XV
20. Maternal mortality and mode of delivery 62
21. Systolic Blood Pressure during admission and delivery 64
22. Diastolic Blood pressure among study subjects 64

1
INTRODUCTION
The term eclampsia is derived from a Greek word, meaning "like a flash of
lightening"1.
The onset of convulsions in a woman with pre-eclampsia that cannot be
attributed to other causes is termed eclampsia2.
The incidence in India ranges from 1 in 500 to 1 in 30. It is more common in
primigravidae (75%), five times more common in twins than in singleton pregnancies
and occurs between the 36th week and term in more than 50%1.
Eclampsia is an obstetric enigma. Though it has almost been eradicated from
the developed world, it continues to be a major cause of maternal and fetal mortality
and morbidity in the developing countries. The real challenge of eclampsia has not
been met. In spite of considerable progress made in the field of obstetrics, the
incidence of eclampsia and its consequent complications has not decreased
significantly in our country over the past few decades. It is indeed sad that even today
antenatal care is available only to a fraction of our rural population. However, the
management of eclampsia still poses a fascinating challenge to the obstetrician,
requiring the greatest skill, judgement and patience3.
Eclampsia is essentially a disease of low socio economic status of
primigravida, a product of ignorance and neglect. Ideally, it is a preventable disease or
almost so. But unfortunately its incidence is still uncomfortably high in any hospital
accepting unbooked cases. Menon et al (1989) quoted an incidence of 0.83% to 1.6%
from leading centres of India.
Faced with this reality, a plan of management has to be evolved. Though the
exact pathophysiology leading to the occurrence of fits is still not understood, one

2
thing has been proved beyond doubt that termination of pregnancy, removes the basic
cause of the disease. Keeping this in view an attempt has been made in the present
study to ascertain if caesarean section has any distinct advantage over vaginal delivery
in lowering maternal and perinatal deaths4.
3
AIMS AND OBJECTIVES
1. To evaluate the role of termination of pregnancy by caesarean section and
termination by vaginal delivery in antepartum eclampsia occurring in
primigravidae with more than 32 weeks gestation, with reference to perinatal
morbidity and mortality and maternal morbidity and mortality.
2. To compare the results of termination of pregnancy by caesarean section with
those obtained by routine or induced vaginal delivery in primi with more than
32 weeks gestation with antepartum eclampsia, with reference to perinatal
morbidity and mortality and maternal morbidity and mortality.
4
REVIEW OF LITERATURE
Historical Aspects:
The oldest source for eclampsia literature starts from 2200 BC, when Kahun
Papyrus mentioned the use of a wooden stick to prevent the mother from biting her
tongue on the day of delivery.
Indian Atharvaveda described an amulet to be worn by the mother at her 8th
month of pregnancy for warding off convulsions during childbirth.
In Sushrutha Samhita, it has been mentioned that, 'the child moving in the
womb of a dead mother, who has just expired from convulsions, should be delivered
by cutting open the abdomen'.
Hippocrates, in his aphorisms section VI, No. 39, wrote convulsion take place
either from repletion or depletion. He noted that headaches, convulsions and
drowsiness represented omnious signs in postpartum period.
Rossilin (1513) listed unconsciousness with convulsions as the ominous sign
of eclampsia.
Gaebel Khouren (1596) stated that pregnant uterus causes convulsions
particularly if it contains a malformed fetus5.
Dexter and his associates mentioned that the term "eclampsia" first appeared
in a treatise on gynecology written by Varandaeus in 1619.
Pew (1694) described clonic spasms in association with pregnancy.
Mauriceau (1668) stated that convulsions often cease with delivery and
recommended prompt termination of pregnancy as the best treatment. He set forth
several aphorisms dealing with eclampsia. Among them were:

5
• The mortal danger to mother and fetus is greater when the mother does
not recover consciousness between convulsions.
• The primigravidae are at greater risk of convulsions than the
multigravidae.
• Convulsions during pregnancy are more dangerous than those
beginning after delivery.
• Convulsions are more dangerous if the fetus is dead.
Eclampsia has been a therapeutic problem since it was first recognized as a
definite disease. Its treatment has undergone an evolutionary process consisting of six
periods as described by Dieckmann;
The First Period: beginning in 1745 and lasting approximately 100 years, was
considered a non-operative era and had as its stalwarts purging, sweating and blood
letting.
The Second Period: began about 1845 and lasted approximately 50 years. This was
characterized by the initial introduction of veratrum viride as well as the more radical
trend toward immediate delivery by manual dilatation of the cervix.
The Third and Fourth Periods: Overlapped each other, beginning about 1895 and
terminating in 1915. They represented the era of ultra radicalism. During this period,
immediate delivery by caesarean section, vaginal hysterectomy, or accouchement
force (Boosidilator) was the treatment of choice.
The Fifth Period: Extended from 1915 to 1927 and brought into focus conservative
medical management utilizing intravenous hypertonic glucose solution, sedation,
elimination and parenteral magnesium sulphate, which was introduced by Titus

6
(1920). The slogan in the late 1920s thus became, "treat the eclampsia medically and
ignore the pregnancy".
The Sixth Period: Started in 1928 when Stroganoff advocated artificial rupture of
membranes for induction of labour in addition to profound sedation and narcosis to
prevent and control seizures. Stroganoff regime included:
• A darkened room
• Liberal use of chloroform, chloralhydrate and morphine
• Artificial rupture of membranes
• Magnesium sulphate
• Administration of oxygen during fits.
He reported a maternal mortality rate of 2.6% and uncorrected perinatal mortality of
16.6% with his regime.
All the periods as described were overlapping eras of therapy, which came
into existence after the discovery of a new drug, procedure, or method of treatment by
a noted person of the time. A wide variety of both operative and non-operative
methods was used in an attempt to lower the exceedingly high maternal mortality
rates. Some of these, such as:
• Retromammary injection of potassium iodide or air
• Radical mastectomy
• Renal decapsulation
• Trephining of the skull
• Massive venesection
7
• Lumbar puncture with withdrawal of large amounts of spinal fluid and
• Massive doses of thyroid undoubtedly seemed barbaric
When one also considers the radical procedures of the day for emptying the
uterus, however, it becomes quite obvious that the accoucheurs of that period were
desperate in their attempts to conquer a disease with a fantastically high mortality
rate6.
The following years (1929-1950) saw the use of varied drugs like veratone,
bromethanol caudal anesthesia with 15% solution of methycaine, tribromethanol,
sodium thiopentone, etc.
Morris and Dewar (1947) during their trials with rectal bromethal in eclampsia
recommended caesarean section in cases where prompt uterine responses to artificial
rupture of membranes was unlikely as judged by the nature of the cervix on vaginal
examination.
Then, followed a period of indecision, obstetricians all over the world began to
realize that the results could not be improved further by the conservative line of
treatment in whatever shape it is adopted. It was then that caesarean section came into
focus. Several authors started recommending caesarean section: prominent among
them were Dieckmann (1952) remarked "caesarean section is performed if there is
cephalopelvic disproportion or if the eclampsia is severe and the cervix is closed and
uneffaced7.
River Forest8 (1956) who commented further on the use of caesarean section
in eclampsia, that it should be selected primarily in patients in whom the cervix was
not ripe because of prematurity.
8
Corhill TF9 (1957) who stated that there was no place for caesarean section as
a last desperate measure in cases, which were rapidly deteriorating. He advocated
caesarean section whenever the eclampsia was severe and occurred earlier in
gestation.
Tenny and Dandrow10 (1961) who asserted that caesarean section is a life
saving procedure especially in the young primigravida with premature baby and an
unfavourable cervix.
Krishna Menon7 (1961) who studied 104 cases of eclampsia by subjecting
them to caesarean section. He was surprised when contrary to the heavy maternal
mortality reported earlier and because of which caesarean section was literally
contraindicated in the eclamptic state, he obtained a maternal mortality of 4.8% and
one death in his series was not attributable to operative procedure. He was convinced
that in properly selected cases under modernconditions, caesarean section did not
enhance the inherent maternal mortality. Menon made 2 pertinent observations:
• Firstly, that antepartum eclampsia has the maximum mortality
• Secondly, that in the severe type of eclampsia the longer the time
interval between the onset of fits and delivery, the greater the
mortality.
He advocated caesarean section in all severe cases of eclampsia in which
convulsions could not be controlled. From his study of caesarean section, two things
struck him"
1. Caesarean section in the eclamptic under modern condition is
not so very dangerous to the mother.

9
2. There is remarkable improvement in the patient within 24 hours
of section.
Derek Crichton11 (1962) who gave his firm belief that earlier recourse to
caesarean section would reduce the incidence of eclampsia in patients with severe pre-
eclampsia who were not responding satisfactorily to treatment. Similarly, he
considered that, caesarean section should play an important role in eclamptic patients,
whose onset or progress in labour was not rapid, who did not come into labour rapidly
after induction of labour, or who were unfavourable for induction.
Lokenath Bhose12 (1964) who remarked that none of the women with non
conclusive toxaemia developed convulsion after abdominal delivery.
Alan Alexander13 (1966) who obtained a low MMR of 4.2% and a low PNM
by rapid stabilization of patients and early delivery of the fetus. He found that those
delivered by caesarean section after stabilization, without an attempt to induce labour
had no PNM and none of the surviving babies showed any neurological sequelae,
whereas 50% babies born by caesarean section after an attempt at induction of labour
had neurological damage. Those delivered vaginally following successful induction
had a PNM of 33% and 33% of the surviving infants had neurological damage.
Brooks Ramney (1966) and Mario Lopezllera14 (1967) whose studies agreed
with Alan Alexander's studies. They noted that fetal hypoxia and increasing cerebral
pressure, resulting from strong uterine contractions of a difficult induction, would do
the toxaemic baby no good.
Lean TH, Ratnam SS, Sivasamboo R15 (1968) who reported MMR of 3.3%
and PMR of 11.1% with diazepam therapy. 2.2% was the incidence of recurrence of
fits after initiation of the therapy. Caesarean section was done in primigravidae who

10
were not in labour or with less than 5cms dilatation 1 hour after sedation and in multi
gravidae who were not in labour or whose cervix was unfavourable.
Derek Crichton, Morris Notelo Vitz and Heller16 (1968) who resorted to
caesarean section if the patient was not in labour or if fits could not be controlled.
Preliminary hypotensive and pethidine therapy was not given if immediate caesarean
section was to be carried out. The MMR was 4.2% to 4.8% in the caesarean section to
vaginal route delivery and the PMR was 27.6% to 45.7% in the caesarean section to
vaginal delivery route groups. They advocated prompt caesarean section unless easy
vaginal delivery could be anticipated within 4-6 hours and also if convulsions could
not be adequately controlled.
Villiers and Slabber17 (1970) who advocated an early termination by caesarean
section and the rate of caesarean section in their series was 76%. The overall fetal
mortality was 23.3% and the corrected PMR was 14.4%. Eclamptic patients recovered
smoothly from caesarean section, more smoothly than after vaginal delivery in 24-48
hours after the last fit. MMR was 4.3% to 12.7% in the caesarean section to vaginal
delivery groups.
Ajay Ghosh18 (1974) who reported favourably on caesarean section in ante
and intrapartum eclampsia. There was no mortality in his series and was impressed
with the dramatic recovery of the cases after caesarean section. He observed that early
operation when the patient was in good condition was much safer than delayed
operation after an unpredictable or failed conservative regime.
Chesley5 (1978) who has favoured caesarean section to reduce maternal and
perinatal mortality.

11
Nanda Smiti19 (1989) who studied 172 patients of eclampsia to analyze
perinatal mortality and stated that mortality increased with increase in blood pressure,
increase in first fit treatment interval and first fit delivery interval. This study,
perinatal mortality was lowest (20%) where caesarean section was performed.
Swain S20 (1993) who suggested that more frequent use of properly timed
caesarean section can improve the maternal outcome.
Arupkumar Majhi21 (2001) who found that the outcome of mother and fetus
was relatively better in cases who were actively managed delivered by caesarean
section than in those who waited deliveries by vaginal route, in his study of 877
eclamptic women.
Lee W Connell115 studied maternal and perinatal outcomes of eclampsia found
increased rates of caesarean section 79%. No maternal deaths, maternal complications
were 32%, perinatal mortality rate was 64 in 1000 deliveries112
Taj116 studied 100 patients of eclampsia, among them 71 patients were normal
vaginal delivery, 25 patients needed caesarean section. Maternal mortality was 2%
perinatal mortality was 38%. Perinatal mortality was higher in vaginal group 12%
than LSCS group 7%113.
Kamilya G, Bharracharyya SK, Mukherji J22 (2005) who analyzed maternal
and perinatal outcomes in eclampsia after the introduction of magnesium sulphate and
liberarization of caesarean section over a period from August 2002 to September
2004. They found that the caesarean section rate for eclampsia has increased from
near 10% to 49.7%. Both maternal mortality and perinatal mortality are lowest in the
caesarean section group.

12
Jamila117 study conducted on 254 cases found that maternal death is 0.4% that
is 1 and perinatal mortality was 11 % in caesarean section114.
Barret118 M discussed vaginal delivery is the optimum mode of delivery in
women with severe preeclampsia and eclampsia116.
M Khanum119 studied 100 cases of eclampsia out of which vaginal delivery
had better apgar than caesarean section group. Perinatal mortality was 38%118.
Incidence
The incidence of Pregnancy induced hypertension is between 5% to 15%. The
incidence of Eclampsia varies from country to cou'ntry. Incidence ranges from 0.02%
in United Kingdom (Douglas, Redman) 1994 to 2.3% in India (Arup Kumar Kanhi
1998)24.
The incidence in various University Hospital are24,25,26,27,28,29
1. National University Hospital Singapore 1990 0.1%
2. Women's Hospital, Madras 1990 0.5%
3. NRS Medical College Hospital, Calcutta 1990 1.2%
4. Collaborative Eclampsia Trial Group 1995 1.0%
5. Arup Kumar Kanhi 1998 2.3%
6. Nilesh Dalal 1998 1.59%
In a one year descriptive study, Dr. Suchita Mundle27 found the incidence to
be 1.13% Dr. Srinivas Gadappa in a prospective study of 175 cases over a 2 year
period (1995-1997) found the incidence to be 1.5%.

13
Age:
Most studies found Eclampsia27,30,31 to be high between 20-25 years of age
Some studies found Eclampsia to be more common in age less than 20 years.

14
Parity:
Eclampsia is very common in primigravidae as found out by most
studies24,29,30,32,33.
Table-l: Incidence of Eclampsia in Primis
Author Year Primis
Low 11 1995 64%
A.K. Kanhi 1998 88.6%
Vinita Bansal 1998 74.4%
Arati Srivastav 1998 70%
Srividya 1998 70%
Socioeconomic Status:
Eclampsia is found to be high in women with low socioeconomic
status24,27,28,32.
Arup Kumar Kanhi(l998) found 53% of the Eclamptic women to be in low
socioeconomic status.
Unbooked Status:
According to the following studies24,29,32,34. Unbooked status is found to be a
significant risk factor for development of Eclampsia.
Table-2: Incidence of Unbooked Cases
Author Year Percentage unbooked
A.K.Kanhi 1998 82.3%
Srividya 1998 70%
Arati Srivastav 1998 96%
Conde Aguedelo (1997)35 an Mwinyoglee Amoko 199636 were other authors
who found un booked status to be high.

15
Gestational Age:
The mean gestational age found out by various studies are as follows
Low JJ33 1995 35.9 weeks
S Mundle27 1998 29 to 36 weeks
Hungarga31 1998 33 to 37 weeks
Clinical Features:
The women with Eclampsia will have generalized tonic clonic convulsions,
mostly preceded by imminent signs like headache, vomiting, epigastric pain and
visual disturbances. The frequency of various signs and symptoms of impending
Eclampsia as found out by Sibai 198137 are as follows.
Symptoms Patients in whom present %
Headache 83%
Proteinuria 80%
Oedema 60%
Clonus 46%
Visual Signs 45%
Epigastric pain 20%
Low JJ in 199533 has found out that 40.7% patients were asymptomatic prior
to first fit. Headache was next common symptom.
Sibai et al (1992 to 1997)38 has studied the association between various
imminent signs and symptoms and development of Eclampsia. Only headache, deep
tendon reflexes and protenuria more than 3+ were found to be significantly associated
with development of Eclampsia. He has found no association between Eclampsia and
systolic, diastolic or Mean Arterial Pressure, epigastric pain, gestational age at
delivery or laboratory values including platelet count and Liver Function Tests.

16
Convulsions are of tonic clonic nature. Tonic phase lasts for 15 to 20 seconds.
Clonic phase lasts for 1 minute. Respiration is halted followed by deep stertorous
breathing. The woman usually recovers some degree of consciousness after each
attack. On general examination patient can be conscious, semiconscious, restless,
irritable or comatose.
Other clinical features are
• Increased respiratory rate due to hypercarbia Cyanosis
• Fever
• Proteinuria
• Decreased Urine output Edema
• Exaggerated deep tendon reflexes Increased Blood Pressure
Points to be remembered:
• Deep coma and fever more than 39°C are grave signs.
• The number of convulsions, interval between convulsions, convulsion
• delivery interval are important in influencing maternal and perinatal
out come.
• Once the convulsion occurs, prognosis becomes uncertain. Prognosis
depends on may factors and the ominous features are:
1. Long interval between fit and commencement of treatment.
2. Antepartum Eclampsia with long convulsion delivery interval.
3. Fits more than 10.
4. Coma in between fits.
5. Temperature more than 102° F with pulse rate more than 120 per minute.
6. Blood pressure more than 200 mm of Hg systolic.
7. Oliguria less than 400 ml per 24 Hours.
8. Proteinuria more than 5 grams per 24 Hours.

17
9. Non response to treatment 10. Jaundice.
Differential Diagnosis:
Though Eclampsia is easily diagnosed on clinical grounds, other conditions
have to be considered especially when Eclampsia is unresponsive to Magnesium
Sulphate therapy.
According to Friedman, Sibai (1997) the following are the differential diagnosis.
1. Status epilepticus
2. Head injury
3. Intra cranial bleeding
4. Cerebral tumors
5. Meningitis
6. Cerebral infarction
7. Cerebral aneurysms
Sejal V.Desai et. al., (I 998)40 conducted a retrospective study and found that
out of 84 cases 24.7% were non eclamptic convulsions. Non eclamptic causes of
convulsions were cerebral malaria, cortical venous thrombosis, encephalopathy,
tuberculosis, infarct, hemorrhage.

18
Type of Eclampsia:
Various authors have found the following incidence of different types of
Eclampsia in their studies.
Table-3: Incidence of Different types of Eclampsia in Different Studies
Name of the Author Type of Eclampsia Incidence
Sibai (I 981 )37 Antepartum Eclampsia
Intrapartum Eclampsia
Postpartum Eclampsia
46.3%
16.4%
37.3%
Mwinyoglee Amoko (I 996)36
Antepartum Eclampsia
Intrapartum Eclampsia
Postpartum Eclampsia
77.3%
18.2%
4.50%
Leitch, Cameron(1997)41 Antepartum Eclampsia
Intrapartum Eclampsia
Postpartum Eclampsia
77.3%
18.2%
4.50%
A. Srivastava (I998)32 Antepartum Eclampsia
Intrapartum Eclampsia
Postpartum Eclampsia
48.0%
24.0%
28.0%
Leitch et al have conducted that due to decreased incidence in antepartum and
intrapartum Eclampsia, there is a relative increase in incidence of postpartum
Eclampsia in United Kingdom.
Laboratory Abnormalities in Eclampsia:
Laboratory values reflect the effects of Eclamptic process on kidney, liver,
hematological elements and fetoplacental unit. In complicated Eclampsia renal
parameters like serum creatinine, blood urea nitrogen and serum uric acid are

19
increased. Liver parameters like serum bilirubin, SGPT, SGOT and LDH are
increased.
Coagulation abnormalities:
Pritchard (1976)62 found thrombocytopenia in 29% of 95 cases, prolonged
prothrombin time in 50% and increase serum fibrin degradation products in 3%. Overt
hemolysis was seen in only less than 2%. Coagulation disorders in Eclampsia are rare
in the absence of abruption.
Thrombocytopenia can be induced acutely by preeclampsia and Eclampsia.
Leudec et al 199225 found that thrombocytopenia is more common in severe
preeclampsia/ eclampsia and depends upon the length of delay between the onset of
preeclampsia and delivery and the frequency with which platelet counts are
performed. Overt thrombocytopenia, defined by a platelet count less than one lakh is
an ominous sign.
Causes of thrombocytopenia in Eclampsia were investigated by Torres
associates, 199644 Pritchard of colleagues 197642 Samuels and colleagues 198745
Burrows and colleagues 198746 , Kelton and colleagues 198547, Kilby associates
199048 Weinstein 1982 referred to the combination of thrombocytopenia, elevated
liver enzymes and hemolysis as HELLP syndrome which is more ominous than
Eclampsia.
Dickmann 195249 Pritchard 198450 have found hemoconcentration and absent
hypervolemia in Eclampsia. Eclamptic women are unduly sensitive to vigorous fluid
therapy and tend to go for pulmonary edema easily (Lopez-Llera 1982)51

20
Pathology and Pathophysiology in Eclampsia:
Main pathology is in brain, which shows vasospasm. Sheehan 1950 52 in his
study observed edema, hyperemia, thrombosis and hemorrhage in 56% (in
histopathological examination). 75% of Eclamptic women show abnormal
electroencephalograms within .48 hours of seizures, which become normal by 3
months (Sibai 1985)53.
Brown and colleagues 198854 studied CT scans and found abnormal findings
in 50% of Eclamptic women. The most common findings in CT were hypodense
cortical areas corresponding to petechial hemorrhage. Moriss and colleagues 199755
showed changes especially in the area of posterior cerebral artery in MRI studies.
21
Pathophysiology:
Exact pathogenesis of Eclampsia remains unknown. It is possible that severe
arterial vasospasm causes rupture of the vascular endothelium and peri capillary
hemorrhage with the development of foci of abnormal electrical discharge that may
generalize and cause convulsions.
Horn and Filshie 199056 found that nimodipine, which is a selective cerebral
vasodilator, caused rapid reversal of symptoms in an Eclamptic patient. Donaldson in
198757, proposed that with acute severe hypertension the upper level of auto
regulation is reached producing a reactive vasospasm, leading to seizures. According
to this theory, upper limit of cerebral perfusion pressure varies among individuals.
Patient with chronic hypertension are capable of tolerating higher mean arterial
pressure than others. So a young preeclamptic patient may convulse with a systemic
blood pressure of 140/96 mm of Hg, where as a patient with chronic hypertension and
superimposed preeclampsia may
Tolerate pressure as high as 226/150mm of Hg or more without convulsions.
Retina:
Retinal artery vasospasm is associated with visual distrubances. Fundoscopy
shows focal or generalised vasospasm. Belfort and associates in 199258 showed that
Magnesium sulphate dilates retinal artery.
Liver:
Liver shows periportal hemorrhagic necrosis reflected by raised liver function
tests. Manas and colleagues59 have done CT scan study and found that 5 out of 7
women with preeclampsia and upper abdominal pain had hepatic hemorrhage. Smith

22
and coworkers 199160 reviewed 28 cases of spontaneous hepatic rupture associated
with preeclampsia and found the mortality rate to be 30%.
Kidney:
Renal perfusion and glomerular filtration rate are reduced with development of
preeclampsia/eclampsia. Plasma uric acid concentration is typically elevated
especially in women with more severe disease. The elevation of plasma creatinine is
likely due to intrinsic renal changes caused by severe vasospasm (Pritchard et al
198450 Lee and associates 1987)61 In the absence of underlying chronic renovascular
disease, complete recovery of renal function is anticipated after delivery. Sibai and
associates 199062 have concluded that if renal cortical necrosis supervenes, oliguria is
irreversible.
Maternal outcome is Eclampsia:
Eclampsia is one of the most dangerous conditions that can afflict a pregnant
women and her fetus. Fortunately maternal mortality due to Eclampsia has fallen in
the past 3 decades.
Given below are the maternal mortality figures in different studies, using
different treatment regimens, from 1960's to 1990's:

23
TABLE-4 MATERNAL MORTALITY FIGURES IN DIFFERENT STUDIES
USING DIFFERENT REGIMES
Sl.
No Study Year Treatment Mortality %
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Menon 7
Llewellyn Jones63
Byrant Fleming64
Zuspanos65
Lopez-Llerasl51
Lean and coworkers 15
Gedekoh and colleagues66
Pritchard and associates50
Bhalla and coworkers68
Eclampsia trail collaborative Group69
Frangieh and associates 70
Porapakkam 71
Harrison 72
Giri26
WH073
Mwinyoglee Amoko36
Saumundal B.K74
S. MundleD37
S. GadappaL28
Khanum119
1961 1961 1962 1964 1967 1970 1973 1976 1979 1968 1981 1984 1994 1995 1996 1979 1985 1991 1991 1996 1998 1998 1998 2004
Lytic cocktail Lytic cocktail Magnesium Sulphate Magnesium Sulphate Lytic cocktail Lytic cocktail Diazepam+Reserpine Furosemide+Reserpine+ Alb umin+antithrombotic Barbiturates+ MgSo4. 7H2O+ Resperpine Chlordiazepoxide MgS04.7H2O+ Hydrallazine MgS04.7H2O+Hydrallazine + standard regimen MgS04. 7H2O + nifedipine Lytic cocktail + nifedipine MgS04.7H2O; Diazepam MgS04.7H2O; Phenytoin MgS04.7H2O+ Hydrallazine Thailand Nigeria India Malaysia South Africa India India India Rajshahi
2.20 6.60 1.60 3.40 10.20 11.70 17.50 12.50 16.20 3.30 5.80 0.40 4:40 3.8; 5.1 2.6; 5.2 0.50 4.70 10.80 6.20 12.00 21.20 5.30 7.00 1.41 2.00
The maternal mortality has ranged from less than 1.0% to as much as 20% in
these studies.
Maternal Complications:
Cerebral haemorrhage:
Govan( 1961 )75 investigated the cause of death in 110 fatal cases of
Eclampsia and concluded that cerebral hemorrhage was responsible in 39 of them.

24
Coma:
Prognosis for comatose eclamptic women in guarded. Extreme cerebral edema
is documented in most of these cases. Sheehan and Lynch 197376 reported that 6 out
of 76 women with fatal Eclampsia had massive white matter hemorrhage that caused
coma and death. They also reported a high mortality rate with bleeding into basal
ganglia or pons.
Hellp Syndrome:
Liver involvement in preeclampsia/eclampsia is serious and is frequently
accompanied by evidence of other organ involvement especially kidney, brain along
with hemolysis and thrombocytopenia (DE Boer 199177 , Pritchard 195478 , Weinstein
1985 )79 Sibai and co. workers 199380 found the incidence to be 2.3% in eclampsia.
When HELLP syndrome occurs in Eclampsia, the incidence of other complications is
also increased (Audibert Associates 1996)81
Pulmonary Edema:
Eclamptic women are prone to develop left ventricular failure and pulmonary
edema in response to even minimal fluid overload (Lopez-Llera 198251, Gedekoh
198166 , Sibai 198782 ) Cinocotta and Ross A found the incidence of pulmonary
edema to be 3%. Bansal V 19986 found the incidence to be 4.6%.
Blindness:
The causes for visual disturbances in Eclampsia are retinal artery vasospasm,
retinal detachment, occipital lobe ischemia. Cunningham and associates 199583
described 15 women with severe preeclampsia or Eclampsia who also had blindness.
In all women it resolved between 4 hours to 8 days. Even with retinal detachment,
vision usually returns within a week.

25
Abruption:
Sibai38 found the incidence of abruption to be 16% in Eclampsia. Bansal V in
199830 found the incidence of abruption in her study to be 6.9%. Abruption in
Eclampsia increases the occurrence of complications like acute renal failure and Ole.
Acute Renal Failure:
Los Angeles country study 198384 implicated acute renal failure in 7 out of 67
maternal deaths (10.4%). Collaborative Eclampsia trial group 199569 found 5 cases of
renal impairment in 110 maternal deaths due to Eclampsia (4.5%). Sibai 1990
concluded that incidence of acute renal failure is high in Eclampsia complicated with
abruption.
Psychosis:
It rarely follows Eclampsia and it can last of several days to 2 weeks.
Perinatal outcome:
Perinatal outcome is compromised in eclampsia. Perinatal Mortality has been
evaluated in various studies.
26
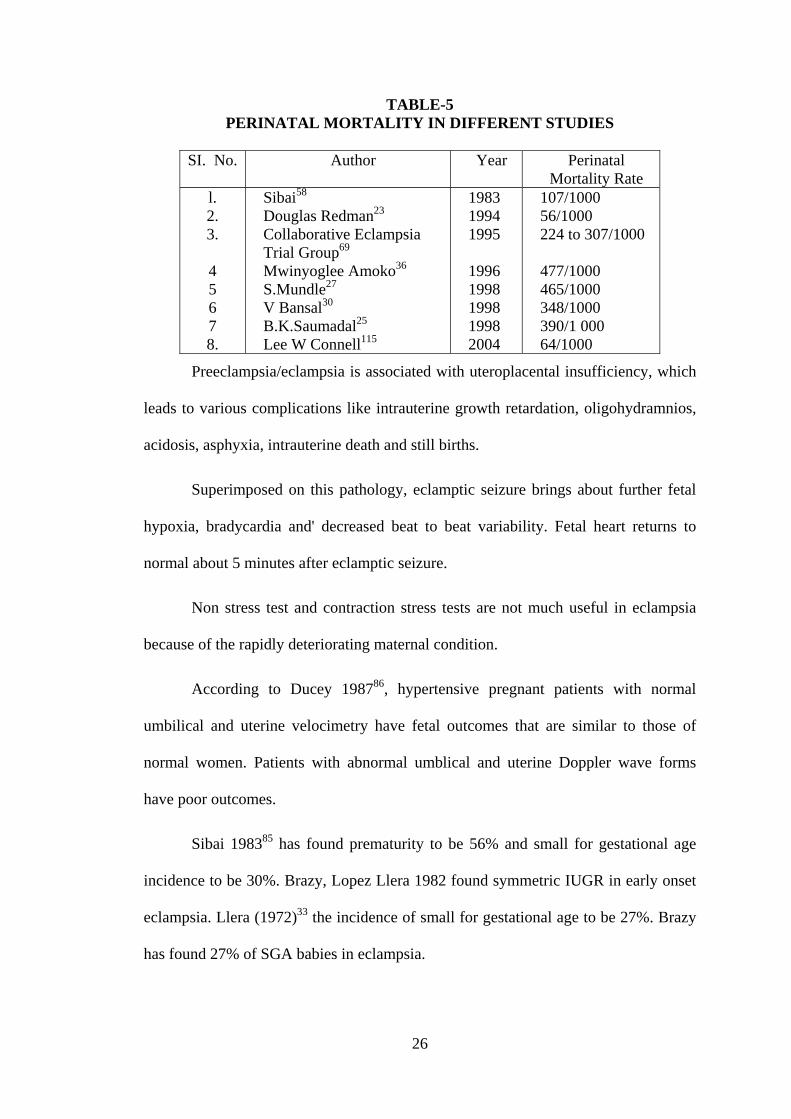
TABLE-5 PERINATAL MORTALITY IN DIFFERENT STUDIES
SI. No.
Author
Year
Perinatal
Mortality Rate l. 2. 3. 4 5 6 7 8.
Sibai58
Douglas Redman23
Collaborative Eclampsia Trial Group69
Mwinyoglee Amoko36
S.Mundle27
V Bansal30
B.K.Saumadal25
Lee W Connell115
1983 1994 1995 1996 1998 1998 1998 2004
107/1000 56/1000 224 to 307/1000 477/1000 465/1000 348/1000 390/1 000 64/1000
Preeclampsia/eclampsia is associated with uteroplacental insufficiency, which
leads to various complications like intrauterine growth retardation, oligohydramnios,
acidosis, asphyxia, intrauterine death and still births.
Superimposed on this pathology, eclamptic seizure brings about further fetal
hypoxia, bradycardia and' decreased beat to beat variability. Fetal heart returns to
normal about 5 minutes after eclamptic seizure.
Non stress test and contraction stress tests are not much useful in eclampsia
because of the rapidly deteriorating maternal condition.
According to Ducey 198786, hypertensive pregnant patients with normal
umbilical and uterine velocimetry have fetal outcomes that are similar to those of
normal women. Patients with abnormal umblical and uterine Doppler wave forms
have poor outcomes.
Sibai 198385 has found prematurity to be 56% and small for gestational age
incidence to be 30%. Brazy, Lopez Llera 1982 found symmetric IUGR in early onset
eclampsia. Llera (1972)33 the incidence of small for gestational age to be 27%. Brazy
has found 27% of SGA babies in eclampsia.

27
Low JJ 199529 reported that mean birth weight in his study was 2.328 Kgs.
The incidence of prematurity and birth asphyxia were 51.9% and 29.6% respectively.
Srividya 199824 reported 42.6% of low birth weight babies in her 1 year study
of Eclampsia where as A.K Kanhi 1998 found 49.6% of low birth weight babies in his
study.
V.Bansal 199830 has found the following complications:
Intrauterine growth retardation 48.8%
Prematurity 69%
Still birth 74%
Birth asphyxia 13.9%

28
Management of Eclampsia:
Delivery is the definitive treatment of Eclampsia. The pathological changes
disappear after delivery and eventually are reversed completely.
Pritchard has applied standardized treatment uniformly to all access of
eclampsia at Parkland Memorial Hospital since 1955 to 1975 (1975) 88. This treatment
consisted to:
1. Control of convulsions with MgSO4 7H2O using an intravenous
administered loading dose and periodic intramuscular injections
standardized in dose and frequency of administration.
2. Intermittent intravenous injection of hydrallazine to lower blood pressure
whenever diastolic blood pressure is 110 mm Hg or more.
3. Avoidance of diuretics and hyperosmolar agents
4. Limitation of intravenous fluid administration
Lot of studies have been done to determine the best drug of choice for control
of convulsions, for improving maternal and perinatal outcome. The different drugs,
which have been studied and compared are:
i) Lytic cocktail (chlorpromazine, diethazine, pethidine) (Bhalla et a1
68 Menon77 , Llewellyn Jones63 , Chatterji & Mukherji 90, Lopez
Llera ).91
ii) Diazepam, Chloridazepoxide (Lean 15, 1968; Lopez Llera, 1973)91
iii) Veratrum alkaloids (Bryant Fleming64, 1962).
iv) Frusemide, Reserpine (Lopez Llera, 1976)

29
v) Nifedipine (Bhalla et a168, 1994)
vi) Phenytoin (Eclampsia Trail Group69, 1995).
vii) Magnesium sulphate (Bryant Fleming, 196264 Zuspan , 196465
Gedekoh, 198166 Pritchard, 198450 Bhlla, 199471 Eclampsia Trial
Collaborative Group, 1994)69 to 3.4% (Zuspan64, 1964) for
magnesium sulphate.
30
Mechanism of Action of Magnesium Sulphate:
• Magnesium exerts a specific anticonvulsant action on the cerebral
cortex (Borges Gucer, 1978).
• Cotton and associates (1992) proposed that N-methyl-O aspartate
receptor is implicated in Eclampsia seizures.
• Lipton and Rosenberg (1994) attribute the anticonvulsant effects
to
• Neuronal calcium influx blocking through the glutamate channel.
• Improved mitochondrial calcium buffering.
• Potentiation of adenosine action
MANAGEMENT OF ECLAMPSIA:
I. General Management:
• Eclamptic women are ideally nursed in a dark quiet room with no
bright light
• Suctioning of oropharynx to prevent aspiration.
• Oxygen supply to prevent hypoxia.
• Facilities for endotracheal intubation and ventilation.
• Mouth kept open by a soft gag.
• Nursed in left lateral position with head low to reduce the risk of
aspiration.
II. Medical Management:
1. Anticonvulsant therapy:
Administration of magnesium sulphate as per Pritchard's regime (1975).

31
2. Antihypertensive therapy:
The objective of antihypertensive treatment is to prevent intracranial bleeding
and left ventricular failure. Immediate reduction of blood pressure is desired if
systolic blood pressure is > 170 mm of Hg and diastolic blood pressure is >110 mm of
Hg.
Hydrallazine, diazoxide, sodium nitroprusside, sublingual nifedpine are the
most common antihypertensive drugs used. Pritchard 197588 in his series of 154
patients used intravenous hydrallazine. Sublingual nifedipine is extensively used in
most developing nations including India (Bhalla 68, 1994; Hangarga US , 1998)31.
According to Donaldson (1987)57 antihypertensive treatment may be useful in
avoiding the selective cerebral arterial vasospasm that causes eclamptic seizures.
III. Obstetric Management:
Delivery is the definitive treatment of eclampsia. Pritchard (1975)88 has
incorporated delivery as the essential part of his standardized treatment. Steps were
taken to effect the delivery once the woman regained consciousness to the extent that
she could be oriented to time and space. Once convulsions had been controlled and no
other obstetric complication coexisted without obstetric contraindication to vaginal
delivery, labour was induced with intravenous oxytocin in Pritchard's series.
Dewhurst in 198497 felt that if the fetus is viable and unless the mother is
already in labour with cervix more than 3 cm dilated, early caesarean section is ideal.
But Zuspan 198198 preferred vaginal mode of delivery in view of increased maternal
morbidity for operative delivery.

32
Cunningham and Pritchard (1984) reported 75% vaginal delivery rate out of
209 women with antepartum eclampsia. The following are the incidence for vaginal
delivery given by other
Authors:
Pritchard (1975)88................96.00%
Hangarga (1998)31...............90.62%
Bansal y (1998)30 ................65.00%
The caesarean section in different studies is as follows:
Mwinyoglee Amok036 (1996) 66.70%
Bansal y30 (1998) 9.00%
Kale Y 99 (1998) 21.00%
Kahni AK24 (1998) 8.00%
The modes of induction in these studies were extra amniotic ethacrydyl lactate
instillation, intravenous oxytocin, prostaglandins, amniotomy or the combination of
the above.
The maternal and perinatal prognosis depends directly on convulsion delivery
interval and induction delivery interval (Menon71961). The longer the duration, the
worse is the prognosis (Mundle S27, 1998).
The induction delivery interval in Pritchard88 1975 study ranged between 3
and 51 hours. In a study by Hangarga31 US (1998), the mean induction delivery
interval was 15.78 hours and 80% delivered within 24 hours of admission.

33
Anaesthesia and Analgesia in Eclampsia:
For labour analgesia intravenous pethidine and intravenous phenergan at 2
hours or longer (avoided 2 hours before delivery) was used by Pritchard 88(1975) in
his study.
Anaesthesia for Caesarean Section:
Spinal blockade produces hypotension and potential for pulmonary edema
following infusion of large volumes of crystalloid solutions. General anesthesia and
tracheal intubation may result in severe sudden hypertension further complicated by
pulmonary or cerebral edema or intracranial hemorrhage. Over the past two decades,
most obstetrical anesthesiologists have to come to favour epidural blockade for labour
and caesarean section in eclampsia (Cheek & Samuels, 1001991; Chadwick &
Easterling , 1011991; Ramanathan ,102 1991).
Neonatal Complications:
Sibai103 (1983) has found that neonatal complications in eclampsia were
related to prematurity and unrelated to maternal eclamptic process. There were no
differences between premature babies of eclampsia and premature babies of control
population.
Infant Follow-up:
Long-term follow-up data 4 years of age seems favourable according to Sibai
study (1983).

34
Postpartum Care:
Consists of fluid and electrolyte balance, input, output chart, continuation of
MgSO4.H2O for 24 hours and blood pressure monitoring.
Long term prognosis:
Recurrence rate of pre-eclampsia is 30% according to Sibai. Risk of
recurrence of eclampsia is 1.4%. Most of the complications are however completely
reversible.

35
METHODLOGY
The study period extended from October 2010 to September 2011 a period of
12 months. The study was done in VIMS, Bellary.
A total of 100 patients were studied. Patients with the following criteria were
studied.
1. Primigravida
2. Duration of gestation more than 32 weeks
3. Antepartum eclampsia
Exclusion criteria
1. Patients with pregnancy induced hypertension without eclampsia,
2. Patients with epilepsy or other causes of convulsions with pregnancy.
3. Multigravida with pregnancy induced hypertension with anaemia.
4. Patients with chronic hypertension with eclampsia.
5. Patients with connective tissue disorder with eclampsia.
100 Patients were studied by delivering them into two (2) groups for
comparative analysis.
The first group consisted of patients whom conservative obstetric management
& delivey per vaginum was carried and was called the “VD group”.
The second group consisted of patient in whom lower segment cesarean
section was carried out due to eclampsia & varied associated indications was called
“C D group”.

36
METHODS
On admission a detailed history was taken regarding
1. Name, age, socioeconomic status, religion and address of the patients
2. the antenatal check-up
3. the duration of gestation in terms of months of amenorrhoea
4. The time of onset of convulsion, total number of convulsion, interval
between convulsion, duration of each convulsion, the time of case
convulsion, history of loss consciousness & history of frothing longitude,
passing urine/stood during convulsion
5. Premonitory symptoms like headache epigastric pain nausea, vomiting and
blurred vision.
6. Any history pain abdomen trauma pervaginal leak or bleeding pervaginal.
7. Obstetric menstrual, past history, family history and personal history
8. Any nature of treatment before hospitalization
A rapid general examination was subsequently made noting the grade of
consciousness of patients, temperature, pulse rate blood pressure, presence
of edema, evidence of injuries, condition of heart, lungs & knee jerk
The second group consisted of patients in whom lower segment caesarean
section was carried out due to eclampsia and varied associated indications and was
called the "C.D. group".

37
Methods:
On admission, a detailed history was taken regarding:
1. The name, age, socioeconomic status, religion and address of the patient.
2. The antenatal checkups.
3. The duration of gestation in terms of months of amenorrhea.
4. The time of onset of convulsion, total number of convulsions, interval
between convulsions, duration of each convulsion, the time of last convulsion, history
of loss of consciousness and history of frothing, tongue bite, passing urine/ stools
during the convulsions.
5. Premonitory symptoms like headache, epigastric pain, nausea, vomiting and
blurred vision.
6. Any history of pain abdomen, trauma, per vaginal leak or bleeding
7. Obstetric, menstrual, past, family and personal history
8. Any nature of treatment taken before hospitalization.
A rapid general examination was subsequently made noting the grade of
consciousness of the patient, temperature, pulse rate, respiratory rate, blood pressure,
presence of edema, evidence of tongue bite, condition of the heart, state of the lungs
and knee jerk.
A detailed obstetric examination was conducted noting the height of the
uterus, presence, frequency and duration of uterine contraction, lie and presentation of
the fetus, relation of the presenting part to the brim and the rate and regularity of the
fetal heart.
Vaginal examination was done and the condition of the cervix - position,
consistency, dilatation, effacement and station of the presenting part i.e., Bishop's
score was noted. Presence of bag of membrane and adequacy of the pelvis was also

38
noted.
Bladder was catheterized and urine output was noted.
IV line was started and 1 pint of Ringer lactate was given for hydration.
Investigations were sent for complete hemogram, urine analysis, blood
grouping and Rh-typing, renal and liver function tests and coagulation profile.
Medical Management:
1. Anticonvulsants:
Magnesium sulphate as per single dose regime on admission, loading dose
4gm of MgSO4 (MgS04.7H20) as a 20% solution was given intravenously at the rate
of 1 gm per minute followed by 4gms of 50% MgS04 2 gm was injected deeply in the
upper outer quadrant of one buttock and another half (2gm) injected similarly in the
other buttock with a 3 inch long 20 gauge needle.
If the patient has recurrence then Pritchard’s regime was followed, 2gms of
50% MgS04 solution to each buttock was injected as above.
Maintenance dose: Every 4 hours thereafter, 5 g of 50% solution of MgS04 was given
in alternate buttocks but only after ascertaining the following:
a) The patellar reflex is present
b) Respiratory rate is more than 14/ minute
c) Urine output in the previous 4 hours was 100 ml or more
This was continued for 24 hours after delivery.
2. Antihypertensive; Nifedipine 10 mg
On admission, if diastolic blood pressure was more than 110 mm Hg,

39
nifedipine 10 mg was given orally. Thereafter, the dose was titrated as per blood
pressure response.
Labetolol, if diastolic blood pressure was more than 110 mm of Hg inj.
labetolol 20mg IV bolus is given. If blood pressure is not decreased to desirable level
in 10 minutes then 20mg, 40 mg upto 220mg is given
3. Antibiotics were given stat and continued for an average of 1 week.
Obstetric Management:
Due consideration was given to:
1. Age of the patient
2. Gestational age
3. Whether the patient was in labour or not
4. Rate and regularity of fetal heart
5. Bishop's score
Then, either induction was done with pervaginal misoprostol or dinoprostone
gel following conservative obstetric management or were taken up for caesarean
section directly with unfavourable cervix as the associated indication. Patients who
delivered per vaginum following successful induction (if not in labour), with
prostoglandins patients who were in labour (augmented with ARM or pitocin or both)
who also delivered per vaginum and those who were fully dilated and effaced on
admission and went for spontaneous delivery/outlet forceps, were all included under
the "V.D. group".
Caesarean section was also done in those cases wherein induction failed or
other varied associated obstetric indications were present. Thus, all the patients where
in caesarean section was done were included in the "C.D. group".

40
The associated indication for caesarean, induction delivery interval in induced
vaginal deliveries, total blood loss and intraoperative/intrapartum complications if any
were noted. Baby notes were noted.
Follow up : The mother and the neonate were followed till discharge at
hospital and then details noted in the proforma.

41
OBSERVATIONS
TABLE-6 AGE-WISE DISTRIBUTION OF STUDY SUBJECTS
Delivery Total Age group
Caesarean Vaginal
Up to 20 years 19 (46.3%) 24 (40.7%) 43 (43%)
21 – 24 years 20 (48.8%) 27 (45.8%) 47 (47%)
More than 24 years 02 (4.9%) 08 (13.6%) 10 (10%)
Total 41 (100%) 59 (100%) 100 (100%)
Chi-square – 2.05 df-2 p value – 0.35
Incidence of eclampsia found be high in primigravida between 21-24 years.
1. Age wise distribution
46.30% 48.80%
4.90%
40.70%45.80%
13.60%
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00%
upto 20 yrs 21 - 24 yrs > 24 yrs Age group
Ceaserean Vaginal

42
TABLE.7 RELIGION-WISE DISTRIBUTION OF STUDY SUBJECTS
Delivery Age group
Caesarean Vaginal
Total
Hindu 37 (90.2%) 51 (86.4%) 88 (88%)
Muslims 03 (7.3%) 08 (13.6%) 11 (11%)
Christian 01 (2.4%) 00 01 (01%)
Total 41 (100%) 59 (100%) 100 (100%)
Chi-square – 2.33 df-2 p value – 0.31
In my study Hindus were affected when other groups.
2. Religion wise distribution
90.20%
7.30%
2.40%
86.40%
13.60%
0.00%
0.00% 10.00 %
20.00%
30.00%
40.00%
50.00%
60.00%
70.00 %
80.00 %
90.00 %
100.00%
Hindu
Muslims
christian
Religion
Ceaserean Vaginal

43
TABLE-8 RELATION BETWEEN NUMBER OF CONVULSIONS AND MODE OF
DELIVERY
Delivery Convulsions
Caesarean Vaginal
Total
1 -3 34 (82.9%) 49 (83.1%) 83 (83%)
4 – 6 06 (14.6%) 10 (16.9%) 16 (16%)
More than 6 01 (2.4%) 00 01 (01%)
Total 41 (100%) 59 (100%) 100 (100%)
Chi-square – 1.52 df-2 p value – 0.46 p value insignificant
0.00% 20.00% 40.00% 60.00% 80.00%
100.00%
1 to 3 4 to 6 >6 Covulsions
3. Relation b/w no. of convulsions and mode of delivery
Ceaserean Vaginal

44
TABLE-9 RELATION BETWEEN CONSCIOUSNESS B/W CONVULSIONS AND
MODE OF DELIVERY
Delivery Consciousness
Caesarean Vaginal
Total
Yes 40 (97.6%) 57 (96.6%) 97 (97%)
No 01 (2.4%) 02 (3.4%) 03 (03%)
Total 41 (100%) 59 (100%) 100 (100%)
Fischer exact test p value – 0.46
97.60%
2.40%
96.60%
3.40%
0.00%
20.00%
40.00%
60.00%
80.00%
100.00%
Ceaserean Vaginal
Mode of delivery
4. Relation b/w consciousness and mode of delivery
YesNo

45
TABLE-10 RELATION BETWEEN ANTE NATAL CHECKUP AND MODE OF
DELIVERY
Delivery ANC
Caesarean Vaginal
Total
Yes 26 (63.4%) 36 (61%) 38 (38%)
No 15 (36.6%) 23 (39%) 62 (62%)
Total 41 (100%) 59 (100%) 100 (100%)
Chi-square – 0.05 df-1 p value – 0.80
TABLE-11 RELATION BETWEEN PATIENT GENERAL CONDITION AND MODE OF
DELIVERY
Delivery Patient condition
Caesarean Vaginal
Total
Conscious 33 (80.5%) 47 (79.7%) 80 (80%)
Irritable 07 (17.1%) 06 (10.2%) 13 (13%)
Un conscious 01 (2.4%) 06 (10.2%) 07 (07%)
Total 41 (100%) 59 (100%) 100 (100%)
Chi-square – 2.95 df-2 p value – 0.22
80.50%79.70%
17.10%10.20%
2.40% 10.20%
0.00% 20.00% 40.00% 60.00% 80.00%
100.00%
Conscious Irritable Unconscious
5. General condition and mode of delivery
Ceaserean Vaginal

46
TABLE-12 RELATION BETWEEN CONJUNCTIVA STATUS AND MODE OF
DELIVERY
Delivery Conjunctiva
Caesarean Vaginal
Total
Pink 36 (87.8%) 59 (100%) 95 (95%)
Pale 05 (12.2%) 00 05 (05%)
Total 41 (100%) 59 (100%) 100 (100%)
Fischer exact test p value – 0.01
TABLE-13 RELATION BETWEEN TONGUE CONDITION AND MODE OF DELIVERY
Delivery Tongue
Caesarean Vaginal
Total
Pink 30 (73.2%) 46 (78%) 76 (76%)
Pale 01 (2.4%) 01 (1.7%) 02 (02%)
Bite 10 (24.4%) 12 (20.3%) 22 (22%)
Total 41 (100%) 59 (100%) 100 (100%)
Chi-square – 0.32 df-2 p value – 0.85
6. Distribution of study subjects based on tongue status
Pink76%
Pale2%
Bite22%

47
TABLE-14 MODE OF DELIVERY
Mode of delivery Frequency Percentage
CD 41 41%
VD 59 59%
Total 100 100%
Incidence of vaginal delivery is 59% caesarean section is 41%.
7. Mode of delivery
41%
59%
0% 10% 20% 30% 40% 50% 60% 70%
CD
VD

48
TABLE-15 RELATION BETWEEN GESTATIONAL AGE AND MODE OF DELIVERY
Delivery Gestational age
Caesarean Vaginal
Total
32 – 34 weeks 01 (2.4%) 17 (28.8%) 18 (18%)
34 – 36 weeks 03 (7.3%) 06 (10.2%) 09 (09%)
36 – 40 weeks 37 (90.2%) 36 (61.0%) 73 (73%)
Total 41 (100%) 59 (100%) 100 (100%)
Chi-square – 12.39 df-2 p value – 0.00
8. GESTATIONAL AGE AND MODE OF DELIVERY
0
5
10
15
20
25
30
35
40
32 34 wk 34 ‐ 36 wk 36 ‐ 40 wk
Caesarean
Vaginal
It was found that there was increase in evidence of antepartum eclampsia with increase in gestational age the maximum incidence being 36 – 40 weeks in both the groups.

49
TABLE-16 INDICATIONS FOR CAESAREAN SECTION
Indications Frequency Percentage
Cervical factors
Unfavourable cervix
Failure to progress
Cervical dystocia
11
20
02
26.8%
48.8%
04.9%
Fetal distress
CPD
06
02
14.6%
04.9%
Total 41 100%
Failure to progress induction topped the list for caesarean section. Next common indication is fetal distress.
26.80%
48.80%
4.90%
14.60%
4.90% 0.00%
10.00% 20.00% 30.00% 40.00% 50.00%
Unfavourablecervix
Failure toprogress
Cervicaldystocia
Fetal distress CPD
Indications
16 Indications for caeserean section

50
TABLE-17 INCIDENCE OF IUD’S ON ADMISSION
VD group CD group Total FHR
No. of cases % No. of cases % No. of cases %
Present 58 98.3 41 100% 99 99%
Absent 1 1.7 _ _ 1 1%
Total 59 100 41 100% 100 100%
Fischer exact test p value – 1.00 P value is insignificant on admission There was no IUD’s in CD group only one VD group.
TABLE-18 RELATION BETWEEN MODIFIED BISHOP SCORE FINDING AND MODE
OF DELIVERY
Delivery Bishop score
Caesarean Vaginal
Total
0 11 (26.8%) 12 (20.3%) 23 (23%)
2 13 (31.7%) 15 (25.4%) 28 (28%)
3 06 (14.6%) 08 (13.6%) 14 (14%)
4 11 (26.8%) 23 (39%) 34 (34%)
5 00 01 (1.7%) 01 (01%)
Total 41 (100%) 59 (100%) 100 (100%)
Chi-square – 42.55 df-4 p value – 0.63
P value is insignificant, Bishop’s score was unfavourable in all most all cases.

51
TABLE-19 BISHOP’S CERVICAL SCORING SYSTEM
Factors 0 1 2 3
Dilatation of cervix < 1cm 1-2 cm 2-4 cm > 4 cm
Length of cervix 4 cm 2-4 cm 1-2 cm < 1 cm
Consistency Firm average Soft
Position posterior Mid anterior
Station of presenting part -3 -2 -1/0 +1,+2
Bishop’s score was unfavourable in 90% of the cases in.
In CD group, Bishop’s score was 0.
In VD group also, Bishop’s score was 0 but vaginal delivery was opted.
Incidence of operative vaginal delivery
Outlet forceps was applied in all cases of 36-40 weeks gestation and ventouse was
applied in one case in vaginal delivery group.
Indications for application of forceps:
1. To cut short second stage of labour .
2. Fetal distress.
Indication for application of ventouse:
Poor maternal efforts.
Incidence of induced vaginal delivery
95% of cases who delivered vaginally were either not in labour or in latent phase of
labour. Those patients are induced with prostaglandins, that is misoprostol tablets and
dinoprostone gel.
TABLE-20

52
CONVULSION- DELIVERY INTERVAL
VD group CD group Convulsion-delivery interval
No. of cases % No. of cases %
0-6 hrs 2 3.4 6 14.6
6-12 hrs 18 30.5 11 26.8
12-18 hrs 20 32.2 11 26.8
18-24 hrs 12 20.3 9 21.9
>24 hrs 8 13.6 4 9.9
Total 59 100 41 100
P value 0.34 insignificant
Net convulsion delivery interval was less than 6 hrs in13.15% of cases in CD group
and 3.22% of cases in VD group.
70% of the cases CD group delivered within 18 hours of the first convulsion
TABLE-21
INDUCTION-DELIVERY INTERVAL
VD group Induction delivery interval
No. of cases %
0-6 hrs 1 1.5%
6-12 hrs 34 54.8%
12-18 hrs 20 32.3%
18-24 hrs 2 3.2%
> 24 hrs 2 3.2%
Perinatal outcome
VD group: No. of cases were 59 and no. of babies were 58
CD group: No. of cases were 41 and no. of babies were 41

53
TABLE-22 PERINATAL MORBIDITY
VD group CD group P value Perinatal outcome
No. of cases % No. of cases %
Apgar < 5 at 1 min. 15 25.5 4 9.7 0.04
Need for resuscitation 8 13.5 2 4.9 0.19
Need for NICU 19 32.2 9 21.9 0.26
Mean duration of stay in NICU in CD group 5.78 days
Mean duration of stay in VD group 3 days
P value 3.8
Apgar < 5 at 1 min. p value significant
25.40%
9.70%13.50%
4.90%
32.20%
21.90%
0.00% 5.00%
10.00% 15.00% 20.00% 25.00% 30.00% 35.00%
APGAR < 5 at ! Min Need for resuciation need for NICU
10. Perinatal morbidity
VD CD

54
TABLE-23 COMPARISON OF BIRTH WEIGHT, APGAR SCORE AND NICU STAY
Delivery Parameters
Caesarean (mean+/-sd) Vaginal (mean+/-sd)
P value *
Birth weight (Kgs) 2.51 +/- 0.44 2.03 +/- 0.42 0.00
APGAR score 1 min 5.8 +/- 0.6 5.3 +/- 1.4 0.03
APGAR score 5 min 7.7 +/-0.9 7.1 +/-1.6 0.02
NICU stay (days) 5.78 +/- 0.85 3.00 +/- 1.37 0.16
* student‘t’ test
Birth weight of babies, Apgar score at 1minute & 5 minute was more in CD group than vaginal group
11. Birth weight of babies
2.51
2.03
0 0.5 1 1.5 2 2.5 3
Ceaserean
VaginalMode of delivery
Kgs
5.8 5.3
7.77.1
0
2
4
6
8
Score
At 1 min At 5 min
Time
12. APGAR score
Ceaserean Vaginal

55
TABLE-24 PERINATAL MORTALITY
VD group CD group Perinatal outcome
No. of cases % No. of cases %
Live births 46/59 78 38/41 92.68
Still births 5/59 8.4 _ _
NND 7/59 11.4 3 7.3
IUD an admission 1/59 1.7 100
Corrected perinatal mortality was 7.35% in CD group than 18.6% vaginal group.
13. Perinatal outcome
78% 92.60%
8.40% 0%
11.40% 7.30% 1.70% 0%0%
20% 40% 60% 80%
100%
VD CD Delivery
Live births Still births NND IUD

56
TABLE-25 ANALYSIS OF CAUSES OF PERINATAL MORTALITY WITH
GESTATIONAL AGE >32 WEEKS
VD group CD group P value Cause
No. of cases % No. of cases %
H I E 5 8.5 1 2.4 0.39
Septicemia 1 1.7 _ _
RDS 1 1.7 _ _
MAS 1 1.7 2 4.8 0.56
In CD group PNM was due to MAS in VD group HIE is commonest cause
P value is insignificant
8.50%
1.70%1.70%1.70%2.40%
0.00%0.00%
5%
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
VD CD
14. Causes of perinatal mortality with gestational age > 32 weeks
HIE Septicemia RDS MAS

57
TABLE-26 COMPARISON OF PNM WITH RESPECT TO GA (EXCLUDING IUDS)
VD group CD group P value Gestational
No. of
cases
PNM % No. of
cases
PNM %
32-34 17 5 29.2 1 _ _
34-36 7 4 57.2 3 _ _
36-40 35 3 8.6 37 3 8.10
Total 59 12 13.5 41 8.10 0.51
For both gestational ages between 36-40 PNM was lesser in CD group P value is insignificant
29%
57.20%
8.50%0.00% 0%
8.82%
0% 10% 20% 30% 40% 50% 60%
VD CD
Delivery
15. Relation of PNM with respect to gestational age
32 - 34 weeks 34 - 36 weeks 36 - 40 weeks

58
TABLE-27 COMPARISON OF PNM WITH RESPECT TO BIRTH WEIGHT
VD group CD group P value Birth weight
(KGs) No. of cases PNM % No. of cases PNM %
1.5-2 40 7 11.8 11 1 9.9 1.00
2-2.5 16 4 6.77 15 1 6.6 1.00
2.5-3 2 1 50 15 1 6.7 0.22
3-3.5 1
>3.5
Total 59 12 18.5 41 3 7.3
For all birth weights PNM was lesser CD group
P value is insignificant
12% 6.77%
50.00%
0.00%0%
9.90%7%6.60%0% 0%
0% 10% 20% 30% 40% 50%
VD CD
Delivery
16. Relation between PNM and Birth weight
1.5 - 2.0 Kgs 2.0 - 2.5 kgs 2.5 - 3.0 Kgs 3.0 - 3.5 Kgs > 3.5 Kgs
59
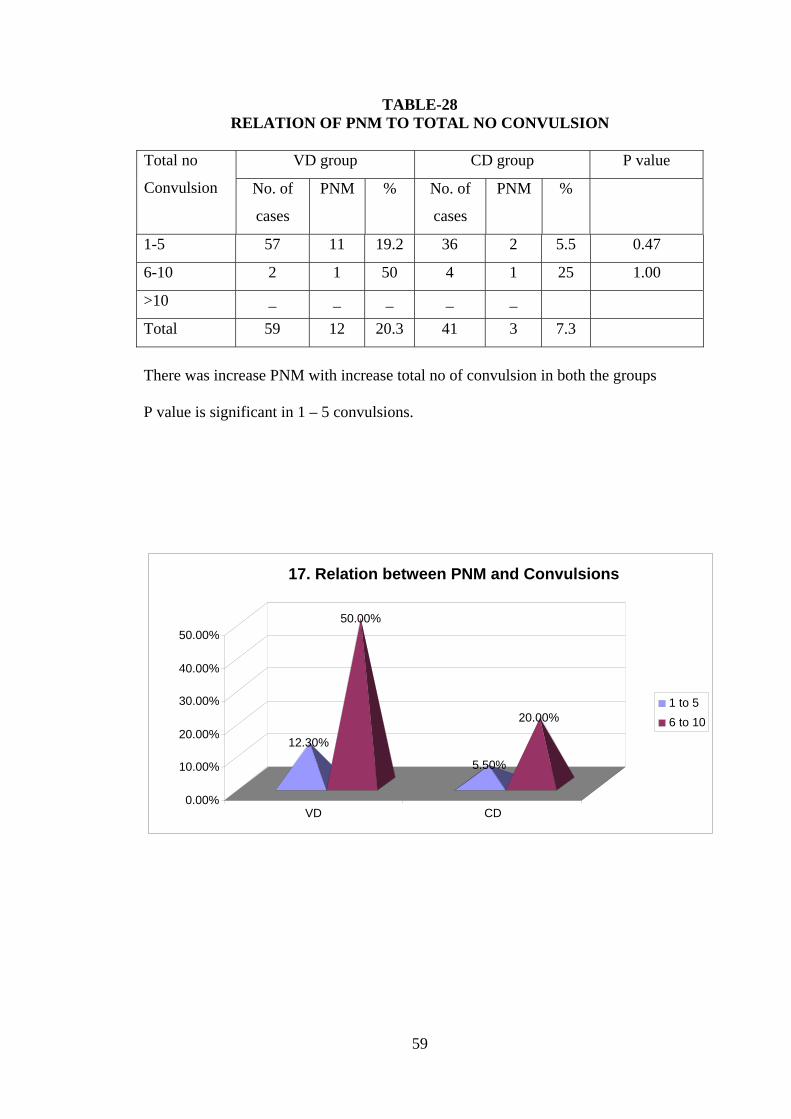
TABLE-28 RELATION OF PNM TO TOTAL NO CONVULSION
VD group CD group P value Total no
Convulsion No. of
cases
PNM % No. of
cases
PNM %
1-5 57 11 19.2 36 2 5.5 0.47
6-10 2 1 50 4 1 25 1.00
>10 _ _ _ _ _
Total 59 12 20.3 41 3 7.3
There was increase PNM with increase total no of convulsion in both the groups
P value is significant in 1 – 5 convulsions.
12.30%
50.00%
5.50%
20.00%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
VD CD
17. Relation between PNM and Convulsions
1 to 56 to 10

60
TABLE-29 MATERNAL COMPLICATIONS
Delivery Maternal complications
Caesarean Vaginal
Total
Pulmonary edema 01 (2.4%) 01 (17.0%) 02 (02%)
Placental abruption/HELLP 00 03 (5.1%) 03 (03%)
UTI 03 (7.2%) 00 03 (03%)
PPH 01 (2.4%) 01 (1.7%) 02 (02%)
Cerebral infarction 01 (2.4%) 01 (1.7%) 01 (01%)
Cortical Blindness 01 (2.4%) 01 (1.7%) 02 (02%)
Nil 35 (84.0%) 52 (88.4%) 87 (87%)
Total 41 (100%) 59 (100%) 100
(100%)
Chi-square – 7.32 df-6 p value – 0.29
There was progressive increase in maternal morbidity with increase in induction
delivery interval.

61
TABLE-30 RELATION MATERNAL COMPLICATIONS TO CONVULSION DELIVERY
INTERVAL
VD group CD group P value Time
interval in
hours
No
of
cases
With
complications
% No of
cases
With
complications
%
0-6 04 1 25 5 1 20 1
6-12 32 2 6.2 13 2 15.4 0.56
12-18 19 2 10.52 10 2 20 1
18-24 2 2 100 8 1 12.5 0.01
>24 2 5
P value is significant in 18-24 time interval in hours
There was progressive increase in incidence of maternal complication with increase in
convulsion delivery interval in both the groups. The incidence of maternal
complication was found to be higher in VD group.
25.00%20.00%6.20%
15.40% 15.80%20%
100.00%
12.50%
0.00% 20.00% 40.00% 60.00% 80.00%
100.00%
0 to 6 6 to 12 12 to 18 18 to 24 Time interval (hours)
19. Relation between maternal complications and convulsion delivery interval
VD CD

62
TABLE-31 RELATION MATERNAL COMPLICATIONS TO INDUCTION DELIVERY
INTERVAL
Time interval in hours
No of cases No of cases With
complications
%
0-6 10 1 7.1
6-12 14 1 7.1
12-18 10 2 20
18-24 2 2 20
>24 2
TABLE.32 MATERNAL MORTALITY AND MODE OF DELIVERY
Delivery Maternal mortality
CD VD
Total
Yes 00 01 (1.7%) 01 (1%)
No 41(100%) 58 (98.3%) 99 (99%)
Total 41(100%) 59 (100%) 100
(100%)
There was no maternal death in CD group, 1 in VD group
0%
100%
1.70%
98.30%
0%
20%40%60%80%
100%
Maternal mortality
CD VD
Delivery
20. Maternal mortality and mode of delivery
Yes No

63
TABLE-33 RELATION BETWEEN CESSATION OF PROTEINURIA AND MODE OF
DELIVERY
Delivery Proteinuria nil
Caesarean Vaginal
Total
Day 1 09 (22%) 20 (33.9%) 29 (29%)
Day 2 17 (40.8%) 19 (32.2%) 36 (36%)
Day 3 12 (29.6%) 16 (27.1%) 28 (28%)
Day 4 03 (7.6%) 04 (6.8%) 07 (07%)
Total 41 (100%) 59 (100%) 100 (100%)
Chi-square – 1.81 df-3 p value – 0.61
Cesasation of proteinuria early in vaginal group then CD group
TABLE-34 COMPARISON OF TIME BETWEEN EVENTS
Delivery Time (hours)
Caesarean (mean+/-sd) Vaginal (mean+/-sd)
P value *
Admission – convulsions 5.24 +/- 2.36 5.5 +/- 2.4 0.60
Convulsions - delivery 17.3 +/- 7.0 17.0 +/- 5.5 0.84
Admission - delivery 14.2 +/-9.0 13.0 +/-9.1 0.52
* student‘t’ test
TABLE-35 COMPARISON BLOOD PRESSURE
Delivery Blood pressure
Caesarean (mean+/-sd) Vaginal (mean+/-sd)
P value *
SBP (admission) 159.27 +/- 16.15 152.75 +/- 13.35 0.03
SBP (delivery) 139.46 +/- 16.24 136.78 +/- 15.42 0.40
DBP (admission) 104.88 +/- 14.98 102.58 +/- 13.03 0.41
DBP (delivery) 92.20 +/- 7.89 92.03 +/- 7.61 0.91
* student ‘t’ test

64
TABLE-36 COMPARISON BLOOD PRESSURE DURING ADMISSION AND DELIVERY
Blood pressure Mean +/- sd P value*
SBP
Admission
Delivery
155.42 +/- 14.8
137.88 +/- 15.7
0.00
DBP
Admission
Delivery
103.52 +/- 13.83
92.10 +/- 7.56
0.00
*Paired ‘t’ test
21. Systolic Blood Pressure during admission and delivery
159.27
139.46
152.75
136.78
125 130 135 140 145 150 155 160 165
SBP(admission) SBP(delivery)
Mean (mmHg)
Ceaserean Vaginal
104.88102.58
92.2 92.03
85
90
95
100
105
Mean(mmHg)
DBP(admission) DBP(delivery)
22. Diastolic Blood pressure among study subjects
Ceaserean Vaginal
65
DISCUSSION
Eclampsia a dreaded complication in pregnancy is still associated with a great
deal of maternal and fetal loss.Some decades ago the conventional treatment of
eclampsia was conservative approach, with the use of sedatives anticonvulsants and
antihypertensives to be followed by induction or stimulation of labour after the fits are
controlled.
Caesarean section was considered to be extremely risky procedure and
reserved for highly selected cases.
Now in twenty first century with advancement in the field of anesthesiology
caesarean section in eclampsia is no more risky and promises reassuring maternal and
perinatal outcome.
In the present series 100 primigravidae with more than 32weeks gestation with
antepartum eclampsia were studied.
1. VD group where vaginal delivery was done.
2. CD group where caesarean section was performed.
Comparative incidence of CD vs VD Incidence of caesarean section was 41% and that of vaginal delivery was 59%.
This was comparable with study of MarioLopezllera series,out of 107 cases the
incidence of caesarean section was 40.4% .the incidence quoted by other authors are
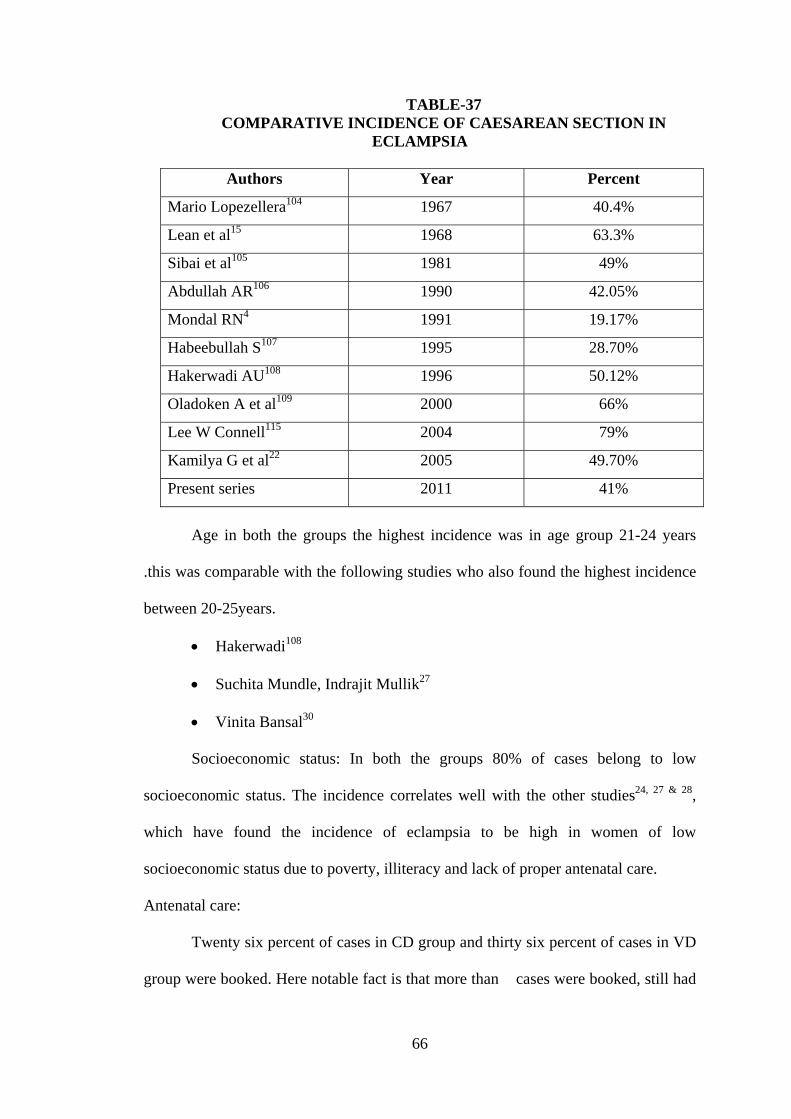
66
TABLE-37 COMPARATIVE INCIDENCE OF CAESAREAN SECTION IN
ECLAMPSIA
Authors Year Percent
Mario Lopezellera104 1967 40.4%
Lean et al15 1968 63.3%
Sibai et al105 1981 49%
Abdullah AR106 1990 42.05%
Mondal RN4 1991 19.17%
Habeebullah S107 1995 28.70%
Hakerwadi AU108 1996 50.12%
Oladoken A et al109 2000 66%
Lee W Connell115 2004 79%
Kamilya G et al22 2005 49.70%
Present series 2011 41%
Age in both the groups the highest incidence was in age group 21-24 years
.this was comparable with the following studies who also found the highest incidence
between 20-25years.
• Hakerwadi108
• Suchita Mundle, Indrajit Mullik27
• Vinita Bansal30
Socioeconomic status: In both the groups 80% of cases belong to low
socioeconomic status. The incidence correlates well with the other studies24, 27 & 28,
which have found the incidence of eclampsia to be high in women of low
socioeconomic status due to poverty, illiteracy and lack of proper antenatal care.
Antenatal care:
Twenty six percent of cases in CD group and thirty six percent of cases in VD
group were booked. Here notable fact is that more than cases were booked, still had

67
eclamptic seizure. This was because in few cases there was no mid trimester fall of
blood pressure and this was overlooked by attending doctor. Infrequent antenatal
visits and refusal to get admitted when advised were instrumental in causing
eclampsia in these cases.
Gestational age:
The highest incidence was found between 36-40weeks. 90.2% in CD group
and 61.0% in VD group. Most studies found that the incidence to be high when the
age is less than 37weeks.
Low JJ33 found maximum incidence between 33-37 weeks (60%).
Mundle S27 found maximum incidence between 29-36weeks (70%).
Most of the referrals constituted term gestation with viable fetus and poor cervical
scores.
After 32weeks gestation - out of 100cases 59 were delivered vaginally because
• 1 was IUD
• 23 were preterm
• 25 were induced
• 10 cases did not give consen.
Condition at admission:
Most of the patients were admitted in a compromised state after throwing a
number of convulsions at home. However almost 80% of the cases in both the groups
had thrown less than 4 convulsions. None of cases in both the groups had more than
six convulsions. Most of them were conscious on admission. All three signs of
toxemia were seen in 78% of cases.
Bishop score on admission:

68
It was unfavourable in 72.5% of cases in CD group and 78% of cases in VD
group. All these 78% group who were otherwise not ideal candidates for vaginal
delivery were allowed to deliver vaginally either because of poor expectancy of fetal
salvage or refusal for caesarean section by the patient’s attender in view of poor fetal
salvage. To be more precise 59 cases with unfavourable cervix who were allowed
vaginal delivery one was IUD, 23 were preterm, 10 cases did not give consent.
Zuspan FP111 asserted that condition of cervix is a fetal prognostic indicator
and presents the obstetrician with the challenge as to how, when and what means of
delivery are most appropriate for best results.
Indications for caesarean section:
Eleven cases were operated for unfavourable cervix, cervical factors top the
list of indications for caesarean section 30. Next commonest indication was fetal
distress accounting for 6 cases.
In Mondal RN series4, 41 out of 62 cases (62.12%) CD was a deliberate
decision with the sole purpose of shortening the exposure to delivery.
Hakerwadi AV108 quoted fetal distess 36.18% of section patients followed by
failed induction in 20.6%.
Habebullah107 quoted fetal distress 34.7% of CD.
Incidence of operative vaginal delivery:
Outlet forceps was applied in almost all cases the commonest indication being
cut short second stage of labour followed by fetal distress. Ventouse was applied in
one case due to poor maternal efforts.
Induction delivery interval:
All the cases with VD were induced of which required more than twelve hours
for delivery.

69
Perinatal Mortality:
The incidence in the C.D. and V.D. group of live births was 92.3 and 73%
respectively, of still births was nil and 11.8% respectively and that of neonatal deaths
was 7.3% and 8.4% respectively. The striking difference in the incidence of live birth
and still births in the two groups could be partly attributed to the comparatively
increased rates of, low birth weight and preterm babies in the V.D. group. However,
still the difference was considerable. The corrected PNM figures in the C.D. and V.D.
groups were 7.3% and 18.6% respectively. This was comparable with Dandekar
LM113 series (1992).

70
TABLE-38 COMPARATIVE INCIDENCE OF PNM TO MODE OF DELIVERY
Authors Year PNM in CD VD
Derek Crichton
Morris11
1968 21.6% 45.70%
Dandekar L M112 1992 10% 40%
Taj116 2004 7% 12%
Present Series 2011 7.3% 18.6%
Comparison of Causes of PNM:
Between 32- 34 Weeks: In the C.D. group, there was 1 case no deaths. In the V.D.
group, out of 17 cases 7 had perinatal deaths, the predominant causes being
intrauterine hypoxia (where FHR was lost during the process of induction, and birth
asphyxia) resulting in fresh still births, accounting for 11.8% of the total deaths).
After 34 Weeks:, There were 3 perinatal deaths in the C.D. group of which 2 were
due to meconium aspiration syndrome and 1 each due to birth asphyxia and
intrauterine hypoxia. 4 of these had their C-D intervals more than 16 hours. Only 1
case had C-D interval of 8 hours but however it was a case of failed induction with
fetal distress. In the V.D. group, intrauterine hypoxia was the predominant cause
(13.4%).
Comparison of PNM with respect to gestational age (excluding IUDs): For all
gestational age, PNM was found to be lesser in the C.D. group, when compared with
the V.D. group.

71
In the V.D. group: There were 12 perinatal deaths of which:
• 24 were between 32 to 36 weeks, but were preterm IUGRs with poor fetal
expectancy and so were let to deliver vaginally, as a result of which, , 4 were fresh
stillbirths and 5 were neonatal deaths.
• 35 were more than 36 weeks gestation and were opted for vaginal delivery because
patients opted for vaginal delivery ,out of which 1 was fresh still birth 2 were
neonatal deaths, .
In the C.D. group: Of the 3 neonatal deaths, 1 was born in a bad state due to birth
asphyxia with and the other 2 were due to fetal distress (MAS).
Comparison of PNM with respect to birth weight (excluding IUDs):
For all birth weights, PNM was found to be lesser in the C.D. group, except 2 cases;
one baby 2kgs which was delivered by caesarean section when 11 hours of induction
failed and another baby of 2.5kgs, 2.7Kgs where caesarean section was done for failed
induction and fetal distress. Both the babies died in postnatal period.
In the V.D. group:
• Of the 40 babies between 1.5 to 2 Kgs,4 were stillborn due to birth asphyxia and 2
had neonatal death due to respiratory distress syndrome & HIE – they were let to
deliver vaginally as they were preterm babies.
• 16 babies between 2 to 2.5kgs were induced except 1 where consent for surgery was
not given – as a result, 3 were fresh stillborn and 2 had neonatal deaths.
• One baby of 2.5-3Kgs 1 was neonatal death. In the C.D. group: One baby died with birth weight 2.5kgs due to HIE.
72
• Two babies with birth weights 2.2 and 2.5kgs respectively had neonatal deaths due
to meconium aspiration syndrome, both the babies being taken for caesarean section
with fetal distress in utero.
Factors affecting PNM:
1. Number of convulsions: PNM increased in proportion to increase in the number of
convulsions. Similar finding was observed by Mundle S27. (1998) and Swain S20
(1993). Dutta DC1 quotes bad prognosis for mother and fetus if number of
convulsions are more than 10.
2. Induction delivery interval: PNM increased progressively with increase in the
induction delivery interval beyond 24 hours. Nanda S19 (1989) also asserted that
increased induction delivery interval is associated with adverse perinatal outcome
because of increased duration
of exposure to fetal asphyxia.
3. Convulsion delivery interval: PNM also increased proportionately as the first
convulsion-delivery interval increased in both the groups. Similar finding was
observed by Lopezllera et al104 (1967), Nanda Smiti19 (1989) and Swain S20
(1993).73.

73
TABLE-39 COMPARATIVE STUDY OF PNM TO CONVULSION-DELIVERY
INTERVAL IN LOPEZLLERA SERIES104 (1967)
Convulsion – delivery interval hours PNM %
< 6 Hours 14%
6 – 12 Hours 19%
12 – 24 Hours 62%
> 24 Hours 53%
4. Time when caesarean section was performed: PNM was decreased when
caesarean section was performed within 6 hours and was when
performed after 6 hours of admission. So, early decision for caesarean
section when delivery is not anticipated within 6 hours of admission helps
in improving fetal outcome.
Maternal Outcome:
Maternal Complications:
Maternal complications were encountered in 14% of the cases in the C.D. group and
27.2% of the cases in the V.D. group. The complications were:
1. Postpartum hemorrhage was seen in 1.75% of the cases in the V.D. group,
all of which were controlled with oxytocin and carboprost .two bottles of blood was
transfused.on the other hand one case in CD group had postpartum haemorrhage.
intraoperatively but was controlled with B-lynch sutures.
2. Abruptio placenta was seen in 5.1% of the cases in the V.D. group.
However, they improved after component therapy. Hakerwadi AV108 (1995) quoted an
incidence of 19.6% and Sibai et. al.,38 (1993) quoted an incidence of 20% in
eclampsia.

74
3.Cerebral infarction: One case in the C.D. group, on third postoperative day
developed cerebral infarction in occipitoparietal region. Other case in VD group on
4th postnatal day developed cerebral infarction. Both the patients recovered
uneventfully with conservative treatment.
Los Angeles Country study84 (1983) found a case fatality rate of 10.4% for cerebral
infarction in eclampsia.
4. Pulmonary edema was seen in one case in the V.D. group (17%) and did not
respond to medical line of therapy. Patient died on second post natal day. Bansal V6
(1998) found the incidence to be 4.6%.
5. Cortical blindness was encountered in both VD and CD group. They however
regained back their vision within 4 days in VD group and 5 days in CD group.
6. Urinary tract infection was seen in 7.2% of the cases in the C.D. group for which
cases are treated according to culture and sensitivity.
Maternal Mortality:
Maternal deaths occurred in 1.7% of the cases in the V.D. group while there were no
maternal deaths in the C.D. group.77

75
TABLE-40 COMPARATIVE INCIDENCE OF MATERNAL MORTALITY TO MODE OF
DELIVERY MATERNAL MORTALITY (%)
Authors Year Maternal mortality VD CD
Mario Lopezllera104 1967 12 12
RatnamSS8
Sivasamboo5 1968 6 1.7
Derek Crichton16 1968 4.8 4.2
Villiers&Slabber17 1970 12.7 4.3
MondalRN4 1991 15.48 8.06
HabeebullahS103 1995 7.10 4.30
Present series 2011 1.7% -
Cause for Maternal Deaths:
1 Women out of total 59 in the V.D. group died, accounting for a maternal mortality
of 1.7%.
One woman had pulmonary edema following induction of labour. Induction delivery
interval was ten hours. She delivered dead male baby. Her pulmonary edema did not
respond to oxygen inhalation. Diuretic therapy. Later developed acute respiratory
distress syndrome died 22hours following delivery.
Relation of Maternal Mortality to First Convulsion-Delivery Interval:
In the present series, the mother who died had an induction-delivery interval more
than 10 hours and convulsion-delivery interval more than 14 hours.
Menon7 (1961) observed that maternal mortality increased with increase in the first
convulsion-delivery interval. His results were:

76
TABLE-41
RELATION OF MATERNAL MORTALITY TO FIRST CONVULSION-DELIVERY INTERVAL
First Convulsion-delivery
interval (hours)
Maternal Mortality (%)
0 – 2 7
2 – 4 13
4 – 8 19
8 – 12 22
12 – 18 25
18 – 24 32
>24 42
Thereby, we infer, that both the maternal and perinatal outcome may be considerably
improved in primigravid eclamptics if an early decision for caesarean section is taken,
in cases where delivery is not anticipated within 6 hours of adminssion or 12 hours of
the first fit, whichever is earlier.

77
SUMMARY
1. The study period extended from October 2010 to September 2011, a period of
12 months.
2. 100 primigravidas with more than 32 weeks gestation with antepartum
eclampsia were studied by dividing them into two groups for comparison.
• The C.D. group consisted of patients in whom caesarean section was
performed.
• The V.D. group consisted of patients who delivered vaginally.
3. The incidence of caesarean section was 41% and that of vaginal delivery was
59%.
4. Highest incidence of antepartum eclampsia was seen in the age group of 20-24
years in both the groups.
5. Majority of the cases in both the groups were Hindus of low socioeconomic
status from rural areas with improper antenatal care.
6. Maximum incidence of antepartum eclampsia was seen between 36-40 weeks
in both the groups.
7. Most of the cases had thrown less than 5 convulsions and were conscious on
admission in both the groups.
8. Pedal edema was predominant in both groups but the V.D. group had
comparatively more number of cases with nil edema.
9. Most of the patients presented with all the 3 signs of toxaemia in both the
groups.
10. Bishop’s score was unfavorable the C.D. group and the V.D. group.

78
11. Almost all the vaginal deliveries were induced. Outlet forceps was applied in
all cases and ventouse was applied in 1 case in the V.D. group.
12. 11 of the cases were taken for caesarean section for unfavourable. Cervical
factor were responsible for 80.2% of cases in the C.D. group.
13. 11 of the cases were operated within 6 hours and 31 cases were operated
within 24 hours of admission in the C.D. group.
14. 26.8% of the cases in the C.D. group were delivered within 12 hours of
admission, while in the V.D. group only one case delivered within 6 hours.
15. 41.4% of the cases in the C.D. group was delivered within 12 hours of the first
fit, while 33.9% of the cases in the V.D. group did so.
16. 88.6% of the cases in the V.D. group required more than 18 hours for delivery
after the start of induction.
17. Live birth rate was 92.23% in the C.D. group and 78% in the V.D. group.
18. Corrected perinatal mortality rate was 7.35% in the C.D. group and 18.64% in
the V.D. group.
19. NICU admission rate was 21.9% in the C.D. and 32.2% in the V.D. group.
20. Mean duration of stay in NICU in the C.D. group was 5.75 days and in the
V.D. group was 3 days.
21. The predominant cause for PNM was intrauterine hypoxia in the V.D. group
while it happened to be the second commonest cause in the C.D.
22. PNM was lesser in the C.D. group irrespective of the gestational age and birth
weight.
23. PNM increased with increase in the total number of convulsions, admission-
delivery, induction-delivery and convulsion-delivery intervals.

79
24. Both PNM and incidence of NICU admission were lesser when caesarean
section was performed within 6 hours of admission.
25. Incidence of maternal complications was 84% in the C.D. and 88.6% in the
V.D. group.
26. The incidence of maternal complications increased with increase in the total
number of convulsions, convulsion-delivery and induction-delivery intervals.
27. Maternal mortality was 1.7% in the V.D. group and nil (0%) in the C.D group.
28. Maternal deaths had their induction delivery interval more than 6 hours and
convulsion-delivery interval more than 12 hours.
29. Both perinatal morbidity and mortality and maternal morbidity and mortality
were found to be lesser in the C.D. group in comparison with the V.D. group.
30. Thus, early decision for caesarean section especially when delivery is not
anticipated with 6 hours of admission is detrimental in improving the perinatal
as well as maternal outcome in eclampsia in primigravidas with more than 32
weeks pregnancy.

80
CONCLUSION
“In antepartum eclampsia in primigravidas with more than 32 weeks gestation with
unfavourable cervix on admission with expected fetal weight >1.5 kgs, an early
decision for caesarean section either within 6 hours of admission or 12 hours of first
fit whichever is earlier is detrimental in improving the fetomaternal outcome”.
Prompt termination of pregnancy by caesarean section reduces maternal and
perinatal mortality, improves maternal outcome by reducing complications and also
improves perinatal outcome with better one minute Apgar scores and reduced NICU
admission.
With advanced expert surgical and anaesthetic techniques in modern
obstetrics, caesarean section is not unsafe as seen in previous years.
Both maternal and perinatal outcome can be improved by taking an early
decision for caesarean section when on admission cervix is unfavourable or delivery
is not anticipated within 6 hours. In severe antepartum eclamptic with a closed
uneffaced cervix and unengaged presenting part, it might give better results if
onservative treatment is supplemented by timely caesarean section instead of
withholding it.
As this study comprised of young primigravidae, it was seen that most had
unfavourable cervix and induction failure and moreover the duration of labour was
more in comparison with multigravidae patients.

81
Therefore, from my study of a small number of cases, I have come to a
conclusion that caesarean section if done promptly leads to more favourable outcome
than conservative obstetric management with vaginal delivery in eclampsia in
primigravidae after 32 weeks of pregnancy with unfavourable cervix on admission.
“Caesarean section should be done at the optimum time and not as a last resort when
conservative management has failed in eclampsia especially in primigravidas after32
weeks of pregnancy”.

82
BIBLIOGRAPHY
1. Dutta DC. “Textbook of Obstetrics”, 6th Ed., Calcutta, New Central Book
Agency Pvt. Ltd.; 2004: 233-242 pp.
2. Williams Obstetrics, 23rd Ed., McGraw Hill Co. Inc., 2010: 709-740 pp.
3. Bhaskar Pal, Geeta N, Vivek P. A study of eclampsia. J. of Obstetrics &
Gynec., 1996 Feb; 46(1): 34-39.
4. Bhattacharya PK, Purkayastha S, Basu M, Robinsanath M. Caesarean section
in eclampsia: Still a dilemma. J. of Obstet & Gynaec of India, 1992 Feb;
42(1): 51-55.
5. Chesley LC. Hypertensive disorders in pregnancy. New York Appleton-
Century Crafts, 1978: 1-628.
6. Vern n Walker, Williams S Baker, San Diego, California. A comparison study
of antihypertensive drug therapy and the modified stroganoff method in the
management of severe toxaemia of pregnancy.
7. Krishna Menon. Caesarean section in eclampsia. Jr of Obstet & Gynec, Brit.
Emp., 1961; 68: 461pp.
8. River Forest. Comquest of eclampsia. JAMA, 1956; 160: 251-255.
9. Corhill TF. Eclampsia – changes in pattern. Jr of Obstet & Gynec, Brit. Emp.
1957; 64: 67 pp.
10. Tenny, Dandrow. Clinical study of hypertensive disease in pregnancy. Am. J
of Obtet & Gynec, 1961; 81: 8 pp.86
11. Derek Crichton, Quinlan DK. Avoidable hospital deaths in obstetric practice.
J. Obstet Gynec Brit Cwlth, 1962; 69: 239.
12. Lokenath Bhose. Postpartum eclampsia. Am J of Obstet & Gynec, 1964;89:
898 pp.

83
13. Alan Alexander. A follow up of infants born of eclamptic mothers. Am J of
Obstet & Gynec, 1966; 95: 19.
14. Mario Lopezllera. Eclampsia 1963-1966, Evaluation of the treatment of 107
cases. Jr of Obstet & Gynec Brit Emp., 1967; 74: 379.
15. Lean, Ratnam SS, Sivasamboo. Use of benzodiazepines in the management of
eclampsia. Jr of Obstet & Gynec. Brit Emp, 1968;75: 856.
16. Derek Crichton, Morris Notelovitz, Heller. Less conservation in the treatment
of eclampsia. Jr of Obstet & Gynec Brit Emp., 1968;75(10): 1019-1023.
17. Villiers, Slabbers. Tratment of eclampsia at Karl Brenner Hospital. South
Africa M.J., 1970; 18: 48-50.
18. Ajay K Ghosh. Eclampsia – A radical approach by quick caesarean section. Jr
of Obstet & Gynec of India, 1974 Dec; 552-555.
19. Nanda Smite, Jai Bhagwan Sharma and Nirmal Gulati. Perinatal mortality in
eclampsia. Jr of Obstet & Gynecol of India, 1989; 39: 792-94.
20. Swain S et al. Maternal and perinatal mortality due to eclampsia. Ind J.Pediatr,
1993;30(6): 771-3.87
21. Arup Kumar Majhi, Partha Sarathi Chakraborty, Asima Mukhopadhyay.
Eclampsia –present scenario in a referral medical college hospital. J Obstet
Gynecol India, 2001;51(3): 143-47.
22. Kamilya G, Bharracharyya SK, Mukherji J. Changing trends in the
management of eclampsia from a teaching hospital. J Indian Med Assoc, 2005
Mar; 103(5): 132-5.
23. Douglas KA, Redman CWG. Eclampsia in the United Kingdom. BMJ 1994;
309: 1395.

84
24. Arup Kumar Kanhi. Abstracts, free communication papers, 42nd All India
Congress of Obstetrics & Gynecology, 1998.
25. Ratnam SS, Bhaskar Rao K, Arul Kumar S, Vol. 2, Eclampsia, P. 74:1996.
26. Nilesh Dalal, Thakur R. Comparative study of magnesium sulphate, phenytoin
sodium and lytic cocktail in eclampsia. Abstracts free communication papers.
42nd All India Congress of Obstetrics & Gynecology, 1998.
27. Suchita Mundle, Indrajit Mullik. Risk factors in pregnancy outcome in
eclampsia. Abstracts Free Communication Papers, 42nd All India congress of
Obstetrics & Gynecology 1998.
28. Srinivas Gadappa. Critical care and obstetric management in eclampsia in a
teaching hospital. Abstract, free communication papers, 42nd All India
Congress of Obstetrics & Gynecology, 1998.
29. Srividya. Maternal outcome in eclampsia. Abstract, free communication
papers, 42nd All India Congress of Obstetrics & Gynecology, 1998. 88
30. Vanita Bansal. Maternal and perinatal outcome in Eclampsia. Abstract, free
communication papers, 42nd All India Congress of Obstetrics & Gynecology,
1998.
31. Hangarga US. Maternal and perinatal outcome in eclampsia using phenytoin
sodium. Abstract, free communication papers, 42nd All India Congress of
Obstetrics & Gynecology, 1998.
32. Arati Srivastava. Comparative evaluation of magnesium sulphate, diazepam
and lytic cocktail regimes in the management of eclampsia. Abstract, free
communication papers, 42nd All India Congress of Obstetrics & Gynecology,
1998.
85
33. Low JJ, Yeo GS. Eclapsia, are we doing enough? Singapore Medical Journal,
1995 Oct; 36(5): 505-9.
34. Conde Agudelo et al. Case control study of risk factors for complicated
eclampsia. OBGY, 1997 Aug; 90(2): 172-5.
35. Conde-Agudelo A, Kafurycoeta AC. Case control study of risk factors for
complicated eclampsia. Obstet. Gynecol, 1997 Aug; 90(2): 172-5.
36. Mwinyoglee J, Amoko DH et al. Eclampsia at Ga Ran Kuwa Hospital. South
African Medical Journal, 1996; 85(12): 1536-9.
37. Sibai BM, McCubbin JM, Anderson GD et al. Eclampsia – Observations from
67 recent cases. Obstet Gynecol 1981; 58: 609-613.
38. Sibai MD, Andrea G Witlin DO, George R, Saade MD. Risk factors for
abruptio lacentae and eclampsia. Analysis of 445 consecutively managed
women with severe pre-clampsia and eclampsia. Am. J.Obstet Gynecol 1999;
1322-9.89
39. Wiltin AG, Friedman SA, Sibai BM. Cerebrovascular disorders complicating
pregnancy – beyond eclampsia. Am. J. Obstet Gynecol. 176(6): 1139-45.
40. Sejal V Desai. Critical care and convulsions in pregnancy. Abstract, free
communication papers, 42nd All India Congress of Obstetrics & Gynecology,
1998.
41. Leitch CR, Cameron AD, Walker JJ. The changing pattern of eclampsia over a
60 years period. Br. J. Gynecol, 1997; 104(8): 917-22.
42. Pritchard JA, Cunningham FG, Mason RA. Coagulation changes in eclampsia:
Their frequency and pathogenesis. Am. J. Obstet. Gynecol, 1976; 124: 855.
43. Leduc L, Wheeler JM, Kirshon B, Mitchell P, Cotton DB. Coagulation profile
in severe pre-eclampsia. Obstet Gynecol, 1992; 81: 235.

86
44. Torres PJ, Escolar G, Palacio M, Gratacos E, Alonso PL. Platelet sensitivity to
prostaglandin E, inhibition is reduced in preeclampsia but not in non-
proteinuric gestational hypertension. Br. J. Obstet Gynecol, 1996; 19: 103.
45. Samuel SP, Main EK, Tomaski A, Mennuti MT, Gabbe SG, Cines
DB.Abnormalities in platelet antiglobulin tests in pre-eclamptic mothers and
their neonates. Am. J. Obstet Gynecol, 1987; 157:109.
46. Burrows RF, Hunter DJS, Andrew M, Kelton JG. A prospective study
investigating the mechanism of thrombocytopenia in preeclampsia. Obstet.
Gynecol, 1987; 70: 334.90
47. Kelton JG, Hunter DJS, Naeme PB. A platelet function defect in preeclampsia.
Obstet. Gynecol, 1985; 65: 107.
48. Kilby MD, Broughton Dipkin F, cockbill S, Heptinstall S. A cross sectional
study of basal platelet intracellular free calcium concentration in normotensive
and hypertensive primigravid pregnancies. Clin Sci, 1990; 78: 75.
49. Dickmann WJ. The toxemias of pregnancy. 2nd Ed. St. Louis, Mosby, 1952.
50. Pritchard JA, Cunningham FG, pritchard SA. The Parkland Memorial Hospital
protocol for treatment of eclampsia: Evaluation of 245 cases. Am. J. Obstet
Gynecol, 1984; 148: 951.
51. Lopez-Llera M. Complicated eclampsia: 15 years experience in a referral
medical center. Am. J. Obstet Gynecol, 1982; 28: 142.
52. Sheehan HL. Pathological lesions in the hypertensive toxemias of pregnancy.
Huma & Verterinary, Philadelphia, Blakiston, 1950.
53. Sibai BM, Spinnato JA, Watson DL, Lewis JA, Anderson GA. Eclampsia 4.
Neurological findings and future outcome. Am. J. Obstet Gynecol, 1985a;
152: 184.

87
54. Brown CEL, Purdy PD, cunningham FG. Head computed tomography scan in
women with eclampsia. Am. J. Obstet Gynecol, 1988a:159-915.
55. Morris MC, Twickler DM, Hatab MR, Clarke GD, Peshok RM, Cunningham
FG. Cerebral blood flow and cranial MRI in eclampsia and severe
preeclampsia. Obstet Gynecol 1997.91
56. Horn EH, Filshie M, Kerslake RW et al. Widespread cerebral ischemia treated
with nimodipine in a patient with eclampsia. Br. Med. J., 1990; 301: 794.
57. Donaldson JO. Neurology of pregnancy. Philadelphia WB Saunders Co.,
1987: 216.
58. Belfort MA, Saade GR, Moise KJ Jr. The effect of magnesium sulphate on
maternal retinal blood flow in preeclampsia: A randomized placebo controlled
study. Am. J. Obstet. Gynecol, 1992; 167:1548.
59. Manas KJ, Welsh JD et al. Hepatic hemorrhage without rupture in
preeclampsia. N. Engl. J. Med., 1985; 312: 426.
60. Smith LG Jr, Moise KJ Jr, Dildy GA III et al. Spontaneous rupture of liver
during pregnancy: Current Therapy. Obstet Gynecol, 1991;77: 171.
61. Lee W, Gonik B, Cotton DB. Urinary diagnostic indices in preeclampsia
associated oliguria: Correlation with invasive hemodynamic monitoring. Am.
J. Obstet. Gynecol, 1987; 156: 100.
62. Sibai BM, Villar MA et al. Acute renal failure in hypertensive disorders of
pregnancy Pregnancy outcome and remote prognosis in 31 consecutive cases.
Am. J. Obstet Gynecol, 1990C; 162: 777.
63. Llewellyn Jones D. The treatment of eclampsia. Br. J. Obstet. Gynecol, 1961;
68: 33.

88
64. Bryant RD, Fleming JG. Veratrum viride in the treatment of eclampsia.
Obstet. Gynecol, 1962; 19: 372.92
65. Zuspan FP, Ward MC. Treatment of eclampsia. South Med. J, 1964; 57:954.
66. Gede Kohn RH, Hayashi TT, McDonald HM. Eclampsia at Magee Women’s
Hospital, 1970-1980.
67. Pritchard JA. The use of magnesium sulfate in preeclampsia-eclampsia. J.
Reprod Med, 1979; 23: 107.
68. Bhalla AK, Dhall GI, Dhall K. A safer and more effective treatment regimen
for eclampsia. Aust. NZ J Obstet Gynecol, 1994; 34: 144.
69. Eclampsia Trial Collaborative Group: Which anticonvulsant for women with
eclampsia? Evidence from the collaborative eclampsia trial. Lancet, 1995;
345: 1455.
70. Frangeih AY, friedman SA, Audibert F, Usta et al. Maternal outcome in
women with eclampsia. Am. J. Obstet Gynecol, 1996; 174: 453.
71. Porapakkam S. Epidemiology of eclampsia. Obstet. Gynecol, 1979; 54:26-30.
72. Harrison KA. Eclampsia. Br. J. Obstet Gynecol, 1985; 92 S: 86-99.
73. WHO, 1991. Hypertensive disorders of pregnancy. Report of WHO/MCH
Collaborative Study, Geneva, 1991.
74. Saumandal BK. Management of eclampsia with low dose magnesium
sulphate. Abstracts free communication papers. 42nd All India Congress of
Obstetrics & Gynecology, 1998.93.
75. Govan ADT. The pathogenesis of eclamptic lesions. Pathol Microbiol, 1961;
24: 561.
76. Sheehan HL Lynch JB (Ed): Cerebral lesions in: Pathology of Toxemia of
Pregnancy. Baltimore, Williams & Wilkins, 1973.

89
77. DeBoer K, Buller Hr, Tencate JW et al. Coagulation studies in the syndrome
of hemolysis. Elevated liver enzymes and low platelets. Br. J. Obstet Gynecol,
1991; 98: 42:98.
78. Pritchard JA, Weisman R Jr, Ratnoff OD, Vosburgh G. Intravascular
hemolysis, thrombocytopenia and other hematological abnormalities
associated with severe toxemia of pregnancy. N Engl. J. Med, 1954; 250: 87.
79. Weinsten L. Pre-eclampsia with hemolysis. Elevated liver enzymes and
thrombocytopenia. Obstet Gynecol, 1985; 66: 657.
80. Sibai BM, Ramadan MK, USTA I et al. Maternal morbidity and mortality in
442 pregnancies with HELLP syndrome. Am. J. Obstet Gynecol, 1991; 98: 42.
81. Audibert F, Friedman SA, Frangeih et al. Diagnostic criteria for HELLP
syndrome. Tedious or “HELLPFUL”? Am. J. Obstet Gynecol, 1996; 174: 454.
82. Sibai BM, Mabie BC et al. Pulmonary edema in severe
preeclampsiaeclampsia: Analysis of 37 consecutive cases. Am. J. Obstet
Gynecol, 187b; 156; 1174.94
83. Cunningham FG, Fernandez CO, Hernandez C. Blindness associated with
preeclampsia and eclampsia. Am. J. Obstet Gynecol, 1995; 172:1291.
84. Hibbard LT. Maternal mortality due to acute toxemia. Obstet Gynecol, 1985;
123: 159.
85. Sibai BM, Spinnato JA et al. Eclampsia IV Neurologic findings and future
outcome. Am. J. Obstet Gynecol, 1985; 152: 184-192.
86. Ducey J, Schulman H et al. A classification of hypertension in pregnancy
based on Doppler velocimetry. Am. J. Obstet Gynecol, 1987; 157:680.
87. Brazy JE et al. Neonatal manifestations of severe maternal hypertension
occurring before the 36th week of pregnancy. J. Pediatric, 1982;100: 165.

90
88. Pritchard JA, Pritchard SA. Standardized treatment of 154 cases of eclampsia.
Am. J. Obstet. Gynecol, 1975; 123: 543-548.
89. Hallak M, Berry SM et al. Fetal serum and amniotic fluid magnesium
concentration with maternal treatment. Obstet. Gynecol, 1993; 81:185.
90. Chatterji A, Mukherji J. Comparative study of different anti-convulsants in
eclampsia. Journal of Obstetrics & Gynecology Research, 1997 June; 23(3):
289-93.
91. Sawhney h, Vasista k, Rani K. Comparison of lytic cocktail and magnesium
sulfate regimens in eclampsia: A retrospective analysis. J. Obstet. Gynecol
Research, 1998; 24(40: 261-6.95
92. Lopez-Llera M, Hernandez Horta JL. Retarded fetal growth in eclampsia.J.
Reprod. Med. 1972; 9: 229.
93. Borges LF, Gucer G. Effect of magnesium on epileptic foci. Epilepsia, 1978;
19: 81.
94. Cotton DB, Janusz CA. Anti-convulsant effects of magnesium sulfate oh
hippocampal seizures: Therapeutic implications in pre-eclampsia-Eclampsia.
Am. J. Obstet. Gynecol, 1992; 166: 1127.
95. Lipton SA, Rosenberg PA. Excitatory amino acids as a final common pathway
for neurologic disorders. N. Engl. J. Med., 1994; 330:613.
96. Attkinson MW, Belfort MA et al. The relation between magnesium sulfate
therapy and fetal heart rate variability. Obstet Gynecol, 1994a; 83: 967.
97. Dewhurst SJ. Pre-eclampsia, eclampsia, hypertension and chronic renal
disease. Integrated obstetrics and gynecology for postgraduates: Singapure,
Blackwell Scientific Publications, 3rd Ed.: 259.

91
98. Zuspan FP. Toxemia of pregnancy, In: Sciarra JJ and Gerby AB (ed.).
Gynecology and Obstetrics, Vol. 2 revised edition. Hagerstown: Harper and
Row Publishers, P. 44.
99. Kale VJ, Sapre S. Critical care in eclampsia – Comparison of various anti-
convulsant regimes. Abstracts, Free Communication Papers, 42nd All India
Congress of Obstetrics & Gynecology, 1998.
100. Cheek TG, Samuels P. PIH in Datta S (ed) Anesthesia and management of
high-risk pregnancy. St. Louis Mosby Year Book, 1991.96
101. Chadwick HS, Easterling T. Anesthetic concerns in the patients with
preeclampsia. Semin Perinatal, 1997; 15: 397.
102. Ramanathan J. Anesthetic considertions in preeclampsia. Clin Perinatol, 1991;
18: 875.
103. Sibai BM, Anderson GD, Abdella TN et al. Eclampsia III. Neonatal outcome,
growth and development. Am. J. Obstet. Gynecol, 1983;146: 307.
104. Mario Lopez-Llera, Rubio Linares and Hernandez Horta. Maternal mortality
rates in eclampsia. Am J of Obstetric Gynec, 1976 Jan;124(2): 149-155.
105. Sibai BM, McCubin JH, Anderson GD, Zipshitz AJ, Dilts PV. Obstet Gynec,
1981; 58: 609 pp.
106. Abdullah AR, Nalliah S. Eclampsia in kelantan. West Aft J Med., 1990 Jul-
Sept; 9(3): 157-63.
107. Habeebullah S, Agarwal A, Swain S, Arora R. Impact of mode of delivery on
maternal mortality in eclampsia. JIMA 1997 Apr; 95(40.
108. Hakerwadi AV, Taner CE, Aban M, Garden AC, Ozelbaykal V. Prevalence,
management and outcome in eclampsia. Lancet, 1996 Aug 10; 348(9024):
364-9.

92
109. Oladokun A, Okewole AI, Adewole IF, Babarinsa IA. Evaluation of cases of
eclampsia in the University College of Hospital, Ibadan ober a 10 year period.
West Afr J Med, 2000 Jul-Sep; 1993): 192-4.97
110. Kameshwari Devi, Shameem Sultana, Suresh Rao Santapur. Review of
eclampsia 369 cases. J. of Obstet & Gynec of India, 1976 Feb.
111. Zuspan FP, Eduardo Talledo, Katherine Rhodes RN. Factors affecting delivery
in eclampsia – The condition of the cervix and uterine activity. Am. J. Obstet
& Gynec, 1968; 100(5): 672-85.
112. Dandekar LM< Biren Shah. Eclampsia: Peripheral Hospital Experience. Jl of
Obstet & Gynec of India, 1993 Feb; 43(1): 42-44.
113. Subodh Mitra & Kanak Das. Management of eclampsia. J. of Obstet & Gynec,
Brit Emp., 1957; 64: 74-78.
114. Anjaneyulu R, Amina Paperwala. Puerperal psychosis. J of Obstet & Gynec of
India, 1974 April.
115. Lee W Connell CM. Maternal & perinatal outcome in eclampsia J Obstet &
Gynaecol.2004 Feb: 26(2):119-23.
116. TAJ, Clinical study of 100 cases eclampsia Dec 2004;17(2) 80-83.
117. Jamila, M M Muhammad IS, Wajiha A maternal and perinatal outcome in
eclampsia. J Postgraduate Medical 2004;18(3) 470-6.
118. Barret M. Schroeder ACOG practice Bulletin on Diagnosing and managing
preclampisa & eclampisa. Am Obstet & Gynaecol.2007;June 196(6); 514.el-9.
119. M Khanum 2009 PDF Original article. A clinical study of eclampsia i.e. file
format.

93
PROFORMA
NAME I.P.NO.
AGE
DATE OF ADMISSION
HUSBAND DATE OF DISCHARGE
OCCUPATION DATE OF DELIVERY
SE STATUS BOOKED/UNBOOKED
RELIGION
ADDRESS
CHIEF COMPLAINTS WITH PERIOD OF AMENORHOEA
H/O CONVULSIONS
NUMBER OF CONVULSIONS BEFORE ADMISSION
AFTER ADMISSION
LAST CONVULSION
DURATION OF EACH CONVULSION
CONSCIOUSNESS BETWEEN ATTACKS
H/O FROTHING/TONGUE BITE/INCONTINENCE OF URINE/STOOLS
PREMONITORY SYMPTOMS : H/O HEADACHE1 / EPIGASTRIC PAIN2 /
NAUSEA3 / VOMITING4 / BLURRED VISION5
OBSTETRIC HISTORY : M.L. CONSANGINOUSC/
NONCONSANGINOUSN
ANTENATAL I
II
III
ANC YESY/NON
DATE OF LAST/B.P.RECORDING
MENSTRUAL HISTORY: AGE OF MENARCHE
CYCLES
FLOW
PAST HISTORY : HTN/DM/TB/HEART DISEASES/LIVER &RENAL /ANY
MAJOR ILLNESS
FAMILY HISTORY:HTN/DM/TB/ECLAMPSIA IN MOTHER OR SISTER

94
PERSONAL HISTORY:
GENERAL PHYSICAL EXAMINATION
CONSCIOUS1/IRRITABLE2/UNCONSCIOUS3
EYE : CONJUNCTIVA :PINK1/PALE2/ICTERIC3
TONGUE : PINK1/PALE2/BITE3
NECK : THYROID/LYMPH NODES
BREAST
EDEMA: PEDALa/VULVALb/ABDOMENc/GENERALISEDd
VITALS : TEMP
PULSE
BP
RR
PUPILS-NORMAL1 / SLUGGISH REACTING2
KNEE JERK – NORMAL1 / EXAGGERATED2
SYSTEMIC EXAMINATION
C.V.S
R.S
C.N.S
OBSTETRIC EXAM
P/A – 32 – 34 WEEKS1, 34 – 36, WEEKS2, 36 – 403 WEEKS
P/S
P/V - BISHOP’S SCORE
INVESTIGATIONS :
HAEMOGRAM
LFT – SGOT/STPT/LDH /S.BILIRUBIN
RFT – BLOOD UREA/SERUM CREATININE/SERUM URIC ACID
USG
FUNDOSCOPY – Y/N
BLOOD GROUPING AND TYPING
HBsAG HIV I & II
COAGULATION PROFILE
CT BRAIN IF NECESSARY

95
MANGEMENT
SEDATION -
ANTIHYPERTESIVES - NIFIDEPINEN
ANTICONVULSANT - LABETOLOLL
ANTIBIOTICS
MODE OF DELIVERY : VAGINAL/LSCS
DELIVERY NOTES
BABY NOTES LBW/SFG/NND
GA/SEX/PLACENTA
ADMISSION TO NICU : DURATION OF STAY
DIAGNOSIS – HIE1/SEPTICAEMIA2/RDS3/MAS4
OBSERVATIONS
1. B.P AT ADMISSION
2. PROTEINURIA AT ADMISSION
3. TIME B/N ADMISSION AND CONVULSION (HOURS)
4. TIME B/N CONVULSION AND DELIVERY (HOURS)
5. TIME B/N ADMISSION AND DELIVERY (HOURS)
6. IMMEDIATE POST DELIVERY B.P.
7. URINE ALBUMIN NIL FOLLOWING DELIVERY
8. MATERNAL COMPLICATIONS
• PULMONARY EDEMA6
• PLACENTAL ABRUPTION/HELLP1
• CEREBRAL INFARCTION3
• UTI2
• PPH4
• CORTICAL BLINDNESS5
9. DURATION OF STAY IN HOSPITAL
10. CONDITION OF MOTHER AND BABY AT DISCHARGE

BIBLIOGRAPHY
1. Dutta DC. “Textbook of Obstetrics”, 6th Ed., Calcutta, New Central Book
Agency Pvt. Ltd.; 2004: 233-242 pp.
2. Williams Obstetrics, 23rd Ed., McGraw Hill Co. Inc., 2010: 709-740 pp.
3. Bhaskar Pal, Geeta N, Vivek P. A study of eclampsia. J. of Obstetrics &
Gynec., 1996 Feb; 46(1): 34-39.
4. Bhattacharya PK, Purkayastha S, Basu M, Robinsanath M. Caesarean section
in eclampsia: Still a dilemma. J. of Obstet & Gynaec of India, 1992 Feb;
42(1): 51-55.
5. Chesley LC. Hypertensive disorders in pregnancy. New York Appleton-
Century Crafts, 1978: 1-628.
6. Vern n Walker, Williams S Baker, San Diego, California. A comparison study
of antihypertensive drug therapy and the modified stroganoff method in the
management of severe toxaemia of pregnancy.
7. Krishna Menon. Caesarean section in eclampsia. Jr of Obstet & Gynec, Brit.
Emp., 1961; 68: 461pp.
8. River Forest. Comquest of eclampsia. JAMA, 1956; 160: 251-255.
9. Corhill TF. Eclampsia – changes in pattern. Jr of Obstet & Gynec, Brit. Emp.
1957; 64: 67 pp.
10. Tenny, Dandrow. Clinical study of hypertensive disease in pregnancy. Am. J
of Obtet & Gynec, 1961; 81: 8 pp.86
11. Derek Crichton, Quinlan DK. Avoidable hospital deaths in obstetric practice.
J. Obstet Gynec Brit Cwlth, 1962; 69: 239.
12. Lokenath Bhose. Postpartum eclampsia. Am J of Obstet & Gynec, 1964;89:
898 pp.

13. Alan Alexander. A follow up of infants born of eclamptic mothers. Am J of
Obstet & Gynec, 1966; 95: 19.
14. Mario Lopezllera. Eclampsia 1963-1966, Evaluation of the treatment of 107
cases. Jr of Obstet & Gynec Brit Emp., 1967; 74: 379.
15. Lean, Ratnam SS, Sivasamboo. Use of benzodiazepines in the management of
eclampsia. Jr of Obstet & Gynec. Brit Emp, 1968;75: 856.
16. Derek Crichton, Morris Notelovitz, Heller. Less conservation in the treatment
of eclampsia. Jr of Obstet & Gynec Brit Emp., 1968;75(10): 1019-1023.
17. Villiers, Slabbers. Tratment of eclampsia at Karl Brenner Hospital. South
Africa M.J., 1970; 18: 48-50.
18. Ajay K Ghosh. Eclampsia – A radical approach by quick caesarean section. Jr
of Obstet & Gynec of India, 1974 Dec; 552-555.
19. Nanda Smite, Jai Bhagwan Sharma and Nirmal Gulati. Perinatal mortality in
eclampsia. Jr of Obstet & Gynecol of India, 1989; 39: 792-94.
20. Swain S et al. Maternal and perinatal mortality due to eclampsia. Ind J.Pediatr,
1993;30(6): 771-3.87
21. Arup Kumar Majhi, Partha Sarathi Chakraborty, Asima Mukhopadhyay.
Eclampsia –present scenario in a referral medical college hospital. J Obstet
Gynecol India, 2001;51(3): 143-47.
22. Kamilya G, Bharracharyya SK, Mukherji J. Changing trends in the
management of eclampsia from a teaching hospital. J Indian Med Assoc, 2005
Mar; 103(5): 132-5.
23. Douglas KA, Redman CWG. Eclampsia in the United Kingdom. BMJ 1994;
309: 1395.

24. Arup Kumar Kanhi. Abstracts, free communication papers, 42nd All India
Congress of Obstetrics & Gynecology, 1998.
25. Ratnam SS, Bhaskar Rao K, Arul Kumar S, Vol. 2, Eclampsia, P. 74:1996.
26. Nilesh Dalal, Thakur R. Comparative study of magnesium sulphate, phenytoin
sodium and lytic cocktail in eclampsia. Abstracts free communication papers.
42nd All India Congress of Obstetrics & Gynecology, 1998.
27. Suchita Mundle, Indrajit Mullik. Risk factors in pregnancy outcome in
eclampsia. Abstracts Free Communication Papers, 42nd All India congress of
Obstetrics & Gynecology 1998.
28. Srinivas Gadappa. Critical care and obstetric management in eclampsia in a
teaching hospital. Abstract, free communication papers, 42nd All India
Congress of Obstetrics & Gynecology, 1998.
29. Srividya. Maternal outcome in eclampsia. Abstract, free communication
papers, 42nd All India Congress of Obstetrics & Gynecology, 1998. 88
30. Vanita Bansal. Maternal and perinatal outcome in Eclampsia. Abstract, free
communication papers, 42nd All India Congress of Obstetrics & Gynecology,
1998.
31. Hangarga US. Maternal and perinatal outcome in eclampsia using phenytoin
sodium. Abstract, free communication papers, 42nd All India Congress of
Obstetrics & Gynecology, 1998.
32. Arati Srivastava. Comparative evaluation of magnesium sulphate, diazepam
and lytic cocktail regimes in the management of eclampsia. Abstract, free
communication papers, 42nd All India Congress of Obstetrics & Gynecology,
1998.

33. Low JJ, Yeo GS. Eclapsia, are we doing enough? Singapore Medical Journal,
1995 Oct; 36(5): 505-9.
34. Conde Agudelo et al. Case control study of risk factors for complicated
eclampsia. OBGY, 1997 Aug; 90(2): 172-5.
35. Conde-Agudelo A, Kafurycoeta AC. Case control study of risk factors for
complicated eclampsia. Obstet. Gynecol, 1997 Aug; 90(2): 172-5.
36. Mwinyoglee J, Amoko DH et al. Eclampsia at Ga Ran Kuwa Hospital. South
African Medical Journal, 1996; 85(12): 1536-9.
37. Sibai BM, McCubbin JM, Anderson GD et al. Eclampsia – Observations from
67 recent cases. Obstet Gynecol 1981; 58: 609-613.
38. Sibai MD, Andrea G Witlin DO, George R, Saade MD. Risk factors for
abruptio lacentae and eclampsia. Analysis of 445 consecutively managed
women with severe pre-clampsia and eclampsia. Am. J.Obstet Gynecol 1999;
1322-9.89
39. Wiltin AG, Friedman SA, Sibai BM. Cerebrovascular disorders complicating
pregnancy – beyond eclampsia. Am. J. Obstet Gynecol. 176(6): 1139-45.
40. Sejal V Desai. Critical care and convulsions in pregnancy. Abstract, free
communication papers, 42nd All India Congress of Obstetrics & Gynecology,
1998.
41. Leitch CR, Cameron AD, Walker JJ. The changing pattern of eclampsia over a
60 years period. Br. J. Gynecol, 1997; 104(8): 917-22.
42. Pritchard JA, Cunningham FG, Mason RA. Coagulation changes in eclampsia:
Their frequency and pathogenesis. Am. J. Obstet. Gynecol, 1976; 124: 855.
43. Leduc L, Wheeler JM, Kirshon B, Mitchell P, Cotton DB. Coagulation profile
in severe pre-eclampsia. Obstet Gynecol, 1992; 81: 235.

44. Torres PJ, Escolar G, Palacio M, Gratacos E, Alonso PL. Platelet sensitivity to
prostaglandin E, inhibition is reduced in preeclampsia but not in non-
proteinuric gestational hypertension. Br. J. Obstet Gynecol, 1996; 19: 103.
45. Samuel SP, Main EK, Tomaski A, Mennuti MT, Gabbe SG, Cines
DB.Abnormalities in platelet antiglobulin tests in pre-eclamptic mothers and
their neonates. Am. J. Obstet Gynecol, 1987; 157:109.
46. Burrows RF, Hunter DJS, Andrew M, Kelton JG. A prospective study
investigating the mechanism of thrombocytopenia in preeclampsia. Obstet.
Gynecol, 1987; 70: 334.90
47. Kelton JG, Hunter DJS, Naeme PB. A platelet function defect in preeclampsia.
Obstet. Gynecol, 1985; 65: 107.
48. Kilby MD, Broughton Dipkin F, cockbill S, Heptinstall S. A cross sectional
study of basal platelet intracellular free calcium concentration in normotensive
and hypertensive primigravid pregnancies. Clin Sci, 1990; 78: 75.
49. Dickmann WJ. The toxemias of pregnancy. 2nd Ed. St. Louis, Mosby, 1952.
50. Pritchard JA, Cunningham FG, pritchard SA. The Parkland Memorial Hospital
protocol for treatment of eclampsia: Evaluation of 245 cases. Am. J. Obstet
Gynecol, 1984; 148: 951.
51. Lopez-Llera M. Complicated eclampsia: 15 years experience in a referral
medical center. Am. J. Obstet Gynecol, 1982; 28: 142.
52. Sheehan HL. Pathological lesions in the hypertensive toxemias of pregnancy.
Huma & Verterinary, Philadelphia, Blakiston, 1950.
53. Sibai BM, Spinnato JA, Watson DL, Lewis JA, Anderson GA. Eclampsia 4.
Neurological findings and future outcome. Am. J. Obstet Gynecol, 1985a;
152: 184.

54. Brown CEL, Purdy PD, cunningham FG. Head computed tomography scan in
women with eclampsia. Am. J. Obstet Gynecol, 1988a:159-915.
55. Morris MC, Twickler DM, Hatab MR, Clarke GD, Peshok RM, Cunningham
FG. Cerebral blood flow and cranial MRI in eclampsia and severe
preeclampsia. Obstet Gynecol 1997.91
56. Horn EH, Filshie M, Kerslake RW et al. Widespread cerebral ischemia treated
with nimodipine in a patient with eclampsia. Br. Med. J., 1990; 301: 794.
57. Donaldson JO. Neurology of pregnancy. Philadelphia WB Saunders Co.,
1987: 216.
58. Belfort MA, Saade GR, Moise KJ Jr. The effect of magnesium sulphate on
maternal retinal blood flow in preeclampsia: A randomized placebo controlled
study. Am. J. Obstet. Gynecol, 1992; 167:1548.
59. Manas KJ, Welsh JD et al. Hepatic hemorrhage without rupture in
preeclampsia. N. Engl. J. Med., 1985; 312: 426.
60. Smith LG Jr, Moise KJ Jr, Dildy GA III et al. Spontaneous rupture of liver
during pregnancy: Current Therapy. Obstet Gynecol, 1991;77: 171.
61. Lee W, Gonik B, Cotton DB. Urinary diagnostic indices in preeclampsia
associated oliguria: Correlation with invasive hemodynamic monitoring. Am.
J. Obstet. Gynecol, 1987; 156: 100.
62. Sibai BM, Villar MA et al. Acute renal failure in hypertensive disorders of
pregnancy Pregnancy outcome and remote prognosis in 31 consecutive cases.
Am. J. Obstet Gynecol, 1990C; 162: 777.
63. Llewellyn Jones D. The treatment of eclampsia. Br. J. Obstet. Gynecol, 1961;
68: 33.

64. Bryant RD, Fleming JG. Veratrum viride in the treatment of eclampsia.
Obstet. Gynecol, 1962; 19: 372.92
65. Zuspan FP, Ward MC. Treatment of eclampsia. South Med. J, 1964; 57:954.
66. Gede Kohn RH, Hayashi TT, McDonald HM. Eclampsia at Magee Women’s
Hospital, 1970-1980.
67. Pritchard JA. The use of magnesium sulfate in preeclampsia-eclampsia. J.
Reprod Med, 1979; 23: 107.
68. Bhalla AK, Dhall GI, Dhall K. A safer and more effective treatment regimen
for eclampsia. Aust. NZ J Obstet Gynecol, 1994; 34: 144.
69. Eclampsia Trial Collaborative Group: Which anticonvulsant for women with
eclampsia? Evidence from the collaborative eclampsia trial. Lancet, 1995;
345: 1455.
70. Frangeih AY, friedman SA, Audibert F, Usta et al. Maternal outcome in
women with eclampsia. Am. J. Obstet Gynecol, 1996; 174: 453.
71. Porapakkam S. Epidemiology of eclampsia. Obstet. Gynecol, 1979; 54:26-30.
72. Harrison KA. Eclampsia. Br. J. Obstet Gynecol, 1985; 92 S: 86-99.
73. WHO, 1991. Hypertensive disorders of pregnancy. Report of WHO/MCH
Collaborative Study, Geneva, 1991.
74. Saumandal BK. Management of eclampsia with low dose magnesium
sulphate. Abstracts free communication papers. 42nd All India Congress of
Obstetrics & Gynecology, 1998.93.
75. Govan ADT. The pathogenesis of eclamptic lesions. Pathol Microbiol, 1961;
24: 561.
76. Sheehan HL Lynch JB (Ed): Cerebral lesions in: Pathology of Toxemia of
Pregnancy. Baltimore, Williams & Wilkins, 1973.

77. DeBoer K, Buller Hr, Tencate JW et al. Coagulation studies in the syndrome
of hemolysis. Elevated liver enzymes and low platelets. Br. J. Obstet Gynecol,
1991; 98: 42:98.
78. Pritchard JA, Weisman R Jr, Ratnoff OD, Vosburgh G. Intravascular
hemolysis, thrombocytopenia and other hematological abnormalities
associated with severe toxemia of pregnancy. N Engl. J. Med, 1954; 250: 87.
79. Weinsten L. Pre-eclampsia with hemolysis. Elevated liver enzymes and
thrombocytopenia. Obstet Gynecol, 1985; 66: 657.
80. Sibai BM, Ramadan MK, USTA I et al. Maternal morbidity and mortality in
442 pregnancies with HELLP syndrome. Am. J. Obstet Gynecol, 1991; 98: 42.
81. Audibert F, Friedman SA, Frangeih et al. Diagnostic criteria for HELLP
syndrome. Tedious or “HELLPFUL”? Am. J. Obstet Gynecol, 1996; 174: 454.
82. Sibai BM, Mabie BC et al. Pulmonary edema in severe
preeclampsiaeclampsia: Analysis of 37 consecutive cases. Am. J. Obstet
Gynecol, 187b; 156; 1174.94
83. Cunningham FG, Fernandez CO, Hernandez C. Blindness associated with
preeclampsia and eclampsia. Am. J. Obstet Gynecol, 1995; 172:1291.
84. Hibbard LT. Maternal mortality due to acute toxemia. Obstet Gynecol, 1985;
123: 159.
85. Sibai BM, Spinnato JA et al. Eclampsia IV Neurologic findings and future
outcome. Am. J. Obstet Gynecol, 1985; 152: 184-192.
86. Ducey J, Schulman H et al. A classification of hypertension in pregnancy
based on Doppler velocimetry. Am. J. Obstet Gynecol, 1987; 157:680.
87. Brazy JE et al. Neonatal manifestations of severe maternal hypertension
occurring before the 36th week of pregnancy. J. Pediatric, 1982;100: 165.

88. Pritchard JA, Pritchard SA. Standardized treatment of 154 cases of eclampsia.
Am. J. Obstet. Gynecol, 1975; 123: 543-548.
89. Hallak M, Berry SM et al. Fetal serum and amniotic fluid magnesium
concentration with maternal treatment. Obstet. Gynecol, 1993; 81:185.
90. Chatterji A, Mukherji J. Comparative study of different anti-convulsants in
eclampsia. Journal of Obstetrics & Gynecology Research, 1997 June; 23(3):
289-93.
91. Sawhney h, Vasista k, Rani K. Comparison of lytic cocktail and magnesium
sulfate regimens in eclampsia: A retrospective analysis. J. Obstet. Gynecol
Research, 1998; 24(40: 261-6.95
92. Lopez-Llera M, Hernandez Horta JL. Retarded fetal growth in eclampsia.J.
Reprod. Med. 1972; 9: 229.
93. Borges LF, Gucer G. Effect of magnesium on epileptic foci. Epilepsia, 1978;
19: 81.
94. Cotton DB, Janusz CA. Anti-convulsant effects of magnesium sulfate oh
hippocampal seizures: Therapeutic implications in pre-eclampsia-Eclampsia.
Am. J. Obstet. Gynecol, 1992; 166: 1127.
95. Lipton SA, Rosenberg PA. Excitatory amino acids as a final common pathway
for neurologic disorders. N. Engl. J. Med., 1994; 330:613.
96. Attkinson MW, Belfort MA et al. The relation between magnesium sulfate
therapy and fetal heart rate variability. Obstet Gynecol, 1994a; 83: 967.
97. Dewhurst SJ. Pre-eclampsia, eclampsia, hypertension and chronic renal
disease. Integrated obstetrics and gynecology for postgraduates: Singapure,
Blackwell Scientific Publications, 3rd Ed.: 259.
98. Zuspan FP. Toxemia of pregnancy, In: Sciarra JJ and Gerby AB (ed.).
Gynecology and Obstetrics, Vol. 2 revised edition. Hagerstown: Harper and
Row Publishers, P. 44.
99. Kale VJ, Sapre S. Critical care in eclampsia – Comparison of various anti-
convulsant regimes. Abstracts, Free Communication Papers, 42nd All India
Congress of Obstetrics & Gynecology, 1998.
100. Cheek TG, Samuels P. PIH in Datta S (ed) Anesthesia and management of
high-risk pregnancy. St. Louis Mosby Year Book, 1991.96
101. Chadwick HS, Easterling T. Anesthetic concerns in the patients with
preeclampsia. Semin Perinatal, 1997; 15: 397.
102. Ramanathan J. Anesthetic considertions in preeclampsia. Clin Perinatol, 1991;
18: 875.
103. Sibai BM, Anderson GD, Abdella TN et al. Eclampsia III. Neonatal outcome,
growth and development. Am. J. Obstet. Gynecol, 1983;146: 307.
104. Mario Lopez-Llera, Rubio Linares and Hernandez Horta. Maternal mortality
rates in eclampsia. Am J of Obstetric Gynec, 1976 Jan;124(2): 149-155.
105. Sibai BM, McCubin JH, Anderson GD, Zipshitz AJ, Dilts PV. Obstet Gynec,
1981; 58: 609 pp.
106. Abdullah AR, Nalliah S. Eclampsia in kelantan. West Aft J Med., 1990 Jul-
Sept; 9(3): 157-63.
107. Habeebullah S, Agarwal A, Swain S, Arora R. Impact of mode of delivery on
maternal mortality in eclampsia. JIMA 1997 Apr; 95(40.
108. Hakerwadi AV, Taner CE, Aban M, Garden AC, Ozelbaykal V. Prevalence,
management and outcome in eclampsia. Lancet, 1996 Aug 10; 348(9024):
364-9.

109. Oladokun A, Okewole AI, Adewole IF, Babarinsa IA. Evaluation of cases of
eclampsia in the University College of Hospital, Ibadan ober a 10 year period.
West Afr J Med, 2000 Jul-Sep; 1993): 192-4.97
110. Kameshwari Devi, Shameem Sultana, Suresh Rao Santapur. Review of
eclampsia 369 cases. J. of Obstet & Gynec of India, 1976 Feb.
111. Zuspan FP, Eduardo Talledo, Katherine Rhodes RN. Factors affecting delivery
in eclampsia – The condition of the cervix and uterine activity. Am. J. Obstet
& Gynec, 1968; 100(5): 672-85.
112. Dandekar LM< Biren Shah. Eclampsia: Peripheral Hospital Experience. Jl of
Obstet & Gynec of India, 1993 Feb; 43(1): 42-44.
113. Subodh Mitra & Kanak Das. Management of eclampsia. J. of Obstet & Gynec,
Brit Emp., 1957; 64: 74-78.
114. Anjaneyulu R, Amina Paperwala. Puerperal psychosis. J of Obstet & Gynec of
India, 1974 April.
115. Lee W Connell CM. Maternal & perinatal outcome in eclampsia J Obstet &
Gynaecol.2004 Feb: 26(2):119-23.
116. TAJ, Clinical study of 100 cases eclampsia Dec 2004;17(2) 80-83.
117. Jamila, M M Muhammad IS, Wajiha A maternal and perinatal outcome in
eclampsia. J Postgraduate Medical 2004;18(3) 470-6.
118. Barret M. Schroeder ACOG practice Bulletin on Diagnosing and managing
preclampisa & eclampisa. Am Obstet & Gynaecol.2007;June 196(6); 514.el-9.
119. M Khanum 2009 PDF Original article. A clinical study of eclampsia i.e. file
format.

PROFORMA
NAME I.P.NO.
AGE
DATE OF ADMISSION
HUSBAND DATE OF DISCHARGE
OCCUPATION DATE OF DELIVERY
SE STATUS BOOKED/UNBOOKED
RELIGION
ADDRESS
CHIEF COMPLAINTS WITH PERIOD OF AMENORHOEA
H/O CONVULSIONS
NUMBER OF CONVULSIONS BEFORE ADMISSION
AFTER ADMISSION
LAST CONVULSION
DURATION OF EACH CONVULSION
CONSCIOUSNESS BETWEEN ATTACKS
H/O FROTHING/TONGUE BITE/INCONTINENCE OF URINE/STOOLS
PREMONITORY SYMPTOMS : H/O HEADACHE1 / EPIGASTRIC PAIN2 /
NAUSEA3 / VOMITING4 / BLURRED VISION5
OBSTETRIC HISTORY : M.L. CONSANGINOUSC/
NONCONSANGINOUSN
ANTENATAL I
II
III
ANC YESY/NON
DATE OF LAST/B.P.RECORDING
MENSTRUAL HISTORY: AGE OF MENARCHE
CYCLES
FLOW
PAST HISTORY : HTN/DM/TB/HEART DISEASES/LIVER &RENAL /ANY
MAJOR ILLNESS
FAMILY HISTORY:HTN/DM/TB/ECLAMPSIA IN MOTHER OR SISTER

PERSONAL HISTORY:
GENERAL PHYSICAL EXAMINATION
CONSCIOUS1/IRRITABLE2/UNCONSCIOUS3
EYE : CONJUNCTIVA :PINK1/PALE2/ICTERIC3
TONGUE : PINK1/PALE2/BITE3
NECK : THYROID/LYMPH NODES
BREAST
EDEMA: PEDALa/VULVALb/ABDOMENc/GENERALISEDd
VITALS : TEMP
PULSE
BP
RR
PUPILS-NORMAL1 / SLUGGISH REACTING2
KNEE JERK – NORMAL1 / EXAGGERATED2
SYSTEMIC EXAMINATION
C.V.S
R.S
C.N.S
OBSTETRIC EXAM
P/A – 32 – 34 WEEKS1, 34 – 36, WEEKS2, 36 – 403 WEEKS
P/S
P/V - BISHOP’S SCORE
INVESTIGATIONS :
HAEMOGRAM
LFT – SGOT/STPT/LDH /S.BILIRUBIN
RFT – BLOOD UREA/SERUM CREATININE/SERUM URIC ACID
USG
FUNDOSCOPY – Y/N
BLOOD GROUPING AND TYPING
HBsAG HIV I & II
COAGULATION PROFILE
CT BRAIN IF NECESSARY

MANGEMENT
SEDATION -
ANTIHYPERTESIVES - NIFIDEPINEN
ANTICONVULSANT - LABETOLOLL
ANTIBIOTICS
MODE OF DELIVERY : VAGINAL/LSCS
DELIVERY NOTES
BABY NOTES LBW/SFG/NND
GA/SEX/PLACENTA
ADMISSION TO NICU : DURATION OF STAY
DIAGNOSIS – HIE1/SEPTICAEMIA2/RDS3/MAS4
OBSERVATIONS
1. B.P AT ADMISSION
2. PROTEINURIA AT ADMISSION
3. TIME B/N ADMISSION AND CONVULSION (HOURS)
4. TIME B/N CONVULSION AND DELIVERY (HOURS)
5. TIME B/N ADMISSION AND DELIVERY (HOURS)
6. IMMEDIATE POST DELIVERY B.P.
7. URINE ALBUMIN NIL FOLLOWING DELIVERY
8. MATERNAL COMPLICATIONS
• PULMONARY EDEMA6
• PLACENTAL ABRUPTION/HELLP1
• CEREBRAL INFARCTION3
• UTI2
• PPH4
• CORTICAL BLINDNESS5
9. DURATION OF STAY IN HOSPITAL
10. CONDITION OF MOTHER AND BABY AT DISCHARGE

1 2 3 4 5 6 7 8 9 10 11 13 14 15 16 17 18 19 20 21 22 23 24 25 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48
Sl. No.
Name AgeOccupat
ion
SE Status
Religion
Address
I.P. No DOA DO Del DOD
No Convulsi
ons Before/After
Consciousness
between attacks
Premonitory
symptoms a/b/c/d
Married Life Year
Consanginous/ nonconsanginous
Antenatal
I/II/III
Anc yes/no
BP Recordi
ng
GPE 1/2/3
Eye Conjunctiva 1/2/3
Tongue
1/2/3
Edema a/b/c/d
Vitals/ pulse
RRKJ a/b
Pupils
PA 1/2/3
PV bishop’s score
Haemogram
LFT 1/2/3 USGRFT 1/2
Serum Uric acid
Fundoscopy
VIMSAntihypertesives N/L
VD/CD
B/W ApgarNICU
Diagnosis/Stay
Diagnosis
1/2/3/4
Proteinuria A/D
Admission &
Convulsion
Admission & Deliver
y
Convulsion &
delivery
Complications 1/2/3/4/5/6
Dead
Systole Diastole
1 Jaidunissa 22 Cooli Low M Bellary 500872 1.7.11 2.7.11 8.7.11 3 Y a 1 C N N N 1 1 1 a 82 22 a 2 2 2/10Hb 9.6 Plt.1.6 lacs
26, 30, 429 IU/L
N0.6, 28 DL
4.6 Y Y N CD 2kg6/10 8/10
7dys 21+/Nil 4day
4hrs 24 hrs 26 hrs160 140
100 90
3 Renuka 19 Cooli Low H Bellary 501026 3.7.11 3.7.11 6.7.11 3 Y ab 3 C N N N 3 1 1 a 92 20 b 2 3 2/10Hb 11.2 Plt.2 lacs
60, 67 498 IU/L
N18 0.7
5 Y Y N VD 2kg4/10 6/10
3dys 14+/Nil 4day
6hrs 10 hrs 18 hrs150 130
110 90
4 Kavitha 22 Cooli Low H Bellary 501644 8.7.11 9.7.11 10.7.11 4/1 Y a 3 N Y Y Y 1 1 1 a 80 18 b 2 3 2/10Hb 12.2 Plt.3.8 lacs
28, 19 340 IU/L
Y20 0.6
4.2 Y Y N VD 2.8kg6/10 8/10
‐ ‐3+/Nil 3day
2hrs 6 hrs 6 hrs160 100
140 90
5 Basamma 22 Cooli Low H Bellary 502344 14.7.11 14.7.11 20.7.11 1 Y a 2 N Y Y Y 1 1 1 a 92 20 b 2 3 0/10Hb 11.6 Plt.2.4 lacs
56, 48 378 IU/L
Y22 1
3 Y Y N CD 2.5kg6/10 8/10
3dys 23+/Nil 5day
6hrs 12hrs 18 hrs170 150
120 100
4
6 Honnuramma 30 Cooli Low H Bellary 502999 17.7.11 19.7.11 22.7.11 4/1 Y ab 2 C Y Y Y 1 1 3 a 98 20 b 2 3 2/10Hb 10 Plt.1.6 lacs
21, 16 460 IU/L
Y20 .9
5.6 Y Y N VD 2.5kg6/10 8/10
‐ ‐3+/Nil 5day
5hrs 16hrs 22 hrs170 150
110 100
7 Fathima 18 Cooli Low M Bellary 503865 26.7.11 28.7.11 30.7.11 2 Y a 2 N Y Y Y 1 1 3 a 92 18 a 2 2 0/10Hb 9.5 Plt.2.8 lacs
34, 28 300 IU/L
Y20 .6
6 Y Y N VD 1.5kg ‐ ‐ ‐1+/Nil 2day
4hrs 20hrs 24 hrs140 120
90 80
8 lacshmi 22 Cooli Low H Bellary 504685 2.8.11 3.8.11 6.8.11 2 Y abc 1 N Y Y Y 1 1 1 82 22 a 2 1 2/10Hb 9.6 Plt.1.8 lacs
10, 15 310 IU/L
Y20 .8
7 Y Y N VD 1.7kg6/10 8/10
3dys 32+/Nil 2day
5hrs 18hrs 26 hrs130 128
80 80
9 Maremma 20 Cooli Low H Durga 505803 11.8.11 13.8.11 15.8.11 2 Y ad 2 C Y Y Y 2 1 3 ab 82 20 b 1 1 0/10Hb 9 Plt.1.4 lacs
18, 15 676 IU/L
N20 .8
3.8 Y Y N VD 2kg6/10 8/10
‐ ‐2+/Nil 3day
5hrs 28hrs 30 hrs160 158
100 90
10 Shabana 20 Cooli Low M Hospet 505803 15.8.11 17.8.11 21.8.11 2 Y a 1.6 C Y Y Y 1 1 1 ac 80 22 a 1 3 3/10Hb 12.7 Plt.2.9 lacs
22, 40 520IU/L
N20 .8
4.2 Y Y N VD 2.25kg ‐ ‐ ‐4+/Nil 5day
4hrs 16hrs 20 hrs170 170
110 100
2
11 Kavitha 19 Cooli Low H Bellary 490849 31.3.11 9.4.11 01.4.11 4 Y ac 1 N Y Y Y 2 1 3 a 90 22 b 1 3 4/10Hb 10 Plt.1.5 lacs
30, 34 510IU/L
Y10 1
5.2 Y Y N VD 2.5kg4/10 6/10
3dys 32+/Nil 6day
4hrs 16hrs 20 hrs140 130
100 90
12 Fathima 20 Cooli Low M Bellary 481970 3.1.11 4.1.11 6.1.11 2 Y ac 1 C Y Y Y 1 1 1 a 98 20 b 1 3 4/10Hb 9.3 Plt.1.9 lacs
32, 20 320IU/L
N20 .6
6.7 Y Y N VD 2.5kg6/10 8/10
‐ ‐2+/Nil 4day
6hrs 10hrs 18 hrs150 140
90 90
13 Yashodamma 20 Cooli Low H Bellary 481975 5.1.11 6.1.11 8.1.11 2 Y ac 2 N Y Y Y 1 1 3 a 90 22 a 1 1 3/10Hb 9.8
Plt.1.2lacs20, 40 610IU/L
N20 .1
4.6 Y Y N VD 1.5kg2/10 4/10
5dys1
Death3+/Nil 4day
5hrs 10hrs 20 hrs170 160
110 910
2
14 PusHbalatha 20 Cooli Low H Bellary 482036 4.1.11 5.1.11 8.1.11 2 Y ad 2 N N N N 1 1 1 a 90 20 b 1 1 2/10Hb 9.8 Plt.1.4 lacs
40, 30 610IU/L
N20 .9
3.9 Y Y N VD1.5kg death
‐ 5dys ‐3+/Nil 5day
6hrs 8hrs 16 hrs160 140
100 100
15 Renuka 22 Cooli Low H Bellary 482196 6.1.11 7.1.11 15.1.11 2 Y ac 10m C Y Y Y 3 1 3 ac 100 20 b 1 3 3/10Hb 1.8
Plt.2 lacs20, 28 490IU/L
Y20 .6
4.7 Y Y L CD 2kg 6/10 8/10
28dys 24+/Nil 8day
5hrs 18hrs 24 hrs180 170
110 90
1
16 Sunitha 22 Cooli Low H Bellary 482297 6.1.11 6.1.11 9.1.11 4 Y ab 1.6 N Y Y Y 3 1 1 abd 90 28 b 1 1 3/10Hb 10 Plt.1.8 lacs
20, 35 549IU/L
N 20 5.2 Y Y L VD 1.6kg2/10 2/10
6hous1 death of 6hrs
3+/Nil 4day
5hrs 10hrs 18 hrs170 160
110 100
17 Manjamma 22 Cooli Low H Bellary 482505 9.1.11 10.1.11 13.1.11 2 Y ad 1 N N N N 3 1 1 a 90 20 b 1 1 0/10Hb 11 Plt.1.8 lacs
20, 24 680IU/L
N 20 .6 5.9 Y Y N VD 1.5kg6/10 8/10
‐ ‐1+/Nil 3day
6hrs 10hrs 18 hrs160 140
100 100
18 Sunitha 22 Cooli Low H Bellary 482515 8.1.11 9.1.11 15.1.11 3 Y a 2 N N N Y 1 1 1 ab 92 20 a 1 2 0/10Hb 9.8 Plt.1.6 lacs
40, 20 688IU/L
N 20 .9 4.9 Y Y N VD 1.6kg2/10 4/10
3dys 13+/Nil 6day
5hrs 10hrs 18 hrs170 150
104 100
2
19 Eramma 22 Cooli Low H Bellary 482514 8.1.11 9.1.11 12.1.11 3 Y ac 2 C Y Y Y 1 1 1 ac 90 22 a 1 3 3/10Hb 12 Plt.1.6 lacs
22, 18 688IU/L
Y 24 .1 3.9 Y Y N VD (F) 2.5kg4/10 6/10
‐ ‐1+/Nil 3day
6hrs 8hrs 14 hrs140 130
90 90
20 Shahena Banu 20 Cooli Low M Bellary 482524 9.1.11 10.1.11 13.1.11 2 Y ad 2 N N N N 1 1 1 a 90 20 a 1 2 2/10Hb 10 Plt.2.8 lacs
20, 18 432IU/L
N 24 .9 4.8 Y Y N VD1.5kg death
‐ ‐ ‐4+/Nil 3day
10hrs 6hrs 8 hrs140 130
90 90
21 lacshmidevi 19 Cooli Low H Hospet 480014 17.12.1018.12.1
024.12.10 5/1 Y ac 2 C Y Y Y 1 1 3 abc 92 20 b 1 3 3/10
Hb 10 Plt.1.6 lacs
34, 26 412IU/L
N 20 .9 4.6 Y Y N CD 2.5kg 6/10 8/10
‐ ‐2+/Nil 5day
6hrs 12hrs 16 hrs160 140
100 100
4
22 Kavitha 22 Cooli Low H Bellary 479985 16.12.1018.12.1
027.12.10 2 Y a 2 C N N N 1 1 1 a 90 24 b 1 3 3/10
Hb 9.8 Plt.3.8 lacs
20, 28 786IU/L
N24 1.1
5.1 Y Y N CD 3kg 6/10 8/10
‐ ‐2+/Nil 5day
8hrs 30hrs 34 hrs150 140
100 90
23 Gangamma 19 Cooli Low H Bellary 480025 16.12.1019.12.1
028.12.10 1 Y a 2 C Y Y C 1 1 1 a 92 22 b 1 3 0/10
Hb 13 Plt.1.8 lacs
40, 20 554IU/L
Y20 1.1
3.7 Y Y N CD 3kg 6/10 8/10
2 2 5day4+/Nil 8day
10hrs 36hrs 38 hrs160 140
100 90
24 Kavitha 20 Cooli Low HAnanth pur
482764 11.1.11 12.1.11 14.1.11 2 Y a 1 N Y Y Y 1 1 1 a 92 20 b 1 3 4/10Hb 936 Plt.1.6 lacs
24, 40 436IU/L
Y30 1.0
3.9 Y Y N VD 2kg 6/10 8/10
‐ ‐2+/Nil 3day
6hrs 12hrs 14 hrs160 140
100 90
25 Geetha 22 Cooli Low H Bellary 483032 13.1.11 14.1.11 16.1.11 2 Y a 2 N Y Y Y 1 1 1 a 92 18 b 1 3 0/10Hb 11 Plt.1.4 lacs
30, 20 430IU/L
Y 20 .8 4.8 Y Y N VD 2kg 6/10 8/10
‐ ‐1+/Nil 3day
6hrs 18hrs 20 hrs160 140
100 90
26 Bhagyamma 22 Cooli Low H Bellary 473126 16.10.10 17.10.10 23.10.10 O2 Y a 2 N N N N 1 1 1 a/c 92 22 a 1 3 4/10HB 9.8 PLT 1.8
26,34, 612
Y20, 1.1
5.2 Y Y N CD 2.2Kg7/10, 9/10
‐ ‐2+/1+, 7day
4hrs 18hrs 24 hrs150 140
100 90
27 Rathnamma 21 Cooli Low HAnanth pur
475077 31.10.10 01.11.10 7.11.10 2 Y a 2 C Y Y Y 3 1 3 a/b 92 22 a 1 3 4/10HB 12.8 PLT 2.7
35,28, 465
N21,0.9
4.7 Y Y N VD 1‐75Kg4/10,6/10
2 3days3+/NIL, 4day
3.5hrs 24hrs 26 hrs160 130
90 80
MASTER CHART
BP Admision & Delivery

28 Mahadevi 19 Cooli Low H Bellary 475009 2.11.10 3.11.10 7.11.10 1 Y a 1 N Y Y Y 1 1 1 c 92 20 a 1 1 4/10Hb 10.5 plt 2.66
16,12, 500
y15,0.9
5.6 y n N VD 2.25Kg6/10,7/10
0 03+/NiL, 3days
30min 16hrs 12 hrs150 130
100 80
29 Rahimbee 20 Cooli Low H Bellary 475328 2.11.10 3.11.10 6.11.10 1 Y a 2 C Y Y Y 1 1 1 a 80 20 a 1 3 0/10Hb 10 plt
1.830,20, 310 N
20,0.9
4.6 Y Y N VD 2Kg7/10,9/10
0 0 0 8hrs 12hrs 18 hrs140 110
90 80
30 Shwetha 20 Cooli Low H Hospet 475325 2.11.10 3.11.10 1O.11.10 1 Y a 1 C Y Y Y 1 1 1 a 80 20 b 1 3 4/10Hb 10 PLT 2 iaks
42,33,215 Y20, 0.9
4.3 Y Y N CD 2.5Kg6/10,8/10
0 0 0 30min 10hrs 6 hrs200 160
120 100
31 Wahida 23 Cooli Low M Bellary 476299 11.11.10 12.11.10 15.11.10 1 Y a/c/d 2 N Y Y Y 1 1 1 a 82 18 a 1 3 0/10Hb 9.6 plt
2.4721,25, 390
y19, 0.7
4.8 Y Y N VD 2.5Kg7/10,9/10
0 01+/nil 3day
3hrs 10hrs 14 hrs130 120
90 90
32 Vedavathi 25 Cooli Low H Bellary 476576 16.11.10 17.11.10 19.11.10 2 Y a 7 N Y Y Y 1 1 1 a 82 20 a 1 3 4/10Hb 9 plt 2.1
43,26, 315
y19, 0.7
3.9 N Y N VD 1.5Kg7/10,9/10
2 41+/NIL 3DAY
3hrs 10hrs 20 hrs148 110
100 80 5
33 Banu 25 Cooli Low m Bellary 476879 16.11.10 17.11.10 20.11.10 2 Y a 1 C Y Y N 1 1 3 a/b 80 20 a 1 3 4/10Hb 12 plt
1.840,30, 162
y27, 1.1
3.7 Y Y N VD 2Kg7/10,9/10
0 01+/nil 3day
10hrs 18hrs 26 hrs160 140
100 90
34 Huligamma 25 Cooli Low H Bellary 479162 8.12.10 9.12.10 13.11.10 1 Y a 6 C N N N 1 1 1 a 82 22 a 1 3 4/10Hb 12.8 PLT 2 iak
30,38, 728
n13. 0.9
5.1 Y Y N VD 1.75Kg7/10,9/10
1 43+/NIL 4day
2hrs 10hrs 16 hrs150 130
100 80
35 Sarita 25 Cooli Low H Bellary 479088 7.12.10 8.12.10 12.12.10 1 Y a 2 N Y Y Y 1 1 1 a/b 82 22 a 1 1 4/10Hb 9.4 plt
3.218,14,3 52
Y21, 0.9
5.1 Y Y N VD 2Kg7/10,9/10
0 03+/NIL 6day
10hrs 18hrs 18 hrs180 134
100 90
36 Radha 19 cooli low H Bellary 479304 9.12.10 9.12.10 12.12.10 1 Y abc 2 c N N N 1 1 1 ab 92 20 a 1 1 4/10Hb 13
plt2.11,21,16.
1,21,16614, 0.7
4.9 Y Y n VD 2Kg6/10 8/10
1+/nil 4day
4 hrs 6hrs 16 hrs140 100
140 100
37 Nagveni 23 cooli low H Bellary 485159 3.2.11 4.2.11 7.2.11 1 Y a 1 N N N N 1 1 1 a 80 22 a 1 2 0/10Hb10.4plt1.093634
490
30,20, 520
n20 0.9
4.5 Y y n VD 1.5Kg6/10, 8/10
3+nil 3day
5hrs 24hrs 28 hrs170 150
100 90
38 Jayamma 22 cooli low H Bellary 485341 5.2.11 6.2.11 13.2.11 1 Y a 2 c N N N 1 1 1 a 92 20 b 1 3 4/10Hb10.4plt3.235,34,
5.8
20,10, 500
y20, 1.1
5.2 Y y L CD 2.5Kg6/10 8/10
3+nil 5day
6 hrs 24hrs 28 hrs190 100
160 100
39 Priyanka 22 cooli low H Hospet 485610 8.2.11 8.2.11 10.2.11 4 Y a 2 N Y Y Y 1 1 3 a 5 20 b 1 2 4/10Hb9plt1.836,20,62
10,10, 200
n24 1.1
5.1 Y y N VD 1.5 IUD1+nil 2day
3hrs 6hrs 10 hrs150 140
110 90
40 Huligemma 23 cooli low H Bellary 486132 13.2.11 13.2.11 15.2.11 1 Y a 2 c Y Y Y 1 1 3 a 90 22 b 1 3 4/10Hb9.2plt2.3,70,72,6
20
30,40, 360
n20 0.8
4.6 Y N N VD 2.8Kg7/10 9/10
2+nil 3day
1hr 6hrs 6 hrs160 140
110 90
41 Honnamma 24 cooli low H Bellary 486402 15.2.11 16.2.11 18.2.11 2 Y a 3 N Y Y Y 1 1 1 ab 80 18 b 1 1 4/10Hb9.1plt80000,28,19,396
20,30, 400
y21 0.8
4.7 Y Y N VD 1.5Kg6/10 8/10
2 42+nil 4day
6hr 18hrs 22 hrs174 160
110 90
42 Gangamma 19 Cooli Low H Bellary 486469 16.02.11 16.02.11 23.02.11 1 Y a 2 N Y Y Y 1 1 1 a 80 22 b 1 3 3/10Hb 9 plt 1.2lac
63,51, 490
Y20, 0.9
3.9 Y Y N CD 2.5Kg4/10 6/10
4 NND3+/Nil 5day
2hrs 6hrs 10 hrs140 140
90 90
43 Jayamma 22 Cooli Low H Bellary 486448 16.2.11 16.2.11 24.2.11 2 Y a 2 C N N N 1 1 3 a 90 20 a 1 3 4/10Hb 9 plt 1.9
30,20, 257
n20, 0.9
3.6 Y Y N CD 2Kg6/10 7/10
0 02+/NIL 3DAY
3hrs 16hrs 12 hrs146 130
96 90
44 Yasmeen 20 Cooli Low M Bellary 486896 21.2.11 22.2.11 1.3.11 2 Y a/d 2 N N N N 1 1 1 a 82 20 a 1 3 4/10Hb 10.8 plt 2lacs
13,14, 310
n22, 0.8
4.7 Y Y N CD 2Kg6/10 8/10
0 02+/Nil 4day
6hrs 16hrs 10 hrs144 140
90 90
45 lacshmamma 22 Cooli Low h Bellary 487884 2.3.11 3.3.11 10.3.11 1 Y a/d 3 C Y Y Y 1 1 1 a 90 22 a 1 3 4/10Hb9.2 plt 2.3lac
42,32, 525
y30, 1.1
4.2 Y Y N CD 2.5Kg6/10 8/10
0 03+/Nil 4day
4hrs 6hrs 12 hrs150 130
110 100
46 Mallamma 22 Cooli Low h Bellary 488674 4.3.11 5.3.11 12.3.11 2 Y a 2 C Y Y Y 1 1 1 a 82 22 a 1 2 4/10Hb 9.9 plt
1.829,31, 512
Y26,0.2
3.9 Y Y N CD 1.5kg6/10,8/10
2 43+/6da
y2hrs 6hrs 10 hrs
150 148
90 80
47 Yellamma 22 Cooli Low H Bellary 487924 3.3.11 4.3.11 10.3.11 1 Y a 2 C Y Y Y 1 1 1 a 80 20 a 1 2 4/10Hb 9.2 plt 1.8lac
42,40, 752
y28, 1.1
3.9 Y Y N CD 2Kg6/10,8/10
0 02+/nil6day
6hrs 8hrs 20 hrs150 130
110 90
48 Shanthamma 25 Cooli Low h Bellary 488267 6.3.11 6.3.11 10.3.11 1 Y a 1 C Y Y Y 1 1 1 a 82 20 b 1 1 0/10Hb 9 plt 2lac
30,26, 567
y20, 0.9
3.7 Y Y N VD 1.75Kg6/10 7/10
5 22+/NIL4day
6hrs 10hrs 18 hrs160 150
90 90
49 Pavithra 20 Cooli Low H Bellary 488533 8.3.11 9.3.11 11.3.11 1 Y a 3 N Y Y Y 1 1 1 a 90 20 b 1 3 4/10Hb 9 plt 2lac
15,30, 423
Y22, 0.9
3.8 Y Y N VD 2.5Kg6/10 8/10
0 01+/nil 2day
8hrs 12hrs 18 hrs170 150
100 90
50 Lagmavva 19 Cooli Low h Belgaum 488598 9.3.11 9.3.11 12.3.11 2 Y a/d 1 N N N N 1 1 1 a 90 20 b 1 1 4/10HB 9.1 plt 1.3lac
30,35, 875
y20, 1.2
5.8 Y Y N VD 1.5Kg6/10 8/10
2 NND 3day2+/nil 3day
3hrs 8hrs 10 hrs150 150
100 100
51 Ambujakshi 23 Cooli Low H Tumkur 488774 11.3.11 12.3.11 19.3.11 2 y a 2 c Y Y Y 1 1 1 a/b/d 82 22 a 1 3 4/10Hb 8.8 ply 2.8lac
20,26, 4800
y24, 0.6
4.9 Y Y N CD 2.5Kg6/10 8/10
0 02+/NIL 6day
6hrs 12hrs 18 hrs150 140
100 90
52 Sunitha 18 Cooli Low H Bellary 489509 18.3.11 19.3.11 26.3.11 1 Y a 1 N Y Y Y 1 1 1 a/c 80 18 b 1 3 4/10Hb 10.3 plt 1.2
30,20, 504
Y20, 1.1
5.1 Y Y N CD 2kg6/10 8/10
0 02+/nil 5day
6hrs 18hrs 20 hrs160 160
100 90
53 Rathnamma 18 Cooli Low H Bellary 489129 13.3.11 14.3.11 19.3.11 2 Y a 1 C Y Y Y 1 1 1 a 92 20 b 1 3 0/10Hb 8.2 plt 2.6lac
16,22, 420
Y20, 04
4.7 Y Y N VD 2Kg4/10 6/10
2 12+/nil 5day
4hrs 6hrs 10 hrs140 130
90 80
54 Shaheen 22 Cooli Low M Bellary 489174 20.3.11 20.3.11 24.3.11 4 Y a 1 C N N N 1 1 1 a 80 20 b 1 3 4/10Hb 11 plt 1.5lac
53,47, 490
Y24, 0.8
5.1 Y Y N VD 2Kg dead 0 02+/nil 3day
10hrs 8hrs 18 hrs150 150
100 100
55 Radhamma 25 Cooli Low H Bellary 489310 16.3.11 16.3.11 22.3.11 6 Y a 10m N Y Y Y 3 1 3 a/b/c 90 20 b 1 3 4/10HB 9.8 PLT 1.8
20,24, 512
N20, 0.9
4.9 Y Y N VD 2KgSTILL birth
0 03+/nil 8day
4hrs 6hrs 10 hrs150 140
110 110
56 Deenakumari 23 Cooli Low C Bellary 488122 10.3.11 11.3.11 18.3.11 6 Y a/d/e 2 C Y Y Y 1 1 3 a/d 92 18 a 1 3 0/10Hb 9.2 plt 1.5lac
18,20, 600
Y16, 0.9
3.9 Y Y N CD 2Kg6/10 8/10
0 02+/NIL 4day
2hrs 10hrs 14 hrs150 160
100 100
57 Gouramma 22 Cooli Low H Bellary 490246 25.3.11 26.3.11 29.3.11 2 Y a 1 C N N N 3 1 3 a/d 92 18 a 2 2 40818Hb 9.8 plt
1.630,10, 600
N20, 0.9
3.7 Y Y N VD 1.5kg dead 0 0 2+ 6hrs 14hrs 16 hrs150 160
110 110 1 Y
58 Manjula 22 Cooli Low H Bellary 490188 24.3.11 28.3.11 1.4.11 2 Y a 1 N N N N 1 1 3 a 82 20 b 1 1 0/10Hb 9.2 plt 1.7lac
34,24, 400
N20, 0.8
3.6 Y Y N VD 1.8Kg4/10 6/10
4 12+/nil 3day
2hrs 72hrs 30 hrs140 120
90 80

59 Manjamma 22 Cooli Low H Koppal 491052 3.4.11 4.4.11 6.4.11 2 Y a/b 4 N Y Y Y 1 1 1 a 90 20 a 1 1 0/10Hb 8.8 plt 1.6lac
21,16, 520
Y28, 1.1
4.5 Y Y N CD 1.5Kg 2 22+/NIL 4day
6hrs 12hrs 11 hrs160 140
100 100
60 Gangamma 22 Cooli Low h Bellary 491142 3.4.11 4.4.11 11.4.11 10 Y a/b/c/d 4 N Y Y Y 1 1 3 a/b 82 20 a 2 3 0/10Hb 10.7 plt 1.7
20,18, 510
Y18, 0.6
4.8 Y Y N CD 2.5Kg6/10 8/10
0 02+/nil 7day
6hrs 12hrs 18 hrs160 150
110 100
61 Hanumanthi 21 Cooli Low H Lingasur 491748 9.4.11 10.4.11 13.4.11 6 Y a/b 1 C Y Y Y 1 1 1 a/d 82 20 a 1 3 4/10Hb 11.2 plt 1.4lac
20,28, 560
Y18, 0.8
4.1 Y Y N VD 2.5Kg6/10 6/10
2 NND1+/nil 3day
13hrs 12hrs 18 hrs120 120
90 90
62 Sharada 20 Cooli Low H Hospet 482305 15.1.11 21.1.11 2.1.11 1 Y a/b 2 C N N N 2 1 1 a 90 24 b 1 1 2/10Hb 9.8 plt 1.8 lac
30,50, 478
Y20, 0.9
4.2 Y Y N VD 2.Kg6/10 8/10
1+/nil 5day
6hrs 18hrs 20 hrs120 120
90 90
63 Mahalacshmi 22 Cooli Low H Bellary 484211 25.1.11 26.1.11 29.1.11 4 Y a/c 2 C Y Y Y 1 1 1 a/b 92 22 b 1 3 4/10Hb 9.8 plt 1.6 lac
38,30, 485
Y20, 0.8
5.1 Y Y L VD 2.Kg6/10 8/10
1+/nil 2day
6hrs 8hrs 10 hrs180 140
110 100
64 Nagavani 20 Cooli Low H Bellary 484003 23.1.11 23.1.11 30.1.11 2 Y a/c 2 C Y Y Y 2 1 2 a/c 92 20 b 1 3 0/10Hb 9.6 plt 3.3 lac
30,28, 390
Y20, 0.9
4.7 Y Y L CD 3 Kg6/10 5/10
3+/nil 6day
6hrs 6hrs 12 hrs170 100
120 90
65 Mallamma 20 Cooli Low H Bellary 484043 23.1.11 21.1.11 28.1.11 1 N a/b 2 C N N N 2 1 1 a 90 20 a 1 3 3/10Hb 9.2 plt 1.3 lac
36, 30, 516
Y28, 0.9
4.6 Y Y N VD 2.5 Kg1/10 6/10
2 23+/nil 5day
10hrs 12hrs 24 hrs150 150
108 100
66 Kamalamma 25 Cooli Low H Bellary 484024 23.1.11 24.1.11 30.1.11 2 Y a/c 1 C N N N 1 1 1 a/c 96 20 b 1 3 2/10Hb 9.8 plt 2.1 lac
30, 20, 400
Y20, 0.9
3.9 Y Y N CD 3 Kg6/10 8/10
2+/nil 5day
4 hrs 10 hrs 16 hrs140 130
100 90
67 Gangamma 22 Cooli Low H Bellary 484430 27.1.11 28.1.11 02.2.11 3 Y a/b 2 N Y Y Y 1 1 1 a 92 20 b 1 3 4/10Hb 10 plt 2.1 lac
40, 40, 502
Y20, 0.8
3.2 Y Y N VD 2.5 Kg2/10 4/10
1+/nil 4day
2 hrs 10 hrs 12 hrs140 130
100 80
68 Sujatha 23 Cooli Low H Bellary 484415 27.1.11 27.1.11 30.1.11 2 Y a/c 2 N Y Y Y 1 1 1 a 88 20 b 1 3 3/10Hb 9.8 plt 2.1 lac
20, 30, 586
Y20, 0.9
3.7 Y Y N VD (F) 2.4 Kg6/10 8/10
1+/nil 4day
6 hrs 10 hrs 18 hrs140 130
100 100
69 Mallamma 20 Cooli Low HAnanth pur
484378 26.1.11 27.1.11 30.1.11 2 N a 2 N Y Y Y 1 1 1 a 90 20 b 1 3 2/10Hb 11 plt 1.8 lac
20, 40, 410
Y21, 1.0
3.8 Y Y N VD 2.2 Kg6/10 5/10
2+/nil 3day
6 hrs 10 hrs 18 hrs150 140
100 100
70 Gayathri 20 Cooli Low H Bellary 484553 28.1.11 08.1.11 04.1.11 4/1 N a/b/c/d 1.6 N Y Y Y 2 1 3 a 96 22 a 1 3 0/10Hb 10 plt 2.4 lac
20, 72, 1000
Y28, 1.2
4.1 Y Y N CD 3 Kg6/10 8/10
3+/nil 10day
4 hrs 6 hrs 12 hrs170 160
100 100
71 lacshmi 18 Cooli Low H Bellary 479247 09.12.10 10.02.10 13.12.10 3 Y a 1 N N N N 1 1 1 a 90 20 a 1 1 2/10Hb 9.8 plt 1.4 lac
20, 28, 510
Y20, 0.9
4.6 Y Y N VD 1.6 kg4/10 6/10
3 23+/nil 10day
6 hrs 12 hrs 16 hrs150 130
100 90
72 lacshmi 18 Cooli Low H Bellary 480689 22.12.10 23.02.10 1.1.11 3 Y a 1 N N N N 1 1 1 a 90 20 b 1 3 2/10Hb 10 plt 1.8 lac
30, 20, 600
Y30, 0.9
4.5 Y Y N CD 2 kg6/10 8/10
2NND3+/nil 7day
8 hrs 18 hrs 24 hrs160 150
100 100
73 Shanthamma 20 Cooli Low H Bellary 510201 17.09.11 17.09.11 25.09.11 1 Y a 1 N Y Y Y 2 1 1 a 92 20 a 1 3 0/10Hb 12.6 plt 2.97 lac
22, 17, 439
Y60, 0.9
4.9 Y Y N CD 2.5 kg6/10 8/10
3+/nil 7day
4 hrs 8 hrs 13 hrs160 130
100 90
74 Sujatha 18 Cooli Low H Bellary 510285 18.09.11 19.09.11 27.09.11 5 Y a/b 1 C Y Y Y 2 1 1 a 80 20 b 1 3 2/10Hb 8.9 plt 3.3 lac
28, 19, 1330
Y12, 0.6
5.1 Y Y N CD 3 kg6/10 8/10
1+/nil 3day
4 hrs 12 hrs 12 hrs170 160
100 100
5
75 Jyothi 18 Cooli Low H Bellary 509383 11.09.11 11.09.11 19.09.11 2 Y a 1 C Y Y Y 2 1 3 a 90 22 b 1 3 2/10Hb 10.8 plt 1.6 lac
20, 30, 420
Y20, 0.9
5.2 Y Y N CD 2 kg4/10 4/10
3 NND2+/nil 7day
6 hrs 6 hrs 12 hrs160 110
100 70
76 Anitha 22 Cooli Low H Bellary 511372 26.09.11 26.09.11 03.10.11 2 Y a/d 1 C Y Y Y 1 1 1 a 80 18 b 1 3 4/10Hb 10 plt 4.1 lac
12, 10, 1099
Y20, 1.4
5.8 Y Y N CD 3 kg6/10 8/10
1+/nil 4day
2 hrs 6 hrs 8 hrs140 130
94 90
77 Nagalacshmi 19 Cooli Low H Bellary 480600 22.12.10 22.12.10 24.12.10 2 Y a/c 2 N N N N 1 1 1 a 84 20 a 1 3 2/10Hb 10 plt 1.26 lac
20, 10, 560
N20, 1.9
3.8 Y Y N VD 1.5kg4/10 4/10
2 NND2+/nil 1day
8 hrs 12 hrs 18 hrs150 150
100 100
78 lacshmi 18 Cooli Low H Bellary 480681 22.12.10 23.12.10 30.12.10 2 Y a 1 C Y Y Y 2 1 1 a/d 90 20 a 1 3 2/10Hb 10 plt 1.26 lac
16, 20, 612
N 28, 1 3.9 Y Y N CD 2 kg6/10 8/10
2+/nil 7day
6 hrs 12 hrs 16 hrs170 100
160 100
79 Vedavathi 18 Cooli Low H Bellary 480693 24.12.10 24.12.10 02.01.11 2 Y a/d 1.6 C Y Y Y 1 1 1 a 90 22 a 1 3 2/10Hb 9.8 plt 1.6 lac
30, 28, 420
Y20, 1.9
5.6 Y Y N CD 3 kg6/10 8/10
3+/nil 8day
4 hrs 6 hrs 12 hrs160 140
100 90
80 Varalacshmi 19 Cooli Low H Bellary 480712 25.12.10 26.12.10 03.01.11 2 Y a/c 1 C N N N 2 1 1 a/d 92 22 b 1 3 2/10Hb 10 plt 1.8 lac
18, 30, 850
N32, 1.1
4.7 Y Y N CD 3 kg6/10 8/10
4+/nil 7day
4 hrs 16 hrs 18 hrs170 150
100 90
3
81 Shanthi 19 Cooli Low H Bellary 471385 01.01.10 02.10.10 05.10.10 2 Y b 1 N Y Y Y 1 1 2 a 90 20 a 1 3 2/10Hb 10.8 plt 1.8 lac
36, 24, 133
Y28, 0.1
5.7 Y Y N VD 2.5 kg6/10 8/10
3 hrs 12 hrs 16 hrs160 130
110 100
82 lacshmi 19 Cooli Low H Bellary 473910 24.10.10 24.10.10 28.10.10 2 Y a/c 1 N Y Y Y 1 1 1 a 88 22 a 1 3 5/10Hb 10 plt 1.8 lac
25, 18, 460
Y18, 0.7
5.1 Y Y N VD 2.5 kg7/10 9/10
1+/nil 3day
4 hrs 10 hrs 16 hrs160 130
110 90
83 Asma 22 Cooli Low M Bellary 473137 17.10.10 18.10.10 21.10.10 1 Y a/c 2 N Y Y Y 1 1 1 a 82 18 a 1 3 4/10Hb 10.2 plt 1.7 lac
30, 45, 610
Y20, 1.1
5.4 Y Y N VD 2.5 kg6/10 8/10
2+/nil 4day
4 hrs 8 hrs 13 hrs150 140
110 90
84 Pavithra 24 Cooli Low H Bellary 473090 16.10.10 17.10.10 20.10.10 2 Y a 1.6 N N N N 1 1 1 a 82 20 a 1 3 3/10Hb 10 plt 2.5 lac
20, 80, 342
N20, 0.8
3.6 Y Y N VD 2 kg6/10 8/10
2+/nil 4day
4 hrs 12 hrs 16 hrs150 140
96 90
6
85 Shantha 24 Cooli Low H Bellary 472145 08.10.10 09.10.10 12.10.10 1 Y a 1 C N N N 1 1 1 a 82 18 a 1 1 2/10Hb 9 plt 1.6 lac
35, 30, 500
N25, 0.6
4 Y Y N VD 2 kg6/10 8/10
1+/nil 3day
6 hrs 12 hrs 16 hrs160 140
90 90
86 Rudramma 22 Cooli Low H Bellary 492024 12.4.11 13.04.11 16.04.11 1 Y a 2 C N N N 1 1 1 a/d 80 20 b 1 1 0/10Hb 10.08 plt 2.33 lac
22, 70, 479
N11, 0.7
3 Y Y N VD 1.6 kg4/10, 6/10
1+/nil 4day
6 hrs 8 hrs 10 hrs140 130
94 90
87 Neelamma 28 Cooli Low H Bellary 492312 13.4.11 14.04.11 16.04.11 2 Y a 3 N N N N 1 1 1 a/b 82 22 a 1 3 2/10Hb 13.2 plt 1.8 lac
32, 28, 400
N22, 1.2
4.5 Y Y N VD 2 kg4/10, 6/10
3+/nil 5day
6 hrs 12 hrs 16 hrs140 140
100 90

88 Chandramma 22 Cooli Low H Bellary 494107 01.05.11 02.05.11 05.05.11 1 Y a/c 2 C Y Y Y 1 1 1 a 92 22 a 1 3 2/10Hb 9.2 plt 1.67lac
30, 20, 300
Y38, 0.8
4.7 Y Y N VD 2 kg6/10, 8/10
1+/nil 3day
8 hrs 10 hrs 18 hrs170 100
160 100
3
89 Honnur Bee 22 Cooli Low H Bellary 494642 07.05.11 08.05.11 12.05.11 1 Y a/d 2 C Y Y Y 1 1 1 a 90 22 a 1 3 3/10Hb 10.3
plt 2.15lac
33, 28, 858
N20, 0.6
3.6 Y Y N CD 2.8 kg6/10, 8/10
3+/nil 8day
4 hrs 6 hrs 6 hrs200 140
120 90
90 Jayashree 25 Cooli Low H Bellary 496247 21.05.11 22.05.11 28.05.11 2 Y a/d 2 N Y Y Y 1 1 1 a 92 20 a 1 3 0/10Hb 10.3 plt 2.8lac
25, 40, 223
N20, 0.6
5.1 Y Y N CD 2.5 kg6/10, 8/10
1+/nil 2day
6 hrs 12 hrs 18 hrs140 130
90 80
91 Huligemma 20 Cooli Low H Bellary 496061 19.05.11 20.05.11 27.05.11 5 Y a/d 2 N Y Y Y 1 2 1 a 82 20 a 1 3 2/10Hb 11.3 plt 2.8lac
24, 32, 380
N22, 0.8
4.9 Y Y N CD 3 kg6/10, 8/10
3+/nil 5day
4 hrs 6 hrs 26 hrs150 140
90 90
92 Rekhamma 19 Cooli Low H Bellary 498028 06.06.11 07.06.11 07.06.11 3 Y a 1.6 N N N N 1 1 1 a 82 20 a 1 3 2/10Hb 11.4 plt 2.4lac
27, 21, 605
N21, 0.7
3.8 Y Y N CD 2.5 kg6/10, 8/10
2+/nil 7day
10 hrs 16 hrs 18 hrs150 140
120 90
93 Thippamma 20 Cooli Low H Bellary 498933 09.06.11 09.06.11 13.06.11 1 Y a 1 N N N N 1 1 1 a 90 18 a 1 3 4/10Hb 9.8 plt 1.6 lac
20, 30, 340
N26, 0.7
5.7 Y Y N VD 2.5 kg6/10, 8/10
1+/nil 4day
6 hrs 12 hrs 6 hrs150 140
100 90
1
94 Ademma 20 Cooli Low H Bellary 498930 09.06.11 10.06.11 17.06.11 2 Y c 1 N Y Y Y 1 1 1 a 82 20 b 1 3 0/10Hb 8.8 plt 2.9 lac
23, 70, 761
N28, 0.7
3.9 Y Y N CD 2.5 kg6/10, 8/10
12 hrs 18 hrs 18 hrs190 160
110 100
95 Sudha 22 Cooli Low H Bellary 498619 11.06.11 11.06.11 15.06.11 2 Y a/d 1 N N N N 1 1 1 a/d 82 20 b 1 3 3/10Hb 11 plt 1.8 lac
31, 24, 300
N20, 0.1
3.7 Y Y N CD 2.5 kg6/10, 8/10
1+/nil 5day
10 hrs 6 hrs 16 hrs150 140
100 100
96 Ananthamma 22 Cooli Low H Hospet 499320 17.06.11 18.06.11 20.06.11 5 Y a/b/c 1 N N N N 2 1 1 a 82 20 b 1 3 2/10Hb 9 plt 1.8 lac
31, 40, 520
N28, 0.1
4.5 Y Y N VD 2 kg6/10, 8/10
3+/nil 5day
10 hrs 12 hrs 16 hrs160 160
110 100
97 Rajamma 21 Cooli Low H Hospet 484881 31.01.11 01.02.11 04.02.11 2 Y a/b 1 N N N N 2 1 1 a 92 20 b 1 3 3/10Hb 10.2 plt 1.9 lac
36, 30, 610
N20, 0.9
4. Y Y N VD 2.5 kg7/10, 9/10
6 hrs 12 hrs 18 hrs150 150
110 100
98 Kuchamma 20 Cooli Low HChitradurga
472475 13.10.10 14.10.10 21.10.10 6/1 Y a/b/c/d/e 1 N N N N 1 2 3 a 96 22 a 1 3 2/10Hb 10.4 plt 1.33 lac
32, 25, 680
N20, 1.3
5.1 Y Y N CD 2.5 kg4/10, 6/10
11+/nil 4day
4 hrs 10 hrs 26 hrs170 150
100 90
99 Shahida 22 Cooli Low M Bellary 495565 15.5.11 17.5.11 24.5.11 2 y a/c 1 N N N N 1 2 1 a 90 20 a 1 3 0/10Hb 10 Plt 1.8 lac
15,20,450 N 20,1 3.2 Y Y N CD 3 kg 6/10, 8/10
2+/nil 6day
6 hrs 18 hrs 22 hrs170 150
110 90
100 RAthnamma 22 Cooli Low H Bellary 495913 18.5.11 20.5.11 28.5.11 3 Y a/c 1 N N N N 1 2 3 a 88 18 a 1 3 2/10Hb 9.8 plt 1.8 lac
15,14,520 N 18,.9 4 Y Y N CD 3 kg 6/10, 8/10
1+/7 day
4 hrs 40 hrs 18 hrs140 130
100 90

CT IMAGING IN ECLAMPSIA
CT IMAGING SHOWING PARIETAL LOBE INFARCTION IN ECLAMPSIA

CT IMAGING SHOWING OCCIPITAL LOBE INFARCTION IN ECLAMPSIA