Comparative effectiveness of pharmacologic and endoscopic ... · Comparative effectiveness of...
12
Introduction Although endoscopic retrograde cholangiopancreatography (ERCP) is commonly performed for diagnosis and management of pancreato-biliary disease, the procedure itself may result in a host of potential adverse events (AEs) – the most common of Comparative effectiveness of pharmacologic and endoscopic interventions for prevention of post-ERCP pancreatitis: a network meta-analysis Authors Basile Njei 1,* , Thomas R. McCarty 2,3,* , Thiruvengadam Muniraj 1 , Prabin Sharma 4 , Priya A. Jamidar 1 , Harry R. Aslanian 1 , Shyam Varadarajulu 5 , Udayakumar Navaneethan 5 Institutions 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut, United States 2 Department of Gastroenterology, Hepatology and Endoscopy, Brigham and Women’s Hospital, Boston, Massachusetts, United States 3 Harvard Medical School, Boston, Massachusetts, United States 4 Department of Gastroenterology and Hepatology, Yale New Haven Health-Bridgeport Hospital, Bridgeport, Connecticut, United States 5 Center for Interventional Endoscopy, Florida Hospital, University of Central Florida College of Medicine, Orlando, Florida, United States submitted 7.2.2019 accepted after revision 12.8.2019 Bibliography DOI https://doi.org/10.1055/a-1005-6366 | Endoscopy International Open 2020; 08: E29–E40 © Georg Thieme Verlag KG Stuttgart · New York eISSN 2196-9736 Corresponding author Basile Njei, MD, MPH, Yale University School of Medicine, 333 Cedar St, New Haven, CT 06520 Fax: +1-860-679-3159 [email protected] ABSTRACT Background and study aims While several interventions may decrease risk of post-endoscopic retrograde cholan- giopancreatography (ERCP) pancreatitis, it remains unclear whether one strategy is superior to others. The purpose of this study was to compare the effectiveness of pharmacolo- gic and endoscopic interventions to prevent post-ERCP pancreatitis among high-risk patients. Methods A systematic review was performed to identify randomized controlled trials from PubMed, Embase, Web of Science, and Cochrane database through May 2017. In- terventions included: rectal non-steroidal anti-inflamma- tory drugs (NSAIDs), aggressive hydration with lactated ringerʼs (LR) solution, and pancreatic stent placement com- pared to placebo. Only studies with patients at high-risk for post-ERCP pancreatitis were included. Bayesian network meta-analysis was performed and relative ranking of treat- ments was assessed using surface under the cumulative ranking (SUCRA) probabilities. Results We identified 29 trials, comprising 7,862 partici- pants comparing four preventive strategies. On network meta-analysis, compared with placebo, rectal NSAIDs (B= – 0.69, 95% CI [–1.18; – 0.21]), pancreatic stent (B= – 1.25, 95 % CI [–1.81 to –0.69]), LR (B = – 0.67, 95 % CI [–1.20 to –0.13]), and combination of LR plus rectal NSAIDs (B= – 1.58; 95 % CI [–3.0 to –0.17]), were all associated with a reduced risk of post-ERCP pancreatitis. Pancreatic stent placement had the highest SUCRA probability (0.81, 95 % CI [0.83 to 0.80]) of being ranked the best prophylactic treatment. Conclusions Based on this network meta-analysis, pancre- atic stent placement appears to be the most effective pre- ventive strategy for post-ERCP pancreatitis in high-risk pa- tients. Original article * Drs. Njei and McCarty: These authors contributed equally. Supplementary material Online content viewable at: https://doi.org/10.1055/a-1005-6366 Njei Basile et al. Comparative effectiveness of … Endoscopy International Open 2020; 08: E29–E40 E29 Published online: 2020-01-08
Transcript of Comparative effectiveness of pharmacologic and endoscopic ... · Comparative effectiveness of...

IntroductionAlthough endoscopic retrograde cholangiopancreatography(ERCP) is commonly performed for diagnosis and managementof pancreato-biliary disease, the procedure itself may result in ahost of potential adverse events (AEs) – the most common of
Comparative effectiveness of pharmacologic and endoscopicinterventions for prevention of post-ERCP pancreatitis:a network meta-analysis
Authors
Basile Njei1, *, Thomas R. McCarty2, 3, *, Thiruvengadam Muniraj1, Prabin Sharma4, Priya A. Jamidar1, Harry R.
Aslanian1, Shyam Varadarajulu5, Udayakumar Navaneethan5
Institutions
1 Section of Digestive Diseases, Yale University School of
Medicine, New Haven, Connecticut, United States
2 Department of Gastroenterology, Hepatology and
Endoscopy, Brigham and Women’s Hospital, Boston,
Massachusetts, United States
3 Harvard Medical School, Boston, Massachusetts, United
States
4 Department of Gastroenterology and Hepatology, Yale
New Haven Health-Bridgeport Hospital, Bridgeport,
Connecticut, United States
5 Center for Interventional Endoscopy, Florida Hospital,
University of Central Florida College of Medicine,
Orlando, Florida, United States
submitted 7.2.2019
accepted after revision 12.8.2019
Bibliography
DOI https://doi.org/10.1055/a-1005-6366 |
Endoscopy International Open 2020; 08: E29–E40
© Georg Thieme Verlag KG Stuttgart · New York
eISSN 2196-9736
Corresponding author
Basile Njei, MD, MPH, Yale University School of Medicine,
333 Cedar St, New Haven, CT 06520
Fax: +1-860-679-3159
ABSTRACT
Background and study aims While several interventions
may decrease risk of post-endoscopic retrograde cholan-
giopancreatography (ERCP) pancreatitis, it remains unclear
whether one strategy is superior to others. The purpose of
this study was to compare the effectiveness of pharmacolo-
gic and endoscopic interventions to prevent post-ERCP
pancreatitis among high-risk patients.
Methods A systematic review was performed to identify
randomized controlled trials from PubMed, Embase, Web
of Science, and Cochrane database through May 2017. In-
terventions included: rectal non-steroidal anti-inflamma-
tory drugs (NSAIDs), aggressive hydration with lactated
ringerʼs (LR) solution, and pancreatic stent placement com-
pared to placebo. Only studies with patients at high-risk for
post-ERCP pancreatitis were included. Bayesian network
meta-analysis was performed and relative ranking of treat-
ments was assessed using surface under the cumulative
ranking (SUCRA) probabilities.
Results We identified 29 trials, comprising 7,862 partici-
pants comparing four preventive strategies. On network
meta-analysis, compared with placebo, rectal NSAIDs
(B =–0.69, 95% CI [–1.18;–0.21]), pancreatic stent
(B =–1.25, 95% CI [–1.81 to –0.69]), LR (B =–0.67, 95% CI
[–1.20 to –0.13]), and combination of LR plus rectal NSAIDs
(B =–1.58; 95% CI [–3.0 to –0.17]), were all associated with
a reduced risk of post-ERCP pancreatitis. Pancreatic stent
placement had the highest SUCRA probability (0.81, 95%
CI [0.83 to 0.80]) of being ranked the best prophylactic
treatment.
Conclusions Based on this network meta-analysis, pancre-
atic stent placement appears to be the most effective pre-
ventive strategy for post-ERCP pancreatitis in high-risk pa-
tients.
Original article
* Drs.Njei and McCarty: These authors contributed equally.
Supplementary material
Online content viewable at:
https://doi.org/10.1055/a-1005-6366
Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40 E29
Published online: 2020-01-08

which is post-ERCP pancreatitis [1–3]. While the current litera-ture estimates incidence of post-ERCP pancreatitis to be be-tween 3% to 5%, a recent systematic review including over2000 high-risk patients who underwent ERCP demonstrated anincidence of 14.7% with an associated 0.2% mortality rate [4–6].
Given this high incidence of post-ERCP pancreatitis in asso-ciation with substantial morbidity, mortality, and healthcarecosts of $200 million annually in the United States, it is not sur-prising that several preventive strategies, both pharmacologicand endoscopic, have been employed [7]. Currently, there areseveral studies evaluating a variety of pharmacologic prophy-laxes for post-ERCP pancreatitis in high-risk patients that in-clude administration of rectal non-steroidal anti-inflammatorydrugs (NSAIDs) or aggressive hydration with lactated ringerʼssolution (LR) [8–13]. In addition, several studies have demon-strated the efficacy of prophylactic pancreatic stent placementin reducing the rate of post-ERCP pancreatitis and more impor-tantly in reducing the risk of severe post-ERCP pancreatitis[14–16].
However, due to paucity of data, it remains unclear whetherpharmacologic, endoscopic, or a combination of both approa-ches is the preferred strategy to prevent post-ERCP pancreati-tis. While previous direct pairwise meta-analyses have attempt-ed to answer this question about prevention of post-ERCP pan-creatitis, these types of studies are only able to provide partialinformation due to inherent design limitations. The primaryaim of this study is to design a network meta-analysis, simulta-neously analyzing direct and indirect evidence, to compare theeffectiveness of pharmacologic and endoscopic treatment ap-proaches to prevent post-ERCP pancreatitis.
MethodsStudy design
This systematic review was performed according to the Prefer-red Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA) statement outline for reporting systematic reviewsand meta-analyses and was conducted following a priori estab-lished protocol [17, 18]. We utilized a network meta-analysisand Bayesian framework to combine direct and indirect evi-dence comparing the relative efficacy of pharmacologic andendoscopic prophylaxis treatments for post-ERCP pancreatitis.This method was chosen to compare multiple interventionsand synthesize evidence across a network of randomized con-trolled trials [19, 20]. In brief, this method allows for simulta-neous analysis of direct evidence from comparator trials aswell as indirect evidence from different treatments comparedto a common comparator (i. e., placebo or no intervention)[21].
Selection criteria and study outcomes
Only randomized controlled trials for high-risk patients were in-cluded in this network meta-analysis. High-risk patients weredefined in randomized controlled trials by procedure-relatedfactors such as difficult cannulation, pancreatic duct injection,pancreatic sphincterotomy, and pre-cut sphincterotomy in ad-
dition to patient-associated factors including female sex, thosewith sphincter of Oddi dysfunction, and patients with recurrentpancreatitis or prior history of post-ERCP pancreatitis [22–24].Only trials involving high-risk patients were included.
Included studies involved adult patients (age ≥18 years) whounderwent ERCP involving use of rectal NSAIDs (i. e., indome-thacin or diclofenac), aggressive hydration with LR solution (de-fined as ≥3mL/kg/h during the procedure and post-procedureintravenous bolus or high-rate infusion), prophylactic pancreat-ic stent placement, or placebo. Studies evaluating these treat-ments alone or in combination as well as studies evaluating di-rect comparator studies to placebo were included. Observa-tional studies and trials evaluating prevention or reduction ofpost-ERCP pancreatitis were excluded. Post-ERCP pancreatitiswas defined by the consensus criteria as a clinical syndromeconsistent with pancreatitis as typical epigastric abdominalpain with an amylase or lipase level at least three times [25].
Data sources and literature search strategy
Two authors (BN and TRM) independently conducted a compre-hensive search of the literature to identify articles that exam-ined multiple electronic databases. Systematic searches ofPubMed, EMBASE, Web of Science, the Cochrane Library data-bases, and major annual gastroenterology conference proceed-ings were performed from inception through May 31, 2017.Published abstract proceedings were extracted from major gas-trointestinal meetings from January 2010 to May 2017. Scienti-fic meetings included Digestive Disease Week (DDW), UnitedEuropean Gastroenterology Week (UEGW), and the AmericanCollege of Gastroenterology (ACG) annual meeting.
Search terms included: “post-endoscopic retrograde cho-langiopancreatography (ERCP) pancreatitis,” “rectal non-ster-oidal anti-inflammatory drugs (NSAIDs),” “lactated ringerʼs(LR),” “prophylactic pancreatic stent,” and “post-ERCP pancrea-titis prophylaxis.” All relevant articles irrespective of language,year of publication, type of publication, or publication statuswere included. Titles and abstracts of all potentially relevantstudies were screened for eligibility. Reference lists of studiesof interest were then manually reviewed for additional articleswith additional references acquired through cross-checkingbibliographies of retrieved full-text papers. Any differenceswere resolved by mutual agreement and in consultation withthe third reviewer (UN). In the case of studies with incompleteinformation, contact was attempted with the principal authorsto obtain additional data.
Data abstraction and quality assessment
Study data were abstracted by two authors (BN and TRM) inde-pendently. Risk of bias of individual studies was evaluated andassessed in the context of the primary outcome (i. e., develop-ment of post-ERCP pancreatitis) using the Cochrane Risk of Biasassessment tool [26]. The GRADE approach to rate the qualityof evidence of estimates derived from this network meta-anal-ysis was also performed [27, 28]. Direct evidence from random-ized controlled trials was initially identified as high quality;however, it could be down-graded based on risk of bias, indir-ectness, imprecision, heterogeneity, or publication bias. Rating
E30 Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40
Original article

of indirect estimates began at the lowest rating of the two pair-wise estimates that contribute as first-order loops to the indir-ect estimate but could be down-graded further for imprecisionor intransitivity. If direct and indirect estimates were similar(i. e., coherent), then the higher of their rating was assigned tothe network meta-analysis estimates.
Statistical analysis
Direct meta-analysis was performed using DerSimonian andLaird random effects model to estimate pooled odds ratio (OR)and 95% confidence interval (CI) [29]. Multivariate random-effects meta-regression was utilized to present results usingthe Stata mvmeta command extension [30]. Heterogeneitywas assessed using I2 statistic with values > 50% indicating sub-stantial heterogeneity [31]. With regard to publication bias,funnel plot asymmetry and Egger’s regression test were per-formed as well [32]. Direct comparisons were performed usingRevMan v5.3 (Cochrane Collaboration, Copenhagen, Denmark)[33].
Indirect comparisons using a fixed effects Bayesian networkmeta-analysis was performed using a Markov chain Monte Carlomethod in WinBUGS statistical analysis program version 1.4.4(MRC Biostatistics Unit, Institute of Public Health, Cambridge,UK) and Network Plots were created in Stata SE-13 [31, 34].The Bayesian meta-analysis approach offers greater flexibilityfor the use of more complex models and different outcometypes, thereby enabling the simultaneous comparison of alltreatment options [35]. Comparative effectiveness of any twotreatments were modeled as a function of each treatment in re-lation to the reference treatment (i. e., placebo or no interven-tion) to assume consistency of treatment effects across all in-cluded randomized controlled trials. This thereby ensures thedirect and indirect effect estimates are the same effects.
With regard to network consistency, direct and indirect esti-mates were evaluated using a node-splitting technique. Poster-ior distribution of all parameters was estimated using non-in-formative priors to limit inference to data derived from thetrials. No assumptions about efficacy of rectal NSAIDs, aggres-sive resuscitation with LR, or prophylactic pancreatic stentplacement from data external to the trials was included in thissystematic review and network meta-analysis.
We used the Markov chain Monte Carlo method to obtainpooled effect sizes [35]. All chains were run with 50,000 sim-ulated draws after a burn-in of 5,000 iterations. The median ofthe posterior distribution based upon 50,000 simulations wasobtained using the 2.5th and 97.5th percentiles, after adjustedfor multiple arms. Risk of post-ERCP pancreatitis was reportedusing the estimate of the beta coefficient and calculated the95% credible interval.
Information on the relative effects was converted into aprobability that a treatment was best, (i. e., first-best, second-best, etc) and into a ranking for each treatment, called the sur-face under the cumulative ranking curve (SUCRA) [36, 37]. ASUCRA value of 1.0 guarantees when a treatment is certainlythe best and 0 when a treatment is certainly the worst. SUCRAvalues enable overall ranking of treatments for a particular out-come. SUCRA simplifies the information about the effect of
each treatment into a single number, thereby assisting the de-cision-making process.
Sensitivity analysis
Sensitivity analyses were also performed to assess the robust-ness and generalizability of our findings. Sensitivity analysiswas performed for high-quality studies as determined byGRADE assessment. Low-quality studies were excluded. Addi-tional sensitivity analysis was performed for full-text manu-scripts. Abstracts that did not result in full manuscript publica-tion were excluded.
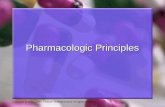
ResultsBased on previously discussed literature search criteria, a totalof 29 trials were included in this study – comprising 7,862 par-ticipants comparting four preventive strategies for post-ERCPpancreatitis. A PRISMA flow chart of search results is shown in
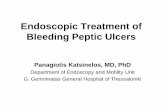
▶Fig.1. A network plot of network meta-analysis comparisonsof included studies is highlighted in ▶Fig. 2.
Characteristics of included studies
The primary outcome of post-ERCP pancreatitis was reported inall studies (▶Table 1). Thirteen studies, including 5,955 pa-tients with rectal NSAID use for prevention of post-ERCP pan-creatitis were included [8–10, 17, 38–46]. All but one study(abstract) were fully published manuscripts [45]. Eight studiesinvolving 754 patients evaluated use of aggressive hydrationwith LR solution in the prophylaxis of post-ERCP pancreatitis[11–13, 47–51]. Four studies were fully published manu-scripts, three studies were major gastroenterology meeting ab-stracts, and a final study was a RCT identified through Clinical-Trials.gov. One of the fully published manuscripts was a double-blinded, placebo-controlled trial that included both LR solutionindependently, as well as in combination with rectal NSAID use(n =96) [51]. Nine studies, including a total of 1057 partici-pants, evaluated use of prophylactic pancreatic stent place-ment [14–16, 52–57].
Quality assessment
GRADE assessment was performed for all included studies.These review authors’ judgements about each risk of bias itemfor each included study is highlighted in Supplemental Fig. 1. Arisk of bias summary graph is also available in SupplementalFig. 2.
Direct treatment comparisons
For direct treatment comparisons, all pharmacologic and endo-scopic modalities were compared to placebo or no intervention(Supplemental Table1). Compared to placebo, use of rectalNSAID therapy significantly reduced odds of post-ERCP pan-creatitis by 49% (OR=0.51, 95% CI [0.33 to 0.77]) (▶Fig.3).With regard to the effect of aggressive LR solution, this strategywas also effective in significantly reducing post-ERCP pancrea-titis by 52% (OR=0.48, 95% CI [0.24 to 0.97]) (▶Fig. 4). Whenthese two modalities were combined and compared to placebo,use of rectal NSAID and aggressive LR solution demonstrated
Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40 E31

75% reduced odds of developing post-ERCP pancreatitis; how-ever, this was not statistically significant (OR=0.25, 95% CI[0.06 to 0.99]). Prophylactic pancreatic duct stent placementwas effective in decreasing post-ERCP pancreatitis by 71% (OR=0.29, 95% CI [0.17 to 0.48]) (▶Fig. 5).
Sensitivity analyses
Results from sensitivity analyses are reported in the Supple-mental Table1. Overall, for the primary outcome, the resultswere largely similar to the main analysis.
Publication bias
There was no evidence of publication bias, based upon eitherqualitative on funnel-plot asymmetry or quantitative (i. e., Eg-ger regression test, P >0.05 for all comparisons) (Supplemen-tal Fig. 3, Supplemental Fig. 4, Supplement Fig. 5).
Network meta-analysis comparisons
With this network meta-analysis, we calculated the mixed ef-fect estimate as a weighted average of both direct and indirecttreatment effects. On direct network meta-analysis, all strate-gies (i. e., both pharmacologic and endoscopic treatments)were associated with a reduced risk of post-ERCP pancreatitis.In a direct network meta-analysis, compared with placebo, useof rectal NSAIDs (B =–0.69, 95% CI [–1.18 to –0.21]), pancre-atic stent (B =–1.25, 95% CI [–1.81 to –0.69]), high-volumeLR solution (B =–0.67, 95% CI [–1.20 to –0.13]), and com-bination of LR plus rectal NSAIDs (B =–1.58, 95% CI [–3.0 to–0.17]), were all associated with a reduced risk of post-ERCPpancreatitis. Summary results of our network meta-analysisare summarized in ▶Table2. Indirect comparisons were largelysimilar to those obtained in direct meta-analysis for treatment
Electronic database search:▪ Rectal NSAIDs (n = 3592)▪ Aggressive LR (n = 212)▪ Pancreatic stent (n = 1307)
Additional records identified through other sources (manual
abstract search)(n = 43)
Excluded based on title and abstract review (n = 3320)▪ Basic science articles, review articles, editorials▪ Observational studies▪ Reported non-effective interventions or interventions not used in clinical practice
Records after duplicates removed (n = 3416)
Abstracts and full-text reviewed (n = 3416)
Full-text articles excluded (n = 67)▪ Review/commentaries▪ Insufficient data▪ Case series/reports▪ Follow-up of initial study
Full-text articles reviewed (n = 96)
Studies included in quantitative synthesis (meta-analysis) (n = 29)
Iden
tific
atio
nSc
reen
ing
Elig
ibili
tyIn
clud
ed
▶ Fig. 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart of search results for the prevention of post-ERCP pancreatitis.
Lactated ringer plus NSAIDs
Lactated ringer
1 RCT; n = 96
1 RCT; n = 96
1 RCT; n = 961 RCT; n = 96
9 RCTs; n = 1057
8 RCTs; n = 754
13 RCTs; n = 5955Pancreatic stent
Rectal NSAIDs
A placebo
▶ Fig. 2 Network meta-analysis design of included studies for theprevention of post-ERCP pancreatitis.
E32 Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40
Original article

▶ Table 1 Summary characteristics of included studies for prevention of post-ERCP Pancreatitis.
Author Year,
place
of
study
Place
of
study
Type of
manu-
script
Study design Sam-
ple
size
Mean age of
treatment
group
(years)
Female
gender
(%)
Primary ERCP
indication of
bile duct stone
(%)
Trial-specific treat-
ment details
Rectal NSAID Therapy
Murray etal.
2003 Scot-land
Fulltext
Single-centercomparator toplacebo
220 55 65% 25.45% Diclofenac 100mg im-mediately post-ERCP
Sotoudeh-manesh etal.
2007 Iran Fulltext
Single-centercomparator toplacebo
490 58.4 53.90% 53.26% Indomethacin 100mgimmediately pre-ERCP
Otsuka etal.
2012 Japan Fulltext
Multicentercomparator toplacebo
104 75 49.04% 77.88% Diclofenac 25– 50mgimmediately pre-ERCP
Elmunzeret al.
2012 UnitedStates
Fulltext
Multicentercomparator toplacebo
602 44.4 79.07% – Indomethacin 100mgimmediately post-ERCP
Dobronteet al.
2012 Hun-gary
Fulltext
Single-centercomparator toplacebo
228 – – – Indomethacin 100mg10 –15 minutes pre-ERCP
Alabd andAbo
2013 Sudan Ab-stract
Single-centercomparator toplacebo
240 – – – –
Dobronteet al.
2014 Hun-gary
Fulltext
Single-centercomparator toplacebo
665 66.8 – – Indomethacin 100mg10 –15 minutes pre-ERCP
Andrade-Davila et al.
2015 Mexico Fulltext
Single-centercomparator toplacebo
166 51.59 66.27% 39.76% Indomethacin 100mgimmediately post-ERCP
Patai et al. 2015 Hun-gary
Fulltext
Single-centercomparator toplacebo
574 66.25 67.16% 58.63% Indomethacin 100mg60 minutes pre-ERCP
Lua et al. 2015 Malay-sia
Fulltext
Single-centercomparator toplacebo
151 50.3 59.03% 56.25% Diclofenac 100mg im-mediately post-ERCP
Luo et al. 2016 China Fulltext
Multicentercomparator toplacebo
2014 62 52.42% 77.50% Indomethacin 100mg30 minutes pre-ERCP
Levenick etal.
2016 UnitedStates
Fulltext
Single-centercomparator toplacebo
449 64.9 52.56% 27.72% Indomethacin 50mg ×2 during ERCP
Ucar et al. 2016 Turkey Fulltext
Single-centercomparator toplacebo
100 59 66.66% 83% Diclofenac 100mg30 –90 minutes pre-ERCP
Aggressive LR solution
Buxbaumet al.
2014 UnitedStates
Fulltext
Single-centercomparator tostandard hy-dration
62 43 51.61% 74.20% IV LR solution at a rateof 3.0mL/kg/h duringERCP, a bolus of 20mL/kg immediately post-ERCP, followed bypost-ERCP rate of3.0mL/kg/h for 8 h
Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40 E33

▶ Table 1 (Continuation)
Author Year,
place
of
study
Place
of
study
Type of
manu-
script
Study design Sam-
ple
size
Mean age of
treatment
group
(years)
Female
gender
(%)
Primary ERCP
indication of
bile duct stone
(%)
Trial-specific treat-
ment details
Chuank-rekkul etal.
2015 Thai-land
Ab-stract
Single-centercomparator tostandard hy-dration
60 61.9 – – IV LR solution at a rateof 3.0mL/kg/h duringERCP, a bolus of 10mL/kg immediately post-ERCP, followed bypost-ERCP rate of3.0mL/kg/h for 8 h
Shaygan-Nejad et al.
2015 Iran Fulltext
Single-centercomparator tostandard hy-dration
150 49.6 66% 95.35% IV LR solution at a rateof 3.0mL/kg/h duringERCP, a bolus of 20mL/kg immediately post-ERCP, followed bypost-ERCP rate of3.0mL/kg/h for 8 h
Rosa et al. 2016 Portu-gal
Ab-stract
Multicentercomparator tostandard hy-dration
68 – – – IV LR solution at a rateof 3.0mL/kg/h duringERCP, a bolus of 20mL/kg immediately post-ERCP, followed bypost-ERCP rate of3.0mL/kg/h for 8 h
NC-T0205004-8
2016 UnitedStates
– Multicentercomparator tostandard hy-dration
26 59.1 84.62% – Initial bolus LR solu-tion of 7.58mL/kg pre-ERCP, IV LR solution of5.0mL/kg/h duringERCP, following bypost-ERCP bolus of20mL/kg for 90 min-utes
Chang etal.
2016 Thai-land
Ab-stract
Single-centercomparator tostandard hy-dration
171 – – 50% IV LR solution at a rateof 150mL/h starting2h pre-ERCP, and con-tinued during andpost-ERCP for 24h
Choi et al. 2016 Korea Fulltext
Multicentercomparator tostandard hy-dration
510 57.6 45.50% 53.70% Initial bolus LR solu-tion of 10mL/kg pre-ERCP, IV LR solution of3.0mL/kg/h duringERCP and continued8h post-ERCP, follow-ing by post-ERCP bolusof 10mL/kg
Mok et al. 2017 UnitedStates
Fulltext
Single-centercomparatorwith multipletherapies*
48 60.25 60.60% – Treatment arms in-cluded standard nor-mal saline solution vsnormal saline plus in-domethacin versus LRversus LR plus indo-methacin
E34 Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40
Original article

modalities compared to placebo. However, in indirect networkmeta-analysis, there was no statistically significant differencewhen treatment modalities were compared with each other.There were overlapping confidence intervals, although differ-ences were observed in effect size.
Ranking probabilityRanking probability based on SUCRA indicated that prophylac-tic pancreatic duct stent placement had the highest probability(SUCRA=0.81, 95% CI [0.83 to 0.80]) of being ranked the bestprophylactic treatment (▶Fig. 6). As highlighted in the SUCRAprobabilities figure, a combined strategy of LR solution plusrectal NSAIDs was the second most effective treatment to pre-vent post-ERCP pancreatitis (SUCRA=0.76, 95% CI [0.79 to0.72]), followed by aggressive infusion of LR solution alone (SU-
▶ Table 1 (Continuation)
Author Year,
place
of
study
Place
of
study
Type of
manu-
script
Study design Sam-
ple
size
Mean age of
treatment
group
(years)
Female
gender
(%)
Primary ERCP
indication of
bile duct stone
(%)
Trial-specific treat-
ment details
Rectal NSAIDs + LR solution
Mok et al. 2017 UnitedStates
Fulltext
Single-centercomparatorwith multipletherapies*
48 60.25 60.60% – Treatment arms in-cluded standard nor-mal saline solution vsnormal saline plus in-domethacin versus LRversus LR plus indo-methacin
Pancreatic stent placement
Smithlineet al.
1993 UnitedStates
Fulltext
Single-centercomparator toplacebo
99 46 78.79% – 5–7 Fr stent,2–2.5 cm in length
Tarnasky etal.
1998 UnitedStates
Fulltext
Single-centercomparator toplacebo
80 46.05 – – 5–7 Fr stent,2–2.5 cm in length
Fazel et al. 2003 UnitedStates
Fulltext
Single-centercomparator toplacebo
74 44.7 86.49% – Nasopancreatic 5 Frcatheter or 5 Fr stent,2 cm length, 2 barbed
Harewoodet al.
2005 UnitedStates
Fulltext
Single-centercomparator toplacebo
19 48.75 63.16% – Straight, single flan-ged, polyethylene 5 Frstent, 3–5 cm length
Sofuni etal.
2011 Japan Fulltext
Multicentercomparator toplacebo
201 66.4 37.81% – Straight, 5 Fr stent,3 cm in length
Pan et al. 2012 China Fulltext
Single-centercomparator toplacebo
40 58.3 52.50% – Single pigtail, 5 Frstent
Lee et al. 2012 Korea Fulltext
Single-centercomparator toplacebo
101 57.5 62.38% 66.33% Single pigtail unflan-ged 3 Fr stent, 4–8 cmlength
Kawaguchiet al.
2012 Japan Fulltext
Single-centercomparator toplacebo
120 67 56.67% 35.83% Unflanged on pancre-atic duct side, 2 flan-ges on duodenal side5 Fr stent, 3 cm length
Cha et al. 2013 UnitedStates
Fulltext
Single-centercomparator toplacebo
151 56.6 58.94% 15.89% Straight or external3/4 pigtail 5–7 Frstent, 2–2.5 cmlength
ERCP, endoscopic retrograde cholangiopancreatography; NSAID, nonsteroidal anti-inflammatory drug; IV, intravenous; LR, lactated ringer’s
Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40 E35

CRA=0.51, 95% CI [0.55 to 0.49]), and finally independent useof rectal NSAID use (SUCRA=0.41, 95% CI [0.44 to 0.38]). Arankogram of interventions to prevent post-ERCP pancreatitisbased upon cumulative SUCRA probabilities is highlighted inSupplemental Fig. 6.
DiscussionIn this systematic review and network meta-analysis, comparedto other treatment approaches, pancreatic duct stent place-ment appears to be the most effective strategy for the preven-tion of post-ERCP pancreatitis followed by prophylaxis using ag-gressive LR hydration and rectal NSAIDs, followed by high-vol-ume LR infusions alone, and finally use of rectal NSAIDs.
Pancreatic duct stents reduce post-ERCP pancreatitis by re-lieving pancreatic ductal hypertension that may develop as aresult of transient procedure-induced stenosis [58]. The mostrecent European Society of Gastrointestinal Endoscopy (ESGE)guideline on prophylaxis of post-ERCP pancreatitis recom-mends placement of a 5 Fr prophylactic pancreatic stent inhigh-risk cases [59]. However, pancreatic stent placement istechnically challenging. Pancreatic stent requires deep cannu-lation of the duct and placement of a guidewire. Attemptingto place a pancreatic duct stent with subsequent failure actual-ly increases risk of post-ERCP pancreatitis by inducing injury tothe pancreatic orifice. Hence, it is these authors’ belief thatpancreatic stent placement should only be attempted by provi-ders with familiarity and expertise, in individuals deemed to be
Rectal NSAIDs Control Odds ratio Odds ratioStudy or subgroup Events Total Events Total Weight M-H, random, 95 % CI Year M-H, random, 95 % CI
Murray 2003 0 110 2 110 1.9 % 0.20 [0.01, 4.14] 2003Sotoudehmanesh 2007 0 245 5 245 2.1 % 0.09 [0.00, 1.62] 2007Otsuka 2012 0 51 3 53 2.0 % 0.14 [0.01, 2.78] 2012Elmunzer 2012 13 295 27 307 38.2 % 0.48 [0.24, 0.95] 2012Dobronte 2012 2 82 1 98 3.0 % 2.42 [0.22, 27.23] 2012Alabd 2013 1 120 1 120 2.3 % 1.00 [0.06, 16.17] 2013Dobronte 2014 4 347 4 318 9.1 % 0.92 [0.23, 3.69] 2014Andrade-Davila 2015 1 82 3 84 3.4 % 0.33 [0.03, 3.27] 2015Patai 2015 3 287 4 287 7.8 % 0.75 [0.17, 3.37] 2015Lua 2015 3 69 0 82 2.0 % 8.68 [0.44, 171.10] 2015Luo 2016 7 992 17 1022 22.7 % 0.42 [0.17, 1.02] 2016Levenick 2016 0 233 2 226 1.9 % 0.20 [0.01, 4.21] 2016Ucar 2016 1 50 4 50 3.6 % 0.23 [0.03, 2.18] 2016
Total (95 % CI) 2953 3002 100.0 % 0.51 [0.33, 0.77]Total events 35 73Heterogeneity. Tau2 = 0.00; Chi2 = 9.89, df = 12 (P = 0.63); I2 = 0 %Test for overall eff ect: Z = 3.16 (P = 0.002)
0.01 0.1 1 10 100Favours [rectal NSAIDs] Favours [control]
▶ Fig. 3 Direct treatment comparison of rectal NSAIDs to placebo for the prevention of post-ERCP pancreatitis.
Lactated Ringer’s Control Odds ratio Odds ratioStudy or subgroup Events Total Events Total Weight M-H, random, 95 % CI Year M-H, random, 95 % CI
Buxbaum 2014 0 39 4 23 4.5 % 0.05 [0.00, 1.07] 2014Shaygan-Nejad 2015 4 75 17 75 15.9 % 0.19 [0.06, 0.60] 2015Chuankrekkul 2015 3 30 2 30 9.2 % 1.56 [0.24, 10.05] 2015NCT02050048 2016 0 14 1 12 3.8 % 0.26 [0.01, 7.12] 2016Rosa 2016 2 35 5 33 10.3 % 0.34 [0.06, 1.89] 2016Choi 2016 8 92 20 80 19.3 % 0.29 [0.12, 0.69] 2016Chang 2016 13 58 11 62 19.1 % 1.34 [0.55, 3.29] 2016Mok (LR) 2017 9 48 10 48 17.7 % 0.88 [0.32, 2.70] 2017
Total (95 % CI) 391 363 100.0 % 0.48 [0.24, 0.97]Total events 39 70Heterogeneity. Tau2 = 0.44; Chi2 = 14.00, df = 7 (P = 0.05); I2 = 50 %Test for overall eff ect: Z = 2.06 (P = 0.04)
0.01 0.1 1 10 100Favours [lactated Ringer’s] Favours [control]
▶ Fig. 4 Direct treatment comparison of aggressive LR solution to placebo for the prevention of post-ERCP pancreatitis.
E36 Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40
Original article

a high-risk, and in cases in which cannulation is not intentionaland stent placement would be recommended in case of inad-vertent cannulation. In patients in whom pancreatic stentplacement is not feasible, use of alternative measures to reducepost-procedure pancreatitis should be employed.
Based on our study, aggressive hydration with LR appears tobe effective when combined with rectal NSAIDs rather than
using rectal NSAIDs alone or LR alone. Use of rectal NSAIDs, po-tent inhibitors of phospholipase A2, has been increasinglyadopted in to clinical practice [59, 60]. Current ESGE guidelinesrecommend routine rectal administration of diclofenac or indo-methacin immediately before or after ERCP in all patients with-out contraindication [59]. Aggressive hydration with LR, whichattenuates the acidosis that appears to promote zymogen acti-
Pancreatic stent Control Odds ratio Odds ratioStudy or subgroup Events Total Events Total Weight M-H, random, 95 % CI Year M-H, random, 95 % CI
Smithline 1993 6 43 9 50 14.7 % 0.74 [0.24, 2.27] 1993Tarnasky 1998 1 41 10 39 5.4 % 0.07 [0.01, 0.60] 1998Fazel 2003 1 38 10 36 8.7 % 0.14 [0.03, 0.72] 2003Harewood 2005 0 10 3 9 2.6 % 0.09 [0.00, 2.00] 2005Sofuni 2011 17 213 32 213 28.1 % 0.49 [0.26, 0.91] 2011Pan 2011 4 20 14 20 10.1 % 0.11 [0.03, 0.46] 2011Lee 2012 1 60 8 60 5.4 % 0.11 [0.01, 0.91] 2012Kawaguchi 2012 6 50 15 51 16.3 % 0.33 [0.12, 0.93] 2012Cha 2013 2 46 8 58 8.7 % 0.28 [0.06, 1.41] 2013
Total (95 % CI) 521 536 100.0 % 0.29 [0.17, 0.48]Total events 39 109Heterogeneity. Tau2 = 0.15; Chi2 = 10.71, df = 8 (P = 0.22); I2 = 25 %Test for overall eff ect: Z = 4.71 (P < 0.00001)
0.01 0.1 1 10 100Favours [pancreatic stent] Favours [control]
▶ Fig. 5 Direct treatment comparison of pancreatic stent placement to placebo for the prevention of post-ERCP pancreatitis.
▶ Table 2 Summary results from network meta-analysis in the prevention of post-ERCP pancreatitis.
Post-ERCP treatment Beta coefficient (β) 95% credible interval (CI)1 Quality of evidence
Lactated ringer’s vs placebo –0.69 –0.77 to –2.15 ⊕⊕⊕Moderate2
Lactated ringer’s + rectal nsaids vs placebo –0.82 –1.45 to –0.19 ⊕⊕⊕⊕High
Pancreatic stent vs placebo –1.37 –2.98 to –0.23 ⊕⊕⊕⊕High
Rectal NSAIDs vs placebo –1.27 –2.30 to –0.70 ⊕⊕⊕⊕High
Lactated ringer’s + rectal NSAIDs vs lactated ringer’s –0.55 –2.28 to 1.17 ⊕⊕⊕Low3
Pancreatic stent vs lactated ringer’s –0.45 –1.30 to 0.39 ⊕⊕⊕Low3
Rectal NSAIDs vs lactated ringer’s 0.21 –1.32 to 1.74 ⊕⊕⊕Low3
Pancreatic stent vs lactated ringer’s + rectal NSAIDs 0.10 –1.61 to 1.80 ⊕⊕⊕Low3
Rectal NSAIDs vs lactated ringer’s + rectal NSAIDs 0.76 –0.92 to 2.44 ⊕⊕⊕Low3
Rectal NSAIDs vs pancreatic stent 0.66 –0.84 to 2.17 ⊕⊕⊕Low3
ERCP, endoscopic retrograde cholangiopancreatography; NSAID, nonsteroidal anti-inflammatory drug1 If the CI estimates are either all positive or negative (i. e., does not include a zero), it indicates that results are statistically significant.2 Due to risk of bias in imprecision of summary results.3 Due to risk of bias in individual studies, indirectness, and imprecision of summary results.
Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40 E37

vation and pancreatic inflammation, may be an effective inter-vention for preventing post-ERCP pancreatitis. Given the differ-ent mechanisms to prevent pancreatitis, it is not surprising thatboth work synergistically. Moreover, as both rectal NSAID ther-apy and LR infusion are inexpensive with relative few AEs, com-bination strategy is now has become a preferred strategy forpost-ERCP pancreatitis prevention.
Our study observations are different from a previous net-work meta-analysis which reported that use of rectal NSAIDswhen indirectly compared with pancreatic stent placementalone were associated with lower odds for developing post-ERCP pancreatitis [61]. However, that analysis included bothobservational studies and randomized controlled trials, whichmay have contributed to the divergent results. Furthermore,this previous study examined the efficacy of rectal NSAIDs andprophylactic pancreatic duct stent placement among bothaverage-risk and high-risk cohorts. Our study specifically in-cluded only high-quality randomized controlled trials in high-risk patients and demonstrates the superiority of pancreaticstent placement as the best prophylactic measure for post-ERCP pancreatitis. Importantly, these findings do not take intoaccount the cost-effectiveness of various therapies (i. e., rectalNSAIDs are inexpensive, easy to use, efficacious, and low risk).Despite our findings, questions still remain about whether allhigh-risk patients should receive a pancreatic stent– especiallyindividuals who require multiple cannulation attempts of thebiliary orifice.
It is important to note that the current systematic reviewand network meta-analysis is not without limitations. Therewere no studies comparing treatment strategies other thanplacebo except for one study that compared aggressive LR hy-dration to use of rectal NSAIDs. No currently published studieshave examined the role of pancreatic duct stent versus rectalNSAIDs; although it should be pointed out there is an activelyrecruiting clinical trial designed to directly compare these twotreatment modalities [62]. This study, with an expected enroll-ment of over 1400 patients, is a comparative effectiveness mul-ticenter, non-inferiority trial of rectal indomethacin alone ver-sus the combination of rectal indomethacin and prophylactic
pancreatic stent placement for prevention of post-ERCP pan-creatitis.
While we included indirect comparison in a Bayesian net-work meta-analysis design, we cannot discount the possibilityof conceptual heterogeneity whereby differences may exist intrial design, patient population, intervention (i. e., timing ofrectal NSAID administration or operator variability in pancreat-ic duct stent placement), and outcome assessment which maylimit true comparability between included studies [19, 27].Though we performed sensitivity analyses to minimize hetero-geneity and generalize our findings, it is important to under-stand that not all risk factors for post-ERCP pancreatitis are cre-ated equal, and combinations or risk factors are not simply ad-ditive, but multiplicative [63–66]. Additional limitations in-clude a lack of data on follow-up – though the primary endpointof post-ERCP pancreatitis lends itself to definitive diagnosis asdefined over a discrete period of time as detailed above [25].Treatment-related AEs were not reported in our systematic re-view and network meta-analysis as well, which may limit clinicaladoption of these strategies, especially pancreatic duct stentplacement.
Despite these limitations, our study possesses severalstrengths. These include the comprehensive and simultaneousassessment of the relative efficacy of four competing or in-combination strategies to prevent post-ERCP pancreatitis in ahigh-risk cohort. Although SUCRA probabilities may not easilysubstitute for clinical judgement on a patient-by-patient basis,focusing on summary effect estimates and GRADE to rate over-all quality of evidence allows for better approximations [27]. Inaddition, while conceptual heterogeneity was present in ourstudy, strategies to limit the effect of conceptual heterogeneityincluded strict inclusion and exclusion criteria and use of multi-ple sensitivity analyses to assess the robustness of the results.
Furthermore, although there are several available strategiesavailable to potentially reduce incidence post-ERCP pancreati-tis, our results validate the current American Society of Gastro-intestinal Endoscopy (ASGE) guidelines recommending pancre-atic duct stenting in high-risk individuals – strong recommen-dation [22]. Future trials such as the one discussed above to as-sess rectal indomethacin alone versus combination therapy
Lactated Ringer
1 2 3 4
SUCRA = 0.51
Rank = 3
5
Cum
ulat
ive
prob
abili
ties 1
0.8
0.6
0.4
0.2
0
Placebo Rectal NSAIDs
1 2 3 4
SUCRA = 0.2
Rank = 5
5
1
0.8
0.6
0.4
0.2
01 2 3 4
SUCRA = 0.41
Rank = 4
5
1
0.8
0.6
0.4
0.2
0
Pancreatic stent
RankGraphs by treatment
1 2 3 4
SUCRA = 0.81
Rank = 1
5
1
0.8
0.6
0.4
0.2
0
Lactated Ringerplus NSAIDs
1 2 3 4
SUCRA = 0.76Rank = 2
5
1
0.8
0.6
0.4
0.2
0
▶ Fig. 6 SUCRA cumulative probability plots for the prevention of post-ERCP pancreatitis.
E38 Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40
Original article

with rectal NSAID and prophylactic pancreatic stent placementmay help development of future recommendations; however,these are unlikely to occur [62]. Comparison of these differentstrategies alone may be of limited benefit clinically because thecombination of the different treatments has already readilybeen adopted in clinical practice and shown to be effectivewith few complications.
ConclusionIn conclusion, based upon this systematic review and networkmeta-analysis, prophylactic pancreatic stent placement ap-pears to be the most effective preventive strategy for post-ERCP pancreatitis in high-risk patients. Despite these findings,it is these authors’ belief that combination therapy will likelypredominate clinical practice. This is in part due to the in-creased risk of post-ERCP pancreatitis with failed cannulationof the pancreatic duct and the ease and cost of combinationtherapy with rectal NSAID use and aggressive LR infusion.
Competing interests
Dr. Shyam Varadarajulu is a consultant for Boston Scientific
and Olympus. Dr. Udayakumar Navaneethan is a consultant
for Janssen, AbbVie, Pfizer and Takeda.
References
[1] Peery AF, Dellon ES, Lund J et al. Burden of gastrointestinal disease inthe United States: 2012 update. Gastroenterology 2012; 143: 1179–1187 e1-3
[2] Sherman S. ERCP and endoscopic sphincterotomy-induced pancrea-titis. Am J Gastroenterol 1994; 89: 303–305
[3] Silviera ML, Seamon MJ, Porshinsky B et al. Complications related toendoscopic retrograde cholangiopancreatography: a comprehensiveclinical review. J Gastrointestin Liver Dis 2009; 18: 73–82
[4] Freeman ML, Nelson DB, Sherman S et al. Complications of endo-scopic biliary sphincterotomy. N Engl J Med 1996; 335: 909–918
[5] Glomsaker T, Hoff G, Kvaloy JT et al. Patterns and predictive factors ofcomplications after endoscopic retrograde cholangiopancreatogra-phy. Br J Surg 2013; 100: 373–380
[6] Kochar B, Akshintala VS, Afghani E et al. Incidence, severity, andmortality of post-ERCP pancreatitis: a systematic review by usingrandomized, controlled trials. Gastrointest Endosc 2015; 81: 143–149 e9
[7] Arata S, Takada T, Hirata K et al. Post-ERCP pancreatitis. J Hepatobili-ary Pancreat Sci 2010; 17: 70–78
[8] Murray B, Carter R, Imrie C et al. Diclofenac reduces the incidence ofacute pancreatitis after endoscopic retrograde cholangiopancreato-graphy. Gastroenterology 2003; 124: 1786–1791
[9] Otsuka T, Kawazoe S, Nakashita S et al. Low-dose rectal diclofenac forprevention of post-endoscopic retrograde cholangiopancreatographypancreatitis: a randomized controlled trial. J Gastroenterol 2012; 47:912–917
[10] Sotoudehmanesh R, Khatibian M, Kolahdoozan S et al. Indomethacinmay reduce the incidence and severity of acute pancreatitis afterERCP. Am J Gastroenterol 2007; 102: 978–983
[11] Chang AS, Pausawasdi N, Charatcharoenwitthaya P et al. A random-ized, controlled trial of aggressive fluid hydration for the preventionof post-ERCP pancreatitis. Gastroenterol 2016; 150: S209
[12] Buxbaum J, Yan A, Yeh K et al. Aggressive hydration with lactatedRinger’s solution reduces pancreatitis after endoscopic retrogradecholangiopancreatography. Clin Gastroenterol Hepatol 2014; 12:303–307 e1
[13] Choi JH, Kim HJ, Lee BU et al. Vigorous periprocedural hydration withlactated ringer’s solution reduces the risk of pancreatitis after retro-grade cholangiopancreatography in hospitalized patients. Clin Gas-troenterol Hepatol 2017; 15: 86–92 e1
[14] Fazel A, Quadri A, Catalano MF et al. Does a pancreatic duct stentprevent post-ERCP pancreatitis? A prospective randomized studyGastrointest Endosc 2003; 57: 291–294
[15] Smithline A, Silverman W, Rogers D et al. Effect of prophylactic mainpancreatic duct stenting on the incidence of biliary endoscopicsphincterotomy-induced pancreatitis in high-risk patients. Gastroin-test Endosc 1993; 39: 652–657
[16] Tarnasky PR, Palesch YY, Cunningham JT et al. Pancreatic stentingprevents pancreatitis after biliary sphincterotomy in patients withsphincter of Oddi dysfunction. Gastroenterology 1998; 115: 1518–1524
[17] Dobronte Z, Szepes Z, Izbeki F et al. Is rectal indomethacin effective inpreventing of post-endoscopic retrograde cholangiopancreatogra-phy pancreatitis? World J Gastroenterol 2014; 20: 10151–10157
[18] Hutton B, Salanti G, Chaimani A et al. The quality of reporting meth-ods and results in network meta-analyses: an overview of reviews andsuggestions for improvement. PLoS One 2014; 9: e92508
[19] Cipriani A, Higgins JP, Geddes JR et al. Conceptual and technical chal-lenges in network meta-analysis. Ann Intern Med 2013; 159: 130–137
[20] Mills EJ, Ioannidis JP, Thorlund K et al. How to use an article reporting amultiple treatment comparison meta-analysis. JAMA 2012; 308:1246–1253
[21] Lu G, Ades AE. Combination of direct and indirect evidence in mixedtreatment comparisons. Stat Med 2004; 23: 3105–3124
[22] Chandrasekhara V, Khashab MA et al. ASGE Standards of PracticeCommittee. Adverse events associated with ERCP. Gastrointest En-dosc 2017; 85: 32–47
[23] Testoni PA, Mariani A, Giussani A et al. Risk factors for post-ERCPpancreatitis in high- and low-volume centers and among expert andnon-expert operators: a prospective multicenter study. Am J Gastro-enterol 2010; 105: 1753–1761
[24] Chen JJ, Wang XM, Liu XQ et al. Risk factors for post-ERCP pancreati-tis: a systematic review of clinical trials with a large sample size in thepast 10 years. Eur J Med Res 2014; 19: 26
[25] Cotton PB, Eisen GM, Aabakken L et al. A lexicon for endoscopic ad-verse events: report of an ASGE workshop. Gastrointest Endosc 2010;71: 446–454
[26] Higgins JPT, Altman DG, Sterne JAC. Cochrane Handbook for Sys-tematic Reviews of Interventions. In: Higgins JPT, ed. The CochraneCollaboration; 2011: Available from http://www.cochranehandbook.org
[27] Puhan MA, Schunemann HJ, Murad MH et al. A GRADE Working Groupapproach for rating the quality of treatment effect estimates fromnetwork meta-analysis. BMJ 2014; 349: g5630
[28] Guyatt G, Oxman AD, Sultan S et al. GRADE guidelines: 11. Making anoverall rating of confidence in effect estimates for a single outcomeand for all outcomes. J Clin Epidemiol 2013; 66: 151–157
[29] DerSimonian R, Laird N. Meta-analysis in clinical trials. Control ClinTrials 1986; 7: 177–188
[30] White IR. Multivariate random-effects meta-regression: Updates tomvmeta. The Stata Journal 2011; 11: 255–270
Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40 E39

[31] Higgins JP, Thompson SG, Deeks JJ et al. Measuring inconsistency inmeta-analyses. BMJ 2003; 327: 557–560
[32] Egger M, Davey SmithG, Schneider M et al. Bias in meta-analysis de-tected by a simple, graphical test. BMJ 1997; 315: 629–634
[33] Review Manager (RevMan), ver. 5.3. The Cochrane Collaboration;(ed.) 2014
[34] Lu G, Ades AE. Combination of direct and indirect evidence in mixedtreatment comparisons. Stat Med 2004; 23: 3105–3124
[35] Caldwell DM, Ades AE, Higgins JP. Simultaneous comparison of multi-ple treatments: combining direct and indirect evidence. BMJ 2005;331: 897–900
[36] Chaimani A, Higgins JP, Mavridis D et al. Graphical tools for networkmeta-analysis in STATA. PLoS One 2013; 8: e76654
[37] Salanti G, Ades AE, Ioannidis JP. Graphical methods and numericalsummaries for presenting results from multiple-treatment meta-a-nalysis: an overview and tutorial. J Clin Epidemiol 2011; 64: 163–171
[38] Dobronte Z, Toldy E, Mark L et al. [Effects of rectal indomethacin inthe prevention of post-ERCP acute pancreatitis]. Orv Hetil 2012; 153:990–996
[39] Andrade-Davila VF, Chavez-Tostado M, Davalos-Cobian C et al. Rectalindomethacin versus placebo to reduce the incidence of pancreatitisafter endoscopic retrograde cholangiopancreatography: results of acontrolled clinical trial. BMC Gastroenterol 2015; 15: 85
[40] Patai A, Solymosi N, Patai AV. Effect of rectal indomethacin for pre-venting post-ERCP pancreatitis depends on difficulties of cannulation:results from a randomized study with sequential biliary intubation.J Clin Gastroenterol 2015; 49: 429–437
[41] Lua GW, Muthukaruppan R, Menon J. Can rectal diclofenac preventpost endoscopic retrograde cholangiopancreatography pancreatitis?Dig Dis Sci 2015; 60: 3118–3123
[42] Luo H, Zhao L, Leung J et al. Routine pre-procedural rectal indometa-cin versus selective post-procedural rectal indometacin to preventpancreatitis in patients undergoing endoscopic retrograde cholan-giopancreatography: a multicentre, single-blinded, randomised con-trolled trial. Lancet 2016; 387: 2293–2301
[43] Levenick JM, Gordon SR, Fadden LL et al. Rectal indomethacin doesnot prevent post-ERCP pancreatitis in consecutive patients. Gastro-enterology 2016; 150: 911–917; quiz e19.
[44] Ucar R, Biyik M, Ucar E et al. Rectal or intramuscular diclofenac re-duces the incidence of pancreatitis afterendoscopic retrograde cho-langiopancreatography. Turk J Med Sci 2016; 46: 1059–1063
[45] Alabd M, Abdo A. Role of rectal NSAIDs in the prevention of post-ERCPpancreatitis. J Gastroenterol Hepatol 2013; 28: 495–496
[46] Elmunzer BJ, Scheiman JM, Lehman GA et al. A randomized trial ofrectal indomethacin to prevent post-ERCP pancreatitis. N Engl J Med2012; 366: 1414–1422
[47] Chuankrerkkul P. Aggressive lactated Ringer’s solution for preventionof post ERCP pancreatitis (preliminary data of a prospective random-ized trial). Gastrointest Endosc 2015; 81: AB410–AB411
[48] Rosa B, Carvalho PB, De Castro FD et al. Impact of intensive hydrationon the incidence of post-ERCP pancreatitis: doubleblinded random-ized controlled trial. Gastrointest Endosc 2016; 83: AB250
[49] Shaygan-Nejad A, Masjedizadeh AR, Ghavidel A et al. Aggressive hy-dration with Lactated Ringer’s solution as the prophylactic interven-tion for postendoscopic retrograde cholangiopancreatography pan-creatitis: A randomized controlled double-blind clinical trial. J ResMed Sci 2015; 20: 838–843
[50] NorthShore University Health System, Medical College of Wisconsin.et al. High volume lactated Ringer’s solution and pancreatitis. Na-
tional Library of Medicine (US); 2016: Available at: https://clinical-trials.gov/show/NCT02050048 [Accessed December 21, 2016.]
[51] Mok SRS, Ho HC, Shah P et al. Lactated Ringer’s solution in combina-tion with rectal indomethacin for prevention of post-ERCP pancreati-tis and readmission: a prospective randomized, double-blinded, pla-cebo-controlled trial. Gastrointest Endosc 2017; 85: 1005–1013
[52] Harewood GC, Pochron NL, Gostout CJ. Prospective, randomized,controlled trial of prophylactic pancreatic stent placement for endo-scopic snare excision of the duodenal ampulla. Gastrointest Endosc2005; 62: 367–370
[53] Sofuni A, Maguchi H, Itoi T et al. Prophylaxis of post-endoscopicretrograde cholangiopancreatography pancreatitis by an endoscopicpancreatic spontaneous dislodgement stent. Clin Gastroenterol He-patol 2007; 5: 1339–1346
[54] Pan XP, Dang T, Meng XM et al. Clinical study on the prevention ofpost-ERCP pancreatitis by pancreatic duct stenting. Cell BiochemBiophys 2011; 61: 473–479
[55] Lee TH, Moon JH, Choi HJ et al. Prophylactic temporary 3F pancreaticduct stent to prevent post-ERCP pancreatitis in patients with a diffi-cult biliary cannulation: a multicenter, prospective, randomizedstudy. Gastrointest Endosc 2012; 76: 578–585
[56] Kawaguchi Y, Ogawa M, Omata F et al. Randomized controlled trial ofpancreatic stenting to prevent pancreatitis after endoscopic retro-grade cholangiopancreatography. World J Gastroenterol 2012; 18:1635–1641
[57] Cha SW, Leung WD, Lehman GA et al. Does leaving a main pancreaticduct stent in place reduce the incidence of precut biliary sphincter-otomy-associated pancreatitis? A randomized, prospective studyGastrointest Endosc 2013; 77: 209–216
[58] Olsson G, Lubbe J, Arnelo U et al. The impact of prophylactic pancre-atic stenting on post-ERCP pancreatitis: A nationwide, register-basedstudy. United European Gastroenterol J 2017; 5: 111–1118
[59] Dumonceau JM, Andriulli A, Elmunzer BJ et al. Prophylaxis of post-ERCP pancreatitis: European Society of Gastrointestinal Endoscopy(ESGE) Guideline - updated June 2014. Endoscopy 2014; 46: 799–815
[60] Yokoe M, Takada T, Mayumi T et al. Japanese guidelines for the man-agement of acute pancreatitis: Japanese Guidelines 2015. J Hepato-biliary Pancreat Sci 2015; 22: 405–432
[61] Akbar A, Abu Dayyeh BK et al. Rectal nonsteroidal anti-inflammatorydrugs are superior to pancreatic duct stents in preventing pancreati-tis after endoscopic retrograde cholangiopancreatography: a net-work meta-analysis. Clin Gastroenterol Hepatol 2013; 11: 778–783
[62] Medical University of South Carolina. Stent vs. indomethacin for pre-venting post-ERCP pancreatitis (SVI). National Library of Medicine(US); 2018: Available at: https://clinicaltrials.gov/ct2/show/NCT02476279?cond=stent+vs.+indomethacin+for+preventing+post-ercp+pancreatitis&rank=1 [Accessed March 21, 2018.]
[63] Cote GA. The end of prophylactic pancreatic duct stents? Proceedwith caution and courage Clin Gastroenterol Hepatol 2014; 12: 528
[64] Cheng CL, Sherman S, Watkins JL et al. Risk factors for post-ERCPpancreatitis: a prospective multicenter study. Am J Gastroenterol2006; 101: 139–147
[65] Cotton PB, Garrow DA, Gallagher J et al. Risk factors for complicationsafter ERCP: a multivariate analysis of 11,497 procedures over 12years. Gastrointest Endosc 2009; 70: 80–88
[66] Freeman ML, DiSario JA, Nelson DB et al. Risk factors for post-ERCPpancreatitis: a prospective, multicenter study. Gastrointest Endosc2001; 54: 425–434
E40 Njei Basile et al. Comparative effectiveness of… Endoscopy International Open 2020; 08: E29–E40
Original article