Companion May2009
28
The essential publication for BSAVA members How To… Get great ultrasound images P10 Congress Snapshots BSAVA Congress 2009 in pictures P4 companion MAY 2009 CPD Create your own film reading course P19 Investigation of collapse in a young Boxer dog
Transcript of Companion May2009

The essential publication for BSAVA members
How To…Get great ultrasound imagesP10
Congress SnapshotsBSAVA Congress 2009 in picturesP4
companionMAY 2009
CPDCreate your own film reading courseP19
Investigation of collapse in a young Boxer dog
The essential publication for BSAVA members
companioncompanionThe essential publication for BSAVA members
companionThe essential publication for BSAVA members
Investigation of collapse in a young Boxer dog

companion
2 | companion
3 Round UpMeet your President
4–5 Congress SnapshotsFour days in focus
6–8 Clinical ConundrumA case of collapse in a young Boxer dog
9 Suicide in Our ProfessionDavid J. Bartram reports on the increased suicide risk in the veterinary profession
10–13 How To…Get great ultrasound images
14–15 GrapeVINeFrom the Veterinary Information Network
16–18 Spotlight on Small Animal DiseasesJohn Bonner reports on The Small Animal Veterinary Surveillance Network
19 Create Your Own Film Reading CourseCPD from the BSAVA
20–21 Gut FeelingsAdvances and prospects in small animal gastrointestinal disease
22 PetsaversLatest fundraising news
23–25 WSAVA NewsWorld Small Animal Veterinary Association
26 The companion InterviewDuncan Lascelles
27 CPD DiaryWhat’s on in your area
companion is produced by BSAVA exclusively for its members.BSAVA, Woodrow House, 1 Telford Way, Waterwells Business Park, Quedgeley, Gloucester GL2 2AB.Telephone 01452 726700 or email [email protected] to contribute and comment.
THE NEW BSAVA WEBSITE
Additional stock photography Dreamstime.com© Eric Isselée | Dreamstime.com© Fernando Soares | Dreamstime.com© Hanna Monika Cybulko | Dreamstime.com© Tony Campbell | Dreamstime.com
The new BSAVA website has now been launched. The site will provide members with exclusive member-
only content, news and views. Accessible through the site will be archived versions of:
JSAP ■
The ■ Formularycompanion ■ ; as well asDiscounted BSAVA manuals ■
Courses; and ■
Four years of archived BSAVA Congress ■
downloads, equating to over 1,200 hours of continuing professional development (CPD).
The site has been developed by its members, for its members and will continue to evolve from this embryonic state. With this in mind, the Association welcomes suggestions for areas of development. Notable new features include the launch of the new BSAVA Guide to the Use of Veterinary Medicines, providing the latest guidelines on legislation, dispensary information and waste disposal. The BSAVA has also made available to its members a new CPD Log, which will allow members to keep track of their latest CPD.
The site is split into seven categories, each of which will allow the veterinary surgeon to remain at the top of their profession. The divisions include CPD, giving information on course topics, veterinary and nursing courses, road shows and regional CPD. The membership section covers renewal and member benefits,
including access to JSAP, companion and the Small Animal Formulary, as well as an overview of the BSAVA structure and function. The Congress category provides information on the largest Small Animal Veterinary exhibition in the world, detailing the illustrious BSAVA Awards, Scientific Programme and Social Calendar. The Advice category gives veterinary professionals access to a host of veterinary resources, including practice information, policy statements, medicine issues and the new BSAVA Guide to the Use of Veterinary Medicines.
Members are well advised to regularly visit the BSAVA Publications area, which gives details, and allows online ordering, of the renowned BSAVA Manuals. The Forum and News sections will be developed over time in conjunction with VIN, allowing a unique tool to cross-reference professional diagnosis and further embellish the BSAVA membership community.
Existing members have been sent a password in order to gain access to member-only content. Once logged in, which will involve using your email address (membership number if email address is incorrect); it would be appreciated if you could take the time to ensure your profile information is up to date. Should you have any problems logging in to the BSAVA site, please telephone 01452 726700, or email [email protected] ■
including access to JSAP companion and

companion | 3
ROUND UP
MEET YOUR PRESIDENT
With experience in the regions, publications and finance at the BSAVA, Richard Dixon has built
a wealth of knowledge about the Association to take into his presidential year.
Veterinary careerRichard grew up in Edinburgh and studied at Glasgow University veterinary school, where he graduated in 1993. After a spell with the PDSA in Hull, he returned to Glasgow’s Small Animal Medicine Department, where he dealt with general internal medicine cases before completing a PhD in canine hypothyroidism. It was here, at the suggestion of his supervisor Dr Carmel Mooney, that Richard first got involved as a volunteer by organising Scottish Region CPD meetings for BSAVA.
After working as a staff member in Bearsden for seven years, he moved to Devon to work as a clinical pathologist for Axiom Laboratories in Teignmouth. Having set up the out-of-hours emergency service, Vets Now as a part-time project in December 2001, Richard soon realised this had become a full-time job in itself, so he and his wife Jan, who he met at vet school, returned to Scotland to run the business, and now live there with their three boys – the youngest, born just six weeks ago.
Association ambitionsThroughout his career and busy life Richard has managed to undertake key roles within BSAVA; leading local CPD provision as Regions’ Co-ordinator, directing the production of manuals as Chairman of Publications Committee, and steering the Association’s finances in his first role on the Board as Honorary Treasurer for three years. Now the longest serving Officer on
the Board, he says what a privilege it is to have worked with the volunteers and rest of the team at BSAVA.
“Everybody brings something different to the work of an organisation like the BSAVA”, says Richard, “and the skills you need to contribute to the running of a veterinary business and a not-for-profit organisation are actually very similar. The BSAVA has been hugely successful – largely because it is run by its own members – talented people who care about this profession, but we cannot take future success for granted. I will be using my year as President to try and get closer to our members, to find out exactly what they want from their Association, and to help ensure we are structured and run in a manner that enables us to respond to those needs into the future.”
As well as continuing to fulfil the original remit of providing quality CPD and advancing veterinary knowledge, Richard is keen that members appreciate the sense of community and support that belonging to BSAVA can mean. “We all know that life in practice can be a pretty lonely experience at times, especially when you first start. You move from a place where you know everybody and you have a tight group of friends to one where you may not know a
soul or have any personal support – this is where BSAVA comes in, especially through our regional network of CPD events and of course through the annual Congress. BSAVA is a great way of staying in touch with professional colleagues, and sharing experiences good and bad. Having that professional and personal support network is invaluable in addition to the day-to-day relationships with your boss and the people that you work with every day.” n
At BSAVA’s Annual General Meeting on the Sunday of Congress Ed Hall passed the presidential baton to Richard Dixon
A bonus issueWe have included atCongress with this edition of companion – the Congress magazine that was given out to delegates during the event, illustrating that once again BSAVA has delivered an event that we can all be proud of as members of the Association. Thank you to those who came and made it such a success. If you didn’t manage to come this year we hope to see you in 2010 – and of course, as a member you can download the MP3s online, so no need to miss out entirely!
Richard Dixon with the children from his old primary school who have created the artwork for his 2010 Congress design
ROUND UP
4 | companion
CONGRESS
Concourse Café gave delegates a welcome interlude from the main exhibition
Concourse Café gave delegates a Concourse Café gave delegates a Concourse Café gave delegates a Concourse Café gave delegates a welcome interlude from the main exhibition
Concourse Café gave delegates a welcome interlude from the main exhibition
Concourse Café gave delegates a welcome interlude from the main exhibition
Concourse Café gave delegates a welcome interlude from the main exhibition
Concourse Café gave delegates a Concourse Café gave delegates a
With delegate fi gures once again up,
visitors were able to access the
expertise of over 200 industry
specialists in the commercial exhibition
CONGRESS SNAPSHOTS
With delegate fi gures once again up, With delegate fi gures once again up,
visitors were able to access the With delegate fi gures once again up,
visitors were able to access the With delegate fi gures once again up,
visitors were able to access the With delegate fi gures once again up,
visitors were able to access the With delegate fi gures once again up,
expertise of over 200 industry
expertise of over 200 industry
specialists in the commercial exhibition expertise of over 200 industry
specialists in the commercial exhibition expertise of over 200 industry
expertise of over 200 industry
specialists in the commercial exhibition expertise of over 200 industry
specialists in the commercial exhibition With delegate fi gures once again up,
visitors were able to access the With delegate fi gures once again up,
visitors were able to access the With delegate fi gures once again up,
expertise of over 200 industry
specialists in the commercial exhibition expertise of over 200 industry
specialists in the commercial exhibition expertise of over 200 industry
The brand new BSAVA Balcony proved a great success, giving delegates an imperious view of the exhibition
Mark Oyama from the USA lectured on several topics, and was one of many revered overseas speakers to light up the scientifi c programme
Co-editors Anna Meredith and Emma Keeble enjoy the launch of their new BSAVA Manual of Rodents and Ferrets at the authors’ and editors’ lunch
Once again BSAVA Congress provided thousands of delegates with four days of world-class CPD and memorable social events
CONGRESSSNAPSHOTSSNAPSHOTS

companion | 5
CONGRESS
Frankie Boyle lit up the Comedy Club with his dark and satirical adult humour
Frankie Boyle lit up the Comedy Club with Frankie Boyle lit up the Comedy Club with
Irish super group The Saw
Doctors delivered the best of
Irish rock
Fantastic renditions from The Four
Tops, The Temptations, Stevie Wonder
and The Isley Brothers saw guests
demand a lengthy encore
The Motown Show set the Banquet Night alive as guests swayed to each soulful melody
Fantastic renditions from The Four
Fantastic renditions from The Four
Tops, The Temptations, Stevie Wonder Tops, The Temptations, Stevie Wonder
and The Isley Brothers saw guests and The Isley Brothers saw guests and The Isley Brothers saw guests and The Isley Brothers saw guests
demand a lengthy encoreand The Isley Brothers saw guests
demand a lengthy encoreand The Isley Brothers saw guests
demand a lengthy encoreand The Isley Brothers saw guests
demand a lengthy encoreand The Isley Brothers saw guests Glamorous guests congregate for a group picture during the most stylish night of Congress
Phil Hammond opened the BSAVA proceedings with a lecture of hilarity, anecdotes and comparisons between human and veterinary medicine
Past President John Bower presents
Nicola Bromley with the Frank
Beattie Travel Scholarship, allowing her to
spend time at TUFTS University, New EnglandBeattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to
spend time at TUFTS University, New Englandspend time at TUFTS University, New Englandspend time at TUFTS University, New Englandspend time at TUFTS University, New EnglandBeattie Travel Scholarship, allowing her to
spend time at TUFTS University, New EnglandBeattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to
spend time at TUFTS University, New EnglandBeattie Travel Scholarship, allowing her to Beattie Travel Scholarship, allowing her to
spend time at TUFTS University, New EnglandBeattie Travel Scholarship, allowing her to
spend time at TUFTS University, New EnglandBeattie Travel Scholarship, allowing her to
spend time at TUFTS University, New EnglandBeattie Travel Scholarship, allowing her to
After an extremely successful year in offi ce, Professor Ed Hall hands over presidential duties to Richard Dixon
The dancefl oor was jam-packed as The Hoosiers delivered a lively, energetic performance

6 | companion
CLINICAL CONUNDRUM
CLINICALCONUNDRUMNat Whitley of Davies Veterinary Specialists discusses a case of collapse in a young Boxer dog
Case Presentation
A 2-year-old male entire Boxer was presented with a history of three episodes of sudden-onset weakness and collapse occurring over a 2-week period. All episodes had occurred during the day and without preceding clinical signs. On two occasions the dog had just entered the house after running in the garden. On the third occasion the dog had just woken up and got to its feet and had a drink. All occasions were characterised by staggering, followed by leaning against the wall and falling into sternal or lateral recumbency, where the dog remained for 10–20 seconds, with a glazed expression, before rapid recovery within 1–2 minutes. On one occasion the forelimbs appeared rigid. On the other occasions the limbs were flaccid. There had been no changes in appetite, thirst or body weight. The owner reported that the dog had always snored and had noisy breathing. On physical examination, heart rate was 80 beats per minute with marked respiratory sinus arrhythmia. No murmurs were present. The nares were stenotic and causing increased upper respiratory noise. The rest of the examination, including neurological examination, was unremarkable.
Based on the information you have so far, create a problem list
Collapsing episodes n
Stenotic nares (Figure 1). n
What differential diagnoses should be considered at this stage?The term ‘collapse’ is very broad, simply referring to inability to stand, and requires further scrutiny to make progress with the case. The description of the episodes fits best with syncope or near syncope rather than seizure activity. Syncope refers to transient loss of consciousness associated with cerebral hypoxia. The most common cause of syncope is reduced cardiac output resulting from paroxysmal cardiac arrhythmia. Weakness associated with
hypoglycaemia can resemble cardiogenic syncope. Other systemic or metabolic derangements (anaemia, hypocalcaemia, hepatic encephalopathy) could cause these symptoms but are often associated with additional symptoms or physical examination abnormalities. For upper airway obstruction to cause the episodes through hypoxia there would be a more consistent association with exercise or excitement. Myaesthenia gravis would also tend to be exercise-induced. The distinction between syncope and seizure can be challenging but rapid onset and offset of symptoms without pre- or post-ictal signs, and lack of consistent extensor rigidity or neurological abnormalities on physical examination, made a seizure disorder less likely.
What initial investigations are appropriate?In light of the number of possible causes for the symptoms, haematology, biochemistry and urinalysis are appropriate to rule out systemic disease. In this case the results were all within normal limits. However, with metabolic causes of weakness, the metabolite in question can fluctuate; so, when suspicion of a metabolic problem is high, serial sampling or further investigations (such as measurement of ionised calcium if hypocalcaemia is suspected, especially if total calcium is at the lower end of normal) may be appropriate.
Given the history and lack of other changes (normal total calcium and lack of a hepatic insufficiency profile on biochemistry), hypoglycaemia was the only metabolic cause considered. Sepsis, glucocorticoid deficiency (atypical hypoadrenocorticism) and insulinoma are important causes of hypoglycaemia in adult Figure 1: Stenotic nares

companion | 7
CLINICAL CONUNDRUM
dogs. All of these were unlikely. Glucocorticoid deficiency normally causes chronic malaise before progressing to hypoglycaemia and although Boxers are predisposed to insulinoma, the author is not aware of reports in dogs less than 4 years old. Where there is a real suspicion of insulinoma and serial blood glucose readings are normal, measurement of fructosamine is useful, with low concentrations suggestive of insulinoma.
Boxers are also predisposed to cardiogenic syncope and further investigations were pursued along those lines.
What cardiac conditions are associated with syncope in young Boxers?
Aortic stenosis is common in Boxers n
and in severe cases can cause syncope via ventricular arrhythmia or simply outflow obstruction. However, such a defect is characterised by a loud heart base murmur, not present in this case.Cardiomyopathy – arrhythmogenic right n
ventricular cardiomyopathy (ARVC) is the most common type of cardiomyopathy to affect Boxers. Many affected dogs have ventricular arrhythmias of a characteristic morphology with or without syncope. Some progress to show evidence of myocardial (systolic) dysfunction,
supraventricular arrhythmias and congestive heart failure. Rarely, sudden cardiac death is the first and only symptom of the disease.Neurocardiogenic syncope – this n
condition may also be referred to as vasodepressor syncope, vasovagal syncope or reflex-mediated syncope, and can occur in healthy dogs or those with systemic disease. Expressed in lay terms, the dog has ‘fainted’. Understanding of this condition in dogs is poorly understood, but certain activities or concurrent conditions trigger a sudden autonomic imbalance characterised by appropriate sympathetic nervous system activation being rapidly and inappropriately aborted, coincident with increased vagal input to the cardiovascular centre of the brainstem, leading to increased vagal output. The result is sudden vasodilation and bradycardia (sinus bradycardia, sinus arrest or transient atrioventricular block), hence hypotension and cerebral hypoxia. When a given situation or activity triggers syncope this is often referred to as ‘situational syncope’. In the author’s experience this is particularly common in brachycephalics – examples of triggers include:– Cough– Urination
– Defecation– Vomiting– Exertion/excitement (being startled,
barking, climbing stairs, going from inactivity to ‘normal activity’).
What cardiac investigations are appropriate when cardiogenic syncope is suspected?Most cardiogenic syncope is associated with arrhythmia. Definitive diagnosis can only be made by auscultation and/or ECG and blood pressure recording during a syncopal episode. Video recordings obtained by the owner (preferably with concurrent palpation of the apex beat or femoral pulse and observation of membrane colour) are variably useful. Cardiac assessment is indicated using the conventional and widely available tools of standardised paper trace ECG recording, thoracic radiographs and echocardiography. This is in order to rule out macroscopic evidence of cardiac disease (congenital and acquired disorders) and radiographic evidence of lung disease. In this case these were performed and results were normal, with only a respiratory sinus arrhythmia present on the ECG recording (Figure 2). Blood pressure and serum cardiac troponin concentration were also measured and were normal. Elevation in cardiac troponin may be present in any cardiac disease when inflammation or necrosis is occurring within the myocardium,
Figure 2: ECG recording showing sinus arrhythmia (25 mm/s, 0.5 cm/mV)

8 | companion
CLINICAL CONUNDRUM
CLINICAL CONUNDRUM
such as in many cardiomyopathies, myocarditis and infarction.
Is any further assessment required or can a diagnosis be made at this point?Due to the short duration of the standard paper ECG recording (rhythm strips are normally recorded for 1–2 minutes), occult ARVC had still not been excluded and longer duration ECG recording was appropriate. Options include hospitalisation for on-screen ECG monitoring or ambulatory Holter monitoring. Holter monitoring is preferable, since the dog can resume normal activity at home whilst wearing the monitor, with more chance of a syncopal event being recorded. Owners are instructed to keep a log recording the timing of significant activities and events while the Holter monitor is in place (for example, when the dog is sleeping, feeding, exercising, greeting visitors).
A 24-hour Holter recording was performed in this case. No syncopal events occurred during this time. Analysis of the
recording did not reveal any periods when heart rate was considered inappropriate for the dog’s activity level. Very occasional ventricular ectopic beats were recorded, but most of these were isolated escape beats following sinus pauses when the dog was asleep rather than ventricular premature complexes (VPCs). Rare atrial premature complexes were recorded. In total there were 48 aberrantly conducted complexes in 24 hours. These findings were not suggestive of occult ARVC based on criteria derived from a screening programme using 600 asymptomatic dogs, which suggested that a normal Boxer has < 50 VPCs per 24 hours (Meurs and Spier, 2009).
DiagnosisBased on the description of the episodes and the lack of evidence for cardiac or other disease on investigations, a presumptive diagnosis of neurocardiogenic syncope was reached. This is quite a common scenario when the syncope is not sufficiently frequent or predictable to
ReferenceMeurs KM and Spier AW (2009) Cardiomyopathy in Boxer dogs. In: Current Veterinary Therapy XIV, Eds Bonagura and Twedt, pp.797–799. Philadelphia, Saunders
document the heart rhythm at the time of the event, and the presumptive diagnosis must be kept under scrutiny in light of any further developments.
How could the stenotic nares be implicated in syncope?Brachycephalic dogs often have high vagal tone and this may be exacerbated by upper airway obstruction. Since neurocardiogenic syncope may be precipitated by both situations and by medical conditions that alter autonomic balance, it is logical to correct or avoid possible contributing factors. In this case it was decided to anaesthetise the dog for surgical correction of the stenotic nares and rule out other components of brachycephalic airway syndrome (overlong soft palate, secondary laryngeal dysfunction), hence reducing excessive vagal tone. The palate and larynx were normal and so the only surgery performed was alar fold resection for the stenotic nares. Recovery was unremarkable and there was no recurrence in syncope on follow-up 2 months after initial presentation.
How is recurrent neurocardiogenic syncope managed?This depends very much on the nature of the trigger. In some cases anticholinergic drugs, such as propantheline, are effective. However, although these may alleviate the bradycardia, some patients may still collapse due to hypotension associated with vasodilation. In other cases beta-blockers (working earlier in the reflex arc that triggers the syncope) have proved more successful. n
Holter monitoringThe connectors are attached to studded self-adhesive electrodes positioned on the skin over the right and left apex and left heart base areas. The leads are secured to the dog using tape and the monitor itself located in a fabric pocket within a protective but non-restrictive jacket/harness worn by the dog. Data are recorded direct to a memory card, and subsequently downloaded to computer and converted by software to a more conventional ECG tracing. Analysis of the ECG is then performed by computer, with additional interpretation of suspect or unusual sections of the trace performed by a cardiologist. Some monitors permit longer recordings or ‘event’ recording.

companion | 9
SUICIDE
SUICIDE IN OUR PROFESSION
Proportional mortality ratios (PMRs) for suicide in the last 25 years indicate that the UK veterinary profession has
around four times the proportion of all deaths certified as suicide than would be expected from the proportion for the general population, and around twice that for other
healthcare professionals. David J. Bartram reports
There has been much speculation regarding possible factors or influences underlying the increased
suicide risk in the profession but little empirical research.
Possible factors include the characteristics of individuals entering the profession, negative effects during undergraduate training, work-related stressors (such as long working hours, inadequate support, emotional exhaustion, client expectations and unexpected clinical outcomes), ready access to and knowledge of means (medicines are typically stored in practice premises and deliberate self-poisoning is the most common method of suicide in both male and female veterinarians), stigma associated with mental illness, professional and social isolation, and alcohol or drug misuse (mainly prescription drugs to which the profession has ready access such as ketamine, benzodiazepines and opiates).
Attitudes to death and euthanasia (formed through the profession’s routine involvement with euthanasia of companion animals and slaughter of farm animals) and suicide contagion (due to direct or indirect exposure to suicide of peers within this small profession) are other possible influences. These occupation-specific factors are assumed to act in association with other variables known to be more widely associated with completed suicide, including male gender and single status, the presence of anxiety or depressive symptoms, and recurrent suicidal thoughts.
Studying suicideThe contribution of mental health and well-being to the elevated risk was assessed through a postal questionnaire survey
(mailed in October/November 2007) of a large stratified random sample of 3,200 veterinary surgeons practising in the UK: A cross-sectional study of mental health and well-being and their associations in the UK veterinary profession. Academic supervision for the study was provided by the School of Medicine, University of Southampton. Anxiety and depressive symptoms, alcohol consumption, negative thoughts about life, positive mental well-being, aspects of the working environment, and work–home interaction were assessed.
The completed questionnaire was returned by 1,796 participants, a response rate of 56%. Compared to the general population, the sample reported: high levels of anxiety and depressive symptoms; higher 12-month prevalence of suicidal thoughts; less favourable psychosocial working conditions, especially in regard to the high level of demands and low level of managerial support; lower levels of positive mental well-being; and higher levels of negative work–home interaction. The levels of psychological distress reported suggest ready access to and knowledge of lethal means is probably not operating in isolation to increase suicide risk within the profession.
The questionnaire was anonymous but respondents were given the option to provide their contact details if they were willing to be considered for a possible subsequent phase of research involving confidential interviews of selected individuals. Over half of the respondents supplied their name and telephone contact details.
BSAVA and SPVS kindly provided financial support for the next phase of the research which began in spring 2009, a telephone interview study of respondents
who reported suicidal thoughts in the 12 months prior to completing the questionnaire. The main objectives are to explore the causes to which suicidal thoughts are attributed, investigate help-seeking behaviours and barriers to help-seeking within the profession, and to identify potential implications for the provision of interventions.
If you are concerned about your mental health or well-being, you may wish to contact your GP or other healthcare professional, Vet Helpline (Tel: 07659 811 118, www.vetlife.org.uk) or Samaritans (Tel: 08457 909 090, www.samaritans.org). n
David graduated from the RVC in 1988 and after three years in farm animal practice began a career in the pharmaceutical industry, working in both animal and human health sectors. In addition to his full-time work he is a part-time PhD student at the University of Southampton, where he is involved with research into the mental health of the veterinary profession. David is also a Samaritans volunteer and a Director of the Veterinary Benevolent Fund.
David J. BartramBVetMed, DipM, MCIM, CDipAF, MRCVS

10 | companion
HOW TO…
GET GREAT ULTRASOUND IMAGES
HOW TO…
Diagnostic ultrasonography is an imaging modality that is now widely available in general practice. It has developed from a useful means of pregnancy diagnosis to an invaluable
diagnostic tool, with a wide range of potential applications. In order to glean as much diagnostic information as possible from an ultrasound examination, it is vital to acquire good quality images. Even the most experienced operator may struggle to obtain good images in some situations; it is more difficult, for example, to acquire really nice ultrasound images from an obese patient than from a lean one. However, there are important steps which can be taken to optimise the images and thus the information available from them.
Key steps to success
Step 1: Position the patient correctlyRoutine abdominal ultrasound imaging may be performed with the patient in lateral (Figure 1) or dorsal recumbency, according to personal preference and patient tolerance. It can be useful to adjust patient position if gastrointestinal gas obscures an area of interest (Figure 2), in order to redistribute gas away from the area. Routine cardiac ultrasound examinations are usually carried out with the patient in lateral recumbency, imaging from the dependent side to reduce the interference from air-filled lung.
Step 2: Select and prepare the scanning site carefullyThe scanning site should be an area of the body overlying the area of interest, which avoids intervening gas or bone as far as possible. For example, an approach to the liver may be made either from behind the xiphisternum and ribs, angling the sound beam cranially, or from between the ribs. The scanning site should ideally be clipped to remove hair/fur and the skin cleaned with surgical spirit to remove dirt and grease before applying liberal quantities of acoustic gel. If there is poor skin preparation, there will be poor
Frances Barr, Past President and pioneer in the use of ultrasound in veterinary medicine, shares her tips for success with companion readers
Figure 2: Ultrasonographic image of the cranial abdomen, showing part of the liver and the stomach. Gas within the stomach produces shadowing and reverberation, and prevents visualization of deeper structures
Figure 1: A Labrador Retriever positioned in right lateral recumbency for ultrasound examination of the left kidney

companion | 11
HOW TO…
transducer contact, resulting in concentric or parallel lines across the image or a very dark image (Figure 3).
Step 3: Choose the appropriate sound frequencyMost modern ultrasound machines offer a choice of sound frequency, either by changing transducer or by altering the frequency within the defined range of an individual transducer. High frequencies (7.5 MHz or above) generally result in improved image resolution but reduced tissue penetration (Figure 4A). The converse is true of low frequencies (5 MHz or lower) (Figure 4B). The highest frequency available should be selected, consistent with the depth of penetration required. A 7.5 MHz transducer is satisfactory for most small animal examinations. A higher frequency can be used for very superficial structures (e.g. eye, thyroid) or in cats or small dogs; and a lower frequency may be required for the heart or deeper abdominal organs in larger dogs.
Step 4: Adjust the gainThis is a very important step in optimisation of the image, yet one
that is often ignored. The gain controls adjust the electronic amplification of the returning echoes, and thus the brightness of the image. There is often an overall gain control which brightens or darkens the whole image. Of more importance are the controls, usually a series of knobs or sliders, which allow selective amplification of the image at different depths. Since the echoes returning from deeper tissues have been attenuated to a greater extent than those returning from superficial tissues, they require more amplification. The aim is to obtain an image of even brightness throughout the depth of field. Where gain is too low, important image information will be lost; where gain is too high, detail may be lost within the ‘background noise’ (Figure 5).
Step 5: Adjust the depth of fieldThis is another important step which may be overlooked. A large depth of field may be useful at the start of an ultrasound examination, since this allows an overview of organs and ensures deeper structures are not missed. However, when examining a particular tissue or organ in detail, it is important to adjust the depth of field so that the region of interest occupies a reasonable proportion of the field of view. Too small a depth of field may result
GET GREAT ULTRASOUND IMAGES
Figure 3: Ultrasonographic image of a cat’s kidney, showing mild dilatation of the renal pelvis. Poor contact between the skin surface and the edge of the transducer has resulted in loss of the image along the right margin
Figure 4: Ultrasonographic images of the liver of a large breed dog. (A) 8.5 MHz transducer: although image detail is good for the superficial parts of the liver, there is little information from the deeper parts of the liver due to inadequate penetration of the sound beam. (B) 5.5 MHz transducer: improved penetration of the sound beam results in better visualization of the deeper parts of the liver
A B

12 | companion
HOW TO…
GET GREAT ULTRASOUND IMAGES
Figure 5: Ultrasonographic images of the canine spleen. (A) There is loss of image information in the superficial part of the organ. The near field gain has been set too low. Nonetheless, multiple anechoic foci are visible scattered throughout the splenic parenchyma. (B) For this image from a different dog, the overall gain was set too high, resulting in an excessively bright image. (C) For the same dog as b, reducing the gain has produced an image of even brightness throughout the depth of field, avoiding excessive ‘noise’ but retaining all relevant architectural information
A
B
CFigure 6: Ultrasonographic image of the left kidney of a cat. (A) The depth of field is excessive, resulting in the kidney appearing to be very small at the top of the image. (B) The depth of field has been adjusted so that the kidney occupies much of the field of view, allowing more detailed evaluation of its architecture
A
B
in a rather pixellated image and/or exclusion of the margins of the region of interest. Too large a depth of field results in a tiny image at the top of the screen which cannot be evaluated accurately (Figure 6).
Step 6: Adjust the focal zoneMany modern ultrasound machines allow the position of the focal zone to be changed, as indicated by a tab or other marker on the edge of the image. The focal zone determines the depth of the image at which lateral resolution is optimal, and so should be adjusted to correspond with location of the tissue or organ of particular interest (Figure 7).
Step 7: Adjust the sector angleWhen using a sector or curvilinear transducer, it may be possible to adjust the sector angle. It is useful to start the ultrasound examination with a broad angle to give a wide field of view,

companion | 13
HOW TO…
GET GREAT ULTRASOUND IMAGES
Figure 7: Ultrasonographic image of the neck of the bladder and the prostate. The calipers mark the edges of a small intraprostatic cyst. The tab circled in red to the right of the image indicates the focal zone; this has been positioned to correspond with the area of interest.
allowing a better appreciation of the relationship between structures. It can then be helpful to reduce the angle to examine a region in more detail, since a narrower sector angle results in improved image resolution.
Step 8: Adjust the frame rateA high frame rate is ideal for evaluation of moving structures, but results in a reduction in the number of scan lines per frame and thus reduced image detail. Conversely, a low frame rate allows a higher number of scan lines per frame and improved detail, but movements will be seen less accurately and may appear jerky and disconnected. A high frame rate is therefore usually selected for cardiac examinations, while a lower frame rate is used for most abdominal examinations; this is often taken into account in the presets selected when choosing ‘cardiac’ or ‘abdominal’ imaging, but may also be adjusted independently.
Correcting a poor imageOnce the patient has been prepared and positioned, and the ultrasound machine settings adjusted to take all of the above factors into account, the ultrasound image will usually be good. But occasionally the image is still poor. In such instances it is worth considering whether:
The scanning site has not been well prepared. Inadequate ■■
clipping, or dirty or crusty skin can compromise contact between the transducer and skin surface. Cleaning gel from the site, cleaning the skin again and reapplying the gel can sometimes helpGastrointestinal contents (food, gas, faecal material) may be ■■
interfering with the image. If this is the case, adjusting the position of the animal to redistribute the gas can be helpful. Sometimes using a different approach allows the organ of
Figure 8: Lateral abdominal radiograph of a dog with peritonitis. There is a marked lack of abdominal detail and free peritoneal gas is visible dorsocranially. Good-quality ultrasound images might be difficult to obtain in such a patient
interest to be viewed without intervening gas or ingesta. For example, a lateral approach to the kidneys, as an alternative to a ventral approach, may avoid intervening intestine. Walking a canine patient can encourage evacuation of the colon, while allowing a drink of water can reduce the interference from stomach gasThere may be free gas in the body cavity or subcutaneous ■■
emphysema which is interfering with sound transmission. The latter is usually readily identified clinically. A pneumothorax or pneumoperitoneum may be suspected if ultrasound images are unexpectedly poor, but radiography is the way to confirm this (Figure 8)Analgesia or sedation may be indicated if the patient is panting, ■■
restless or uncooperative.
Take your timeThere is increasing use of ultrasound as a diagnostic modality in veterinary medicine, and consequently a developing confidence and expertise in the acquisition and interpretation of images. A little extra time when preparing the patient for an ultrasound examination and when adjusting the controls of the ultrasound machine can yield enormous benefits in the quality of images obtained and the resultant information available from them. ■
14 | companion
VIN
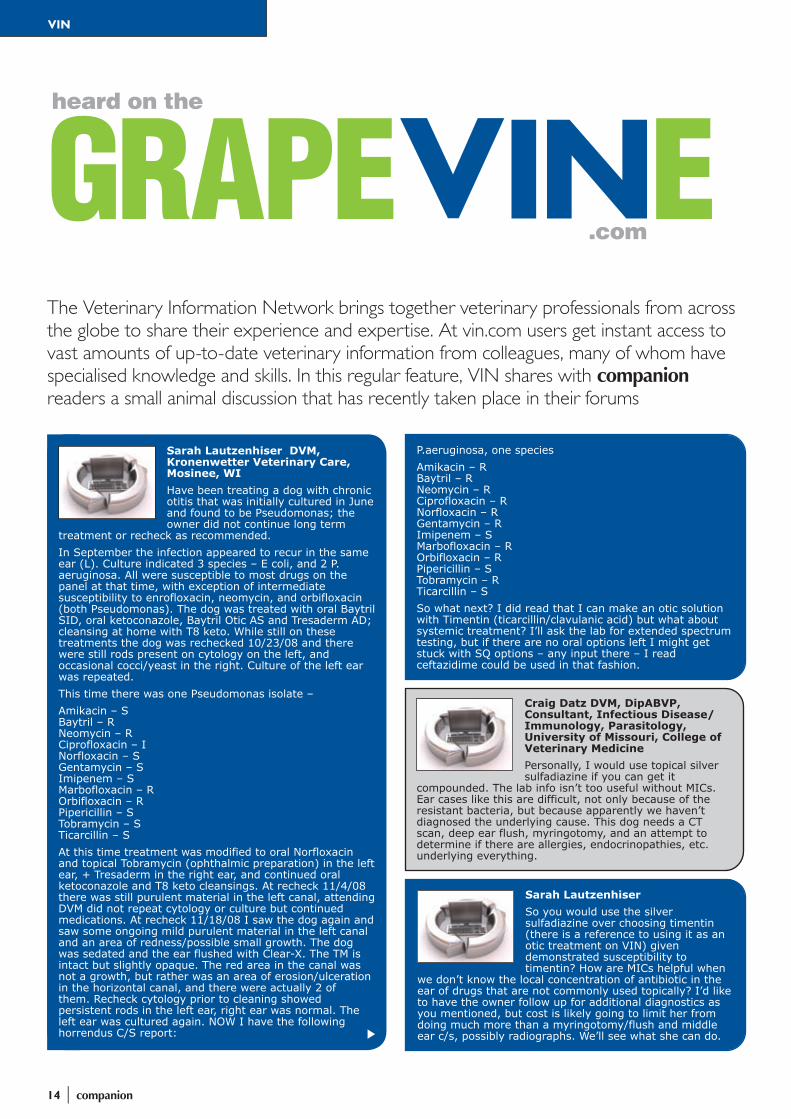
The Veterinary Information Network brings together veterinary professionals from across the globe to share their experience and expertise. At vin.com users get instant access to vast amounts of up-to-date veterinary information from colleagues, many of whom have specialised knowledge and skills. In this regular feature, VIN shares with companion readers a small animal discussion that has recently taken place in their forums
.comGRAPEVINEheard on the
Craig Datz DVM, DipABVP, Consultant, Infectious Disease/Immunology, Parasitology, University of Missouri, College of Veterinary MedicinePersonally, I would use topical silver sulfadiazine if you can get it
compounded. The lab info isn’t too useful without MICs. Ear cases like this are difficult, not only because of the resistant bacteria, but because apparently we haven’t diagnosed the underlying cause. This dog needs a CT scan, deep ear flush, myringotomy, and an attempt to determine if there are allergies, endocrinopathies, etc. underlying everything.
Sarah Lautzenhiser So you would use the silver sulfadiazine over choosing timentin (there is a reference to using it as an otic treatment on VIN) given demonstrated susceptibility to timentin? How are MICs helpful when
we don’t know the local concentration of antibiotic in the ear of drugs that are not commonly used topically? I’d like to have the owner follow up for additional diagnostics as you mentioned, but cost is likely going to limit her from doing much more than a myringotomy/flush and middle ear c/s, possibly radiographs. We’ll see what she can do.
Sarah Lautzenhiser DVM, Kronenwetter Veterinary Care, Mosinee, WIHave been treating a dog with chronic otitis that was initially cultured in June and found to be Pseudomonas; the owner did not continue long term
treatment or recheck as recommended. In September the infection appeared to recur in the same ear (L). Culture indicated 3 species – E coli, and 2 P. aeruginosa. All were susceptible to most drugs on the panel at that time, with exception of intermediate susceptibility to enrofloxacin, neomycin, and orbifloxacin (both Pseudomonas). The dog was treated with oral Baytril SID, oral ketoconazole, Baytril Otic AS and Tresaderm AD; cleansing at home with T8 keto. While still on these treatments the dog was rechecked 10/23/08 and there were still rods present on cytology on the left, and occasional cocci/yeast in the right. Culture of the left ear was repeated.This time there was one Pseudomonas isolate –Amikacin – S Baytril – R Neomycin – R Ciprofloxacin – I Norfloxacin – S Gentamycin – S Imipenem – S Marbofloxacin – R Orbifloxacin – R Pipericillin – S Tobramycin – S Ticarcillin – SAt this time treatment was modified to oral Norfloxacin and topical Tobramycin (ophthalmic preparation) in the left ear, + Tresaderm in the right ear, and continued oral ketoconazole and T8 keto cleansings. At recheck 11/4/08 there was still purulent material in the left canal, attending DVM did not repeat cytology or culture but continued medications. At recheck 11/18/08 I saw the dog again and saw some ongoing mild purulent material in the left canal and an area of redness/possible small growth. The dog was sedated and the ear flushed with Clear-X. The TM is intact but slightly opaque. The red area in the canal was not a growth, but rather was an area of erosion/ulceration in the horizontal canal, and there were actually 2 of them. Recheck cytology prior to cleaning showed persistent rods in the left ear, right ear was normal. The left ear was cultured again. NOW I have the following horrendus C/S report:
P.aeruginosa, one speciesAmikacin – R Baytril – R Neomycin – R Ciprofloxacin – R Norfloxacin – R Gentamycin – R Imipenem – S Marbofloxacin – R Orbifloxacin – R Pipericillin – S Tobramycin – R Ticarcillin – SSo what next? I did read that I can make an otic solution with Timentin (ticarcillin/clavulanic acid) but what about systemic treatment? I’ll ask the lab for extended spectrum testing, but if there are no oral options left I might get stuck with SQ options – any input there – I read ceftazidime could be used in that fashion.

companion | 15
VIN
All content published courtesy of vin.com. For more details about the Veterinary Information Network visit vin.com. As VIN is a global veterinary discussion forum not all diets, drugs or equipment referred to in this feature will be available in the UK, nor do all drug choices necessarily conform to the prescribing rules of the Cascade. Discussions may appear in an edited form.
Sarah LautzenhiserHello everyone and thanks for your input. We finally cleared up this ear, using the topical Timentin preparation. It’s prepared according to the manufacturer’s recommendation (13 ml sterile water added to the vial of
3.1 g Timentin) and stored frozen in aliquots. I prepared this for the owner in 2 ml aliquots, for her to thaw one aliquot each day and place 1 ml in the affected ear BID (keep the unused portion refrigerated.) We treated with the Timentin for I believe 4–6 weeks.Oral prednisone was also used because of the ulceration. This did appear to clear up the infection, without myringotomy. Had a little trouble with a bout of mild yeast otitis as the rods were going away, which responded to oral ketoconazole. Thankfully, the ear did check clean cytologically and looked good on two separate exams after that, a few weeks apart. Need to get him in to recheck again soon!Thanks again everyone for some great ideas on treating this case.
Michelle Harvath, DVM, VIN ISG Team (Database Division), Lake Orion, MIHere is the paper alluded to by Craig and CarolEvaluation of outcome of otitis media
after lavage of the tympanic bulla and long-term antimicrobial drug treatment in dogs: 44 cases (1998–2002)J Am Vet Med Assoc. August 2004;225(4):548–53.OBJECTIVE: To evaluate the outcome of otitis media in dogs after video-otoscopic lavage of the tympanic bulla and long-term antimicrobial drug treatment.CONCLUSIONS AND CLINICAL RELEVANCE: Results indicate that lavage of the tympanic bulla combined with medical management is an effective and viable option for treatment of otitis media in dogs.
Links to more information, the full journal articles mentioned and an unedited version of this discussion are available at VIN.com by following the link http://vin.com/Link.plx?ID=44761
Carol Foil MS DVM DipACVD, VIN Consultant, Louisiana State University, Baton Rouge, LAA couple of points beyond what Craig has said.1) It is good to note that C&S results
are based on systemic blood levels of antibiotics … and that is usually in µg/ml, WAAY below what can be acheived in topical meds in the ear. That is why topical 10 mg/ml solutions of Baytril (usually in Tris EDTA which potentiates their efficacy) is often effective despite C&S results being resistant to enro. It is still what we usually recommend in your situation.2) What usually limits the efficacy of any topical therapy is not resistance but access to the nidus. This can be limited by volume of treatment … it takes 0.5–2 ml of liquid to even get to the tympanum in a normal dog ear. That is another advantage of Tris EDTA/Baytril solutions .. you can afford to use the proper volume frequently. It is the limitation of preparations like Baytril Otic (which has silver sulfadiazine in it, btw) and ophthalmic tobramycin. Another thing that limits efficacy is either stenosis of the ear canal or the presence of otitis media …3) This dog very likely has otitis media. That is a surgical disease. I appreciate that owners can find it very difficult to afford proper treatment, but that does not change medical facts. Other practitioners faced with the grim reality of not being able to treat this with GA flush, myringotomy (which I consider as a surgical approach) bulla osteotomy etc have turned to using BNT ointment as a second best thing or ear wicks.
Craig Datz I’ve used both (sulfadazine, timentin). Silver is better for ulceration that you mentioned. There are other options, of course, including topical quinolones. Given that the organisms is showing resistance to all fluoroquinolones
that’s where MICs come in. Resistance is predicted based on attainable serum levels of antibiotics and in vitro growth characteristics. If you’ve ever looked at the Baytril dose label, you can legally use 5–20 mg/kg. Some bacteria are easily killed with the 5 dose, others need 10, and still others will be resistant at 15 but susceptible at 20.>>> cost is likely going to limit her >>> understood. When I started doing referral ear cases, I had to learn how to look clients in the eye and tell them it may be $1,000 or more to clear up a chronic or resistant ear infection. That’s quite a shock when they’ve been used to spending $50–75 at the vet.

16 | companion
SAVSNET
SPOTLIGHT ONSMALL ANIM AL DISEASES‘Common things are common’ is an old medical maxim that has been passed on to generations of veterinary students. A reasonable response when receiving that advice would be ‘How do we tell?’ That’s because there are rarely any objective data on the prevalence of diseases affecting companion animals and opinions on their relative significance are often based on the personal impressions of senior practitioners. However, a project at Liverpool vet school may soon provide some of the first reliable information on what is really happening in consult rooms around the country. John Bonner reports
If you want to know which endemic diseases are causing concern for farm animal vets across Britain, you need look
no further than the Veterinary Laboratories Agency and the Scottish Agricultural College’s monthly VIDA disease surveillance reports. Ask the same question of an equine practitioner, and he or she will refer you to the Animal Health Trust website and its quarterly reports based on submissions to laboratories testing samples from the UK horse population.
In contrast, trying to get a handle on what is happening in small animal practice is much trickier. A new disease entity may produce a letter in the Veterinary Record, and an academic survey may highlight changes in the estimated prevalence of a particular condition over past decades. But there is no effective ‘real time’ surveillance system looking for new or emerging diseases and no satisfactory database which will give an accurate picture of the health status of the country’s canine and feline inhabitants.
New surveillance projectSAVSNET, the Small Animal Veterinary Surveillance Network, is an attempt to remedy these deficiencies being developed by staff at the University of Liverpool veterinary faculty. The project is a collaboration with the computer software company Vet Solutions and backed by a consortium including BSAVA, Defra, the AHT, and a group of leading pharmaceutical companies.
Developing some form of surveillance system has long been a pet project of Professor Rosalind Gaskell, head of the research group on small animal infectious diseases at Liverpool. Her efforts brought
companion | 17
SAVSNET
SPOTLIGHT ONSMALL ANIM AL DISEASES
the consortium together about three years ago to begin the complex process of getting the initiative off the ground. In September 2008 Áine Tierney was appointed to the job of coordinating the project after completing her BSc in bioveterinary science at Liverpool vet school and an MSc in veterinary parasitology at the Liverpool School of Tropical Medicine.
Diagnostic dataSAVSNET encompasses two important elements; the first involves recruitment of veterinary diagnostic laboratories from around the UK, the collection and collation of their anonymised results, and the compilation of quarterly reports based on the findings. Initially, the focus will be on infectious disease in cats and dogs but will expand as the project develops to include other diseases and species. “The project will evolve in stages; it is a continual process of development. We are working closely with the diagnostic labs who have been very supportive of this project and we are ironing out any problems we encounter as we go along,” Ms Tierney explains.
This part of the project has already been successfully run on a pilot scale during the last quarter (October–December) of 2008 and the SAVSNET team are currently analysing the results. “Because it is based on actual diagnostic results, we will be able to combine data for similar tests, even though they may have been carried out by several different labs” said Dr Alan Radford, Senior Lecturer in Small Animal Infectious Diseases at the University of Liverpool. “This way we can gain an impression of the number of cats and dogs infected with a particular pathogen, and how this varies over time and in different parts of the country”.
At practice levelIn the second part of the project, which is perhaps more challenging, SAVSNET aims to capture data on the diagnosis and treatment by practitioners of more syndromic conditions, for example, diarrhoea in a dog or persistent vomiting in a cat. But how can you access such information? The solution identified lies within the practice management software produced by Vet Solutions. Each animal’s details (such as age, sex, breed) are already recorded in the practice database. In addition, at the end of each consultation, the computer will ask the duty vet a series of questions about the case and the proposed treatment strategy.
Simplicity is the key goal in this process as a busy practitioner will not have time to fill out a long questionnaire during the consultation and if left to later, he/she may forget certain details, limiting the scientific value of the report. “Once a vet has gone through the questions a couple of times, we would not expect the answers to take more than about 10 seconds. We have to get good compliance from the practitioners involved – if they find it awkward and time-consuming they will simply remove themselves from the project,” Dr Radford warns.
Another advantage of the approach taken by SAVSNET is that the vet does not have to remember to file the report. All details entered into the clinical records are automatically backed up and stored at the company’s headquarters in Edinburgh from where they will be anonymised before sending to the SAVSNET team.
Engagement essentialParticipation in this part of the SAVSNET project will be completely voluntary. The
team are aiming to enrol as many veterinary premises as possible to provide a representative sample for the UK. If all 765 veterinary premises using Vet Solutions software agree to participate in the scheme, it could potentially gather details from more than 150,000 veterinary consultations a day. However, practices which, for whatever reason, decline to take part will still be able to use the company’s software. Two medium sized practices – the Andale Veterinary Centre in Widnes and the Rufford Veterinary Group in Ormskirk, have agreed to be the ‘guinea pigs’ for the pilot phase. “We will work closely with these two practices and Vet Solutions in this the pilot phase to ‘perfect’ the software before we roll it out on a national scale,” Ms Tierney explains.
“Apart from needing it to be straightforward, there are two other factors which will determine vets’ willingness to take part. We have to ensure that all the questions we are asking are clinically relevant and, when we have gathered in the data, we have to make them available to the practices concerned. The

18 | companion
SAVSNET
data will be completely anonymised before going on a publicly accessible website soon to be launched (www.liv.ac.uk/SAVSNET). We also hope to tell the individual practices how their results compare with national averages,” Dr Radford explains. “It is important to us to be able to give something back to the vets who are helping us run this part of the project.”
Building on experienceDr Richard Newton from the Animal Health Trust is also a member of the management team for the SAVSNET project and has been a key advisor during the planning process. Richard and his colleagues in the Trust’s epidemiology department are responsible for the system of quarterly reports on horse diseases set up in 2004. This has support from both Defra and the British Equine Veterinary Association and was a response to the concerns about the
adequacy of disease surveillance raised in the wake of the 2001 foot-and-mouth disease epidemic.
The SAVSNET system has been partially modelled on the Trust’s work but with a few additional ‘bells and whistles’. The equine database focuses on infectious disease reports submitted by the responsible individual within a network of commercial and practice laboratories. The AHT system makes no attempt to gather the syndromic data included in the second part of the SAVSNET project. In addition, the Trust no longer aims to collect data on antimicrobial resistance which SAVSNET also intends to collect.
“We tried to collect that information but it became too complicated and we realised that with the data gathering system we have, it would not produce consistent and scientifically meaningful data,” Dr Newton recalls. “But the SAVSNET
approach is very different in placing an onus on the individual vet using the practice computer system. It will be very interesting to see how that works and we hope that we will be able to learn some lessons that will allow us to extend and improve our equine database.”
BSAVA Honorary Secretary Alison Speakman explains the Association’s involvement: “BSAVA are pleased to support this exciting and challenging new project which will provide valuable information to the veterinary profession about the prevalence of companion animal infectious diseases, including the identification of potential disease outbreaks and novel pathogens. There are huge potential benefits for small animals and veterinary practitioners alike and I hope that as many practices as possible will choose to become involved in this important initiative.” n
SPOTLIGHT ON SMALL ANIMAL DISEASES
The SAVSNET team (left to right): Prof Rosalind Gaskell, Miss Áine Tierney, Dr Susan Dawson, Dr Alan Radford, Dr Karen Coyne

companion | 19
CPD
CREATE YOUR OWN FILM READING COURSEHow often do you undertake CPD only to find that it isn’t quite what you thought or isn’t as relevant to you as you had hoped? For the first time we are offering you the chance to directly influence the delivery of a film reading course by telling the speakers what you want in advance
We have all looked at the content description of a course and thought that it looked
interesting, but how much better it could be if only it covered another angle or aspect – something you are especially interested in, or find particularly difficult.
In June, BSAVA is offering film reading CPD with a difference. Of course there will be the opportunity to examine X-ray images and try to reach a diagnosis or list of differentials, with plenty of opportunity to discuss the findings with the two lecturers and the other delegates. The innovative aspect is that each delegate is invited to choose their preferred subject area at least one month before the event – meaning you direct the programme.
The speakers, Frances Barr and Fraser McConnell, will guarantee to include at least two cases for interpretation and discussion from each selected area. When you book on the course you can ask which other subject areas have already been nominated – so you can either choose something different, or repeat a nomination to gain extra coverage of this area during the day.
If you book on this course with a group of friends or colleagues, you could end up
Feline dermatologyCutaneous disease of cats may present with a range of cutaneous reaction patterns and be due to a variety of underlying causes. While skin disease may not be as common in cats as in dogs, the popularity of cats as pets will inevitably bring their skin conditions to the attention of clinical practitioners.
This BSAVA course will aim to review skin diseases in cats, with particular reference to those conditions associated with the paws and the face. For each review, consideration will be given to the methods available to establish a diagnosis and the various therapeutic options available for the control and management of skin diseases. Topics covered will include eosinophilic dermatoses, miliary dermatitis, immune-mediated diseases and zoonotic conditions including dermatophytosis and cowpox infection. Case material will be used to illustrate the reviews and delegates will be invited to discuss several cases during the course. ■
Thursday 11 June 2009Speaker: Aiden FosterVenue: Woodrow House, GloucesterMember: £195.75 (including VAT)Non Member: £293.62 (including VAT)
tailoring the course precisely to your collective design – which is ideal for large practices that find the same issues keep coming up. For more information visit www.bsava.com or email [email protected] for booking details. ■
Tuesday 16 June 200910.00–18.00Speakers: Frances Barr & Fraser McConnellVenue: Woodrow House, GloucesterMember: £261.10 (including VAT)Non Member: £391.65 (including VAT)
CREATE YOUR OWN FILM READING COURSEHow often do you undertake CPD only to find that it isn’t quite what you thought or isn’t as relevant to you as you had hoped? For the first time we are offering you the chance to directly influence the delivery of a film reading course by telling the speakers what you want in advance
COURSECOURSEFILM READING

20 | companion
PUBLICATIONS
GUT FEELINGSDavid Williams, Head of the Veterinary Clinical Medicine Department at the University of Illinois, outlines the advances and prospects in small animal gastrointestinal disease
The last two to three decades have seen dramatic advances in the range and sophistication of diagnostic and
therapeutic methods available to veterinary surgeons managing canine and feline patients with gastrointestinal problems. In-house and specialist laboratory testing have evolved to the point that almost all practitioners can evaluate many of their patients thoroughly without utilising sophisticated referral services.
When required, advanced diagnostic imaging and endoscopic services are more accessible than ever before through an increasing numbers of referral centres, and growing numbers of veterinary surgeons with specialist skills are available for consultation.
Technological advancesTechnological advances have led to the development of affordable but reliable methods that allow accurate patient-side diagnosis (Figure 1) within minutes of presentation of cases with clinical signs compatible with, for example, parvovirus enteritis or pancreatitis. Such patients can be managed most appropriately so as to avoid transmission of infection to other patients, or alternatively be given prompt aggressive fluid therapy that may help offset
a potentially less favourable clinical outcome in patients with pancreatitis.
These diagnostic methods can be employed in most veterinary practices, at a modest additional cost to pet owners. These new methodologies have tremendous potential to be widely applied to facilitate rapid, inexpensive and accurate diagnosis of other gastrointestinal diseases.
Ultrasonographic and endoscopic expertise is increasing across the veterinary profession as the cost of equipment falls and accessibility to it increases. These methods are unfortunately inherently dependent on the skills of the operator and are somewhat subjective, and evaluation of some organs such as the pancreas is not always straightforward. Nonetheless, gross lesions can increasingly be identified early in
the disease process, even without referral to specialists.
At the other end of the skill spectrum, imaging specialists are utilizing new methods such as contrast-enhanced ultrasonography, which permits visualization of poorly perfused areas within organs, such as may occur with pancreatic necrosis, neoplasia or metastatic lesions in the liver (Figure 2). Whilst the cost of equipment will restrict availability to specialist centres for the foreseeable future, much faster computed tomography (CT) methods (such as ‘16 slice CT’) are dramatically reducing the time needed for sophisticated studies (and the associated requirement for general anaesthesia), facilitating non-invasive diagnosis of complex and subtle thoracic and abdominal abnormalities.
Figure 1: The SNAP canine pancreatic lipase (cPL) test is a simple in-hospital test that indicates within 10 minutes if the concentration of pancreas-specific lipase in canine serum is normal or increased (reflecting pancreatitis). (Left) No evidence of immunoreactive pancreatic lipase (only the reference spot is visible). (Right) Result from a patient with pancreatitis in which the serum concentration of pancreas-specific lipase is increased, leading to a sample spot noticeably darker blue in colour than the reference spot. Copyright © IDEXX Laboratories, Inc. All rights reserved
pancreatic lipase (cPL) test
that indicates within 10
of pancreas-specific lipase
or increased (reflecting pancreatitis). (Left) No evidence of immunoreactive pancreatic lipase (only the
(Right) Result from a patient with pancreatitis in which the serum concentration of pancreas-specific lipase is
sample spot noticeably darker blue in colour than the reference spot. Copyright © IDEXX
All rights reserved

companion | 21
PUBLICATIONS
ResearchRapid technological advances in molecular biology have revolutionized the investigation of the role of luminal microflora in gastrointestinal disease. It has long been known that many species of intraluminal bacteria cannot be identified by conventional culture in vitro. Now the presence of these species can be documented with extreme precision by characterization of their genetic material.
These methods are being refined to determine quantities of each species present in different parts of the alimentary tract in different gastrointestinal diseases, as are methods for evaluating the response of the host’s immune system to these intraluminal ‘unknowns’. While much still remains to be determined, we are closer than ever before to understanding the complex relationship between the host’s immune system and the antigenic milieu of the gut lumen, and the role of each in the pathophysiology of gastrointestinal disease in dogs and cats.
TherapeuticsMany excellent commercial diets are available and are often effective in improving clinical signs in patients with gastrointestinal disease, even though their evaluation is often through ‘trial and error’ and we may not know the precise basis for their effectiveness. Increasing numbers of prebiotic and probiotic preparations are available, and offer potential alternative or ancillary treatments to traditional therapy with antibiotics,
Figure 2: Contrast ultrasonogram showing a metastatic lesion of haemangiosarcoma in the liver
David Williams is the co-editor of the BSAVA Manual of Canine and Feline Gastroenterology, 2nd edition. Covering such subjects as laboratory diagnosis, biopsy sampling and interpretation, gastritis and hepatic lipidosis, this Manual provides a comprehensive guide to gastrointestinal conditions.
■ Diagnostic approach■ Common presenting complaints■ Standard format within chapters aids information retrieval■ New sections on critical care, assisted feeding and therapeutics
Member price: £49Non-member price: £75
Contact our Membership and Customer Service Team on 01452 726700 or email [email protected] to purchase your copy.
dietary change, glucocorticoids and/or immunosuppressive agents.
The futureThere has been significant progress and many exciting prospects in small animal gastroenterology. Many diseases such as exocrine pancreatic insufficiency, pancreatitis and some infectious enteropathies (such as Giardia and Tritrichomonas foetus infections) can now be diagnosed with excellent accuracy using laboratory methods, although the pathogenicity of some agents such as Campylobacter is still questionable in dogs and cats. Gastroscopy and colonoscopy are both relatively straightforward techniques, and lesions such as gastric lymphoma and adenocarcinoma are usually readily identified and characterized,
as are most neoplastic diseases in the large intestine.
However, definitive identification and classification of enteropathies affecting the small intestine remains challenging. We have many new tools with which to evaluate, classify and monitor pathophysiological changes in both the small intestinal mucosa and gut lumen, but widespread agreement regarding successful translation of these findings to define specific enteropathies remains elusive.
Many clinical trials need to be undertaken to monitor the effectiveness of the various therapies that are now available, but many of the methods required to establish the efficacy of these treatments for different enteropathies are now established. Hopefully these studies will be forthcoming over the next few years and we will be in a position to diagnose and treat our patients with small intestinal disease in an increasingly efficient and cost-effective way. ■
Standard format within chapters aids information retrieval
22 | companion
Improving the health of the nation’s pets
PETSAVERS
WHAT PRODUCTS WOULD HELP PETSAVERS?
Pet carriersPetsavers cardboard or plastic pet carriers are inexpensive and extremely popular with clients.
They are suitable for cats and there is also a mini carrier for small furries. Cardboard or plastic carriers are supplied flat-packed in packs of 10.
The Petsavers wire carriers are great for cats and small dogs. The hinged lid allows full access to the interior of the carrier, making it easy to get pets in and out. They are highly durable and come in a range of colours.
Heated padsPetsavers heated pads are ideal for all small pets to minimise perioperative hypothermia, or just to keep them warm in hospital. They are safe, robust, and easy to clean. Our pads are much cheaper than an incubator and less hassle than hot water bottles. The pads run on a low voltage so they can be left on constantly. A new plug-in lead means that it can be passed easily through the bars of a cage. The pad surface is easily wiped clean and they can be rolled up for storage when not in use.
Protective collarsPetsavers protective collars are available in either opaque or clear plastic. Assembly is easy and they can be attached to regular collars. They come in a range of sizes to fit any cat or dog from a kitten to a St Bernard. ■
Petsavers is keen to expand the range and would like to know what products you would like to see available. The
person who suggests the best idea will receive a reward of a BSAVA manual of their choice. Just send your idea or ideas to Petsavers – email to [email protected] or write to us at: Petsavers, c/o BSAVA, Woodrow House, 1 Telford Way, Waterwells Business Park, Quedgeley, Gloucester GL2 2AB.
We look forward to hearing from you. The entry deadline is 31 May – the winner will be announced in the July edition of companion. We are not necessarily looking for original products not yet in existence – it might be something you already use a lot in practice that you think would generate funds for us – or it might be something you wish you had ready access to but can’t always get hold of easily. To give you some ideas, here are the products already available from your veterinary supplier that help support the work of Petsavers…
Recovery blanketsThese blankets are a must for every practice and are tough as they are made out of metalised polyester, which retains 95% of radiated body heat.
The blankets are ideal for preventing hypothermia in the perianaesthetic period. Additionally, they are radiolucent; hence diagnostic radiographs can be taken whilst the animal remains wrapped in the blanket. They are especially useful for hypothermic or trauma patients.
There is one size: 2.14m x 1.42m, which can be cut to fit smaller animals.
Petsavers has a range of products designed specifically for small animal practice and we receive a royalty on every sale, so when you buy a Petsavers product you are also helping to fund vital veterinary studies. Now we want your ideas for new products to raise more funds

companion | 23
WSAVA NEWS
Dr Jolle Kirpensteijn explains the WSAVA’s support of specialisation
One of the main goals of the WSAVA is the enhancement of global standardisation projects. By
making standards for all veterinarians, knowledge exchange is improved, communication channels simplified, and good companion animals care ensured. The stimulation of Asian Specialisation started as one of the many initiatives of our Past
President Dr Claudio Brovida. In 2006 Claudio hosted the first meeting during the WSAVA Congress in Prague. Since then, many individuals have become progressively enthusiastic about this initiative.
Because of my experiences with the European College of Veterinary Surgeons, (ECVS) and as President Elect of the WSAVA, I was invited to go to Japan to discuss this important issue and the initiative for starting a Japanese College of Veterinary Surgeons. Upon my arrival I was cordially received by Professor Makoto Washizu, our former WSAVA representative. On Saturday I had my first interview with local practitioners including Dr Akio Yasukawa, the current WSAVA representative and executive director of the Japanese Small Animal Veterinary Association, about specialisation, and I showed a condensed version of my lecture. A Japanese journal was present to take notes and publish the conclusions. On Sunday I had a 3-hour lecture about specialisation for an important group of Japanese veterinary dignitaries.
Following the modelsIt seems very logical to stimulate specialization in Japan and Asia. The United States did it in the 50’s, Europe in the 80’s, and Asia seems to be ready to proceed quickly. The European specialisation process had looked a lot like the process that Asia is going through at the moment. In Europe, we had to deal with different languages, educational systems and cultures, making one system more difficult than in the US but certainly not impossible. We started with five colleges and currently we have 23 colleges and 1800 boarded specialists in Europe.
Attendees at the feasibility meeting for a college of Japanese or Asian specialisation. From left: Professor Washizu, Dr Yakusawa, Professor Shigekatsu Motoyoshiun, Professor Jolle Kirpensteijn, Professor Wakao, and Professor Sasaki
GLOBAL SPECIALISATION

24 | companion
GLOBAL SPECIALISATION
WSAVA NEWSWSAVA NEWS
VACCINATIONThe first phase of the WSAVA
Vaccination Guidelines Group (VGG) is now complete and
international guidelines for veterinarians were published in the Journal of Small Animal Practice and are widely available online via the WSAVA website (www.wsava.org/SAC.htm). The guidelines were formally presented at the 2007 Sydney Congress and since that time members of the VGG have spoken widely on them in the USA, UK, elsewhere in Europe and in Australia.
The VGG has now been re-convened for a second phase of activity following agreement of sponsorship from Intervet/Schering-Plough Animal Health. This
sponsorship will permit a further one year cycle of activity with three face-to-face meetings. The first of these meetings was held 1–3 February 2009.
Under the leadership of the new VGG chair, Professor Michael Day, the second phase of the VGG activity will:
Update the 2007 Guidelines ■
Survey WSAVA member associations to ■
collect and analyse feedback on the VGG guidelinesPrepare a new set of guidelines for pet ■
owners and breedersPresent a discussion paper on key issues ■
in teaching of veterinary immunology and vaccinology. ■
The formation of any specialty college should be preceded by the formation of a Board of Veterinary Specialisation (BVS). The BVS has an important role in setting the guidelines for the acceptance of the colleges and streamlines the similarity in training and examinations. After this general summary, I focused on the European College of Veterinary Surgeons discussing the initiation of the College, the advantages and disadvantages of charter members, the pre-qualification, education of residents, examination systems, and re-evaluation of members. To explain residencies, the Dutch system was highlighted. My lecture was followed by another by Professor Sasaki of the Tokyo University. Professor Sasaki explained that the Japanese surgeons were
well ahead in establishing a specialty college of surgery, mirrored on the ECVS and American College of Veterinary Surgeons.
Moving forwardThe next day an important meeting was set up with major surgery professors of the university and delegates from the JAVMA, JAHA and JSAVA about the College for Japanese Surgeons and a possible College for Asian Veterinary Surgeons and a Board of Asian Specialization. The meeting was taped and will be the basis for a large article in one of the best-read Japanese veterinary journals. The short conclusion was that the Japanese surgeons were very open for the formation of an Asian College and that they appreciated
the help of the WSAVA. The formation of the Japanese college could proceed simultaneously with the Asian College, and collaboration with surrounding countries including Australia, Taiwan, Thailand, Korea, and Malaysia would be actively pursued. The next meeting will be planned most likely at the Federation of Asian Small Animal Veterinary Associations 2009 meeting, so if anybody is interested lease let us know.
The WSAVA is proud to be a main force in the promotion of specialisation in this important part of the world and appreciates the efforts that the Japanese associations have made to get things started. Many thanks go out to Dr Brovida, Professor Washizu, Dr Yakusawa, Professor Sasaki, and Professor Wakao. ■

companion | 25
WSAVA NEWS
Dr Claudio Brovida – scholar, Past President and friend of the WSAVA, and most recently, WSAVA Standardization Coordinator, has decided to retire after years of service to the WSAVA in various capacities and offices
It was the unique vision of Dr Claudio Brovida that led to the WSAVA Standardization Projects bringing the
global academic community together to provide standards for the diagnosis and treatment of common small animal ailments that are of clinical relevance for veterinarians around the world.
When Dr Claudio Brovida became President of the WSAVA, he had the dream of achieving at least one important goal during his term of office; as a result of his foresight and perseverance the WSAVA Standardization Projects were born.
Beginning with visionIn February 2000 Claudio met with the then President of the WSAVA, Dr Klaus Dreir, and the Vice President, Dr Gabriel Varga, in Baden for a strategic planning meeting. Claudio had a vision that we could use our connections within the WSAVA to integrate general companion animal medicine and academia, through linking the various research centres throughout the world. This ambitious project would be aimed at clinical problems and the results would be of benefit to the companion animal practitioner while at the same time maintaining the autonomy of the scientists concerned.
In June 2000 Claudio attended an ACVIM meeting and held discussions with
Professor Robert Washabau and Dr Hylton Bark and planted the first seeds towards establishing the WSAVA Standardization Projects. Soon after he met with Professor Jan Roothuizen of the Utrecht veterinary school who was most enthusiastic about this undertaking and suggested a project focused on liver disease. Claudio and Jan exchanged ideas on a study proposal over the next several months.
Funding the first projectsThe WSAVA however was not in a position to finance such a study at that time and sponsorship was needed. So, Claudio held discussions with Dr Hein Meyer of Hill’s Pet Nutrition who was also very enthusiastic about this proposal. In January 2001 Claudio was invited by Hein to the Hill’s headquarters in Topeka to address the directors and within minutes they agreed to be the sponsors of the first WSAVA Standardization Project.
An international committee of world-
renowned specialists was convened and the WSAVA/Hills Liver Standardization Project was initiated. This three-year project culminated in the publication of a book entitled “WSAVA Standards for Clinical and Histological Diagnosis of Canine and Liver Diseases”.
Since then, the WSAVA Gastrointestinal Standardization and Vaccination Projects have been completed (with the generous support of Hill’s Pet Nutrition and Intervet/Schering-Plough Animal Health, respectively). Phase two of the Vaccination Project began in 2009, as well as a four-year Renal Standardization Project in 2008 (through the generous support of Hill’s Pet Nutrition and Bayer Animal Health). Other projects are also in the pipeline.
Our sincere gratitude is extended to Claudio and we extend good wishes for all of his future endeavours!
For more information on the WSAVA Standardization Projects, visit the WSAVA website at www.wsava.org ■
Dr Claudio Brovida doing what he loved most – clinics
STANDARDIZATION COORDINATOR RETIRES

26 | companion
companion INTERVIEW
Duncan Lascelles was born in a small village in central northern Nigeria, but grew up in England, mainly in Devon, with his two brothers and one sister. His parents were secondary school teachers. After graduating from Bristol in 1991 he remained there to complete a PhD in aspects of pre-emptive/perioperative analgesia. He then completed his surgical residency at Cambridge in 1999 before moving to Colorado for the Fellowship in Oncological Surgery at Colorado State University. Duncan undertook research in feline pain and analgesia at the University of Florida, and is currently Assistant Professor in Small Animal Surgery at North Carolina State University with active clinical and research interests in acute and chronic pain
THEcompanionINTERVIEW
You are known for your work on pain control in oncology patients – how did you first become involved in that area?
My passion for understanding and appropriately controlling pain started prior to my veterinary degree. As a kid, I was fascinated by memory. During an intercalated degree in Zoology, I studied memory in relation to behaviour in animals, and then, during the veterinary degree, was introduced to the concept that pain and memory shared similar mechanisms. Dr Alex Livingston was the person who introduced this concept to me, and also furthered my interest in pain. During the clinical years of the veterinary course, I realised that little was known about pain, and at that point decided to undertake a PhD in the subject, working with Drs Waterman-Pearson and Alex Livingston. My interest in oncological surgery came later, during my residency in surgery, where I was mentored and inspired by Dr Dick White.
Where were you working before taking up your current post?
I had been working at the University of Florida with Dr Sheilah Robertson, looking at opioids in cats.
What do you consider to be your most important achievement so far?
My first ‘ceasarean’ while working at Scott
and Partners in Bedford. I got the call, fell back asleep, woke up, spun off the road trying to read the map on the way there, got lost and arrived just in time to see the cow calve on her own, thankfully. OK, seriously. The PhD.
What has been your main interest outside work?
In terms of time commitment, it would be exercise – gym work, running, cycling. However, probably the most fun interests have been dancing (Ceroc) and photography.
What is your least favourite aspect of veterinary work?
Paperwork and records. There is such a wealth of clinical information to be captured, but I’ve only ever worked with desperately inefficient record systems.
Who has been the most inspiring influence on your professional career?
Many people within veterinary medicine have inspired me, but outside of my immediate colleagues and mentors, it would have to be Clifford Woolf. I know lots of people might have never heard of him, but his ideas have helped to change the way pain is managed and understood and he continues to shape innovative thinking in this area.
Which historical/cultural figure do you most admire?
Does Tarzan count? Or Zorro?
What is the most significant lesson you have learned so far in life?
Be humble and honest in everything.
If you were given unlimited political power, what would you do with it?
Improve education and build a society based on sustainable living at all levels. I’d also bring back red phone boxes, doorstep milk delivery and the Dukes of Hazzard on a Saturday night.
If you could change one thing about your appearance or personality, what would it be?
Height. I’d be taller. Not much – just 6 inches or so.
What is your most important possession?
A small silver crucifix.
What would you have done if you hadn’t been a vet?
If I had not been a vet, or gone into a medical field, I would have gone into advertising – something to do with the power of advertising to manipulate the mind. Back to the brain theme, I guess. n

CPD DIARY
companion | 27
CPDDIARY
20 MayWednesday
Imported disease: diseases to watch out for in travelling petsSpeaker Susan ShawRussell Hotel, Maidstone. Kent Region.Details from Hannah Perrin, [email protected]
EVENINGMEEtING
21 MayThursday
Reading abdominal x-raysSpeakers Nic Hayward and Esther BarrettPark Inn Hotel, Llanederyn, Cardiff. South Wales Region.Details from the Chairman or Secretary, [email protected]
EVENINGMEEtING
28 MayThursday
Endocrinology IISpeaker Mike HerrtageThorpe Park Hotel & Spa, Leeds. Organised by BSAVA.Details from the Membership and Customer Service Team, 01452 726700, [email protected]
DAYMEEtING
4 JuneThursday
Interactive neurological examinationSpeaker Mike TargettExeter University, Streatham Campus. South West Region.Details from Lennon Foo, [email protected]
EVENINGMEEtING
18 MayMonday
BSAVA Cardiology RoadshowSpeakers Rebecca Stepien and Virginia Luis Fuentes.Day meeting at Canalside, Bridgwater, South West Region. Organised by BSAVA.Details from the Membership and Customer Service Team, 01452 726700, [email protected]
TBC May
Neurology: spinal disease in dogs and catsSpeaker to be confirmedLeatherhead Golf Club, Surrey. Surrey and Sussex Region.Details from Jo Arthur, 01243 841111, [email protected], or Jackie Casey, 01483 797707, [email protected]
EVENINGMEEtING
TBC June
Rabbit anaesthesia and surgerySpeaker to be confirmedHoliday Inn, Gatwick. Surrey and Sussex Region.Details from Jo Arthur, 01243 841111, [email protected], or Jackie Casey, 01483 797707, [email protected]
DAYMEEtING
13 MayWednesday
Ocular manifestations of systemic diseaseSpeaker David WilliamsPotters Heron Hotel, Romsey. Southern Region.Details from Michelle Stead, 01722 321185, [email protected]
EVENINGMEEtING
17 MaySunday
Is it respiratory or cardiac disease? A case-based approachSpeaker Clive ElwoodCambridge Belfry, Cambourne. East Anglia Region.Details from Graham Bilbrough, [email protected]
DAYMEEtING
19 MayTuesday
Endocrinology ISpeaker Ian RamseyBSAVA, Woodrow House, Quedgeley. Organised by BSAVA.Details from the Membership and Customer Service Team, 01452 726700, [email protected]
DAYMEEtING
4 JuneThursday
Ferrets and RodentsSpeaker Emma KeebleMottram Hall, Cheshire. Organised by BSAVA.Details from the Membership and Customer Service Team, 01452 726700, [email protected]
DAYMEEtING
8–10 MayFriday–Sunday
24th Annual Scottish Congress‘Raising the bar’ in SA practice, for veterinary surgeons & nursesSpeakers Andrew Mackin and Ronan DoyleFairmont Hotel, St Andrews. Scottish RegionDetails from Susan Macaldowie, 07711 633698, [email protected]
WEEKEND
20 MayWednesday
BSAVA Cardiology RoadshowSpeakers Rebecca Stepien and Mike MartinDay meeting at the Daventry Hotel, Beaconsfield. Midland Region. Organised by BSAVA.Details from the Membership and Customer Service Team, 01452 726700, [email protected]
22 MayFriday
BSAVA Cardiology RoadshowSpeakers Rebecca Stepien and Virginia Luis FuentesDay meeting at the Bellhouse, Beaconsfield. Metropolitan Region. Organised by BSAVA.Details from the Membership and Customer Service Team, 01452 726700, [email protected]
14 MayThursday
BSAVA Cardiology RoadshowSpeakers Rebecca Stepien and Mike MartinDay meeting at the Radisson SAS Hotel, Belfast, Northern Irish Region. Organised by BSAVA.Details from the Membership and Customer Service Team, 01452 726700, [email protected]
For further details of CPD courses in your area, please visit www.bsava.com
Knowledge of anatomy and function of the skin and the physiology of normal wound healing provides a background to the successful management of wounds. This course will enable you to develop a logical and practical approach to the management of the patient and wound.
Wound Management Wound Management Wound Management andandandReconstructive SurgeryReconstructive SurgeryReconstructive Surgery
Thursday 18 June 200910.00–18.00Speaker: Stephen BainesVenue: Mottram Hall, CheshireMember: £195.74 (including VAT)Non Member: £293.62 (including VAT)
Visit www.bsava.comEmail [email protected] 01452 726700
Also available from BSAVA
NEW