Communityyp gy ophthalmology · Communityyp gy ophthalmology ตตวอยางัวอย...
134
Community ophthalmology P bli H lth O hth l l Public Health Ophthalmology P ti f Bli d Prevention of Blindness Pi Primary eye care Community eye care
Transcript of Communityyp gy ophthalmology · Communityyp gy ophthalmology ตตวอยางัวอย...

Community ophthalmology y p gy
P bli H lth O hth l lPublic Health Ophthalmology
P ti f Bli dPrevention of Blindness
P i Primary eye care
Community eye care

Community ophthalmology y p gy
5 questions of blindness
1. What is blindness? DEFINITION
2. How many are blind? MAGNITUDE
3. Why are people blind? ETIOLOGY
4. Why the number increase? TRENDS
5 What can we do ? CONTROL 5. What can we do ? CONTROL

Community ophthalmology y p gy
WHO. Classification of visual impairment
Snellen Visual Acuity
Normal 6/6 to 6/18
Visual impairment < 6/18 to 6/60
Severe Visual impairment < 6/60 to 3/60
Blind < 3/60 to N L PBlind < 3/60 to N.L.P.

Community ophthalmology y p gy
พรบ. ฟนฟสมรรถภาพคนพการลกษณะความพการ ระดบท สายตา ลานสายตา
( ) ๖/ ๘ ๖/๖ สายตาเลอนลาง (VA) ๑ ๖/๑๘ ถง ๖/๖๐ < ๓๐ ถง ๑๐ องศา
สายตาพการ (VF) ๒ < ๖/๖๐ ถง ๓/๖๐( )
ตาบอดขนท๑ ๓ < ๓/๖๐ ถง ๑/๖๐ < ๑๐ ถง ๕ องศา
ตาบอดขนท๒ ๔ < ๑/๖๐ ถง PL < ๕ องศา
ตาบอดขนท๓ ๕ N L Pตาบอดขนท๓ ๕ N.L.P.

Community ophthalmology y p gy
ตวอยาง ตวอยาง
๑) ผปวย ตอกระจกทง๒ขาง สายตามองเหนแคนบนว ทง๒ขาง)
๒) ผปวยตอหนทง๒ขาง มองเหนเฉพาะตรงกลาง VA 20/20 ทง๒
ขาง
ป ไ ๓) ผปวยอบตเหตรถยนต หลงผาตดแลว ตาขวามองไมเหน ตา
ซายปกต
๔) เดกตาขนมวมาตงแตเกด มองไมเหนตวหนงสอเลย

Community ophthalmology y p gy
Prevention of BlindnessPrevention of Blindness
situation 50 m Blind in 2000 worldwide
1-2% in the third world
0.31% in Thailand
estimation 180,000

Community ophthalmology y p gy
Magnitude of Global Blindness
60
70
40
50
20
30 million
0
10
1975 1984 1990 1995 2000 2020

Community ophthalmology y p gy
Distribution of total global blindnessg
America&Europe
rest of Asia
India
China
AfricaAfrica

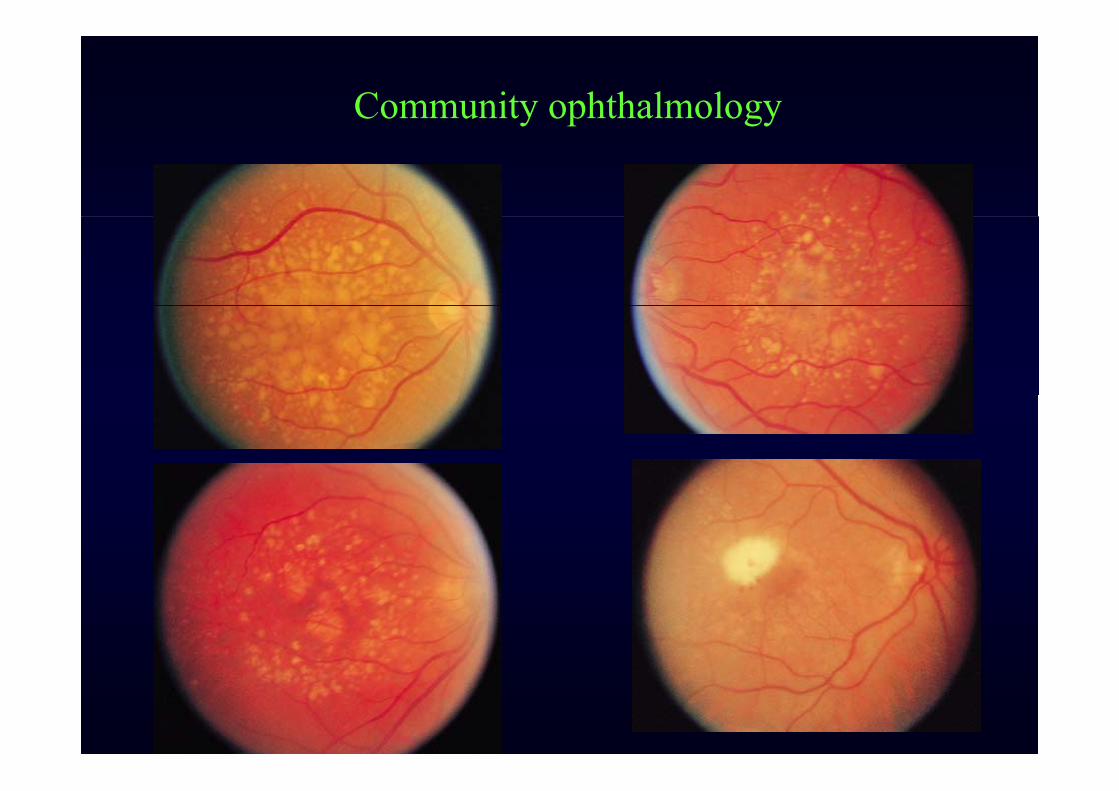
Community ophthalmology y p gyWorldwide blindness
d good poorBlindness rate 0.1 - 0.4 % 0.5 -1.5 %Major causes AMD. Cataract
Glaucoma GlaucomaGlaucoma GlaucomaDR. Trachoma/scar
C it l di O h i iCongenital disease OnchocerciasisHereditary disease Vit. A deficiency
Location Posterior segment Anterior segment% Avoidable 20% 80%% Avoidable 20% 80%Etiology poorly understand usually well known

Community ophthalmology y p gy
Cause of Blindness
developing country preventable/undertreatment
partial developed (0.4-0.65%)
developed complicated/untreatable

Community ophthalmology y p gyCause of worldwide blindness, year 2000
disease blind (million) % trend disease blind (million) % trend# Cataract 25 50 # Glaucoma 8 16# Glaucoma 8 16# DR. 3 6# AMD. 2 4# Corneal scar/Trachoma ? 5 10
Vit. A deficiency ? 0.5 1Onchocerciasis ? 0.5 1Leprosy ? 0.5 1 Refractive error 2 4 Refractive error 2 4 Childhood blindness 1 2Trauma 1 2Trauma 1 2Other 1.5 3

Community ophthalmology y p gy
Cause of Blindness in Thailand (1994)( )
Cataract 74.65% Corneal opacity 4.93%
Glaucoma 3.52% Globe disorder 3.52%
Macular degeneration 2.82%
Vascular retinopathy 2.11%
Community ophthalmology y p gy
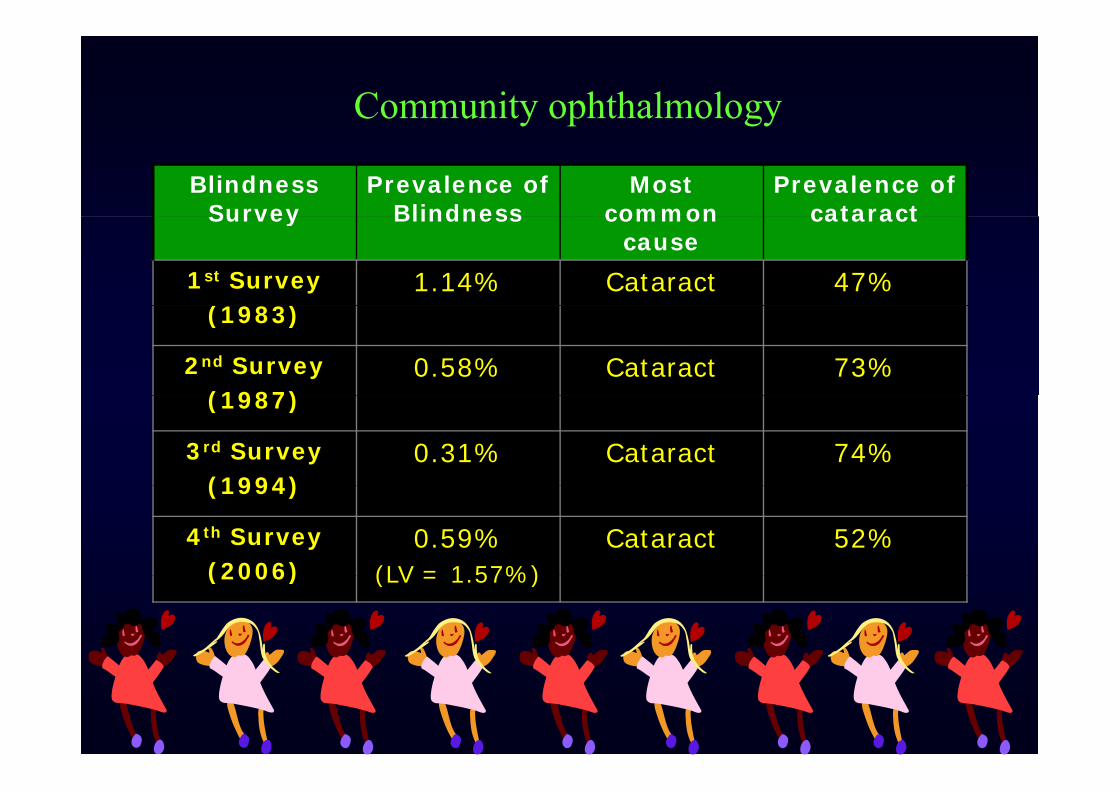
Blindness Survey
Prevalence of Blindness
Most common
Prevalence of cataractSurvey Blindness common
causecataract
1st Survey(1983)
1.14% Cataract 47%(1983)
2nd Survey(1987)
0.58% Cataract 73%(1987)
3rd Survey(1994)
0.31% Cataract 74%(1994)
4th Survey(2006)
0.59%(LV = 1 57%)
Cataract 52%(2006) (LV = 1.57%)

Community ophthalmology y p gy
Visual impairment
Weighted Prevalence
Estimated total Visual impairment
(%) numbers
Low Vision one eye 2 18% 1 369 362Low Vision one eye 2.18% 1,369,362
Low Vision both eyes 1.57% 987,993
Blindness one eye 1 59% 996 040Blindness one eye 1.59% 996,040
Blindness both eyes 0.59% 369,013
Bli d l i i Blindness one eye, low vision one eye 0.39% 242,562
Total 6.32% 3,964,9706.32% 3,964,970

Community ophthalmology y p gy
Cause of Visual Impairment (Blind both Eye)
Di b ti ti thDiabetic retinopathy 2%
Optic atrophy 4%
Age-related macular degeneration
Cataract 52%
degeneration 7%
Glaucoma Refractive errors, Glaucoma 10% uncorrected aphakia
2%

Community ophthalmology y p gy
Cause of Visual Impairment (Low vision both eyes)p ( y )
Significant pterygium 3%
Diabetic retinopathy 5%
Age-related macular degeneration
4%
3%
4%
Glaucoma 10%
Cataract 57%
Refractive errors, uncorrected aphakia
14%

Community ophthalmology y p gyIncreasing number of blindness
increase in population
increase in life expectancyp yinadequate eye care service
age year2000 future % increase0-4 years 900 900 00 4 years 900 900 05-19 years 1300 1300 020-64 years 3400 5000 50>64 years 400 800 100ytotal 6000 8000 33

Community ophthalmology y p gy
4450
30
40/1
000
1920
prev
alen
ce/
0.8 110
p
0
0-14 15-44 45-59 60+

Community ophthalmology y p gy
Primary preventionIncidence 6 million /years
Secondary preventionPrevalence
Secondary prevention
50 million
blind
Sight restoration MortalitySight restoration
1 million / year
Mortality
4 million / yearIncrease of1 million/year

Community ophthalmology Healthy y p gy
Birth controlHealth
Di
Healthy
general populationBirth control
promotionDisease
Prevention
Chronic illness
Impairment
Increase life expectancy
Medical care deathIncrease quality of life
More education
HandicapRehabilitation
More wants
More etc. HandicapRehabilitation

Community ophthalmology y p gy
Primary prevention
Promotion of Community Immune
Environmental Health
Health Management
Community ophthalmology y p gy
Secondary preventionSecondary prevention
screening criteriascreening criteria
morbidity/mortality prevalence natural Hxy y p
effective Rx benefit of early Rx appropriate test

Community ophthalmology y p gyStrategy approach to control of blindness
primary prevention prevent from occuringp y p p gVitamin A deficiency good nutritionTrachoma good water & sanitationTrachoma good water & sanitationRubella & Measles immunization
secondary prevention prevent loss of vision from diseasesecondary prevention prevent loss of vision from diseaseCataract surgery when vision is decreaseGlaucoma sight prevention; surgical/medicalDiabetic retinopathy sight preserving LASER treatment
tertiary prevention restore vision to a blind personCataract sight restoration in bilateral blinding cataractCorneal scar keratoplastyLow vision service visual rehabilitation

Community ophthalmology y p gy
4 groups of blindness community control programsg p y p g 1. Priority&majority highly cost- effective intervention
Cataract & significant refractive error (50-67%)Cataract & significant refractive error (50 67%)2. Focal blinding disease cost-effective, prevention&treatment
Trachoma, Vitamin A deficiency etc (10-15%) Trachoma, Vitamin A deficiency etc (10 15%) Primary health care & community eye worker training
3. Complicated disease effective early treatment (by specialist)3. Complicated disease effective early treatment (by specialist)Glaucoma, Diabetic retinopathy etc (20%)community screening program & referral systemcommunity screening program & referral system
4. Blinding disease no effective prevention&treatmentaged related macular degeneration, retinitis pigmentosaaged e ated acu a dege e at o , et t s p g e tosa
congenital ocular abnormalities

Community ophthalmology y p gy
Blinding eye diseases
CATARACT TRACHOMA
GLAUCOMA
DIABETIC RETINOPATHY
ONCOCERCIASIS
VITAMIN A DEFICIENCYDIABETIC RETINOPATHY VITAMIN A DEFICIENCY
Occur everywhereaffect individual
Focal diseaseaffect communityaffect individual
affect mainly adultrequires surgery
affect communitystart in children
requires medicinerequires surgeryneed an eye doctor
equ es ed c edoes not requires an eye doctor
HOSPITAL BASE COMMUNITY BASE

Community ophthalmology Primary eye care in the communityScreening
Simple Medication y p gy
P i h it l Health voluntierScreening
Simple Medication
Primary care hospital
Midlevel health personel
Health voluntierScreening
Simple Medication
& treatment
Case refer Academic support
Midl l h lth Seconary care hospital
OphthalmologistSimple Surgery
Research
Midlevel health
personelOphthalmologist
Case refer Academic support
Research
Tertiary care hospital
pp
Complicated Surgery
ResearchSubspecialty Ophthamologist Resident Research
Policy setting

Community ophthalmology Comprehensive Eye Carey p gyComprehensive Eye Care
Provincial Hospital Planning &Provincial Hospital Eye Unit
Planning &
Management Curative Services
Community Hospital
P i C U iPrimary Care Unit
Community Prevention & Promotion
Dec 08 Phnom Penh 17
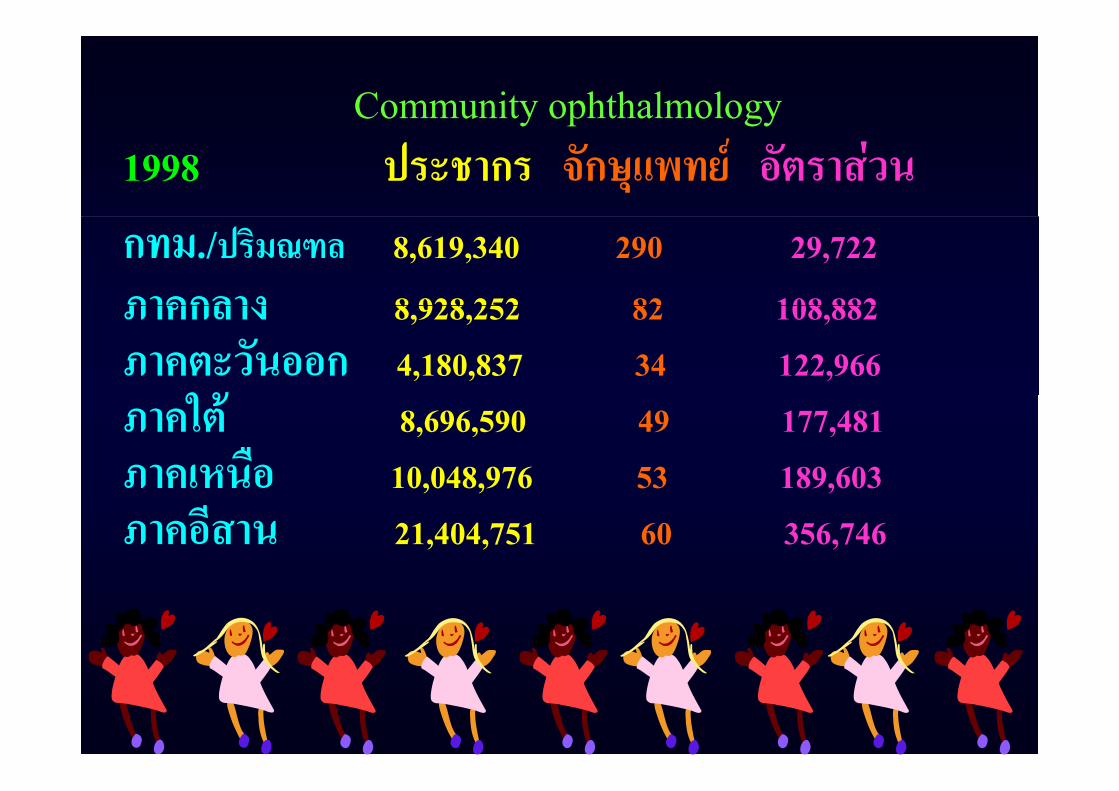
Community ophthalmology y p gy1998 ประชากร จกษแพทย อตราสวน
กทม./ปรมณฑล 8,619,340 290 29,722
ภาคกลาง 8 928 252 82 108 882ภาคกลาง 8,928,252 82 108,882
ภาคตะวนออก 4,180,837 34 122,966
ใ ภาคใต 8,696,590 49 177,481
ภาคเหนอ 10,048,976 53 189,603ภาคเหนอ 10,048,976 53 189,603
ภาคอสาน 21,404,751 60 356,746

Community ophthalmology Distribution of ophthamologist in Thailandy p gySurvey in 2007 63m population 803 ophthalmologist
area ophthalmologist ratio
gov pri total
Bangkok 244 129 373 1:15171
Central 93 18 111 1:101691
Eastern 42 9 51 1:73230Eastern 42 9 51 1:73230
Southern 66 12 78 1:98124
Northern 70 9 79 1:136781
Northeastern 91 10 101 1:211169
Total 606 187 793 1:78711

Community ophthalmology y p gyBlind person years, four major condition
diti ti t d N d ti bli d condition estimated No ave. duration blind person yearscataract 25 x 5 = 125 1glaucoma 8 x 8 = 64 3DR 3 x 5 = 15 4child blindness 1.5 x 50 = 75 2
20
25
100
120
140
5
10
15
40
60
80
0
5
cataract glaucoma DR child blindness0
20
cataract glaucoma DR child blindness

Community ophthalmology y p gy6 step of problem solving paradigm
1. Define the problem
2 Measure the magnitude2. Measure the magnitude
3. Define the key determinationy
4. Decision of intervention
5. Set policy
6. Implement/evaluation

Community ophthalmology y p gyKey determination
Biological factor
genetic, age, microbiology, diseasegenetic, age, microbiology, disease
Social/culture/behavior
knowledge, fear, life style
Environment/occupationEnvironment/occupation
geographic, manpower, barrier

Community ophthalmology y p gyHealth system evaluation
Equity/Equality
Quality Quality
Efficiency
Social acceptance
Relevant

Important things are not visible to the eye.p g y
By a Fox (in “Little Prince”)
All the lonely people, y p p ,where do they come from?
All the lonely people, where do they belong?where do they belong?
“Eleanor Rigby”
( I can ) change the world( I can ) change the world.
E. Clapton

Community ophthalmology y p gyproblem solving paradigm for blinding cataract
1. Define the problem What is blinding cataract?
2. Measure the magnitude How many blinding catract 2. Measure the magnitude How many blinding catract are there in Thailand?
3. Define the key determination What is the risk?
4. Decision of intervention What will we do?
5. Set policy How will we support it?
6. Implement/evaluation How does it work?

Community ophthalmology y p gyBlinding cataract
DefinitionDefinition
Blinding 10/200 g
Cataract lens opacity must R/O other cause of blindness
Magnitude
prevalence (backlock)
incidenceincidence
Community ophthalmology y p gyKey determination for cataract
Biological factor
age, disease(DM), trauma, congenitalage, disease(DM), trauma, congenital
Social/culture/behavior
knowledge, attitude, life style, socioeconomic
Environment/occupationEnvironment/occupation
geographic, manpower, barrier, health system

Community ophthalmology y p gyCataract Decision of intervention
Screening of casesScreening of cases
community base/hospital base
health voluntier/health personel
R f l Referal system
routine/fast tract
Operation
satelite hospital/provincial hospital
routine/campaignroutine/campaign
ECCE/PE with IOL

Community ophthalmology y p gyCataract Decision of intervention
Education Education
mass media
patient
i i ltraining personel
Follow up
Ophthalmologist requirement ?

Community ophthalmology y p gyStrategies for finding the cataract blind
1. Wait for patients
Surgical camp2. Surgical camp in community
Screening clinic3. Screening clinic in community
4 S d i l t llit h it l Satellite hospital
4. Secondary surgical satellite hospital
Community based referral
5. CBR case detection in community

Community ophthalmology y p gyCataract policy setting
Target settingTarget settingwaiting timeblinding cataract operation rateblinding cataract operation rate
Supportdoctor fee per case private/governmentequipmentIOLmanpower Ophthalmologist, nurse, personel, etc.p p g , , p ,complication managementspecial supporting group ?special supporting group ?

Community ophthalmology y p gy
Cataract program implement & evaluationRegistration/report
waiting timeblinding cataract operation rateregister of blindnessg
Quality assurancegood health care systemgood health care systemaudit
O h ffOther effectother health care systempersonel

Community ophthalmology y p gy
Ophthalmic screening (general)p g (g )
asymtomatic early/late damageasymtomatic early/late damage
central/peripheral visioncentral/peripheral vision
monocular/binocularmonocular/binocular
l o w / h i g h r i s k a g el o w / h i g h r i s k a g e
Community ophthalmology y p gy
Ophthalmic screening (special purpose)p g ( p p p )
student human rightstudent human right
driver/pilot safetydriver/pilot safety
worker efficiencyworker efficiency
etcetc.

Community ophthalmology y p gy
Normal visual developmentintermittent fixation at birth
nearby face fixation 2-3 month
smooth follow near movement 3 month
full accomodation 3-4 month
onset of stereopsis 3-5 month
well distant fixation 6 month
subjective VA test 3 year
adult-type VA test 5-6 year

Community ophthalmology y p gy
VA for 6 month children
C enteringg
S teadyS teady
M aintainM aintain
Community ophthalmology y p gy

Community ophthalmology y p gy
Community ophthalmology y p gy
High risk children High risk adultg g
prematurity RD, severe ocular trauma prematurity RD, severe ocular trauma
family Hx family Hxfamily Hx family Hx
intrauterine infection one eye, age > 65intrauterine infection one eye, age > 65
systemic disease systemic diseasesystemic disease systemic disease

Community ophthalmology y p gy
มค ๒๕๔๗ มการตดเชอตาแดงในneonatal
ward ทานจะทาอยางไร

Community ophthalmology y p gy
๒๕๓๓ หยอด formalin ลงในตาเดกแรกเกด
๒๕๔๘ หยอด silver nitrate แลวมsevere ๒๕๔๘ หยอด silver nitrate แลวมsevere
reaction & corneal scar
How do we do to solve this problem?p

Community ophthalmology y p gy
Ophthalmia Neonatorum
cause GC / Chlamydia /Chemical / Herpes simplex
prophylacis 1% Silver nitrate (solution)
1% Tetracyclin / 0.5% Erythromycin (ointment)
Providone iodine (solution)Providone iodine (solution)
ceftriaxone 125mg Erythromycin base 50mg/kg/day x14 day

Community ophthalmology y p gy
Community ophthalmology y p gy
Amblyopiay p
refractive error / strabismus /other refractive error / strabismus /other
1-4 % in population occlusion therapy
preschool age 4-6 year
visual screening VA / stereopsis

Community ophthalmology y p gy

Community ophthalmology y p gy
Amblyopic treatment

Community ophthalmology y p gy
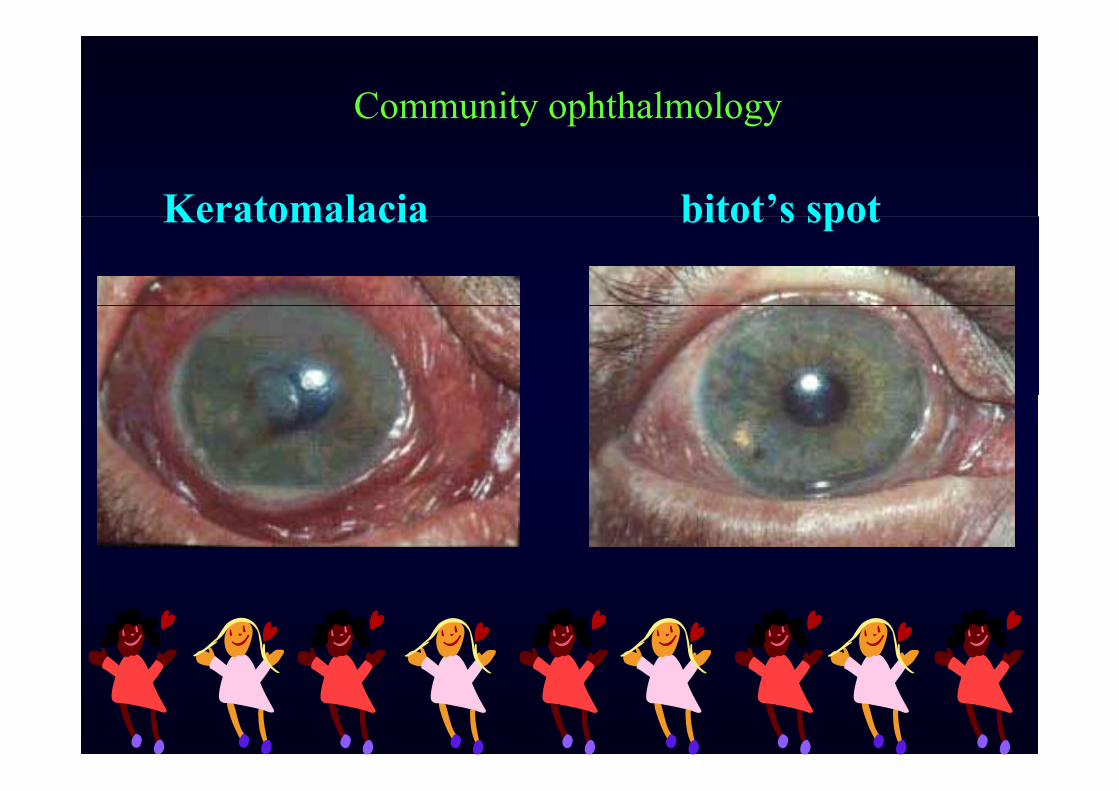
Xerophthalmia
Vitamin A deficiency
dry eye /corneal perforation Measle
nutrition breast feeding immunization
vitamin A supplement ? regular/ periodic
Community ophthalmology y p gy
Keratomalacia bitot’s spotKeratomalacia bitot s spot

Community ophthalmology y p gy
Trachoma
chlamydial infection
poor environment/water supply
superimpose bacterial infection flies
i i i i / i / lid ulcer trichiasis / entropian corneal ulcer/ scar

Community ophthalmology y p gy
Trachoma
Rx ineffective, long course, complication, cost
topical tetracyclin / erythromycin bid x 5d/m x 6 month
aim severity population control
surgical correction of entropian

Community ophthalmology y p gy

Community ophthalmology y p gy
Retinopathy of Prematurityp y y
prematurity / oxygen therapy
vasoconstriction neovascularization traction RD
retrolental fibroplasia
high risk grouphigh risk group
BW < 1500 gm GA < 32 week oxygen Rx > 4 hour
Community ophthalmology y p gy
Retinopathy of Prematurity
dilated fundus examination as soon as possible
Threshold ROP stage 3 plus >3 hour cont. / 8 hour sum.
Cryotherapy / laser treatment retinal surgery
follow up look for high myopic astigmatism glaucomafollow up look for high myopic astigmatism, glaucoma
amblyopic treatmentamblyopic treatment

Community ophthalmology y p gy
ROP
1 2
3 4 3 4

Community ophthalmology y p gy
ROP

Community ophthalmology y p gy
Glaucoma ocular hypertension
increase IOP normal tension glaucoma
optic nerve damage physiologic large cupping
visual field defect
POAG PACG SOAG SACG

Community ophthalmology y p gy
GlaucomaGlaucoma
Screening testScreening test
IOP Schiotz / applanation tonometry
optic nerve cupping non - stereopsis / stereopsis
visual field confrontation / Goldman perimetry / CTVF
Community ophthalmology y p gy
Glaucoma
High risk group
> 40 year old DM, thyroid
HT IHD hi h iHT, IHD high myopia
family history of POAG y s o y o O G
angle recess glaucoma steroid induced glaucoma

Community ophthalmology y p gy
normal

Community ophthalmology y p gy

Community ophthalmology y p gy

Community ophthalmology y p gy

Community ophthalmology y p gy
Goldman ‘s perimetry

Community ophthalmology y p gy
CTVF

Community ophthalmology y p gy
Retinal vascular diseaseRetinal vascular disease
Diabetic retinopathy Diabetic retinopathy
DM type1 5year after Dx
DM type2 at time of Dx
annually dilated fundus examination till Dx of DR

Community ophthalmology y p gy
Diabetic retinopathy
lif ti / lif tinon - proliferative / proliferative
clinical significant macular edema ( CSME ) ?clinical significant macular edema ( CSME ) ?
LASER Rx PMP PRP vitrectomyy

Community ophthalmology y p gy

Community ophthalmology y p gy
CSMECSME

Community ophthalmology y p gy
Aged macular degenerationAged macular degeneration
central scotoma blur vision metamorphopsiacentral scotoma blur vision metamorphopsia
non - exudative / exudative
screening test Amsler’s grid nutritional support?
LASER Rx stop smoking

Community ophthalmology y p gy
Community ophthalmology y p gy
Community ophthalmology y p gy
Ocular trauma
workplace recreation/sport home transportation
protective device environment law individual
screening test

Community ophthalmology y p gy

Community ophthalmology y p gy
Disorder change in anatomy/physiology of an organ systemorgan system
Impairment functional change in organ system
Disability skill / ability of the individual
Handicap the societal/economic consequence of a disabilitydisability

Community ophthalmology y p gy
• the organ the person
disorder impairment disability handicapanatomical change functional change skill /ability social /economico c c ge u c o c ge s / b y soc /eco o c
inflammation visual acuity reading extraeffort
atrophy visaul field daily living dependence
scar color vision mobility

Community ophthalmology y p gy
Disorder Impairment Disability Handicap
Medical/surgicalintervention
Visual aidsadapted equipment
Social interventiontrainingintervention adapted equipment training
counselingeducationeducation

Community ophthalmology y p gy
Visual rehabilitation
medical visual aid orientation/mobility trainingy g
educational blind/low vision special schoolp
social behavior, recreation, sex etc , ,
occupational p

Community ophthalmology y p gy
Visual field orientation / mobilityVisual field orientation / mobility
51-70 degree normal 31-50 degree normal, use more scanning 11-30 degree near-normal, constant scanning 11 30 degree near normal, constant scanning
6 -10 degree slower, require scanning & cane3 - 5 degree use cane for detection ,vision for
identification less unreliable, use blind mobility skill NLP no visual orientation NLP no visual orientation

Community ophthalmology y p gymobility training
t li i i 3/200 ith 50 d VFtraveling vision 3/200 with > 50 degree VF< 20 degree VF orientation problem < 20 degree VF orientation problem
1) sight guide2) long cane3) dog guide4) electronic mobility device4) electronic mobility device

Community ophthalmology y p gyการนาทางคนตาบอด
๑) ผนาทาง หบแขนขางลาตว งอขอศอกเลกนอย๒) ผตาม ใชมอจบทเหนอขอศอก หางผนา๑/๒กาว๒) ผตาม ใชมอจบทเหนอขอศอก หางผนา๑/๒กาว๓) ผนาทาง เดนพอใหผตาม สามารถเดนตามทนได ๔) ผนาทาง ขยบขอศอกไปดานหลง เพอเปนสญญาณวา ทางแคบลง มปร ต วา ทางแคบลง มประต
๕) ผนาทาง คอยบอกวามสงสงเกตทสาคญ อยทใด๕) ผนาทาง คอยบอกวามสงสงเกตทสาคญ อยทใด๖) เมอจะปลอยใหผตามอยตามลาพง ควรไวทตดเกาอหรอ กาแพง
Community ophthalmology y p gy
Cane
long cane foot to 1 1/2 inch above sternum bottomcontact feed back scanningno forewarning of overhead obstaclesno forewarning of overhead obstacleswhite cane sign of visual impairmentg p

Community ophthalmology y p gy
dog guide
extensive training maturity & intelligence 18 60 d h lth d h i d age 18 -60, good health, good hearing and no
residual visionGerman shepherd, Golden/Labrador retriever and Boxer
F l d f d Female dogs are preferred.
Community ophthalmology y p gy
Low vision care
1) diagnosis2) di l & i l t t t2) medical & surgical treatment3) analysis of visual function3) ys s o v su u c o4) problem discussion 5) low vision examination6) h i l 6) psychosocial assessment7) provision of a range of equipment7) provision of a range of equipment

Community ophthalmology y p gylow vision care
8) d ti & i t ti f ti l d i8) recommendation & instruction of optical device9) prescription9) prescription10) dispensing11) patient education12) vision & other rehabilitation service13) access to available funding sources13) access to available funding sources14) continuing eye care15) training & continuous education

Community ophthalmology y p gy
Range of VA reading ability general ability
20/12 - 20/25 normal normal c reserve
20/30 - 20/60 shorter distance normal s reserve
20/80 - 20/160 near - normal near normal require aids 20/80 - 20/160 near - normal near normal require aids
20/200 -20/400 slower than normal slower than normal
20/500 -20/1000 limited reading some task c aids
20/1250 20/2500 li bl f k b i20/1250 -20/2500 unreliable few task, use substitute
NLP not possible no task p

Community ophthalmology y p gy
adaptive low vision device
1) relative size device) i /i i i 2) light/illumination control
3) posture/positioning device3) posture/positioning device4) writing /communication device5) medical assistive device6) mobility assistive device7) sensory substitution device7) sensory substitution device

Community ophthalmology y p gysensory substitution device
A dit b tit tAuditory substitutetalking book/device, computer program etc.talking book/device, computer program etc.
Tactile substituteBraille, Nonbraille
Vision substituteneural prosthesisneural prosthesis

Community ophthalmology y p gyBraille
6 raised dot 3 high / 2 wide6 raised dot 3 high / 2 widegrade 1 letterggrade 2 contraction/abbreviated word grade 3 personal note taking
b tt l i i hildbetter learning in children100 word/ min but talking book 175 word/min100 word/ min but talking book 175 word/min

Community ophthalmology y p gy
Optical aids
Hand-held magnifiers Stand magnifiersIll i t d ifi R di lIlluminated magnifiers Reading glassesLoupes and visors Reading telescopes oupes d v so s e d g e escopes Telescopes Video magnifiersPrisms Reverse telescopes

Community ophthalmology y p gy
Hand - held magnifiers
inexpensive / familiar / easy to use
normal working distance
i imust be held steadily at an exact distance
limited viewing field make slow readinglimited viewing field make slow reading

Community ophthalmology y p gy

Community ophthalmology y p gy
Stand magnifiers
stand hold the lens steadily at fixed / proper distance
i i i fuse with reading glasses to obtain best focusotherwise same as Hand - held magnifiers otherwise same as Hand held magnifiers

Community ophthalmology y p gy
Illuminated magnifiers
build in lighti S ifieither Hand - held or Stand magnifiers
AC / batteries / rechargeable batteriesAC / batteries / rechargeable batteriesincandescent, halogen, or fluorescent

Community ophthalmology y p gy
Reading glasses
leave the hands free i fi f iwidest field of view
very close working distancevery close working distancetraining program

Community ophthalmology y p gy
Loupes & Visors
small field of viewsmall field of viewheadgear cumbersome gusually inexpensive can be flipped in or flipped out

Community ophthalmology y p gy
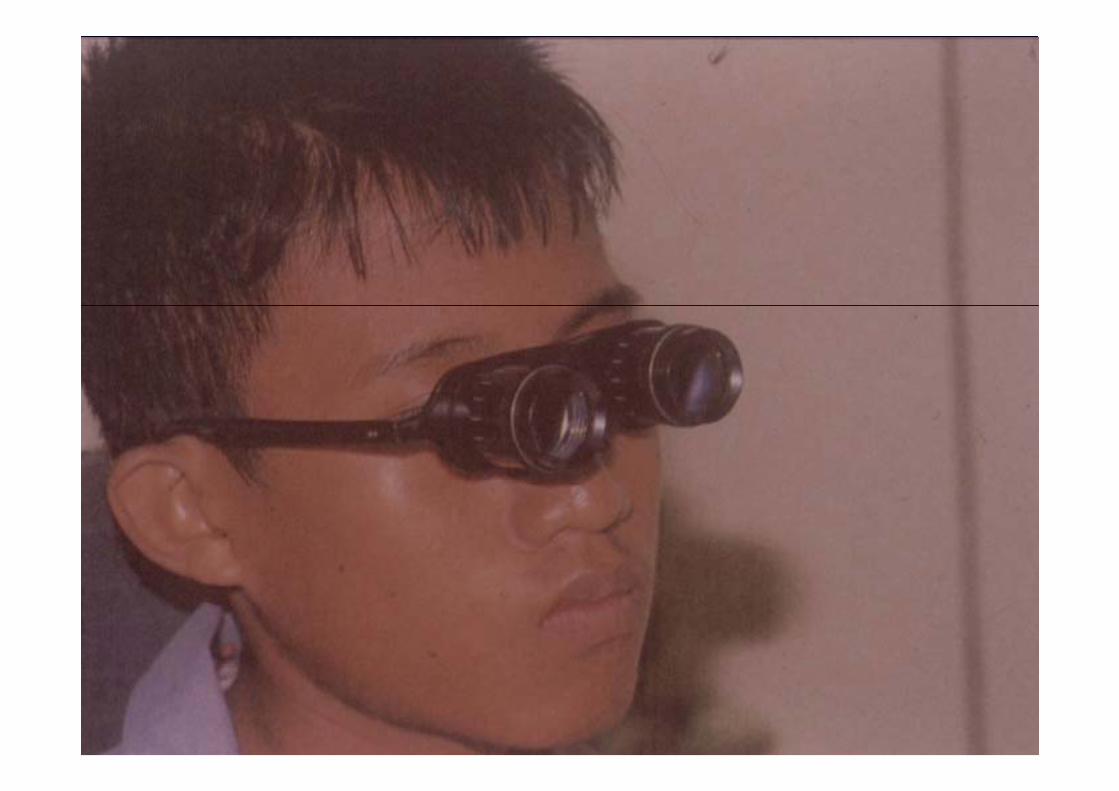
Reading telescopedifficult to use high magnification but constrict field /shallow depth of fieldhigh magnification but constrict field /shallow depth of field
arm’s length working distance mounted in lower part of a pair of glasses bioptic telescope mounted in middle part of a pair of glasses easier to usemultifocal turning end / reading capmultifocal turning end / reading cap

Community ophthalmology y p gy
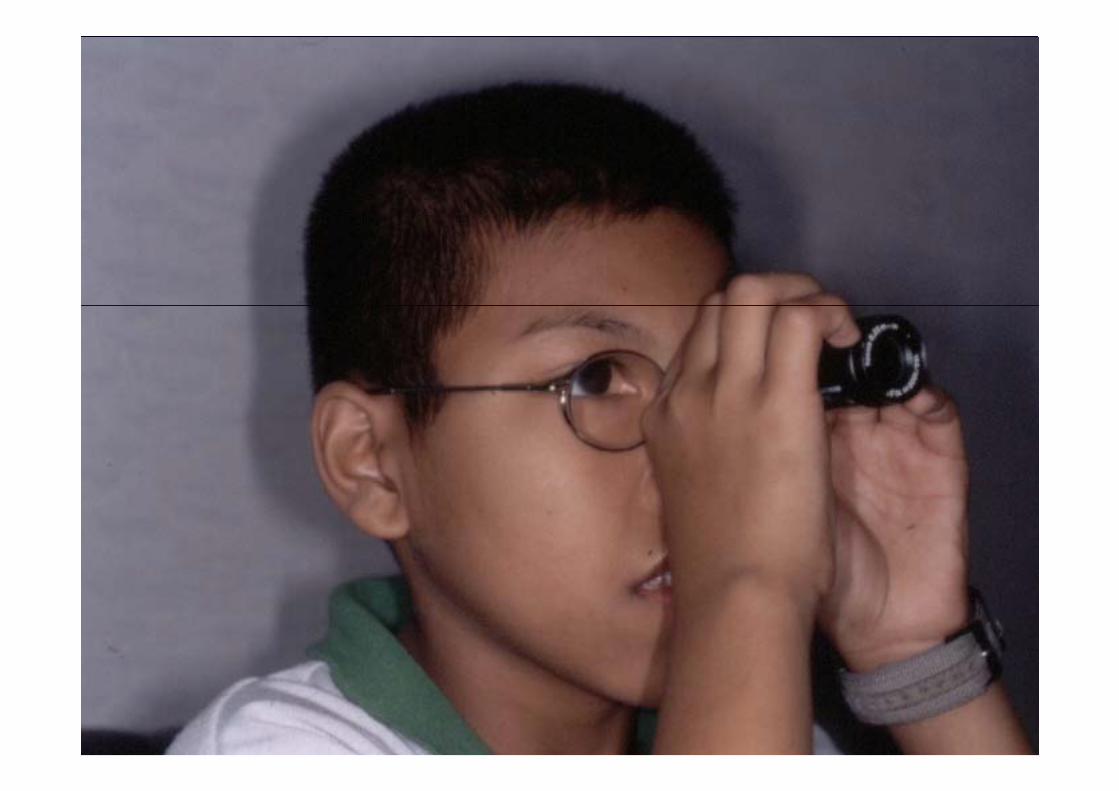
Telescope
the only visual aids for distance visionl / bi lmonocular / binocular
Galilean (distance) / Keplerian ( closer)G e (d s ce) / ep e ( c ose )small field of view / must be held very steadilymagnification >8X are not routinely recommended

Community ophthalmology y p gy
Monocular telescopeMonocular telescope

Community ophthalmology y p gy
Community ophthalmology y p gy
Community ophthalmology y p gy

Community ophthalmology y p gy
Video magnifiersg
small video camera with a zoom closed-up lens connected with a monitor
make the image as large as necessarymake the image as large as necessaryreverse polarity may be more contrast
iexpensive

Community ophthalmology y p gy

Community ophthalmology y p gy
Aids for visual field loss
Prismsexpand VF awareness in loss side vision
f i / di i ti d t i iconfusing / disorienting, need trainingReverse telescopesReverse telescopes
smaller magnification but larger field
Community ophthalmology y p gyRelative size devices
Large printsharp edgesharp edgeat least 2.7 mm. height letter 18 point typeg p yphigh contrast & good opaque paper
Large print typewriters & computer

Community ophthalmology y p gy
Lighting & illumination controlSunlight natural but control problemFluorescent lower contrast but fewer shadow coolerFluorescent lower contrast, but fewer shadow, coolerIncandescent more contrast, more shadow, less scatter
Neodymium sunlight improve reading performanceHalogen UV may be phototoxic, should be caution
Rheostat use to control light sourceRheostat use to control light source

Community ophthalmology y p gy
Filter
control glarel t l l di t ticolor neutral gray no color distortion
green very little effect on color perceptiong y p pyellow increase contrast by absorbing scattering
blue light

Community ophthalmology y p gy

Community ophthalmology y p gy

Community ophthalmology y p gy

Community ophthalmology y p gy

Community ophthalmology y p gy
Occupational healthhealth assessment
) & 1) pre & post employment exam2) exam for hazard exposure2) exam for hazard exposure3) treatment as family doctor4) emergency treatment at workplace

Community ophthalmology y p gy
Occupational health
Advisory service1) prevention of occupational disease1) prevention of occupational disease2) forensic medicine3) di l t f k / i t3) medical aspect of work process / environment4) prevention of common non-occupational disease5) t i i fi t id5) training first aid6) plan for major disaster

Community ophthalmology y p gy
Eye protection program
1) environment survey
2) vision screening
3) implementation of the program
4) maintenance of the program

Community ophthalmology y p gy
Environment surveychemical
identify occupational hazardchemical
physical
control hazard biological
ergonomic
emergency first aid deviceemergency first aid device
accident recordaccident record

Community ophthalmology y p gy
advantage of vision screening in industry1) l i f l i bl1) selection of personnel suitable2) identify visual disable transfer/rehabilitation3) improve relationship4) improve visual efficiency increase productivity4) improve visual efficiency increase productivity
reduce accidentreduce visual fatiguing
5) appropriate compensatory claim5) appropriate compensatory claim

Community ophthalmology y p gy
Implementation of the program 1) elimination / control of ocular hazard
2) provision of eye protectors) p y p3) hazard zoning with warning sign4) first aid facility4) first aid facility5) lens cleaning station6) safety committee6) safety committee7) education /training

Community ophthalmology y p gy
Prevention & control strategy
1) specification 2) substitution
3) segregation 4) local extract ventilation
) )5) dilution ventilation 6) personal hygiene
7) reduce time exposure 8) personal protection7) reduce time exposure 8) personal protection

Community ophthalmology y p gy
Safety sign
type prohibition mandatory warning safe condition
meaning STOP MUST CAUTION way to gomeaning STOP MUST CAUTION way to go
symbol

Community ophthalmology y p gy

Community ophthalmology y p gy

Community ophthalmology y p gy

Community ophthalmology y p gy

Community ophthalmology y p gy