Community Task Force on Oral Health Needs of People with Developmental Disabilities
14
Community Task Force on Oral Health Needs of People with Developmental Disabilities KEY FINDINGS
description
Community Task Force on Oral Health Needs of People with Developmental Disabilities. KEY FINDINGS. Workgroup Leaders. Demographics: Who is Receiving What from Whom ? – Ann Costello and Brian Klafehn Consumer Perceptions and Satisfaction – Lenora Colaruotolo - PowerPoint PPT Presentation
Transcript of Community Task Force on Oral Health Needs of People with Developmental Disabilities

Community Task Force on Oral Health Needs of People with Developmental Disabilities
KEY FINDINGS

Workgroup Leaders
Demographics: Who is Receiving What from Whom?– Ann Costello and Brian Klafehn
Consumer Perceptions and Satisfaction– Lenora Colaruotolo
Provider Experiences and Expectations– Lisa DeLucia
Current and Unfolding Policy– Rich Speisman
Model IDD Oral Health Care Programs– Maricelle Abayon.
Facilitator– Larry Belle

Demographics: Who is ReceivingWhat from Whom?
FLDDSO - 9,300 individuals in 2012 - Monroe, Wayne, Ontario, Livingston, Orleans.
12,000 in the 11 county Finger Lakes region.
Monroe County (55%); with 40% between the ages of 21-44 years; and 35% living in some type of certified residence.
EIOH, RGH, Anthony Jordon, CP Rochester and FLDDO Dental Clinic - 2,786 patients (2011)-Wait time -ambulatory <6 months, OR >12 months.
<17% private DDS see Medicaid.

Development of a standard patient classification system to be used by the community-based clinics as well as private practice dentists.
Clarify the actual number of individuals receiving dental services on an annual basis by using DOH Medicaid claims data.
Determine how many individuals are not receiving routine, preventive dental services and why?
Work collaboratively with local area hospitals to reduce wait-time for needed OR services and improve oral health to mitigate the need for OR services.
Demographics: Who is ReceivingWhat from Whom?

Consumer Perceptions and Satisfaction
Determine areas of oral health satisfaction, perception and need.
Survey of local agencies and Focus groups of constituents.
8% Individual
32% Parent
2% Guardian
29% Other
29% Care Provider
Type of Respondent

Type of Respondant
Regularity of Past Dental Attendancen=560
102,18.20%
48, 8.60%
410, 73.20%
Regular Dental VisitOccasional Dental VisitOnly if Trouble with Teeth
Consumer Perceptions and Satisfaction

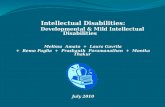
Perceptions on Oral Health Care
Oral H
ealth
: Exc
ellen
t/Good
Oral H
ealth
: Fair
/Poor
Oral H
ealth
Importa
nt
Anxiety
about D
entis
try
Provid
er Optio
ns: Diss
atisfi
ed
Provid
er Optio
ns: Sati
sfied
Knowledge/F
riendly:
Hyg
ienist
Knowledge/F
riendly:
Den
tist
Satisfi
ed w
ith tre
atmen
t
Saw a
dentis
t in th
e pas
t yea
r
Visit D
entis
t eve
ry 6 m
onths0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
47%53%
70%74%
20%
60%
77% 77%72%
85%
73%

Suggestions for Improvement
80% of dental disease occurs in 20% of the population-the most underserved and least likely to access services and care. (NOT SAMPLED)
Patient-centered care.
Knowledgeable staff and practitioners.
Universal design.
The concerns and requests of the family members should be incorporated into any systemic design of oral health services for this population.

Provider Experiences and Expectations
Surveys and Focus Groups.
7th District Dental Society and Dental Hygiene Society, RGH and EIOH.
151 respondents – DDS 59% (high % specialists and institutional providers), OH 41%.
Close to 70% of respondents treated individuals with IDD and feel relatively comfortable and competent doing so.
Respondents felt more competent and prepared to treat patients with mobility issues than they did with patients who had communication and behavioral limitations.
High % wanted additional training.

Topics for Continuing Education
0%
10%
20%
30%
40%
50%
60%
70%
41%
59% 60%
25%21% 19%
38%42%

Current and Unfolding Policy
Managed Care.
Fragile and ever-changing dental reimbursement picture.
Reduction or elimination of services.
Dental Accreditation.
Role of Dental Hygienists.
Inefficient and limited use of OR care.
Dental Disco Advisory Group (DDSG).
Opportunity for demonstration projects.

Model IDD Oral Health Care Programs
Atlantic County Special Services School District by University of Medicine and Dentistry of New Jersey.
The Special Smiles Program – Philadelphia.
Tufts, Boston – closed.
Glassman, San Francisco.

Glassman Model California
Focuses on prevention of dental diseases.
Utilizes a case management approach.
Employs a tiered delivery system.
Provides care as close as possible to where individuals with IDD disabilities live, work and go to school.
Enables hygienists to play a major role in oral health maintenance, as well as in education of family and caregivers.
Use of Tele-health.
Uses existing community health professionals in new ways.
Rewards services that will improve oral health.

Website
Full report and executive summary can be found on the following website:
http://www.urmc.rochester.edu/dentistry/news-events.aspx