
Community Needs AssessmentDepartment of Health and Human Services by April 1, ... treatment for...
70
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis March 2016
Transcript of Community Needs AssessmentDepartment of Health and Human Services by April 1, ... treatment for...

Alliance Behavioral Healthcare
Community Needs Assessment and Gaps Analysis
March 2016

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 2
Table of Contents
Section One: Executive Summary and Overview ................................................................... 3
I. Executive Summary ......................................................................................................... 3
II. Update on FY 2015-16 Network Development Plan......................................................... 6
III. Description of Service Region and Demographics ......................................................... 12
IV. Methodology for Consumer and Family Input ................................................................ 16
V. Methodology for Stakeholder Input ................................................................................ 17
Section Two: Access and Choice Standards, Service Needs, Gaps and Strategies ............... 18
I. Outpatient Services ....................................................................................................... 19
II. Location-Based Services ............................................................................................... 21
III. Community and Mobile Services ................................................................................... 24
IV. Crisis Services ............................................................................................................... 27
V. Inpatient Services .......................................................................................................... 29
VI. Specialized Services ..................................................................................................... 31
VII. State-Funded Services Items ........................................................................................ 33
Section Three: Geoaccess Maps............................................................................................ 36
Section Four: Departmental (DHHS) Initiatives ....................................................................... 37
Appendices ............................................................................................................................ 42
A. Geographic Access Maps .............................................................................................. 43
B. Specialized Services List ............................................................................................... 46
C. Stakeholder Survey Questions ...................................................................................... 62
D. Community Feedback .................................................................................................... 64
E. DHHS Waiver Attachments............................................................................................ 68
Prepared by:
Carlyle Johnson, Ph.D.
Director, Provider Network Strategic Initiatives
Alliance Behavioral Healthcare

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 3
Section One Executive Summary and Overview
I. Executive Summary
On an annual basis Alliance conducts a review of its provider capacity, community needs and
service gaps to inform our strategic plan for improving accessibility and effectiveness of care and
supports. The report period covers Fiscal Year 2014-15 and is submitted to the North Carolina
Department of Health and Human Services by April 1, 2016 as required by DHHS-MCO contracts.
The 2016 Alliance Community Needs Assessment and Gaps Analysis includes a summary of the
previous year’s actions, review of provider capacity, assessment of service accessibility and choice,
and incorporation of community feedback about needs and gaps. The resulting analysis and
conclusions are the basis for network development priorities and the Alliance Network Development
Plan for FY16-17.
Alliance Behavioral Healthcare manages behavioral health services for Cumberland, Durham,
Johnston and Wake counties in a catchment area that includes a mix of urban and rural areas. Our
region is experiencing higher than average population growth and is challenged to meet the needs of
a diverse population with important needs such as those who do not speak English, homeless
individuals with mental illness and substance use disorders, and members of the military, veterans
and their families.
The Community Needs Assessment process has provided an opportunity to review the status of the FY16 Network Development Plan, obtain additional community input and identify strategic goals for network development for FY17. The following analysis provides a summary of information obtained through this process and the themes and objectives that have emerged as highest priority actions for FY17. Priorities were determined based on multiple factors and sources, including demographic information, utilization data, emerging trends and input from consumers, stakeholders, providers and staff. Recommendations for priority items also considered the importance of alignment with Alliance’s mission, vision and values.
Accomplishments and Updates
Alliance has made progress on a number of significant needs and gaps that were identified as priorities for the FY16 Network Development Plan. Over the past year, we have:
Expanded access to Medicaid (b)(3) services such as Individual Support and Peer Support
Added State contracts to resolve gaps identified last year
Improved crisis capacity and access through expansion of Behavioral Health Urgent Care/Same Day Access, transition of Durham crisis services to a peer recovery model, implementation of rapid response crisis services for children and adolescents, pending addition of a new crisis facility in Wake County, and training for advanced practice paramedics and support for alternative drop-off locations
Initiated pilot projects to improve outcomes for high risk youth and provide evidence-based treatment for youth with co-occurring IDD/MI
Promoted evidence-based Intensive In-Home services, treatment for first episode psychosis, and integrated behavioral health/medical care
Developed alternative service definitions and supports to improve continuity and effectiveness of care.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 4
We have also worked collaboratively with consumers, providers and stakeholders to raise awareness of behavioral health issues through the “It’s Time to Rethink” public awareness campaign, and have developed a comprehensive plan for improving community awareness and support for principles of recovery. Alliance has refined its Mission, Vision and Values statements and made significant advancements on its Strategic Plan development. In particular, the focus on whole-person care, recovery, and evidence-based practices are significant factors that will help frame our network development efforts in the upcoming year.
Service Needs and Gaps
Alliance conducted an extensive review of service needs that included review of data and input from
consumers and families, stakeholders, providers and staff. Analysis of survey results identified
consistent issues and themes both across and within age/disability areas. Consistent with the
findings of past network gaps analysis, residential treatment, housing, and transportation remain
areas of concern and ongoing barriers for promoting treatment engagement and positive outcomes.
Other common findings include gaps in services for individuals with co-occurring IDD/MI, service
access for non-English speaking, and the adequacy of crisis, respite and hospital diversion service
capacity.
Several noteworthy priorities include:
Development of a comprehensive, evidence-based continuum of care for individuals with
substance use disorders and concerns about the increased prevalence of opioid abuse and
overdoses in our communities
Plans to address disparities between uninsured and insured, and geographic disparities in
service availability for the uninsured
Increased information about services and system navigation
Several areas identified in the FY15-16 Network Development Plan remain areas of focus for the
upcoming year and will be included in the FY16-17 Network Development Plan. These areas include
development of a more uniform State benefit package, improving accessibility of high quality mobile
crisis services, addressing gaps for individuals with co-occurring IDD/MI.
Network Development Priorities for FY17
A primary objective of the Community Needs Assessment and Gaps Analysis is to identify and
prioritize community service needs and gaps that will inform and guide further development
activities. Based on extensive review of data and community input, Alliance has identified the
following priorities for network development that will be included in the FY17 Network
Development Plan:
Expand services to meet geographic access and choice standards
Develop a more uniform State benefit package across the four-county Alliance area
Expand capacity for crisis, hospital diversion and respite services for all ages/disabilities
Increase breadth, access and quality of residential treatment and housing options
Increase capacity to serve consumers with IDD or co-occurring IDD/MI
Develop and enhance the continuum of care for individuals with Substance Use Disorders
with specific focus on increasing access to Medication Assisted Treatment
Improve access to services for underserved populations
Increase availability, tracking and oversight of specialty services and evidence-based
practices

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 5
Increase availability of resources for transportation
Increase availability of resources for employment
These priorities will serve as the foundation for FY17 network development activities and further
discussions with our consumers, stakeholders and providers on strategies for improving access,
quality and outcomes of care.
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 6
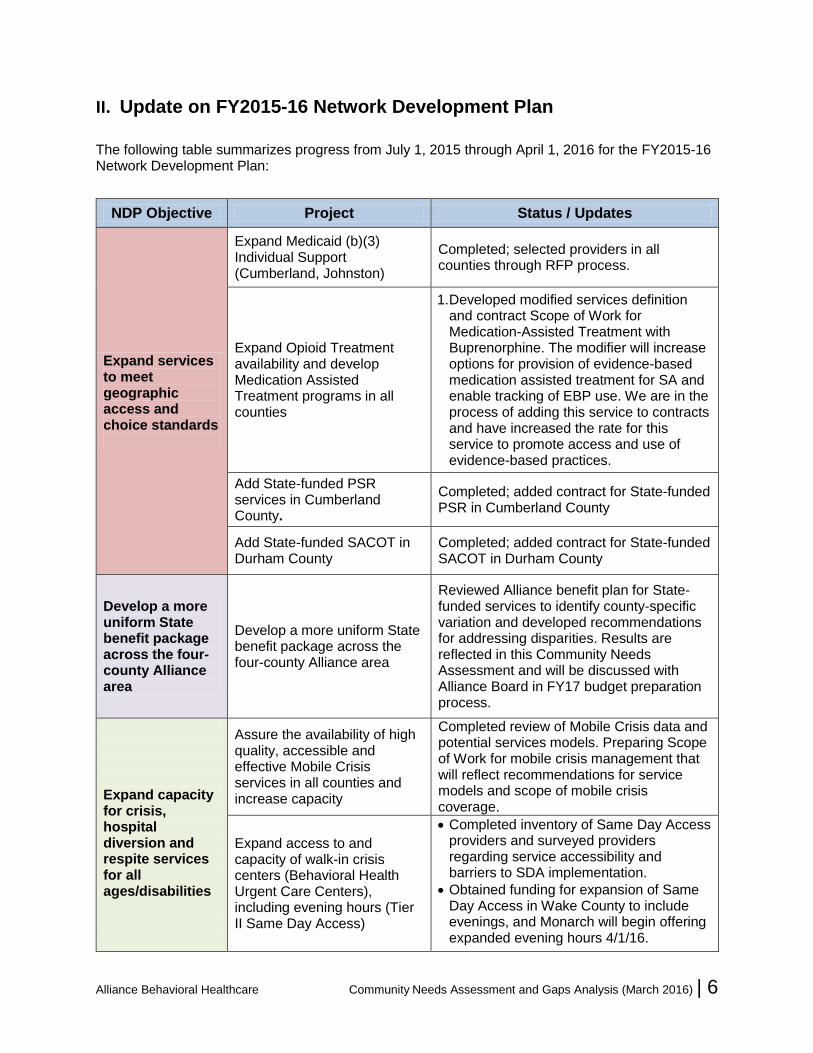
II. Update on FY2015-16 Network Development Plan The following table summarizes progress from July 1, 2015 through April 1, 2016 for the FY2015-16 Network Development Plan:
NDP Objective Project Status / Updates
Expand services to meet geographic access and choice standards
Expand Medicaid (b)(3) Individual Support (Cumberland, Johnston)
Completed; selected providers in all counties through RFP process.
Expand Opioid Treatment availability and develop Medication Assisted Treatment programs in all counties
1. Developed modified services definition and contract Scope of Work for Medication-Assisted Treatment with Buprenorphine. The modifier will increase options for provision of evidence-based medication assisted treatment for SA and enable tracking of EBP use. We are in the process of adding this service to contracts and have increased the rate for this service to promote access and use of evidence-based practices.
Add State-funded PSR services in Cumberland County.
Completed; added contract for State-funded PSR in Cumberland County
Add State-funded SACOT in Durham County
Completed; added contract for State-funded SACOT in Durham County
Develop a more uniform State benefit package across the four-county Alliance area
Develop a more uniform State benefit package across the four-county Alliance area
Reviewed Alliance benefit plan for State-funded services to identify county-specific variation and developed recommendations for addressing disparities. Results are reflected in this Community Needs Assessment and will be discussed with Alliance Board in FY17 budget preparation process.
Expand capacity for crisis, hospital diversion and respite services for all ages/disabilities
Assure the availability of high quality, accessible and effective Mobile Crisis services in all counties and increase capacity
Completed review of Mobile Crisis data and potential services models. Preparing Scope of Work for mobile crisis management that will reflect recommendations for service models and scope of mobile crisis coverage.
Expand access to and capacity of walk-in crisis centers (Behavioral Health Urgent Care Centers), including evening hours (Tier II Same Day Access)
Completed inventory of Same Day Access providers and surveyed providers regarding service accessibility and barriers to SDA implementation.
Obtained funding for expansion of Same Day Access in Wake County to include evenings, and Monarch will begin offering expanded evening hours 4/1/16.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 7
NDP Objective Project Status / Updates
Expand capacity for crisis, hospital diversion and respite services for all ages/disabilities
Further analysis will assist with identifying challenges, opportunities and cost model assumptions for further development.
Expand/Enhance Capacity of Facility Based Crisis
Completed RFP process for Durham Crisis services and selected provider.
Posted RFP for additional Wake crisis facility and vendor, Monarch, has been selected. Implementation plans are being developed and Monarch is exploring potential facility locations.
Provide education to urgent care and primary care practices about Alliance and crisis response resources and how to access them, including Open Access, mobile crisis, facility based crisis
Collaborated with CCNC to identify priority practices for training, develop joint training information, and set up primary care/behavioral health provider meetings.
Purchased software to run routine reports on primary care practices with high number of behavioral health consumers.
Established and hired new Integrated Care Director position.
Implemented CMT software with initial focus on notification for consumers who did not fill antipsychotic medication prescriptions and notifying PCPs about potential opioid abuse issues.
Developed communication strategy for education of primary care physicians about non-ED crisis services available to their patients.
Implement Advanced Practice Paramedics program in Durham
Coordinated training program for Durham CIT-certified EMS paramedics to receive additional on-line training. Both Wake and Durham EMS have completed webinar training. We received allocation letters for Wake and Durham to be reimbursed for alternative drop off destinations.
Develop capacity for IDD Crisis Respite
Working with residential provider to identify and implement service model for short-term (30-45 days) PRTF for children with autism. Provider is evaluating models from other states.
Review outcomes for rapid response crisis diversion services for children and adolescents
Completed evaluation of Wake rapid response service and additional data will be available for more extensive analysis in April. A workgroup has been convened and is working through issues related to 131D

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 8
NDP Objective Project Status / Updates
licensure rules and crisis beds. We have also developed a Medicaid alternative service definition to expand this service to all Alliance counties and will be submitting for DMA approval in April.
Implement Critical Time Intervention (CTI) in Cumberland
Completed selection of provider through RFP and have implemented services in Cumberland.
Increase breadth, access and quality of residential options
Evaluate transitional living outcomes and capacity and determine need for expansion
Completed analysis of claims data and developed survey to gather additional information from Transitional Living providers. Follow-up evaluation of outcomes is planned for Summer 2016.
Develop Comprehensive Assessment for youth with complex needs prior to referral to residential services
Identified provider, reviewed list of standard measures that will be required in assessment, and requested rate proposal from provider. Contract pending with UNC to provide this service, with services expected to begin in April 2016.
Complete residential continuum study
Contracted with the Technical Assistance Collaborative (TAC) to conduct an evaluation of the Alliance residential continuum. Developed Alliance Housing Plan and established new Director of Housing position that will implement specific project plan to address housing gaps.
Increase capacity to serve dually diagnosed (IDD/MI) consumers
Implement pilot Youth Villages Choices model for dually diagnosed (IDD/MI) youth
Completed implementation of pilot model through Youth Villages, and program has begun serving consumers. Augmenting pilot with addition of residential services through RFP.
Evaluate increased funding support for NC START
Identified funding for an adolescent START program, based on proposal submitted by Easter Seals UCP. Contract is in place and services have initiated.
Offer dual diagnosis (IDD/MI) training for Mobile Crisis teams
Completed training.
Offer training on IDD/MI dual diagnosis issues to large behavioral health practices
Completed training

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 9
NDP Objective Project Status / Updates
Develop plan to address service gaps between enhanced benefit and outpatient services and to address need for case management
Develop alternative service definition for Medicaid-funded outpatient treatment
Working with consultant, Partners MCO and providers to develop proposed alternative service definition. Draft has been completed and submitted to DMA.
Develop service definition to fill service gap between ACTT and CST
We have worked with a consult, Partners MCO and providers to develop alternative service definitions for Critical Time Intervention (CTI) enhanced outpatient, enhanced CST (CST Plus) and ACTT Step-Down services. CTI and ACTT Step-Down have been approved by DMA and CST Plus will be submitted to DMA in April.
Increase availability, tracking and oversight of specialty services and evidence-based practices
Increase number of evidence based practices meeting fidelity for substance abuse providers
Working with SA providers through SA Treatment Provider Collaborative, and developed contract to provide individualized provider consultations on EBPs. Requested proposals from SA providers and selected six providers who will received individualized on-site consultations. Consultation has been completed with Cape Fear and written recommendations are being prepared.
Contract for EBP models for IIH and require independent fidelity reviews
Met monthly with IIH providers to implement change in contract requiring family-oriented EBPs and have convened multiple meetings and workgroups with providers, developers and implementation resources to refine implementation plans.
Developed cost models for training and long-term sustainability of EBPs, in collaboration with providers and EBP developers.
FY17 Medicaid contracts will include Scopes of Work for IIH EBPs, and Alliance is supporting training on two EBP models that will be incorporated into contracts.
Develop process for development and implementation of EBPs with external fidelity verification
Completed.
Promote EBPs for PSR programs including peer led programs, recovery oriented programs, and for dually diagnosed (MH/IDD)
Gathered information about PSR services, EBP models and prepared written recommendations for further development of evidence-based services within PSR.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 10
NDP Objective Project Status / Updates
Provide Training and Consultation for Providers to promote improved quality and implementation of evidence based practices
Hired consultant, Promise Resource Network, to provide Peer Support training on two dates for all Peer Support providers.
Completed DBT intensive training for Alliance DBT providers. We are working with Behavioral Tech and providers regarding DBT sustainability planning.
Provided SE Collaborative to promote evidence-based MH/SA IPS model supported employment services.
Convened and supported provider collaboratives to promote EBP implementation, including CST, IIH, Substance Use Disorder treatment, and Therapeutic Foster Care.
Identify high cost/high need populations and match with EBP
Implement pilots for Youth Villages Intercept model, Kidspeace TFC and Mentor Family Centered Treatment model for high needs youth
Pilots all launched effective July 1.
Implement First Episode Psychosis Program in Wake County
Completed implementation.
Improve access to services for non-English speaking consumers
Conduct survey of providers with identified services for non-English speaking consumers. Clarify service availability and capacity for more robust bilingual/bicultural program emphasis.
Worked with Alliance Cultural Competency committee to develop and administer provider survey. Results will be included in development of FY17 Network Development Plan.
Increased capacity to serve TBI population
Participate in TBI HRSA grant
Conducted screening for TBI through Call Center and collected data for State analysis.
Working with Brain Injury Association of NC and neuroresource facilitator to develop TBI-specific provider trainings
Will begin reviewing data through TBI Grant Steering Committee.
DHHS has announced plans for a TBI waiver that will be piloted with Alliance in the first year of the waiver. There are 49 slots attached to the waiver for Alliance.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 11
NDP Objective Project Status / Updates
Expand integrated behavioral health/medical care
Conduct Inventory of current integrated care initiatives (e.g., Turning Point, Lincoln, UNC WakeBrook; Johnston Public Health, exploring Duke/CBC co-location and reverse co-location; FHR Dartmouth In-Shape, Southlight)
Completed inventory.
Implement integrated healthcare pilots
Developed charters and project plans for each pilot. Hired consultant to evaluate pilots. Contracts executed for new initiatives with Carolina Outreach, Easter Seals UCP, Duke, Carolina Behavioral Care and UNC.
Conduct evaluation of current integrated behavioral health/medical care initiatives and development of recommendations for further expansion
Hired NC Center of Excellence for Integrated Care to evaluate pilot projects. Evaluation is in process and the consultation report is expected in December 2016.
Increase availability of resources for transportation
Review transportation initiatives in other states, inventory provider and stakeholders efforts and develop recommendations
Review of transportation initiatives in progress.
Increase availability of resources for employment
Increase number of persons receiving MH/SA SE/LTVS
Conducted RFP for SE/LTVS services in Cumberland, selected vendor and in the process of expanding services in Cumberland. Meeting regularly with SE/LTVS providers through collaborative.
NC is now working with several other states and federal government through Vision Quest and Office of Disability and Employment Policy (ODEP) to look at sustainability of IPS at a statewide level. Alliance is participating in this planning process.
We are looking at feasibility of aligning b3 rate and service definition with State rate and service definition.
Evaluate impact of MH/SA SE-LTVS
Transitioned to Alliance Business Process Team, which will be conducting ongoing analysis of IPS SE/LTVS as part of TCLI monitoring.
Explore models and supports for consumer-run businesses
Review of consumer-run models in progress.
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 12
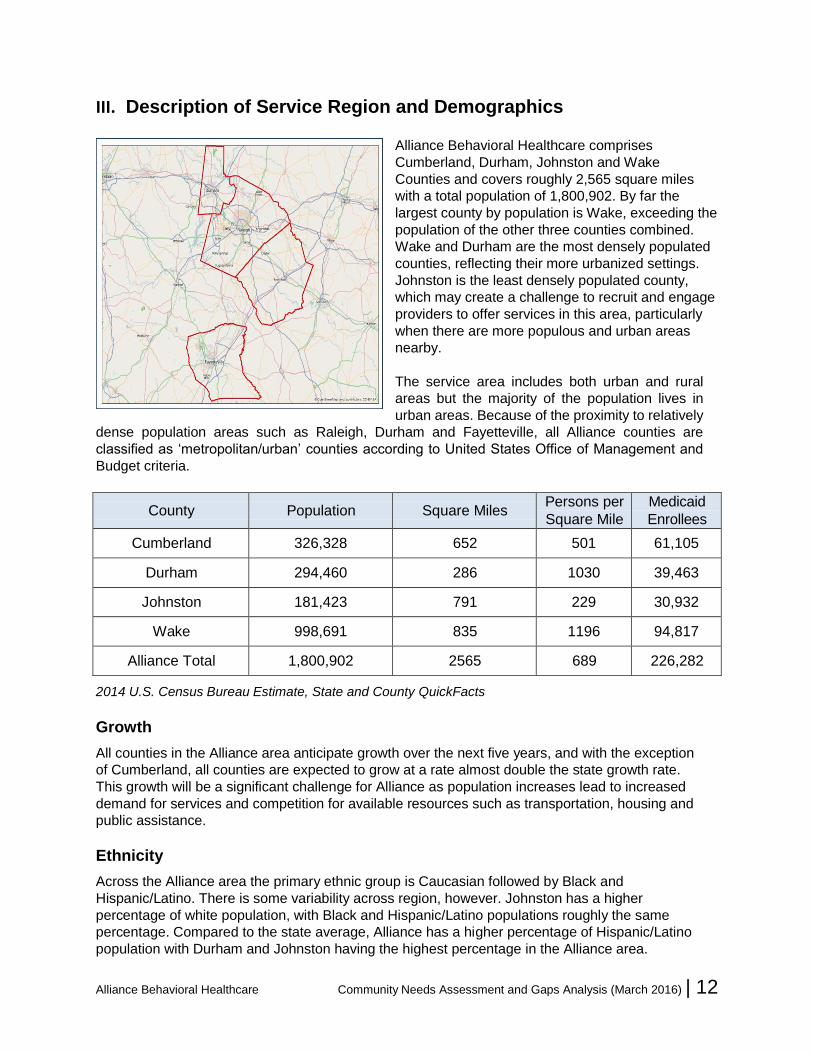
III. Description of Service Region and Demographics
Alliance Behavioral Healthcare comprises
Cumberland, Durham, Johnston and Wake
Counties and covers roughly 2,565 square miles
with a total population of 1,800,902. By far the
largest county by population is Wake, exceeding the
population of the other three counties combined.
Wake and Durham are the most densely populated
counties, reflecting their more urbanized settings.
Johnston is the least densely populated county,
which may create a challenge to recruit and engage
providers to offer services in this area, particularly
when there are more populous and urban areas
nearby.
The service area includes both urban and rural
areas but the majority of the population lives in
urban areas. Because of the proximity to relatively
dense population areas such as Raleigh, Durham and Fayetteville, all Alliance counties are
classified as ‘metropolitan/urban’ counties according to United States Office of Management and
Budget criteria.
County Population Square Miles Persons per
Square Mile
Medicaid
Enrollees
Cumberland 326,328 652 501 61,105
Durham 294,460 286 1030 39,463
Johnston 181,423 791 229 30,932
Wake 998,691 835 1196 94,817
Alliance Total 1,800,902 2565 689 226,282
2014 U.S. Census Bureau Estimate, State and County QuickFacts
Growth
All counties in the Alliance area anticipate growth over the next five years, and with the exception
of Cumberland, all counties are expected to grow at a rate almost double the state growth rate.
This growth will be a significant challenge for Alliance as population increases lead to increased
demand for services and competition for available resources such as transportation, housing and
public assistance.
Ethnicity
Across the Alliance area the primary ethnic group is Caucasian followed by Black and
Hispanic/Latino. There is some variability across region, however. Johnston has a higher
percentage of white population, with Black and Hispanic/Latino populations roughly the same
percentage. Compared to the state average, Alliance has a higher percentage of Hispanic/Latino
population with Durham and Johnston having the highest percentage in the Alliance area.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 13
County White Black Asian American
Indian
Hispanic/
Latino
Cumberland 53.2% 37.6% 2.7% 1.8% 11.0%
Durham 53.0% 38.6% 4.9% 1.0% 13.4%
Johnston 80.4% 16.0% 0.8% 0.9% 13.4%
Wake 69.0% 21.3% 6.4% 0.8% 10.0%
NC 71.5% 21.5% 2.7% 1.6% 9.0%
Will not equal 100% due to more than one race being reported. Source: US Census Bureau, 2014
QuickFacts
Languages Spoken
The primary language spoken across the Alliance area is English, followed by Spanish most notably
in Durham and Johnston Counties where the rate exceeds 10% of the population. Alliance exceeds
the state average with respect to non-English languages. Although the primary non-English
language spoken is Spanish, it is noteworthy that other languages account for over 6% of the
population and that there are 20 languages or language groups for which there are over 1,000 or
more speakers in the Alliance catchment area.
Military/Veterans
The Alliance catchment area includes several important resources for active military, veterans and
their families, including the Fort Bragg military installations, VA Hospitals in Fayetteville and Durham,
Reserve Command and local units, and NC National Guard units. An estimated 135,496 veterans
live in the Alliance catchment area, according to the 2014 NC Veterans Annual Report, with the
following distributions by county:
Wake 58,436
Cumberland 47,298
Durham 15,846
Johnston 13,916
The largest concentration per capita is in Cumberland County, with approximately 14.5% of its
residents having served in the military, compared to the NC state average of 7.8%. Alliance works
closely with community stakeholders, providers, military and veterans’ organizations and all levels of
government to promote effective and accessible care for military, veterans and family members.
Alliance has developed a draft FY 2015/16 Veterans Plan that provides additional information about
current and planned initiatives to improve services for the military/veterans population.
Homeless Population
Three of the four Alliance counties have higher rates of homelessness than the surrounding region
and rates of homelessness for Cumberland and Durham exceed the state average, while Wake
County’s rate is approximately equal to the state average, based on the 2014 North Carolina Point-
in-Time Count of People Experiencing Homelessness. Rates are highest per capita for Durham and
Cumberland, but the number of homeless individuals is highest in Wake County. The highest rates

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 14
of chronic homelessness were observed in Cumberland. Homeless populations in Durham and
Wake were found to have higher rates of serious mental illness and substance use among the
homeless than were observed in Cumberland or Johnston.
Health Outcomes and Disparities
Alliance counties vary significantly with respect to health outcomes, and population health data
reveals higher needs for health care improvements particularly in Cumberland and Johnston
counties. Research has demonstrated significant health disparities for individuals with mental illness,
substance use and intellectual and developmental disabilities, and growing evidence indicates that
shortened lifespans are primarily associated with chronic health conditions, health behaviors,
substance use and limited access to appropriate medical care. Both the demographic data and
research evidence support an increased emphasis on integrated behavioral health/medical care and
on increased substance abuse prevention and treatment efforts all counties.
Description of Provider Network
Alliance has a large network of credentialed providers and most organization types are available in
each county, as are prescribers and licensed practitioners. Providers by categories for FY15 are as
follows:
1849 licensed professionals
281 agencies
291 outpatient practices
37 Hospitals/Residential Treatment Facilities

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 15
Services available in the network include a broad array of Medicaid and State-funded care, and
providers served 39,560 Medicaid consumers and 17,492 with State funds in FY15.
The following table provides a summary of service expenditures for FY16:
Source Amount % of Total
Medicaid $419,717,116 82%
State $58,851,040 11%
Local $36,758,095 7%
Total $515,326,251 100.0%

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 16
IV. Methodology for Consumer and Family Input
The process for soliciting consumer and family feedback included the following approaches:
1. Consumer and Family Advisory Committee (CFAC) Feedback
Feedback approaches included presentation and discussion at CFAC meetings, and submission
of a CFAC summary of identified needs and gaps. CFAC members also helped inform others
about the electronic survey and distributed hard copy version of the survey to those without
internet access and those who preferred to submit a handwritten response.
2. Community Survey
Feedback was solicited through an internet-based survey using SurveyMonkey®. The survey
included separate sections for Intellectual and Developmental Disabilities (IDD), Child Mental
Health/Substance Abuse (Child MH/SA), Adult Mental Health and Substance Abuse (Adult
MH/SA) and Traumatic Brain Injuries (TBI), with the option for respondents to skip those sections
with which they were unfamiliar. Additional sections were included regarding needs and gaps in
areas of housing, employment and transportation. The same questions were used for all
respondents, which included consumers and family members, stakeholders, providers and
Alliance staff. Surveys were administered anonymously and no identifying information was
required. Survey links were posted on the Alliance website and distribute to multiple consumer,
provider and stakeholder e-mail lists. A request was sent to all Alliance staff requesting that links
be forwarded to community contacts, and Alliance staff were surveyed regarding community
needs and gaps.
Community Needs Assessment Survey Questions
Introductory questions collected limited background information about respondent category, county of respondent, and respondent’s organization type if applicable. Each section of the survey included a similar format and consisted of the following sections/questions:
1. Listing of service types and Likert rating scale for availability of each service.
2. Follow-up questions (text box) for entry of additional feedback about service availability,
including:
a. Services not covered on survey questions
b. Barriers to receiving services
c. Identification of underserved groups or populations
3. Questions for all respondents soliciting input (text boxes) regarding the most significant needs
for:
a. Housing
b. Employment
c. Transportation
d. Other comments regarding service needs and gaps
Hard copy versions of the survey were posted on the Alliance website in formats that included a full version and separate versions for IDD, Child MH/SA, Adult MH/SA and TBI. The full hard copy version is available at the following link: http://www.alliancebhc.org/2016-cna-survey-full/.
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 17
V. Methodology for Stakeholder Input
The process for soliciting stakeholder feedback included the following approaches:
1. Alliance Provider Advisory Committee (APAC) Feedback
Provider feedback included discussion at APAC meetings as well as follow-up discussion and
feedback from local PAC meetings in each county.
2. Community Survey
As described above, the online survey solicited responses from consumers, family members,
providers, stakeholders and staff.
3. Collective Feedback from Community Workgroups, Collaboratives and
Committees
Alliance staff contacted existing groups such as crisis collaboratives, System of Care
collaboratives, provider collaboratives, and Alliance staff meetings to request collective responses
regarding highest priority needs and gaps. A survey form was provided to each group with
suggested questions for group discussion, and groups submitted summaries of group
recommendations. Copies of the Alliance Staff Group Feedback Form and Alliance Stakeholder
Feedback Form are provided in Appendix C.
Community Input Sources
Numerous community groups were invited to provide input through collective responses, completion
of on-line surveys, or both. Alliance staff attended meetings of many of these groups to solicit and
summarize feedback. Sources of feedback included the following:
Consumer and Family Advisory Committee (CFAC)
NAMI-Wake, NAMI-Durham and NAMI-Cumberland
Alliance Provider Advisory Committee (APAC), including local PAC meetings in each county
Durham and Wake Juvenile Justice SA/MH Partnership (Durham JJSAMHP, Wake JJSAMHP)
Cumberland County Reclaiming Futures
MH/SA Supported Employment Provider Collaborative
Provider Collaboratives for Community Support Team (CST), Substance Abuse Treatment, Intensive In-Home (IIH), and Therapeutic Foster Care (TFC)
Crisis Collaboratives in Cumberland, Durham and Wake
SOC Community Collaboratives in each county
All-Provider Meeting
Next Steps (Wake)
Alliance Hospital Partners Collaborative
MH/SA Care Coordinators
IDD Care Coordinators
Alliance Clinical Operations Staff
Alliance Utilization Management Staff
Alliance Provider Network Evaluators
Alliance Compliance Staff
Alliance Call Center Staff

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 18
Section Two
Access and Choice, Service Needs, Gaps and Strategies Introduction
Although the counties comprising Alliance Behavioral Healthcare’s catchment area vary significantly
in population density, all are classified as “metropolitan/urban” counties according to United States
Office of Management and Budget criteria. Accordingly the DHHS-MCO contract requires that
Alliance ensure availability of providers within a 30-mile radius or 30-minute drive time for any
consumer residing in the Alliance catchment area. The following section provides a summary of
geographic access and choice data for Alliance services in several categories:
Outpatient Services include psychiatric care, medication management, evaluations, and
individual, group and family psychotherapy.
Location-Based Services include an array of services that are facility or site-based, such as
Psychosocial Rehabilitation, Child and Adolescent Day Treatment, and SA Intensive Outpatient
Treatment.
Community-Based and Mobile Services include those services that are provided in home and
community settings such as Supported Employment, Peer Support and Community Guide
services.
Crisis Services include Respite, Facility-Based Crisis and Non-Hospital Detoxification services.
Inpatient Services include inpatient psychiatric care all ages
Specialized Services includes a specific list of services, most of which are residential treatment
services.
Geographic access and choice standards are specified for each category of service and vary
depending on the service category and funding source. The following table provides a summary of
DHHS requirements for each:
Medicaid State
Outpatient TWO (2) providers within 30
miles or 30 minutes
Choice of TWO (2) providers within
30 miles or 30 minutes
Location-Based Choice of TWO (2) providers
within 30 miles or 30 minutes
Access to ONE (1) provider within
30 miles or 30 minutes
Community / Mobile Choice of TWO (2) providers
within ABH catchment area
Access to ONE (1) provider within
ABH catchment area
Crisis Access to ONE (1) provider within
ABH catchment area
Access to ONE (1) provider within
ABH catchment area
Inpatient Access to ONE (1) provider within
ABH catchment area
Access to ONE (1) provider within
ABH catchment area
Specialized Access to ONE (1) provider within
ABH catchment area
Access to ONE (1) provider within
ABH catchment area
For each category, service accessibility and provider choice were evaluated using a methodology
and report format determined by DHHS. The tables provided below include summary results of this
analysis as well as specific needs and gaps identified through the community survey, as described in
Section One.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 19
I. Outpatient Services
A. Medicaid and State-funded outpatient services access and choice standard
All eligible individuals must have a choice of two different outpatient services provider agencies
within 30 miles or 30 minutes (45 miles or 45 minutes in rural counties) of their residences.
Outpatient behavioral health services can include psychiatric and biopsychosocial assessment,
medication management, individual, group, and family therapies, psychotherapy for crisis, and
psychological testing. Tables below were completed for outpatient services as one group, using
geomapping software to calculate the number and percentages of individuals with choice:
Medicaid State-Funded
Categories
# of enrollees
with choice of
two providers
within 30/45
miles*
# of
Medicaid
Enrollees
%
# of consumers
with choice of
two providers
within 30/45
miles*
# of
Consumer
s
%
Reside in urban counties 221,145 221,145 100 17,356 17,356 100
Reside in rural counties n/a n/a n/a n/a n/a n/a
Total (standard = 100%) 221,145 221,145 100 17,356 17,356 100
Adults (age 18+) 81,794 81,794 100 15,893 15,893 100
Children (age 17 and
younger) 139,351 139,351 100 1,463 1,463 100
Total (standard = 100%) 221,145 221,145 100 17,356 17,356 100
*”30/45 miles” is the abbreviated term used in this document for individuals having choice within 30 miles or 30 minutes (45 miles or 45 minutes in rural counties) of their residences.
Medicaid State-Funded
If not at 100%, has an exception been requested but not yet finalized? n/a. If no, briefly explain and give date it will be requested:
If not at 100%, has written justification and a plan to meet needs been submitted? n/a. If no, briefly explain and give date it will be submitted:
If not at 100%, is an exception to the standard in place? n/a If no, briefly explain: n/a
If not at 100%, are written justification and a plan to meet needs in place? n/a attach copy to this report. If no, briefly explain: n/a
Effective date of exception approval: n/a Effective date of written justification and plan approval: n/a
Next exception review date, if applicable: n/a Next review date, if applicable: n/a
B. What outpatient service gaps were identified by consumers and family members?
Services to support development and implementation of behavior plans
Increased community awareness and education for consumers and families
Development of service to address gap between outpatient and enhanced benefit services and need for case management

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 20
C. What outpatient service gaps were identified by other stakeholders?
Need for increased community awareness and education for consumers and families
Enhanced access to an effective comprehensive continuum of care for individuals with substance use disorders
D. What specific geographic, cultural or demographic groups experience outpatient services gaps
that need to be addressed? Describe gaps and how the information was gathered.
Elderly, non-English speaking (primarily Spanish language), individuals with co-occurring IDD and mental illness, youth engaged in sexual harm, individuals with substance use disorders, LGBTQ populations and individuals with traumatic brain injuries. Underserved populations were identified through the community survey and feedback from consumer, stakeholder, provider and staff workgroups. A summary of findings regarding underserved populations and detailed feedback regarding needs and gaps is available in Appendix D.
E. Goals, strategies and timelines for addressing outpatient services gaps identified in I.A., I.B., I.C.
and I.D. Briefly identify the service gap, goal and target date for reducing or eliminating the gap,
and strategies planned or in progress to achieve the goal.
Medicaid
Service Gap Goal and Target Date Strategies to achieve goal,
noting if planned or in progress
Services to support development and implementation of behavior plans
Conduct further evaluation by 6/30/16 to determine if this area remains a gap and needs to be included in FY17 Network Development Plan.
Include in FY17 Network Development Plan If gap remains as of 6/30/16.
Development of service to address gap between outpatient and enhanced benefit services and need for case management
FY16 Network Development Plan objective in progress, with expected completion by 6/30/16
Implementation of new Medicaid service definition for enhanced outpatient services.
Increased community awareness and education for consumers and families
This is an ongoing goal of the Alliance Community Awareness Campaign, which focuses on increasing community awareness of behavioral health conditions, services and how to access care.
Alliance has an ongoing public awareness campaign and multiple collaborative efforts with community partners that focus on addressing this gap.
Service access for underserved populations such as elderly, non-English speaking and other identified populations.
Conduct further evaluation by 6/30/16 to identify extent to which populations are underserved and to clarify priorities for inclusion in FY17 Network Development Plan.
Incorporate findings of evaluation into FY17 Network Development Plan goals.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 21
State-Funded
Service Gap Goal and Target Date Strategies to achieve goal,
noting if planned or in progress
Increased community awareness and education for consumers and families
See above See above
Service access for underserved populations such as elderly, non-English speaking and other identified populations.
See above See above
II. Location-Based Services
A. 1. Medicaid location-based services access and choice standard: All eligible individuals must
have a choice of two different provider agencies for each location-based service in the chart
below within 30 miles or 30 minutes (45 miles or 45 minutes in rural counties) of their residences.
2. State-funded location-based services access and choice standard: All eligible individuals have
access to at least one provider agency for each location-based service in the chart below within
30 miles or 30 minutes (45 miles or 45 minutes in rural counties) of their residences.
Medicaid State-Funded
Service
# and % of enrollees with
choice of two providers
within 30/45 miles of their
residences
Total # of
Medicaid
Enrollees
# and % of consumers with
at least one provider within
30/45 miles of their
residences
Total # of
Consumers
# % # %
Psychosocial
Rehabilitation 81,794 100 81,794 8,986 82.56 10,884
Child and Adolescent
Day Treatment 139,215 99.90 139,351 986 90.21 1,093
SA Comprehensive
Outpatient Treatment
Program
221,145 100 221,145 3,846
100
3,886
SA Intensive Outpatient
Program 221,145 100 221,145 3,886 100 3,886
Opioid Treatment 56,743 68.53 81,794 2,847 66.61 3,824
Day Supports 221,145 100 221,145
Adult Developmental
Vocational Program 1,528 100 1,528

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 22
Medicaid State-Funded
If not at 100%, have exceptions been requested but not yet finalized? Yes. If no, briefly explain and give dates each will be requested: n/a
If not at 100%, have written justifications and plans to meet needs been submitted? Yes
If no, briefly explain and give dates each will be submitted: n/a
If not at 100%, are exceptions to the standard in place? Yes
Please list: Waiver of provider choice has been approved by DMA; developed new service definition modifier for Medication-Assisted Treatment that will be used to expand access to opioid treatment. We will resubmit waiver request to DMA for FY17. If no, briefly explain: n/a
If not at 100%, are written justifications and plans to meet needs in place? Yes Attach copy to this report. If no, briefly explain See Appendix E
Effective dates of each exception approval: 9/22/15 Effective date of each written justification and plan approval: 3/27/15
Next review dates for each exception, if applicable: n/a Next review dates, if applicable: n/a
B. What location-based services gaps were identified by consumers and family members?
Improve service accessibility, including:
Expansion of same day access
Psychiatry availability
Transportation options
C. What location-based services gaps were identified by other stakeholders?
Improve access to short-term daily structured programs to support behavioral and emotional stability
(e.g., Day Treatment, Partial Hospitalization)
Enhanced access to an effective and comprehensive continuum of care for individuals with
substance use disorders
Improved quality and effectiveness of psychosocial rehabilitation
D. What specific geographic, cultural or demographic groups experience gaps in the location-based
services above that need to be addressed? Describe gaps and how the information was
gathered.
Elderly, non-English speaking (primarily Spanish language), individuals with co-occurring IDD and
mental illness, youth engaged in sexual harm, individuals with substance use disorders, LGBTQ
populations and individuals with traumatic brain injuries.
Underserved populations were identified through the community survey and feedback from consumer,
stakeholder, provider and staff workgroups. A summary of findings regarding underserved
populations and detailed feedback regarding needs and gaps is available in Appendix D.
E. Goals, strategies and timelines for addressing location-based services gaps identified in II.A, II.B.,
II.C. and II.D. Briefly identify the service gap, goal and target date for reducing or eliminating the
gap, and strategies planned or in progress to achieve the goal.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 23
Medicaid
Service Gap Goal and Target Date
Strategies to achieve goal,
noting if planned or in
progress
Child & Adolescent Day
Treatment
DMA has approved Medicaid Access
and Choice Waivers for this service.
Exploring opportunities for
collaboration with Cumberland
County schools regarding Day
Treatment plans.
Opioid Treatment
Addressed in FY16 Network
Development Plan. Developed new
service definition modifier for
Medication Assisted Treatment with
Buprenorphine with plans to
implement by 6/30/16.
Continued goal for FY17
Network Development Plan.
Improved accessibility of
outpatient psychiatric
services and same-day
intake appointments
Develop plan and timeframes for
addressing in FY17 Network
Development Plan by 6/30/16.
FY17 Network Development
Plan will include specific plans
for development of Behavioral
Health Urgent Care.
Access to short-term daily
structured programs such as
Day Treatment and Partial
Hospitalization
May be addressed by current plans
and initiatives. Conduct further
evaluation by 6/30/16 to identify
extent to which this area remains a
gap and needs to be included in FY17
Network Development Plan.
Include in FY17 Network
Development Plan If gap
remains as of 6/30/16.
Enhanced access to an
effective and
comprehensive continuum
of care for individuals with
substance use disorders
Develop plan and timeframes for
addressing in FY17 Network
Development Plan by 6/30/16
FY17 Network Development
Plan will include specific plans
for evaluation of barriers and
strategies for addressing this
gap.
Improved quality and
effectiveness of
psychosocial rehabilitation
FY16 Network Development Plan
objective in progress, evaluating PSR
models and preparing
recommendations for further
development, with expected
completion by 6/30/16
Continued goal for FY17
Network Development Plan.
Service access for
underserved populations
such as elderly, non-English
speaking and other
identified populations.
Conduct further evaluation by 6/30/16
to identify extent to which populations
are underserved and to clarify
priorities for inclusion in FY17
Network Development Plan.
Incorporate findings of
evaluation into FY17 Network
Development Plan goals.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 24
State-Funded
Service Gap Goal and Target Date
Strategies to achieve goal,
noting if planned or in
progress
Psychosocial Rehabilitation
(no provider in Cumberland
with State contract)
Resolved: added contract with PSR
provider in Cumberland County. Completed
Child & Adolescent Day
Treatment (Cumberland)
Requests for services will be handled
through single-case agreements or
contracts with existing providers if
necessary. We will request
continuation of DMH waiver for FY17.
Exploring opportunities for
collaboration with Cumberland
County schools regarding Day
Treatment plans.
Service access for
underserved populations
such as elderly, non-English
speaking and other
identified populations.
See above See above
III. Community/Mobile Services
A. 1. Medicaid community/mobile services access and choice standard: All eligible individuals must
have a choice of two provider agencies for each community/mobile service in the chart below
within the LME-MCO catchment area.
2. State-funded community/mobile services access and choice standard: All eligible individuals
have access to at least one provider agency for each community/mobile service in the chart
below within the LME-MCO catchment area.
Medicaid State-Funded
Service
# and % of enrollees with
choice of two provider
agencies within the LME-
MCO catchment area
Total #
of
Medicaid
Enrollee
s
# and % of consumers with
access to at least one provider
agency within the LME-MCO
catchment area
Total # of
Consume
rs
# % # %
Assertive Community Treatment Team
81,794 100 81,794 10,884 100 10,884
Community Support Team
81,794 100 81,794 14,725 100 14,725
Intensive In-Home 139,351 100 139,35
1 1,093 100 1,093
Mobile Crisis 221,145 100 221,14
5 17,356 100 17,356
Multi-systemic Therapy 139,351 100 139,35
1 1,093 100 1,093
Home-based I/DD
Services 221,145 100
221,14
5

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 25
Medicaid State-Funded
Service
# and % of enrollees with
choice of two provider
agencies within the LME-
MCO catchment area
Total #
of
Medicaid
Enrollee
s
# and % of consumers with
access to at least one provider
agency within the LME-MCO
catchment area
Total # of
Consume
rs
# % # %
(b)(3) MH/SA
Supported Employment
Services
221,145 100 221,14
5
(b)(3) I/DD MH/SA
Supported Employment
Services
221,145 100 221,14
5
(b)(3) Waiver
Community Guide
221,145 100 221,14
5
(b)(3) Waiver Individual
Support (Personal
Care)
221,145 100
221,14
5
(b)(3) Waiver Peer
Support
221,145 100 221,14
5
(b)(3) Waiver Respite
221,145 100 221,14
5
I/DD Supported
Employment Services
(Innovations)
221,145 100 221,14
5
I/DD Supported
Employment Services
(State-funded)
1,528 100 1,528
MH/SA Supported
Employment Services
(IPS-SE) (State-funded)
14,725 100 14,725
Developmental
Therapies (State-
funded)
1,528 100 1,528
Medicaid State-Funded
If not at 100%, have exceptions been requested but not yet finalized? n/a If no, briefly explain and give dates each will be requested: n/a
If not at 100%, have written justifications and plans to meet needs been submitted? n/a
If no, briefly explain and give dates each will be submitted: _ n/a
If not at 100%, are exceptions to the standard in place? n/a Please list. If no, briefly explain: n/a
If not at 100%, are written justifications and plans to meet needs in place? n/a attach copy to this report. If no, briefly explain n/a
Effective dates of each exception approval: n/a Effective date of each written justification and plan approval: n/a
Next review date of each exception, if applicable: n/a Next review dates, if applicable: n/a

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 26
B. What community/mobile services gaps were identified by consumers and family members?
Improved availability of services to assist with vocational and educational needs
Improved access to services to provide relief to primary caretakers (Respite, Crisis respite, emergency
and planned respite)
Improved quality and accessibility of community-based intensive treatment services (e.g., Community
Support Team, Assertive Community Treatment Team), especially for uninsured
C. What community/mobile services gaps were identified by other stakeholders?
Improved availability of services to assist with vocational and educational needs
Enhanced quality of mobile crisis and capacity for to serve children and dually diagnosed IDD/MH
population
D. What specific geographic, cultural or demographic groups experience gaps in the
community/mobile services above that need to be addressed? Describe gaps and how the
information was gathered.
Elderly, non-English speaking (primarily Spanish language), individuals with co-occurring IDD and
mental illness, youth engaged in sexual harm, individuals with substance use disorders, LGBTQ
populations and individuals with traumatic brain injuries.
Underserved populations were identified through the community survey and feedback from consumer,
stakeholder, provider and staff workgroups. A summary of findings regarding underserved populations
and detailed feedback regarding needs and gaps is available in Appendix D.
E. Goals, strategies and timelines for addressing community/mobile services gaps identified in III.A.,
III.B., III.C. and III.D. Briefly identify the service gap, goal and target date for reducing or
eliminating the gap, and strategies planned or in progress to achieve the goal.
Medicaid
Service Gap Goal and Target Date Strategies to achieve goal,
noting if planned or in progress
Improved access to services to provide relief to primary caretakers (Respite, Crisis respite, emergency and planned respite)
Develop plan and timeframes for continuing this goal in FY17 Network Development Plan by 6/30/16.
This objective will continue in FY17 Network Development Plan.
Improved availability of services to assist with vocational and educational needs
FY16 Network Development Plan objectives in progress related to Supported Employment and consumer-operated businesses, with expected completion by 6/30/16.
Develop plan and timeframes by 6/30/16 for continuing this goal in FY17 Network Development Plan
This objective will continue in FY17 Network Development Plan.
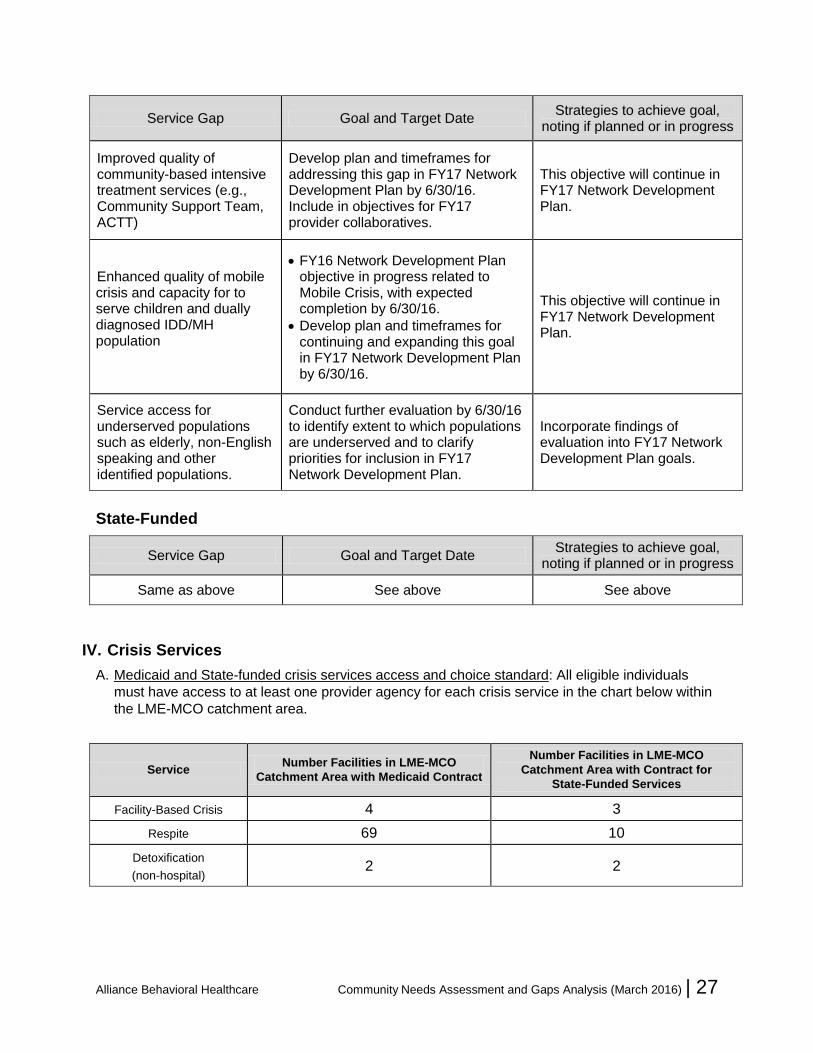
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 27
Service Gap Goal and Target Date Strategies to achieve goal,
noting if planned or in progress
Improved quality of community-based intensive treatment services (e.g., Community Support Team, ACTT)
Develop plan and timeframes for addressing this gap in FY17 Network Development Plan by 6/30/16. Include in objectives for FY17 provider collaboratives.
This objective will continue in FY17 Network Development Plan.
Enhanced quality of mobile crisis and capacity for to serve children and dually diagnosed IDD/MH population
FY16 Network Development Plan objective in progress related to Mobile Crisis, with expected completion by 6/30/16.
Develop plan and timeframes for continuing and expanding this goal in FY17 Network Development Plan by 6/30/16.
This objective will continue in FY17 Network Development Plan.
Service access for underserved populations such as elderly, non-English speaking and other identified populations.
Conduct further evaluation by 6/30/16 to identify extent to which populations are underserved and to clarify priorities for inclusion in FY17 Network Development Plan.
Incorporate findings of evaluation into FY17 Network Development Plan goals.
State-Funded
Service Gap Goal and Target Date Strategies to achieve goal,
noting if planned or in progress
Same as above See above See above
IV. Crisis Services
A. Medicaid and State-funded crisis services access and choice standard: All eligible individuals
must have access to at least one provider agency for each crisis service in the chart below within
the LME-MCO catchment area.
Service Number Facilities in LME-MCO
Catchment Area with Medicaid Contract
Number Facilities in LME-MCO
Catchment Area with Contract for
State-Funded Services
Facility-Based Crisis 4 3
Respite 69 10
Detoxification
(non-hospital) 2 2
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 28
Medicaid State-Funded
If standard not met, have exceptions been requested but not yet finalized? n/a . If no, briefly explain and give dates each will be requested: n/a
If standard not met, have written justifications and plans to meet needs been submitted? n/a
If no, briefly explain and give dates each will be submitted: n/a
If standard not met, are exceptions to the standard in place? n/a If no, briefly explain: n/a
If standard not met, are written justifications and plans to meet needs in place? n/a; attach copy to this report. If no, briefly explain n/a
Effective dates of each exception approval: n/a Effective date of each written justification and plan approval: n/a
Next review dates, if applicable: n/a Next review dates, if applicable: n/a
B. What crisis services gaps were identified by consumers and family members?
Expanded crisis continuum, including access to respite and crisis respite services
Enhanced access to an effective comprehensive continuum of care for individuals with substance use disorders
C. What crisis services gaps were identified by other stakeholders?
Need for an expanded crisis continuum, including access to respite and crisis respite services
D. What specific geographic, cultural or demographic groups experience gaps in the crisis services
above that need to be addressed? Describe gaps and how the information was gathered.
Elderly, non-English speaking (primarily Spanish language), individuals with co-occurring IDD and mental illness, youth engaged in sexual harm, individuals with substance use disorders, LGBTQ populations and individuals with traumatic brain injuries.
Underserved populations were identified through the community survey and feedback from consumer, stakeholder, provider and staff workgroups. A summary of findings regarding underserved populations and detailed feedback regarding needs and gaps is available in Appendix D.
E. Goals, strategies and timelines for addressing crisis services gaps identified in IV.A., IV.B., IV.C.
and IV.D. Briefly identify the service gap, goal and target date for reducing or eliminating the gap,
and strategies planned or in progress to achieve the goal.
Medicaid
Service Gap Goal and Target Date Strategies to achieve goal,
noting if planned or in progress
Expanded crisis continuum,
including access to respite
and crisis respite services
Develop plan and timeframes for addressing in FY17 Network Development Plan by 6/30/16
FY17 Network Development Plan will include specific plans for evaluation of barriers and strategies for addressing this gap.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 29
Enhanced access to an effective comprehensive continuum of care for individuals with substance use disorders
Develop plan and timeframes for addressing in FY17 Network Development Plan by 6/30/16
FY17 Network Development Plan will include specific plans for evaluation of barriers and strategies for addressing this gap.
Service access for underserved populations such as elderly, non-English speaking and other identified populations.
Conduct further evaluation by 6/30/16 to identify extent to which populations are underserved and to clarify priorities for inclusion in FY17 Network Development Plan.
Incorporate findings of evaluation into FY17 Network Development Plan goals.
State-Funded
Service Gap Goal and Target Date Strategies to achieve goal,
noting if planned or in progress
Same as above See above See above
V. Inpatient Services
A. Medicaid and State-funded inpatient services access and choice standard: All eligible individuals
must have access to at least one inpatient provider agency listed in the chart below within the
LME-MCO catchment area.
Service Number Facilities in LME-MCO
Catchment Area with Medicaid
Contract
Number Facilities in LME-MCO
Catchment Area with Contract for
State-Funded Services
Inpatient Hospital – Adult
a. Acute care hospitals with adult inpatient psychiatric bed
b. Other hospitals with adult inpatient psychiatric beds
c. Acute care hospitals with adult inpatient substance use beds
d. Other hospitals with adult inpatient substance use beds
4 3
3 2
1 1
1 1
Inpatient Hospital – Adolescent
a. Acute care hospitals with adolescent inpatient psychiatric beds
b. Other hospitals with adolescent inpatient psychiatric beds
c. Acute care hospitals with adolescent inpatient substance use beds
d. Other hospitals with adolescent inpatient substance use beds
0 0
2 1
0 0
0 0
Inpatient Hospital – Child
a. Acute care hospitals with child inpatient psychiatric beds
b. Other hospitals with child inpatient psychiatric beds
0 0
2 1

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 30
Medicaid State-Funded
If standard not met, have exceptions been requested but not yet finalized? n/a . If no, briefly explain and give dates each will be requested: n/a
If standard not met, have written justifications and plans to meet needs been submitted? n/a
If no, briefly explain and give dates each will be submitted: n/a
If standard not met, are exceptions to the standard in place? n/a If no, briefly explain: n/a
If standard not met, are written justifications and plans to meet needs in place? n/a ; attach copy to this report. If no, briefly explain n/a
Effective dates of each exception approval: n/a Effective date of each written justification and plan approval: n/a
Next review dates of each exception, if applicable: n/a Next review dates, if applicable: n/a
B. What inpatient services gaps were identified by consumers and family members?
Inpatient psychiatric treatment for dually diagnosed IDD/MI
C. What inpatient services gaps were identified by other stakeholders?
Lack of inpatient psychiatric beds (both short-term and long-term) for MI and SA
D. What specific geographic, cultural or demographic groups experience gaps in the inpatient
services above that need to be addressed? Describe gaps and how the information was
gathered.
Elderly, non-English speaking (primarily Spanish language), individuals with co-occurring IDD and mental illness, youth engaged in sexual harm, individuals with substance use disorders, LGBTQ populations and individuals with traumatic brain injuries.
Underserved populations were identified through the community survey and feedback from consumer, stakeholder, provider and staff workgroups. A summary of findings regarding underserved populations and detailed feedback regarding needs and gaps is available in Appendix D.
E. Goals, strategies and timelines for addressing inpatient services gaps identified in V.A., V.B., V.C.
and V.D. Briefly identify the service gap, goal and target date for reducing or eliminating the gap,
and strategies planned or in progress to achieve the goal.
Medicaid
Service Gap Goal and Target Date Strategies to achieve goal, noting
if planned or in progress
Lack of inpatient psychiatric beds (both short-term and long-term) for MI and SA
This item reflects statewide service needs and gaps that will require ongoing planning efforts.
Address through participation in statewide advocacy, development and strategic planning efforts.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 31
Inpatient for dually diagnosed IDD/MI
Goal for this area will be to evaluate options for decreasing inpatient utilization and development of appropriate alternatives to inpatient care.
Develop plan and timeframes for addressing in FY17 Network Development Plan by 6/30/16
FY17 Network Development Plan will include specific plans for evaluation of barriers and strategies for addressing this gap.
Service access for underserved populations such as elderly, non-English speaking and other identified populations.
Conduct further evaluation by 6/30/16 to identify extent to which populations are underserved and to clarify priorities for inclusion in FY17 Network Development Plan.
Incorporate findings of evaluation into FY17 Network Development Plan goals.
State-Funded
Service Gap Goal and Target Date Strategies to achieve goal, noting
if planned or in progress
Same as above See above See above
VI. Specialized Services
A. Medicaid and State-funded specialized services access and choice standard: All individuals
eligible for the services below must have access to at least one provider agency.
A chart is available in Appendix B with a listing of Medicaid and State-funded specialized
services that Alliance contracts with, by county served. The following table provides a list of
Specialized Services and whether there is availability of services in the Alliance catchment area:
Service Medicaid State
Partial Hospitalization No No
MH Group Homes N/A Yes
Psychiatric Residential Treatment Facility Yes N/A
Residential Treatment Levels 1-4 Yes N/A
Child MH Out-of-Home Respite Yes N/A
SA Non-Medical Community Residential Treatment Yes Yes
SA Medically Monitored Community Residential Treatment
Yes Yes
SA Halfway Houses N/A Yes
I/DD Group Homes and AFLs Yes N/A
I/DD Out-of-Home Respite Yes N/A
I/DD Facility-Based Respite Yes N/A
Intermediate Care Facility/IDD Yes N/A

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 32
B. What specialized services gaps were identified by consumers and family members?
ICF/IDD
Short-term daily structured programs to support behavioral and emotional stability (e.g. Partial
Hospitalization
C. What specialized services gaps were identified by other stakeholders?
Effective residential treatment options, including short-term residential treatment for substance abuse,
transitional living, half-way houses, and housing with supports
Therapeutic secure residential treatment for children and adolescents (e.g., Psychiatric Residential
Treatment Facility (PRTF) and Level IV residential treatment)
Improved access and quality of residential options such as Group Living, Supervised Living,
Residential Supports, and Semi- and/or independent living
D. What specific geographic, cultural or demographic groups experience gaps in the specialized
services above that need to be addressed? Describe gaps and how the information was
gathered.
Elderly, non-English speaking (primarily Spanish language), individuals with co-occurring IDD and
mental illness, youth engaged in sexual harm, individuals with substance use disorders, LGBTQ
populations and individuals with traumatic brain injuries.
Underserved populations were identified through the community survey and feedback from consumer,
stakeholder, provider and staff workgroups. A summary of findings regarding underserved populations
and detailed feedback regarding needs and gaps is available in Appendix D.
E. Goals, strategies and timelines for addressing specialized services gaps identified in VI.A., VI.B.,
VI.C. and VI.D. Briefly identify the service gap, goal and target date for reducing or eliminating the
gap, and strategies planned or in progress to achieve the goal.
Medicaid
Service Gap Goal and Target Date Strategies to achieve goal,
noting if planned or in progress
Partial Hospitalization This gap will be resolved by 6/30/16 by addition of provider contracts.
N/A
Service access for underserved populations such as elderly, non-English speaking and other identified populations.
Conduct further evaluation by 6/30/16 to identify extent to which populations are underserved and to clarify priorities for inclusion in FY17 Network Development Plan.
Incorporate findings of evaluation into FY17 Network Development Plan goals.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 33
State-Funded
Service Gap Goal and Target Date Strategies to achieve goal,
noting if planned or in progress
Effective residential
treatment options and
supports
Completed comprehensive evaluation of residential continuum and development of Alliance Housing Plan.
Housing and residential treatment needs and gaps will be addressed through the Housing Plan.
New Director of Housing position will provide leadership for implementation of housing plan initiatives, pending availability of funds.
Therapeutic secure
residential treatment
(Psychiatric Residential
Treatment Facility (PRTF),
Level IV)
Goal for this area will be to evaluate options for decreasing out of home placement
Develop plan and timeframes for addressing in FY17 Network Development Plan by 6/30/16
See above
Service access for underserved populations such as elderly, non-English speaking and other identified populations.
See above See above
VII. State-Funded Services Items
The following two items apply to services referenced in:
State-Funded Enhanced Mental Health and Substance Abuse Services 2015 effective 8/1/15
State-Funded ACT Policy
State-Funded DMHDDSAS Service Definitions 2003-2014 effective 8/1/14
Individual Supportive Employment with Long-Term Vocational Supports YP630/YM645
For additional information, see http://www.ncdhhs.gov/providers/provider-info/mental-health/service-definitions. A. For State-funded services, describe any geographic discrepancies in services included in the
LME-MCO’s local Benefit Plan. That is, are residents of some counties excluded from coverage
under the LME-MCO benefit plan, or have stricter eligibility requirements? Include which services,
why this occurred, and whether there is a plan in place to ensure equal access based on need
across all geographic areas.
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 34
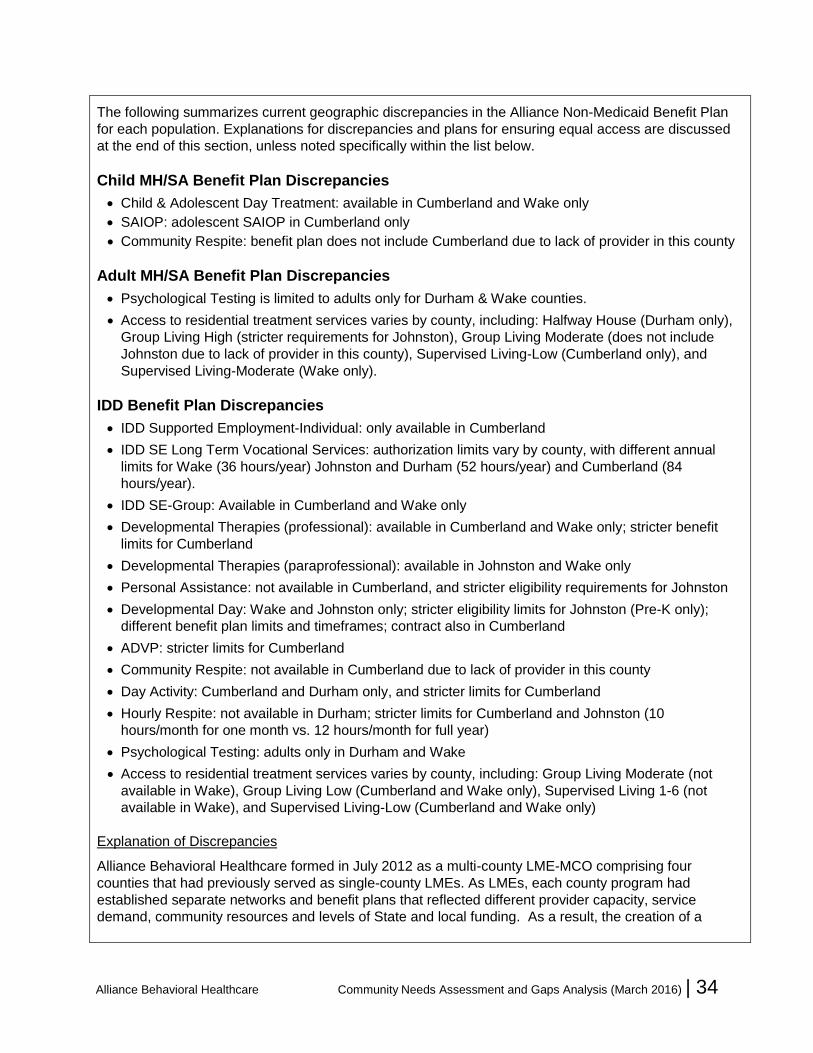
The following summarizes current geographic discrepancies in the Alliance Non-Medicaid Benefit Plan
for each population. Explanations for discrepancies and plans for ensuring equal access are discussed
at the end of this section, unless noted specifically within the list below.
Child MH/SA Benefit Plan Discrepancies
Child & Adolescent Day Treatment: available in Cumberland and Wake only
SAIOP: adolescent SAIOP in Cumberland only
Community Respite: benefit plan does not include Cumberland due to lack of provider in this county
Adult MH/SA Benefit Plan Discrepancies
Psychological Testing is limited to adults only for Durham & Wake counties.
Access to residential treatment services varies by county, including: Halfway House (Durham only),
Group Living High (stricter requirements for Johnston), Group Living Moderate (does not include
Johnston due to lack of provider in this county), Supervised Living-Low (Cumberland only), and
Supervised Living-Moderate (Wake only).
IDD Benefit Plan Discrepancies
IDD Supported Employment-Individual: only available in Cumberland
IDD SE Long Term Vocational Services: authorization limits vary by county, with different annual
limits for Wake (36 hours/year) Johnston and Durham (52 hours/year) and Cumberland (84
hours/year).
IDD SE-Group: Available in Cumberland and Wake only
Developmental Therapies (professional): available in Cumberland and Wake only; stricter benefit
limits for Cumberland
Developmental Therapies (paraprofessional): available in Johnston and Wake only
Personal Assistance: not available in Cumberland, and stricter eligibility requirements for Johnston
Developmental Day: Wake and Johnston only; stricter eligibility limits for Johnston (Pre-K only);
different benefit plan limits and timeframes; contract also in Cumberland
ADVP: stricter limits for Cumberland
Community Respite: not available in Cumberland due to lack of provider in this county
Day Activity: Cumberland and Durham only, and stricter limits for Cumberland
Hourly Respite: not available in Durham; stricter limits for Cumberland and Johnston (10
hours/month for one month vs. 12 hours/month for full year)
Psychological Testing: adults only in Durham and Wake
Access to residential treatment services varies by county, including: Group Living Moderate (not
available in Wake), Group Living Low (Cumberland and Wake only), Supervised Living 1-6 (not
available in Wake), and Supervised Living-Low (Cumberland and Wake only)
Explanation of Discrepancies
Alliance Behavioral Healthcare formed in July 2012 as a multi-county LME-MCO comprising four
counties that had previously served as single-county LMEs. As LMEs, each county program had
established separate networks and benefit plans that reflected different provider capacity, service
demand, community resources and levels of State and local funding. As a result, the creation of a

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 35
unified Non-Medicaid benefit plan resulted in geographic discrepancies that have been partially but not
completely resolved. Alliance has adjusted the benefit plan to achieve consistency when possible, but
some adjustments will require either additional State funding or service reductions, which require planful
consideration of impact on communities and consumers.
Plans to Ensure Equal Access
As reflected in the FY16 Network Development Plan, Alliance has prioritized the revision of its Non-
Medicaid Benefit Plan to improve geographic consistency, and we will continue to address discrepancies
in the upcoming fiscal year when possible. This issue will be discussed with the Alliance Board in the
budget planning process for FY17, but will be impacted significantly by any reductions in State
MH/IDD/SA funding.
B. For State-funded services, describe any services that were closed to new admissions or not
offered during the year. Include which services, why this occurred, the period of time, and how the
LME-MCO ensured priority populations continued to access appropriate levels of care.
Services were closed to new admissions for consumers in Durham for ADVP and Personal Assistance.
See above for an explanation of reasons for this discrepancy and Alliance plans for addressing in the
upcoming fiscal year.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 36
Section Three
GeoAccess Maps
For each of the Location-Based and Community/Mobile services, geographic access was evaluated using specialized software that calculated identified the location of both consumers and
providers to evaluate whether services are accessible within a 30-mile radius. Separate approaches
were used for Medicaid and State-funded services:
For Medicaid-funded services, accessibility was determined by using the addresses of all
Medicaid recipients for the Alliance catchment area from July 1, 2014 through June 30, 2015.
For State-funded services, addresses were used for individuals who received State-funded
services between July 1, 2014 and June 30, 2015.
For both Medicaid and State-funded services, accessibility calculations were based only on
those who met the age/disability requirements for the service being evaluated. For example,
Child and Adolescent Day Treatment access was evaluated based on Medicaid-eligible or
uninsured children and adolescents.
As required by DHHS, geographic access maps are provided (See Appendix A) for services where
less than 90% of consumers have the required access and/or choice. The following services did not
meet the 90% benchmark:
Psychosocial Rehabilitation (State): 82.6%
Opioid Treatment (Medicaid): 68.5%
Opioid Treatment (State): 66.6%
As noted in Section Two, the following actions have been taken to address accessibility gaps for
these services:
Psychosocial Rehabilitation (State)
This gap was noted for FY15 due to the lack of a State-funded provider in Cumberland County. This
gap has been addressed by addition of a contract for PSR in Cumberland County.
Opioid Treatment (Medicaid and State)
This area has been an identified goal for the FY16 Network Development Plan, which has led to the
development of a Medicaid service definition modifier to expand access to Medication-Assisted
Treatment in all counties. This area will remain as a priority in the FY17 Network Development Plan.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 37
Section Four
Departmental (DHHS) Initiatives
The NC Department of Health and Human Services (DHHS) has established seven priority initiatives
for MCOs for the past year. The following section provides an update on the status of each initiative,
including goals, actions taken, accomplishments and plans for further development.
Recovery-Oriented System of Care
Through our strategic planning process, Alliance Behavioral Healthcare began an initiative to
develop a transformation plan to help shift the paradigm towards a recovery oriented system of care
in our communities. Operating a managed care organization within a recovery oriented system of
care is the right thing to do, and is the most cost effective way to manage our behavioral healthcare
costs. This organization has already taken many steps toward implementing recommendations
identified in this planning process. It is recognized that changing a system is not a quick or easy
task, however Alliance remains committed to move forward to establish a system that honors the
people it serves, believes and invests in their ability to live a life of quality, meaning and purpose,
and treats people with dignity and respect. Below is a strategic framework that is being utilized to
implement the recommendations made by our cross departmental initiative team.
Strategic Framework
Establish a Recovery and Self-Determination steering committee to oversee this transformation.
(Include at least 1 member of the Executive Leadership Team)
Adopt the guiding principles for recovery and self-determination outlined in this document
Develop a Recovery Education Institute to offer additional training to our staff, providers,
consumers and families, and other community partners
Align our policies and procedures with a recovery-oriented system of care
Put “teeth” in our contracts and align outcomes in our contracts with a recovery oriented system
of care
Consider all of our service array recommendations as well as other evidence-based and
emerging best practice models
Include consumers and families in the transformation process
Utilize effective Peer Support Services and family partners
Fund consumer operated services throughout our catchment area.
Invest in the future of this organization and our communities by funding this transformation
process appropriately
Additional actions taken include:
Implementation of a peer recovery based program in our Durham Crisis facility, the Durham
Recovery Response Center.
Development of a white paper outlining our commitment to implementing a Recovery-Oriented
System of Care and convened a workgroup of diverse and interested employees to implement
the vision.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 38
Training for providers focused on improvement in the quality of Person-Centered Plans (PCPs),
particularly in health and safety elements, the comprehensive crisis plan, and individualization
of goals and interventions.
Crisis Solutions Initiative
Alliance is an active participant in initiatives focused on improving accessibility, quality and
performance of the crisis system. We have established crisis collaboratives in Cumberland, Durham
and Wake counties that include representation from multiple community stakeholders such as
hospitals, crisis centers, law enforcement, judicial system, providers, paramedics and others.
Alliance has also responded to three Crisis Solutions Initiative funding opportunities from DMH and
has been awarded grants that resulted in the following:
Implemented First Episode Psychosis Clinic to expand identification and treatment of first
episode psychosis for youth and young adults in Wake County.
Established Critical Time Intervention program in Cumberland County to provide evidence-
based jail post-release services that target more effective engagement and treatment for
individuals with mental illness and substance use disorders who have been released from the
Cumberland County jail. Developed Medicaid alternative service definition with plans for
implementation in FY17.
The Community Paramedicine grant has assisted in development of policies and procedures
related to advanced paramedicine in Durham County and MH/SA training in preparation for
designating alternative drop-off locations other than hospital emergency departments.
We have implemented a peer recovery based program in our Durham Crisis facility, the Durham
Recovery Response Center, and we are locating a second facility for Wake that will use a peer
recovery approach as well. We are drafting the Rapid Response definition to improve crisis
response for youth and plan to submit to DMA be approved as a Medicaid Alternative Service.
Crisis Services QIP – Alliance identified opportunities for improvement in crisis services,
particularly in Wake and Cumberland Counties, due to the regular overcapacity of the Wake
County crisis facility in the evenings and high rate of Emergency Department use primarily for
psychiatric reasons in Cumberland. Alliance is expanding the availability of Tier II services after
regular business hours in Wake County and evidence-based, intensive services for youth in
Cumberland County.
Additional Tier IV facility – Due to the rapid population expansion in the state’s largest county,
Alliance identified resources and issued an RFP for an additional Tier IV in Wake County. The
contract has been awarded and the provider is identifying potential sites in the highest need
location based on data from Alliance’s geo-access mapping.
Advancing Technology
Over the past year Alliance has partnered with Night Owl and Simply Home to provide several family
and consumer education sessions regarding the availability of independence enabling technology
that can be provided under the Innovations Waiver. The sessions allowed individuals to learn about
technology and how technology and professional and natural supports can be combined to enhance
and individuals’ ability to live safely and more independently in the community. A number of
consumers have elected to implement a range of technologies and are in the implementation
process, which consists of significant levels of person centered planning regarding the types of
devices and monitoring that will be implemented.
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 39
Additionally, Alliance is developing a technology enabled transition home that will be used to help
individuals and families learn to use independence enabling technology is a safe and closely
supervised home. The goal is that over time, direct staff oversight is faded until a consumer can
move into a their own home or apartment that has been outfitted with the technology devices and
monitoring can occur through either paid staff, natural supports or some combination.
Employment
Several FY16 Network Development Plan initiatives have addressed employment goals, including
continued implementation of evidence-based Supported Employment services and exploration of
models and supports for consumer-run businesses. Progress updates on these initiatives are
provided above on page 11.
Housing
Contracted with TAC to complete a study of the Alliance residential continuum.
Prepared Alliance Housing Plan per DHHS request
Housing Plan includes overview of current community-based housing initiatives, identified
needs relating to housing capacity and access to quality affordable permanent supportive
housing, wraparound services and supports needed to promote sustainable housing, and crisis
planning objectives for consumers
Alliance has created a new Director of Housing position to provide leadership for housing
initiatives
Current housing initiatives:
o Independent Living Initiative
o Transitions to Community Living Initiative
o Ready to Rent training: plan to expand to all counties
o Voucher and subsidized housing, including Section 8 Housing Choice Vouchers, Shelter
Plus Care
o Exploring further partnerships with public housing authorities
o Included housing allocation in Alliance savings reinvestment plan.
o Exploring Master Leasing agreements and piloting in Wake for TCLI
o Exploring financial incentives to developers
o Expanding wraparound services and supports
o Convening a Housing Learning Collaborative
o Training for providers on supportive housing
o Exploring expansion of key treatment services that support housing tenure
o Continued consultation with TAC and Corporation for Supportive Housing
Children’s Services
Implemented pilot programs, including Intercept, Enhanced Therapeutic Foster Care (E-TFC)
and Family-Centered Treatment (FCT) to expand the continuum of children’s’ services by
allowing additional intensive community based options for families. In addition, we have
submitted OPT+ for approval which will give youth and families a more intensive service
between OPT and IIHS, and we also are drafting a Medicaid alternative service definition for
Rapid Response, a crisis prevention and respite program, for implementation in all Alliance
counties.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 40
Intensive In-Home QIP – Alliance identified a need to improve outcomes and emotional well-
being of youth receiving Intensive In-Home services. Alliance has identified evidence-based
models, in collaboration with contracted providers, that will be the required modes of service
delivery. Providers have an opportunity to select the model to deliver and receive training,
subsidized by Alliance, no later than December 2016.
Implemented Therapeutic Foster Care Collaborative, with focus on implementation of evidence-
based interventions by therapeutic parents and development of a more trauma-informed
network of care.
Integration of Physical and Behavioral Health Care
Alliance has multiple initiatives that promote integration of behavioral health and medical care. We
believe this is a priority area for continued development and is consistent with research findings,
emerging evidence-based practices and identified community needs. We have recently established
and filled a new position, Director of Integrated Care, to promote and guide the development of
integrated care initiatives. Current initiatives include the following:
Conducted inventory of integrated care initiatives
Implemented multiple integrated care initiatives and hired consultant to conduct evaluation of
these pilot projects.
Wake County integrated care project with Turning Point Family Care, Urban Ministries and
Alliance Medical Ministry. Services include integrated, on-site, bilingual behavioral health
services at two agencies that serve the uninsured, many of whom speak Spanish.
Integrated care clinic operated by UNC Health Care on the WakeBrook campus that includes
crisis and assessment, facility-based crisis, non-hospital detoxification and inpatient psychiatric
services.
Alliance Care Coordinator located on-site at Duke.
Fellowship Health Resources is implementing the Dartmouth “In Shape” model within their PSR
program in Wake County. This program, funded by a combination of grant and Alliance
funding, provides health promotion and wellness activities for individuals with serious mental
illnesses.
Integration of Lincoln Community Health Center services at Durham Crisis and Assessment,
including assessments, lab work, medical examinations and follow-up treatment.
Duke Outpatient Clinic has received technical support to integrate behavioral health licensed
consultants into the practice. Implemented a set of routine mental health screening, workflows
and protocols to provide team based care to address total health needs within the practice.
Carolina Behavioral Care, in Partnership with the Duke Division of Community Health and
Northern Piedmont CCNC to integrate primary care services into their outpatient psychiatric
practice. Model includes an embedded nurse care manager who helps address consumers
overall needs.
Alliance is supporting efforts for the UNC ACTT team to receive primary care consultation and
for the ACTT Team medical staff to assist in the provision of primary care during routine client
visits.
Carolina Outreach has placed a behavioral health clinician within a large primary care Practice,
Eastover medical. The clinician provides consultation to primary care providers, brief
counseling and behavior change support to patients of the practice and coordinates referral to
and from the behavioral health system

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 41
Alliance will be expanding pilots to include an initiative with Southlight Healthcare to address
physical care gaps within their organization, including providing them with enhanced data
analytics to better manage their entire patient population. Additionally, Alliance is working with
a representatives for the IDD Council and local providers to pilot an IDD Health Home model.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 42
APPENDICES

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 43
Appendix A: Geographic Access Maps
The following maps are provided per funding source only for services where less than 90% of
consumers have the required access and/or choice:

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 44

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 45

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 46
Appendix B: Specialized Services
Specialized Service Provider Location(s) Funding Source
Child MH Out-of-Home Respite The Alpha Management Community Services,Inc. Durham State
Child MH Out-of-Home Respite Stan B Treatment Services Inc Johnston State
Child MH Out-of-Home Respite Lutheran Family Services in the Carolinas Wake State
Child MH Out-of-Home Respite National Mentor Healthcare, LLC Wake State
Child MH Out-of-Home Respite Pinnacle Family Services of North Carolina, LLC Wake State
I/DD Facility-Based Respite A Bridge to Learning Davidson Medicaid
I/DD Facility-Based Respite A Caring Heart Case Management, Inc. Johnston Medicaid
I/DD Facility-Based Respite A Small Miracle, Inc. Wake Medicaid
I/DD Facility-Based Respite A TOUCH OF GRACE INC Cumberland Medicaid
I/DD Facility-Based Respite Abilities Inc Lenoir Medicaid
I/DD Facility-Based Respite ACI SUPPORT SPECIALISTS INC Cumberland, Wake Medicaid
I/DD Facility-Based Respite ADG Associates LLC Cumberland Medicaid
I/DD Facility-Based Respite Advanced Health Resources, Inc. Johnston, Wake Medicaid
I/DD Facility-Based Respite Advantage Care In Home Services, Inc. Durham, Vance Medicaid
I/DD Facility-Based Respite Alberta Professional Services, Inc. Caswell Medicaid
I/DD Facility-Based Respite Alpha Management Services, Inc. Durham Medicaid
I/DD Facility-Based Respite Autism Services, Inc. Wake Medicaid
I/DD Facility-Based Respite Autism Society of North Carolina, Inc. Cumberland Medicaid
I/DD Facility-Based Respite BAILEY'S RESPITE CARE, INC Wilson Medicaid
I/DD Facility-Based Respite BAYADA HOME HEALTH CARE, INC. Guilford Medicaid
I/DD Facility-Based Respite Bethesda Care dba Keston Care Orange Medicaid
I/DD Facility-Based Respite Bob Inman Inc. dba Inman Home Health Cumberland Medicaid
I/DD Facility-Based Respite CANAAN CARE HOME LLC Wake Medicaid
I/DD Facility-Based Respite Caring Hands and Supplementary Enrichment Education
LLC Durham Medicaid
I/DD Facility-Based Respite Changing Outcomes, LLC Cumberland Medicaid

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 47
Specialized Service Provider Location(s) Funding Source
I/DD Facility-Based Respite CNC/ACCESS dba ResCare HomeCare Durham, Wake Medicaid
I/DD Facility-Based Respite Community Alternative Housing, Inc. Cumberland Medicaid
I/DD Facility-Based Respite Community Based Developmental Services Inc Cumberland Medicaid
I/DD Facility-Based Respite COMPREHENSIVE COMMUNITY CARE INC Durham Medicaid
I/DD Facility-Based Respite Eagle Healthcare Services, Inc Wake Medicaid
I/DD Facility-Based Respite Easter Seals UCP North Carolina & Virginia, Inc. Durham, Wake, Guilford, Surry Medicaid
I/DD Facility-Based Respite Educare Community Living Corporation - NC dba
Community Alternatives North Carolina Wake Medicaid
I/DD Facility-Based Respite Elite Care Service Inc Cumberland Medicaid
I/DD Facility-Based Respite Enhancement Health Care Durham Medicaid
I/DD Facility-Based Respite Great Expectations Day Facility and Enrichment Program,
LLC Cumberland Medicaid
I/DD Facility-Based Respite Guardian Trac LLC dba GT Independence Wake Medicaid
I/DD Facility-Based Respite HomeCare Management corporation Columbus, Edgecombe, New
Hanover Medicaid
I/DD Facility-Based Respite House of Care, Inc. Durham Medicaid
I/DD Facility-Based Respite Howell Support Services Wayne Medicaid
I/DD Facility-Based Respite J-1 CONSULTANTS, LLC Orange Medicaid
I/DD Facility-Based Respite Jeanette Purifoy dba Michael's World Cumberland Medicaid
I/DD Facility-Based Respite Johnson's House of Hope Family Care Home, LLC Durham Medicaid
I/DD Facility-Based Respite Kaleo Supports Inc Cumberland Medicaid
I/DD Facility-Based Respite Lee County Industries Lee Medicaid
I/DD Facility-Based Respite Life Based Conceptions LLC Durham Medicaid
I/DD Facility-Based Respite Lindley Habilitation Services, LLC Wake Medicaid
I/DD Facility-Based Respite MAKIN' CHOICES INC. Durham Medicaid
I/DD Facility-Based Respite Maxim Healthcare Services, Inc. Cumberland, Durham, Wake,
Guilford Medicaid
I/DD Facility-Based Respite MHS Unlimited, Corporation Durham Medicaid
I/DD Facility-Based Respite MULTI-THERAPEUTIC SERVICES, INC. Davidson, Forsyth, Randolph Medicaid

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 48
Specialized Service Provider Location(s) Funding Source
I/DD Facility-Based Respite Murchison Residential Corporation Wake Medicaid
I/DD Facility-Based Respite NEW BEGINNINGS OF NORTH CAROLINA Cumberland Medicaid
I/DD Facility-Based Respite Parker Investments, LTD. Cumberland Medicaid
I/DD Facility-Based Respite Pathways for People, Inc. Wake Medicaid
I/DD Facility-Based Respite Patterson Home Care, Inc. Cumberland Medicaid
I/DD Facility-Based Respite Pearl's Angel Care Inc. Cumberland Medicaid
I/DD Facility-Based Respite Person County Group Homes Inc Person Medicaid
I/DD Facility-Based Respite Philip House Therapeutic Services, Inc. Wake Medicaid
I/DD Facility-Based Respite PHP of NC, Inc. Durham Medicaid
I/DD Facility-Based Respite Professional Family Care Services, Inc Cumberland Medicaid
I/DD Facility-Based Respite Q- CLINICAL CONSULTANTS LLC Wake Medicaid
I/DD Facility-Based Respite QC, Inc. Wake, Franklin Medicaid
I/DD Facility-Based Respite Quest Provider Services, LLC Mecklenburg Medicaid
I/DD Facility-Based Respite Rainbow 66 Storehouse, Inc. Durham Medicaid
I/DD Facility-Based Respite Rainbow of Sunshine, Inc. Cumberland Medicaid
I/DD Facility-Based Respite ReNu Life, LLC Wayne Medicaid
I/DD Facility-Based Respite Restoration Family Services, Inc. Johnston Medicaid
I/DD Facility-Based Respite RHA Health Services, Inc. Cumberland, Durham, Wake,
Bumcombe, Granville, Harnett, Iredell, Robeson, Rowan
Medicaid
I/DD Facility-Based Respite RUSMED CONSULTANTS LLC Wake Medicaid
I/DD Facility-Based Respite Securing Resources for Consumers, Inc. Durham Medicaid
I/DD Facility-Based Respite ShineLight, Inc. Cumberland Medicaid
I/DD Facility-Based Respite Sophia B. Pierce & Associates, Inc. Cumberland Medicaid
I/DD Facility-Based Respite Specialized Services and Personnel Wake Medicaid
I/DD Facility-Based Respite Spigner Management Systems dba BJ Hill and
Associates Cumberland Medicaid
I/DD Facility-Based Respite Structured Family Interventions, LLC Durham Medicaid
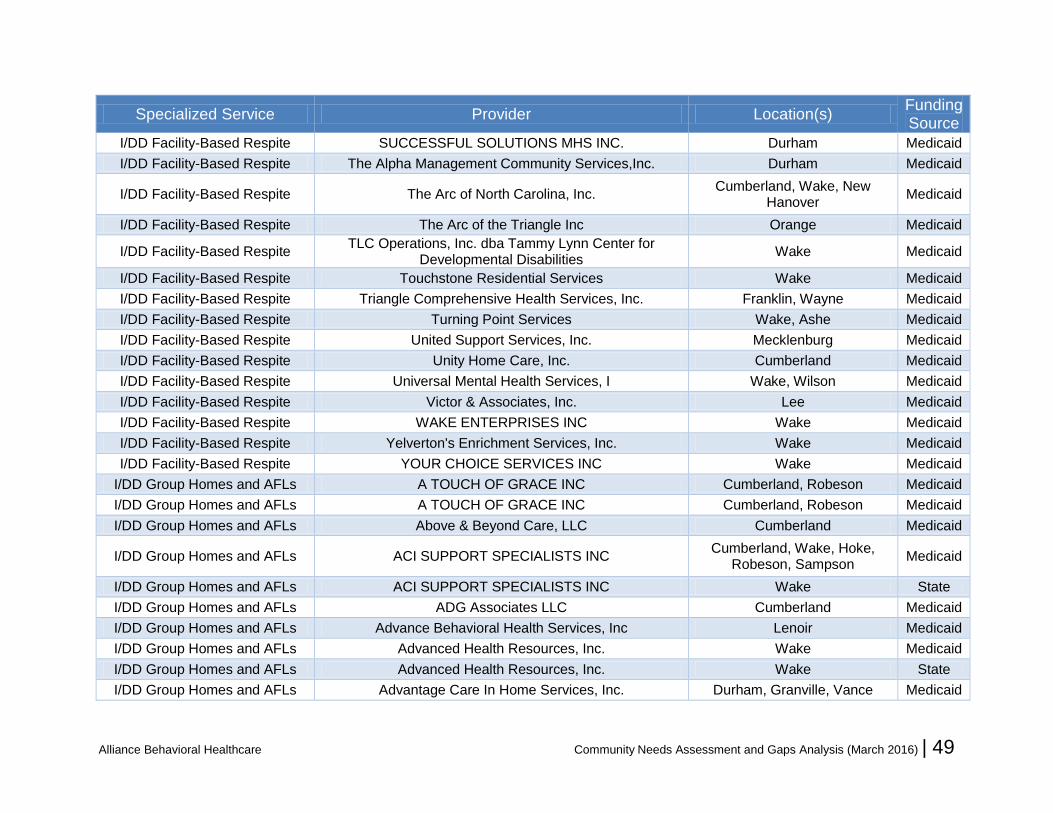
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 49
Specialized Service Provider Location(s) Funding Source
I/DD Facility-Based Respite SUCCESSFUL SOLUTIONS MHS INC. Durham Medicaid
I/DD Facility-Based Respite The Alpha Management Community Services,Inc. Durham Medicaid
I/DD Facility-Based Respite The Arc of North Carolina, Inc. Cumberland, Wake, New
Hanover Medicaid
I/DD Facility-Based Respite The Arc of the Triangle Inc Orange Medicaid
I/DD Facility-Based Respite TLC Operations, Inc. dba Tammy Lynn Center for
Developmental Disabilities Wake Medicaid
I/DD Facility-Based Respite Touchstone Residential Services Wake Medicaid
I/DD Facility-Based Respite Triangle Comprehensive Health Services, Inc. Franklin, Wayne Medicaid
I/DD Facility-Based Respite Turning Point Services Wake, Ashe Medicaid
I/DD Facility-Based Respite United Support Services, Inc. Mecklenburg Medicaid
I/DD Facility-Based Respite Unity Home Care, Inc. Cumberland Medicaid
I/DD Facility-Based Respite Universal Mental Health Services, I Wake, Wilson Medicaid
I/DD Facility-Based Respite Victor & Associates, Inc. Lee Medicaid
I/DD Facility-Based Respite WAKE ENTERPRISES INC Wake Medicaid
I/DD Facility-Based Respite Yelverton's Enrichment Services, Inc. Wake Medicaid
I/DD Facility-Based Respite YOUR CHOICE SERVICES INC Wake Medicaid
I/DD Group Homes and AFLs A TOUCH OF GRACE INC Cumberland, Robeson Medicaid
I/DD Group Homes and AFLs A TOUCH OF GRACE INC Cumberland, Robeson Medicaid
I/DD Group Homes and AFLs Above & Beyond Care, LLC Cumberland Medicaid
I/DD Group Homes and AFLs ACI SUPPORT SPECIALISTS INC Cumberland, Wake, Hoke,
Robeson, Sampson Medicaid
I/DD Group Homes and AFLs ACI SUPPORT SPECIALISTS INC Wake State
I/DD Group Homes and AFLs ADG Associates LLC Cumberland Medicaid
I/DD Group Homes and AFLs Advance Behavioral Health Services, Inc Lenoir Medicaid
I/DD Group Homes and AFLs Advanced Health Resources, Inc. Wake Medicaid
I/DD Group Homes and AFLs Advanced Health Resources, Inc. Wake State
I/DD Group Homes and AFLs Advantage Care In Home Services, Inc. Durham, Granville, Vance Medicaid
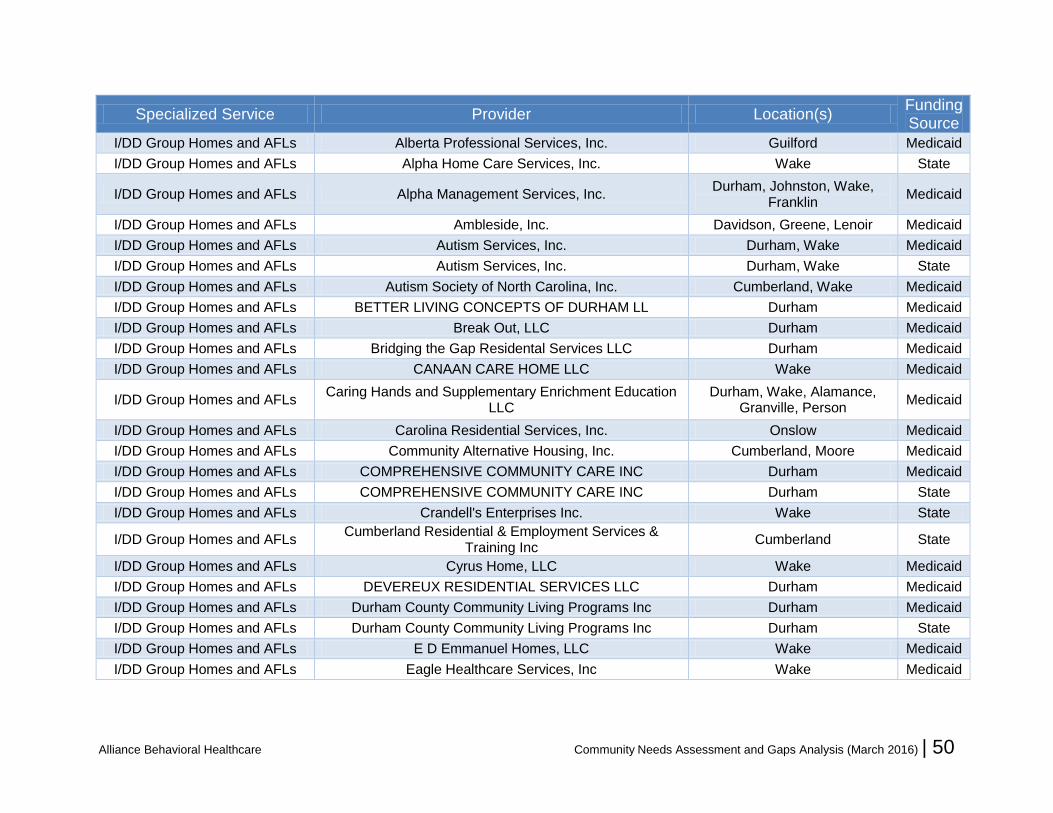
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 50
Specialized Service Provider Location(s) Funding Source
I/DD Group Homes and AFLs Alberta Professional Services, Inc. Guilford Medicaid
I/DD Group Homes and AFLs Alpha Home Care Services, Inc. Wake State
I/DD Group Homes and AFLs Alpha Management Services, Inc. Durham, Johnston, Wake,
Franklin Medicaid
I/DD Group Homes and AFLs Ambleside, Inc. Davidson, Greene, Lenoir Medicaid
I/DD Group Homes and AFLs Autism Services, Inc. Durham, Wake Medicaid
I/DD Group Homes and AFLs Autism Services, Inc. Durham, Wake State
I/DD Group Homes and AFLs Autism Society of North Carolina, Inc. Cumberland, Wake Medicaid
I/DD Group Homes and AFLs BETTER LIVING CONCEPTS OF DURHAM LL Durham Medicaid
I/DD Group Homes and AFLs Break Out, LLC Durham Medicaid
I/DD Group Homes and AFLs Bridging the Gap Residental Services LLC Durham Medicaid
I/DD Group Homes and AFLs CANAAN CARE HOME LLC Wake Medicaid
I/DD Group Homes and AFLs Caring Hands and Supplementary Enrichment Education
LLC Durham, Wake, Alamance,
Granville, Person Medicaid
I/DD Group Homes and AFLs Carolina Residential Services, Inc. Onslow Medicaid
I/DD Group Homes and AFLs Community Alternative Housing, Inc. Cumberland, Moore Medicaid
I/DD Group Homes and AFLs COMPREHENSIVE COMMUNITY CARE INC Durham Medicaid
I/DD Group Homes and AFLs COMPREHENSIVE COMMUNITY CARE INC Durham State
I/DD Group Homes and AFLs Crandell's Enterprises Inc. Wake State
I/DD Group Homes and AFLs Cumberland Residential & Employment Services &
Training Inc Cumberland State
I/DD Group Homes and AFLs Cyrus Home, LLC Wake Medicaid
I/DD Group Homes and AFLs DEVEREUX RESIDENTIAL SERVICES LLC Durham Medicaid
I/DD Group Homes and AFLs Durham County Community Living Programs Inc Durham Medicaid
I/DD Group Homes and AFLs Durham County Community Living Programs Inc Durham State
I/DD Group Homes and AFLs E D Emmanuel Homes, LLC Wake Medicaid
I/DD Group Homes and AFLs Eagle Healthcare Services, Inc Wake Medicaid
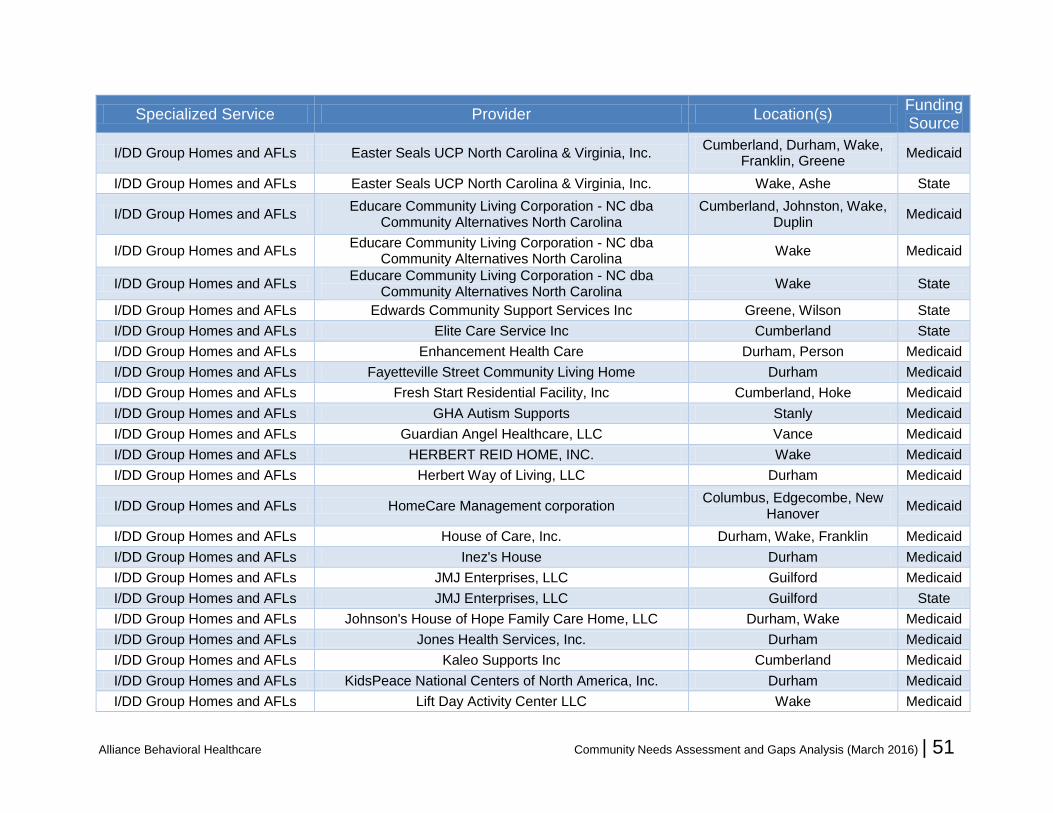
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 51
Specialized Service Provider Location(s) Funding Source
I/DD Group Homes and AFLs Easter Seals UCP North Carolina & Virginia, Inc. Cumberland, Durham, Wake,
Franklin, Greene Medicaid
I/DD Group Homes and AFLs Easter Seals UCP North Carolina & Virginia, Inc. Wake, Ashe State
I/DD Group Homes and AFLs Educare Community Living Corporation - NC dba
Community Alternatives North Carolina Cumberland, Johnston, Wake,
Duplin Medicaid
I/DD Group Homes and AFLs Educare Community Living Corporation - NC dba
Community Alternatives North Carolina Wake Medicaid
I/DD Group Homes and AFLs Educare Community Living Corporation - NC dba
Community Alternatives North Carolina Wake State
I/DD Group Homes and AFLs Edwards Community Support Services Inc Greene, Wilson State
I/DD Group Homes and AFLs Elite Care Service Inc Cumberland State
I/DD Group Homes and AFLs Enhancement Health Care Durham, Person Medicaid
I/DD Group Homes and AFLs Fayetteville Street Community Living Home Durham Medicaid
I/DD Group Homes and AFLs Fresh Start Residential Facility, Inc Cumberland, Hoke Medicaid
I/DD Group Homes and AFLs GHA Autism Supports Stanly Medicaid
I/DD Group Homes and AFLs Guardian Angel Healthcare, LLC Vance Medicaid
I/DD Group Homes and AFLs HERBERT REID HOME, INC. Wake Medicaid
I/DD Group Homes and AFLs Herbert Way of Living, LLC Durham Medicaid
I/DD Group Homes and AFLs HomeCare Management corporation Columbus, Edgecombe, New
Hanover Medicaid
I/DD Group Homes and AFLs House of Care, Inc. Durham, Wake, Franklin Medicaid
I/DD Group Homes and AFLs Inez's House Durham Medicaid
I/DD Group Homes and AFLs JMJ Enterprises, LLC Guilford Medicaid
I/DD Group Homes and AFLs JMJ Enterprises, LLC Guilford State
I/DD Group Homes and AFLs Johnson's House of Hope Family Care Home, LLC Durham, Wake Medicaid
I/DD Group Homes and AFLs Jones Health Services, Inc. Durham Medicaid
I/DD Group Homes and AFLs Kaleo Supports Inc Cumberland Medicaid
I/DD Group Homes and AFLs KidsPeace National Centers of North America, Inc. Durham Medicaid
I/DD Group Homes and AFLs Lift Day Activity Center LLC Wake Medicaid

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 52
Specialized Service Provider Location(s) Funding Source
I/DD Group Homes and AFLs Lindley Habilitation Services, LLC Wake Medicaid
I/DD Group Homes and AFLs Lutheran Family Services in the Carolinas Wake, Davidson, Forsyth Medicaid
I/DD Group Homes and AFLs Lutheran Family Services in the Carolinas Wake State
I/DD Group Homes and AFLs MAKIN' CHOICES INC. Cumberland, Durham Medicaid
I/DD Group Homes and AFLs MHS Unlimited, Corporation Durham Medicaid
I/DD Group Homes and AFLs MONARCH Johnston, Wake, Randolph,
Montgomery, Stanly Medicaid
I/DD Group Homes and AFLs MONARCH Johnston State
I/DD Group Homes and AFLs Moores House Durham Medicaid
I/DD Group Homes and AFLs More Than Conquerors Youth Center, Inc. Granville Medicaid
I/DD Group Homes and AFLs Multicultural Resources Center, Inc. Hoke State
I/DD Group Homes and AFLs MULTI-THERAPEUTIC SERVICES, INC. Davidson, Randolph Medicaid
I/DD Group Homes and AFLs Murchison Residential Corporation Wake Medicaid
I/DD Group Homes and AFLs NEW BEGINNINGS OF NORTH CAROLINA Cumberland, Wake Medicaid
I/DD Group Homes and AFLs New Destinations, Inc. Durham State
I/DD Group Homes and AFLs New Hope Management Service Wake Medicaid
I/DD Group Homes and AFLs Omni Visions, Inc. Wake Medicaid
I/DD Group Homes and AFLs Onas's Place, Inc. Buncombe, Rutherford Medicaid
I/DD Group Homes and AFLs Parker Investments, LTD. Cumberland Medicaid
I/DD Group Homes and AFLs Pathways for People, Inc. Durham, Wake Medicaid
I/DD Group Homes and AFLs Patterson Home Care, Inc. Cumberland Medicaid
I/DD Group Homes and AFLs Person County Group Homes Inc Caswell, Person Medicaid
I/DD Group Homes and AFLs Philip House Therapeutic Services, Inc. Wake Medicaid
I/DD Group Homes and AFLs PHP of NC, Inc. Durham, Person Medicaid
I/DD Group Homes and AFLs Professional Family Care Services, Inc Cumberland, Harnett, Lee Medicaid
I/DD Group Homes and AFLs Q- CLINICAL CONSULTANTS LLC Durham, Wake, Chatham,
Harnett Medicaid
I/DD Group Homes and AFLs QC, Inc. Wake Medicaid

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 53
Specialized Service Provider Location(s) Funding Source
I/DD Group Homes and AFLs Quest Provider Services, LLC Wake, Franklin Medicaid
I/DD Group Homes and AFLs Rainbow of Sunshine, Inc. Cumberland Medicaid
I/DD Group Homes and AFLs ReNu Life Extended Wayne State
I/DD Group Homes and AFLs ReNu Life, LLC Wayne Medicaid
I/DD Group Homes and AFLs Residential Services, Inc Durham, Orange Medicaid
I/DD Group Homes and AFLs Residential Support Services Wake State
I/DD Group Homes and AFLs Resources for Human Development Wake Medicaid
I/DD Group Homes and AFLs Resources for Human Development Durham, Wake State
I/DD Group Homes and AFLs RHA Health Services NC, LLC Cumberland, Wake, Bladen, Granville, Harnett, Robeson,
Rowan, Sampson Medicaid
I/DD Group Homes and AFLs RHA Health Services NC, LLC Wake, Granville, Harnett,
Robeson State
I/DD Group Homes and AFLs RHA Health Services, Inc. Cumberland, Durham, Wake,
Bladen, Granville, Harnett, Robeson, Rowan
Medicaid
I/DD Group Homes and AFLs RHA Health Services, Inc. Durham, Wake, Bladen,
Granville, Harnett, Robeson, Rowan
Medicaid
I/DD Group Homes and AFLs RHA Health Services, Inc. Wake, Granville, Harnett,
Robeson State
I/DD Group Homes and AFLs RUSMED CONSULTANTS LLC Durham, Wake Medicaid
I/DD Group Homes and AFLs Saguaro Group, LLC dba Community Innovations, Inc. Columbus, Harnett Medicaid
I/DD Group Homes and AFLs Securing Resources for Consumers, Inc. Durham Medicaid
I/DD Group Homes and AFLs Securing Resources for Consumers, Inc. Durham Medicaid
I/DD Group Homes and AFLs Serenity Therapeutic Services, LLC Cumberland, Hoke Medicaid
I/DD Group Homes and AFLs Serenity Therapeutic Services, LLC Cumberland, Hoke State
I/DD Group Homes and AFLs ShineLight, Inc. Cumberland Medicaid
I/DD Group Homes and AFLs Sophia B. Pierce & Associates, Inc. Cumberland Medicaid

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 54
Specialized Service Provider Location(s) Funding Source
I/DD Group Homes and AFLs Specialized Services and Personnel Wake Medicaid
I/DD Group Homes and AFLs Specialized Services and Personnel Wake State
I/DD Group Homes and AFLs Spigner Management Systems dba BJ Hill and
Associates Cumberland Medicaid
I/DD Group Homes and AFLs Spirit of Excellence Community Outreach, Inc. DBA
Guardian Care Onslow State
I/DD Group Homes and AFLs The Arc of the Triangle Inc Wake Medicaid
I/DD Group Homes and AFLs THE LOVING HOME INC Cumberland Medicaid
I/DD Group Homes and AFLs THE LOVING HOME INC Cumberland State
I/DD Group Homes and AFLs TLC Operations, Inc. dba Tammy Lynn Center for
Developmental Disabilities Wake Medicaid
I/DD Group Homes and AFLs Touchstone Residential Services Cumberland, Wake Medicaid
I/DD Group Homes and AFLs Touchstone Residential Services Wake State
I/DD Group Homes and AFLs Turning Point Services Wake Medicaid
I/DD Group Homes and AFLs United Living LLC Guilford Medicaid
I/DD Group Homes and AFLs United Methodist Agency for the Retarded Western NC,
Inc. Forsyth, Guilford Medicaid
I/DD Group Homes and AFLs United Residential Services of North Carolina, Inc. Cumberland Medicaid
I/DD Group Homes and AFLs United Support Services, Inc. Durham, Wake, Franklin,
Granville Medicaid
I/DD Group Homes and AFLs Unity Home Care, Inc. Cumberland Medicaid
I/DD Group Homes and AFLs Universal Mental Health Services, I Durham, Wake, Franklin,
Orange Medicaid
I/DD Group Homes and AFLs Upscale Residential Care, Inc. Sampson Medicaid
I/DD Group Homes and AFLs Victor & Associates, Inc. Harnett Medicaid
I/DD Group Homes and AFLs YOUR CHOICE SERVICES INC Wake Medicaid
I/DD Out-of-Home Respite Community Based Developmental Services Inc Cumberland State
I/DD Out-of-Home Respite Easter Seals UCP North Carolina & Virginia, Inc. Durham Medicaid
I/DD Out-of-Home Respite Easter Seals UCP North Carolina & Virginia, Inc. Cumberland, Wake State
I/DD Out-of-Home Respite Lutheran Family Services in the Carolinas Wake State

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 55
Specialized Service Provider Location(s) Funding Source
I/DD Out-of-Home Respite Murdoch Developmental Center Granville Medicaid
I/DD Out-of-Home Respite RHA Health Services NC, LLC Craven Medicaid
I/DD Out-of-Home Respite RHA Health Services, Inc. Craven Medicaid
I/DD Out-of-Home Respite Saguaro Group, LLC dba Community Innovations, Inc. Cumberland, Wake Medicaid
I/DD Out-of-Home Respite SAVIN GRACE LLC Johnston State
I/DD Out-of-Home Respite Specialized Services and Personnel Wake Medicaid
I/DD Out-of-Home Respite Stan B Treatment Services Inc Johnston State
I/DD Out-of-Home Respite The Alpha Management Community Services,Inc. Durham State
I/DD Out-of-Home Respite TLC Operations, Inc. dba Tammy Lynn Center for
Developmental Disabilities Wake State
I/DD Out-of-Home Respite Touchstone Residential Services Wake State
I/DD Out-of-Home Respite Universal Mental Health Services, I Caldwell State
ICF-IDD Autism Services of Mecklenberg County, Inc Mecklenburg Medicaid
ICF-IDD Autism Services, Inc. Durham, Wake Medicaid
ICF-IDD Carobell, Inc. Onslow Medicaid
ICF-IDD Carter Clinic, PA Cumberland Medicaid
ICF-IDD Caswell Developmental Center Lenoir Medicaid
ICF-IDD Center for Comprehensive Services, Inc. dba
NeuroRestorative Florida Out of State Medicaid
ICF-IDD Comserv, Inc. Burke Medicaid
ICF-IDD D & L Health Care Services, Inc. Cumberland Medicaid
ICF-IDD Educare Community Living Corporation - NC dba
Community Alternatives North Carolina Wake Medicaid
ICF-IDD GHA Autism Supports Stanly Medicaid
ICF-IDD Greater Image Healthcare, Corp. Moore Medicaid
ICF-IDD Horizons Residential Care Center Forsyth Medicaid
ICF-IDD Howell Support Services Lenoir Medicaid
ICF-IDD Irene Wortham Residential Center, Inc. Buncombe Medicaid
ICF-IDD J. Iverson Riddle Developmental Center Burke Medicaid

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 56
Specialized Service Provider Location(s) Funding Source
ICF-IDD KEYWEST CENTER INC Durham Medicaid
ICF-IDD Life, Inc. Brunswick, Halifax, Wayne,
Wilson Medicaid
ICF-IDD Lutheran Family Services in the Carolinas Forsyth Medicaid
ICF-IDD MID STATE HEALTH SYSTEMS INC Cumberland Medicaid
ICF-IDD MONARCH Craven, Forsyth, Richmond,
Montgomery, Stanly Medicaid
ICF-IDD Murdoch Developmental Center Granville Medicaid
ICF-IDD NOVA-IC, INC. Lenoir, Wayne Medicaid
ICF-IDD O'Berry Neuromedical Treatment Center Wayne Medicaid
ICF-IDD Person County Group Homes Inc Person Medicaid
ICF-IDD Residential Services, Inc Orange Medicaid
ICF-IDD RHA Health Services NC, LLC
Cumberland, Durham, Wake, Bumcombe, Granville, Harnett,
Iredell, Lenoir, Lincoln, Robeson, Rowan, Guilford, Hoke, Mecklenburg, Moore, Pitt, Transylvania, Watauga
Medicaid
ICF-IDD Saguaro Group, LLC dba Community Innovations, Inc. Wake, Columbus, Guilford,
Hertford, Lee, Randolph Medicaid
ICF-IDD Skill Creations, Inc. Durham, Halifax, Pitt,
Edgecombe, Nash, Sampson, Wayne
Medicaid
ICF-IDD Sophia B. Pierce & Associates, Inc. Cumberland Medicaid
ICF-IDD T.L.C. HOME, INC. Lee Medicaid
ICF-IDD TLC Operations, Inc. dba Tammy Lynn Center for
Developmental Disabilities Wake Medicaid
ICF-IDD UNC TEACCH Chatham Medicaid
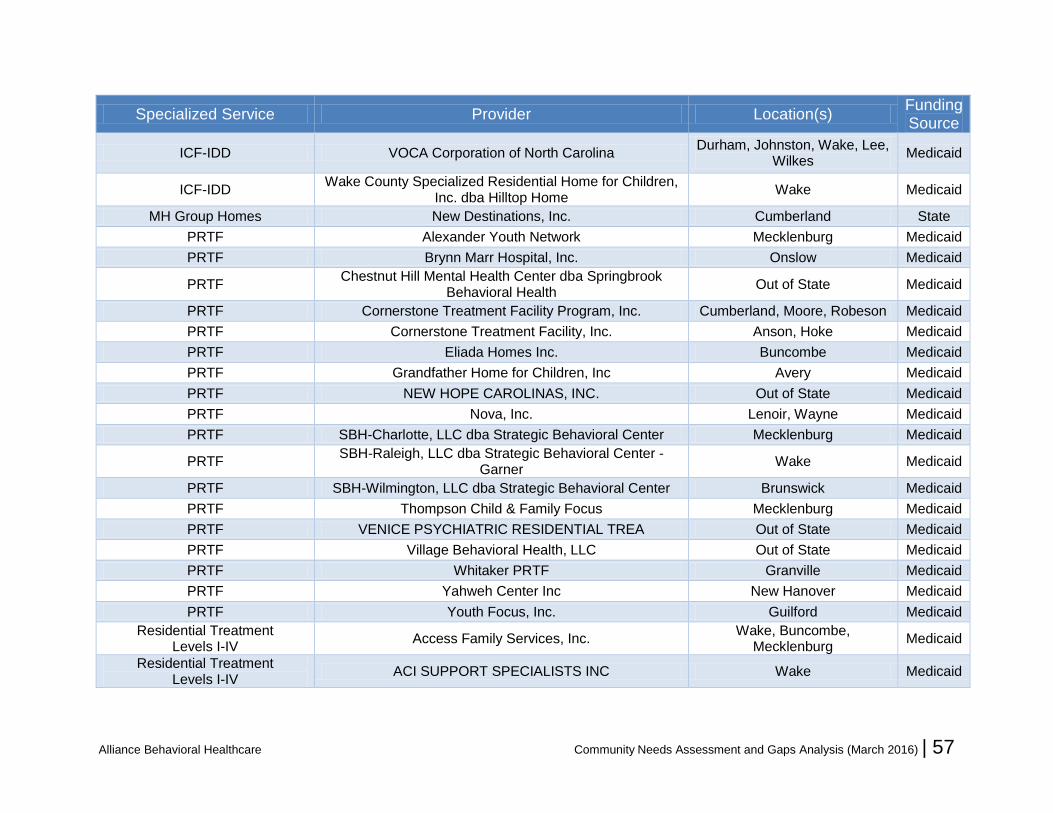
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 57
Specialized Service Provider Location(s) Funding Source
ICF-IDD VOCA Corporation of North Carolina Durham, Johnston, Wake, Lee,
Wilkes Medicaid
ICF-IDD Wake County Specialized Residential Home for Children,
Inc. dba Hilltop Home Wake Medicaid
MH Group Homes New Destinations, Inc. Cumberland State
PRTF Alexander Youth Network Mecklenburg Medicaid
PRTF Brynn Marr Hospital, Inc. Onslow Medicaid
PRTF Chestnut Hill Mental Health Center dba Springbrook
Behavioral Health Out of State Medicaid
PRTF Cornerstone Treatment Facility Program, Inc. Cumberland, Moore, Robeson Medicaid
PRTF Cornerstone Treatment Facility, Inc. Anson, Hoke Medicaid
PRTF Eliada Homes Inc. Buncombe Medicaid
PRTF Grandfather Home for Children, Inc Avery Medicaid
PRTF NEW HOPE CAROLINAS, INC. Out of State Medicaid
PRTF Nova, Inc. Lenoir, Wayne Medicaid
PRTF SBH-Charlotte, LLC dba Strategic Behavioral Center Mecklenburg Medicaid
PRTF SBH-Raleigh, LLC dba Strategic Behavioral Center -
Garner Wake Medicaid
PRTF SBH-Wilmington, LLC dba Strategic Behavioral Center Brunswick Medicaid
PRTF Thompson Child & Family Focus Mecklenburg Medicaid
PRTF VENICE PSYCHIATRIC RESIDENTIAL TREA Out of State Medicaid
PRTF Village Behavioral Health, LLC Out of State Medicaid
PRTF Whitaker PRTF Granville Medicaid
PRTF Yahweh Center Inc New Hanover Medicaid
PRTF Youth Focus, Inc. Guilford Medicaid
Residential Treatment Levels I-IV
Access Family Services, Inc. Wake, Buncombe,
Mecklenburg Medicaid
Residential Treatment Levels I-IV
ACI SUPPORT SPECIALISTS INC Wake Medicaid

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 58
Specialized Service Provider Location(s) Funding Source
Residential Treatment Levels I-IV
Alamance Academy, LLC Alamance Medicaid
Residential Treatment Levels I-IV
Alberta Professional Services, Inc. Caswell Medicaid
Residential Treatment Levels I-IV
Alexander Youth Network Mecklenburg, Moore Medicaid
Residential Treatment Levels I-IV
All God's Children of Burlington, LLC Alamance Medicaid
Residential Treatment Levels I-IV
Children Under Construction Treatment Center, Barnes Inc.
Johnston Medicaid
Residential Treatment Levels I-IV
COASTAL BEHAVIOR HEALTH SERVICES, INC. Cumberland Medicaid
Residential Treatment Levels I-IV
Community Support Service, LLC Guilford Medicaid
Residential Treatment Levels I-IV
Easter Seals UCP North Carolina & Virginia, Inc. Wake Medicaid
Residential Treatment Levels I-IV
Echelon Consulting, Inc dba Echelon Care Mecklenburg Medicaid
Residential Treatment Levels I-IV
Educare Community Living Corporation - NC dba Community Alternatives North Carolina
Wake Medicaid
Residential Treatment Levels I-IV
Eliada Homes Inc. Buncombe Medicaid
Residential Treatment Levels I-IV
FACT Specialized Services, LLC dba Methodist Home for Children, Inc
Wake, Onslow Medicaid
Residential Treatment Levels I-IV
Falcon Crest Residential Care, Inc. Alamance Medicaid
Residential Treatment Levels I-IV
Family Services of America Corp (ICAN) Cumberland Medicaid
Residential Treatment Levels I-IV
FIRM FOUNDATION, INC. Cumberland Medicaid
Residential Treatment Levels I-IV
Grandfather Home for Children, Inc Avery Medicaid
Residential Treatment Levels I-IV
Heartfelt Alternatives Inc Wake Medicaid

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 59
Specialized Service Provider Location(s) Funding Source
Residential Treatment Levels I-IV
Improving Life, Inc. Cumberland Medicaid
Residential Treatment Levels I-IV
Inspirationz, LLC Forsyth Medicaid
Residential Treatment Levels I-IV
Keep Hope Alive, LLC Pitt Medicaid
Residential Treatment Levels I-IV
KidsPeace National Centers of North America, Inc. Wake Medicaid
Residential Treatment Levels I-IV
KMG Holdings, INC Johnston, Wake Medicaid
Residential Treatment Levels I-IV
Life Changez, Inc Wake Medicaid
Residential Treatment Levels I-IV
Life Opportunities Therapeutic Home Robeson Medicaid
Residential Treatment Levels I-IV
Life Opportunities, Inc. Robeson Medicaid
Residential Treatment Levels I-IV
Lutheran Family Services in the Carolinas Mecklenburg Medicaid
Residential Treatment Levels I-IV
New Possibilities Home for Children, LLC Alamance Medicaid
Residential Treatment Levels I-IV
Omni Visions, Inc. Cumberland, Wake, Alamance,
Wayne Medicaid
Residential Treatment Levels I-IV
Pearl's Angel Care Inc. Cumberland Medicaid
Residential Treatment Levels I-IV
Pinnacle Family Services of North Carolina, LLC Cumberland, Wake Medicaid
Residential Treatment Levels I-IV
PRECIOUS HAVEN INC. Cumberland, Hoke Medicaid
Residential Treatment Levels I-IV
Quality Care Solutions, Inc. Durham, Wake Medicaid
Residential Treatment Levels I-IV
S & T WeCare, Incorporated Cumberland Medicaid
Residential Treatment Levels I-IV
S. Martin, LLC dba Inner Wealth Residential Durham Medicaid
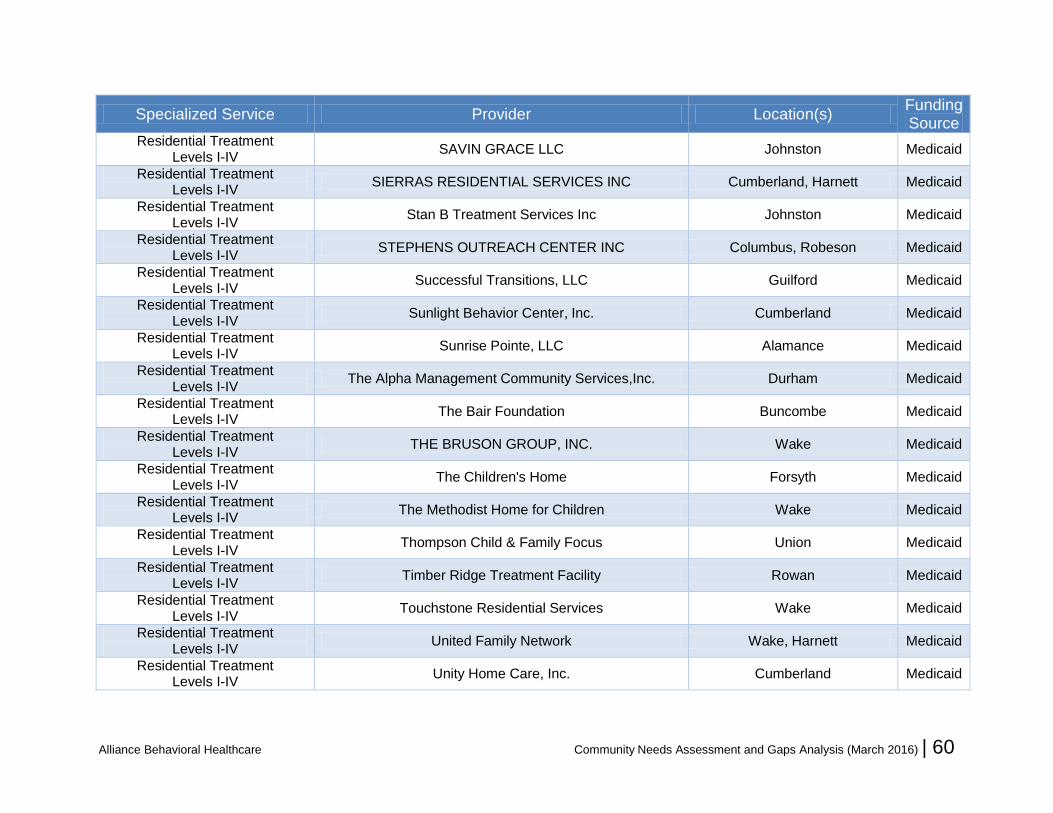
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 60
Specialized Service Provider Location(s) Funding Source
Residential Treatment Levels I-IV
SAVIN GRACE LLC Johnston Medicaid
Residential Treatment Levels I-IV
SIERRAS RESIDENTIAL SERVICES INC Cumberland, Harnett Medicaid
Residential Treatment Levels I-IV
Stan B Treatment Services Inc Johnston Medicaid
Residential Treatment Levels I-IV
STEPHENS OUTREACH CENTER INC Columbus, Robeson Medicaid
Residential Treatment Levels I-IV
Successful Transitions, LLC Guilford Medicaid
Residential Treatment Levels I-IV
Sunlight Behavior Center, Inc. Cumberland Medicaid
Residential Treatment Levels I-IV
Sunrise Pointe, LLC Alamance Medicaid
Residential Treatment Levels I-IV
The Alpha Management Community Services,Inc. Durham Medicaid
Residential Treatment Levels I-IV
The Bair Foundation Buncombe Medicaid
Residential Treatment Levels I-IV
THE BRUSON GROUP, INC. Wake Medicaid
Residential Treatment Levels I-IV
The Children's Home Forsyth Medicaid
Residential Treatment Levels I-IV
The Methodist Home for Children Wake Medicaid
Residential Treatment Levels I-IV
Thompson Child & Family Focus Union Medicaid
Residential Treatment Levels I-IV
Timber Ridge Treatment Facility Rowan Medicaid
Residential Treatment Levels I-IV
Touchstone Residential Services Wake Medicaid
Residential Treatment Levels I-IV
United Family Network Wake, Harnett Medicaid
Residential Treatment Levels I-IV
Unity Home Care, Inc. Cumberland Medicaid

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 61
Specialized Service Provider Location(s) Funding Source
Residential Treatment Levels I-IV
VOCA Corporation of North Carolina Pitt Medicaid
Residential Treatment Levels I-IV
WesCare Professional Services, LLC Guilford, Rockingham Medicaid
Residential Treatment Levels I-IV
Yelverton's Enrichment Services, Inc. Wake Medicaid
Residential Treatment Levels I-IV
Youth Builders, LLC Alamance Medicaid
Residential Treatment Levels I-IV
YOUTH ENRICHMENT GROUP HOME, INC. Caswell, Guilford Medicaid
Residential Treatment Levels I-IV
Youth Focus, Inc. Guilford Medicaid
SA Halfway House Freedom House Recovery Center, Inc. Durham State
SA Halfway House Recovery Connections Durham State
SA Medically Monitored Community Residential
Treatment UNC Wake Medicaid
SA Medically Monitored Community Residential
Treatment UNC Wake State
SA Non-Medical Community Residential Treatment
Community Choices dba CASCADES Durham State
SA Non-Medical Community Residential Treatment
Southlight Wake State

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 62
Appendix C: Stakeholder Survey Questions
Alliance Staff Group Feedback Form Alliance Behavioral Healthcare is conducting its annual assessment of service needs and gaps and is requesting feedback from the community about service needs, gaps and priorities. In addition to electronic surveys that will be administered in January 2016, we are encouraging collective responses from staff groups that would like to provide input. The questions below are recommended as a framework for a collective group response, although groups are welcome to submit feedback in other formats. Please send responses to Carlyle Johnson at [email protected] by Feb. 1, 2016.
Group Name: Submitted by (name and e-mail contact information): Group Feedback:
1. Describe the population(s) with which the group is most familiar.
2. For each population, what are the most significant service needs and gaps in your
community?
3. What are the most significant barriers to accessibility of these services?
4. Identify any groups or populations that you believe are underserved, have special needs or
have difficulty obtaining needed care.
5. Has your group prepared any written reports, surveys, or other documents in the past year
that discuss community needs and service gaps? Are you aware of any other
documentation of community needs that has been prepared by other organizations? If so,
please provide additional information about how to access these reports and/or send
copies by e-mail to [email protected].
6. Do you have any other feedback that may help Alliance understand community needs,
service gaps and priorities for network development?
7. What actions or strategies would you recommend as Alliance priorities for the upcoming
year to help address these needs and gaps?

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 63
Alliance Stakeholder Feedback Form Alliance Behavioral Healthcare is conducting its annual assessment of service needs and gaps and is requesting feedback from the community about service needs, gaps and priorities. In addition to electronic surveys that will be administered in January 2016, we are encouraging collective responses from local community organizations, committees, collaboratives and other stakeholder groups that would like to provide input. The questions below are recommended as a framework for a collective group response, although groups are welcome to submit feedback in other formats. Please send responses to Carlyle Johnson at [email protected] by Feb. 1, 2016. Group Name: Group Scope (e.g., counties covered, organizations represented, and general missions and goals): Submitted by (name and e-mail contact information): Group Feedback:
1. Describe the population(s) with which the group is most familiar.
2. For each population, what are the most significant service needs and gaps in your
community?
3. What are the most significant barriers to accessibility of these services?
4. Identify any groups or populations that you believe are underserved, have special needs or
have difficulty obtaining needed care.
5. Has your group prepared any written reports, surveys, or other documents in the past year
that discuss community needs and service gaps? Are you aware of any other
documentation of community needs that has been prepared by other organizations? If so,
please provide additional information about how to access these reports and/or send
copies by e-mail to [email protected].
6. Do you have any other feedback that may help Alliance understand community needs,
service gaps and priorities for network development?
What actions or strategies would you recommend as Alliance priorities for the upcoming year to help address these needs and gaps?

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 64
Appendix D: Community Feedback The process for soliciting community feedback included multiple approaches, including input provided through an on-line survey, stakeholder
meetings and collective feedback from consumer, provider, stakeholder and staff groups. Additional details about the survey methodology are
contained in Appendix C. The tables below provide summaries of survey data, focus group and stakeholder feedback data.
Survey Responses
The survey was conducted during the month of January 2016 and yielded a total of 573 responses, including 49 hard copy submissions. The
following provides a breakdown of submissions by respondent group:
Consumer and Family ................. 126
Provider ....................................... 242
Stakeholder ................................... 72
Staff ............................................. 133
TOTAL......................................... 573
Analysis of responses by county indicates that, although all counties are represented in each respondent group, Johnston representation is
relatively low for consumers/families and stakeholders while Cumberland has relatively strong representation from both groups. Note that provider
counts are duplicated because many providers are present in multiple counties.
County Consumers and Families Providers Stakeholders
Cumberland 54 64 27
Durham 13 74 17
Johnston 7 69 7
Wake 42 150 25
Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 65
Feedback from Consumer, Stakeholder, Provider and Staff Groups As noted in Appendix C, collective input was solicited from multiple community groups and collaboratives in addition to individual input provided
through the on-line survey. The following groups submitted feedback regarding community needs, gaps and priorities (abbreviations are for
reference in reviewing subsequent tables):
Consumer and Family Advisory Committee (CFAC)
Alliance Provider Advisory Committee (APAC), including local PAC meetings in each county
Durham and Wake Juvenile Justice SA/MH Partnerships (Durham JJSAMHP, Wake JJSAMHP )
Cumberland, Durham and Wake Crisis Collaboratives (Crisis Collabs)
Wake County Community Collaborative for Children & Families (WCCC&F)
Alliance Hospital Partners Collaborative (Hospital Partners)
Alliance MH/SA Care Coordinators (MHSA CC)
Alliance IDD Care Coordinators (IDD CC)
Alliance Utilization Management Staff (UM Staff)
Alliance Provider Network Evaluators (PN Evaluators)
Alliance Compliance Staff (Compliance)
Alliance Call Center Staff (Call Center)
Autism Society The following tables provide summaries of community feedback:
1. D-1: Summary of Community Priorities
2. D-2: Summary of populations identified as underserved

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 66
Table D-1: Summary of Community Priorities
ID
D S
urv
ey
CM
H/S
A S
urv
ey
AM
H S
urv
ey
TB
I S
urv
ey
CF
AC
AP
AC
MH
SA
CC
ID
D C
C
Ca
ll C
ente
r
UM
Sta
ff
Co
mp
liance
Du
rha
m J
JS
AM
HP
Wa
ke J
JS
AM
HP
WC
CC
&F
Ho
spita
l P
art
ners
Crisis
Co
llabo
rative
s
PN
Eva
luato
rs
Au
tism
So
cie
ty
Transportation
Services for uninsured / State benefit plan limitations
Crisis Continuum
Education and Awareness
Enhanced Benefit Development
Evaluation & Consultation
Services for co-occurring IDD/MI
Psychiatry/medication
Quality of Care Concerns
Substance Use Disorder Continuum
Residential Treatment
Housing
Service accessibility
Bilingual/bicultural services (Spanish)
Services for Transition-Age Youth

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 67
Table D-2: Summary of Populations Identified As Underserved
ID
D S
urv
ey
CM
H/S
A S
urv
ey
AM
H S
urv
ey
TB
I S
urv
ey
CF
AC
AP
AC
MH
SA
CC
ID
D C
C
Ca
ll C
ente
r
UM
Sta
ff
Co
mp
liance
Du
rha
m J
JS
AM
HP
Wa
ke J
JS
AM
HP
WC
CC
&F
Ho
spita
l P
art
ners
Crisis
Co
llabo
rative
s
PN
Eva
luato
rs
Au
tism
So
cie
ty
Bilingual/bicultural services (Spanish)
Transition-Age Youth
Co-occurring IDD/MI
Autism Spectrum
Youth engaged in sexual harm
Deaf and hard of hearing
Traumatic Brain Injuries
Substance Use Disorders
LGBTQ
Forensic/judicial involvement
Others Listed
1. Individuals with complex presenting problems, co-occurring medical and psychiatric conditions
2. individuals needing specialized treatment
3. Elderly, including those with co-occurring dementia needing residential placement
4. Youth offenders / DJJ involvement
5. Youth with complex medical problems
6. Aging IDD population
7. Co-occurring mental illness & substance use disorder
8. Homeless and those needing housing or residential treatment

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 68
Appendix E: FY16 DMH Waiver Request As requested in Section Two (see above, page 22), the Alliance waiver request to the Division of
MH/IDD/SA is provided below.

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 69
To: Dennis Farley
From: Beth Melcher, Ph.D; Chief Network Development and Evaluation
Date: 3/27/15
Re: Request for Waiver of Access and Choice Standards
Based on the recently completed Community Needs and Gaps Analysis, Alliance would like to request
a waiver of the geographic access requirement (30 miles/30 minutes) for the following:
Child and Adolescent inpatient psychiatric
treatment in Cumberland Co.
Service expansion constrained by limited
statewide availability of this service as well as
the CON process required for new inpatient
psychiatric beds. Alliance has contracts with
hospitals for this service but outside of the
standard, approximately an hour drive.
Child and Adolescent Day Treatment for
Cumberland, Durham, and Johnston
Counties
Most consumers utilizing this service have
Medicaid, and utilization by State-funded
consumers has been low in Wake. Limited
service volume and availability of funding. If
an individual need were identified Alliance
would develop a person specific contract with
a Medicaid provider. If a service capacity
need were identified Alliance could offer a
State contract to an existing Medicaid
provider.
Non-Hospital Detoxification for Johnston
County
Southeastern portion of Johnston County is
beyond geographic access standard. This is
a very rural, low population area. Service
expansion is constrained by limited service
volume and availability of funding. Individuals
may access services in both Wake and
Cumberland Counties
Facility Based Crisis for Johnston County
Southeastern portion of Johnston County is
beyond geographic access standard. This is
a very rural, low population area. Service
expansion is constrained by limited service
volume to support sustainability. Health
Department offers crisis beds in the local
emergency department to respond to crisis
needs. Facility based crisis services may be
accessed in Wake and Cumberland counties

Alliance Behavioral Healthcare Community Needs Assessment and Gaps Analysis (March 2016) | 70
TBI non-residential for Cumberland and
Johnston
Access standard is not met in these two
counties but since this is a community-based
service access is available in all Alliance
counties.
Alliance would like to request a waiver of the provider choice requirement for the following:
Child Adolescent Day Treatment for
Cumberland, Durham, and Johnston
Counties
Choice of provider is constrained by limited
service demand and funding availability. If an
individual need were identified Alliance would
develop a person specific contract with a
Medicaid provider. If a service capacity need
were identified Alliance could offer a State
contract to an existing Medicaid provider.
Opioid Treatment for Durham, Wake,
Cumberland and Johnston
Alliance is committed to developing access to
this service in all counties. Choice of provider
is constrained by limited service demand and
funding availability. Access will be available
in other counties.
PSR for Cumberland and Durham
Choice of provider is constrained by limited
funding availability. If an individual need were
identified Alliance would develop a person
specific contract with a Medicaid provider. If a
service capacity need were identified Alliance
could offer a State contract to an existing
Medicaid provider.
SACOT for Durham
Choice of provider is constrained by limited
service demand and funding availability. If an
individual need were identified Alliance would
develop a person specific contract with a
Medicaid provider. If a service capacity need
were identified Alliance could offer a state
contract to an existing Medicaid provider.
Thank you for your consideration of this request. Feel free to contact me if you have additional
questions.
cc: Shealy Thompson
Carol Potter


















