Community Care Alliance of Illinois Integrated Care ...ccaidev.com/medicaid/files/Provider...
53
1 Community Care Alliance of Illinois Integrated Care Program QI Program/Plan 2016
-
Upload
phungthien -
Category
Documents
-
view
213 -
download
0
Transcript of Community Care Alliance of Illinois Integrated Care ...ccaidev.com/medicaid/files/Provider...

1
Community Care Alliance of Illinois Integrated Care Program
QI Program/Plan 2016
2
Contents Contents .......................................................................................................................................... 2 I. Organizational Overview/Background .................................................................................... 5 II. Quality Improvement Program Description [QI1] .................................................................. 9
A. Strategic Goals, Objectives and Priorities ............................................................................ 9 B. Purpose ................................................................................................................................ 9 C. Scope of Services ................................................................................................................. 9 D. Goals [QI1A-3] ...................................................................................................................... 9 E. Objectives [QI1A-4] ............................................................................................................ 10
III. Quality Improvement/Management Summary [QI1A-1] ..................................................... 11 IV. Quality Improvement Methodology ..................................................................................... 12
A. BCAP Typology ................................................................................................................... 12 B. Rapid Cycle Improvement .................................................................................................. 14 C. Measurement and Evaluation ........................................................................................... 15 D. Sustainability and Diffusion ............................................................................................... 15
V. Annual Work Plan [QI1A-7] ................................................................................................... 15
E. Quality Improvement Program Activities .......................................................................... 15
CAHPS .................................................................................................................................... 16 Provider Engagement ........................................................................................................... 16 Member Engagement ........................................................................................................... 17 Electronic Learning Media Resource (ELMR) ........................................................................ 17 Clinical Practice Guidelines ................................................................................................... 17 Individuals Ages Nineteen (19) and Twenty (20) .................................................................. 18 Pregnancy Related Activities: ............................................................................................... 18 Hypertension Improvement Project: .................................................................................... 19 Member-directed Gaps in Care Letters: ............................................................................... 19 Provider education: .............................................................................................................. 20 Care Coordination HEDIS Education ..................................................................................... 20 HEDIS / HQOL: ....................................................................................................................... 20
F. Collaborative QI Activities [QI1A1] .................................................................................... 21
Care Coordination Performance Improvement Project (PIP): ................................... 21 Behavioral Health Process Improvement Project (PIP) .............................................. 21
VI. Behavioral Healthcare [QI1A2, QI1A5] ................................................................................. 22
A. Monitoring and Improving Behavioral Healthcare ............................................................ 22 B. Involvement of a Designated Behavioral Healthcare Practitioner [QI1A-5] ..................... 23

3
VII. Serving a Diverse Membership [QI1A8] ............................................................................. 23
A. Cultural Competency plan: ................................................................................................ 23 B. Disability Community Stakeholder Forum ......................................................................... 23 C. Educational Material at 6th grade reading level ................................................................ 24 D. Multi-lingual printed material............................................................................................ 24 E. Language Line .................................................................................................................... 24 F. Hiring Diverse Employee Base: .......................................................................................... 24
VIII. Serving Members with Complex Health Needs [QI1A9] .................................................... 24
A. Complex Case Management (CCM) ................................................................................... 24 B. Disease Management (DM) ............................................................................................... 25 C. CMDM report analysis: ...................................................................................................... 25 D. Waiver Audits ..................................................................................................................... 26
IX. Patient Safety [QI1A3] .......................................................................................................... 26
A. Medication Reconciliation ................................................................................................. 26 B. HTN Improvement Project ................................................................................................. 27 C. Flu Campaign ...................................................................................................................... 27 D. Flu Campaign for the Care-Coordinators: .......................................................................... 28 E. HEDIS / HQOL ..................................................................................................................... 28 F. ELMR .................................................................................................................................. 28
X. Quality Improvement Program Structure ............................................................................. 28
A. Roles and Responsibilities [QI1A1, QI1A4, QI1A6] ............................................................ 28
Board of Directors ...................................................................................................... 28 President ..................................................................................................................... 29 Chief Operating Officer ............................................................................................... 29 The Chief Medical Officer [QI1A-4] ............................................................................ 29 VP of Healthcare Management .................................................................................. 31 VP of Population Health and Quality .......................................................................... 32 VP of Utilization and Transitional Care Management ................................................ 33
Chief Information Officer............................................................................................ 34 Chief Financial Officer ................................................................................................. 34 Chief Compliance Officer ............................................................................................ 35
B. Functional Areas [QI1A1, QI1A4, QI1A6] ........................................................................... 35
1. Operations .................................................................................................................. 35 2. Healthcare Management ............................................................................................ 35 3. Compliance ................................................................................................................. 35

4
4. Information Technology ............................................................................................. 35 5. Finance ........................................................................................................................ 36
C. Responsibilities of the Quality Improvement Team .......................................................... 36
1. Manager, Quality Improvement ................................................................................. 36 2. Quality Improvement Specialist ................................................................................. 36 3. HEDIS Analyst .............................................................................................................. 36
D. Organizational Chart [QI1A1] ............................................................................................. 38 E. Committee Structure and Oversight [QI1A-6] ................................................................... 38
1. CCAI’s Board of Directors ........................................................................................... 39
F. QI/UM Committee/Oversight of QI [QI1A1, QI1A4, QI1A5, QI1A6] [QI2A1, QI2A2, QI2A3, QI2A4, QI2A5] ........................................................................................................................... 40
1. CCAI QI/UM Committee ............................................................................................. 40
G. Committees [QI1A6] .......................................................................................................... 43
1. Consumer Advisory Committee .................................................................................. 43 2. Peer Review (PR) Committee ..................................................................................... 43 3. Credentialing Committee (FHN/CCAI) ........................................................................ 45 4. Delegated Oversight Committee (FHN/CCAI) ............................................................. 45 5. Cultural Competency Workgroup (FHN/CCAI) ........................................................... 46 6. Customer Service Quality Committee (FHN/CCAI) ..................................................... 47 7. Compliance Committee .............................................................................................. 48
H. Resources and Analytic Support [QI1A1] ........................................................................... 48 I. Delegated QI Activities [QI1A1] ......................................................................................... 50
Attachment 1 .............................................................................................................. 52
XI. Acknowledgement and Approval.......................................................................................... 53

5
I. Organizational Overview/Background
Community Care Alliance of Illinois (CCAI) is a Managed Care Community Network (MCCN) that was incorporated as a not-for profit wholly owned subsidiary of Family Health Network (FHN) and initiated providing services to its members effective July 1, 2013. The governing board of CCAI is comprised of consumers/beneficiaries as well as the providers and health plan leadership. CCAI’s plan enrolls Seniors and Persons with Disabilities (ages 19-64) who are eligible to receive Integrated Care Program (ICP) services as determined by the Illinois Department of Healthcare and Family Services (IDHFS). Membership is comprised of individuals from various cultural backgrounds and various primary languages. CCAI delivers health plan related services to an underserved population. CCAI prides itself on the ability to identify, address and coordinate services for its members that come from various cultures, ethnicities and religious backgrounds. CCAI works diligently to close the gaps in health disparities for its ethnically diverse members. CCAI population includes members receiving home and community-based services waivers (HCBS) in order to meet member needs and promote their residential independence within their homes rather than institutions such as aging waivers, traumatic brain injury waivers, HIV/AIDS waivers, people with developmental disabilities waivers, people with disabilities and Supportive/Assisted Living Facility waivers. 12.41% of CCAI served membership receives assistance through one of the HCBS waivers described above. We also provide services for members residing in Long Term Care Facilities. 9.4% of the total population is stratified as high risk with 41.7% being moderate risk and 49.00% as low risk. High and Moderate risk members require intense Care Coordination in order to meet all their healthcare needs. 78.2% of the high risk and 58.1% of the moderate risk population is enrolled in care coordination for the purpose of improving health outcomes. The top five (5) of most common medical diagnosis for the CCAI population are: (1) Hypertension, (2) Dyslipidemia, (3) Diabetes, (4) Obesity and (5) Osteoarthritis. Tally based on unduplicated member count. Percentages based on total membership.
6
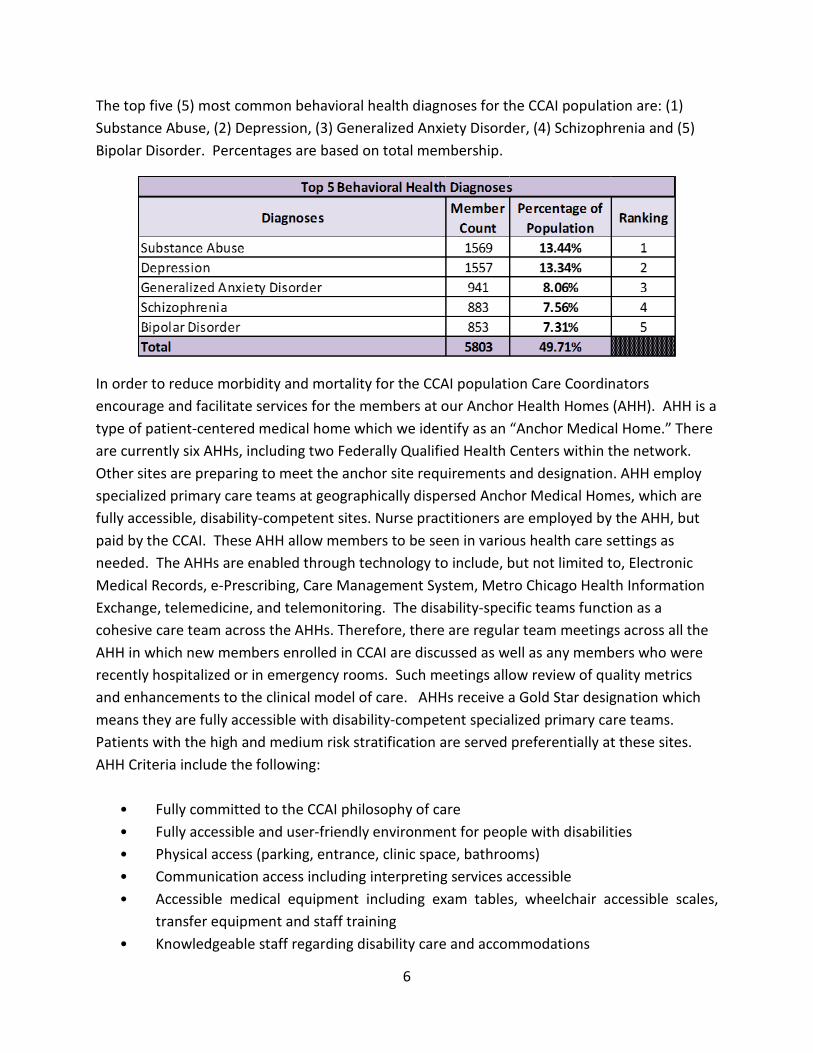
The top five (5) most common behavioral health diagnoses for the CCAI population are: (1) Substance Abuse, (2) Depression, (3) Generalized Anxiety Disorder, (4) Schizophrenia and (5) Bipolar Disorder. Percentages are based on total membership.
In order to reduce morbidity and mortality for the CCAI population Care Coordinators encourage and facilitate services for the members at our Anchor Health Homes (AHH). AHH is a type of patient-centered medical home which we identify as an “Anchor Medical Home.” There are currently six AHHs, including two Federally Qualified Health Centers within the network. Other sites are preparing to meet the anchor site requirements and designation. AHH employ specialized primary care teams at geographically dispersed Anchor Medical Homes, which are fully accessible, disability-competent sites. Nurse practitioners are employed by the AHH, but paid by the CCAI. These AHH allow members to be seen in various health care settings as needed. The AHHs are enabled through technology to include, but not limited to, Electronic Medical Records, e-Prescribing, Care Management System, Metro Chicago Health Information Exchange, telemedicine, and telemonitoring. The disability-specific teams function as a cohesive care team across the AHHs. Therefore, there are regular team meetings across all the AHH in which new members enrolled in CCAI are discussed as well as any members who were recently hospitalized or in emergency rooms. Such meetings allow review of quality metrics and enhancements to the clinical model of care. AHHs receive a Gold Star designation which means they are fully accessible with disability-competent specialized primary care teams. Patients with the high and medium risk stratification are served preferentially at these sites. AHH Criteria include the following:
• Fully committed to the CCAI philosophy of care • Fully accessible and user-friendly environment for people with disabilities • Physical access (parking, entrance, clinic space, bathrooms) • Communication access including interpreting services accessible • Accessible medical equipment including exam tables, wheelchair accessible scales,
transfer equipment and staff training • Knowledgeable staff regarding disability care and accommodations

7
• Dedicated specialized disability-competent primary care team (primary care providers will be NPs and MDs), Care Coordinator (RN), LTSS Care Coordinator, and behavioral health services provided by PsycHealth, Ltd.
• Committed to the model of consumer-directed, person-centered services • Committed to working with CCAI nurse care coordinators/intake specialists who
complete screenings, triage, and initial risk stratification, and communicate with primary care provider about initial contact for new members. Once a care plan is developed by PCP and patient, PCP will communicate the plan back to the care coordinator to incorporate into CCAI care coordination tools, and to assist in arranging all appointments, services and follow-up of all ordered tests, consults, etc.
• Committed to incorporating CCAI care coordination tools, health information technologies and enhancements into anchor site health information systems
• Committed to using the care coordination tools, clinical pathways, quality metrics and provider networks of CCAI
• Participation in team meetings, case reviews, quality indicators, and disability/ chronic illness continuing activities across the anchor sites
CCAI’s Mission Statement is: “The Community Care Alliance of Illinois is a health plan dedicated to consumer-directed., community-based innovative health services specializing in the care of seniors and people with disabilities.” CCAI’s Vision Statement is: “To be the leader in Choice, Access and Quality of Health Services for the people we serve.” CCAI’s Values are:
1. Respect 2. Integrity 3. Teamwork 4. Service 5. Stewardship 6. Transparency
CCAI uses its Model of Care (MOC) as the fundamental framework of its operations which focuses on member-driven needs. The MOC is an all-encompassing philosophy of a holistic approach to member care addressing the medical, functional, psychological, social support, financial and environmental domains of its Biopsychoecological framework of operations. Salient features of the CCAI clinical model include:

8
1. Person-centered, consumer-driven community health care plans integrating medical, behavioral/mental health, DME, social and home-based care (including consumer driven personal assistant services).
2. Specialized primary care services with disability competent Interdisciplinary Care Teams comprised of Primary Care Providers (PCPs): Nurse Practitioners (NPs) or MD/DO, Nurse Care Coordinators and Long Term Services and Supports (LTSS) Coordinators delivering and coordinating first line care to a cohort of complex patients. The NPs will need to be skilled not only in primary care, chronic disease and care management, but the particulars of caring for people with physical disabilities. Other core team members will include psychiatrists, allied health professionals, DME and Personal Assistant (PA) coordinators, social workers, behavioral/mental health specialists, internists, family physicians and pediatricians. The model provides frequent contact, early intervention with an emphasis on preventive care, homecare and availability of CCAI staff with access to patient care plans and record, to decrease the need for emergency room visits and recurring hospitalizations. The CCAI care model allows for customization based on variations in the complexity and type of care required by the member and, at the same time, provides structure for care planning and evaluation. For example, the type of assessment will vary according to the site of care (e.g. house calls will include environmental assessments) and individualized member problems (e.g. diabetes, cognitive functioning). This framework also enhances communication with team members and other resources and supports a comprehensive view of APN practice – considering the entire person.
3. Fully accessible and committed to Anchor Health Homes with specialized primary care teams in geographically disperse areas of Cook, Boone and Winnebago and the six (6) collar counties (DuPage, Kane, Kankakee, Lake, McHenry and Will).
4. Primary and secondary prevention emphasis in clinical pathways and care plans, with individualized health and wellness plans and availability of integrated exercise classes, nutrition and weight management for the members.
5. A network of centers of excellence (for rehabilitation and mental health services) and contractual specialty care providers and resources to support the specific disability medical needs (orthotics, DME providers, urologists, neurologists, plastic surgeons, pulmonologists, orthopedic physicians, etc.).
CCAI integrates physical health, long term services and supports (LTSS) and behavioral health services to offer and provide unified high quality services to members across the continuum of delivered care and services. Various processes are utilized to ensure consistent services are offered. CCAI employs and partners with qualified individuals and business entities that are culturally competent to meet the needs of populations served. CCAI contracts with providers and networks that meet the needs of its diverse consumer base.

9
II. Quality Improvement Program Description [QI1]
A. Strategic Goals, Objectives and Priorities CCAI continually strives to deliver high quality care and services to its members across the healthcare continuum and serves as the ideal partner for providers, networks, state and federal agencies. The Quality Improvement (QI) Program (referenced as a Plan throughout the document) establishes the standards that incorporate all quality improvement activities. Daily operations are driven by CCAI’s core values which are respect, integrity, teamwork, service, stewardship and transparency. CCAI address unique needs of the members by engaging members in effective disease management, complex case management and care coordination programs on a daily basis. Quality-driven and safety-focused services for both, the member and the provider, are the driving forces behind CCAI’s culture. In order to meet strategic goals and objectives, CCAI systematically monitors effectiveness of its activities and makes improvements accordingly.
B. Purpose The purpose of the QI Plan is to execute the Mission and support the Vision Statement in order to meet the multi-faceted healthcare needs of its members. It is to have a significant positive impact on the access to care, services and health outcomes for the population served. Quality Improvement and Utilization Management Departments work collaboratively to provide on-going monitoring and improvement of activities as is outlined in this plan and supported by the Work Plan.
C. Scope of Services The scope of the Quality Improvement Plan is comprehensive, addressing the quality of health care/services as well as the quality and efficacy of the processes for providing services. Evaluation of systems and processes that support the delivery of services performed by CCAI staff and provider groups will also be an integral part of the program. CCAI will be conducting quality projects and activities to achieve this program’s goals.
D. Goals [QI1A-3] The overall goal of the QI Plan is to ensure that our members receive the right care at the right time in the right settings. In order to meet the overall goal CCAI has identified the following goals for the 2016 QI Plan:
1. Implement measures to obtain National Committee of Quality Assurance (NCQA) accreditation in 2017.

10
2. Monitor and improve the access to care, safety, efficiency and effectiveness of clinical and non-clinical care and services by:
a. Implementing the CCAI 2016 QI Plan. b. Educating CCAI staff, providers and networks regarding the 2016 QI Plan and all
the activities involved for the measurement year of 2016. c. Reevaluating current evidence based clinical guidelines and implement
accordingly. d. Ensure that programs of care and services meet the culturally and linguistically
diverse needs of the CCAI Members. e. Improving member satisfaction results reported in the Consumer Assessment of
Healthcare Providers and Systems (CAHPS®). f. Developing and implementing CCAI specific member satisfaction survey; establish
benchmarks by end of 2016. g. Improving the 2016 Health and Quality of Life (HQOL) Performance Measures and
NCQA® benchmarks. h. Actively participating in two (2) collaborative process improvement projects (PIP): i. Developing, implementing and operating an effective Complex Case Management
(CCM) Program. j. Developing, implementing and operating an effective Disease Management (DM)
Program. k. Increasing ICP populations’ engagement and participation in Care Coordination
program for the High and Moderate risk stratified members.
E. Objectives [QI1A-4] CCAI has identified the following objectives in order to meet the set-forth 2016 QI Plan goals:
1. Successfully operationalize NCQA standards required for six months look back period by 4/1/2016.
2. Review and approve the 2016 QI Plan by January, 2016 by the Board of Directors. 3. CCAI staff will understand the QI Plan’s 2016 goals and objectives through an on-going
education. 4. CCAI providers will be informed of the approved 2016 QI Plan and comply with all Work
Plan activities and initiatives as is defined in their service contracts. 5. Reassess new evidence based clinical guidelines and update accordingly by 04/30/2016. 6. The member reported survey (CAHPS) results will be favorable:
a. Increase the GNC measure to reach 80.5%. b. Increase the GCQ measure to reach 79.9%. c. Increase the Flu Vaccinations measure to 75th percentile rate

11
7. Improve healthcare outcomes for HQOL/HEDIS rates for the ICP population to reach the 75th percentile for 40% of the required measures.
a. Decrease the 30 days same cause readmission rate by end of 2016. b. Decrease Emergency Department utilization rate by end of 2016.
8. Successfully implement collaborative PIPS: Behavioral Health, Care Coordination and HTN CCIP.
9. Identify, offer and enroll the top 1% of risk score and 1% of total utilization cost members in the Complex Case Management.
10. Identify, offer, enroll and manage members’ uncontrolled diseases for the following selected conditions: HTN and Diabetes (DM) through the Disease Management Program.
11. At least 60% of high and moderate risk -stratified members enrolled in Care Coordination Program.
III. Quality Improvement/Management Summary [QI1A-1]
In order to satisfy the goals and objectives of the 2016 QI Plan, CCAI has incorporated quality improvement activities and/or initiatives into the plan’s functional areas. These [functional areas] include, but are not limited to the following:
1. Care Coordination (Nursing and LTSS) a. Care Coordination b. Complex Case Management c. Disease Management
2. Member Services Department 3. Operations
a. Finance b. Claims and Encounter Data
4. Appeals, Grievances and Compliance 5. Information Technology (IT)
a. Systems interface 6. Pharmaceutical Data
a. CVS 7. Provider and Network Management
a. Credentialing and recredentialing b. Provider relations c. Medical health care
Access and availability of services
12
Utilization of Services 8. Behavioral health care
a. Access and availability of services b. Utilization of Services
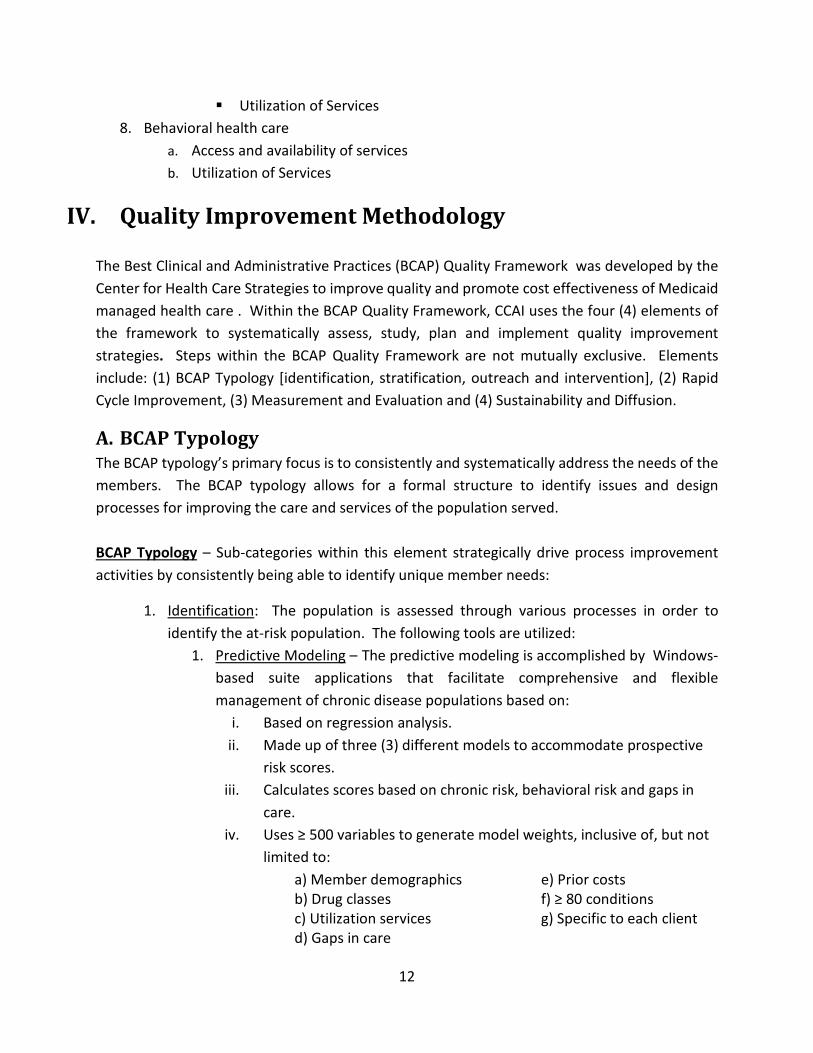
IV. Quality Improvement Methodology The Best Clinical and Administrative Practices (BCAP) Quality Framework was developed by the Center for Health Care Strategies to improve quality and promote cost effectiveness of Medicaid managed health care . Within the BCAP Quality Framework, CCAI uses the four (4) elements of the framework to systematically assess, study, plan and implement quality improvement strategies. Steps within the BCAP Quality Framework are not mutually exclusive. Elements include: (1) BCAP Typology [identification, stratification, outreach and intervention], (2) Rapid Cycle Improvement, (3) Measurement and Evaluation and (4) Sustainability and Diffusion.
A. BCAP Typology The BCAP typology’s primary focus is to consistently and systematically address the needs of the members. The BCAP typology allows for a formal structure to identify issues and design processes for improving the care and services of the population served. BCAP Typology – Sub-categories within this element strategically drive process improvement activities by consistently being able to identify unique member needs:
1. Identification: The population is assessed through various processes in order to identify the at-risk population. The following tools are utilized:
1. Predictive Modeling – The predictive modeling is accomplished by Windows-based suite applications that facilitate comprehensive and flexible management of chronic disease populations based on:
i. Based on regression analysis. ii. Made up of three (3) different models to accommodate prospective
risk scores. iii. Calculates scores based on chronic risk, behavioral risk and gaps in
care. iv. Uses ≥ 500 variables to generate model weights, inclusive of, but not
limited to: a) Member demographics b) Drug classes c) Utilization services d) Gaps in care
e) Prior costs f) ≥ 80 conditions g) Specific to each client

13
2. Health Risk Screening (HRS) – Member completed and self-reported health survey distributed to all new members with each enrollment. This screening/survey is risk stratified based on the answer-driven produced score. Risk stratification is as follows:
i. High Risk: Risk score of ≥ 10. ii. Medium Risk: Risk score of 5-9.
iii. Low Risk: Risk score of ≤ 4. 3. Health Risk Assessment (HRA) – Comprehensive assessment completed by
Care Coordinators. The HRA questions are designed to assess overall physical and psychosocial health as well as the economic, environmental and behavioral risks of each member by assessing responses to questions regarding:
i. Health Status ii. Compliance with preventive care
iii. Chronic health conditions, including behavioral health iv. Activities of daily living (ADL) / Instrumental activities of daily
living (IADL) v. Lifestyle risks, e.g. use/abuse of alcohol or controlled substances
vi. Suitability of living environment vii. Barriers to care
viii. Primary support ix. Quality of life x. Life-planning needs
xi. Continuity-of-care needs xii. Medication compliance
The member’s immediate concerns will be elicited during this process (urgent concerns or needs will be triaged to high priority status for the PCP), as well as self-evaluation of their health status, life satisfaction and identified goals (including desire for further education about health and wellness needs).
4. Historical Encounter Data – Historical encounter data/claims is also used to assess members’ risk stratification.
5. Utilization data – Utilization reports are used to identify high-risk population based on service utilization. This activity allows to identify, develop and implement quality improvement initiatives. Various utilization reports are used to identify the at-risk population based on high utilizations. This includes the Utilization Management report (UR1) and Prior Auth report. The UR1 report includes the following area utilizations: Emergency Department (ED),

14
inpatient hospitalizations: medical and behavioral health, readmissions, rehabilitation, long-term care facilities (LTFs) and outpatient settings.
6. Case Management/Disease Management (CMDM) reports – These reports are used to identify members’ assessed and/or stratified risks based on Predictive Modeling System. This report allows for identical and trending of risk stratified members.
2. Stratification: Some of the tools mentioned above are utilized to identify and allocate appropriate resources to the identified vulnerable population (high or moderate risk members). CCAI uses the stratification process to assign risk/severity or priority of need to enrolled and stratified members. The Predictive Modeling system is used to drive the initial risk stratification based on historical encounter data, existing conditions, pharmacy claims and utilization of services. Once an HRA is complete the Care Coordinator stratifies the member based on the HRA. This stratification supersedes the Predictive Modeling stratification. Stratification based on predictive modeling is also utilized in the identification of high risk members that qualify for Complex Case Management and Disease Management.
3. Outreach: Outreach is accomplished through a multimodal approach: telephonically, in person at the Anchor Health Home sites, EDs, hospitals or at the member’s home. The outreach mode is based on the member’s preferences and physical ability. Additional enhancement initiatives have been implemented to assist the outreach efforts such as:
1. CVS claims data and Skip Trace reports are being utilized in order to cross reference existing contact information of the hard to reach members.
4. Intervention: On-going monitoring of at-risk members’ (population) needs and continual modifications (if applicable) to process improvements are applied to this interventional subgroup within the BCAP Quality Framework.
B. Rapid Cycle Improvement Rapid Cycle Improvement – This element promptly and efficiently measures progress of ongoing activities and refines them as appropriate to meet the set goals. Elements of this process include:
1. Aim 2. Measure 3. Change 4. Plan-Do-Study-Act Cycles. These cycles allow rapid analysis and evaluation of on-
going needs. The PDSA model allows CCAI to:

15
a. Plan – evaluate data, identify improvement opportunities and determine appropriate intervention strategies.
b. Do – implement processes to address the identified needs and barriers. c. Study – measure the effects of implemented strategies and assess their
effectiveness. d. Act – continue the process if results yield favorable outcomes or adjust
processes accordingly to meet the need of the identified area of improvement.
C. Measurement and Evaluation Measurement and Evaluation – Application of realistic measures which are incorporated into the quality initiatives to establish baseline data, guide and monitor improvement efforts and demonstrate the success of change strategies. Various reports are used to measure and evaluate quality initiatives such as utilization management reports, readmission rates, discharge assessment reports, HEDIS/HQOL rates, CAHPS, HRS and HRA completion reports, HTN Chronic Care Improvement Program (CCIP) results, grievances and complaints report, discharge assessments and risk stratification.
D. Sustainability and Diffusion Sustainability and Diffusion – Development of tools that are utilized to institutionalize and implement best practices to ensure long-term success of quality efforts. Based on results and evaluation of quality initiatives and processes, various tools are developed such as dashboards, workflows and reference guides. Education and process implementation takes place with those involved.
V. Annual Work Plan [QI1A-7]
E. Quality Improvement Program Activities Quality Improvement Program Activities are not mutually exclusive. Integration is essential to successful quality improvement management across all functional areas. Activities are integrated through coordinated referral systems and include, but are not limited to:
1. Maintaining a system for monitoring the quality and effectiveness of care and services that is continuous, methodical and successful.
2. Collecting monitoring and analyzing required HEDIS and other QI measures and performance levels.
3. Prioritizing measures and study topics according to epidemiological characteristics of the membership.
4. Establishing processes for improvements. 5. Designing interventions to have maximum impact on health outcomes.

16
6. Tracking actions to determine that the desired outcomes are achieved. 7. Partnering with members in a way that promotes optimal health, satisfaction and
functional status through health education, active collaboration and community integration.
8. Integrating coordination between behavioral and physical healthcare components into all aspects of the program.
CAHPS CAHPS is administered annually to a sample population and is used by CCAI to assess consumer’s experience and report on the plan’s overall quality. Objective: Systematically measure member’s experience with offered services and reach 80.5% for Getting Needed Care measure, 79.9% in Getting Care Quickly measure and improve Flu Vaccination Status to reach 75th percentile rate. Rapid Cycle Improvement: Systematically monitor set objectives through: Annual Assessment and Evaluation of the CAHPS results. Evaluate the following CAHPS domains: Getting Needed Care, Getting Care Quickly, How Well Doctors Communicate, Customer Service, Shared Decision Making, Health Promotion and Education, Coordination of Care, Providing Needed Information, Ease of Filling out Forms, Health Care, Provider and Plan Ratings, Effectiveness of Care Measures.
Provider Engagement The Quality Improvement Department coordinated efforts with multiple functional areas to improve access and availability of care for the membership. Provider outreach has been established in order to monitor and/or improve high quality of services. Objective: To provide continuous care to members by keeping the providers informed of needed services, closure of gaps-in-care and collaborate outreach efforts between network/provider and the plan. To reach HEDIS/HQOL 75th percentile rates for 40% of the required measures and to ensure members receive appropriate and needed care. Rapid Cycle Improvement: Systematically monitor set objective and keep providers informed of progress and areas of improvement through: monthly assessment of all reported HEDIS/HQOL measures, identification of outstanding/negative numerator members against assigned providers. Monthly distribution of gaps-in-care reports to contracted networks and associated providers respectively. Identification of assigned Care Coordinators and coordination of outreach efforts with assigned providers. Pay-for-Performance program for providers to incentivize closure of gaps-in-care.

17
Member Engagement Care Coordinators continuously participate in the member engagement processes. Care Coordinators (RN and LTSS) attend bi-monthly department meetings that address any areas/concerns that have been identified through the P-D-S-A process of various Quality Improvement activities. Additionally, Care Coordinators participate in electronic learning modules that address HEDIS education: purpose, significance, reported measures, measure definitions, expected return rates and time-lines. Care Coordinators reach out to members that still need services and provide education regarding the need to see a provider. Another area of member engagement is the Gaps in Care letters. Each letter identifies the gaps-in-care for the member and provides directives on how to meet the healthcare needs. A copy of the gaps-in care letter is also sent to the member’s provider. Objective: To improve member reported satisfaction and overall quality of services. To engage members in their own healthcare planning; thus creating a collaborative effort to meet member’s needs. Overall objective is to ensure that members close their gaps-in-care through collaborative efforts as will be evidenced by reaching the 75th percentile rates on reported measures. Rapid Cycle Improvement: CCAI systematically and methodically measures the set objective by monthly assessments of HEDIS/HQOL rates, identifying continued gaps-in-care and monthly gaps-in-care report distribution to Care Coordinators for member engagement, outreach and facilitation efforts.
Electronic Learning Media Resource (ELMR) To ensure continued education and high quality of services, a web-based educational program is offered through an Electronic Learning Media Resource (ELMR). CCAI develops learning modules to educate the staff on subjects related to safety and quality of clinical and non-clinical services. Intent of ELMR is to maintain staff highly aware and motivated to provide and execute high quality services.
Clinical Practice Guidelines Evidenced-based clinical practice guidelines are adapted and annually reviewed in order to monitor and improve quality and safety of clinical care provided by participating practitioners. Clinical practice guidelines are adopted from accredited healthcare bodies. The QI/UM Committee reviews current clinical care guidelines, adapts new or updates current guidelines and presents them to the Peer Review Committee for approval. Once Peer Review Committee approves the guidelines notification of the new clinical care guidelines approval and availability is communicated to the providers via provider newsletter, CCAI website and network meetings. Currently the following guidelines have been adapted and distributed for the listed, but not limited to, conditions/services:
18
a. Asthma b. Chronic Obstructive Pulmonary Disease (COPD) c. Congestive Heart Failure (CHF) d. Coronary Artery Disease (CAD) e. Diabetes (DM) f. Cerebrovascular Accidents and Transient Ischemic Attacks (CVA & TIA) g. Preventative guidelines:
i. Adult Immunizations ii. Cervical Cancer Screening
iii. Colorectal Cancer Screening iv. Breast Cancer Screening v. Prevention of catheter-associated urinary tract infections
vi. Prevention of Pressure Ulcers h. Early and Periodic Screening, Diagnostic and Treatment (EPSDT) for 19-20 year old
members i. Mental and Behavioral Health
i. Multiple disorder guidelines ii. Psychotropic medications guidelines
j. Tobacco Use and Dependence k. Nutritional guidelines l. Medication Management Guidelines m. Coordination of Community Support and Services for members enrolled in Home &
Community based waivers (HCBS) n. Transitions of Care in the Long Term Continuum o. Dental Services
Individuals Ages Nineteen (19) and Twenty (20) This population segment requires monitoring of preventive and age appropriate visits. Monitoring of this age group includes the following:
a. Immunization status. b. Number of hospitalization. c. Length of hospitalizations. d. Medical management for medically complicated conditions.
Pregnancy Related Activities: Objective in monitoring this population is to ensure timely pre ad perinatal care, services and monitoring entails analysis and Care Coordination of the following:
a. Timeliness and frequency of prenatal visits. b. Provisions of ACOG recommended prenatal screening tests. c. Birth outcomes. d. Referral to the Perinatal Centers, as appropriate. e. Length of hospitalization for the mother.

19
f. Length of newborn hospital stays for the infant. g. Assist the member in finding appropriate provider for the infant.
Hypertension Improvement Project: Hypertension (HTN) has been identified, through BCAP typology, as a prevalent condition for the population served. In order to reduce HTN associated morbidity and mortality, this CCIP intends to improve quality of care pertaining to this disease domain by ensuring that members have adequate access to care, understand HTN disease process through member education provided by Care Coordinators, and improved pharmaceutical compliance. Objective: The primary objective is to improve clinical outcomes for the target population by improving control of high blood pressure, improving adherence to hypertension medication, and improving the rate of visits to members’ PCP and to increase HTN drug class pharmaceutical compliance to 80% for target population. Rapid Cycle Improvement: Systematically monitor set objectives through HQOL/HEDIS® Access to Ambulatory and Preventive Care (AAP) measure to evaluate on-going access to care and identify any barriers. Monitor Care Coordination interactions on a quarterly basis with the target population to assess current state of condition and provide educational guidance.
Member-directed Gaps in Care Letters: Addressing quality of clinical care starts with identification of healthcare needs. CCAI believes that proper member engagement and outreach will ensure that quality care is achieved. Identified gaps in care are communicated to members in writing and are sent to members. A copy of the gaps in care letter is also sent to the member’s provider. Collaboration of outreach efforts and keeping the member and provider informed of gaps-in-care will have a positive impact on the quality of clinical care as member’s needs will be addressed during provider visits. Objective: To improve quality of care to the member by educating them and informing their providers of gaps in care as per national guidelines. Overall objective is to ensure that members close their gaps-in-care through collaborative efforts with their PCP and Care Coordinator as evidenced by reaching the 75th percentile rates on pertinent measures. Rapid Cycle Improvement: Systematically measures the set objective by monthly assessments of HEDIS rates, identification of continued gaps-in-care and facilitation of monthly reports to Care Coordinators.

20
Provider education: In order to keep providers well informed of the plan’s activities, required HEDIS/HQOL reported measures and overall HEDIS/HQOL driven care requirements: diagnostic, management or preventative, CCAI uses a multimodal approach to educating providers regarding quality activities. Providers are notified of any operational, quality improvement updates on a quarterly basis through the company website and a Provider Newsletter which is published quarterly. QI, along with the network staff, discuss initiatives, projects and updates during each provider/network encounter.
a. Introduction to HEDIS – what it is, what is the significance, reporting timelines. b. Reportable measures, measure definitions, measure descriptions along with source of
measure, e.g. HEDIS, State of Illinois or State modified measures. c. Medical Record Abstraction tool – identifies needed data points from medical record for
medical record dependent measures. d. Clinical Practice Guidelines. e. 2016 QIP Goals and objectives.
Care Coordination HEDIS Education Several activities are taking place to educate the Care Coordination Team in order to ensure complete understanding of HEDIS/HQOL and what is entailed in this process to measure the quality of care of its members. HEDIS education will be provided upon on-boarding through ELMR. Objective: To educate Care Coordinators on HEDIS/HQOL processes and performance measures for the purpose of improved quality of care.
HEDIS / HQOL: CCAI actively participates in the HEDIS/HQOL reporting by collecting, analyzing and reporting all required State of Illinois performance measures to ensure that members have proper access to care and are able to address all healthcare needs accordingly. Interventions provided to members include mailing letters, postcards, and direct contact with Care Coordinators. Letters and Postcards notify members of needed healthcare activities. Messages to members are kept brief, made available in multiple languages and comply with health literacy guidelines. Various educational materials have been developed on chronic conditions such as COPD and Diabetes that Care Coordinators can mail to the members. These educational materials empower members with knowledge about their conditions as well as needed provider visits or laboratory testing. CCAI reports on the following seven (7) domains of care:
a. Effectiveness of Care b. Access/Availability of Care c. Experience of Care d. Utilization and Risk Adjusted Utilization

21
e. Relative Resource Use f. Health Plan Descriptive Information g. Measures Collected Using Electronic Clinical Data Systems
This process allows for clear evaluation of the quality of care received by members which result in positive health outcomes. Objective: To assess effectiveness, access and availability of care, to review utilization data and to improve how members’ needs are met. Rapid Cycle Improvement: Systematically assess and evaluate performance rates to develop and implement Quality Improvement activities based on results.
F. Collaborative QI Activities [QI1A1]
Care Coordination Performance Improvement Project (PIP): In September 2015 DHFS has implemented a collaborative Care Coordination PIP with all managed care organizations in the state of Illinois to target the high and moderate risk stratified population. Goal of this PIP will be to decrease the rate of readmissions and increase the rate of follow up post hospitalization. The intent of the Care Coordination PIP is to explore the relationship between care coordination, timely ambulatory care services and readmissions within 30 days post discharge for moderate to high risk members. Interventions will be targeted towards increase care coordination. Objective: The primary objective of the Care Coordination PIP will be to reduce the rate of readmissions for the high and moderate risk target population. As this PIP is still in the developmental stages, DHFS has not issued explicit quantitative goals at this time.
Behavioral Health Process Improvement Project (PIP) In September 2015 DHFS has implemented a collaborative PIP with all managed care organizations in the state of Illinois to target the behavioral/mental health-related population; specifically individuals who experienced an inpatient admission for behavioral/mental health reasons. Purpose of this project is to facilitate post hospital discharge follow up with a provider in order to reduce readmissions in the behavioral/mental health population. As per DHFS there is a clinical significance associated with this initiative as “about one in four adults in the United States lives with a mental illness, those who experience a mental illness are less likely to use medical care and follow treatment plans. Each year, on average, 60 percent of adults do not
22
receive the mental health services they need.” Baseline data was collected in 2015. 2016 will serve as a measurement year. Objective: Reduce preventable readmissions for the behavioral/mental health target population by facilitating follow up with a provider within 7 days and 30 days post behavioral/mental health hospitalization and reach the 50th percentile rate for both sub-measures. Rapid Cycle Improvement: CCAI will systematically monitor set objectives through NCQA’s: HEDIS Follow up After Hospitalization (FUH) measure that is further sub-categorized into two (2) sub-measures: 7 days and 30 days follow up. Monitoring and reporting will take place quarterly.
VI. Behavioral Healthcare [QI1A2, QI1A5]
A. Monitoring and Improving Behavioral Healthcare CCAI has developed a robust behavioral health network in order to serve the behavioral healthcare needs of our members within the community in which the members reside. CCAI collaborates with its behavioral health providers via care coordination and case management, which enables CCAI to collect and analyze data and implement actions to improve the coordination of behavioral health care with medical care. Coordination of care between providers of medical and behavioral health services enables improved follow-up and continuity of care. In order to improve behavioral healthcare, CCAI has contracted with an external NCQA-accredited organization with behavioral healthcare experience which is delegated to provide behavioral healthcare inpatient and outpatient utilization management and behavioral health case management. The delegated organization will work directly with behavioral healthcare providers and with CCAI’s internal care coordination staff to ensure continuity of care and management of members needing behavioral healthcare. The delegated organization will work with members and behavioral healthcare providers to develop a member care plan and provision of an appropriate level of care.
CCAI will conduct regular meetings with the delegated organization to discuss operational issues and to ensure that behavioral healthcare is being provided to members in as optimal a manner as possible. The delegated organization will utilize CCAI’s care management system to carry out UM services and behavioral health case management services, allowing CCAI to monitor these functions in real-time and to recognize opportunities for improvement. In addition, the delegated organization will provide monthly and quarterly activity and productivity reports to CCAI.

23
B. Involvement of a Designated Behavioral Healthcare Practitioner [QI1A-5]
A designated behavioral healthcare practitioner is an active member of CCAI’s QI/UM Committee, and provides expertise regarding behavioral healthcare issues, utilization management issues, and quality improvement activities that serve the member population accessing behavioral healthcare services. The current designated behavioral healthcare practitioner is a medical doctor in psychiatry who is with a facility in CCAI’s provider network. A behavioral healthcare practitioner with the delegated organization is actively involved in implementing the behavioral healthcare aspects of the UM program.
VII. Serving a Diverse Membership [QI1A8] CCAI specialized in serving Seniors and Persons with disabilities. CCAI takes great pride in being able to acknowledge and provide services to its members from various cultural backgrounds. CCAI addresses the communication needs of its members and ensures the availability of language services to optimally engage, direct and support each member and his/her family and/or support systems. CCAI operates under the National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care (The National CLAS Standards). CCAI respectively observes, follows and oversees the Principal, Governance, Leadership, Workforce, Communication and Language Assistance, Engagement, Continuous Improvement and Accountability Standards under the National CLAS guidelines.
A. Cultural Competency plan: To ensure and operate a culturally competent plan for the purpose of best quality care for the members served with the purpose of providing services which value diversity, support member communication, reduce barriers and optimize health goals and outcomes. A Cultural Competence Plan is in place and is offered as a mandatory on-boarding training for all new hires.
B. Disability Community Stakeholder Forum CCAI has a Disability Community Stakeholder Forum. This committee is comprised of company and member stake-holders, addressing unique and cultural member needs. The charge of this forum is to serve as a liaison between the disability community and CCAI’s administrative leadership and governing board relaying consumer perspectives on policies and decisions and
24
helping shape and influence program design, implementation, oversight and evaluation in accordance with recommendations of the National Council on Disability.
C. Educational Material at 6th grade reading level All written communications to the members are written at a 6th grade level.
D. Multi-lingual printed material Educational and enrollment information is translated to meet the linguistic needs of the members. Translations are verified by a certified vendor.
E. Language Line In the event a member speaks other languages than English, Polish or Spanish, CCAI is contracted with Argo Translation Language Line Services to ensure proper communication between members and the HealthCare Management team. This service is available to members and staff 24 hour a day. Access to TTY services is also available to meet the needs of the hearing-impaired population.
F. Hiring Diverse Employee Base: CCAI is committed to establishing and maintaining a diverse workforce that is representative of the people in the areas served. Employment opportunities are available for all people regardless of race, color, creed, ancestry, gender, marital status, national origin, age, political or religious affiliation, sexual orientation, mental or physical disability, and any other protected classification and follow all Equal Employment Opportunity Commission’s mandates. Care coordinators who speak languages other than English are recruited. Currently there are Care Coordinators available who are fluent in Polish and Spanish. CCAI makes it a priority to assign culturally competent and paralleled Care Coordinators to each unique member.
VIII. Serving Members with Complex Health Needs [QI1A9]
A. Complex Case Management (CCM) The CCM program addresses the complex healthcare needs of the most vulnerable members. CCM recognizes vulnerable members by evaluating individualized utilization costs: (hospitalizations, readmissions, ED visits), uncontrolled conditions, pharmaceutical non-compliance and predictive modeling risk stratification by identifying members that fall in the top 1% for risk score and top 1% for costs- which is determined by using predictive modeling system.
25
Objective: To manage complex healthcare needs of identified at-risk members by driving and directing well-coordinated resources toward recovery of optimum health and functional capacity. Rapid Cycle Improvement: monthly assessments and evaluations of predictive modeling risk stratifications, monthly assessment and evaluation of the Utilization Management reports. Annual comprehensive overview of the program’s success and identification of areas for improvement.
B. Disease Management (DM) DM program addresses the disease processes for select diseases prevalent among the membership. Through this program, identified members will have additional resources (facilitation, education) that will assist them in management of their conditions. The intent of this program is to minimize morbidity and mortality associated with member-identified prevalent diseases. This program is driven and established based on evidence based clinical guidelines that have been adopted by CCAI. Ultimate goal of this program is disease control and improved quality of life. Objective: To provide DM enrolled members with appropriate resources (facilitation, education) as directed by the CCAI’s adapted evidence based clinical guidelines that would result in optimal disease control/management. Rapid Cycle Improvement: Systematically monitor the effectiveness of the DM program with monthly assessments of Predictive Modeling risk levels, medical conditions and gaps in care.
C. CMDM report analysis: Case Management/Disease Management (CMDM) report identifies risk stratified members and current risk-driven trends. Intent of this evaluation is to reallocate care coordination resources based on identified trends and weighted risk score in order to meet each member’s healthcare needs. Objective: To allocate appropriate resources to identified at-risk groups. To ensure that the at-risk identified members have appropriate resources to improve their health status. Rapid Cycle Improvement: Systematically monitor the CMDM trends through monthly assessments and evaluations of the CMDM report, weekly assessments and evaluations of Risk-stratification (cases work-load) report, reassignment of cases based on identified risk and their associated risk-weights.
26
D. Waiver Audits This membership also receives Home and community-based waiver services HCBS): aging, persons with disabilities, supportive living facility, traumatic brain injury and HIV/AIDS. Members who are enrolled and receive the HCBS waiver services need significant degree of assistance with their ADLs and IADLs in order to remain in their communities and reduce the risk of hospitalization while minimizing co-morbidities and enhancing quality of life. The intensity of managing HCBS members is appropriately weighted in the Care Coordinator’s case-workload report as these members require additional support and resources to meet members’ needs. To ensure HCBS waiver services compliance Care Coordination audits are performed to confirm that all approved services are delivered. Objective: To ensure all HCBS enrolled member needs are identified, addressed, services delivered and properly documented. Rapid Cycle Improvement: Systematically monitors the efficiency, effectiveness and waiver compliance by:
1. Performing Waiver Audits based on risk stratification : a. Initially: at least once within 90 days of Care Coordination’s employment. b. Randomly: throughout the calendar year all Care Coordinators are audited at least
quarterly. c. Performance Based: when performance, e.g. quality of work, Care Coordination
concerns are identified. d. Remediation Audit: the same 3-5 members are re-audited when there are findings
for an initial, random or performance-based audit. e. P-D-S-A methodology: identify barriers and areas of improvement, modify
processes, monitor effects of modified processes, continue to monitor systematically and act accordingly.
IX. Patient Safety [QI1A3]
A. Medication Reconciliation Avoidance of the duplication of medications or life-threatening drug-drug interactions is a must when it comes to safety initiatives. Medication reconciliation ensures that a member is compliant with all prescribed medications for the purpose of disease/condition treatment and/or management. Additionally, this process allows for members to understand their medications. Medication errors/abuse/overuse can contribute to the overall morbidity, mortality and overall

27
cost of care. Lack of medication reconciliation for members post hospital/facility discharge can lead to a higher re-admission rate due the aforementioned factors. Objective: The primary objective of this activity is to ensure member safety as it relates to medications: avoid adverse events, avoid duplication of medications/over medicating, increase medication compliance, and avoid potentially life-threatening/altering drug-drug interactions.
B. HTN Improvement Project Please refer to Quality Improvement Activities section for a detailed outline of this project.
C. Flu Campaign During the months of September through April, Care Coordination performs active outreach efforts to educate on and facilitate the flu vaccinations. The campaign starts off in early fall with informational mailings to all enrolled members regarding the flu and the need for vaccination. The campaign proceeds with its efforts by identifying members who are at-risk based on the Center for Disease Control (CDC) risk identification:
1. High Risk: a. Adults 65 years of age or older b. Pregnant Women c. American Indian or Alaskan Natives d. High risk members as defined by Predictive Modeling stratification
2. Chronic Diseases: a. Asthma b. Neurological Conditions: TBI, SCI, Cerebral Palsy, Epilepsy, Stroke, Dementia c. Lung disease: COPD, Cystic Fibrosis d. Heart Disease: Congenital, Heart Failure, Coronary Artery Disease e. Blood Disorders: Sickle Cell Anemia f. Endocrine Disorders: Diabetes g. Kidney Disorders h. Liver Disorders i. Compromised Immune Systems: HIV/AIDS, Malignancy j. Morbid Obesity: BMI ≥ 40.
Outreach efforts for the high risk members are completed telephonically. On-going monitoring of members’ flu vaccination status allows for a second mailing post telephonic outreach to capture the members that have not been vaccinated yet after two (2) outreach efforts.
28
Objective: To increase overall flu immunization status for the membership, to increase knowledge of the benefits of the flu vaccine and to minimize any risk to members’ health due to lack of the flu vaccination. Rapid Cycle Improvement: Monitoring of this activity is accomplished by monitoring of flu-focused interactions between Care Coordination and identified as at-risk members, monitoring of all members and their flu vaccination status via review of encounter data and pharmacy reports.
D. Flu Campaign for the Care-Coordinators: Care Coordinators operating within Anchor Health Homes are required to receive flu vaccinations. If staff declines to receive the flu vaccination, they must take additional precautions when in direct contact with a member, such as wearing a mask during flu season while working at the AHH. CCAI also provides on-site flu vaccinations available to all staff on an annual basis.
E. HEDIS / HQOL Please refer to Quality Improvement Activities section for a detailed outline of this process.
F. ELMR Please refer to Quality Improvement Activities section for a detailed outline of this project.
X. Quality Improvement Program Structure
A. Roles and Responsibilities [QI1A1, QI1A4, QI1A6]
Board of Directors The CCAI Board of Directors (BOD) has the ultimate responsibility to establish, maintain, and support CCAI’s Quality Improvement Program and Plan through CCAI’s Administration and participating health care providers. The BOD delegates these responsibilities to the CCAI President who further delegates this responsibility to the Chief Operating Officer and Chief Medical Officer. Additional Board of Directors responsibilities include:
• Annual review and approval of the Quality Improvement Program and Plan, including
• Development and adoption of goals and objectives; • Oversight of CCAI's progress in meeting the established goals and objectives;
and, • Annual review and approval of the QI evaluation.
29
President The President maintains full authority over all aspects of daily conduct and general administration of the Health Plan to ensure that the requirements set forth in the State of Illinois Health and Family Services Contract are met. The President reports directly to the CCAI Board of Directors.
Chief Operating Officer The COO reports directly to the President/CEO. As delegated by the President /CEO, the Chief Operating Officer (COO) oversees all aspects and integrated functions of the health plan. The COO ensures that prioritization and execution of mission-critical elements of the CCAI Quality Plan and Utilization Management / Transition of Care Program occur through alignment of goals, objectives and organizational resources. Chairs (or designates chairperson) of Grievance Committee.
The Chief Medical Officer [QI1A-4] The Chief Medical Officer reports directly to the President and is a member of the CCAI executive staff. The Chief Medical Officer serves as a representative to group medical directors and participating physicians, and functions as a conduit of communication from the participating providers to CCAI staff. The Chief Medical Officer assumes an important role in promoting CCAI within the community and to prospective participating physicians. The Chief Medical Officer works closely with the medical groups to promote the mission, vision and values of the organization and plays a vital role in the development and oversight of the Quality and Utilization Management / Transition of Care programs. Other key functions of Chief Medical Officer include:
• In collaboration with the VP-Population Health & Quality (VPPHQ), oversees all clinical functions of the Quality Program and provides leadership and direction to the clinical teams.
• Chairs or designates chair for the CCAI Quality Improvement/Utilization Management and Peer Review Committees.
• Represents the committees to participating professionals on matters of medical practice, policy, quality of care, cost control and complaint resolution, grievance and utilization review programs.
• In collaboration with the VPPHQ, VPHCM (VP-Health Care Management) and VPUT (VP Utilization Management & Transitional Care), serves as an executive sponsor for focused quality studies and improvement initiatives.
• Monitors care and services throughout the continuum among providers: hospitals, skilled nursing facilities and home care agencies to ensure quality, costs-efficiency and continuity of care and recommends/ oversees corrective actions for improvement, when indicated.
30
• Oversees the development of Healthcare Management policies and compliance standards to assure the delivery of quality, cost-effective health care and medical services.
• Collaborates with Finance in Medical Economics initiatives. • Educates and interacts with network and group providers and medical managers
regarding utilization practices, guidelines, pharmacy utilization and effective resource management.
• Partners with the Network Management Department for contract negotiations. • Ensures medical care providers meet standards for acceptable medical care and
medical protocols and rules of conduct are followed. • Reviews claims and appeals, and resolve grievances related to medical quality of
care. • Participates in regulatory, professional and community activities to provide input
and become knowledgeable regarding regulatory, professional and community standards and issues.
• Strategy development and implementation of innovative clinical programs that include collaboration with strategic business partners.
• Intervenes as necessary in evaluating and implementing corrective actions toward the resolution of member complaints. Serves as an intermediary when there are disputes between providers and members.
• Approves all health education materials sent to enrollees. • Serves as a medical resource to CCAI management and staff
Medical Director: [QI1A-Factor 4] The Medical Director reports directly to the Medical Director, serves as a representative to group medical directors and participating physicians, and functions as a conduit of communication from the participating providers to CCAI staff and key leadership. The Medical Director maintains an important role in promoting CCAI within the community and to prospective participating physicians. In collaboration with the Chief Medical Officer, the Medical Director works closely with medical groups to promote the mission, vision and values of the organization and plays a vital role in the development, implementation, and oversight of the Quality and Utilization Management/ Transition of Care programs. Other key functions of Chief Medical Officer include:
• Assists in the development of the formal Utilization Management, Care Management and Quality Improvement Plans.
• Develops and implement medical policies and procedures. • In collaboration with the Chief Medical Officer, VPHCM, VPPHQ, & VPUT,
provides direction for the development, implementation, administration and

31
evaluation of the Quality Improvement Program, the UM Program, and the Case Management Program.
• Participates in risk management, pharmacy utilization management, catastrophic case reviews, outreach programs, HEDIS reporting, site visit review coordination, provider orientation, credentialing, and profiling.
• In collaboration with other responsible individuals and committees, establishes and maintains medical policies, treatment guidelines, quality indicators, standards of care, UM and CM policies and procedures
• Chairs and directs the activities of the QI/UM Committee and co-chairs the Professional Peer Review Committee toward stated objectives as reflected in the Quality Plan.
• Identifies those instances where the competence or conduct of a physician or other health care provider has an adverse effect on the patient care (and/or the goals of CCAI) and takes appropriate action.
• Promotes wellness and ensures programs of prevention, education and outreach to members and providers are consistent with CCAI's mission, vision and values.
• Monitors practitioner practice patterns, identifies opportunities for improvement, and recommends corrective actions.
• Works collaboratively with medical groups' Medical Directors to maintain compliance with the medical aspects of the formal CCAI-Provider agreements.
• Provides information and education to physicians and other providers related to the delivery of medical services.
• Reviews claims and appeals, and resolve grievances related to medical quality of care
Behavioral Health Practitioner: [QI1A-5] A licensed, CCAI- credentialed physician, who is board certified in Psychiatry, formally serves as an appointed member of the CCAI Quality and Utilization Management Committee. The behavioral health physician reviews and advises the Committee on behavioral health matters, including but not limited to, evaluation of mental health pharmacy data, patterns of provider care delivery and clinical care outcomes, performance of the UM delegate(s), mental health utilization, and the appropriateness of the authorization process for mental health services. This practitioner may also participate in weekly interdisciplinary behavioral health rounds, and reviews/consults on behavioral health treatment plans and medication utilization as needed.
VP of Healthcare Management The Vice President of Healthcare Management is responsible for all healthcare management activities.

32
• Requires regular interaction with executives of medical groups, community representatives, state regulators, external auditors and plan executives and managers
• Develops and implements departmental goals and objectives with the Medical Director to insure successful accomplishment of corporation mission, goal and objectives
• Develops and implements departmental policies and procedures • Implements care management assessments and protocols to insure FHN & CCAI
members receive the appropriate care, counseling and education • Implements disease specific programs to improve outcomes in care and disease
management • Insures protocols are implemented and monitored for delegated services in the
areas of healthcare management • Analyzes reports and develops report specifications to monitor departmental
activities • Responsible for participating in the Quality/Utilization Committee and Peer
Review Committee, assisting the Medical Director in all committee activities • Reviews and approves reports as necessary, including state mandated reports • Assures appropriate implementation and continued compliance with Care
Coordination, performance improvement plan, reviewing plan annually and processing all aspects of corrective action plans
• Works with and supports all levels of staff in problem solving issues related to medical care
• Attends relevant meetings, HFS meetings as FHN & CCAI representative expert in healthcare management
• Prepares reports for Board of Directors, HFS, HSAG and other accrediting organizations
• Oversees healthcare management activities to meet accreditation standards.
VP of Population Health and Quality The Vice President of Population Health and Quality reports directly to the Chief Medical Officer. In collaboration with the Medical Director, the VPPHQ oversees all functions and reporting responsibilities of the Care Management and Quality Improvement Programs. This includes quarterly reports of the program's activities to CCAI's President and Board of Directors. Other key functions of the VPPHQ include:
• In collaboration with the Chief Medical Officer and Medical Director, serves as an executive sponsor for focused quality studies and improvement initiatives.
33
• Approves the staffing plan and resources allocated to integrate Population & preventive health, and Quality Management programs toward achievement of organizational goals and objectives.
• Serves as a resource for CCAI management and staff. • Ensures that CCAI quality management structure and processes are adequate to
meet goals and objectives. Develops task forces, subcommittees and infrastructure as needed.
• Responsible for the NCQA / HEDIS, CMS STARS and HFS Quality Reporting and Medical Record Review Programs.
• Oversees the activities of QI/UM and Peer Review Committee(s). Charters and guides progress of quality initiatives.
• Reports process and outcome metrics to the QI/UM Committee, Executive Staff and Board of Directors;
• Oversees compliance with quality, regulatory, accreditation and peer review requirements in risk-delegated groups. Manages annual review and process for corrective action plans. Supports collaborative efforts to improve compliance of delegated functions by medical groups.
• Serves as steward for internal and external quality audits. • Develops and implements policies and procedures which support CCAI Healthcare
Management goals.
VP of Utilization and Transitional Care Management The Vice President of Utilization and Transitional Care reports directly to the Chief Medical Officer. In collaboration with the Medical Director, the VPUT oversees all functions and reporting responsibilities of the Utilization Management / Transition of Care Programs. This includes quarterly reports of the program's activities to CCAI's President. Other key functions of the VPUT include:
• In collaboration with the Medical Director, serves as an executive sponsor for focused studies and improvement initiatives.
• Oversees the design of policies and procedures that affect service delivery and standards of care.
• Oversees the appropriateness of referrals and admissions through the prior authorization programs.
• Approves the staffing plan and resources allocated to integrate Utilization Management/Transition of Care programs toward achievement of organizational goals and objectives.
• Serves as a resource for CCAI management and staff.
34
Chief Information Officer The Chief Information Officer reports directly to the President/CEO. As delegated by the President/CEO, the Chief Information Officer (CIO) is responsible for the development, maintenance, and oversight of the Health Plan enterprise systems, their functionality, integration, and integrity to support accurate analytics and reporting of health plan data to internal and external sources. Other key functions of the Chief Information Officer include:
• Works with IDHFS to ensure the timely and accurate receipt and transfer of member, provider and encounter data as defined and required under the HFS contract.
• Oversees and supports the timely reporting of business and healthcare analytics needed to facilitate prompt and accurate member and population care/disease management based on administrative data from management service organization (MSO) and group partners.
• Drives and oversees management of IT vendor partners and the services they provide.
• Ensures that the staffing and technology resources allocated to data, analytics and reporting for internal and external quality and performance improvement are aligned with goals and objectives of the Quality Plan.
Chief Financial Officer The Chief Financial Officer reports directly to the President/CEO. As delegated by the President/CEO, the Chief Financial Officer (CFO) is responsible for the administrative and financial risk management operations of the company, to include the development of a financial and operational strategy, metrics tied to that strategy, and the ongoing development and monitoring of control systems. Other key functions of the Chief Financial Officer include:
• Strategic planning to assist in formulating direction and supporting tactical initiatives
• Managing the capital request and budgeting processes • Develops and reports performance measures that support the company's
strategic plan, and provides timely reports to medical groups and providers as to their earning potential and opportunities for improvement in financial management.

35
Chief Compliance Officer The Chief Compliance Officer reports directly to the President/CEO. As delegated by the President/CEO, the Chief Compliance Officer (CCO) is responsible for the development and oversight of all aspects of the CCAI compliance plan. Other key functions of the Chief Compliance Officer include:
• Works with the IDHFS Office of the Inspector General (OIG) in investigating and responding to suspected fraud, abuse, and misconduct in accordance with CCAI administrative policies and/or IDHFS recommendations as appropriate.
• Oversees internal and external audit preparation and follow up activities. • Chairs (or designates chairperson) of Compliance Committee. • Chairs (or designates chairperson) of Delegation Oversight Committee.
B. Functional Areas [QI1A1, QI1A4, QI1A6]
1. Operations Overseen by the Chief Operating Officer. The Operations division aligns health plan activities supporting member and provider communication and relationships with functional areas including data throughput and analytics. The Project Management Department is a cross functional unit which deploys skilled management support to mission-critical Health Plan initiatives. Network Management department houses staff that are responsible for credentialing file management and preparation for review by the Professional Peer Review Committee.
2. Healthcare Management Overseen by the Chief Medical Officer. The Healthcare Management division responsibilities and key leadership functions are discussed in detail in the preceding section.
3. Compliance Overseen by the Chief Compliance Officer. The Compliance Department staff is responsible to ensure that Health Plan programs adhere to regulatory and statutory requirements set forth by HFS, CMS, and other governing bodies and/or accrediting agencies.
4. Information Technology Overseen by the Chief Information Officer. Information Technology ensures that the staffing and technology resources allocated to data, analytics and reporting for internal and external quality and performance improvement are aligned with goals and objectives of the Quality Plan.
36
5. Finance Overseen by the Chief Financial Officer, the staff within this division are responsible for the financial risk management operations of the company, to include the development of a financial and operational strategy, metrics tied to that strategy, and the ongoing development and monitoring of control systems. This team works collaboratively with Healthcare Management teams on initiatives related to medical economics to promote cost-quality valuation.
C. Responsibilities of the Quality Improvement Team
1. Manager, Quality Improvement • Perform and monitor the quality management improvement functions per the Quality
Improvement Program Plan, its annual updates, and intermittent quality and/or performance improvement plans.
• Supervises staff that performs quality assurance/improvement activities on a daily basis. • Conducts all aspects of HEDIS/medical evaluation studies including data collection,
analysis, evaluation and reporting. • Ensures implementation of all quality improvement strategies across the entire network. • Monitors and reports quality performance to internal committees, workgroups and
external groups as assigned. • Supports analysis of CCAI metrics and operational performance to prioritize and assist in
development of improvement initiatives. • Attend QI/UM Committee meetings and other meetings as assigned.
2. Quality Improvement Specialist • Perform and monitor the quality management improvement functions per the Quality
Management Plan, its annual updates, and intermittent quality and/or performance improvement plans.
• Conducts all aspects of HEDIS/medical evaluation studies including data collection, analysis, evaluation and reporting.
• Ensure implementation of all quality improvement strategies across the entire network. • Assist medical groups in meeting CCAI QI goals. • Functions as a knowledge expert for quality improvement activities, educating staff and
providers of the quality measures and the QI process. • Attend QI/UM Committee meetings.
3. HEDIS Analyst • Evaluate workflows within clinical and operational systems and plans, coordinates,
verifies and distributes reports on key quality and clinical measures.

37
• Ensure report specifications for process and outcome measures are valid, reliable and accurate.
• Conduct analytics as required and assembles reporting templates / dashboards based on specifications and regular report feeds.
• Collaborate with IT team to manage data needs of clinical users

38
D. Organizational Chart [QI1A1]
Health Plan Functional Areas and Staffing
E. Committee Structure and Oversight [QI1A-6] Responsibility for CCAI’s QI program is integrated throughout the organization, and involves several committees as well as committees jointly shared by CCAI and FHN that fulfill specific functions. The committees involved in CCAI’s QI program consist of the following:
1. CCAI Board of Directors a. CCAI QI/UM Committee
i. CCAI Consumer Advisory Committee ii. Peer Review Committee (FHN/CCAI)
1) Credentialing Committee (FHN/CCAI) iii. HEDIS Oversight Committee iv. Delegated Oversight Committee (FHN/CCAI) v. Cultural Competency Work Group (FHN/CCAI)
Board of Directors (2)
President
Operations
Member Services/ HRS
Network Mgmt/ Credentialing
Project Management
Healthcare Management
Medical Director
Utilization Management /
Transitional Care
Care Management
Education/ Quality
Management
Compliance Information Technology Finance

39
vi. Customer Service Quality Committee (FHN/CCAI) vii. Compliance Committee
The CCAI QI/UM Committee and the Compliance Committee report to the CCAI Board of Directors. The Compliance Committee reports Quality-related complaints and grievances to the QI/UM Committee Board; all other Compliance issues are reported to the Board of Directors. All other committees listed above report to the CCAI QI/UM Committee. Those committees which are shared with FHN also report to FHN’s Board of Directors. The Credentialing Committee (FHN/CCAI) reports to the CCAI Peer Review Committee. The CCAI Peer Review Committee reports to the CCAI QI/UM Committee.
CCAI Quality Improvement Committee Structure
1. CCAI’s Board of Directors Role: CCAI’s Board of Directors, as the governing body, has the ultimate responsibility to establish, maintain, and support the QI Program through administration and through the participating health care providers.
Key Responsibilities and Functions: The Board of Directors is responsible for:
• Annual review and approval of the QI Program and the QI Work plan. • Review regular reports from the QI Committee on performance and opportunities
to improve care or service.
CCAI Board of Directors
Quality Improvement/ Utilization Management
Delegated Oversight
CCAI Consumer Advisory
CCAI Peer Review(FHN/CCAI)
Credentialing Committee (FHN/CCAI)
Cultural Competency Work Group (FHN/CCAI)
Customer Service Quality Committee
(FHN/CCAI)
Compliance

40
• Review QI/UM Committee reports to determine progress in meeting QI objectives and goals.
• Recommend modifications to the QI Program as needed. • Review the annual QI Program evaluation.
Reporting Relationships and Structures: The Board delegates the responsibility to establish, maintain, and support the QI Program to the CCAI President who further delegates this responsibility to the CCAI Medical Director and the CCAI VP of Healthcare Management. The CCAI Medical Director and the VP of Healthcare Management collaborate with the Director of Quality Improvement on the implementation and evaluation of the plan.
Meetings: Quarterly
F. QI/UM Committee/Oversight of QI [QI1A1, QI1A4, QI1A5, QI1A6] [QI2A1, QI2A2, QI2A3, QI2A4, QI2A5]
1. CCAI QI/UM Committee Role: The QI/UM Committee provides oversight and approval of quality improvement and utilization management activities and programs for CCAI.
Chaired by: CCAI Medical Director
Membership: Members of the Committee include the following (* indicates voting member):
i. Medical Director* ii. Behavioral health practitioner
iii. Anchor Health Home Provider representative* iv. Contracted Practitioners and Providers* v. Contracted practitioners and providers with specialties*
vi. Specialty service providers as appointed* vii. Chief Compliance Officer*
viii. Vice President Population Health and Quality* ix. Vice President Health Care Management* x. Vice President Utilization Management and Transitional Care*
xi. Vice President Network Management* xii. Director of Quality Management*
xiii. Director, Utilization and Transitional Care Management xiv. Director of Pharmacy Services* xv. Director LTSS
xvi. Director Nurse Care Coordination
41
Key Responsibilities and Functions: The QI/UM Committee responsibilities include the following:
QI/UM Committee Core Responsibilities:
i. Recommend policy decisions. ii. Analyze and evaluate the results of QI activities.
iii. Ensure practitioner participation in the QI program through planning, design, implementation or review.
iv. Identify needed actions. v. Ensure follow-up as appropriate.
QI/UM Committee Functions i. Review, evaluate and approve CCAI’s QI Program Plan and QI Work Plan at
least annually. ii. Review and oversee the QI Work Plan and QI activities and programs to ensure
timely completion of initiatives and reporting. iii. Identify, plan, implement and evaluate the Quality Improvement/Process
Improvement projects and monitor care outcomes and HEDIS measures. iv. Review key operational and clinical reports periodically, and at least annually
to identify opportunities for improvement. Review of CCAI’s administrative functions in order to identify opportunities for improvement. This will be done through review of grievances, telephone calls to services, satisfaction surveys, employee suggestions, etc.
v. Provide oversight for subcommittees’ QI initiatives and reporting to the QI Committee.
vi. Review, recommend and approve policies and procedures for effective operation of QI program, to include those related to utilization management, network management, credentialing and re-credentialing, members’ rights and responsibilities, member connections, and Medicaid benefits and services.
vii. Review and approval of practice guidelines utilized by the plan and develop clinical pathways for care management.
viii. Appoint subcommittees on a permanent or ad hoc basis, depending on the nature of the areas to be studied and evaluated and the specific needs of CCAI. The QI/UM Committee can determine the composition of any subcommittee as specific needs arise. Examples of future subcommittees may include:
1) Clinical Subcommittees 2) Medical Records 3) Pharmacy and Therapeutics 4) Utilization Management

42
5) Claims Review ix. At such times as these additional subcommittees may be formed, the QI/UM
Committee will serve in a coordinating function for all operations of these committees.
x. Membership for subcommittees will be selected from CCAI’s participating Anchor Health Home provider or other PCPs in the network and any other professional contracted providers as required by the CCAI Medical Director and/or the VP of Healthcare Management to meet CCAI’s objectives. The QI/UM Committee will make recommendations for the membership of each subcommittee. Membership on these committees will have a specific term as their role will be consultative and they will not determine policy. Members may be added or deleted at the discretion of the Medical Director along with advice from CCAI staff.
Reporting Relationships and Structures: i. Chairpersons of QI/UM Subcommittees and other Committees reporting up to
the QI/UM Committee will coordinate the required reporting of Subcommittee/Committee meeting minutes and metrics to the Committee as needed to evaluate performance and determine whether further action is required.
ii. Minutes from the QI/UM Committee meeting will be recorded and maintained as appropriate. Approved QI/UM Minutes will be reported to and approved by the CCAI Board of Directors.
iii. QI Department staff report to the Director of Quality. iv. QI Department staff are not members of the QI/UM Committee but do attend
QI/UM Committee meetings and are actively involved in multidisciplinary work groups tasked with planning, designing and implementing QI and HEDIS-related activities as outlined in the QI Program Plan and the QI Work Plan.
Procedures i. A majority (50% or more) of the Committee voting members or their
designee(s) shall be present to constitute a quorum for the transaction of the Committee's business which includes minimum of three practitioners.
ii. Committee voting cannot take place unless a quorum is present. iii. The Committee may take action through the vote of a majority (50% or more)
of the quorum present. iv. Members must be present in order to vote on Committee matters. Member
presence via telephone or video conference is acceptable. v. Committee activities will be documented by meeting minutes which are
reviewed and approved by the Committee and signed by the committee Chairperson or designee.

43
Agenda: The Medical Director in collaboration with Vice President of Healthcare Management and the Director of Quality Improvement is responsible for organizing the agenda for each meeting and ensuring that the Committee uses its time and resources to adequately manage the activities for each of its functional areas according to established goals and objectives.
Meetings: The Committee meets quarterly, or more frequently, as determined by the Medical Director.
Minutes: Meeting minutes are reported to the CCAI Board of Directors.
G. Committees [QI1A6]
1. Consumer Advisory Committee Chaired by: Director of Member Services
Membership: Randomly selected members, family members and other caregivers. CCAI appoints 8 random members to serve on the committee. Upon selection of the eight (8) individuals, CCAI will appoint four (4) members to serve a two (2) year term and four (4) members to serve a one (1) year term. Upon completion of these terms, CCAI will either re-appoint a committee member or appoint a new member.
Responsibilities and Functions: i. Provide member perspective of CCAI performance
ii. Recommend program enhancements based on the member needs: 1) review Provider and member satisfaction survey results; 2) evaluate performance level and telephone respond timelines;
iii. Evaluate access and provider feedback on issues requested by QI/UM Committee;
iv. Forward specific complaints to CCAI for resolution. Meetings: Quarterly
Minutes: Meeting minutes are reported to the QI/UM Committee.
2. Peer Review (PR) Committee Chaired by: CCAI Medical Director
Membership: i. Anchor Health Home Medical Directors (or physician designees)
ii. Other practitioners including nurse practitioners representative of all PCPs and specialties (e.g. Family Practice, Internal Medicine, Obstetrics/Gynecology, Dentist and General Practice),
iii. Other specialists will be consulted on an as needed basis,
44
iv. CCAI Medical Director, v. Medical Director of Behavioral Health
vi. The CCAI VP of Healthcare Management, vii. Other CCAI UM/QI staff, CCAI provider/credentialing staff - for the
credentialing portion of the meeting only
Responsibilities and Functions: i. Peer review is specifically the process by which individual providers of care,
behavioral health services, waiver and long term care services are reviewed and evaluated for patterns of care and utilization of resources where instances of care delivery vary from the established standards.
ii. Receive specific cases and/or incidents for review from the Medical Director. Member records may also be reviewed according to diagnosis, condition, procedures, medications, referral, and outcome. In general, sources of items for peer review include:
1) Individual claims and aggregate claims data; 2) Routine and special UM reports indicating performance that varies
significantly from established policies and standards; 3) UM reports indicating significant deviations from normative standards
relative to costs, to procedures, to quality or type of services used and to the outcome(s) derived;
4) Member complaints; 5) Member survey results; 6) Enrollment and disenrollment reports; 7) Review of provider practice patterns; 8) Provider office site visits; 9) Ambulatory medical record reviews; 10) Studies analyzing patterns of clinical care and services; 11) Potential quality of care issues; 12) Provider site visit reports by the IDHFS/CMS and, 13) Investigation by the Illinois Department of Financial and Professional
Regulation. i. Review for compliance with availability of services and access to care
standards through site visits’ reports, follow-up of member complaints and review of the results of the access monitoring tools. CCAI follows HEDIS and state of Illinois standards, which establish guidelines for access to primary and specialty care for CCAI members.
ii. Establish standards for credentialing and re-credentialing. Re-credentialing occurs every three years as per Illinois law.
45
iii. Complete annually at least two medical evaluation (administrative and/or clinical) studies that analyze pressing problems that were identified with the results and appropriate action taken. Brief follow-up study will take place for each medical evaluation in order to assess the actual effect of any action taken. Medical evaluation studies’ topics need Prior Approval.
Meetings: Quarterly, or more often as needed. Under the direction of Medical Director a quorum will be a minimum of five (5) provider committee members.
Minutes: Meeting minutes are reported to the QI/UM Committee.
3. Credentialing Committee (FHN/CCAI) Chaired by: FHN/CCAI Medical Director or Medical Director designee
Membership: i. CCAI Medical Director
ii. CCAI Behavioral Health Medical Director iii. Primary Service Providers as Appointed (5)
1) Internal Medicine (1) 2) Family Medicine (2) 3) Women’s Health and Obstetrics (2)
Responsibilities and Functions: i. Uses participating practitioners to provide advice and expertise for
credentialing decisions. ii. Reviews all data collected in accordance with the credentialing/re-
credentialing criteria. Credentialing policies provide an itemized list of the credentialing/ recredentialing criteria. Any and all QA/UM/PR data will be utilized in the recredentialing process. Reviews credentials for practitioners who do not meet established thresholds.
iii. Implements standards approved by the Peer Review Committee in recommending credentialing and recredentialing decisions to assure that each professional serving CCAI members is appropriately qualified and credentialed and that all license requirements are current.
iv. Ensures that files that meet established criteria are reviewed and approved by a medical director or designated physician.
v. Reports to Peer Review Committee.
Meetings: Approximately monthly, for a minimum of 10 meetings annually
Minutes: Meeting minutes are reported to the CCAI Peer Review Committee.
4. Delegated Oversight Committee (FHN/CCAI) Chaired by: Director of Compliance

46
Membership: Multi-disciplinary administrative leaders.
Committee members are as follows: i. CCAI Chief Operating Officer
ii. FHN Chief Operating Officer iii. Chief Compliance Office iv. Vice President of Network Management v. CCAI Vice President of Health Care Management
vi. FHN Vice President of Utilization Management vii. FHN Vice President of Care Management & Quality
viii. Vice President of Operations ix. Director of Pharmacy Services x. Director of Claims
Responsibilities and Functions: i. Oversight of all activities delegated to any subcontractor to which CCAI or FHN
delegates contractual responsibility; ii. Management of oversight and monitoring activities to ensure compliance with
the delegated clinical and administrative functions; iii. Ongoing assessment and evaluation of delegates to ensure performance
meets expectations and contractual requirements; iv. Review and analysis of delegate data to identify trends, opportunities for
improvement, and potential need for corrective action plan(s); v. Development and implementation of corrective action plans in response to
identified issues and trends; vi. Establishment of tracking mechanisms to monitor progress of corrective
action plans and routine evaluation of progress made against performance metrics; and
vii. Development and maintenance of performance goals and indicators.
Meetings: Approximately monthly, but no less than ten times per calendar year as the standard. Additional ad hoc Committee meeting and Subcommittee meetings may be as frequent as needed.
Minutes: Meeting minutes are reported to the QI/UM Committee.
5. Cultural Competency Workgroup (FHN/CCAI) Chaired by: Director of Compliance or designee.
Membership: Multidisciplinary CCAI leadership from key areas including Member Services, Network Management, Compliance, CCAI Quality Improvement.
Responsibilities and Functions:

47
i. Develop, oversee and monitor the CCAI Cultural Competency Plan. ii. Oversee all aspects of cultural and linguistic competency in the delivery and
support of healthcare services to members including: iii. Establish and enforce organizational policies which support culturally
competent business practices. • Strategy and method for establishing and maintaining a diverse workforce
that is representative of the people in the areas we serve. • Adherence to federal and State rules and regulations applicable to hiring
process such as those enforced by the Equal Employment Opportunity Commission.
iv. Establish initiatives to educate and monitor provider groups and practices in compliance with the CCAI Cultural Competency Program.
v. Approve communications and curriculum tailored to meet the diverse needs of the CCAI member population ensuring proper language and sensitivities to cultural, societal, racial, religious, ethnic, sexual and gender orientation, persons with disability, and communication topics and preferences.
vi. Maintains methodology to ensure that CCAI staff receive ongoing education which supports and aligns with the requirements of the Cultural Competency Plan.
Meetings: Bi-monthly.
Minutes: Meeting minutes are reported to the QI/UM Committee.
6. Customer Service Quality Committee (FHN/CCAI)
Chaired by: Vice-President Operations
Membership: Multi-disciplinary leadership from key areas including Member Services, Network Management, Compliance, Information Technology, Communications, Operations, Human Resources, CCAI Quality Improvement.
Responsibilities and Functions: i. Oversees the delivery of consistently high quality service to CCAI and FHN,
members and providers. ii. Responsible for the comprehensive assessment and oversight of customer
service programs at FHN and CCAI to ensure that the “voice of the customer” is been integrated to program planning and monitoring activities.
iii. Ensures the systemic analysis of service access and quality of service provided to valued members and providers.
iv. Ensures that program planning, action steps, and performance improvement objectives are structured to deliver the highest quality experience possible to members, providers and other internal/external customers of the Health Plan.
v. Ensures compliance with relevant contract, accreditation, and state and federal requirements.

48
vi. Adopts a formal, continuous quality improvement process, to facilitate open and effective communication among internal departments and oversight committees for the benefit of FHN and CCAI members and providers.
Meetings: Monthly.
Minutes: Meeting minutes are reported to the QI/UM Committee.
7. Compliance Committee
Chaired by: Chief Compliance Officer
Membership: CCAI Executive Staff: President, VP Healthcare Services, Chief Marketing Officer, CFO, CIO, VP Operations
Responsibilities and Functions:
i. Identify areas of risk. Assess the effectiveness of the Compliance Program to determine areas of risk and, if necessary, identify measures to address areas of risk. Analyze issues affecting CCAI and legal requirements with which the CCAI must comply.
ii. Monitor internal and external audits and investigations to identify potential risk areas and recommend and implement corrective and preventive action.
iii. Work with CCAI personnel to develop policies and procedures to address areas of risk and promote compliance with the Compliance Program and applicable laws.
iv. Develop and monitor internal systems and controls to ensure compliance with CCAI written policies and procedures.
v. Analyze and develop methods for promoting compliance, identifying potential violations and soliciting, evaluating and responding to complaints and reports of non-compliance.
vi. Periodically review resources assigned for compliance efforts to assess their adequacy.
Meetings: Monthly. Minutes: Meeting minutes are reported to the CCAI Board of Director
H. Resources and Analytic Support [QI1A1] Resources devoted to CCAI’s QI program include dedicated staff, data sources, and analytical resources. The QI program is integrated throughout the organization and involves key areas and positions.

49
Resources devoted to quality improvement activities include:
1. Staff a. CCAI Medical Director b. President, CCAI c. Vice President Population Health and Quality d. Vice President Utilization management and Transitional Care e. Vice President, Healthcare Management f. Director, Quality Improvement g. Manager, Quality Improvement h. Manager, Accreditation & Quality i. Quality Specialist
2. Data Sources a. HEDIS Software Application b. Service Overview – helps to define, measure, and manage risk c. HEDIS software application reporter for QA Team HEDIS monitoring and reporting
system i. Missing Services Reports
ii. Gaps in Care Letter Generation iii. Ad hoc reporting for targeted goals
d. HEDIS software application engine for IT HEDIS Team monitoring and reporting
system i. Monthly HEDIS Refreshes
ii. Control and Optimization of Patient-Level Data (PLD) e. Care Management System
i. Service Overview – care management system to identify, stratify, assess, and report quality of care and utilization of services delivered
1) Utilization Management – pre-authorization, Utilization Review
2) Case Management – Initial Health Risk Survey (HRS), Comprehensive (HRA), and/or specific disease assessments, as appropriate
3) Letter Generation – Program Enrollment and Participation to members and providers
ii. Predictive Modeling System 1) Identifies enrollees with specific conditions who will benefit
from Care Coordination.
50
2) Stratifies enrollees using relative and absolute risk scores related to chronic conditions, total costs and behavioral health costs. This allows Care Coordination to focus on those enrollees with the greatest opportunity to improve care.
3) Identifies gaps in care for preventive measures, disease management and wellness checks.
f. Analytical Resources i. Clinical Data Management Coordinator
1) Clinical Data Management Coordinator provides reports to analyze trends in utilization of services, demographics, and key indicators for quality initiatives.
ii. Internal Data Warehouse developers 1) Data Warehouse Architect – data models data from across
the enterprise and architects loading into the warehouse 2) Data Warehouse ETL – writes the ETL to load all data into
the warehouse iii. Internal IT Report Writers
1) Reporting business analysts – work directly with the business team to gather report requirements, and develop the report for the end user.
2) Manager, Business Intelligence – manages Reporting business analysts both administratively and technically
3) IT Consultant – automates existing reports into the reporting portal, builds marts and cubes off the data warehouse
iv. Business Intelligence Analysts 1) BI Analysts provide reports to monitor member risk, care
coordinator caseloads, utilization, key performance metrics, and member bonus incentives.
I. Delegated QI Activities [QI1A1] 1. In order to improve behavioral healthcare, CCAI has contracted with an external NCQA-
accredited organization with behavioral healthcare experience which is delegated to provide behavioral healthcare inpatient and outpatient utilization management (UM) and behavioral health case management.

51
2. CCAI has contracted with the same external NCQA-accredited organization referenced above which is delegated to provide medical UM after hours and on weekends and holidays, in addition to medical outpatient UM overflow.
3. CCAI contracts with an NCQA-certified delegated pharmacy benefits manager (PBM). The PBM is contracted to assist in managing our formularies, to encourage clinically appropriate cost-effective prescribing. The PBM also supports our plans in clinical management, utilizing tools such as drug utilization review, medication therapy management and disease management to realize the best clinical outcomes related to medication use for our members.
4. CCAI contracts with an NCQA-certified delegated credentialing verification organization (CVO). The CVO provides primary source verification services of provider and practitioner licensure, DEA or CDS certificates, education and training, board certification status, work history and malpractice history. The CVO is also responsible for providing reporting and credentialing data collection of practitioners and provider. Additionally, a small number of medical or physician groups are delegated for credentialing. In order to be delegated for credentialing, the group must show proof of NCQA certification for credentialing or CVO, or complete a pre-delegation survey tool and mutually agree to the delegated responsibilities. All delegated credentialing entities are overseen by the Delegated Oversight Committee.
See Attachment 1 for a list of NCQA-accredited organizations to which CCAI delegates QI activities.

52
Attachment 1 External NCQA-Accredited Organizations to which CCAI Delegates QI Activities
Delegated Entity Delegated Responsibility Delegated QI Activity NCQA-Certified Y/N
Health Integrated
Behavioral Health UM Behavioral Health
Complex Case Management
Behavioral healthcare inpatient and
outpatient utilization management (UM) and behavioral health case
management
UM: Y CCM: Y
BH CCM: Y
Health Integrated Utilization Management
Medical UM after hours and on weekends and
holidays
UM: Y CCM: Y
BH CCM: Y
CVS Health (PBM) UM, Appeals, Call Center
Manage pharmacy benefits UM: Y
Gemini Diversified Services Inc.
Credentialing and Recredentialing
Credentialing verification CVO:Y
53
XI. Acknowledgement and Approval
Approved as revised by the Community Care Alliance of Illinois quality improvement/utilization management committee on 10/19/2016 .