Community Based Primary Health Care The Answer to Addressing Child Mortality Paul Freeman Chairman...
25
Community Based Primary Health Care The Answer to Addressing Child Mortality Paul Freeman Chairman CBPHC-WG APHA
-
Upload
julian-oneal -
Category
Documents
-
view
219 -
download
2
Transcript of Community Based Primary Health Care The Answer to Addressing Child Mortality Paul Freeman Chairman...

Community Based Primary Health Care
The Answer to Addressing Child Mortality
Paul FreemanChairman CBPHC-WG APHA

Content Overview
The need OVCs
What is CBPHC
Evidence of What works
Examples OVC programs

Where We Stand on Child Survival U5MR declined ¼ between 1990 & 2006
Source. UNICEF

Global distribution of cause-specific mortality among children under five
Undernutrition is implicated in up to 50% of all deaths of children under five
Source: World Health Organization and UNICEF

Where We Stand on Malnutrition: South Asia and Africa have highest levels

Where We Stand on HIV/AIDS: Sub-Saharan Africa accounts for 90% of paediatric HIV infections
Source: UNICEF

Orphans & Vulnerable ChildrenOrphans SubSahara Africa
30.9 Million 1990 48 Million 2005 53 Million 2010 30% due AIDS >12% of all children
AIDS related At risk for schooling, food security, HIV 0-3 yrs old whoes mother dies are 3.9 times more likely to die in 1yr 0-5 yrs 16% of all orphans ->physical, nurturing needs greatest 12-17yrs 50% of all OVCs 66% of double orphans
The closer to biological family-better care, schooling
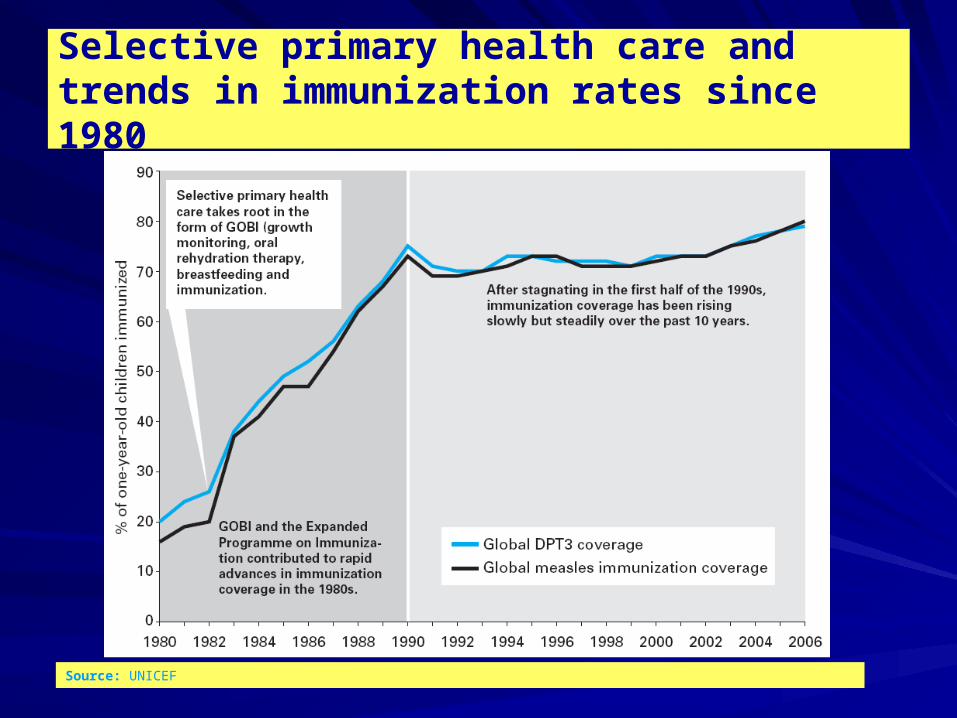
Selective primary health care and trends in immunization rates since 1980
Source: UNICEF

9
41
15
8
Tanzania
Uganda
Bangladesh
Low Utilization of Health Facilities
% sick children who were taken first to a health facility
Source: Arifeen S, Paryio G, Schellenberg J et al

10
Overall Conclusions of Multi-country Facility-Based IMCI Evaluation
IMCI improves quality of care
IMCI does not increase overall costs– Either for providers or out-of-pocket
IMCI dramatically reduces cost per child managed correctly
IMCI is the gold standard for facility care of children aged 7 days – 5 years

11
IMCI can have an impact on mortality and nutrition
But this requires:– Strengthening health systems– Reaching out to the community
IMCI was least likely to be implemented well where it was needed most
IMCI did not expand to areas of greatest need and there was no prioritization given to these areas
Overall Conclusions of Facility-Based IMCI Evaluation (cont.)

From 70 – 90% of all sickness care takes place in the home Household members, especially mothers: – make the primary diagnoses of illnesses – assess the severity and likely outcomes – select among available providers and treatment options– procure and administer treatments
How about sickness care?
WHO, World Health Report 2002. Reducing Risks, Promoting Healthy Life Slide Source Henry Moseley
Why CBPHC?Lessons Learned from a hundred years
• Scaling-up will not be achieved through facility-based and outreach services alone: Community Partnerships are central to achieving coverage, creating demand and achieving sustainability.
• Ensuring a continuum of care by delivering integrated packages of health, nutrition, HIV, water and sanitation interventions will be critical to achieving maximal impact on maternal, newborn and child survival.
• Strengthening of ‘health-systems for outcomes’ combines the strength of selective/vertical approaches and comprehensive/horizontal approaches to scaling up evidence-based, high-impact intervention packages and practices, while removing system-wide bottlenecks to health care provision and usage.
(Source R.Knippenburg UNICEF)

What Is CBPHC?What Is CBPHC?
CBPHC is a process through which health programs and CBPHC is a process through which health programs and communities work together to improve health and control communities work together to improve health and control disease. disease.
CBPHC includes the promotion of key behaviors at the CBPHC includes the promotion of key behaviors at the household level as well as the provision of health care household level as well as the provision of health care and health services OUTSIDE of static facilities at the and health services OUTSIDE of static facilities at the community level. community level.
CBPHC can (and of course should) connect to existing CBPHC can (and of course should) connect to existing health services, health programs, and health care health services, health programs, and health care provided at static facilities (including health centers and provided at static facilities (including health centers and hospitals) and be closely integrated with them. hospitals) and be closely integrated with them.

What is CBPHC? (cont.)What is CBPHC? (cont.)
CBPHC also includes multi-sectoral approaches to CBPHC also includes multi-sectoral approaches to health improvement beyond the provision of health health improvement beyond the provision of health services per se, including programs which seek to services per se, including programs which seek to improve education, income, nutrition, living standards, improve education, income, nutrition, living standards, and empowerment.and empowerment.
CBPHC programs may or may not be in collaboration CBPHC programs may or may not be in collaboration with governmental or private health care programs; they with governmental or private health care programs; they may be either comprehensive in scope or highly may be either comprehensive in scope or highly selective; and they may or may not be part of a program selective; and they may or may not be part of a program which includes the provision of services at fixed facilities. which includes the provision of services at fixed facilities.

What Is CPBHC? (cont.)What Is CPBHC? (cont.)
CBPHC includes the following three different types of CBPHC includes the following three different types of activities:activities:
(1) Communications with individuals, families and (1) Communications with individuals, families and communities to improve key practices;communities to improve key practices;
(2) Social mobilization and community involvement for (2) Social mobilization and community involvement for planning, delivering and using health services;planning, delivering and using health services;
(3) Provision of health care in the community, including (3) Provision of health care in the community, including preventive services (e.g., immunizations) or curative preventive services (e.g., immunizations) or curative services (e.g., community-based treatment of services (e.g., community-based treatment of pneumonia).pneumonia).

A Continuum of Care in Time and Place
Source: PMNCH (www.who.int/pmnch/about/continuum_of_care/en/index.htm), accessed 30 September 2007

Technical Interventions Priority child survival interventions for scale up
Insecticide-treated materials and/or indoor residual spraying for malariaMalaria treatmentIntermittent preventive therapy for malaria for pregnant womenExclusive breastfeeding promotion for first 6 monthsContinued breastfeeding promotion until at least 24 monthsReady to use therapeutic foods for severely malnourished childrenPromotion of complementary feeding for children focused on 6 to 23 monthsSupplementary feeding for food-insecure families focused on 6 to 23 months

Technical Interventions (cont.) Priority child survival interventions for scale up
Insecticide-treated materials and/or indoor residual spraying for malariaMalaria treatmentIntermittent preventive therapy for malaria for pregnant womenExclusive breastfeeding promotion for first 6 monthsContinued breastfeeding promotion until at least 24 monthsReady to use therapeutic foods for severely malnourished childrenPromotion of complementary feeding for children focused on 6 to 23 monthsSupplementary feeding for food-insecure families focused on 6 to 23 months

Setting Stage for Successful Interventions
Community partnerships in PHC
Scaling up community partnerships, a continuum of care, effective health systems for outcomes
Participative planning, implementation, monitoring & evaluation
Uniting for Child Survival Pivotal actions at the macro-level Planning, funding, cooperation

Comprehensive needs OVCsSupport for caregivers-extended family, communities
Multisectoral core needs-physical/mental health, nutrition, education, material support, day/after school
Commitment from government- policy, legislation, situational analysis, planning, monitoring, resources, accelerated evidence based prevention & ARV access for all members of society.
Child & female led households special needs
Meet needs without setting OVCs apart from rest of societyNote also needs of children with chronically ill parents

Bana ba Keletso Orphan Day Care Centre, urban village Botswana
Actively reaches out to orphaned children
Preschool children cared for during the day
Older children –meals, skilled based activities, psychosocial counseling
Family outreach program –counseling and support through home visits.
Comprehensive, quality but labor intensive, maybe hard to scale up, sets orphans apart.

Ikamva Labantu Organization Cape Town South Africa
DecentralizedTwo outreach strategies –identifies OVC through network of 250 creches & by word of mouth request for assistance.
Follow Up visits to OVC and familiesSupport –indirectly through creches
-directly through home visits, material & nutritional support, capacity building in home, access to government grants.Helps families to build resources in the long run, does not separate out OVCs as attend creches with other children, uses local structures, serve more children, cheaper, more easily scalable.

FBOs can offer
Christian unconditional love as basis towards building self love and efficacy
“Immunization” against future trials
Moving away from dependence towards building confidence in community participation and empowerment

Conclusion
Getting community commitment is an essential part of addressing child health if we are going to reach the most needy children & achieve sustainable programs.
This involvement should be in all phases of program planning, implementation and evaluation.