Community based Integrated Maternal, Neonatal & Child Survival … files/Reports/Project...
84
1 Project Completion Report Community based Integrated Maternal, Neonatal & Child Survival (MNCS) Interventions A Collaborative effort of IMCI (DGHS) and UNICEF Bandarban Sadar and Lama Upazilas of Bandarban District Duration: May 2008 - October 2012 Submitted to UNICEF Bangladesh BCL Office Complex, 1 Minto Road, Dhaka-1000 Submitted by Partners in Health and Development (PHD) and GRAUS IMCI Programme Directorate General of Health Services, MoHFW
Transcript of Community based Integrated Maternal, Neonatal & Child Survival … files/Reports/Project...
1
Project Completion Report
Community based Integrated Maternal, Neonatal & Child Survival (MNCS) Interventions
A Collaborative effort of IMCI (DGHS) and UNICEF
Bandarban Sadar and Lama Upazilas of Bandarban District
Duration: May 2008 - October 2012
Submitted to
UNICEF BangladeshBCL Office Complex, 1 Minto Road, Dhaka-1000
Submitted by
Partners in Health and Development (PHD) and GRAUS
IMCI ProgrammeDirectorate General of Health Services, MoHFW
2
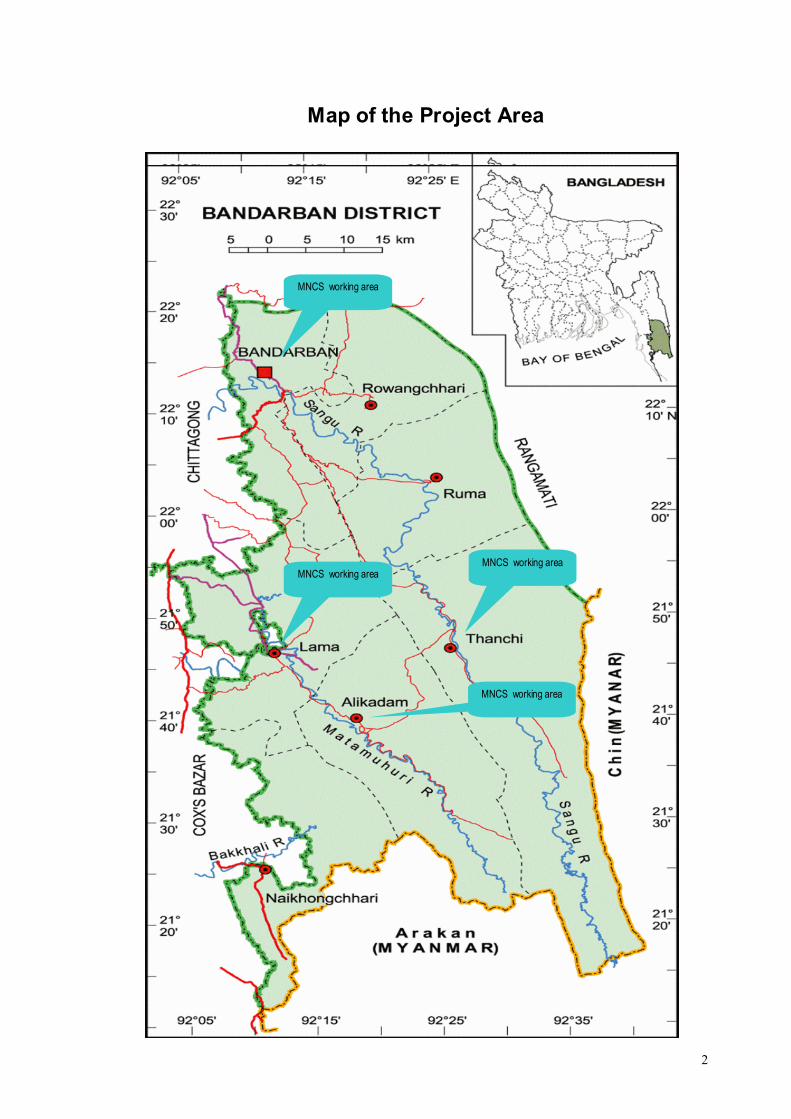
Map of the Project Area
Project Completion Report for
MNCS working area
MNCS working area
MNCS working area
MNCS working area
MNCS working area
MNCS working area
3
Project Completion Report for Maternal, neonatal and child survival (MNCS) Intervention
PROGRAMME SUMMARY
Name of Project: An Integrated Package of Maternal, Neonatal & Child Survival (MNCS) Interventions
Donor: UNICEF
PCA #:For2Up UNICEF/PCA/2008/053, UNICEF/PCA/2011/006, UNICEF/PCA/2011/006-Amdt.01, UNICEF/PCA/2011/006-Amdt.02, UNICEF/PCA/2011/006-Amdt.03
PCA #:For4Up UNICEF/PCA/2010/001, UNICEF/PCA/2010/001 Amdt.01, UNICEF/PCA/2010/001 Amdt.02, UNICEF/PCA/2010/001 Amdt.03
Duration: 1st September 2008 to 31 October 2012
Total Programmable Fund: Taka133,196,282 and USD 1620392.72
Total Fund Utilized: Taka 121,164,637 and USD 1474022.34
Fund Utilization rate 90.96%
Period covered by this Report: 1st September 2008 to 31 October 2012
Implementing Agency: Partners in Health and Development (PHD)
Implementing partners: Gram Unnayan Sangathan (GRAUS)
Beneficiaries: Approximately 2,22,740 people in 6 upazilas of Bandarban District
Women 15-49 yrs: 52537Pregnant women: 12635Neonates: 9882
Geographical Coverage: Bandarban Sadar, Lama, Alikadam, Rowangchari, Ruma, and Thanchi
Contact person and address: Md. Abdus Salam. Managing Director House SWD12/A, Road No# 8, Gulshan # 1 , Dhaka1212
Email: [email protected]
Conversion rate: 1 USD= 82.20 Taka Dated: 29 November 2012
4
List of Acronyms
ANC Anti-natal check up
ARI Timer Acute Respiratory Infection Timer
CC Community Clinic
CHT Chittagong Hill Tracts
CM Community Mobilizer
CN Community Nurse
CS Civil Surgeon
CSG Community Support Group
ED Executive Director
ENC Essential Newborn Care
EPI Extended Programme for Immunization
FPI Family Planning Inspector
FWA Family Welfare Assistant
FWV Family Welfare Volunteer
GO Government Organization
GoB Government of Bangladesh
GRAUS Gram Unnayan Sangathan
HA Health Assistant
HNPSP Health, Nutrition and Population Sector Programme
HP Health Promoter
HTR Hard to Reach
ICDP Integrated Community Development Program
IMCI Integrated Management of Childhood Illness
KABPA Knowledge, Attitude, Behavioral Practices Analysis
MD Managing Director
MDG Millennium Development Goal
MMR Maternal Mortality Rate
MNCS Maternal, Neonatal & Child Survival
MO Medical Officer
NGO Non Government Organization
NID National Immunization Day
PNC Post-Natal Check up
PSSC Pahari Shasthya Seva Centre/Kendra
ToT Training of Trainers
UFPO Upazila Family Planning Officer
UHC Upazila Health Complex
UHFPC Upazila Health & Family Planning Complex
UHFPO Upazila Health & Family Planning Officer
UM Upazila Manager
Upazila (Bangla)
Sub-District
5
Executive Summary
MNCS, a UNICEF and Government of Bangladesh supported project, implemented by PHD and its partner organization GRAUS addressing survival and new born issues by improving home care health practices, increasing care seeking behavior of communities and utilization of neonatal and child health services by the families. MNCS implemented its activities in 25 unions of Six Upazilas of Bandarban District.
For smooth implementation of the MNCS, a total of 94 staff and 420 volunteers as Health Promoters were provided with different types of training and orientation to develop their skills in various aspects of C-IMCI, ENC, PNC, Planning, PRA, supervision and Monitoring, Surveillance Registrar, etc. Under the intervention, trained community health promoters visit households to register pregnant women, newborn and under 5 children and provide antenatal information, neonatal kits and counseling on essential newborn care and danger signs for newborn and mothers. The trained health promoters also accomplished postnatal visit to ensure essential neonatal care, assisted the mothers to do birth registration, provided five counseling visit immediate after identification of a woman as pregnant and referred sick children of < 5 aged and mothers and neo born with danger sign to the health facilities as needed.
The MNCS aimed to implement sustainable interventions in the hard-to-reach areas of Bangladesh through building the capacity of communities, government agencies, local government representatives and other relevant stakeholders. To ensure community involvement, MNCS established 198 Community Support Groups (CSG) at community level and 25 Health and Family Planning Committee (UH&FPO) at union level. Later on, PHD organized intensive training for CSG members along with others. MNCS is supporting to 14 Pahari Shasthya Seva Kendra (PSSK) by appointing 14 Community Nurses to ensure health care services to pregnant mothers and children in the remote areas.
With a view to analyse the different health related situation, practices and types of health services providers, an assessment tool KABPA (Knowledge, Attitude, Belief, Practice and Assessment) was applied prior to implementation of the MNCS activities. Based on the analysis, CSGs developed a yearly action plan followed by monthly micro plan. Each CSG prepared a health map containing the households with pregnant mothers, neonates, under 5 children, and service providers, and updated in every month. MNCS supported the Government of Bangladesh (GoB) in running the EPI sessions and satellites to ensure the participation of people. It also assists the government staff in 6 Community Clinics (CC) and 1 Family Welfare Center (FWC) to run the health services without any interruption due to shortage of staff. Establishment of joint GO-NGO monitoring process and introduction of monitoring strategy like involvement of CSG members in citizen monitoring, etc. has improved the quality of the MNCS intervention.
With the implementation of effective activities, MNCS had to brawl against some challenges and accomplished some major achievements-
Initiatives were undertaken by CSGs and UH&FPCs in different aspects like communication and mobilization of the community people towards health services have promoted a smooth community support system in the community.
C4D Intervention created a demand in the community through disseminating the messages at all level. Organizing sharing session, workshops, rally, quiz program/debate with the community people and school students of different schools on MNCS issues and videos show increased the knowledge level of the community on maternal and neonatal health issues.
6
Proper birth planning of the pregnant mothers along with her family addressed the three delays of maternal health which was considered as one of the common reasons for maternal and infant mortality. Introducing penny bank to each pregnant mother has enhanced the savings tendency of the pregnant mothers and members which they use as referral cost to help the poor mothers to get modern treatment from the institutional and qualified service providers.
Institutional delivery is one of the major challenges in Bandarban. Continuous mobilization through courtyard meeting, home visit, individual counseling and influence of CSG members has increased the rate of ANC Check-up and institutional deliveries among the mothers. Capacity building support to the Birth Attendance through providing training on safe delivery, essential new born care, etc. has reduced the death of newborn and rate of maternal mortality.
Established liaison between communities and government health facilities has promoted a smooth community support system.
The intervention has finally developed an inimitable phase out plan with identification of potential actors to carry out the minimum packages of services and prepare the community people to act in a more united way.
7
TABLE OF CONTENTS
Content Page
1. Project Background 08
1.1 Project Context 08
1.2 Goal, Purpose, Outcomes and Outputs 08
1.3 Geographical Coverage 09
1.4 Project Management and Project Staffs 10
1.5 Major Components and Implementation Strategies 11
2. Progress Against Planned Results 12
2.1. Overall Progress of MNCS 12
2.2. Progress Against Goal 13
2.3 Progress at Output Level 14
3. INNOVATION FOR MNCS 16
4. Evidences Generated and Major lessons learned 17
5. Major Bottlenecks and Challenges and Measure Undertaken 18
6. RISK and RISK MANAGEMENT 18
7. Phase-out and Sustainability Plan-implemented 19
8. PROJECT FINANCIAL INFORMATION (summary by year) 22
9. RECOGNITION OF GOB/AusAID/UNICEFS CONTRIBUTION- 24
10. Conclusion 25
ANNEX 1. Major achievements against selected Log-Frame indicators 26
ANNEX 2. Case studies 27
Case Study 01. Case of safe delivery at the Hospital. 27
Case Study 02. Mother’s Dream comes true 28
Case Study 03. Jingrumoy Bom 29
Case Study 04. Halima’s Story-A citizen Initiative 30
Case Study 05. Case Study from Aziznagar, Lama – Bandarban 31
ANNEX 3. Detail Final Report (Quarter and year wise against approved budget 32
ANNEX 4. Photographs with captions on C4D and other major activities 85
8
1. Project Background
1.1 Project Context
Since 2003, the GoB has started to work in health and family planning sector with support of different development partners. With a view to strengthen the country’s health sector and speed up the progress towards addressing Millennium Development Goals of 4 &5 , GoB implemented Health, Nutrition and Population Sector Programme (HNPSP). After providing many efforts the mid–term review OF HNPSP identified some critical gaps in maternal, neonatal and child health and suggested strengthening relevant services to accelerate progress towards achieving the MDGs.
To address the stubbornly status of mortality rate of mothers, children and infants APR of HNPSP (2007) recommended to scale-up community IMCI interventions in the country. Under the community IMCI strategy UNICEF designed the Community-based integrated Maternal, neonatal and Child Survival (MNCS) intervention they would be delivered through linking the health and family planning with local government and community structures.
In 2005, MNCS started its activities as a pilot project in Nilphamari. With a view to promote preventive and curative maternal, neonatal and child care practices through targeted household visits and community mobilization, resulting in a sharp rise in pregnancy identification, antenatal care, and access to skilled birth attendants during delivery it has expanded in 10 districts in Bangladesh.
1.2 Goal, Purpose, Outcomes and Outputs
Goal: The goal of the MNCS was to contribute in achieving the MGD 4 and 5 by reducing <5 mortality rate, Infant neonatal mortality rate and it would contribute in reducing MMR to a great extent.
Purpose:
The purposes of MNCS were to improve the home care health practices, increase care seeking behavior of communities, utilization of neonatal and child health and nutrition services by families, particularly poor and excluded communities’ lives in MNCS intervention areas.
Outputs:
Improve home care Health practices
Increase care Seeking behavior
Utilization of neonatal, child survival and nutrition services by families
Make MNCS Services available to communities lives in hard-to-reach areas
9
The outputs of MNCS were expected at three levels – at community level, local government level and in Local government level.
At Community Level:
Increase Participation in Planning, implementation and Monitoring of MNCS
For Local Government
Participation of Local Government in the MNCSCreate Ownership among the Local Government
For Local Health System
Increase Availability and Quality of MNCS Package at community level
1.3 Geographical Coverage
Bandarban is one of the remotest districts of the country. It has a total area of 4479.03 sq. kilometer with the total population of 3, 83, 000 (male 52.4% and Female 48.61%), where the literacy rate is 43% (Family Planning Profile 2012 June) Bandarban consists of 7 upazilas, 30 unions, 160 Mouzas, 1488 villages, 2 municipality. Ethnic nationals include the Marma, Mro, Tripura, Bawm, Tanchangya, Chakma, Chak, Khyang, Khumi, Lushai and the Pankho. The upazilas are Bandarban Sadar, Rowangchari, Ruma Thanchi, Lama, Alikadam, and Naikhongchari.
For all indigenous peoples in the CHT, ethnic identity is the dominant factor. Although many ethnic groups have similar customs and life styles, there is no single language which unifies all groups. Although there are 11 ethnic groups’ living in Bandarban District but Bangali (Muslim, Hindu, Christian, and Buddhist), Mro, Chak, Marma, Tanchangya, Bawm, Tripura are predominant and each tribe has its own language.
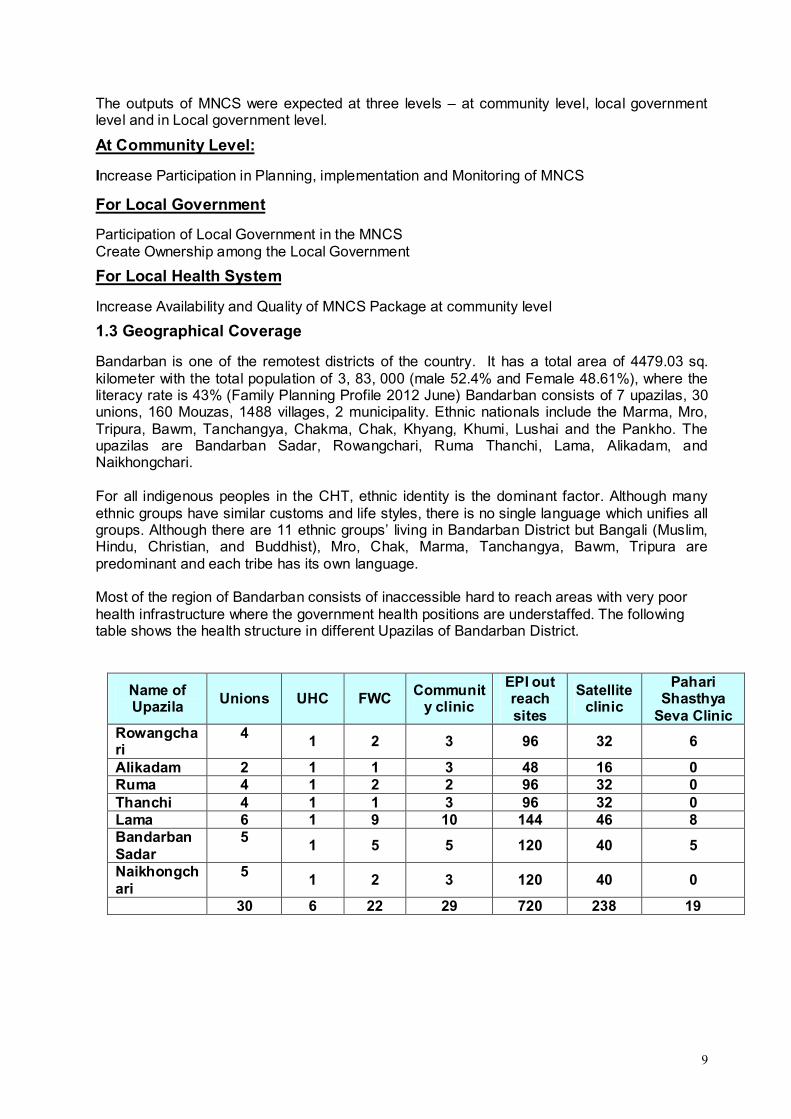
Most of the region of Bandarban consists of inaccessible hard to reach areas with very poor health infrastructure where the government health positions are understaffed. The following table shows the health structure in different Upazilas of Bandarban District.
Name of Upazila
Unions UHC FWCCommunit
y clinic
EPI out reach sites
Satellite clinic
Pahari Shasthya
Seva ClinicRowangchari
41 2 3 96 32 6
Alikadam 2 1 1 3 48 16 0Ruma 4 1 2 2 96 32 0Thanchi 4 1 1 3 96 32 0Lama 6 1 9 10 144 46 8Bandarban Sadar
51 5 5 120 40 5
Naikhongchari
51 2 3 120 40 0
30 6 22 29 720 238 19
10
1.4 Project Management and Project Staffs
Partner in Health and Development (PHD) implemented MNCS in 25 unions of six Upazilas of Bandarban District under the partnership agreement with GRAUS. The main aim of the PHD to move with the GRAUS was that GRAUS is a leading indigenous led organization in Bandarban and solely working for the development of way of life and the living condition of the community people. PHD and GRAUS has a long partnership experience for conduction a project on Mobilizing the Poor and Disadvantaged People to Manage the Local Health Services.
As a part of project management strategy, MNCS established an ‘Implementation Committee’ with the Managing Director of PHD, Executive Director of GRAUS and the Project Coordinator of the project to monitor and review the project direction. On behalf of the consortium, PHD’s managing Director was responsible to conduct all external correspondence and signs contracts.
The Project Coordinator coordinated and managed day-to-day activities and the supervised the resources in line with the Project Implementation Plan (PIP). In order to ensure organizational contribution and to make the project accountable to the consortium, the MD of PHD & the ED of GRAUS included in project’s team to provide 30% time which was gradually decreased in line with level of confidence and capacity gains overtime. The project incorporated an affirmative action in recruitment which was ensured the vertical involvement of vulnerable and marginalized groups within the community, including women, individuals with disabilities. The government especially the district and upazila health authority provided support to MNCS intervention and also played stewardship role for successful implementation of the project.
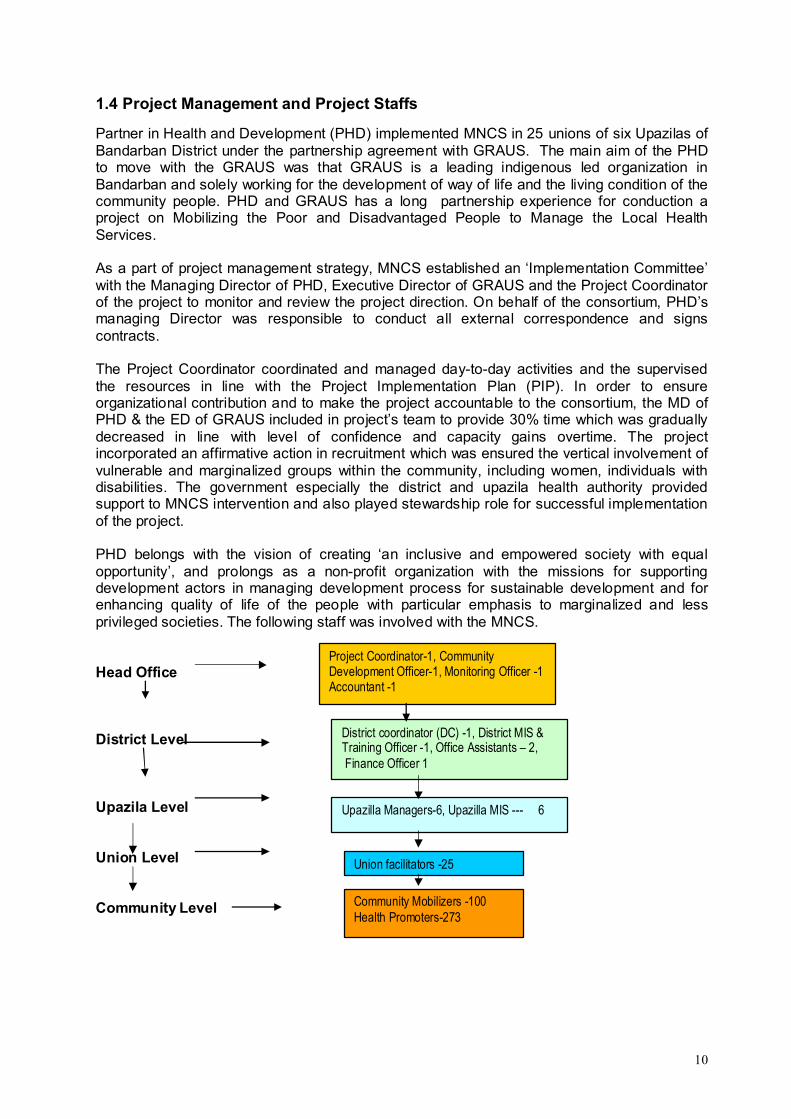
PHD belongs with the vision of creating ‘an inclusive and empowered society with equal opportunity’, and prolongs as a non-profit organization with the missions for supporting development actors in managing development process for sustainable development and for enhancing quality of life of the people with particular emphasis to marginalized and less privileged societies. The following staff was involved with the MNCS.
Head Office
District Level
Upazila Level
Union Level
Community Level
Project Coordinator-1, Community Development Officer-1, Monitoring Officer -1Accountant -1
District coordinator (DC) -1, District MIS & Training Officer -1, Office Assistants – 2, Finance Officer 1
Upazilla Managers-6, Upazilla MIS --- 6
Union facilitators -25
Community Mobilizers -100Health Promoters-273
11
1.5 Major Components and Implementation Strategies
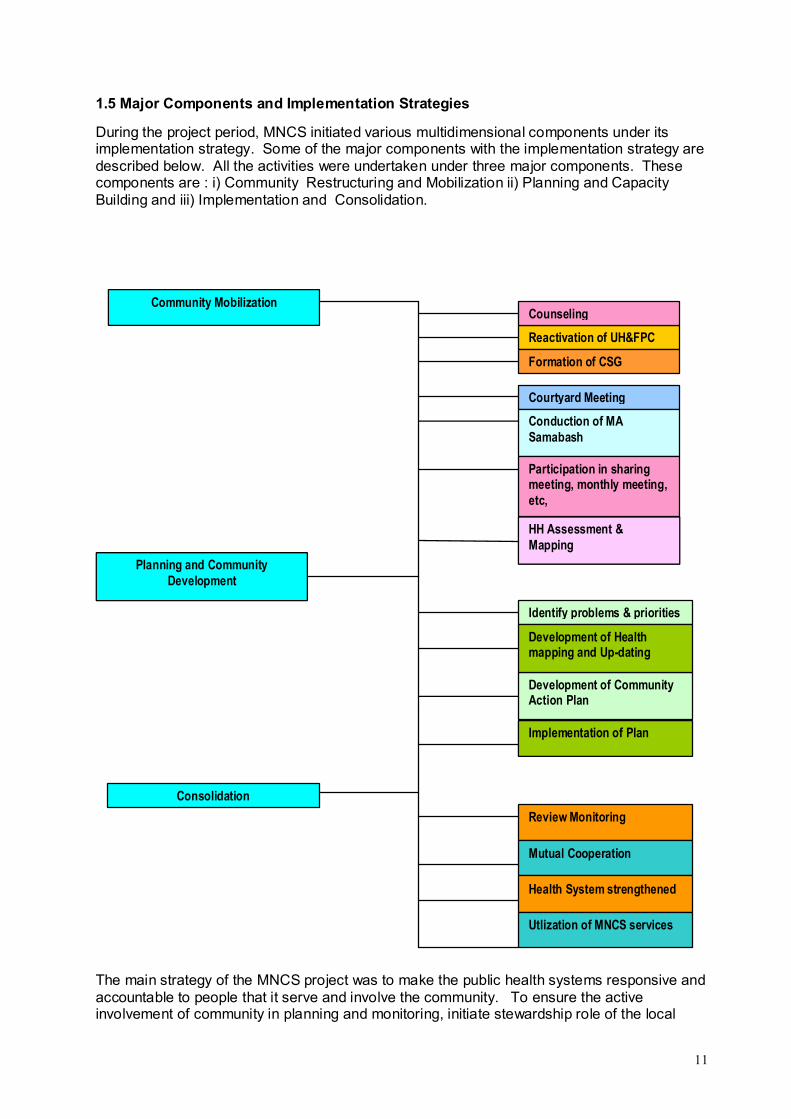
During the project period, MNCS initiated various multidimensional components under its implementation strategy. Some of the major components with the implementation strategy are described below. All the activities were undertaken under three major components. These components are : i) Community Restructuring and Mobilization ii) Planning and CapacityBuilding and iii) Implementation and Consolidation.
The main strategy of the MNCS project was to make the public health systems responsive and accountable to people that it serve and involve the community. To ensure the active involvement of community in planning and monitoring, initiate stewardship role of the local
Community Mobilization
Reactivation of UH&FPC
Formation of CSG
Counseling
Courtyard Meeting
Conduction of MA Samabash
Participation in sharing meeting, monthly meeting, etc,
Planning and Community Development
HH Assessment & Mapping
Identify problems & priorities
Development of Community Action Plan
Development of Health mapping and Up-dating
Implementation of Plan
Consolidation
Review Monitoring
Mutual Cooperation
Health System strengthened
Utlization of MNCS services
12
health delivery and increase availability of MNCS services, the MNCS intervention Package delivered through linking the health and family planning structures with local government and community people. The following diagram shows the implementation strategy of MNCS.
2. Progress Against Planned Results
2.1. Overall Progress of MNCS
This section discuss the overall progress of the MNCS Intervention. Overall progress has included the community participation, involvement of Local Government and strengthening the exiating health system in the MNCS intervention areas.
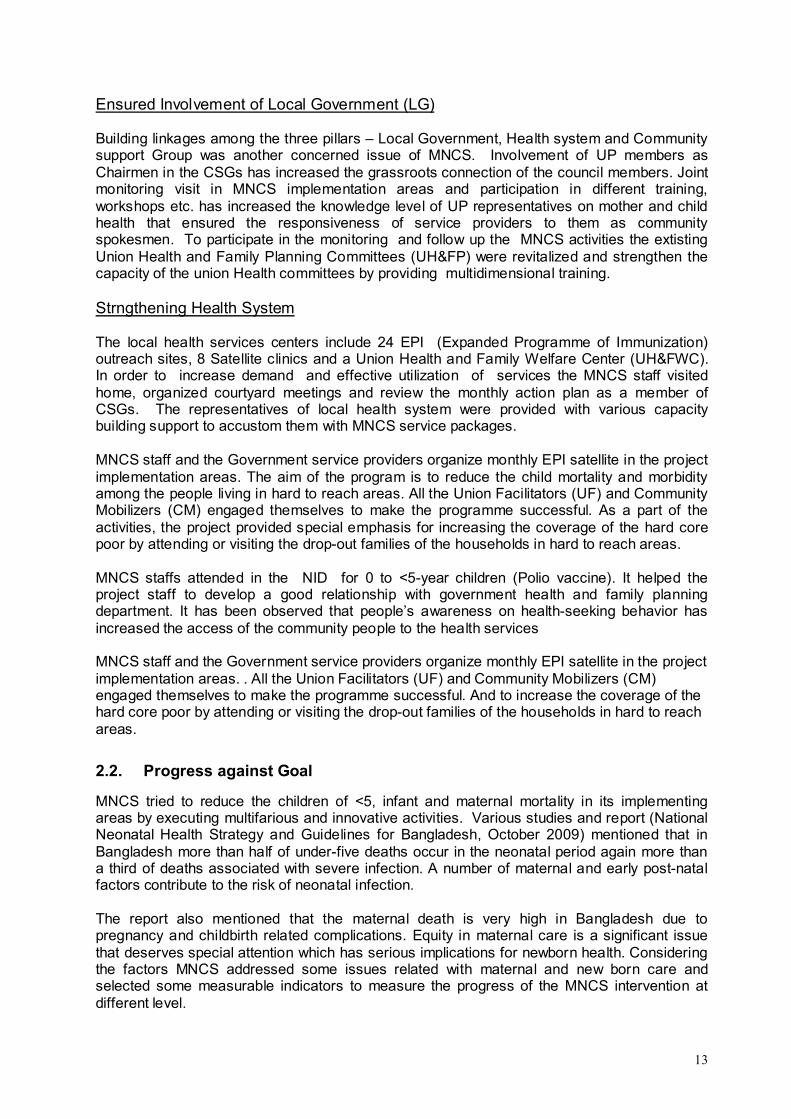
Increased Community Participartion
Under the implementation strategy, a strong Community Support system was established through the formation of Community Support Groups (CSGs) in each ward with the representatives of community leaders, gate keepers, etc. and strengthen the capacity of the community by providing various training, orientation and organizing meetings, sharing sessions, etc. The members of CSGs identified and prioritized community defined health problems and developed action plan to address the problems. In this way, Community support System promoted a boarder participation of the community in health section and also built community solidarity among community. Besides formation of CSGs, some self motivated persons from the community were selected to assist the MNCS staff in mobilization deliver of promotional activities. These volunteers were primarily selected by the CSG members from the own locality to communicate with the community people in their own dialect. The self motivated person willing to support MNCS were called Health Promoter (HP) and they were provided with training, orientation, etc.
CommunityLocal
Government
Health System
13
Ensured Involvement of Local Government (LG)
Building linkages among the three pillars – Local Government, Health system and Community support Group was another concerned issue of MNCS. Involvement of UP members as Chairmen in the CSGs has increased the grassroots connection of the council members. Joint monitoring visit in MNCS implementation areas and participation in different training, workshops etc. has increased the knowledge level of UP representatives on mother and child health that ensured the responsiveness of service providers to them as community spokesmen. To participate in the monitoring and follow up the MNCS activities the extisting Union Health and Family Planning Committees (UH&FP) were revitalized and strengthen the capacity of the union Health committees by providing multidimensional training.
Strngthening Health System
The local health services centers include 24 EPI (Expanded Programme of Immunization) outreach sites, 8 Satellite clinics and a Union Health and Family Welfare Center (UH&FWC). In order to increase demand and effective utilization of services the MNCS staff visited home, organized courtyard meetings and review the monthly action plan as a member of CSGs. The representatives of local health system were provided with various capacity building support to accustom them with MNCS service packages.
MNCS staff and the Government service providers organize monthly EPI satellite in the project implementation areas. The aim of the program is to reduce the child mortality and morbidity among the people living in hard to reach areas. All the Union Facilitators (UF) and Community Mobilizers (CM) engaged themselves to make the programme successful. As a part of the activities, the project provided special emphasis for increasing the coverage of the hard core poor by attending or visiting the drop-out families of the households in hard to reach areas.
MNCS staffs attended in the NID for 0 to <5-year children (Polio vaccine). It helped the project staff to develop a good relationship with government health and family planning department. It has been observed that people’s awareness on health-seeking behavior has increased the access of the community people to the health services
MNCS staff and the Government service providers organize monthly EPI satellite in the project implementation areas. . All the Union Facilitators (UF) and Community Mobilizers (CM) engaged themselves to make the programme successful. And to increase the coverage of the hard core poor by attending or visiting the drop-out families of the households in hard to reach areas.
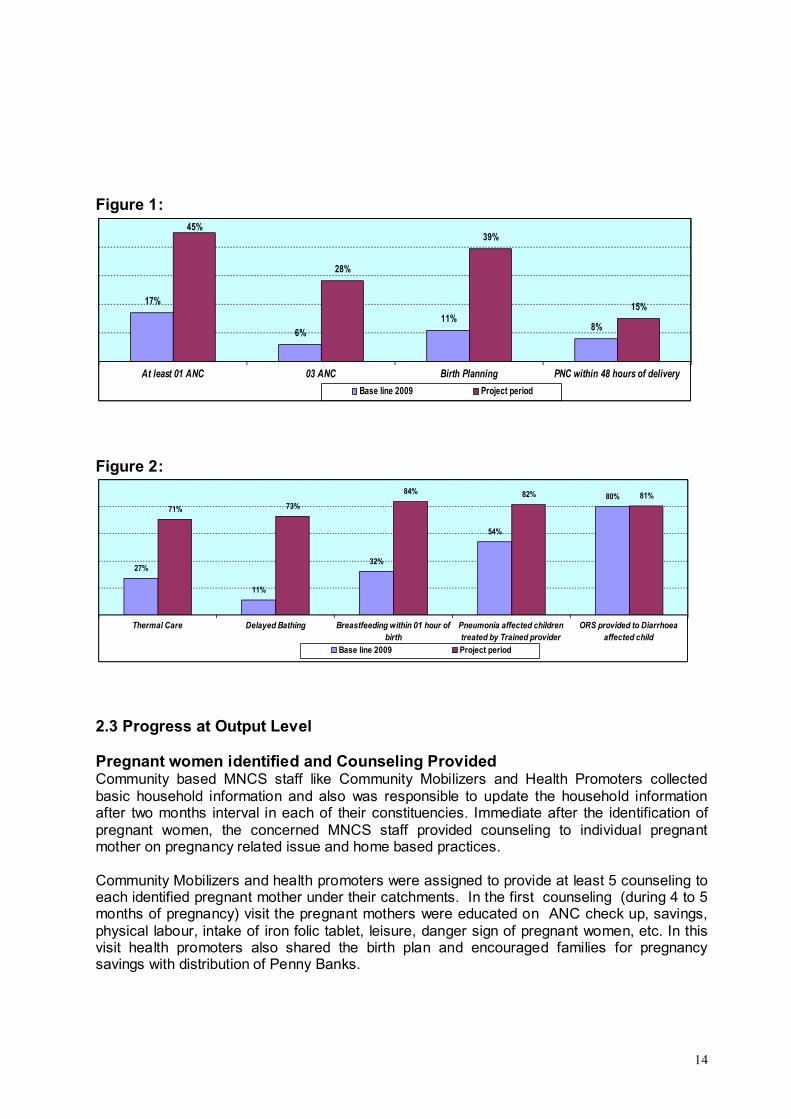
2.2. Progress against Goal
MNCS tried to reduce the children of <5, infant and maternal mortality in its implementing areas by executing multifarious and innovative activities. Various studies and report (National Neonatal Health Strategy and Guidelines for Bangladesh, October 2009) mentioned that in Bangladesh more than half of under-five deaths occur in the neonatal period again more than a third of deaths associated with severe infection. A number of maternal and early post-natal factors contribute to the risk of neonatal infection.
The report also mentioned that the maternal death is very high in Bangladesh due to pregnancy and childbirth related complications. Equity in maternal care is a significant issue that deserves special attention which has serious implications for newborn health. Considering the factors MNCS addressed some issues related with maternal and new born care and selected some measurable indicators to measure the progress of the MNCS intervention at different level.
14
Figure 1:
17%
6%
11%8%
45%
28%
39%
15%
At least 01 ANC 03 ANC Birth Planning PNC within 48 hours of delivery
Base line 2009 Project period
Figure 2:
27%
11%
32%
54%
80%
71% 73%
84% 82% 81%
Thermal Care Delayed Bathing Breastfeeding within 01 hour ofbirth
Pneumonia affected childrentreated by Trained provider
ORS provided to Diarrhoeaaffected child
Base line 2009 Project period
2.3 Progress at Output Level
Pregnant women identified and Counseling Provided Community based MNCS staff like Community Mobilizers and Health Promoters collected basic household information and also was responsible to update the household information after two months interval in each of their constituencies. Immediate after the identification of pregnant women, the concerned MNCS staff provided counseling to individual pregnant mother on pregnancy related issue and home based practices.
Community Mobilizers and health promoters were assigned to provide at least 5 counseling to each identified pregnant mother under their catchments. In the first counseling (during 4 to 5 months of pregnancy) visit the pregnant mothers were educated on ANC check up, savings, physical labour, intake of iron folic tablet, leisure, danger sign of pregnant women, etc. In this visit health promoters also shared the birth plan and encouraged families for pregnancy savings with distribution of Penny Banks.
15
In the 2nd counseling (8-9 months of pregnancy) the staff reviewed the previous issues discussed in 1st counseling and provided detail education on danger sign of neonatal, essential new v born care like wrapping, barest feeding within one hour, delayed bathing, birth planning, etc. The birth plan included information on selection of birth place, selection of skilled birth attendants, assistant during delivery, blood donors, arrange transport for EMOC (Emergency Management of Obstructive Care), etc. In this visit the MNCS staff ensured the presence of birth attendants, husband, mother-in-laws and other female members of the family during the discussion. The MNCS staff also suggested them to take Post Natal care from service providers.
The 3 rd counseling visit conducted during the delivery or after 24 hours of the delivery. This visit ensured the safe delivery by wrapping, breast feeding within one hour and delayed bathing, etc.
The 4th visit was provided after 3 days of the delivery that observed the case of under weight neo born care, neo born with respiratory problems and diarrhea. They also referred the neo born with danger sign to service providers.
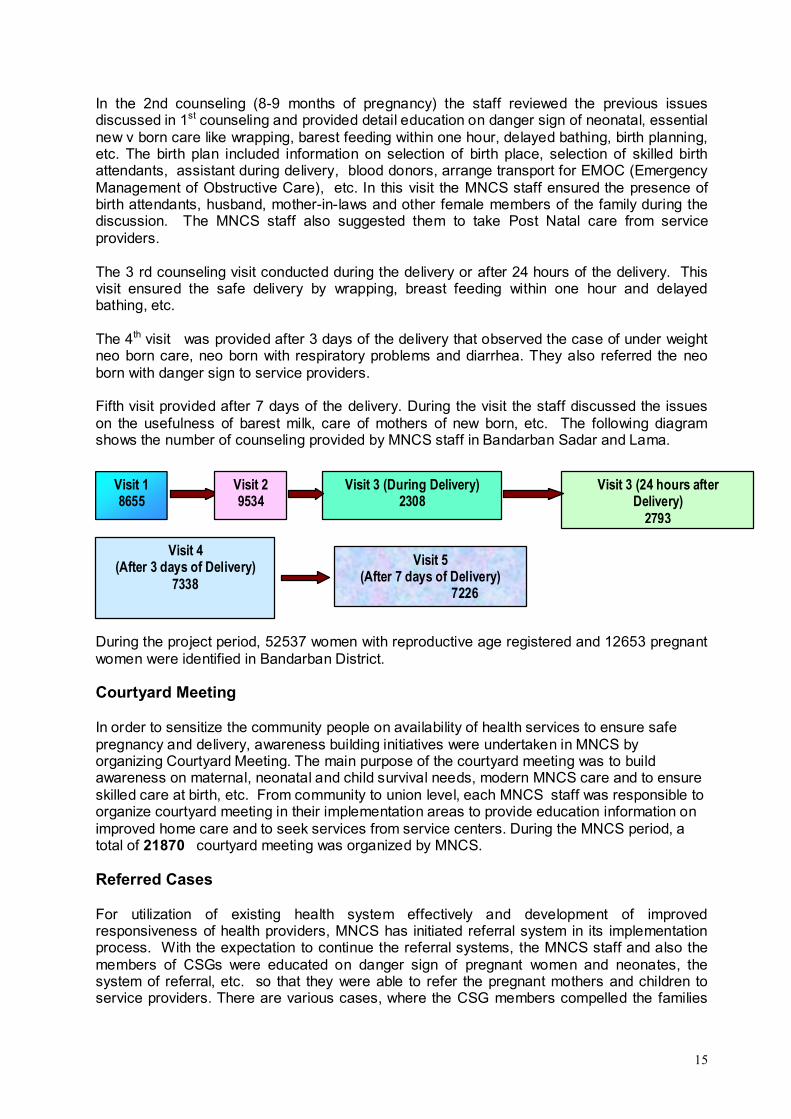
Fifth visit provided after 7 days of the delivery. During the visit the staff discussed the issues on the usefulness of barest milk, care of mothers of new born, etc. The following diagram shows the number of counseling provided by MNCS staff in Bandarban Sadar and Lama.
During the project period, 52537 women with reproductive age registered and 12653 pregnant women were identified in Bandarban District.
Courtyard Meeting
In order to sensitize the community people on availability of health services to ensure safe pregnancy and delivery, awareness building initiatives were undertaken in MNCS by organizing Courtyard Meeting. The main purpose of the courtyard meeting was to build awareness on maternal, neonatal and child survival needs, modern MNCS care and to ensure skilled care at birth, etc. From community to union level, each MNCS staff was responsible to organize courtyard meeting in their implementation areas to provide education information onimproved home care and to seek services from service centers. During the MNCS period, a total of 21870 courtyard meeting was organized by MNCS.
Referred Cases
For utilization of existing health system effectively and development of improved responsiveness of health providers, MNCS has initiated referral system in its implementation process. With the expectation to continue the referral systems, the MNCS staff and also the members of CSGs were educated on danger sign of pregnant women and neonates, the system of referral, etc. so that they were able to refer the pregnant mothers and children to service providers. There are various cases, where the CSG members compelled the families
Visit 18655
Visit 29534
Visit 3 (During Delivery)2308
Visit 3 (24 hours after Delivery)
2793
Visit 4(After 3 days of Delivery)
7338
Visit 5(After 7 days of Delivery)
7226
16
to send their daughters or daughter-in –laws with danger sign to the service provider or health complex. Under the MNCS, a total of 435 pregnant women and 6240 children and neo born with danger sign were referred to service providing. Out of referred pregnant mother with danger sign, 127 (29%) mothers and (24%) children and neo-nates were referred by the members of CSG
3. INNOVATION FOR MNCS
MNCS has tried to commence some novelty in the implementation strategies. For ensuring check up for the pregnant mothers of remote areas, MNCS organized a Ma Samabesh, to create savings tendency among the mothers, MNCS introduced a penny bank, and strengthen the Local health structure, MNCS provided support by assigning MNCS staff in CC and FWC.
Conduction of Ma Samabesh
During the project period, number of Ma Samabesh was organized. Under this activity, all the identified and registered pregnant mothers in the remote areas of a union were gathered. In each Ma Samabesh, about 40-50 pregnant women were gathered from different wards. MaSamabesh was generally organized in FWC (Family Welfare Center) or any school. UH&FPO, Medical Officers, technicians were invited in these Samabesh to discuss the issues on problems and care of pregnant women, danger sign during delivery and after delivery, etc. Two corners were set up during Samabesh. In one corner, FWV provided check up to one to one pregnant mother and necessary consultation. In other corner, technicians provided services to the pregnant mothers on blood grouping and supplied a piece of white paper with the blood group number and registered the mother name and address with blood group in the register book. Pregnant mothers were also provided with quality and nutritious food with 2 hours interval.
Introduction of Penny Banks
With a view to create savings tendency among the pregnant mothers to meet up the emergency need during delivery, MNCS staff provided an earthen penny bank immediate after identified as a pregnant woman. The mothers were asked to start save money (any available amount of Taka) for their future from the beginning. Besides this, in some places, the members of CSG also bought penny banks by collecting money from other members of CSG and provided to the mothers in their concerned areas. .
Provided Logistic and Manpower Support to the Local Health Structure In order to reduce burden of existing local level government health structure, MNCS assisted the government with logistic and manpower support. The other intention of MNCS was to enable the local health structure to manage increased number of patient referred by MNCS staff and Community Support groups. With a view to facilitate the government structure, Community Nurse and paramedics of MNCS assisted the Health Assistants (HA) and Family Welfare Assistant (FWA) in Community Clinics and Paramedic assisted SACMO (Sub Assistant Community Medical Officer) and Family Welfare Visitors (FWV) in FWC. The following diagram shows the number of CC and FWC assisted by the CN and Paramedics.
Bandarban Sadar
1. Kraikong –Bandarban Sadar Union Union2. Yzongshong—Swalok Union3. Pabla-Tongkaboti Union
Lama
4. Aunglapara – Rupashipara5. Yangsha – Fashiakhali6. Purba chambi – Aziznagar7. Doluziri - Sarai
17
4. Evidences Generated and Major lessons learned
· Cultural affinity of field level implementers to that of the project beneficiaries strengthens project implementation. We have seen that Bandarban being an area consisting of beneficiaries of different ethnic backgrounds, language, and cultures, it proved extremely difficult to communicate effectively. Thus, we have tried to place field implementers belonging to the same ethnicity as the beneficiaries themselves.
· The MNCS Project has achieved its strong goal only partially- and given the strong need scenario, the project needs continuation. This issue has time and again come up on different occasions. We may refer to the meeting minutes of different meetings where participants consisted of multi-dimensional stakeholders.
· Mere imparting of health lessons without provision of essential infrastructural and hardware provisions may not be effective. As a result we have tried to ensure that the beneficiaries are able to avail minimum medicine supply. This was possible with the support of UNICEF through the then Civil Surgeon of Bandarban District. However, this support was provided only once and though we had tried to find possibilities of continuation, it was not feasible due to non availability of funds.
· Along with the MNCS staff, CSG members also work as focal point for mobilizing the community people to increase their health seeking behaviour and to receive quality health services from different health service providing organizations. To carry out these activities the performances of the CSG members, we have trained a large number of CSG members on MNCS issues. This is evident in all the quarterly and annual reports of the MNCS project.
· Limited facilities including supply of drugs and apparatus of the PSSCs interrupt the MNCS to provide health services to the community people in heard to reach areas. We had proposed “Half-way home”, which could be an alternative to bring remote risk pregnant to nearest delivery centre and, or develop a complete referral package
· Improved results can be achieved if spiritually driven beliefs and practices can be matched with practical demands. For instance, it is a fact that among some ethnic communities, almost all mothers throw the first milk (colostrums) into the river with a view that the satisfied Gods will in return let the mother’s milk this like flow of in abundance. The UNICEF Country Representative during his visit to Bandarban advised us to convince them to continue this practice, but offer the Gods only a few drops of colostrum and provide the rest to the baby. Implementation of this advice has shown that it is working very effectively.
· GoB counterparts of certain NGO/DP-implemented development projects, lack time to attend affairs of such projects, but they become over-committed to these projects because of lack of communication - finally reducing their dedication to the projects to which they are committed by themselves. We have tried to work on this linkage through frequent visits and sharing sessions according to their convenience, which has gradually helped us in ensuring their presence and cooperation in the MNCS Project.
· Community support system is well functioning at the community level but union committees are yet to effectively contribute in the MNCS efforts. Our efforts to ensure participation of representatives from the CSG and Union committees in the Upazila Level meetings has shown significantly positive results to ensure that Union committees are more responsive.
18
5. Major Bottlenecks and Challenges and Measure Undertaken
· Intensive monitoring is a great challenge in remote areas. As a measure to address this issue, we had incorporated a field monitoring system with support received from ICDDRB. Through this system it was possible to monitor the field level activity implementation status of different levels of staff. Other than this an MIS System was also provided by ICDDRB to ensure flow of information to monitor the project progress.
· Scarcity of qualified Community Nurse (CN) and Depot holders in the hard to reach and impossible areas to provide basic health care services is one of the major challenges of the MNCS in these areas, particularly in Thanchi and Ruma. To address this challenge, we had provided support by employing 09 Paramedics and 14 Community Nurses in remote areas to ensure that the local community is able to avail minimum medical services.
· Frequent drop out of health promoters has proved to be one of the main challenges faced during implementation of the Project. To counter this problem, we had initiated different schemes such as year basis performance incentive for the HPs. Other than this 01 HP from each union was provided a small incentive based on her performance on monthly basis. Although population wise distribution of HPs were quite adequate but geographical scattered ness of villages made it difficult for the HPs to cover all their targeted villages within the stipulated time frame.
· Traditionally, the indigenous groups are known for Jhum cultivators in interior hilly places. During Jhum cultivation people live in the deep forest for longer periods (4-5 months) with all of their belongings. There is no way to trace or reach them during this period. Therefore, project performance during cultivation declines and there would seem to be no practical way to improve performance during these months. However, our HPs played a major role in keeping track of the beneficiaries’ whereabouts and this proved to bring in some god results.
· During the entire project implementation period, one of the major challenges faced was to ensure participation of Government personnel in the process. In order to ensure their participation, MNCS had initially formed a committee at the upazila level with members from local level government personnel. However, this did not succeed, after which the committees were re-structured. These committees also failed to make a mark as most of the government level personnel could not provide time.
· 14 Pahari Shasthya Seva Centres situated in hard-to-reach areas which are the only source of health services are running without necessary medicine. District CS office provided medicine once for which patient turnover was increased after which no medicine was available.
6. RISK and RISK MANAGEMENT
During implementation of its activities, MNCS faced some risk in coordination with different stakeholders, ownership building among the community; ensure MNCS services in the remote areas and sustainability of the results after withdrawal of MNCS in its implementation areas.
Building Linkages with Stakeholders
19
Building linkages with different stakeholders was one of the main strategies of MNCS to move forwards towards the goal of intervention. As a part of intervention strategy, MNCS had to built linkages with different types of stakeholders like government and local government staff, community people, other NGOs, etc by formation of committees, organizing meeting, workshops, providing training and conduction of joint monitoring. With undertaking effective measures to involve the service providers like involve as a member of the committee, a participant in skill development training, finally MNCS convinced them to become a part of the MNCS intervention.
Building Ownership among the community People
Ownership of the project by the stakeholders is vital towards its success. It is described as the degree to which stakeholders feel themselves as owners, actors and decision-makers. Regarding to the ownership issues, involvement of community people in the process is essential. With a view to create ownership among the community, MNCS with its full efforts initiated to involve the community people form its initial stage as one of the potential actors to mobilize the community.
MNCS took the process of “OWNERSHIP” by the community people as a serious consideration for institutionalizing the impact and successfully transferred the ownership of intervention to the community by introducing s excellent and active phase out strategydesigned on active involvement of community.
Ensured MNCS services in the remote areas
To ensure the MNCS minimum services in the remote areas, in its third years, MNCS involved 50 depot-holders in three remote Upazilas like Thanchi, Ruma and Alikadam. The depot holders were trained and oriented on MNCS services and provided them with some simple drugs like vitamin A, iron tablet, ORS, etc.
7. Phase-out and Sustainability Plan-implemented
Sustainability of MNCS means to continue the tangible benefits produced by the MNCS for the beneficiaries after the completion of the intervention. In terms of sustainability, ownership of the stakeholders is vital towards its success. Ownership of a project can be described as the degree to which stakeholders feel themselves as owners, actors and decision-makers.
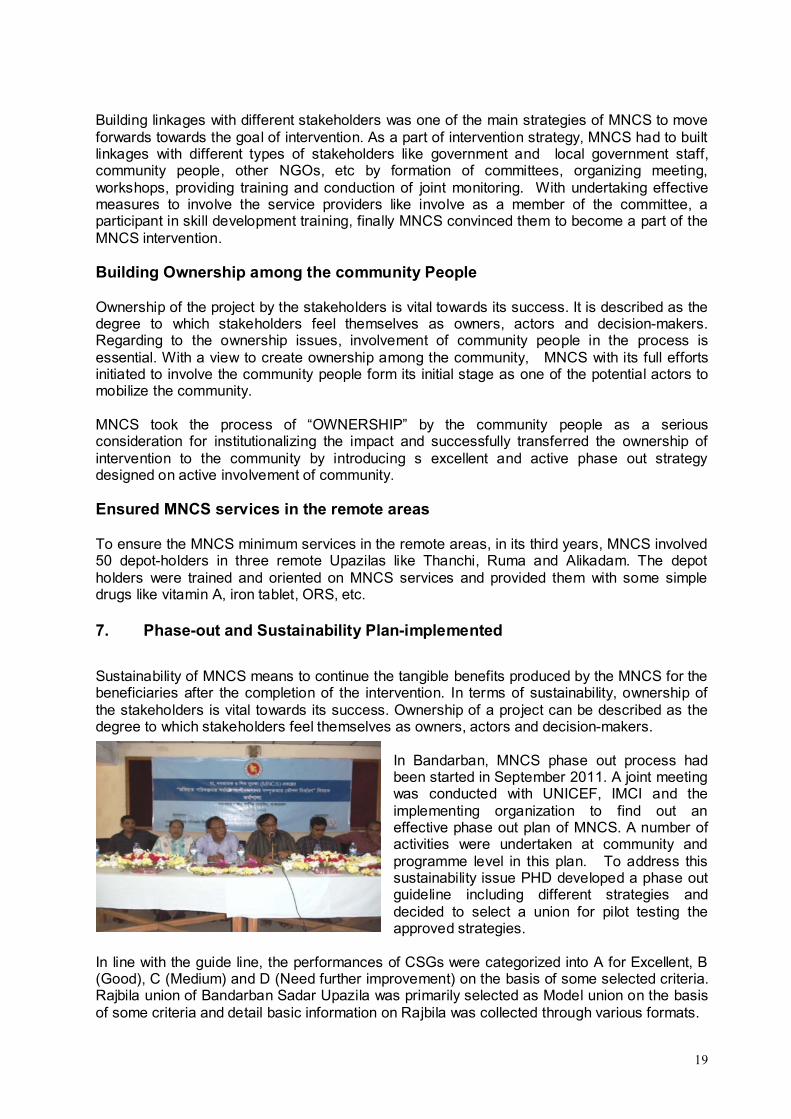
In Bandarban, MNCS phase out process had been started in September 2011. A joint meeting was conducted with UNICEF, IMCI and the implementing organization to find out aneffective phase out plan of MNCS. A number of activities were undertaken at community and programme level in this plan. To address this sustainability issue PHD developed a phase out guideline including different strategies and decided to select a union for pilot testing the approved strategies.
In line with the guide line, the performances of CSGs were categorized into A for Excellent, B (Good), C (Medium) and D (Need further improvement) on the basis of some selected criteria. Rajbila union of Bandarban Sadar Upazila was primarily selected as Model union on the basis of some criteria and detail basic information on Rajbila was collected through various formats.
20
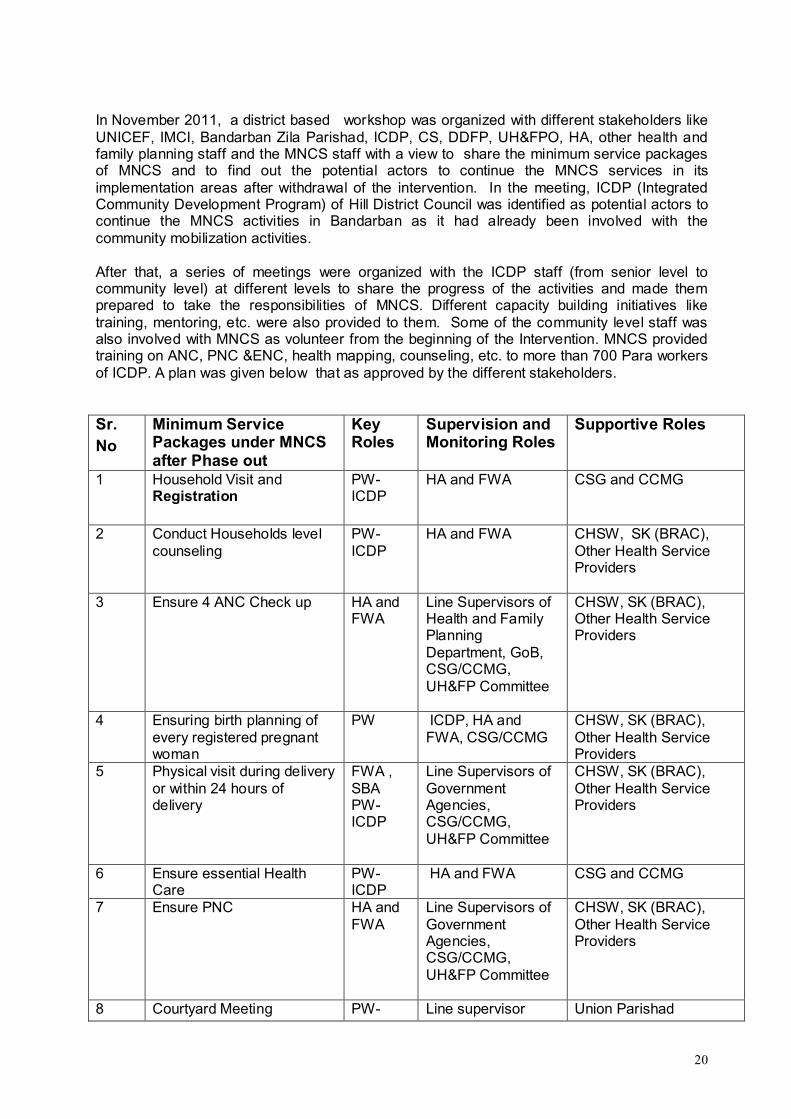
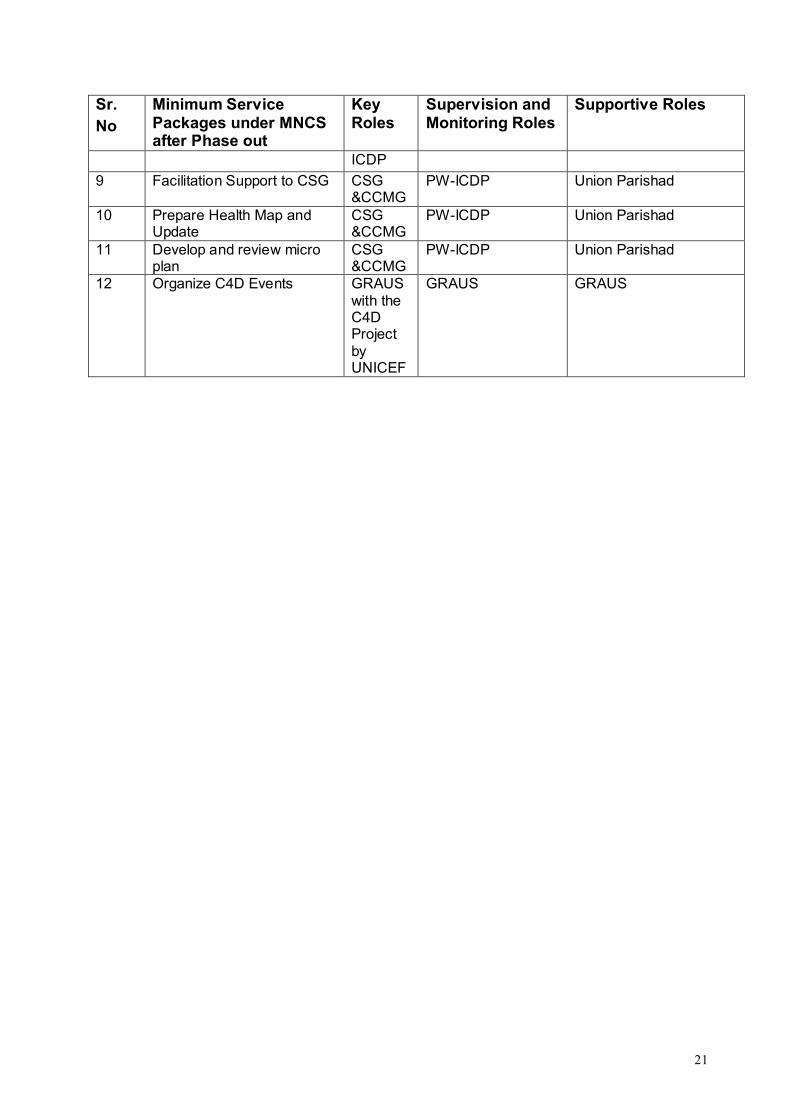
In November 2011, a district based workshop was organized with different stakeholders like UNICEF, IMCI, Bandarban Zila Parishad, ICDP, CS, DDFP, UH&FPO, HA, other health and family planning staff and the MNCS staff with a view to share the minimum service packages of MNCS and to find out the potential actors to continue the MNCS services in its implementation areas after withdrawal of the intervention. In the meeting, ICDP (Integrated Community Development Program) of Hill District Council was identified as potential actors to continue the MNCS activities in Bandarban as it had already been involved with the community mobilization activities.
After that, a series of meetings were organized with the ICDP staff (from senior level to community level) at different levels to share the progress of the activities and made them prepared to take the responsibilities of MNCS. Different capacity building initiatives like training, mentoring, etc. were also provided to them. Some of the community level staff wasalso involved with MNCS as volunteer from the beginning of the Intervention. MNCS provided training on ANC, PNC &ENC, health mapping, counseling, etc. to more than 700 Para workers of ICDP. A plan was given below that as approved by the different stakeholders.
Sr. No
Minimum Service Packages under MNCS after Phase out
Key Roles
Supervision and Monitoring Roles
Supportive Roles
1 Household Visit and Registration
PW-ICDP
HA and FWA CSG and CCMG
2 Conduct Households level counseling
PW-ICDP
HA and FWA CHSW, SK (BRAC), Other Health Service Providers
3 Ensure 4 ANC Check up HA and FWA
Line Supervisors of Health and Family Planning Department, GoB, CSG/CCMG, UH&FP Committee
CHSW, SK (BRAC), Other Health Service Providers
4 Ensuring birth planning of every registered pregnant woman
PW ICDP, HA and FWA, CSG/CCMG
CHSW, SK (BRAC),Other Health Service Providers
5 Physical visit during delivery or within 24 hours of delivery
FWA ,SBA PW-ICDP
Line Supervisors of Government Agencies, CSG/CCMG, UH&FP Committee
CHSW, SK (BRAC), Other Health Service Providers
6 Ensure essential Health Care
PW-ICDP
HA and FWA CSG and CCMG
7 Ensure PNC HA and FWA
Line Supervisors of Government Agencies, CSG/CCMG, UH&FP Committee
CHSW, SK (BRAC), Other Health Service Providers
8 Courtyard Meeting PW- Line supervisor Union Parishad
21
Sr. No
Minimum Service Packages under MNCS after Phase out
Key Roles
Supervision and Monitoring Roles
Supportive Roles
ICDP
9 Facilitation Support to CSG CSG &CCMG
PW-ICDP Union Parishad
10 Prepare Health Map and Update
CSG &CCMG
PW-ICDP Union Parishad
11 Develop and review micro plan
CSG &CCMG
PW-ICDP Union Parishad
12 Organize C4D Events GRAUS with the C4D Project by UNICEF
GRAUS GRAUS
22
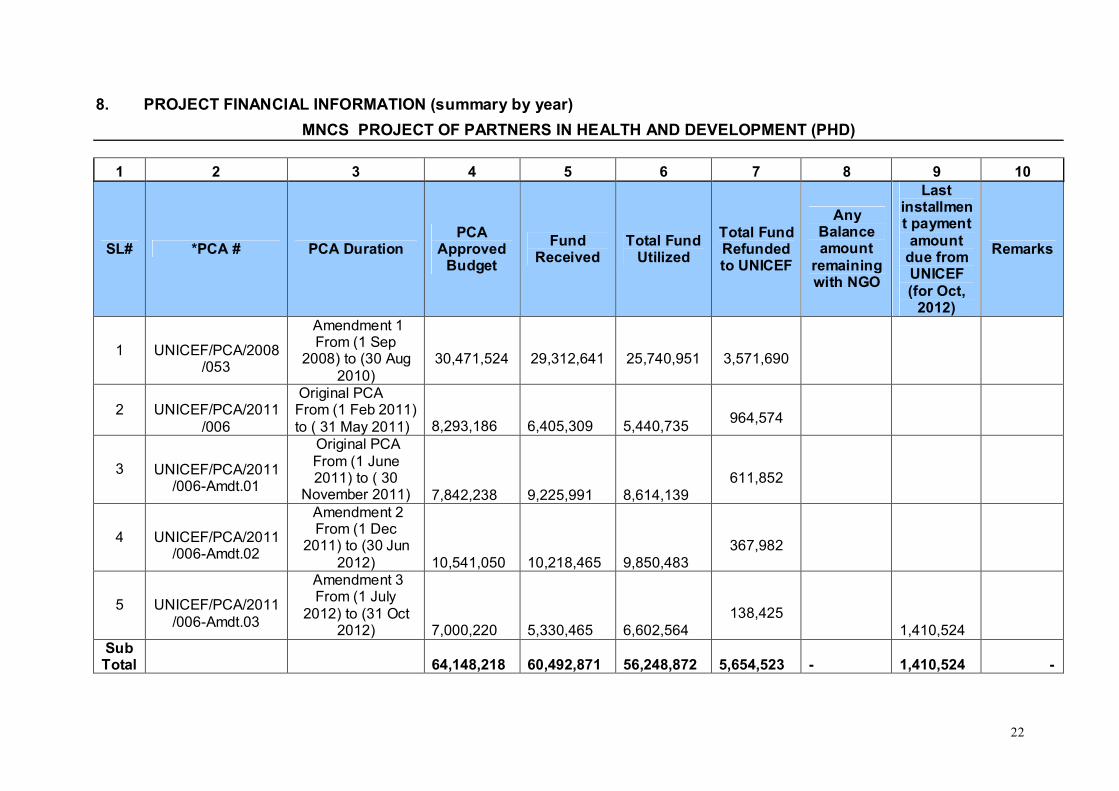
8. PROJECT FINANCIAL INFORMATION (summary by year)
MNCS PROJECT OF PARTNERS IN HEALTH AND DEVELOPMENT (PHD)
1 2 3 4 5 6 7 8 9 10
SL# *PCA # PCA DurationPCA
Approved Budget
Fund Received
Total Fund Utilized
Total Fund Refunded to UNICEF
Any Balance amount
remaining with NGO
Last installment payment amount
due from UNICEF(for Oct,
2012)
Remarks
1 UNICEF/PCA/2008/053
Amendment 1 From (1 Sep
2008) to (30 Aug 2010)
30,471,524 29,312,641 25,740,951 3,571,690
2 UNICEF/PCA/2011/006
Original PCA From (1 Feb 2011) to ( 31 May 2011) 8,293,186 6,405,309 5,440,735
964,574
3 UNICEF/PCA/2011/006-Amdt.01
Original PCA From (1 June 2011) to ( 30
November 2011) 7,842,238 9,225,991 8,614,139 611,852
4 UNICEF/PCA/2011/006-Amdt.02
Amendment 2 From (1 Dec
2011) to (30 Jun 2012) 10,541,050 10,218,465 9,850,483
367,982
5 UNICEF/PCA/2011/006-Amdt.03
Amendment 3 From (1 July
2012) to (31 Oct 2012) 7,000,220 5,330,465 6,602,564
138,425 1,410,524
Sub Total 64,148,218 60,492,871 56,248,872 5,654,523 - 1,410,524 -
23
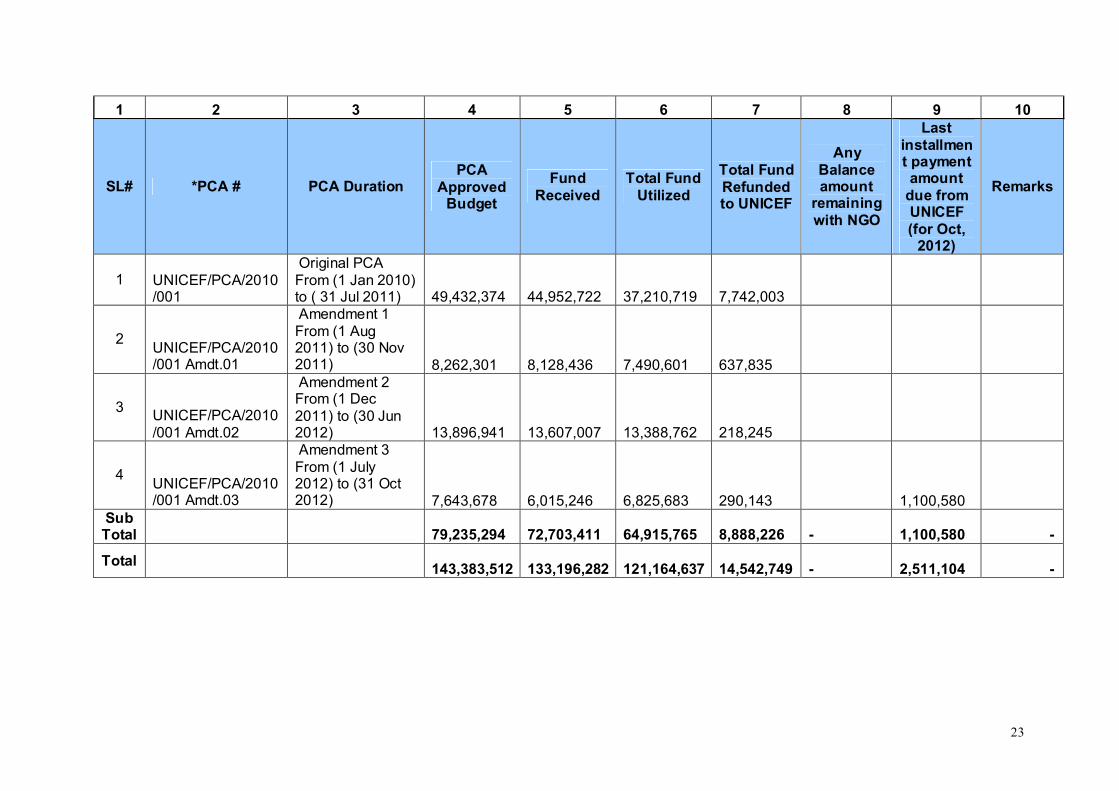
1 2 3 4 5 6 7 8 9 10
SL# *PCA # PCA DurationPCA
Approved Budget
Fund Received
Total Fund Utilized
Total Fund Refunded to UNICEF
Any Balance amount
remaining with NGO
Last installment payment amount
due from UNICEF(for Oct,
2012)
Remarks
1 UNICEF/PCA/2010/001
Original PCA From (1 Jan 2010) to ( 31 Jul 2011) 49,432,374 44,952,722 37,210,719 7,742,003
2UNICEF/PCA/2010/001 Amdt.01
Amendment 1 From (1 Aug 2011) to (30 Nov 2011) 8,262,301 8,128,436 7,490,601 637,835
3UNICEF/PCA/2010/001 Amdt.02
Amendment 2 From (1 Dec 2011) to (30 Jun 2012) 13,896,941 13,607,007 13,388,762 218,245
4UNICEF/PCA/2010/001 Amdt.03
Amendment 3 From (1 July 2012) to (31 Oct 2012) 7,643,678 6,015,246 6,825,683 290,143 1,100,580
Sub Total 79,235,294 72,703,411 64,915,765 8,888,226 - 1,100,580 -
Total143,383,512 133,196,282 121,164,637 14,542,749 - 2,511,104 -

24
9. RECOGNITION OF GOB/AusAID/UNICEFS CONTRIBUTION-· A team of UNICEF, headed by Mr. Louis Georges Arsenault, Country Representative
UNICEF, Bangladesh visited Counseling Session conducted by the MNCS project staffs in Amtoli Tanchangya Para of Shoalok union, Bandarban. This visit was accompanied by the District Program Officer of Unicef of Bandarban, District Coordinator of ICDP project of CHTDB, Medical Officer of Civil Surgeon Office, UFPO of Bandarban Sadar, Managing Director of PHD and Executive Director of GRAUS. The Representative of Unicef Bangladesh discussed with the CSG members and also with local peoples on the benefits they gained from the MNCS project and their expectation from the project. The Managing Director of PHD explained in details on the project strategies and approaches of MNCS.
· Government of Bangladesh (GoB) along with AusAID-UNICEF jointly visited a Paharia Shasthya Seba Clinic run by MNCS project at Manjoy Para, Rajbila union of Bandarban Sadar. The team headed by Ms. Zabeta Elizabeth Moutafis, First secretary of Australian High commission in Dhaka. Dr. Birthe Locatelli-Rossi, Chief- Health & Nutrition section, Ms. Jenny Finch Senior Program officer, Aus AID and other senior officer from the UNICEF was in the team.
. · Ms. Midori Sato, Health Manager, Health and Nutrition Section of Unicef-Bangladesh,
visited MNCS areas-- Jogesh Karbari Para of Rajbila Union and Pora Para of Shoalok Union. Dr Mohsin Ali, Nutrition Specialist of Unicef-Bangladesh, Dr. Ubaswe Chowdhury, Program Officer of Unicef- Bandarban and District Coordinator of ICDP were in the team.
· Mr. Takoa Toda, Chief Representative of JICA and Ms. Saeda MAKIMOTO, Representative (Health, Governance) visited one of the CSG, Amtoli of Soalok union under Bandarban SadarUpazila. In their visit, they discussed different issues with the CSG members.
25
10 Conclusion
The project is one of a unique kind of intervention to improve the health care practices at home and care seeking through utilization of neonatal and child health and nutrition services by families, particularly the poor and excluded communities of Bandarban. The intervention has started a process for the community people to act in a more united way and opened new windows and doors to the women and children with the new experiences of MNCS issues. It has also changed the existing situation of maternal, neonatal and child health regarding neo born care, ANC and PNC check up, treatment of child illness etc. although not in a significant way.
The two years intervention has not yet been well equipped to create ownership among the community people to carry on the MNCS activities with full confidence. MNCS intervention requires support to develop phase out plan with clear and specific future strategies to handover the activities to the community people.
26
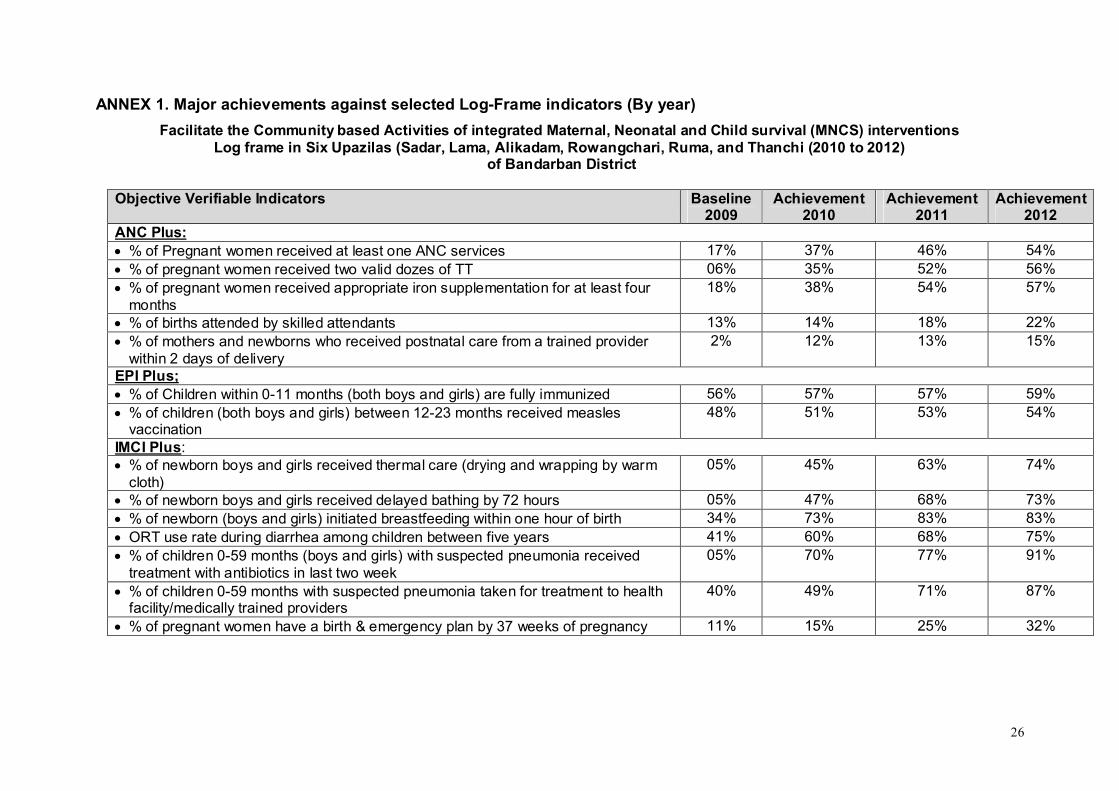
ANNEX 1. Major achievements against selected Log-Frame indicators (By year)
Facilitate the Community based Activities of integrated Maternal, Neonatal and Child survival (MNCS) interventionsLog frame in Six Upazilas (Sadar, Lama, Alikadam, Rowangchari, Ruma, and Thanchi (2010 to 2012)
of Bandarban District
Objective Verifiable Indicators Baseline 2009
Achievement2010
Achievement2011
Achievement2012
ANC Plus:· % of Pregnant women received at least one ANC services 17% 37% 46% 54%· % of pregnant women received two valid dozes of TT 06% 35% 52% 56%· % of pregnant women received appropriate iron supplementation for at least four
months18% 38% 54% 57%
· % of births attended by skilled attendants 13% 14% 18% 22%· % of mothers and newborns who received postnatal care from a trained provider
within 2 days of delivery2% 12% 13% 15%
EPI Plus;· % of Children within 0-11 months (both boys and girls) are fully immunized 56% 57% 57% 59%· % of children (both boys and girls) between 12-23 months received measles
vaccination48% 51% 53% 54%
IMCI Plus:· % of newborn boys and girls received thermal care (drying and wrapping by warm
cloth)05% 45% 63% 74%
· % of newborn boys and girls received delayed bathing by 72 hours 05% 47% 68% 73%· % of newborn (boys and girls) initiated breastfeeding within one hour of birth 34% 73% 83% 83%· ORT use rate during diarrhea among children between five years 41% 60% 68% 75%· % of children 0-59 months (boys and girls) with suspected pneumonia received
treatment with antibiotics in last two week05% 70% 77% 91%
· % of children 0-59 months with suspected pneumonia taken for treatment to health facility/medically trained providers
40% 49% 71% 87%
· % of pregnant women have a birth & emergency plan by 37 weeks of pregnancy 11% 15% 25% 32%
27
ANNEX 2. Case studies
Case Study 01.
Case of safe delivery at the Hospital.owalok is one of many Unions of Bandarban Upazila. This union comprises of 55 Paras (Neighborhoods), among which one is “Headman Para”. Most of the inhabitants here are of the Marma Community. Most people are illiterate and rely mainly on Joom (Traditional
method of harvesting in hilly areas) Cultivation. Needless to say that most people here are economically poor.
Kroma Thui Marma, a 19 year old pregnant woman is an inhabitant of Headman Para. Kroma Thui’s husband’s name is Mong Shing Nu Marma. It is the first time that Kroma Thui Marma is experiencing pregnancy. She has received 1st and 2nd counseling from MNCS Staff Ukhay Pru Marma. As Kroma Thui has been found to be anemic, the MNCS staff has explained to the family regarding the importance of nutritious food for the pregnant woman. Also, she has discussed and explained to the family regarding the importance of a comprehensive birth planning and delivering the child at a hospital. Sadly, the family members did not follow the MNCS staff’s advice. Upon being informed of this, Ukhay Pru Marma (the MNCS staff) met with the CSG Chairperson Mr. Monjurai Tanchangya on the 5th of November 2011 and went with him to Kroma Thui’s home. Together they explained about the importance of delivering the child at a hospital in order to avoid any risk for the mother and child. Upon hearing this, the pregnant woman’s mother-in-law became upset and said that she herself has given birth to 08 (eight) children and all of them were born at home. She said that nothing has happened to her and the Almighty has kept her safe from all harm. Why should she send her daughter-in-law to a hospital? Sending her daughter-in-law to hospital might result in her (daughter-in-law) death. The CSG chairperson and the MNCS staff did not give up and tried to convince them to take a decision for a hospital delivery. As a precaution, they provided their telephone numbers and said to contact them in case of any emergency.
At about 04:00 p.m. on the 10th of November 2011, the pregnant woman’s labour pains began, after which the husband called in a birth attendant. However, even after going through labour for about 13 or 14 hours, the child was not delivered. In this instance, the birth attendant told the husband to sacrifice a chicken to God at the river. When this also did not work, the husband called for a Baidya (Traditional spiritual healer) in the evening, who advised the husband to sacrifice a goat in the name of the Gods. Since the husband could not afford a goat, he saw no other alternative and called the CSG chairperson in his mobile phone at about 11 p.m. and explained his problem. Upon receiving this information, the CSG Chairperson called the MNCS staff and together went to the pregnant woman’s home. They both saw the situation and advised the husband to take his wife to the hospital immediately. The husband said that he did not have enough money to go to the hospital at that moment. In this situation, the CSG Chairperson handed the husband taka 500/- with which the husband took his pregnant wife to the hospital around 12:00 a.m. At approximately 12:50 a.m. the pregnant woman was admitted to the Labour Ward of Bandarban Sadar Hospital.
The doctors and nurses immediately attended to the pregnant mother and through their efforts, a baby was born at about 03:15 a.m. on 11th November 2011. Immediately after birth, the child was facing difficulty in breathing by itself, for which it was given supplementary oxygen for the remainder of the night. The doctors observed that the child’s breathing had stabilized by early morning and could breath on its own.
Mother and child have been released from the hospital and are both doing well at the time of writing this report.
Recorded/Documented by : Zarna Das, Union Facilitator, Sualok Union, Bandarban
December 2011
S

28
Case Study 02.
Mother’s Dream comes true
Dosingnu Marma, an 18 year old pregnant woman from Kamlong Para (Ward No 9) under Khohalog union of Bandarban Sadar Upazila of Bandarban District had been registered in the MNCS Surveillance register by Health Promoter Cho Ma Thui. As Dosingnu had previously lost two babies shortly after delivery, she was treated as a very serious case. The HP also understood the frustration that Dosingnu felt regarding her lost pregnancies.
Dosingnu’s 19 year old husband earned a living for himself and his family through Jum Cultivation. They lived in a very small house and the economic situation was not very stable
The HP took this case as a challenge and provided intensive care through frequent visits and advice on diet, ANC check up, TT, danger sign of pregnant mothers and new born. The HP also took Dosingnu to the FWC for ANC check up, which Dosingnu did not practice previously. The HP and the CM also talked with traditional birth attendants of the areas, who generally deliver babies in the locality and discussed the danger sign of pregnant and neo natal, cleaning and wrapping, delayed bathing, etc. In the monthly meeting of CSG, Cho ma Thui discussed Dosingnu’s case and asked the members of CSG to follow up her physical condition regularly. The CSGs members also provided her a penny bank for savings and advised her to use the savings during her delivery to meet the emergency. Regarding the case, Monjoyshing Marma, the president of CSG said that they had provided her their cell phone numbers so that she could call them at any time if she faces any physical problems during pregnancy.
At the 8th month of her pregnancy, one evening, Dosingnu felt sick and immediately informed the traditional birth attendant, who tried her best to deliver the baby, but finally failed. At that time Dosingnu Marma’s husband was not at home and was involved with Jum cultivation. One of her neighbors immediately called the HP and the secretary of CSG. The secretary of CSG along with some of the CSG members reached her home and initiated to send her to the Sadar Hospital. However, her mother–in law became very annoyed with the decision of CSG members and she started shouting and saying that the
CSG members would be responsible if there were any mishaps of her daughter-in-law. Besides this, it became difficult for them to manage transport to shift her as it was raining heavily. However, the secretary managed a baby- taxi and sent her to Sadar hospital ignoring her Mother-in-law’s shouting. The next day, Dosingnu delivered a healthy baby girl.
Immediately after birth, one of her neighbors, tried to welcome the child with a drop of CHABRISHAKRI (a mixture of local liquor and a gall-bladder of python), which is a traditional practice. The CM who was present in the hospital prohibited her to do that and asked her to immediately allow the mother to provide colostrums to the baby instead. The relatives did not want to listen to the CM and stressed on that fact that this was their tradition. In order to convince the relatives, the CM called the secretary of the CSG, who arrived shortly and after quite a while was able to convince the relative to give colostrums to the baby. During the visit of the PC of MNCS, Dosingnu’s expression of gratitude was through these words: “I am really grateful to all of them who helped me to become a mother of a healthy child. Without their help it would not be possible for me to go the hospital because my mother-in-law would not have allowed me to do so”.

29
Case Study 03.
Jingrumoy Bom lives with her husband Chamsang Bom in Lamai Para under Bandarban Sadar Union of Bandarban District. The family does not have any land and both the husband and wife work as day laborer.
When she was identified as a pregnant of five months, already she had a daughter and a son. She delivered her previous two children at home and previously she did not take any ANC and PNC check up services from any organization or any person.
As our target she was provided with counseling on home care practices and asked her to go to nearby FWC or community clinic for ANC check up. But her husband did not allow her to go for check up and he also compelled her to go to the field to work with him instead of going for check-up. Then CM discussed the issue in the monthly meeting of CSG and after the meeting all of them went to Bom’s family. There they found the house was locked and they were informed that last night the family shifted from here to the hill where they worked.
At the time of delivery the Bom family again came back in the community. It was kept secret. Hearing the information, the CM met the family and found that the pregnant women was so weak to move and a Samon (traditional healer) was organizing a worship to save the mothers from the sin evil. CM felt very nervous and she immediately met some of the CSG members and asked them to take immediate action. After taking many efforts the CSG members was able to convince the family and took her to the Upazila Hospital. There she delivered a male child.
30
Case Study 04.
Halima’s Story-A citizen Initiative
Halima Begum lives in Kadukhola, a remote village of Sualok union under Bandarban Upazilaof Bandarban District. Halima Begum is a house wife and her husband Abdual jalil is a day laborer. One day her only daughter (3 months) became very sick with fever and active convulsion. But Halima did not have enough money to go to the Bamdarban Sadar Hospital, which is 25 kilometers away from her village. Then she met Nurunahar, Community Mobilizer of MNCS Intervention and informed her about her daughter’s sickness. Nurunnahar met some members of Community Support Groups (CSGs) and requested them to help the distressed mother. Considering the reality and condition of Halima, the CSG Members took the responsibility of the daughters of Halima. The members discussed the matter among themselves and collected Tk. 1500 from the members of CSG and also from the Community people. After two days, Halima was released by Sadar Hospital with her sick daughter. After returning from the Sadar Hospital, the condition of Halima’s daughter began to get worse. She again met with Community Mobilizer of sualok union and cried out to save her daughter. Then she talked with the doctor of Bandarban Sadar Hospital but doctor said that the patient would be recovered gradually. Without finding any improvement, Halima with the help of Nurunahar (CM) went to the Hospital again.. There Nurunnahar talked with the doctor and Halim’s a daughter was diagnosed as the patient of pneumonia. Immediately she was admitted in intensive care. After a week Halima was released and came back with her daughter. Regarding the efforts and support of CSG Halima said: I am grateful to CSG and Nurunnahar Apa for providing us both financial and mental support for saving the life of my only child.
31
Case Study 05.PHD-GRAUS
Case Study from Aziznagar, Lama – Bandarban
Aziznagar is one of the six Unions under Lama Upazila. Aziznagar happens to be the most backward in education, Health Service, and many other aspects in comparison to the other Unions of Lama Upazila. As a result a large number of pregnant mothers and new born children fall victim to untimely death every year. Such a story could have been that of PeiGee Marma, a young woman of Headman Para of Ward number 02 from Aziznagar. Peigee Marma’s husband’s name is ThuiHlaching Marma.
Peigee Marma had in the past lost her first child due to not being aware about health care precautions during pregnancy. This has had a profound effect on her and she was reluctant to conceive again due to fear of losing another child.
However, when Piegee became pregnant for the second time, she was provided counseling by MNCS staff, who gradually made her and her family aware regarding the importance of proper health care before and during pregnancy. Now Peigee is aware of issues such as danger signs of pregnancy, Danger signs of new born babies, Importance of Thermal care, breast-feeding within one hour of birth, etc. She also knows the importance of not doing heavy work during pregnancy and the importance of of a balanced diet as well as taking sufficient rest. She now regularly goes for checkup and takes Iron Folet supplements regularly. As a result, she ensured that her second child is delivered in the hospital which resulted in the delivery of a healthy baby.
There is a vast difference between the person that Piegee was and now is. Piegee is a proven fact that it is possible to change peoples’ mentality and behaviour through counseling and information dissemination.
Documented by :Mohammad Asif JoardarUnion FacilitatorAziznagar UnionLama, Bandarban

32
ANNEX 3. Detail Final Report (Quarter and year wise against approved budget)
Status of MNCS Intervention in Bandarban and Lama Upazila
Period: September 2008 to July 2010
August 2010
Submitted to: UNICEF
Submitted by:
Partners in Health and Development (PHD)
Gulshan
33
1. Introduction
Since September 2008, Partners in Health and Development (PHD) has been implementing
the MNCS (Maternal, Neonatal and Child Survival) project of UNICEF with its partner NGO
GRAUS in 11 unions of Bandarban Sadar and Lama Upazilas under Bandarban district. The
unions are: Bandarban Sadar Union, Rajbila Union, Kuhalong Union, Tonkabati Union, Sualok
Union of bandarban Sadar Upazila and Lama Sadar Union, Aziz nagar Union, Soroi Union,
Fasia khali Union, Gojalia Union and Ruposi Union of Lama Upazila.
2. Objectives of the Project
The objectives is to improve the home care health practices and increased care seeking
behaviour of communities and utilization of neonatal and child health and nutrition services by
families particularly poor and excluded communities lives in Sadar and Lama Upazila under
Bandarban District.
3. Specific Objectives of the Project
· Increase participation of the community in planning, implementation and monitoring of MNCS intervention packages
· Increase their participation and ownership of maternal, neonatal and child survival program in their catchments areas
· Increase availability and quality of MNCS package of care and services at health facility and community level.
4. Geographical Context of the Areas
Bandarban is one of the three hill districts of Bangladesh and situated in the south-eastern part of the country. It is not only the remotest district of the country, but also is the least populatedareas. It consists of 7 upazilas, 32 unions, 160 mouzas, 1488 villages, 2 municipality (18 wards and 62 mahallas). The upazilas are bandarban Sadar, rowangchhari, ruma, thanchi, lama, alikadam, and naikhoncchari. This region consists almost entirely of hard-to-reach areas. Most of the parts of this place are inaccessible. Culturally Bandarban is governed by the local King (Bomang Raja) and his local representatives (Headmen and Karbaries).
34
Total number of population is 340337. Out of which 53.39% are male and 46.61% are female. Ethnic identity is a dominant factor for social group formation among indigenous peoples. Ethnic nationals include the marma, mro, tripura, bawm, tanchangya, chakma, chak, khyang, khumi, lushei and the pankho.
5. Staffing
Project staffs consisted of a District coordinator (DC) -1, Upazila Manager (UM)-2, MIS & Training Officer (1), Monitoring Officer (1), Union Facilitators (UF)-11, Community Mobilizers (CM) -44 and Health Promoters (HP)-80.
6. Human Resources and Development
To build the capacities of the staff MNCS provided various ToT, training to its staff and also to the beneficiaries of the MNCS. Some of the important interventions were discussed below. A list of ToT/Training/orientation delivered by UNICEF and PHD is attached as annex 1.
6.1 Capacity Building of Project Staff
· TOT on HH Registration Format, Rapid Assessment Tools and Mapping
A two-day long TOT on Household Registration and Rapid Assessment Tools was conducted by ICDDR, B of Dhaka. A total of 22 project staff attended the ToT. Among them, Union Facilitators (11) and Community Mobilizers (7) attended the ToT. The ToT on HH Registration Format and Rapid Assessment Tools and Mapping. These formats included economic status of the households, households with pregnant mothers and children of under 5, health care practices, sources of health care, situation of care givers-counseling, referral system, etc.
A field-test on application of tools and techniques of assessment was conducted inKuhalong union of Bandarban Sadar Upazila.
· ToT on Community Need Assessment and Knowledge, Attitude, Behaviour Practice and Analysis (KABPA) Tools
A four-day long TOT on Community Need Assessment and Knowledge, Attitude, Behavior, Practice and Analysis (KABPA) tool was provided by Communica. . The ToT provided skills on the application of the techniques of Knowledge, Attitude, behaviour Practice and Analysis (KABPA), conduction of FGDs and Development of report based on KABPA. A total of 14 staff attended the ToT.
A field test was conducted in the two WARDs of Kuhalong Union of Bandarban Sadar upazilla. The participants conducted FGDs, interview and discussion with different stakeholders.
· ToT on Capacity Development for the Formation of Community Support Group (CSG)TOT on Formation of Community Support Group (CSG) was facilitated by the Communica. A total of 19 staff attended the ToT.

35
A field test was conducted in the wards of Shoalog Union of Bandarban Sadar upazilla. The participants conducted FGDs, interview and discussion with different stakeholders. Finally a report was prepared report on the basis of findings generated from the field test.
· Training on Assessment tools Development Training on Social mapping and Problem prioritization
Training on Social map and Problem prioritization was provided to some selected project staff. This training was provided by PHD. A total of 31staff attended the assessment training. The participants were divided into three groups to practice the tools in the field and find out any problem faced during the field operation. The first team visited Manjoy headman Para and Jamchari Para of Rajbila Union and Goal khola of Bandarban Sadar. After the field work, a feed back session was organized in the evening. The group presented their activities in details and reporter presented their reports. The participant discussed the problems they faced in the field.
· ToT on C-IMCI
Communica provided ToT on counseling to the project staff (42) in two batches. The training provided orientation on C-IMCI intervention, group counseling for C-IMCI, danger signs of new born babies, early childhood development, etc.
· ToT on MNCS Ward Committee Formation and Micro Planning
UNICEF provided a ToT on WMNCS Committee Formation and Micro Planning was conducted to the 53 project staff of the MNCS in two batches. The participants orientated on community mobilization, basic concept of Ward MNCS Committee and their roles and responsibilities, process of planning and micro- planning, etc.
· ToT on MIS surveillance registers
Two ToT on MIS Surveillance Register was provided to 42 staff. After that the trained staff provided the training to 78 staff of MNCS. A total of 120 participants attended in these training sessions. After the training the register was used in the field to record the health related information of the community people.
· Training on C-IMCIAfter receiving ToT some selected staff of MNCS provided training to other staff of the MNCS project. A total of 84 staffs of the MNCS received training on C-IMCI.
· Training on Popular Theatre
A total of 15 staff was provided with training on popular theatre. They learned the techniques on how to develop script on various problems and demonstrate the problem to aware the community people on the particular problem.
36
· Orientation on role & responsibility and counseling
75 Health Promoters oriented on basic information of MNCS. They were oriented on MNCSrelated issues like essential care to new born babies, child care and service, role and responsibilities of HPs, effective communication on delivering the message, etc.
· Orientation on MIS Surveillance Register
An orientation on MIS Surveillance format was conducted by the ICDDRB. A total of 17 representatives of different categories of MNCS staff attended the orientation session. The main purpose was to update the existing format developed by ICDDRB. A field test was also conducted and the feed back provided by the different staff.
· Financial management training
Financial management training was provided to 13 staff by PHD. The staff of MNCS was oriented on some financial aspects like internal control, cash management, banking operation management, etc.
· Training on Right Based Approach
PHD provided a training on Right based Approach to 22 MNCS staff. the content of the training focused on human rights, rights and service delivery, advocacy, decision making, staff motivation, etc.
· Orientation Package for UP Representatives
An orientation package on Mother and Neonatal Health was provided to the MNCS Project staff in October. Dr. Tasrina Rahman facilitated the session. A total of 16 MNCS staff oriented on the maternal and neonatal health issues.
· . Training on Participatory Rural Appraisal
A Participatory Rapid Appraisal Training was provided to 15
MNCS staff by PHD. . The participants were oriented on
different tools of PRA like Venn diagram, Force Field
Analysis and Changing Trend. After the completion of the
training the participants practiced the tools in the field. The
main purpose of the training was to strengthen the capacity of the staff members on
Participatory Rapid Appraisal (PRA) so that they would be able to design, develop and
practice participatory monitoring & evaluation tools, etc.
37
· Training on ANC, PNC and ENC
The training was provided to 135 staffs in 5 batches. Trained staff of MNCS who received the TOT training conducted the sessions. The training provided basic concept on present health situation of maternal and child health in Bangladesh, role of community counselor, basic concept on maternal health care, general problems during pregnancy period and risk sign symptoms, postnatal care, newborn care and importance of breast feeding, taking care of sick children, danger signs of newborn and practical demonstration on conduction of counseling and group education etc.
· Refresher Training on C-IMCI
The project organized two batches of C-IMCI refreshers training during 6-7 & 8-9 December 09 at Royal conference room, Bandarban. A total number of 59 MNCS Project staffs attended in this training. The training was conducted by PHD. The training provided basic concept on C-IMCI intervention, group counseling for C-IMCI, danger signs of new born babies, early childhood development, taking care of sick children, danger signs of newborn and practical demonstration on conduction of counseling and group education etc.
· Training on Supportive Supervision
Training on Supportive Supervision and monitoring matrix was provided to the 27 staff. The main purpose of the training was to provide knowledge on supervision and monitoring. Various tools for supervision and monitoring matrix were developed.
6.2 Capacity building of Community People
· Training on MNCS Ward Committee Formation and Micro Planning
After receiving ToT, the trained project staff delivered the training to 1550 CSG/WMNCS/CCMG in 52 batches.
· Orientation with Headmen and Karbaries
Two orientation sessions were provided to the 46 Headmen and Karbaries of 11 unions of Bandarban Sadar and Lama Upazila in September 2009. The participants oriented on aim and objectives of MNCS Project, different perspective of the formation of ward MNCS /CSG committee, role and responsibilities of CSG and finally the roles and responsibilities of Headman and Karbaries on citizen monitoring for implementation of MNCS project effectively.
· Orientation of Opinion Leaders
Three training on Role of opinion Leaders was provided to 193 opinion leaders, where only 10 (11%) were female leaders. In Lama the training was inaugurated by the UH & FPO of Lama Upazila and the Civil Surgeon of Bandarban district in Bandarban. The participants discussed the MNCS project activities and role of opinion leaders in the implementation of project activities.
· Training on Leadership and CSG Management
38
Leadership and CSG management was provided to the selected 176 CSG leaders. In the
training the participants were oriented on the following issues like concept of human resource
development, concept & types of leadership, role of CSG leaders, community participation,
local resource utilization in community mobilization process, meeting management, decision
making process and citizen monitoring.
7. Overall Achievement
7.1 Increased participation of the community in MNCS interventions packages
7.1.1 Formation of CSGs
With a view to ensure the community mobilization and develop ownership among the community people on MNCS intervention, 99 Ward based Community Support Group (CSGs) from each 99 Wards of 11 unions of Lama and Bandarban Upazilas were formed. Each CSG consists with different representatives both from the community leaders like headman, Karbaries and Government propel from Health and Family Planning department. In 14 wards, the CCMG (Community Clinic Management Group) and Pahari Shyastha Seva Clinic (PSSC) Committee were considered as CSGs. In the project implementation areas the number of CCMG is 14 (8 in Lama and 6 in Bandarban).
The Ward based CSG committee consists of women UP members, respective male member, Family Welfare Assistant (FWA), Health Assistant, Headman, Karbari, Health Promoter and two adolescents. The number of the members vary from 11-17. The concerned male or female member and health or Family Planning Assistant work as president and secretary of the CSG committee consequently. The rate of female members in the committee is 48%.
The main responsibilities of the CSGs are
· To conduct regular meeting to discuss the MNCS issues, keep them updated with basic information like total number of households, number of households with pregnant mothers and mothers of new born child, number of neonates, households with < 1 year; households with < 5 years Children,
· To mobilize the community to utilize the health services of EPI outreach, satellite clinics, Community Clinics, Village doctors, other NGO clinics, HA and FWA etc.
· To develop local level action plan and develop action plan on the basis of the micro plans
· To ensure the process of citizen monitoring to ensure the quality of the project initiatives
The members of the CSG meet once a month and the Para Center of ICDP are used as meeting places of the CSG. In the monthly meeting, Health promoter of MNCS share the statues report of the community with the members and the members exchange their views on the report.
7.1.2 Development of Micro Plan
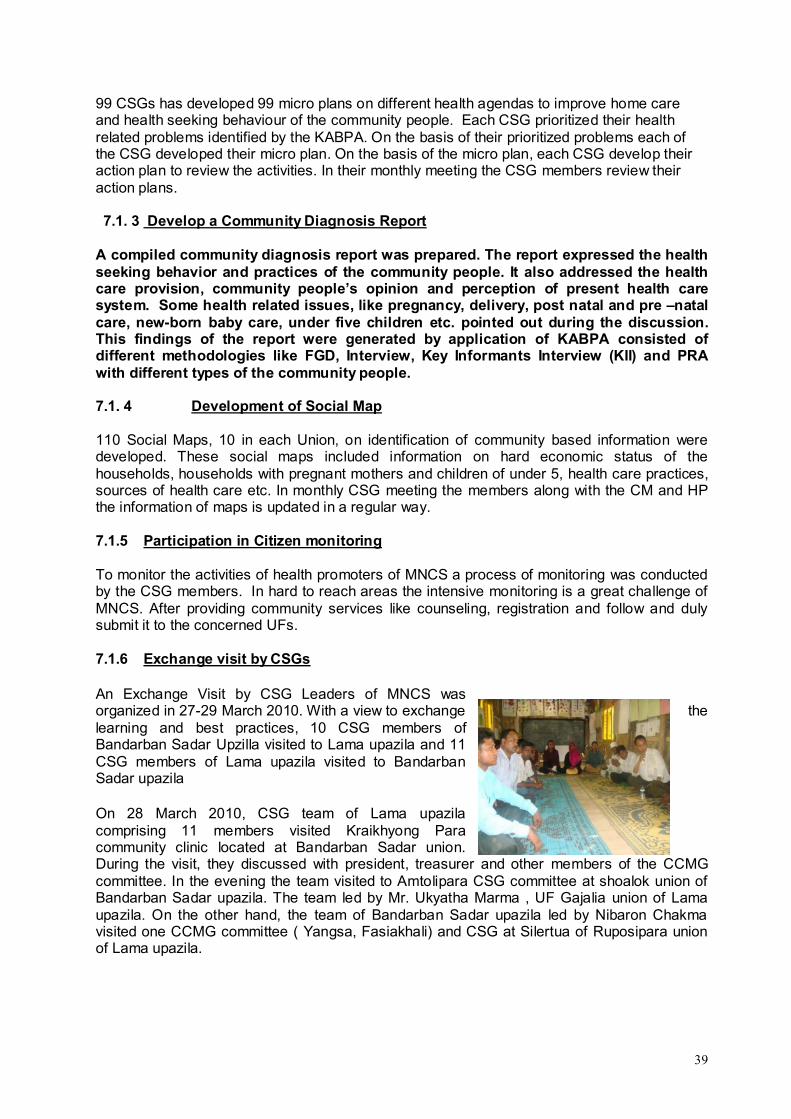
39
99 CSGs has developed 99 micro plans on different health agendas to improve home care and health seeking behaviour of the community people. Each CSG prioritized their health related problems identified by the KABPA. On the basis of their prioritized problems each of the CSG developed their micro plan. On the basis of the micro plan, each CSG develop their action plan to review the activities. In their monthly meeting the CSG members review their action plans.
7.1. 3 Develop a Community Diagnosis Report
A compiled community diagnosis report was prepared. The report expressed the health seeking behavior and practices of the community people. It also addressed the health care provision, community people’s opinion and perception of present health care system. Some health related issues, like pregnancy, delivery, post natal and pre –natal care, new-born baby care, under five children etc. pointed out during the discussion. This findings of the report were generated by application of KABPA consisted of different methodologies like FGD, Interview, Key Informants Interview (KII) and PRA with different types of the community people.
7.1. 4 Development of Social Map
110 Social Maps, 10 in each Union, on identification of community based information were developed. These social maps included information on hard economic status of the households, households with pregnant mothers and children of under 5, health care practices, sources of health care etc. In monthly CSG meeting the members along with the CM and HP the information of maps is updated in a regular way.
7.1.5 Participation in Citizen monitoring
To monitor the activities of health promoters of MNCS a process of monitoring was conducted by the CSG members. In hard to reach areas the intensive monitoring is a great challenge of MNCS. After providing community services like counseling, registration and follow and duly submit it to the concerned UFs.
7.1.6 Exchange visit by CSGs
An Exchange Visit by CSG Leaders of MNCS was organized in 27-29 March 2010. With a view to exchange the learning and best practices, 10 CSG members of Bandarban Sadar Upzilla visited to Lama upazila and 11 CSG members of Lama upazila visited to Bandarban Sadar upazila
On 28 March 2010, CSG team of Lama upazila comprising 11 members visited Kraikhyong Paracommunity clinic located at Bandarban Sadar union. During the visit, they discussed with president, treasurer and other members of the CCMG committee. In the evening the team visited to Amtolipara CSG committee at shoalok union of Bandarban Sadar upazila. The team led by Mr. Ukyatha Marma , UF Gajalia union of Lama upazila. On the other hand, the team of Bandarban Sadar upazila led by Nibaron Chakma visited one CCMG committee ( Yangsa, Fasiakhali) and CSG at Silertua of Ruposipara union of Lama upazila.
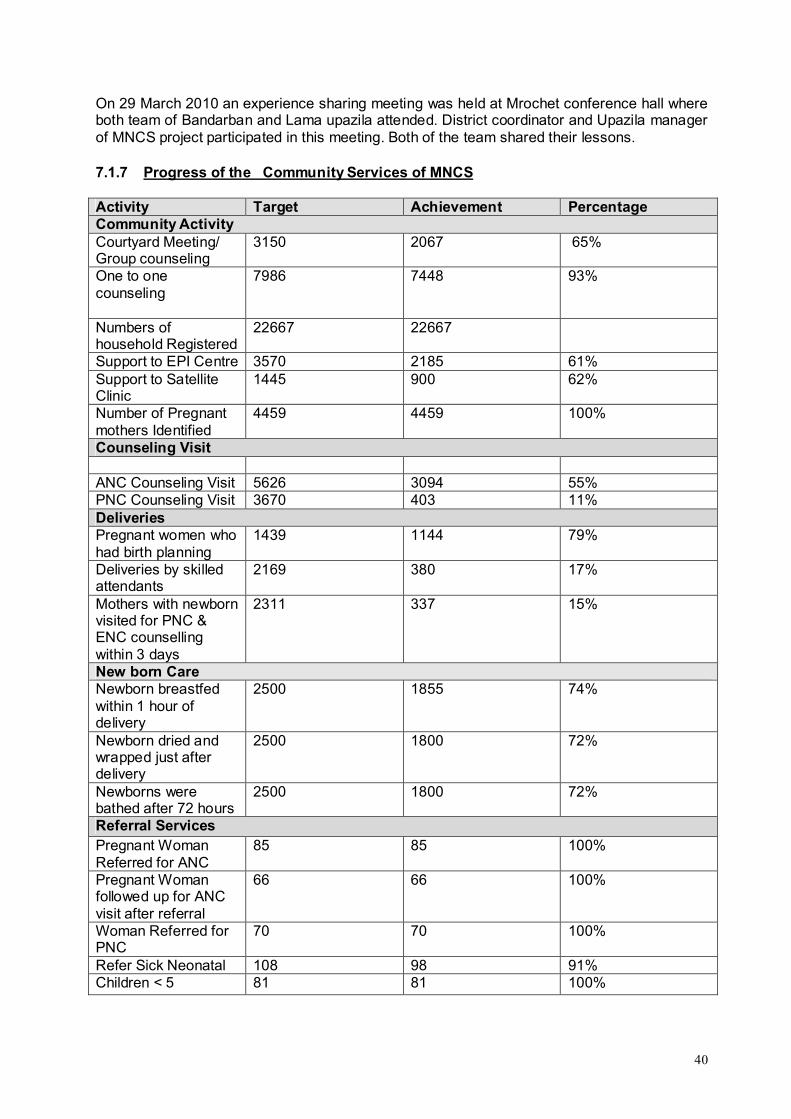
40
On 29 March 2010 an experience sharing meeting was held at Mrochet conference hall where both team of Bandarban and Lama upazila attended. District coordinator and Upazila manager of MNCS project participated in this meeting. Both of the team shared their lessons.
7.1.7 Progress of the Community Services of MNCS
Activity Target Achievement Percentage Community ActivityCourtyard Meeting/ Group counseling
3150 2067 65%
One to one counseling
7986 7448 93%
Numbers of household Registered
22667 22667
Support to EPI Centre 3570 2185 61%Support to Satellite Clinic
1445 900 62%
Number of Pregnant mothers Identified
4459 4459 100%
Counseling Visit
ANC Counseling Visit 5626 3094 55%PNC Counseling Visit 3670 403 11%DeliveriesPregnant women who had birth planning
1439 1144 79%
Deliveries by skilled attendants
2169 380 17%
Mothers with newborn visited for PNC & ENC counselling within 3 days
2311 337 15%
New born CareNewborn breastfed within 1 hour of delivery
2500 1855 74%
Newborn dried and wrapped just after delivery
2500 1800 72%
Newborns were bathed after 72 hours
2500 1800 72%
Referral ServicesPregnant Woman Referred for ANC
85 85 100%
Pregnant Woman followed up for ANC visit after referral
66 66 100%
Woman Referred for PNC
70 70 100%
Refer Sick Neonatal 108 98 91%Children < 5 81 81 100%
41
7.2 Increased local government’s participation and ownership of MNCS programs
7.2.1 Revitalize Union Health &Family Planning Committee (UH&FPC)
With a view to promote MNCS activities and ensure the active participation of the Government and local UP representatives at union level, the existing UH&FPCs were revitalized. The number of the members vary from 17-19. The Union Health &Family Planning Committee consists of HA/FWA, Male and Female UP members, CSG members, Teachers, Karbaries, members of CC and community people. The rate of female members is 43%.The Assistant Health Inspector (AHI)/Family Planning Inspector (FPI) act as the member-secretary. As like as the CSG, the UH&FWC developed a union level plan and on the basis of the plan they develop action plans.
The members of the committee meet once a month at the Union Parishad offices and the Chairman of the respective Union Parishad preside the meeting. In the meeting various problems regarding implementation of the MNCS activities are discussed, progress is shared, the action plan are reviewed, etc.
The responsibility of the UH&FPC is to provided necessary support to the CSGs, develop union based local level plan on the basis of ward level plan, monitor the progress of CSG activities, send progress report to Upazila Development and Coordination Committee (UDCC).
7.2.2 Awareness raising workshop
The project organized 11 awareness raising workshops on Reduction of Maternal and Child Mortality: Role of Local Government, CSG Committee Members and Civil Society in Lama and Bandarban Sadar. In the workshop CSG members, headman, karbaries, female members, health and family planning staffs, UP Chairman were present. The workshop highlighted and thoroughly discussed the following topics.
7.3 Increased availability and quality of MNCS packages of care and services at health facility and community levels
7.3.1 Upazila Health Department of Bandarban Sadar
A coordination meeting with upazila health department of Bandarban Sadar was held on November 2009 at the conference room of UH&FPO office, Bandarban Sadar. The coordination meeting was arranged by MNCS Project of GRAUS & PHD. The meeting was presided by Dr. Arunjit Das, in charge UH&FPO Bandarban Sadar upazila. In the meeting Dr. Sarfaraj khan chowdhury, Civil Surgeon of Bandarban presented as chief guest while Mr. Ubaswe Chowdhury, District Program officer of UNICEF were present as special guest. In the meeting welcome speech was delivered by Mrs. Mayoiching Marma and details meeting objective was presented by Mr. Aung Chano Marma. A total number of 45 HI, AHI and HA and Supervisors of MNCS project were present in the meeting.
7.3.2 Family Planning Department of Bandarban
A coordination meeting with Upazila Family Planning Department of Bandarban Sadar was held on 4 November 2009 at the conference room of maternal and child welfare centre, Bandarban Sadar. The coordination meeting was arranged by MNCS Project of GRAUS &
42
PHD. In the meeting welcome speech was delivered by Ms. Mayoiching Marma and details meeting objective was presented by Mr. Aung Chano Marma. A total number of 46 FWI, FWV and FWA and Supervisors of MNCS project were present in the meeting.
7.3.3 Sharing Meeting with the Family Planning
Two sharing meetings, each one in Bandarban and Lama were organized with different levels of staff in Family Planning in November 2009. A total of 64 (male 29 and 35 Female) participants attended the sharing meeting. The meeting was presided by Dr. Aung Chalu MOCH of Lama. DDFP of Bandarban district was the chief guest and the special guests were Mrs. Fatema Begum, assistant Family Planning Officer and Mr. Aung Channo Marma, District Coordinator of MNCS.
In Bandarban, the sharing meeting was chaired by Mrs.Rokeya Begum, Assistant Family Planning Officer Bandarban. A total of 39 staff from different level of Family Planning office attended the meeting.
MNCS project staff participate District coordination meeting, Upazila coordination meetings, Union Health & Family Planning meetings where the staffs update the progress of the MNCSactivities
7.4 Lessons learned are documented and disseminated
7.4.1 Progress sharing meeting with PM of IMCI
A Six-monthly Progress sharing meeting was held at the civil surgeon office of Bandarban on 19 April 2009 with Program Manager of IMCI- MOHFW, Civil Surgeon of Bandarban, District Program Officer, Health Specialist of UNICEF, representatives of ICDDR,B and concerned project staffs of MNCS project staff. . Managing Director of PHD described a brief progress summary of MNCS project through power point presentation.
In December 9 2009, another progress sharing meeting was held at the civil surgeon office of Bandarban with the Program Manager of IMCI- MOHFW, Civil Surgeon of Bandarban, District Program Officer, Health Specialist of UNICEF, representatives of ICDDR,B, different government people from health and family planning department and concerned project staffs of MNCS project staff.
7.4.2 Annual Planning meetingAnnual Planning meeting of MNCS was organized in the ICDDRB with all the partners of MNCS. Representatives of IMCI, UNICEF, ICDDRB and the MNCS project staff attended the meeting. There the partners shared the yearly progress report and developed action plan for the next year.
7.4.3 Lesson Sharing workshop with Headmen and Karbaries
A workshop on ``Role and responsibilities of Headmen and Karbaries for proper implementation of MNCS Project`` was held on 17 September 2009. A total number of 27 headman and Karbaries were present in the workshop. The main purpose of the workshop was to orient the headmen and Karbaries on the MNCS project and their role in mobilizing the community, monitoring and supervision and proper implementation of MNCS.
43
7.4.4 Advocacy Workshop
The Advocacy workshop on Institutional delivery in saving the lives of mother and newborn -“Local health belief and practice” was arranged by the Health and family planning division, Bandarban, with cooperation from UNICEF on 25th August 2009.
The main aim and objective of the workshop has been to serve as a stimulus towards building awareness of the traditional leadership of the district including the Bohmong chief, political and social leaders, and the government and non-government bodies related to health care systems in the district.
7.5 Establishment of Community Support System
With a view to raise community voice towards the responsiveness of the service providers, effective coordination of services offered by different actors and connection of grassroots with the council MNCS intervention has established a Community Support System by formation of different groups.
Establishment of CSGs in the communities and their initiatives in different aspects like communication and mobilization of the community people towards health services have promoted a smooth community support system in the community. Initiative on mobilization of community people particularly the pregnant mothers, mothers of neonates, mothers of under five, etc. has increased the number of mothers with ANC and PNC check up and has boosted the level of community ownership. The system has enabled the boarder community participation in health action by providing health education, counseling, making arrangement for timely transport for urgent transfer of patients to appropriate pre-identified services centers, etc.
Inclusion of CCMG and Pahari Saystha Seva Committee of GRAUS as CSG has built a functional linkage to utilize comparative advantages of these social committees in the implementation of MNCS project.
Introducing penny bank in the CSG increased the savings tendency of the members which they use as referral cost and help the poor mothers to get modern treatment from the institutional and qualified service providers.
Through developing social maps in their concerned areas the Community Support Groups are able to identify their problems and needs. Effective contribution in designing, planning, implementation and monitoring of actions they can remove the barriers or hurdles by using different strategies and actions.
Revitalization of the UH&FPC has guaranteed the active participation of members of the local government bodies, health systems structure and the community support structures in a same platform. The effort has ensured an effective and sustainable MNCS delivery system. Effective coordination has improved responsiveness of the service providers although in a limited way.
7.6 Empowering the Local government
Involvement of Local Government in the system is very important for sustainable improvement of welfare and development services including MNCS services. To intervene the MNCS activities without any interruption, an effort has been undertaken to build lineages among the local government bodies, health systems structure and the community support structures by including them as members of different committees. Different capacity building initiatives like
44
training to elected UP representatives, orientations, discussions meetings with local level health coordination committees, have increased the knowledge on the health situation in the local areas, different aspect of the MNCS activities. As a member of Union Health and Family Planning Committees the members provide supportive supervision to community support system and union health system and has helped to build a bridge between them and thus taking active part in the implementation MNCS package.
8. Some Activities
Orientation on MNCS
After recruitment of the staff, an orientation on MNCS intervention was organized for the project staffs. All staffs of MNCS project attended in the orientation session. During orientation session the following issues of MNCS project were discussed:
· Project goal · Objectives· Implementation strategy· Approach· Project indicator, targets and services.· MNCS project implementation framework
Conduct Rapid Assessment
With a view to assess the existing situation of the service proving organizations and the community situation 33 (old Ward based) assessments were conducted. Before conduction the assessment training on the format was provided by the ICDDB. The format contained number of villages, characteristics of areas and population, Ngo ‘s activities in the areas, existence of service providing organizations like, nutrition centers, NGO clinics, satellite clinics, ward and UP offices, etc.
Consultative Meeting
99 consultative meetings were conducted in 99 Wards of two Upazilas with various stakeholders. The main purpose of the meetings was to disseminate information of MNCS interventions. It was considered as base to form Community Support Groups (CSGs).
Conduction of KABPA
KABPA is a tool to assess the knowledge, attitude, behavior and practice of the community people on health situation. With a view to assess the different health related situation, practices and types of health services providers, different techniques like FGDs, interviews, Key Informant Interviews, Problem ranking, Venn diagram were used with pregnant mothers, mothers of new born-baby, mothers of children under 1-5 age groups, etc.
Under this process 297 FGDs, 100 interviews, 55 KIIs were conducted in 99 wards. On the basis of the assessment, each UF along with CM developed 99 ward based assessment report on KABPA.

45
Conduct Household Assessment
Training on the household registration was provided to the staff of the MNCS by ICDDRB. The household registration format includes information on: number of children of 0-28 days, number of children of 29 days-5 years, number of couples with reproductive age, number of pregnant mothers, number of mothers with new born babies, number of households with safe latrines, number of households with tube well, etc. After filled up the format, information was compiled by ICDDRB.
Introduction of MIS Surveillance Registrar
HH register system was introduced to keep HH records on which monthly surveillance system started. It helps to see monthly progress of the MNCS services.
School quiz competition
MNCS arranged school quiz competition for students (class eight- new 10) of MNCS intervening areas. 500 students of 10 schools of Bandarban and Lama upazila participated in the competition. The objectives of the competition were to raise awareness of the adolescent boys and girls on personal hygiene, reproductive health care, immunization and new born & child health care. The winners were appraised by providing gift. Government personals from the health and family planning department in Bandraban and Lama launched the competition program.
School Debate Competition on Reproductive Health
Another debate competition was organized with the students of eight schools of Bandarban and Lama. Students of Lama Adarsha girls’ high school, Gajalia high school Lama govt. high schoo and Lama Mukh high school under Lama Upazila and Raichha High school, Mro Abashika High school, Chemi Dolupara High school and Rajbila high school of Bandarban participated in School debate competition. The objectives of the competition were to raise awareness to adolescent boys and girls on reproductive health care, maternal & neonatal health care etc.
Slide Show
MNCS project along with the technical support of District and upazila information office of Bandarban and Lama upazila organized 22 video shows in 11 unions of two Upazilas. The show titled `` Hasibanur Kotha’’ was displayed at the union level. The objectives of the programs were to raise awareness of pregnant women, adolescent boys and girls on personal hygiene, reproductive health care, immunization and new born & child healthcare.
Exposure Visit
An exposure visit for the staff of MNCS was organized in September 2009. Lama Upzilla Manager along with 2 Union Facilitators and 3 Community Mobilizers visited Sylhet to get an idea on the ACCESS program of Save the Children USA. The participants visited four project
46
areas of ACCESS like Bariul, Amura, Kholapar and Kola villages under Gopalgong Upazilas of Sylhet. They were oriented on the activities of Maternal and Neonatal Health, Counseling sessions, Field Registrations, Mobilizations process etc. After coming back from the visit the participants prepared a report and submitted to District Coordinator of MNCS.
The second exposure visit of the staff of MNCS was organized on 6-7 April 2010. Upzilla Manager of Rowangchari and Bandarban Sadar along with 2 Union Facilitators and 4Community Mobilizers visited MNH intervention areas of Moulavibazar, Sylhet to get an idea on Community Support System (ComSS). The participants visited 3 Community clinic locations at Shonkarsena Community clinic, Sayed nagar community clinic and Uttarsur community clinic at Moulavibazar, Sylhet. The MNH project has been implementing by Sylhet Juba Academy and Unnayon Sahayok Songstha (USS) with technical supported of PHD.
9. GO-NGO Coordination
EPI
MNCS staff participate monthly EPI meetings and provides support to routine EPI sessions, NIDs and in observation of national and international health days and events . The aim of EPI is to reduce the child mortality and morbidity among the people living in hard to reach areas. All the Union Facilitators, Community Mobilizers and Health Promoters of MNCS engage themselves with the government staff in their concerned areas to make the programme successful and increase the coverage of the hard core poor in hard to reach areas. 3570
17th and 18th NIDTo make the program successful and to increase the immunization coverage in the hard to reach areas, the project staff of MNCS were involved in motivational works and attended in the 17th NID (1st round) and 18th NID.
National vitamin A plus campaign
MNCS provided support to implement the National vitamin A plus campaign in Bandarban. The national vitamin A plus campaign-2010 was held on 29 May 2010 with a view to preventing childhood blindness, reducing child mortality and strengthening immunity. The slogan for the national vitamin A plus campaign-2010 was ‘supplement vitamin A capsule for better survival of your child.’
National Safe Motherhood Day-2010
MNCS project observed safe motherhood day on 30 May 2010 in joint collaboration with Health and family planning department of Bandarban. A discussion meeting on Safe mother hood was held at Civil surgeon office of Bandarban. The discussion meeting was presided over by Mr. Mojibor Rahman, Convenor, Health standing committee of Hill District Council, Bandarban. Mr. Nurul Afsar, ADC (revenue) of Bandarban was the chief guest of the meeting.
Project staff participate monthly EPI meetings and provides support to routine EPI sessions, NIDs and in day observation of national and international health days and events
47
HP/CMs share and validate their report with HA/ FWA/ FWV in monthly CSG meeting
Day Observation
World Health Day 2009
MNCS in Joint collaboration with Hill District Council, Health and Family planning department, UNDP and World Vision-ADP observed world health day at the Conference room of Sadar Hospital, Bandarban on 7th April 2009. The World health day was observed with a theme on Save lives: Make Hospitals Safe in Emergencies. The meeting was presided by convener (health) of Hill District Council, Bandarban. In the meeting Honorable Chairman of Hill District Council was the chief guest. District Coordinator of UNDP of Bandarban, Deputy Director of Family Planning and District coordinator of MNCS Project, were attended as special guest respectively. In the meeting Key note paper was presented by District Medical Officer (Health) of UNDP, Bandarban.
World Health Day 2010
MNCS in Joint collaboration with Hill district council, Health and Family Planning Department, Save the Children, UK, UNDP and BNKS observed the World Health Day at the Conference room of Sadar Hospital, Bandarban on 7th April 2010. The World Health Day was observed with the theme of Urbanization: a challenge for public health. The discussion was on health challenges related to water, environment, violence and injury, non-communicable diseases (NCDs) and their risk factors like tobacco use, unhealthy diets, physical inactivity and harmful use of alcohol as well as the risks associated with disease outbreaks. It included that the sufferings of urban poor is related with increased risk of violence, chronic disease, and for some communicable diseases such as tuberculosis and HIV/AIDS.
World Hand Washing Day
15 December, 2009 was observed as world Hand Wash day in the project areas of Bandarban district. A total of 1500 students of 11 schools under 11 unions of Bandarban and lama Upazila observed the day with the help of MNCS project staff. Regarding this 321 soaps were distributed to them.
10. Monitoring and Reporting
The MNCS interventions are monitored at two levels-- at the community and organizational level. At the community level, the members of CSG develop action plan to implement and monitor their own work. In the monthly meeting, the CSG members monitor their work as per their monitoring matrix prepared based on their action plan. Each Health promoter is responsible to report the performance of each CSG in their monthly meeting. On the other hand, the UH&FP provide support to CSGs, monitor the work of the CSG’s and review the performance of the union at different levels.
At the MNCS intervention level, there are upzailla based MIS officers who are responsible to monitor the project activities. The Monitoring and Training Officer (MTO) and Upazila (MIS) conduct monitoring at the implementation level with CSGs and UH&FPC and submit monitoring report to the MDO. For smooth monitoring of the project activities, a Monitoring & Reporting Guidelines with necessary Tools & Formats were also developed by ICDDRB and PHD and these have been practicing in the field. Some case studies on health care practices

48
are conducted in the MNCS intervention areas for reviewing results and impact of the intervention.
PHD conducts the progress monitoring in every month by project team through a coordination meeting and system of ‘Experiential Learning”. .
At the beginning of each quarter, a planning Meeting was organized at PHD with the DC, MTO, UM, UF to review the performance & achievement of the project as well as to develop the next quarter Plan. All the findings and recommendations of the different field visit reports, case studies, observation and field level activities are considered and incorporated in the planning system.
Progress monitoring
Process of citizen monitoring has started. Under this process, the CM/HP present and submit their work plan to the CSG members in their monthly meetings.
According to the work plan of HPs and CMs, the CSG members monitor their activities like courtyard meetings, counseling sessions on their concerned areas.
Monthly surveillance system was developed by ICDDR-B’s to see the monthly service progress. With a view to introduce the system orientation was provided by ICDDRB to the MNCS staffs
PHD/GRAUS developed and supplied a family card to families having pregnant and women having children under 0-5 years for monitoring day-to-day pregnancy observation and newborn cares.
Supervision and Monitoring Matrix was developed through a workshop with representation from all level of MNCS staff and introduced in the field. The matrix is practiced in the field. On the basis of information a report is developed.
Go-NGO Monitoring
On 7th January 2010 a high profile team of Health department, headed by Dr. Sarfaraj Khan Chowdhury, Civil Surgeon of Bandarban visited community support group ( CSG) visited a CSG of hard to reach areas at Monjoy Para of Rajbila union of Bandarban. Dr. Farhad Uddin, UH&FPO Bandarban Sadar, Dr.Aurunjit, MO of UH&FPO office Bandarban Sadar, Mr. Chaing Seing Moung, Executive director of GRAUS and Aung Chano Marma,District coordinator of MNCS project were in the team.
On 27 April 2010 a monitoring visit was organized. Md. Firojur Rahman, Upazila Health and Family Planning Officer (UH&FPO) of Lama upazila visited one CSG at Sapzhiri Para of Gajalia union and one counseling session at Line zhiri of Lama Sadar union. Nutan Bikash Chakma, Upazila manager of MNCS Project was in the team.
On 17 May 2010 a team of health department of Bandarban visited counseling session in Liame para under Bandarban sada Union. Mr. Mahbub Rahman, Upazila cooperative officer and Mr. Chawhaimong Marma, upazila manager of MNCS project, Bandarban was in the team. The team talked with CSG members and local peoples on different benefits they received from MNCS activities. He emphasized to provide training on Malaria, diarrhea, pneumonia and primary health care to the community people.
49
11. Some Important Visits
· A team of UNICEF accompanied by Mr. Louis Georges Arsenault, Country Representative UNICEF, Bangladesh visited Counseling Session conducted by the MNCS project staffs at Amtoli Taunchongya para of Shoalok union, Bandarban. District Program Officer of Unicef Bandarban, District Coordinator of ICDP project of CHTDB, Medical Officer of Civil Surgeon Office, UFPO of Bandarban Sadar, Managing Director of PHD and Executive Director of GRAUS.
· On 4 May 2009, GoB-AusAID-UNICEF jointly visited a Pahari Shyastya Seba Clinic run by MNCS project at Manjoy para, Rajbila union of Bandarban Sadar. The team headed by Ms. Zabeta Elizabeth Moutafis, First secretary of Australian High commission in Dhaka. Other honorable team members were: Dr. Birthe Locatelli-Rossi, Chief- Health & Nutrition section, Dr. Mosaddeque Ahmed, Program manager, IMCI, MOHFW,Dhaka, Ms. Jenny Finch Senior Program officer, Aus AIDDr. Shehlina Ahmed, Health specialist, Unicef, .Dr. Ziaul Matin, health Officer, UniCEfDr.U-Ba Swee, Pogram Officer of UNICEF, Dr. Abdul Mannan, Civil surgeon Bandarban,, r. U Khey Win, Deputy Director –Family planning Bandarban., Md. Abdus Salam, Managing Director,
· On 24th August 2009 Mrs. Midori Sato, Health Manager, Health and Nutrition Section of Unicef-Bangladesh, visited MNCS areas-- Jogesh karbary para of Rajbila Union and Pora Para of Shoalok Union. Dr Mohsin Ali, Nutrition Specialist of Unicef-Bangladesh, Dr. Ubaswe Chowdhury, Program Officer of Unicef-Bandarban and District Coordinator of ICDP were in the team. She also attended A lobbying and Advocacy Workshop, organized by the health and Family Planning Division of Bandarban and Hill District Parishad.
· Ms. Patricia C4D Specialist, and Ms. Tania Sultana, Program Communication Specialist from the Unicef-Bangladesh were present in PRA training organized by MNCS. They visited Tonchonga para of Soalok Union,. a MNCS implementation area and discussed with CSG members on Social Mapping process, CSG Action plan, CSG Savings and its utilization. They also talked with a mother & child who referred through project staff and CSG members.
· Dr. Mosaddeqe Ahmed, Program Manager of IMCI of DGHS, Dr. Altaf Hossain DPM of IMCI of DGHS, Dr. Ziaul Motin, Health Officer Health & Nutrition Section, UNICEF Bangladesh observed a training on Surveillance Registrar provided by ICDDRB.
· Dr. Dr Shamina Sharmin, Health Officer (IMCI) of Health and Nutrition Section along with Ms. Tania Sultana, Program Communication Specialist and Dr. Ubasee Chowdhury, Program Officer of UNICEF-Bangladesh visited Talunia Para and FWC Fytung Para of of Aziznagar Union of Lama Upazila.
· Mr. Takoa Toda, Chief Representative of jica and Ms. Saeda MAKIMOTO, Representative (Health, Governance) visited one of the CSG, Amtoli of Soalok union under Bandarban Sadar Upazila. During the visit, they discussed different issues with the CSG members.
12. Lesson Learned
50
· Process of establishing strong coordination mechanism at the Union level between MNCS and the Health and Family Planning systems has started but it needs to be strengthened.
· Limited facilities including supply of drugs and apparatus of the PSSCs interrupt the MNCS to provide health services to the community people in heard to reach areas.
· Along with the MNCS staff, CSG members also work as focal point for mobilizing the community people to increase their health seeking behaviour and to receive quality health services from different health service providing organizations. To carry out these activities the performances of the CSG members should be enriched by providing training on the modern techniques of mobilization and communication.
· Improved results can be achieved if spiritually driven beliefs and practices can be matched with practical demands. The story: Almost all mothers throw first milk (colostrums) into river (a common practice) with a view that the satisfied God will return this like flow of a river. The UNICEF Country Representative during his visit to Bandarban advised us ‘let them through one-drop’ and rest to the baby. Implementation of this advice clicks
· MNCS intervention need to be equipped to provide services in remote places in addition to mobilisation
· Half-way home could be an alternative to bring remote risk pregnant to nearest delivery centre and, or develop a complete referral package
· Training to the Headmen and Karbaries/CSG members on monitoring the MNCS activities may be beneficial for the sustainable involvement in health programme implementation as the social-cultural administration of Bandarban is governed by the territorial Headman and Karbaris
13 Challenges
· Intensive monitoring of the MNCS activities in the hard to reach areas is a great challenge.
· It is challenge to work in the areas where health care practices and hospitalization are deeply associated with spiritually driven deep-rooted beliefs and superstitions.
· Providing services during Jhum shifting cultivation becomes difficult due to the shifting of pregnant women from their homes to fields.
· The main challenge of the MNCS is to provide health services to people lives in hard-to-reach areas (top of hills, deep forest) due to worse road communication. It becomes difficult for the service providers to carry logistics.
· Grassroots service centers are not adequately equipped to provide MNCS services, thus adversely affecting the mobilization process;
· Pahari Saystha Seva Kendras- the only facilities in remote villages can not provide services without drugs

51
· Only possibility to provide MNCS services to Mro communities who lives top of the hills in organizing satellite clinics but it is not possible without medicine support
· Frequent drop out of health promoters interrupt the implementation of MNCS activities.
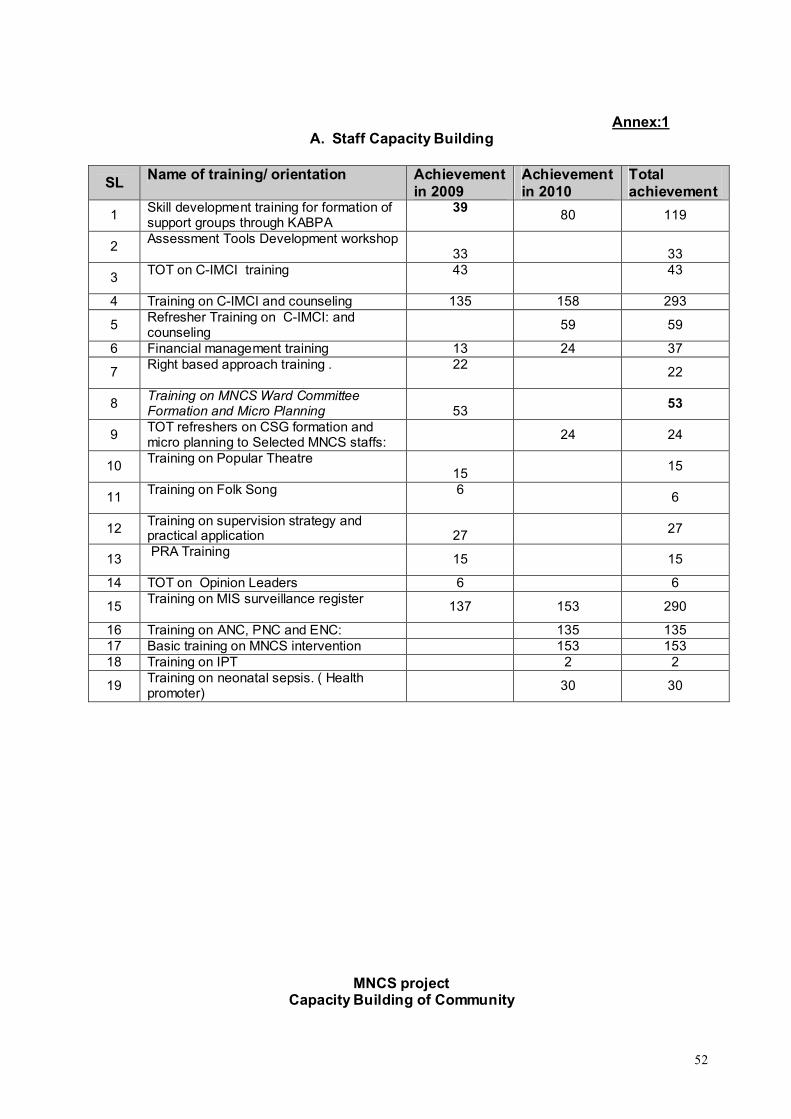
52
Annex:1A. Staff Capacity Building
SLName of training/ orientation Achievement
in 2009Achievement in 2010
Total achievement
1Skill development training for formation of support groups through KABPA
3980 119
2Assessment Tools Development workshop
33 33
3TOT on C-IMCI training 43 43
4 Training on C-IMCI and counseling 135 158 293
5Refresher Training on C-IMCI: and counseling
59 59
6 Financial management training 13 24 37
7Right based approach training . 22
22
8Training on MNCS Ward Committee Formation and Micro Planning 53
53
9TOT refreshers on CSG formation and micro planning to Selected MNCS staffs:
24 24
10Training on Popular Theatre
1515
11Training on Folk Song 6
6
12Training on supervision strategy and practical application 27 27
13 PRA Training
15 15
14 TOT on Opinion Leaders 6 6
15Training on MIS surveillance register
137 153 290
16 Training on ANC, PNC and ENC: 135 13517 Basic training on MNCS intervention 153 15318 Training on IPT 2 2
19Training on neonatal sepsis. ( Health promoter)
30 30
MNCS projectCapacity Building of Community
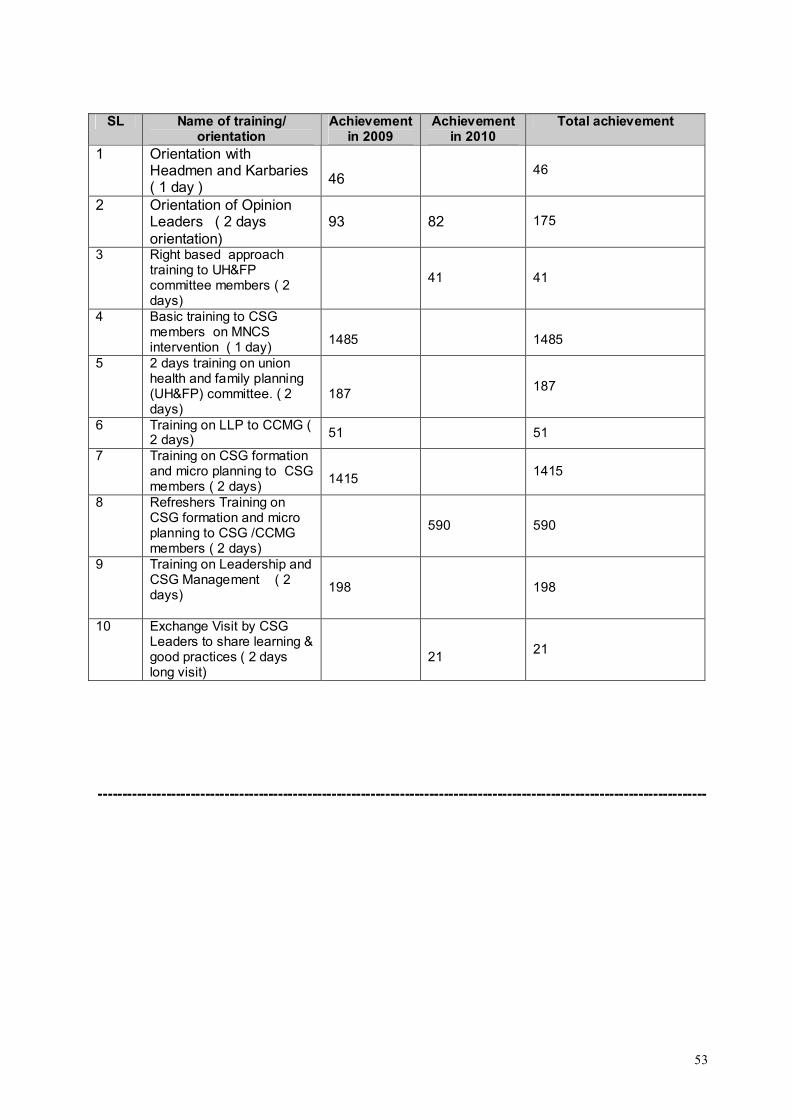
53
SL Name of training/ orientation
Achievement in 2009
Achievement in 2010
Total achievement
1 Orientation with Headmen and Karbaries ( 1 day )
4646
2 Orientation of Opinion Leaders ( 2 days orientation)
93 82 175
3 Right based approach training to UH&FP committee members ( 2 days)
41 41
4 Basic training to CSG members on MNCS intervention ( 1 day)
1485 1485
5 2 days training on union health and family planning (UH&FP) committee. ( 2 days)
187187
6 Training on LLP to CCMG ( 2 days) 51 51
7 Training on CSG formation and micro planning to CSG members ( 2 days)
14151415
8 Refreshers Training on CSG formation and micro planning to CSG /CCMG members ( 2 days)
590 590
9 Training on Leadership and CSG Management ( 2 days)
198 198
10 Exchange Visit by CSG Leaders to share learning & good practices ( 2 days long visit)
2121
-----------------------------------------------------------------------------------------------------------------------------
54
Annual Report Of
Community Based Integrated Maternal, Neonatal and Child Survival (MNCS) Intervention for Expansion Areas of Bandarban
(Rowangchhari, Ruma, Thanchi and Alikadam)
PPeerriioodd:: JJaannuuaarryy 22001100 –– MMaarrcchh 22001111
SSuubbmmiitttteedd TToo:: UUNNIICCEEFF BBaannggllaaddeesshh BBSSLL OOffffiiccee CCoommpplleexx,, 11 MMiinnttoo RRooaadd,, DDhhaakkaa 11000000,, BBaannggllaaddeesshh
Submitted By:
Partners in Health and Development (PHD)House No: SWD 12ARoad 8, Gulshan 1Dhaka---1212Bangladesh
IImmpplleemmeenntteedd bbyy::
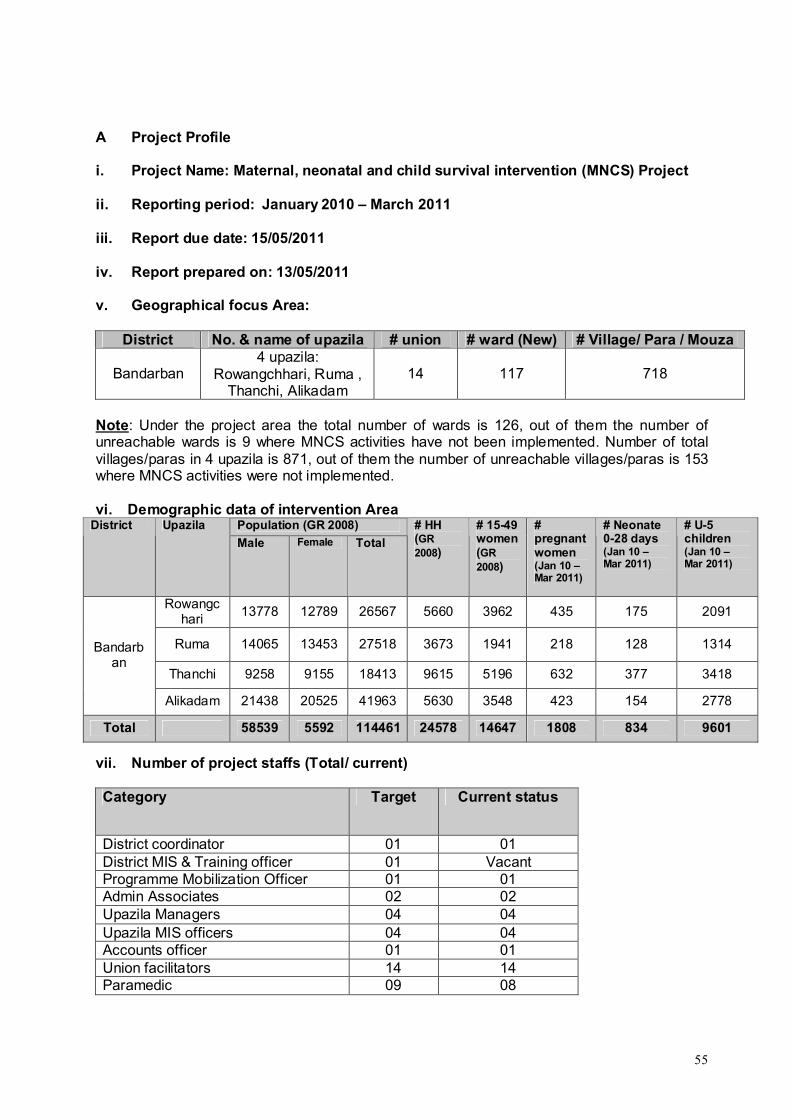
55
A Project Profile
i. Project Name: Maternal, neonatal and child survival intervention (MNCS) Project
ii. Reporting period: January 2010 – March 2011
iii. Report due date: 15/05/2011
iv. Report prepared on: 13/05/2011
v. Geographical focus Area:
District No. & name of upazila # union # ward (New) # Village/ Para / Mouza
Bandarban4 upazila:
Rowangchhari, Ruma , Thanchi, Alikadam
14 117 718
Note: Under the project area the total number of wards is 126, out of them the number of unreachable wards is 9 where MNCS activities have not been implemented. Number of total villages/paras in 4 upazila is 871, out of them the number of unreachable villages/paras is 153 where MNCS activities were not implemented.
vi. Demographic data of intervention Area Population (GR 2008)District Upazila
Male Female Total
# HH(GR 2008)
# 15-49 women(GR 2008)
# pregnant women(Jan 10 –Mar 2011)
# Neonate 0-28 days (Jan 10 –Mar 2011)
# U-5 children(Jan 10 –Mar 2011)
Rowangchari
13778 12789 26567 5660 3962 435 175 2091
Ruma 14065 13453 27518 3673 1941 218 128 1314
Thanchi 9258 9155 18413 9615 5196 632 377 3418
Bandarban
Alikadam 21438 20525 41963 5630 3548 423 154 2778
Total 58539 5592 114461 24578 14647 1808 834 9601
vii. Number of project staffs (Total/ current)
Category Target Current status
District coordinator 01 01District MIS & Training officer 01 VacantProgramme Mobilization Officer 01 01Admin Associates 02 02Upazila Managers 04 04Upazila MIS officers 04 04Accounts officer 01 01Union facilitators 14 14Paramedic 09 08

56
CommunityMobilizer
68 68
Health promoter 116 116Depot holders 52 52
A. Main progress report:
i. Executive summary:
PHD (Partners in Health and Development) along with GRAUS have been implementing the
MNCS (Maternal, Neonatal and Child Survival) intervention of UNICEF in 14 unions of
Rowangchhari, Ruma, Thanchi and Alikadam Upazilas under Bandarban district.
The main objective of the project is to improve the home health care practices and increased
care seeking behaviour of communities and utilization of neonatal, child health and nutrition
services by families, particularly poor and excluded communities, who live in those four
upazilas under Bandarban District.
This Annual report demonstrates the activities performed during the period of January 2010 to March 2011. To assess the effectiveness of the MNCS intervention in the implemented areas of four Upazilas, an MIS system was introduced by ICDDRB in August 2011. This MIS provides information on number of mothers with ANC and PNC check-up, neonates with thermal care up, delayed bath, early and exclusive breast feeding, <5 Children with proper care, etc. Cumulative achievements of MNCS Intervention as per MNCS MIS System are as follows;
During the period, 1808 pregnant women were identified in these 4 Upazilas. Out of targeted women 33% mothers received at least one ANC and only 17% women at least three ANC. During this period, out of 728 mothers who delivered child (still -15 and live birth -713), the total number of neonates is 713 where 40% received immediate thermal care. The rate of birth attended by trained birth attendants is 25%. 42% newborns received delayed bath and 67% newborn initiated breastfeeding within 1 hour.
Under capacity building initiatives, some ToT and Training were to different types of staff at different level. These were: Basic Training on MNCS Intervention (204), ToT on micro planning(98), Training on MNCSWC formation (98), Training on opinion leaders (226), Training on ANC (268), Training on PNC and ENC (268). Training on C-IMCI counseling (268) Different levels of community people were oriented on: Micro planning to members of UHFWC (1309), Training to Traditional Birth attendants (24), Training on MNCS issues to Adolescents (115), PRA to GBA staff (52), Interactive Popular Theater (54), Training to UP secretariat (21).
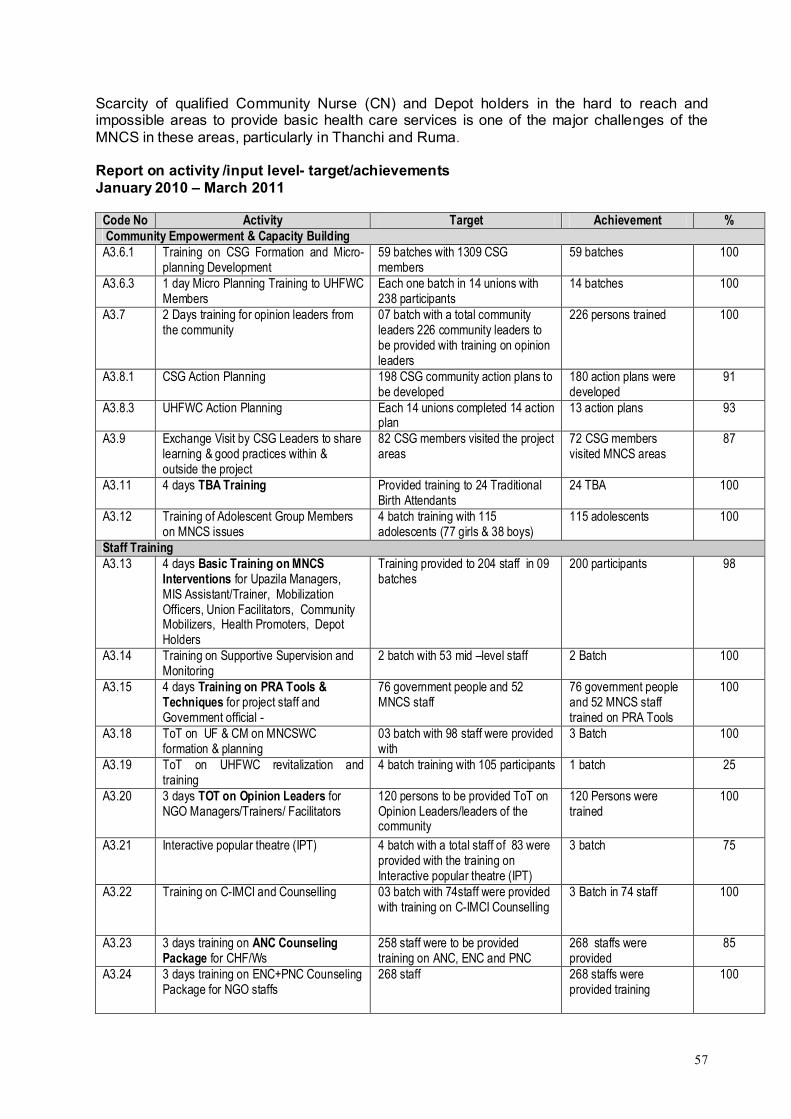
57
Scarcity of qualified Community Nurse (CN) and Depot holders in the hard to reach and impossible areas to provide basic health care services is one of the major challenges of the MNCS in these areas, particularly in Thanchi and Ruma.
Report on activity /input level- target/achievements January 2010 – March 2011
Code No Activity Target Achievement % Community Empowerment & Capacity Building A3.6.1 Training on CSG Formation and Micro-
planning Development59 batches with 1309 CSG members
59 batches 100
A3.6.3 1 day Micro Planning Training to UHFWC Members
Each one batch in 14 unions with 238 participants
14 batches 100
A3.7 2 Days training for opinion leaders from the community
07 batch with a total community leaders 226 community leaders to be provided with training on opinion leaders
226 persons trained 100
A3.8.1 CSG Action Planning 198 CSG community action plans to be developed
180 action plans were developed
91
A3.8.3 UHFWC Action Planning Each 14 unions completed 14 action plan
13 action plans 93
A3.9 Exchange Visit by CSG Leaders to share learning & good practices within & outside the project
82 CSG members visited the project areas
72 CSG members visited MNCS areas
87
A3.11 4 days TBA Training Provided training to 24 Traditional Birth Attendants
24 TBA 100
A3.12 Training of Adolescent Group Members on MNCS issues
4 batch training with 115 adolescents (77 girls & 38 boys)
115 adolescents 100
Staff Training A3.13 4 days Basic Training on MNCS
Interventions for Upazila Managers, MIS Assistant/Trainer, Mobilization Officers, Union Facilitators, Community Mobilizers, Health Promoters, Depot Holders
Training provided to 204 staff in 09 batches
200 participants 98
A3.14 Training on Supportive Supervision and Monitoring
2 batch with 53 mid –level staff 2 Batch 100
A3.15 4 days Training on PRA Tools & Techniques for project staff and Government official -
76 government people and 52 MNCS staff
76 government people and 52 MNCS staff trained on PRA Tools
100
A3.18 ToT on UF & CM on MNCSWC formation & planning
03 batch with 98 staff were provided with
3 Batch 100
A3.19 ToT on UHFWC revitalization and training
4 batch training with 105 participants 1 batch 25
A3.20 3 days TOT on Opinion Leaders for NGO Managers/Trainers/ Facilitators
120 persons to be provided ToT on Opinion Leaders/leaders of the community
120 Persons were trained
100
A3.21 Interactive popular theatre (IPT) 4 batch with a total staff of 83 were provided with the training on Interactive popular theatre (IPT)
3 batch 75
A3.22 Training on C-IMCI and Counselling 03 batch with 74staff were provided with training on C-IMCI Counselling
3 Batch in 74 staff 100
A3.23 3 days training on ANC Counseling Package for CHF/Ws
258 staff were to be provided training on ANC, ENC and PNC
268 staffs were provided
85
A3.24 3 days training on ENC+PNC Counseling Package for NGO staffs
268 staff 268 staffs were provided training
100
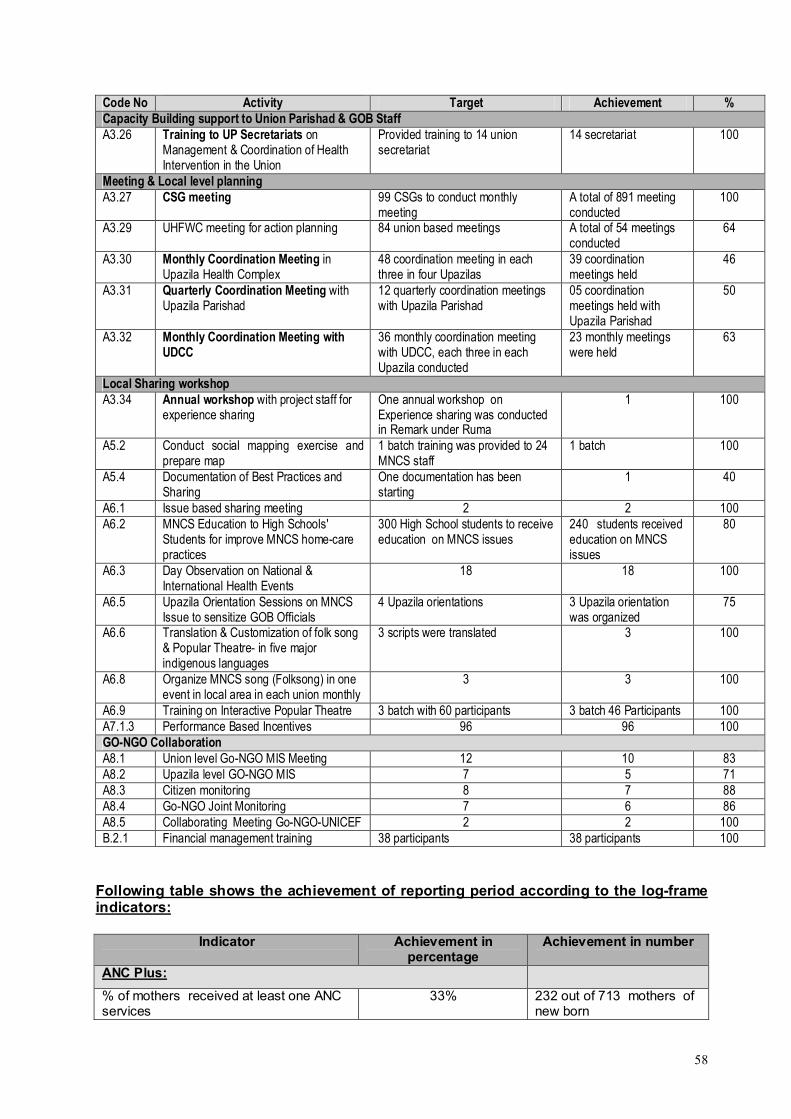
58
Code No Activity Target Achievement %Capacity Building support to Union Parishad & GOB StaffA3.26 Training to UP Secretariats on
Management & Coordination of Health Intervention in the Union
Provided training to 14 union secretariat
14 secretariat 100
Meeting & Local level planningA3.27 CSG meeting 99 CSGs to conduct monthly
meeting A total of 891 meeting conducted
100
A3.29 UHFWC meeting for action planning 84 union based meetings A total of 54 meetings conducted
64
A3.30 Monthly Coordination Meeting in Upazila Health Complex
48 coordination meeting in each three in four Upazilas
39 coordination meetings held
46
A3.31 Quarterly Coordination Meeting with Upazila Parishad
12 quarterly coordination meetings with Upazila Parishad
05 coordination meetings held with Upazila Parishad
50
A3.32 Monthly Coordination Meeting with UDCC
36 monthly coordination meeting with UDCC, each three in each Upazila conducted
23 monthly meetings were held
63
Local Sharing workshopA3.34 Annual workshop with project staff for
experience sharing One annual workshop on Experience sharing was conducted in Remark under Ruma
1 100
A5.2 Conduct social mapping exercise and prepare map
1 batch training was provided to 24 MNCS staff
1 batch 100
A5.4 Documentation of Best Practices and Sharing
One documentation has been starting
1 40
A6.1 Issue based sharing meeting 2 2 100A6.2 MNCS Education to High Schools'
Students for improve MNCS home-care practices
300 High School students to receive education on MNCS issues
240 students received education on MNCS issues
80
A6.3 Day Observation on National & International Health Events
18 18 100
A6.5 Upazila Orientation Sessions on MNCS Issue to sensitize GOB Officials
4 Upazila orientations 3 Upazila orientationwas organized
75
A6.6 Translation & Customization of folk song & Popular Theatre- in five major indigenous languages
3 scripts were translated 3 100
A6.8 Organize MNCS song (Folksong) in one event in local area in each union monthly
3 3 100
A6.9 Training on Interactive Popular Theatre 3 batch with 60 participants 3 batch 46 Participants 100A7.1.3 Performance Based Incentives 96 96 100GO-NGO CollaborationA8.1 Union level Go-NGO MIS Meeting 12 10 83A8.2 Upazila level GO-NGO MIS 7 5 71A8.3 Citizen monitoring 8 7 88A8.4 Go-NGO Joint Monitoring 7 6 86A8.5 Collaborating Meeting Go-NGO-UNICEF 2 2 100B.2.1 Financial management training 38 participants 38 participants 100
Following table shows the achievement of reporting period according to the log-frame indicators:
Indicator Achievement in percentage
Achievement in number
ANC Plus:
% of mothers received at least one ANC services
33% 232 out of 713 mothers of new born
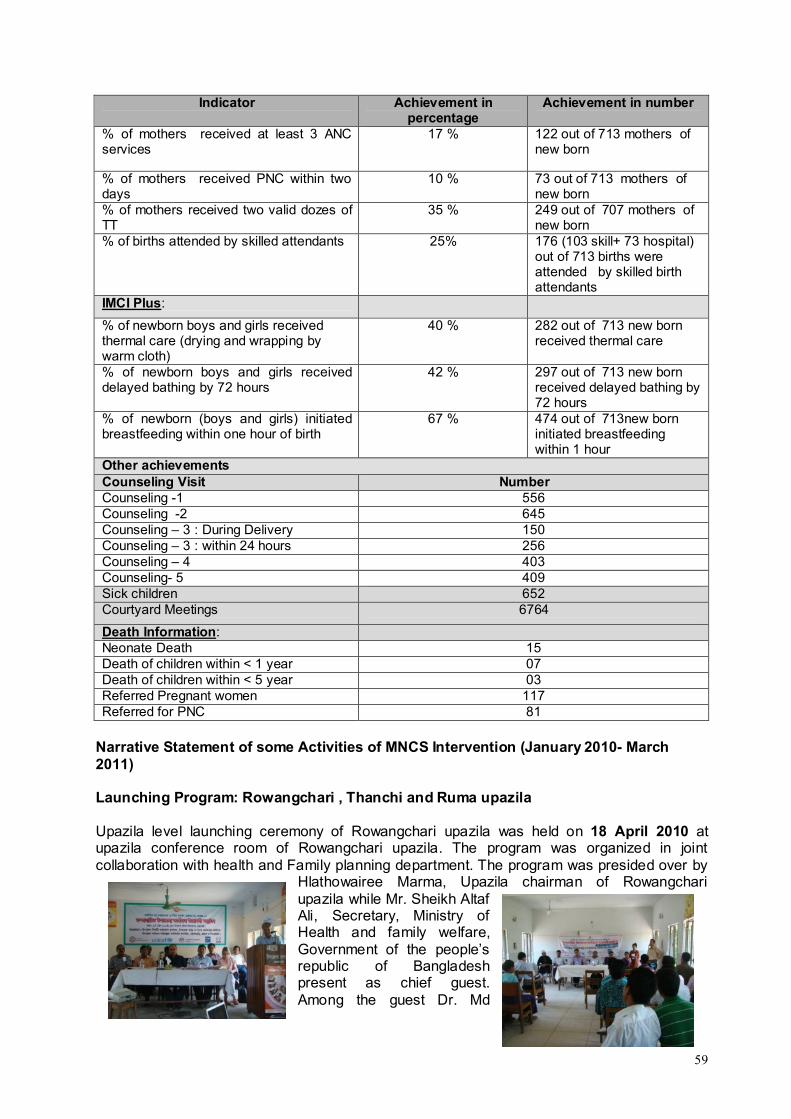
59
Indicator Achievement in percentage
Achievement in number
% of mothers received at least 3 ANC services
17 % 122 out of 713 mothers of new born
% of mothers received PNC within two days
10 % 73 out of 713 mothers of new born
% of mothers received two valid dozes of TT
35 % 249 out of 707 mothers of new born
% of births attended by skilled attendants 25% 176 (103 skill+ 73 hospital) out of 713 births were attended by skilled birth attendants
IMCI Plus:
% of newborn boys and girls received thermal care (drying and wrapping by warm cloth)
40 % 282 out of 713 new born received thermal care
% of newborn boys and girls received delayed bathing by 72 hours
42 % 297 out of 713 new born received delayed bathing by 72 hours
% of newborn (boys and girls) initiated breastfeeding within one hour of birth
67 % 474 out of 713new born initiated breastfeeding within 1 hour
Other achievements Counseling Visit NumberCounseling -1 556Counseling -2 645Counseling – 3 : During Delivery 150Counseling – 3 : within 24 hours 256Counseling – 4 403Counseling- 5 409Sick children 652Courtyard Meetings 6764
Death Information:Neonate Death 15Death of children within < 1 year 07Death of children within < 5 year 03Referred Pregnant women 117Referred for PNC 81
Narrative Statement of some Activities of MNCS Intervention (January 2010- March 2011)
Launching Program: Rowangchari , Thanchi and Ruma upazila
Upazila level launching ceremony of Rowangchari upazila was held on 18 April 2010 at upazila conference room of Rowangchari upazila. The program was organized in joint collaboration with health and Family planning department. The program was presided over by
Hlathowairee Marma, Upazila chairman of Rowangchari upazila while Mr. Sheikh Altaf Ali, Secretary, Ministry of Health and family welfare, Government of the people’s republic of Bangladesh present as chief guest. Among the guest Dr. Md
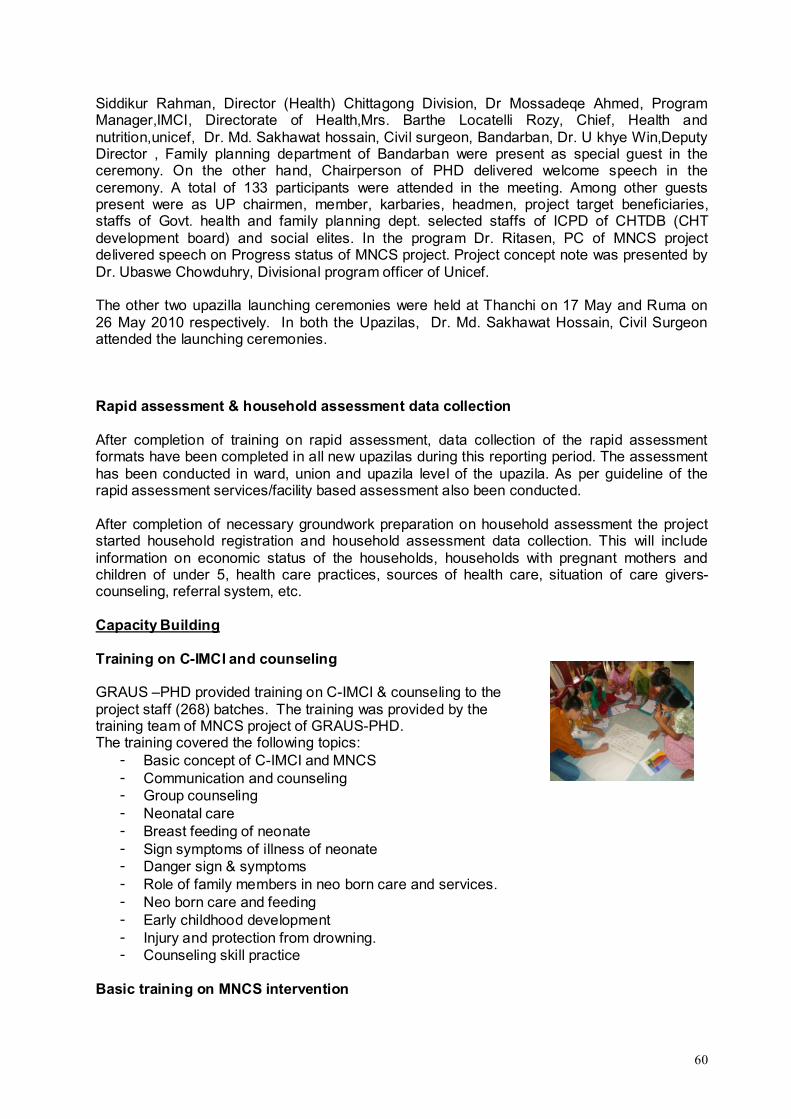
60
Siddikur Rahman, Director (Health) Chittagong Division, Dr Mossadeqe Ahmed, Program Manager,IMCI, Directorate of Health,Mrs. Barthe Locatelli Rozy, Chief, Health and nutrition,unicef, Dr. Md. Sakhawat hossain, Civil surgeon, Bandarban, Dr. U khye Win,Deputy Director , Family planning department of Bandarban were present as special guest in the ceremony. On the other hand, Chairperson of PHD delivered welcome speech in the ceremony. A total of 133 participants were attended in the meeting. Among other guests present were as UP chairmen, member, karbaries, headmen, project target beneficiaries, staffs of Govt. health and family planning dept. selected staffs of ICPD of CHTDB (CHT development board) and social elites. In the program Dr. Ritasen, PC of MNCS project delivered speech on Progress status of MNCS project. Project concept note was presented by Dr. Ubaswe Chowduhry, Divisional program officer of Unicef.
The other two upazilla launching ceremonies were held at Thanchi on 17 May and Ruma on 26 May 2010 respectively. In both the Upazilas, Dr. Md. Sakhawat Hossain, Civil Surgeon attended the launching ceremonies.
Rapid assessment & household assessment data collection
After completion of training on rapid assessment, data collection of the rapid assessment formats have been completed in all new upazilas during this reporting period. The assessment has been conducted in ward, union and upazila level of the upazila. As per guideline of the rapid assessment services/facility based assessment also been conducted.
After completion of necessary groundwork preparation on household assessment the project started household registration and household assessment data collection. This will include information on economic status of the households, households with pregnant mothers and children of under 5, health care practices, sources of health care, situation of care givers-counseling, referral system, etc.
Capacity Building
Training on C-IMCI and counseling
GRAUS –PHD provided training on C-IMCI & counseling to the project staff (268) batches. The training was provided by the training team of MNCS project of GRAUS-PHD.The training covered the following topics:
- Basic concept of C-IMCI and MNCS - Communication and counseling- Group counseling- Neonatal care- Breast feeding of neonate- Sign symptoms of illness of neonate- Danger sign & symptoms- Role of family members in neo born care and services.- Neo born care and feeding- Early childhood development- Injury and protection from drowning.- Counseling skill practice
Basic training on MNCS intervention
61
A basic training on MNCS was provided to 204 staff in 8 batches. District core training team of MNCS project facilitated the orientation. During training, the participants were oriented in details about MNCS project interventions such as: Project goal, objectives, basic concept of C-IMCI and MNCS , MDG target and perspective of Bangladesh, implementation strategy, project Approach,Project indicator, targets and services, MNCS project implementation framework, Job description of CM and HP, etc.
Financial Management training
PHD provided training on financial management to the MNCS staff of these four Upazillas. The training was conducted by Mr. Sharif Ahmed, Finance Officer of PHD. A total number of 23 participants attended in this training program. The participants were oriented on internal control, cash management, advance management, banking operation management, procurement amazement, inventory management, standard books of account and documents, financial monitoring system, internal audit process and follow up, recruitment process, accounting basis, etc.
Training on UF & CM on MNCSWC formation & planning
Training on CSG Committee formation was provided to 98 MNCS staff. Among them, 49 participants were HP, CM –22, Depot holders -33 and UF-3 and paramedic -1. The content of the training covers the introduction of child health situation, government activities for motherand child care, roles of community group in implementation of MNCS activities, etc.
Training on Opinion Leaders for NGO Managers/Trainers/ Facilitators
Two-day ToT on opinion leaders were provided to 105 Participants through 04 batches. The main objective of the ToT was to brief the MNCS staff on the roles of the opinion leaders of the community in implementation of the activities under MNCS interventions. After receiving the training the staff will provide training to the opinion leaders on roles and responsibilities of opinion leaders. The community leaders included, teachers, headman, up members, Village doctors, religious leaders, etc.
Training on CSG Formation and Micro-planning Development
Training was provided to 1309 members of the CSG groups through 59 batches. Through this training the CSG members were sensitized on the issue of why the CSG groups are important to be formed in order to implement the activities of the MNCS project. Furthermore, they were provided the technical support to enhance their knowledge on how to develop their micro-plans for their respective areas.
Training on Supportive Supervision and MonitoringPHD-GRAUS organized a two-day training on Supportive Supervision and Monitoring to 53 mid-level MNCS staff, each 27 of 2 batches. Participants were gathered knowledge on different components of supportive supervision, roles of supervisors, decision-making process, time management, tools and techniques of supervision, supervision matrix, process of citizen monitoring, etc.
ToT on ANC, PNC & ENC

62
A ToT on Antenatal, Postnatal and Essential Newborn Care (ANC, PNC & ENC) was organized by PSTC at Civil Surgeon Office. A total number of 23 participants consists of UHFPO,UFPO, EPI Technicians, Senior Health education Officers, Junior Health Education Officers, Medical officer of Civil surgeon Office under Health & family planning department and MNCS staff attended the ToT.
MNCS organized a 5-day TOT on ANC, PNC & ENC for MNCS staffs. The ToT was conducted by a trained team (who received ToT) of PHD. A total number of 27 participants (MIS officer-4, UF-09, UM-01, Paramedic-02, CN-01, CM-10) attended in this ToT.
Training on ANC, PNC and ENC In December, a 5 days long training course on Antenatal, Postnatal and Essential Newborn Care (ANC, PNC & ENC) was organized at Upazila level for the MNCS staff in 10 batches. A total of 206 participants attended the training courses.
Selected doctors of Health & family planning department (who received TOT) and MNCS training team jointly conducted the sessions.
The training provided information on basic concept of present health situation of maternal and child health in Bangladesh, role of community counselor, basic concept on maternal health care, general problems during pregnancy and danger signs of pregnant mothers, postnatal care, newborn care, importance of breast feeding, taking care of sick children, danger signs of newborn and practical demonstration on conduction of counseling and group education etc.
Training on ANC, PNC and ENC
Training course on Antenatal, Postnatal and Essential Newborn Care (ANC, PNC & ENC) was organized at Upazila level for the MNCS staff. A total of 403 participants attended the training courses. Among them, 49 was HP, 22 was CM, 3 UF, 33 Depot holders and 1 paramedic. Selected Facilitator (who received TOT from UNICEF) and MNCS training team jointly conducted the sessions.
The training provided information on basic concept of present health situation of maternal and child health in Bangladesh, role of community counselor, basic concept on maternal health care, general problems during pregnancy and danger signs of pregnant mothers, postnatal care, newborn care, importance of breast feeding, taking care of sick children, danger signs of newborn and practical demonstration on conduction of counseling and group education etc.
Community Development and Training
Micro Planning Training to UHFWC Members Training was provided to the members of newly formed UHFWC (Union Health and Family Welfare Committee) in Rowangchhari, Ruma, Thanchi and Alikadam Upazilas on Micro planning. A total of 238 community people as members of UHFWC participated the training. Among them, 163 was Male and 75 were female members. The community people were oriented on maternal and child health, care of new born, types of planning, development of plan on the basis of problems identified in the community.
63
A ToT was provided to the 26 staff of MNCS on micro planning to deliver the training at community level. Among 26 staff, UM were 4, MIS were 5, UFs were 11, CMs were 6. The ToT was organized in the Royal Hotel.
Training for opinion leaders from the community 226 Community Leaders were provided training to capacitate them to voice their opinions to the relevant authorities. At the same time they were sensitized to take a leadership role in their respective communities in order to ensure that the MNCS services and activities are carried out according to the project requirements
CSG Action PlanningIn four Upazilas, all of the 99 CSGs completed the action plan. Before development of action plans they were provided with training on action planning. As a process of planning, the problems related with health issues were identified and on the basis of identified issues the problems were prioritized. After prioritization the problems were transferred as issues of planning.
UHFWC Action Planning
In all 14 unions, 14 Union Health and Family Welfare Committees developed 14 action plans except Tindu Union under Thanchi Upazila. On the basis of the CSG action plan the UH&FWC developed their action plans.
Exchange Visit by CSG Leaders
During the reporting period, a total of 72 CSG members participated in the exchange visit. The objective of these exchange visits was for the CSG leaders to have a chance to discuss the lessons learned and their experiences gained from their activities. During the visit they learned the activities of maternal and neonatal health, social mapping, referral mechanism, EPI coverage and communication system. After visit the teams shared their learning in a sharing meeting and developed a report on the basis of their findings and leanings.
4 days TBA Training
During a four day training on MNCS information 24 Traditional Birth Attendants (TBA) were trained at the CS office. All of the TBAs were from the remote areas of Ruma and Thanchi. Dr. Hla Hla Ching, Medical Officer of Bandarban Sadar Hospital and Ms. Mary Rani D’Costa, senior Nurse of Bandarban Sadar Hospital facilitated the training. They were trained on mothers’ care, existing practice, danger sign of pregnant mothers and new born, thermal care, necessity of breast-feeding within one hour, delayed bathing, etc.
Training of Adolescent on MNCS issues
A total of 115 Adolescents were provided with training on MNCS issues in Alikadam, Ruma, Rowangchhari and Thanchi. 115 students of four schools were attended in the training. They were: Rabar Para High School of Alikadam, Boikhongiri Junior High School, Thanchi High School and Ruma Government High School. The adolescents were oriented on objectives of MNCS interventions, government health facilities and their services, breast feeding, counseling, danger sign on new born, etc.
Government Staff
64
Training on PRA to GoB staffPRA training was organized for the government officials. 76 government people including Health Assistants, Health Inspectors, Assistant Health Inspectors and District Health Superintendents attended the training. PHD Training unit facilitated the PRA Training. The participants were oriented on tools of social mapping, force field analysis and problem ranking of Participatory Rapid Appraisal (PRA). As the process of training, the team was divided into two groups and practiced the tools at Majar Para of Sowalok union and Limuziri Para of Bandarban Sadar union. Along with the GoB Officials, 52 MNCS staff were also provided the training for enhancing their skills.
Training to UP Secretariats on Management & Coordination
Training on management and coordination was provided to 14 secretaries and 13 members of union Parishads of Ruma, Thanchi, Rowangchhari and Alikadam. In the meeting, various issues were discussed related on MNCS goal and objectives, strategies, introduction of MNCS and the roles and responsibilities of UP in ensuring MNCS services to mothers and community people. At the end of the training the participants shared their experiences gained during the training.
Meeting and Workshop
Monthly Meeting with CSG Members
The members of 99 CSG conduct monthly meeting. Concerned Union Facilitators and community Mobilizers attend the meetings. The members discuss the local level health issues and take necessary action. The monthly plans are reviewed and take required steps to involve the community people directly into the MNCS Issues related to maternal and child health. They also discuss the coverage of EPI and TT vaccination and no of referred cases of complicated patients to hospitals. Mobilization of the community people towards modern treatment and encourage the community people regarding home care practices are the main responsibilities of the CSG members. The members also discuss the success and failure regarding the above mentioned issues in their monthly meetings. Under this period, 891 monthly meetings were held.
UHFWC meeting
The members of 14 UHFWC conducted monthly meetings. Concerned Union Managers and Union Facilitators attend the meetings. The members review their plan which was developed on the basis of CSG’s plan, and take required steps to involve the community people directly into the MNCS Issues related to maternal and child health. They also discuss the coverage of EPI and TT vaccination and no of referred cases of complicated patients to hospitals. However, out of the planned 84 meetings, it was not possible to hold more than 54 due to unavoidable reasons at the local level.
Monthly Coordination meeting with Health and family planning department/Upazila Parishad/UDCC/ICDP
The staffs of the MNCS attend monthly and quarterly coordination meeting with health and family planning department, UDCC, ICDP and Upazila Coordination Meeting. In these meetings the MNCS staff shares its activities and periodic progress widely with local NGOs and Government and other stakeholders at Upazila and district level coordination meeting at

65
civil surgeon and DDFP office. The executive director of GRAUS attends in the Hill District council. On the other hand, Upazila Managers of MNCS project regularly attend at Upazila level monthly Coordination meeting. Through these Coordination meetings at different level MNCS has built a strong linkage with different stakes at different levels.
Annual workshop with project staff
This activity was implemented during at an excursion tour at Boga Lake under Ruma Sadar Union of Sadar Upazila. It was participated by all level staff (UF to DC) from the MNCS Project. The objective of this workshop was to provide a space for the participants where they would be able to share their experiences in relation to the MNCS project. The discussions during the workshop centered around the following issue: The completion status of the planned activities, the activities that have been planned for the next quarter, problems faced by staff during implementation of the project, possible ways to overcome the problems, challenges that the staff face for implementing the project, feedback received from the beneficiaries and stakeholders, etc.
BCC Activities and Communication
Conduct Social Mapping exercise
24 MNCS staff were Capacitated through this training to improve their skills in conducting Social Mapping. Social Mapping has till date proved to be an extremely effective tool for data collection and assessment of a community through the efforts of the community itself. An end-training evaluation has pointed out that the participants have been able to enhance their knowledge and skills in Social Mapping. They have expressed that they are much more confident to not only conduct Social mapping, but also will be able to pass on this training to others who are relevant with the MNCS project activities.
Documentation of Best Practices and Sharing
Under this activity, an initiative has been undertaken to document the best practices and to share the same with other clients. In line with the process, an outline of the content documentation was prepared. In the design of the documentation, some PRA tools like time line, changing trends and Venn diagram have been incorporated to assess the quality of the services, different milestones initiated by the CSG, changes and finally to snap the best practices that have changed the situation of mothers and child health.
MNCS Education to High Schools' Students
Initiative for improving MNCS home-care practices through providing orientation on MNCS education High school students was undertaken. Under this process, a total of 8 schools, 2 from each Upazilas were selected. The schools were: Ruma Government High school and Ruma Adibashi High School under Ruma Upazila, Bekong Junior High School of Alekhong Union and Rowangchhari High School under Rowangchhari Sadar Union of Rowangchhari Upazila, Choikong High School of Choikhong Union and the Alikadam
66
Madrasha under Alikadam upazila. School debates on the MNCS issues were organized between thestudents of different schools. Before organizing debates the students were oriented on safe motherhood, care of pregnant mothers and care of new born, danger sign of pregnant mothers and new born children.
Day Observation
MNCS observed Mina Day on 24 September 2010 by organizing rallies by the MNCS staff along with the students of primary and secondary schools in ten unions of four Upazilas. They conducted rallies with the slogan: Going to school is the only work for children, No children will remain out of the school anymore
-------------------------Mina
The MNCS Staff observed the following days were observed with the cooperation and required fervor of all concerned :
F World Health Day on 07th April 2010F World Hand Hygiene/washing Day on 05th May 2010F World Population Day on 11th July 2010F World Contraception Day – 26th September 2010F International AIDS Day on 01st December 2010F Safe motherhood day On 08th May 2010
Two National Immunization Days were observed on 8th January and 12th February 2011. In line with the NID observation, two planning meetings were organized in Civil Surgeon office. In the District level planning meetings the dates for the Upazila level planning meetings were fixed. At Upazila level planning meeting a micro plan on the responsibilities of the staff and government officials was develop in presence of concerned UHFPO.
Interactive Popular Theater (IPT)
The IPT or Interactive Popular Theatre is one of such initiatives to raise awareness among the general masses regarding health issues of Mothers and Newborn/Children. Two professional performance groups, namely, Chaga Theatre & Arts, and Chamok Theatre were contracted to develop the skill of three groups of young individuals for performing stage dramas on Mother and Child health issue. In total, the skill of 54 youths has been developed for this purpose.
The Scripts for the performances were developed by UNICEF which was then translated into Marma and Local Chittagong dialect for demonstration to the local communities. During the fifth quarter there were three demonstrations at three upazilas. In Thanchi and Rowangchhari the demonstrations were completed in Marma Language, where as in Alikadam Upazila the performance was done in Local
Chittagong dialect. Through these demonstrations, it is expected that the local community will receive positive messages on MNCS project issues and will be sensitized in the same.
In order to ensure that the performances by the youth groups retain the stipulated standard, the personnel from the Theatre groups to be present at the three demonstrations. In the future, we feel that the youth groups will be able to demonstrate the dramas according to the needs of the project.
Union Level MIS meeting Fourteen union level MIS were organized by the first week of each month. All the Health promoters attended the meeting and shared their reporting with the concerned Union Facilitators. The HP also
67
discussed the problems they face din the filed. The HPs verify their data collected from the field, finalize the report and submit to their concerned UFs. It is the place where the UF share any important decision of the management to the HPs. Under this period a total of 42 Union level MIS meetings were held in 14 unions.
Upazila Level GO-NGO MIS meeting
Each Upazila UM participated in GO-NGO MIS meeting in Upazila Health Complex and Family Planning Offices separately. In the meeting the UM present their reports on the activities, achievements, etc. with the other GO members. Under this quarter a total of 12 Upazila level GO-NGO MIS meetings were held in 4 upazilas.
Citizen Monitoring
As per the activity plan several citizen monitoring were conducted at field level by the representatives of Union Parishads and Upazila Parishads in different times during the reporting period. Some of them are mentioned below:
The Union Chairman of Nayapatang Union under Rowangchhari Upazilas visited east Bagmara and Changa Para to observe counseling of mothers. The chairman of Alakhyong union visited Chalpara to observe CSG meeting.
In Alikadam Upazila, the vice chairman of Upazila Parishad visited Babu Thoaisamong Karbari Para under Alikadam Sadar Union and observed a counseling session of a pregnant mother. He enquired various health related issues, check up and predation for delivery.
The chairman of Thanchi Sadar Union Parishad visited CSG. He attended the CSG monthly meeting and observed the health map and micro plan developed by CSG. He asked various questions on the formation of CSG, roles and responsibilities of CSG and monthly agendas of the meeting. He appreciated the initiatives undertaken by CSGs for moving forward in improving mother and child health.
The Upazila Chairman of Thanchi Upazila Parishad visited Khykrong Para Community Clinic and observed the activities of staff including paramedics of MNCS. He discussed various facilities provided by CC and also the limitations of the CC. He also talked with the community people and discussed the kinds of facilities the community people received from the Community Clinics.
GO-NGO Joint Monitoring
UH&FPO of Alikadam Upazilla visited Think Para and Kanushar para of Alikadam Sadar Panijiripara and Nayapar of Chowaikang Union with the MNCS staff. UHFPO visited the Thinkupara CC and observed the activities of paramedics. There he talked with the mothers of children who received check up from the paramedics. In Panjiri para of Chowaikng para he visited counselling of mothers and monitor the activities of HP
In Roungchori Modeical Officer of Rounagchori Upzilla Health Complex observed a counseling of HP in Wagi para-of Roungachori Sadar. During this period UH&FPO visited the nutun para of roungchori Sadar union. During his visit he discussed the MNCS issues and asses the understanding of CSG members on Micro plan issues.
The Civil Surgeon of Bandarban visited Community Clinic of Paglachora and Bajarpara under Rowangchhari Sadar union. In these CCs he talked with Community Mobilizers and Paramedics of MNCS interventions. The CS provided thanks to the MNCS staff for giving their assistance during NID and observation of other international days.
68
Some other important Activities
Dr. Md. Zia Ziaul Matin of UNICEF along with Ms Anna Barrete, Monitoring and Evaluation Expert, Dr. Zahid Hassan Consultant of MNCS visited Community Clinic of Khaching Para of Bandarban Sadar Upazila. The team also observed a counseling visit of a CM and met CSG members of Kamlong Para under Khohalong union and discussed various activities performed by the CSG.
An Annual review meeting of MNCS was jointly organized by IMCI section, DGHS and UNICEF on 10-11 Nov'10 at EPI conference room of Mohakhali, Dhaka. Health Managers from District/Upazila level, programme personnel from DGHS/UNICEF, UNICEF field colleagues (responsible for the MNCS district) as well as managers from partner NGOs attended the review meeting. In the meeting progress of MNCS implementation was reviewed, lesson learned were shared and on the basis of lesson learned the implmentation strategies were readdressed. You could still propose any other issues to be incorporated in the
Two street dramas were organized in Rowangchhari during this period. The second IPT show was played in Union Parishad Auditorium of Kachhaptoli Para under Rowangchhari Sadar Union. Chaga Art Theater of Bandarban facilitated the drama and the roles were played by the community adolescents received training from Chaga Theater. Ms. Tania Sultana, Communication for Development Specialist and Dr. Zahid Hassan Consultant of MNCS, of UNICEF observed the drama. A team comprising of Mr. Indra Lal Singh, Coordinator, CHT and Cox’s Bazar, Dr. Altaf Hossain, DPM, C-IMCI of DGHS with Dr. Ziaul Matin, Health Officer, H&N Section of UNICEF, Dr Zahid Hassan Consultant of UNICEF, Dr. Emdadul of ICDDRB, Ms. Tania sultana of UNICEF, et al. visited the monthly meeting of CSG of Purba Bagmara of Noapatong Union. The team discussed on health mapping, micro plan, monitoring and referral, etc. The team also visited mother assembly organized in Family Welfare Center (FWC) of Antaha Para under Noapatong union of Rowangchhari Upazila. The team talked with the pregnant mothers on check up and danger sign, etc.
Lesson Learned
MNCS intervention needs to be equipped to provide services in remote places in addition to mobilisation
To carry out the MNCS activities, the performances of the CSG members should be enriched by developing monitoring and Supervision skills
Effective instruction from higher authority is still needed to reactivate the Union committees in an effective way.
Key Challenges faced during this reporting periodNew approaches of service delivery through Dipot Holder were introduced in the upazilas of expansion areas. Scarcity of Depo –holders with minimum qualification (to provide MNCS services to the community in the remote areas) has interrupted the implementation of MNCS services activin time in the expansion areas.
.

69
It was found that most of the depot holders have been facing problems in receiving the message on MNCS issues properly due to their very limited listening skills. As the depot-holders came from different ethnic minority groups and most of them did not have skill on Marma language, it was also difficult for the trainers (Marma) to deliver knowledge in different ethnic languages.
14 Pahari Saystha Seva Centres situated in hard-to-reach areas which are the only source of health services are running without necessary medicine. District CS office provided medicine once, but at present no medicine is available, which has increased patient turnover. The project will further convey the issue with CS Office. Moreover, only possibility to provide MNCS services to MRO communities (who lives top of the hills) by organizing satellite clinics but it is not possible without medicine support.

70
Annual Report Of
Community Based Integrated Maternal, Neonatal and Child Survival (MNCS) Intervention for Expansion Areas of Bandarban
(Rowangchhari, Ruma, Thanchi and Alikadam)
PPeerriioodd:: AApprriill 22001111 –– DDeecceemmbbeerr 22001111
SSuubbmmiitttteedd TToo:: UUNNIICCEEFF BBaannggllaaddeesshh BBSSLL OOffffiiccee CCoommpplleexx,, 11 MMiinnttoo RRooaadd,, DDhhaakkaa 11000000,, BBaannggllaaddeesshh
Submitted By:
Partners in Health and Development (PHD)House No: SWD 12ARoad 8, Gulshan 1Dhaka---1212Bangladesh
IImmpplleemmeenntteedd bbyy::
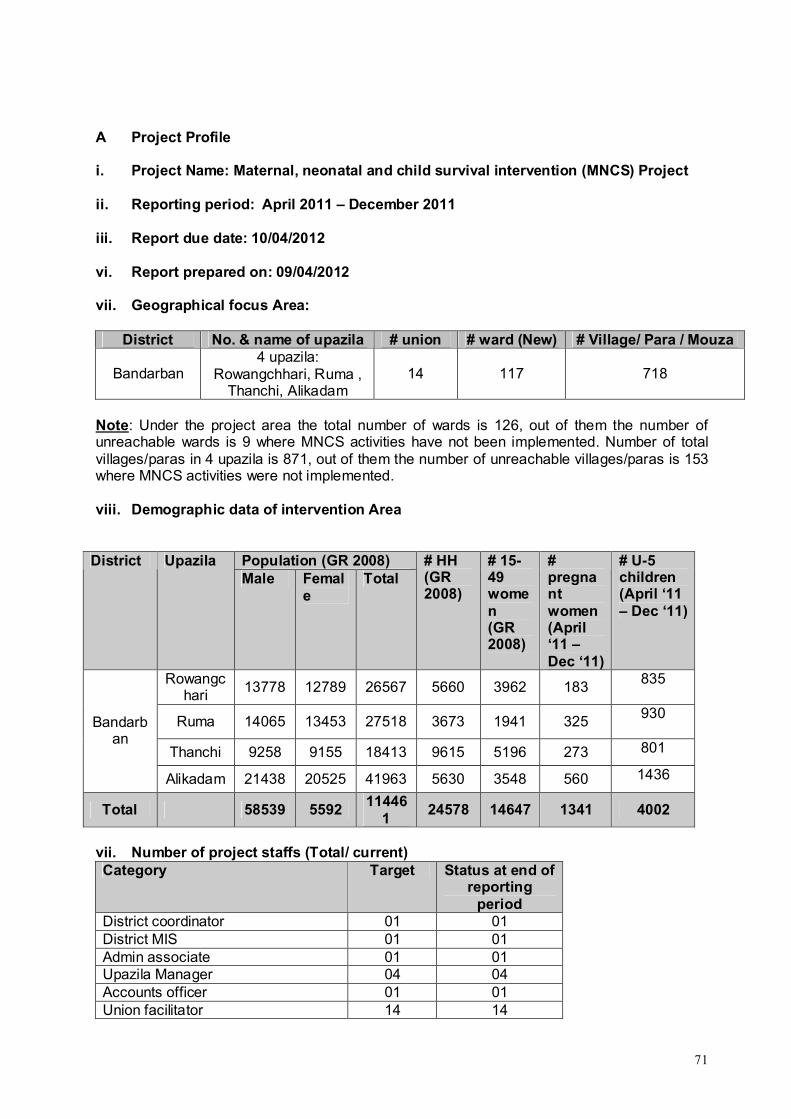
71
A Project Profile
i. Project Name: Maternal, neonatal and child survival intervention (MNCS) Project
ii. Reporting period: April 2011 – December 2011
iii. Report due date: 10/04/2012
vi. Report prepared on: 09/04/2012
vii. Geographical focus Area:
District No. & name of upazila # union # ward (New) # Village/ Para / Mouza
Bandarban4 upazila:
Rowangchhari, Ruma , Thanchi, Alikadam
14 117 718
Note: Under the project area the total number of wards is 126, out of them the number of unreachable wards is 9 where MNCS activities have not been implemented. Number of total villages/paras in 4 upazila is 871, out of them the number of unreachable villages/paras is 153 where MNCS activities were not implemented.
viii. Demographic data of intervention Area
Population (GR 2008)District UpazilaMale Femal
eTotal
# HH(GR 2008)
# 15-49 women(GR 2008)
# pregnant women(April ‘11 –Dec ‘11)
# U-5 children(April ‘11 – Dec ‘11)
Rowangchari
13778 12789 26567 5660 3962 183835
Ruma 14065 13453 27518 3673 1941 325930
Thanchi 9258 9155 18413 9615 5196 273 801
Bandarban
Alikadam 21438 20525 41963 5630 3548 560 1436
Total 58539 559211446
124578 14647 1341 4002
vii. Number of project staffs (Total/ current)Category Target Status at end of
reporting period
District coordinator 01 01District MIS 01 01Admin associate 01 01Upazila Manager 04 04Accounts officer 01 01Union facilitator 14 14
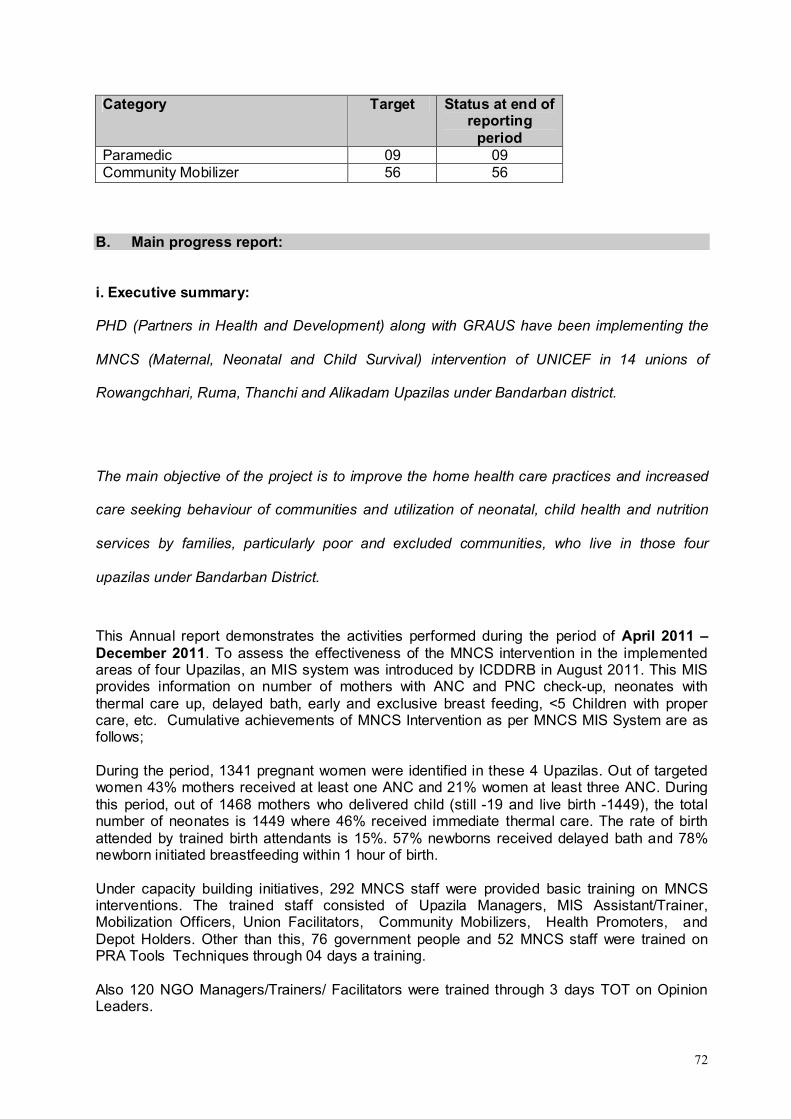
72
Category Target Status at end of reporting
periodParamedic 09 09Community Mobilizer 56 56
B. Main progress report:
i. Executive summary:
PHD (Partners in Health and Development) along with GRAUS have been implementing the
MNCS (Maternal, Neonatal and Child Survival) intervention of UNICEF in 14 unions of
Rowangchhari, Ruma, Thanchi and Alikadam Upazilas under Bandarban district.
The main objective of the project is to improve the home health care practices and increased
care seeking behaviour of communities and utilization of neonatal, child health and nutrition
services by families, particularly poor and excluded communities, who live in those four
upazilas under Bandarban District.
This Annual report demonstrates the activities performed during the period of April 2011 –December 2011. To assess the effectiveness of the MNCS intervention in the implemented areas of four Upazilas, an MIS system was introduced by ICDDRB in August 2011. This MIS provides information on number of mothers with ANC and PNC check-up, neonates with thermal care up, delayed bath, early and exclusive breast feeding, <5 Children with proper care, etc. Cumulative achievements of MNCS Intervention as per MNCS MIS System are as follows;
During the period, 1341 pregnant women were identified in these 4 Upazilas. Out of targeted women 43% mothers received at least one ANC and 21% women at least three ANC. During this period, out of 1468 mothers who delivered child (still -19 and live birth -1449), the total number of neonates is 1449 where 46% received immediate thermal care. The rate of birth attended by trained birth attendants is 15%. 57% newborns received delayed bath and 78% newborn initiated breastfeeding within 1 hour of birth.
Under capacity building initiatives, 292 MNCS staff were provided basic training on MNCS interventions. The trained staff consisted of Upazila Managers, MIS Assistant/Trainer, Mobilization Officers, Union Facilitators, Community Mobilizers, Health Promoters, and Depot Holders. Other than this, 76 government people and 52 MNCS staff were trained on PRA Tools Techniques through 04 days a training.
Also 120 NGO Managers/Trainers/ Facilitators were trained through 3 days TOT on Opinion Leaders.
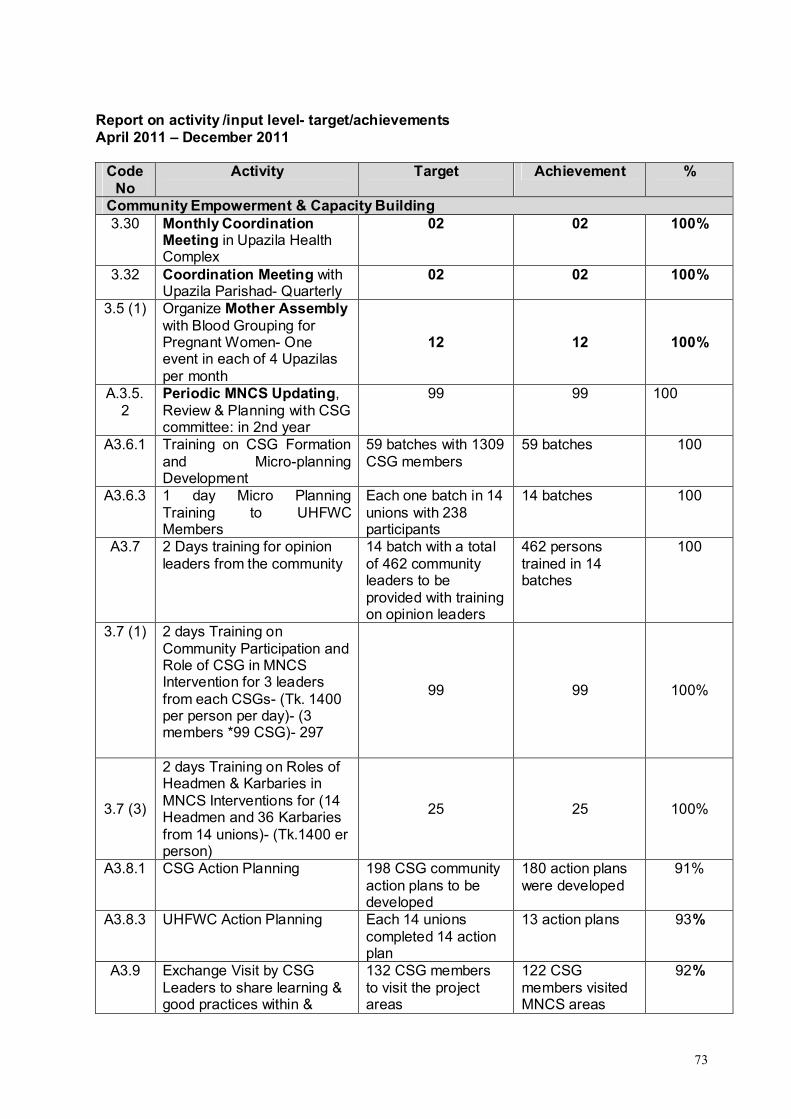
73
Report on activity /input level- target/achievements April 2011 – December 2011
Code No
Activity Target Achievement %
Community Empowerment & Capacity Building 3.30 Monthly Coordination
Meeting in Upazila Health Complex
02 02 100%
3.32 Coordination Meeting with Upazila Parishad- Quarterly
02 02 100%
3.5 (1) Organize Mother Assemblywith Blood Grouping for Pregnant Women- One event in each of 4 Upazilas per month
12 12 100%
A.3.5.2
Periodic MNCS Updating, Review & Planning with CSG committee: in 2nd year
99 99 100
A3.6.1 Training on CSG Formation and Micro-planning Development
59 batches with 1309 CSG members
59 batches 100
A3.6.3 1 day Micro Planning Training to UHFWC Members
Each one batch in 14 unions with 238 participants
14 batches 100
A3.7 2 Days training for opinion leaders from the community
14 batch with a total of 462 community leaders to be provided with training on opinion leaders
462 persons trained in 14 batches
100
3.7 (1) 2 days Training on Community Participation and Role of CSG in MNCS Intervention for 3 leaders from each CSGs- (Tk. 1400 per person per day)- (3 members *99 CSG)- 297
99 99 100%
3.7 (3)
2 days Training on Roles of Headmen & Karbaries in MNCS Interventions for (14 Headmen and 36 Karbaries from 14 unions)- (Tk.1400 er person)
25 25 100%
A3.8.1 CSG Action Planning 198 CSG community action plans to be developed
180 action plans were developed
91%
A3.8.3 UHFWC Action Planning Each 14 unions completed 14 action plan
13 action plans 93%
A3.9 Exchange Visit by CSG Leaders to share learning & good practices within &
132 CSG members to visit the project areas
122 CSG members visited MNCS areas
92%
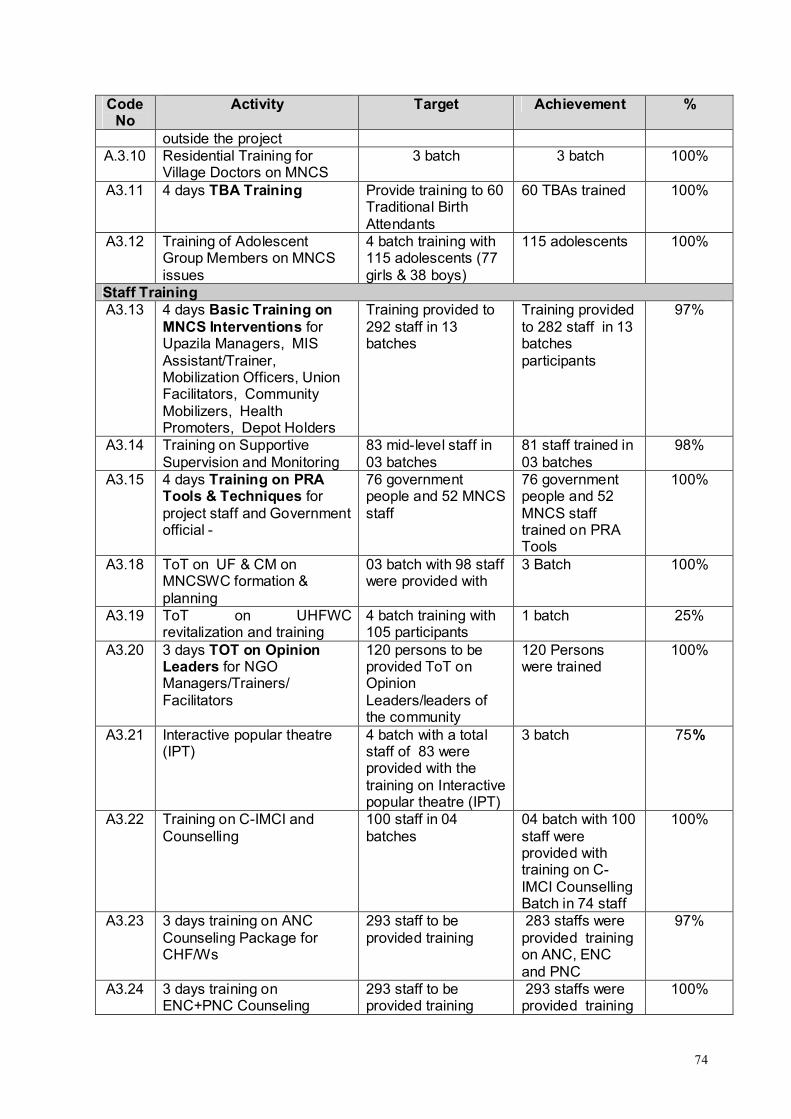
74
Code No
Activity Target Achievement %
outside the projectA.3.10 Residential Training for
Village Doctors on MNCS 3 batch 3 batch 100%
A3.11 4 days TBA Training Provide training to 60 Traditional Birth Attendants
60 TBAs trained 100%
A3.12 Training of Adolescent Group Members on MNCS issues
4 batch training with 115 adolescents (77 girls & 38 boys)
115 adolescents 100%
Staff Training A3.13 4 days Basic Training on
MNCS Interventions for Upazila Managers, MIS Assistant/Trainer, Mobilization Officers, Union Facilitators, Community Mobilizers, Health Promoters, Depot Holders
Training provided to 292 staff in 13 batches
Training provided to 282 staff in 13 batches participants
97%
A3.14 Training on Supportive Supervision and Monitoring
83 mid-level staff in 03 batches
81 staff trained in 03 batches
98%
A3.15 4 days Training on PRA Tools & Techniques for project staff and Government official -
76 government people and 52 MNCS staff
76 government people and 52 MNCS staff trained on PRA Tools
100%
A3.18 ToT on UF & CM on MNCSWC formation & planning
03 batch with 98 staff were provided with
3 Batch 100%
A3.19 ToT on UHFWC revitalization and training
4 batch training with 105 participants
1 batch 25%
A3.20 3 days TOT on Opinion Leaders for NGO Managers/Trainers/ Facilitators
120 persons to be provided ToT on Opinion Leaders/leaders of the community
120 Persons were trained
100%
A3.21 Interactive popular theatre (IPT)
4 batch with a total staff of 83 were provided with the training on Interactive popular theatre (IPT)
3 batch 75%
A3.22 Training on C-IMCI and Counselling
100 staff in 04 batches
04 batch with 100 staff were provided with training on C-IMCI Counselling Batch in 74 staff
100%
A3.23 3 days training on ANC Counseling Package for CHF/Ws
293 staff to be provided training
283 staffs were provided training on ANC, ENC and PNC
97%
A3.24 3 days training on ENC+PNC Counseling
293 staff to be provided training
293 staffs were provided training
100%

75
Code No
Activity Target Achievement %
Package for NGO staffs on ANC, ENC and PNC
Capacity Building support to Union Parishad & GOB StaffA.3.25 4 days refreshers on C-IMCI,
ANC & ENC+PNCCounseling
9 batch 9 batch100%
A3.26 Training to UP Secretariats on Management & Coordination of Health Intervention in the Union
Provided training to 14 union secretariat
14 secretariat 100%
3.26.1 4 days Training on Tools and Techniques of Community Participation for ICDP staff
20 20 100%
3.26.2 Day long training-1 on MNCS Interventions and its achievement (good practices for 13 UP representatives from each of 14 unions- (182 representatives)
16 16 100%
3.26.3 Day long training-2 on Citizen Monitoring in MNCS Intervention and Local Resource Mobilization for 13 UP representatives from each of 14 unions- (182 representatives)
16 16 100%
3.26.4 Day long training-3 on Promotion of Social Responsibility and Integration of MNCS Intervention in Union Development Plan for 13 UP representatives from each of 14 unions- (182 representatives)
1616 100%
3.26.7 Supervision & Monitoring of MNCS Interventions- HA and FWA (80) so as to take responsibility after phase out
16 16 100%
Meeting & Local level planningA3.27 CSG meeting 1007 meetings A total of 1007
meetings conducted
100%
A3.29 UHFWC meeting for action planning
166 union based meetings
A total of 132 meetings conducted
80%
A3.30 Monthly Coordination Meeting in Upazila Health Complex
80 coordination meeting
68 coordination meetings held
85%
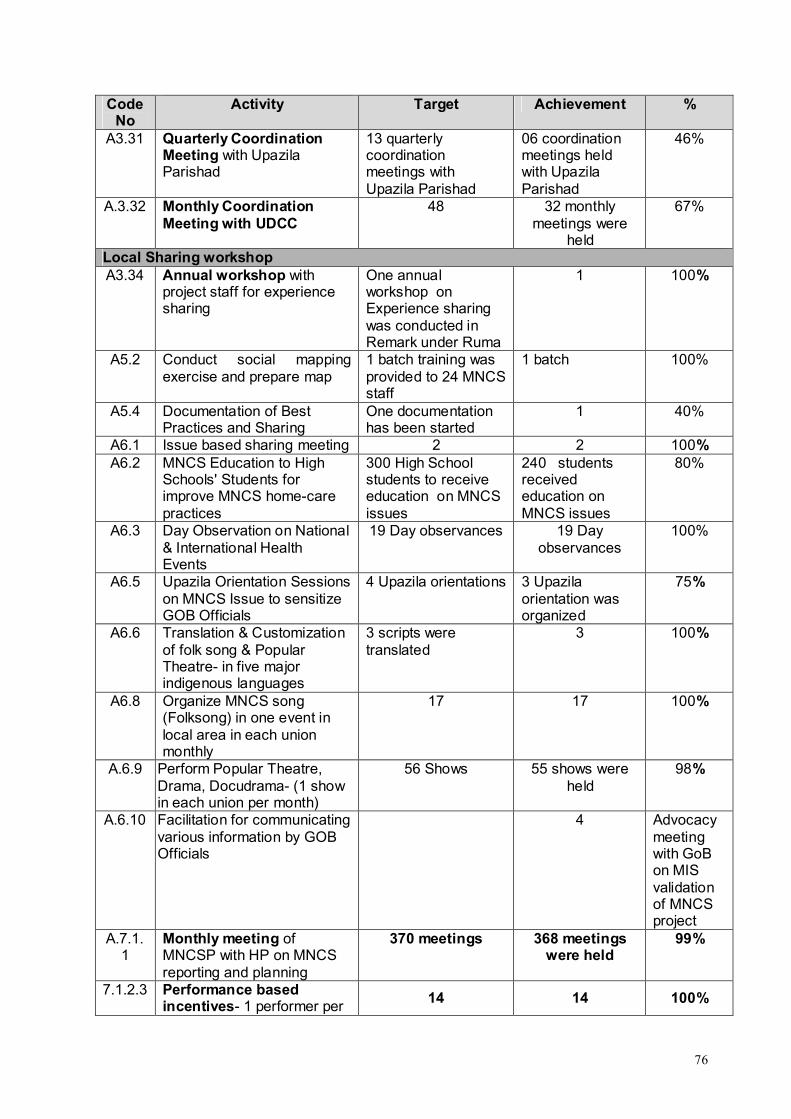
76
Code No
Activity Target Achievement %
A3.31 Quarterly Coordination Meeting with Upazila Parishad
13 quarterly coordination meetings with Upazila Parishad
06 coordination meetings held with Upazila Parishad
46%
A.3.32 Monthly Coordination Meeting with UDCC
48 32 monthly meetings were
held
67%
Local Sharing workshopA3.34 Annual workshop with
project staff for experience sharing
One annual workshop on Experience sharing was conducted in Remark under Ruma
1 100%
A5.2 Conduct social mapping exercise and prepare map
1 batch training was provided to 24 MNCS staff
1 batch 100%
A5.4 Documentation of Best Practices and Sharing
One documentation has been started
1 40%
A6.1 Issue based sharing meeting 2 2 100%A6.2 MNCS Education to High
Schools' Students for improve MNCS home-care practices
300 High School students to receive education on MNCS issues
240 students received education on MNCS issues
80%
A6.3 Day Observation on National & International Health Events
19 Day observances 19 Day observances
100%
A6.5 Upazila Orientation Sessions on MNCS Issue to sensitize GOB Officials
4 Upazila orientations 3 Upazila orientation was organized
75%
A6.6 Translation & Customization of folk song & Popular Theatre- in five major indigenous languages
3 scripts were translated
3 100%
A6.8 Organize MNCS song (Folksong) in one event in local area in each union monthly
17 17 100%
A.6.9 Perform Popular Theatre, Drama, Docudrama- (1 show in each union per month)
56 Shows 55 shows were held
98%
A.6.10 Facilitation for communicating various information by GOB Officials
4 Advocacy meeting with GoB on MIS validation of MNCS project
A.7.1.1
Monthly meeting of MNCSP with HP on MNCS reporting and planning
370 meetings 368 meetings were held
99%
7.1.2.3 Performance based incentives- 1 performer per
14 14 100%
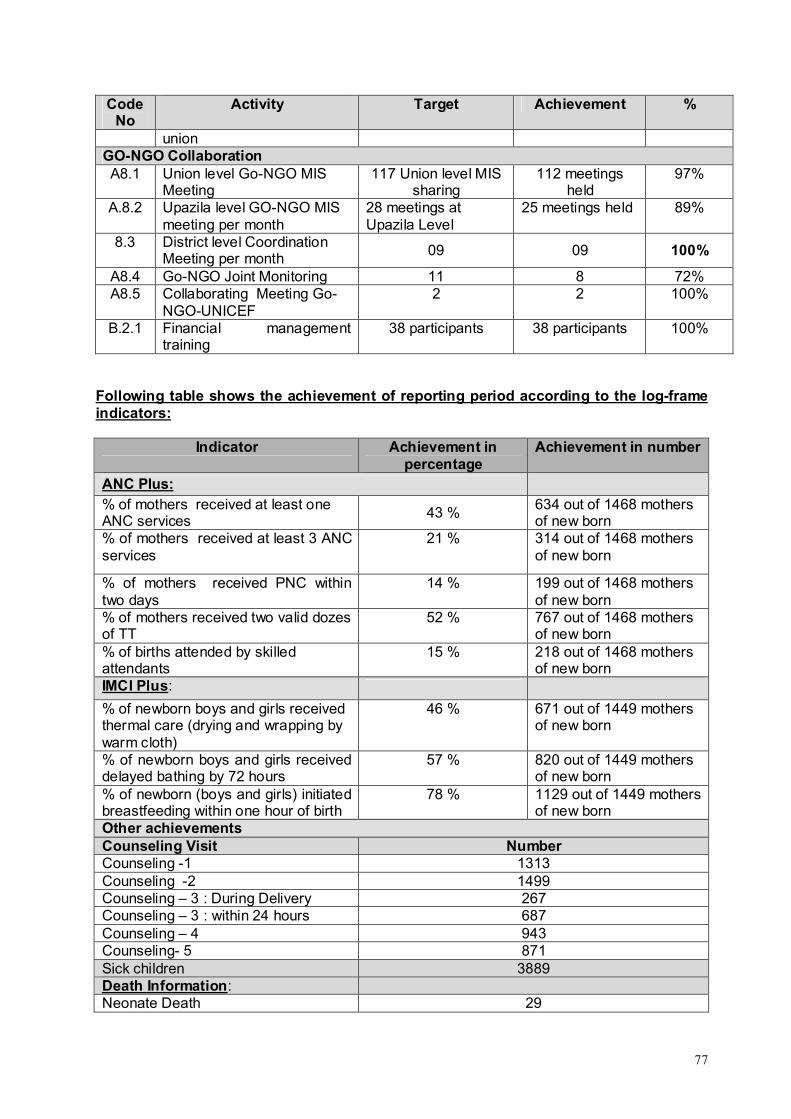
77
Code No
Activity Target Achievement %
unionGO-NGO CollaborationA8.1 Union level Go-NGO MIS
Meeting117 Union level MIS
sharing112 meetings
held97%
A.8.2 Upazila level GO-NGO MIS meeting per month
28 meetings at Upazila Level
25 meetings held 89%
8.3 District level Coordination Meeting per month
09 09 100%
A8.4 Go-NGO Joint Monitoring 11 8 72%A8.5 Collaborating Meeting Go-
NGO-UNICEF2 2 100%
B.2.1 Financial management training
38 participants 38 participants 100%
Following table shows the achievement of reporting period according to the log-frame indicators:
Indicator Achievement in percentage
Achievement in number
ANC Plus:% of mothers received at least one ANC services
43 %634 out of 1468 mothers of new born
% of mothers received at least 3 ANC services
21 % 314 out of 1468 mothers of new born
% of mothers received PNC within two days
14 % 199 out of 1468 mothers of new born
% of mothers received two valid dozes of TT
52 % 767 out of 1468 mothers of new born
% of births attended by skilled attendants
15 % 218 out of 1468 mothers of new born
IMCI Plus:
% of newborn boys and girls received thermal care (drying and wrapping by warm cloth)
46 % 671 out of 1449 mothers of new born
% of newborn boys and girls received delayed bathing by 72 hours
57 % 820 out of 1449 mothers of new born
% of newborn (boys and girls) initiated breastfeeding within one hour of birth
78 % 1129 out of 1449 mothers of new born
Other achievementsCounseling Visit NumberCounseling -1 1313Counseling -2 1499Counseling – 3 : During Delivery 267Counseling – 3 : within 24 hours 687Counseling – 4 943Counseling- 5 871Sick children 3889Death Information:Neonate Death 29
78
Indicator Achievement in percentage
Achievement in number
Death of children within < 1 year 22Death of children within < 5 year 18
Narrative Statement of some Activities of MNCS Intervention (April 2011 – December 2011)
Training on ANC, PNC and ENC
Training course on Antenatal, Postnatal and Essential Newborn Care (ANC, PNC & ENC) was organized at Upazila level for MNCS staff. A total of 283 participants attended the training courses. Selected Facilitator (who received TOT from UNICEF) and MNCS training team jointly conducted the sessions.
The training provided information on basic concept of present health situation of maternal and child health in Bangladesh, role of community counselor, basic concept on maternal health care, general problems during pregnancy and danger signs of pregnant mothers, postnatal care, newborn care, importance of breast feeding, taking care of sick children, danger signs of newborn and practical demonstration on conduction of counseling and group education etc.
Community Development and Training
Micro Planning Training to UHFWC Members
As part of the ongoing initiative to build the capacity of Government level staff and local government representatives, a number of initiatives were taken during the reporting period. A few of the mentionable initiatives are:
14 UP Secretariats were provided training on Management & Coordination of Health Intervention in the Unions. Through this initiat5ive, it is expected that the Union Parishads will be capacitated to understand the needs in their respective Unions and will be better equipped to take informed decisions to ensure that the required MNCS initiatives are taken accordingly. Other than this, 20 batches of ICDP staff were trained in Tools and Techniques of Community Participation. 182 representatives from 14 unions were provided training on MNCS Interventions and its achievement through 16 Day long sessions. Through this initiative, the 13 UP representatives were able to share their good practices with each other.
Other than the above, 80 HAs and FWAs were provided training on Supervision & Monitoring of MNCS Interventions through 16 batches.
Training for opinion leaders from the community 462 Community Leaders were provided training in 14 batches to capacitate them to voice their opinions to the relevant authorities. At the same time they were sensitized to take a leadership role in their respective communities in order to ensure that the MNCS services and activities are carried out according to the project requirements
CSG Action PlanningIn four Upazilas, all of the 180 out of the targeted 198 CSG action Plans were developed. Before development of action plans they were provided with training on action planning. As a process of planning, the problems related with health issues were identified and on the basis of identified issues the problems were prioritized. After prioritization the problems were transferred as issues of planning.
79
UHFWC Action PlanningIn all 14 unions, 13 Union Health and Family Welfare Committees developed 13 action plans except Tindu Union under Thanchi Upazila. On the basis of the CSG action plan the UH&FWC developed their action plans.
Exchange Visit by CSG Leaders
During the reporting period, a total of 122 CSG members participated in the exchange visit. The objective of these exchange visits was for the CSG leaders to have a chance to discuss the lessons learned and their experiences gained from their activities. During the visit they learned the activities of maternal and neonatal health, social mapping, referral mechanism, EPI coverage and communication system. After visit the teams shared their learning in a sharing meeting and developed a report on the basis of their findings and leanings.
4 days TBA Training
During 02 four-day training on MNCS information 60 Traditional Birth Attendants (TBA) were trained at the CS office. Qualified MBBS Doctors from Bandarban Sadar Hospital facilitated the training sessions. The community nurses were trained on mothers’ care, existing practice, danger sign of pregnant mothers and new born, thermal care, necessity of breast-feeding within one hour, delayed bathing, etc.
Training of Adolescent on MNCS issuesA total of 115 Adolescents were provided with training on MNCS issues in Alikadam, Ruma, Rowangchhari and Thanchi. 115 students of four schools were attended in the training. They were: Rabar Para High School of Alikadam, Boikhongiri Junior High School, Thanchi High School and Ruma Government High School. The adolescents were oriented on objectives of MNCS interventions, government health facilities and their services, breast feeding, counseling, danger sign on new born, etc.
Government StaffTraining on PRA to GoB staffPRA training was organized for the government officials. 76 government people including Health Assistants, Health Inspectors, Assistant Health Inspectors and District Health Superintendents attended the training. PHD Training unit facilitated the PRA Training. The participants were oriented on tools of social mapping, force field analysis and problem ranking of Participatory Rapid Appraisal (PRA). As the process of training, the team was divided into two groups and practiced the tools at Majar Para of Sowalok union and Limuziri Para of Bandarban Sadar union. Along with the GoB Officials, 52 MNCS staff were also provided the training for enhancing their skills.
Training to UP Secretariats on Management & Coordination
Training on management and coordination was provided to 14 secretaries and 13 members of union Parishads of Ruma, Thanchi, Rowangchhari and Alikadam. In the meeting, various issues were discussed related on MNCS goal and objectives, strategies, introduction of MNCS and the roles and responsibilities of UP in ensuring MNCS services to mothers and community people. At the end of the training the participants shared their experiences gained during the training.
Meeting and Workshop

80
Monthly Meeting with CSG Members The members of 99 CSG conduct monthly meeting. Concerned Union Facilitators and community Mobilizers attend the meetings. The members discuss the local level health issues and take necessary action. The monthly plans are reviewed and take required steps to involve the community people directly into the MNCS Issues related to maternal and child health. They also discuss the coverage of EPI and TT vaccination and no of referred cases of complicated patients to hospitals. Mobilization of the community people towards modern treatment and encourage the community people regarding home care practices are the main responsibilities of the CSG members. The members also discuss the success and failure regarding the above mentioned issues in their monthly meetings. Under this period, 891 monthly meetings were held.
UHFWC meeting The members of 14 UHFWC conducted monthly meetings. Concerned Union Managers and Union Facilitators attend the meetings. The members review their plan which was developed on the basis of CSG’s plan, and take required steps to involve the community people directly into the MNCS Issues related to maternal and child health. They also discuss the coverage of EPI and TT vaccination and no of referred cases of complicated patients to hospitals. However, out of the planned 166 meetings, it was not possible to hold 34 meetings due to unavoidable reasons at the local level.
Monthly Coordination meeting with Health and family planning department/Upazila Parishad/UDCC/ICDPThe staffs of the MNCS attend monthly and quarterly coordination meeting with health and family planning department, UDCC, ICDP and Upazila Coordination Meeting. In these meetings the MNCS staff shares its activities and periodic progress widely with local NGOs and Government and other stakeholders at Upazila and district level coordination meeting at civil surgeon and DDFP office. The executive director of GRAUS attends in the Hill District council. On the other hand, Upazila Managers of MNCS project regularly attend at Upazila level monthly Coordination meeting. Through these Coordination meetings at different levelMNCS has built a strong linkage with different stakes at different levels.
Annual workshop with project staff
This activity was implemented during at an excursion tour at Boga Lake under Ruma Sadar Union of Sadar Upazila. It was participated by all level staff (UF to DC) from the MNCS Project. The objective of this workshop was to provide a space for the participants where they would be able to share their experiences in relation to the MNCS project. The discussions during the workshop centered around the following issue: The completion status of the planned activities, the activities that have been planned for the next quarter, problems faced by staff during implementation of the project, possible ways to overcome the problems, challenges that the staff face for implementing the project, feedback received from the beneficiaries and stakeholders, etc.
BCC Activities and Communication
Conduct Social Mapping exercise

81
24 MNCS staff was Capacitated through this training to improve their skills in conducting Social Mapping. Social Mapping has till date proved to be an extremely effective tool for data collection and assessment of a community through the efforts of the community itself. An end-training evaluation has pointed out that the participants have been able to enhance their knowledge and skills in Social Mapping. They have expressed that they are much more confident to not only conduct Social mapping, but also will be able to pass on this training to others who are relevant with the MNCS project activities.
Documentation of Best Practices and Sharing Under this activity, an initiative has been undertaken to document the best practices and to share the same with other clients. In line with the process, an outline of the content documentation was prepared. In the design of the documentation, some PRA tools like time line, changing trends and Venn diagram have been incorporated to assess the quality of the services, different milestones initiated by the CSG, changes and finally to snap the best practices that have changed the situation of mothers and child health.
MNCS Education to High Schools' Students Initiative for improving MNCS home-care practices through providing orientation on MNCS education High school students was undertaken. Under this process, a total of 8 schools, 2 from each Upazilas were selected. The schools were: Ruma Government High school and Ruma Adibashi High School under Ruma Upazila, Bekong Junior High School of Alekhong Union and Rowangchhari High School under Rowangchhari Sadar Union of Rowangchhari Upazila, Choikong High School of Choikhong Union and the Alikadam Madrasha under Alikadam upazila. School debates on the MNCS issues were organized between the students of different schools. Before organizing debates the students were oriented on safe motherhood, care of pregnant mothers and care of new born, danger sign of pregnant mothers and new born children.
Interactive Popular Theater (IPT)
The IPT or Interactive Popular Theatre is one of such initiatives to raise awareness among the general masses regarding health issues of Mothers and Newborn/Children. Two professional performance groups, namely, Chaga Theatre & Arts, and Chamok Theatre were contracted to develop the skill of three groups of young individuals for performing stage dramas on Mother and Child health issue. In total, the skill of 54 youths has been developed for this purpose.
The Scripts for the performances were developed by UNICEF which was then translated into Marma and Local Chittagong dialect for demonstration to the local communities. During the fifth quarter there were three demonstrations at three upazilas. In Thanchi and Rowangchhari the demonstrations were completed in Marma Language, where as in Alikadam Upazila the performance was done in Local Chittagong dialect. Through these demonstrations, it is expected that the local community will receive positive messages on
MNCS project issues and will be sensitized in the same.
82
In order to ensure that the performances by the youth groups retain the stipulated standard, the personnel from the Theatre groups to be present at the three demonstrations. In the future, we feel that the youth groups will be able to demonstrate the dramas according to the needs of the project.
Union Level MIS meeting Fourteen union level MIS were organized by the first week of each month. All the Health promoters attended the meeting and shared their reporting with the concerned Union Facilitators. The HP also discussed the problems they face din the filed. The HPs verify their data collected from the field, finalize the report and submit to their concerned UFs. It is the place where the UF share any important decision of the management to the HPs. Under this period a total of 42 Union level MIS meetings were held in 14 unions.
Upazila Level GO-NGO MIS meetingEach Upazila UM participated in GO-NGO MIS meeting in Upazila Health Complex and Family Planning Offices separately. In the meeting the UM present their reports on the activities, achievements, etc. with the other GO members. During thjis reporting period, a total of 112 meetings were held out of the planned 117.
Citizen Monitoring As per the activity plan several citizen monitoring were conducted at field level by the representatives of Union Parishads and Upazila Parishads in different times during the reporting period. Some of them are mentioned below:
The Union Chairman of Nayapatang Union under Rowangchhari Upazilas visited east Bagmara and Changa Para to observe counseling of mothers. The chairman of Alakhyong union visited Chalpara to observe CSG meeting.
In Alikadam Upazila, the vice chairman of Upazila Parishad visited Babu Thoaisamong Karbari Para under Alikadam Sadar Union and observed a counseling session of a pregnant mother. He enquired various health related issues, check up and predation for delivery.
The chairman of Thanchi Sadar Union Parishad visited CSG. He attended the CSG monthly meeting and observed the health map and micro plan developed by CSG. He asked various questions on the formation of CSG, roles and responsibilities of CSG and monthly agendas of the meeting. He appreciated the initiatives undertaken by CSGs for moving forward in improving mother and child health.
The Upazila Chairman of Thanchi Upazila Parishad visited Khykrong Para Community Clinic and observed the activities of staff including paramedics of MNCS. He discussed various facilities provided by CC and also the limitations of the CC. He also talked with the community people and discussed the kinds of facilities the community people received from the Community Clinics.
GO-NGO Joint Monitoring A total of 08 Joint monitoring were held out of the planned 11. through this initiative, the Government level officials were presented with the opportunity to visit the working areas and physically see the initiatives being taken by the MNCS Project. It also provided an opportunity to understand the relevance of Government as well as Non-Government joint efforts for attaining the MNCS objectives.
Lesson Learned

83
MNCS intervention needs to be equipped to provide services in remote places in addition to mobilization
To carry out the MNCS activities, the performances of the CSG members should be enriched by developing monitoring and Supervision skills
Effective instruction from higher authority is still needed to reactivate the Union committees in an effective way.
Key Challenges faced during this reporting period
New approaches of service delivery through Dipot Holder were introduced in the upazilas of expansion areas. Scarcity of Depot–holders with minimum qualification (to provide MNCS services to the community in the remote areas) has interrupted the implementation of MNCS services active time in the expansion areas.
It was found that most of the depot holders have been facing problems in receiving the message on MNCS issues properly due to their very limited listening skills. As the depot-holders came from different ethnic minority groups and most of them did not have skill on Marma language, it was also difficult for the trainers (Marma) to deliver knowledge in different ethnic languages.
Scarcity of qualified Community Nurse (CN) and Depot holders in the hard to reach and impossible areas to provide basic health care services is one of the major challenges of the MNCS in these areas, particularly in Thanchi and Ruma.

84
ANNEX 4. Photographs with captions on C4D and other major activities
World AIDS Day
NIDVitamin A Plus Campaign
@(
Hand washing Day
Safe Motherhood Day
Disaster Preparedness day
Meena day
Population day
Breastfeeding day
11 July: World Heath Day
01 December: World AIDs Day
08 October: Hand Washing Day
28 May: Safe Motherhood Day
04 August: Breast Feeding Day
31 March: Disaster Day
24 September: Meena Day
29 May: NID Campaign