COMMUNITY ASSESSMENT 1: BASIC CONCEPTS · Community Assessment 1: Basic Concepts Gerry Oliva,...
73
Jointly sponsored by California Department of Health Services, Maternal and Child Health Branch, Perinatal Advisory Council: Leadership, Advocacy, and Consultation (PAC/LAC), and Family Health Outcomes Project, UCSF COMMUNITY ASSESSMENT 1: BASIC CONCEPTS October 8, 2003 Sacramento, CA presents
Transcript of COMMUNITY ASSESSMENT 1: BASIC CONCEPTS · Community Assessment 1: Basic Concepts Gerry Oliva,...

Jointly sponsored byCalifornia Department of Health Services, Maternal and Child Health Branch,
Perinatal Advisory Council: Leadership, Advocacy, and Consultation (PAC/LAC),and Family Health Outcomes Project, UCSF
COMMUNITY ASSESSMENT 1: BASIC CONCEPTS
October 8, 2003Sacramento, CA
presents

COMMUNITY ASSESSMENT 1: BASIC CONCEPTS
f
Ger
MC
T
Family Health Outcomes Project Staf
aldine Oliva, MD, MPH Director
Judith A. Hager Belfiori, MA, MPH Director of Planning and Evaluation
Brianna Gass, MPH H Project Coordinator
Nadia Thind, MPH Research Associate
Jennifer Gee
raining Coordinator Mary Tran
Administrative Assistant

TODAY’S AGENDA
By the end of the training, participants should be able to perform and facilitate a community health assessment with other staff for their next scope of work. At the conclusion of this course, the participant will be able to:
• Articulate the steps of a community assessment process • Develop a community health profile • Assess the adequacy of MCH community resources • Assess MCH agency capacity • Measure and assess required Title V indicators • Identify the advantages and disadvantages of qualitative and quantitative data 8:30 am Coffee and Registration
erview of Title V Planning Model 9:00 am Welcome, Introductions, and Ov
Introduction to Planning Cycle Geraldine Oliva, MD, MPH and Judith A. Hager Belfiori, MA, MPH
Session ealth Profile 9:45 am 1. Community H
Nadia Thind, MPH
reak 10:15 am B Session sources Assessment 10:25 am 1. Community Re
Nadia Thind, MPH Session 10:40 am 2. Assessment of MCH Capacity
Judith A. Hager Belfiori, MA, MPH Session rs 11:20 am 3. Measuring and Assessing Required Title V Indicato
Brianna Gass, MPH and Judith A. Hager Belfiori, MA, MPH
unch 12:00 pm L Exercise. 1:00 pm
reak 2:15 pm B
Session 4. Options for Collecting and Presenting Community Assessment Data
2:30 pm
Geraldine Oliva, MD, MPH
eline and Preview of Next Workshop 3:45 pm Review of State MCH TimWrap Up and Evaluation
Geraldine Oliva, MD, MPH

TABLE OF CONTENTS
Overview
“Developing an Effective MCH Planning Process, Community Assessment 1: Basic Concepts”
Geraldine Oliva, MD, MPH 2
Session One. Community Health Profile Participants Guide 7
“Community Health Profile and Community Capacity Assessment” Nadia Thind, MPH 8
Community Health Profile Sources 16
Community Health Profile Examples 17
Session Two. MCH Agency Capacity Participants Guide 41
“MCH Program Capacity Assessment” Judith Hager Belfiori, MA, MPH 42
Assessing Local MCH Program Capacities 43
MCH Capacity Rating and Reporting Tool 51
MCH Program Capacity Assessment Worksheet 55
Session Three. Title V Indicators Participants Guide 57
“Measuring and Assessing Required Title V Indicators” Brianna Gass, MPH 59
Data Sources for Title V Indicators 68
Session Four. Data Options Participants Guide 74
“Options for Collecting and Presenting Assessment Data” Geraldine Oliva, MD, MPH 75

COMMUNITY ASSESSMENT 1: BASIC CONCEPTS
Overview
Developing an Effective MCH Planning Process
Presented by:
Geraldine Oliva, MD, MPH Director
Family Health Outcomes Project
Judith A. Hager Belfiori, MA, MPH Director of Planning and Evaluation
Family Health Outcomes Project

Developing an Effective MCH Planning Process,
Community Assessment 1: Basic Concepts
Gerry Oliva, M.D,MPHFamily Health Outcomes Project
October 8, 2003
HistoricalContext
1989 - OBRA ‘89 requires the federal MCH Bureau to monitor a set of HP 2000 indicators1992 - AB99 Committee in California recommends monitoring a larger number of HP2000 indicators 1993 - California MCH Branch with FHOP initiates data capacity building effort to assist local health jurisdictions (LHJs)
Historical Context (cont)1993 - Government Performance and Results Act (GPRA) mandates performance measures1997 - Federal MCHB Title V grant guidance requires state reporting on performance indicators and outcomes1998 - CAMCHB requires LHJs to include these measures in their 5-year assessments1999 Federal MCHB adds needs indicators to the Title V Guidance
FHOP Community Assessment 1 October 2003 2

2003 and Beyond2003 Federal MCHB 2005 grant guidance includes more indicators
2003 California MCH Branch issues new Title V guidelines for LHJ community assessment due on June 30, 2004.
Components of the 2003 CAMCH Guidelines
Description of the Community Assessment Process MCH Planning Group Mission Statement and Goals Community Assessment Priority IdentificationFormal Problem Analysis for at least one priority problem
Components of the Community AssessmentCommunity health profile Community resource assessmentMCH agency capacity assessmentAnalysis of data on state required Title V indicators and other LHJ selected indicatorsIdentification of problems/assets/unmet needs
FHOP Community Assessment 1 October 2003 3

Resources for the Community Assessment Process
“Developing an Effective Planning Process: A Guide for Local Health Programs 2nd
Edition” on FHOP web siteFHOP and MCH Epi identifying or developing most of the data that local programs will needFHOP posting data or data links as they are prepared/identified on web siteFHOP to send e- newsletter or data alert for new or updated data
REMEMBER the PROGRAM PLANNING CYCLE
ConveneCommunity
Coalition
Assess Community Needs,Assets andResources
Prioritize HealthProblems
Analyze Problems /Develop of Objectives and
Performance Measures
DevelopInterventions
Implement Program/Plan Evaluation
Evaluate Program
Today’s Training Objectives
1. Articulate the steps of a community assessment process
2. Develop a community health profile3. Assess the adequacy of community
MCH related resources
FHOP Community Assessment 1 October 2003 4

Training Objectives (cont)
4. Assess MCH agency capacity5. Measure and assess required Title
V indicators6. Identify the advantages and
disadvantages of qualitative and quantitative data
Today’s AgendaReview of state MCH requirements for 2004 community assessmentDeveloping a Community Health ProfileConducting a Community Resource AssessmentAssessing MCH Agency CapacityAssessing Required MCH and County Selected IndicatorsOptions for Collecting and Presenting Indicator Data
FHOP Community Assessment 1 October 2003 5

COMMUNITY ASSESSMENT 1: BASIC CONCEPTS
Session One
Community Health Profile and Community Capacity Assessment
Presented by:
Nadia Thind, MPH Research Associate
Family Health Outcomes Project

PARTICIPANTS GUIDE
Session Two Community Health Profile and
Community Resources Assessment
LEARNING OBJECTIVES: By the end of the presentation and session, participants will be able to name the components of a community health assessment and:
1. Develop a community health profile 2. Assess the adequacy of MCH community resources
REFERENCES FOR THIS SESSION
1. Developing an Effective Planning Process: A Guide to Local MCH Programs, Chapter 2 “Community Health Assessment: Identifying Maternal, Child Health Needs and Setting Priorities,” Component 1. Compile the Community Health Profile and Component 2. Assess Capacity to Address Health Issues and Appendices II-A and II-B. 2nd edition, 2003
SESSION This session consists of a lecture/slide show presentation. The presentation will include an interactive discussion of the process of developing and finding data for a community health profile. Participants will be asked to discuss how they will develop their community health profile in their programs, using several websites for the profile.
FHOP Community Assessment 1 October 2003 7

Community Health Profile and Community
Resources Assessment
Nadia Thind, MPHFamily Health Outcomes Project
October 8, 2003
Session Objectives
By the end of this session, participants will be able to:
Develop a community health profileSelect appropriate resources for a community health profile
What Does a Community Health Assessment Tell Us?
Overall health status of the populationPopulation’s health problems/ needsPopulation(s) at highest risk for health problemsCommunity’s strengths or assetsResources that are available in the community
FHOP Community Assessment 1 October 2003 8

Community Health Assessment Components
1. Develop a community health profile
2. Assess capacity to address health issues
3. Assess required MCH Indicators / other locally relevant MCH Indicators
4. Collect, analyze, and present the data
5. Identify problems and set priorities
Community Health Profile
- A description of the overall community
- Gives the reader a picture of the quality of life in the community
- In order to describe the health of a community, public health indicatorsmust be used
Public Health Indicators
Definition:Precisely defined, standardized, quantifiable measures of a population’s health risks, health status, or health service utilization
FHOP Community Assessment 1 October 2003 9

Use of Public Health Indicators
Public health agencies use indicators to:- Describe the population’s demographic
characteristics- Describe the health status of the population- Identify unmet health needs- Describe the health delivery system in a
community- Identify areas of service deficiency
A Community Health Profile Contains:
Description of geographic features of the health jurisdictionSummary of relevant data including population, family structures, educational status, income and employment statusCommunicable disease ratesDescription of economic factors
A Community Health Profile Contains:
Highlights from vital records including fertility and birth rates, death rates and causes of deathAvailability of affordable housing and jobsMajor health issues- food safety, bioterrorism, environmental factorsImmigration trends
FHOP Community Assessment 1 October 2003 10

Community Assets Assessment
Some community characteristics and resources are associated with greater well being of residents and include:- Number of libraries- Playgrounds - Health care facilities- Schools with after school programs
Readily Available Data for a Community Health Profile
See Appendix II-B of the Planning Guide (in your binder)
FHOP Website-http://www.ucsf.edu/fhop
Geographic features-http://www.wikipedia.org/wiki/List_of_California_counties or County websiteU.S. Census site-http://quickfacts.census.gov/qfd/states/06000.htmlVital Records-http://www.dhs.cahwnet.gov/chs/OHIR/vssdata/tables.htm
Readily Available Data for a Community Health Profile
FHOP Community Assessment 1 October 2003 11

Communicable Disease Rates-http://www.dhs.ca.gov/ps/dcdc/STD/stddatasummaries.htm and http://www.dhs.ca.gov/ps/dcdc/STD/areports.htmAffordable Housing and Employment-http://www.calmis.ca.gov/htmlfile/subject/lftable.htm
Readily Available Data for a Community Health Profile
Trends in School Enrollment-http://data1.cde.ca.gov/dataquest/Economic Factors-http://www.dof.ca.gov/HTML/FS_DATA/profiles/pf_home.htmOther Major Health Issues-http://www.dhs.cahwnet.gov/ps/ddwem/environmental/epo/EPOBioterrorism.html and http://www.pepps.fsu.edu/epic/
Readily Available Data for a Community Health Profile
Political Issues- refer to your county’s websiteImmigration Trends-http://www.dof.ca.gov/HTML/DEMOGRAP/repndat.htm#immigration and http://eire.census.gov/popest/data/counties.phpHealth Systems- http://www.chis.ucla.edu/ and http://www.healthpolicy.ucla.edu/pubs/publication.asp?pubID=34
Readily Available Data for a Community Health Profile
FHOP Community Assessment 1 October 2003 12

Developing a Community Profile
and Finding the Appropriate Resources
Mini-Exercise
Capacity to Address Health IssuesCommunity Resources Assessment
Every profile should contain information on the capacity of its health care and social services system to meet the needs of its populationIdentify and describe both strengths and gaps in services (access to healthcare, cultural acceptability, availability of specialty care providers)
Capacity to Address Health IssuesCommunity Resources Assessment
Networks, coalitions, and collaboratives that impact theMCH population should also be described
Organize the information into tables, charts or maps http://www.oshpd.cahwnet.gov/HQAD/HIRC/Perspectives/Standard_Pages/county_icons1.htm
FHOP Community Assessment 1 October 2003 13

Family Health Outcomes Project Overview
Provides website links for various indicator data, including:- Population and SES- Economics- Health Services- Educationwww.ucsf.edu/fhop
FHOP Community Assessment 1 October 2003 14

Help is Here!!! www.ucsf.edu/fhop
TrainingsTechnical AssistancePlanning GuideAutomated Tools- EpiBC, EpiInfo, EpiHOSP, Data Templates (perinatal, domestic violence, injuries, maternal/infant screening)
FHOP Community Assessment 1 October 2003 15

COMMUNITY HEALTH PROFILE SOURCES
Source What's There?Geographic/ Demographic Features http://www.wikipedia.org/wiki/List_of_California_counties Land area, Population, Income
County website Geographic description
nhttp://quickfacts.census.gov/qfd/states/06000.html (U.S. Census)
Population, Race/ethnicity break-down, Household info, Education info, Business info
Vital Records http://www.dhs.cahwnet.gov/chs/OHIR/vssdata/tables.htmFertility and birth rates, death rates, causes of death
Communicable Diseases http://www.dhs.ca.gov/ps/dcdc/STD/stddatasummaries.htm STD cases and ratesAffordable Housing and Employment http://www.calmis.ca.gov/htmlfile/subject/lftable.htm Unemployment, workforce
http://www.dof.ca.gov/HTML/FS_DATA/profiles/pf_home.htm Housing info, home prices
School enrollment nhttp://data1.cde.ca.gov/dataquest/ Enrollment trends, Graduation, test results
Economic Factors http://www.dof.ca.gov/HTML/FS_DATA/profiles/pf_home.htmBusiness establishments, Income, Sales, Manufacturing, Agriculture
Other Major Health Issues http://www.dhs.cahwnet.gov/ps/ddwem/environmental/epo/EPOBioterrorism.html Bioterrorism, SARS, Smallpox
nhttp://www.pepps.fsu.edu/epic/ Environmental factors
Political Issues County website Updates on local political issues
Immigration Trends http://www.dof.ca.gov/HTML/DEMOGRAP/repndat.htm#immigration Legal immigration
nhttp://eire.census.gov/popest/data/counties.php Migration trends
Health Systems http://www.chis.ucla.edu/ *Need to register
Health insurance info, access and utilization, public program participation
http://www.healthpolicy.ucla.edu/pubs/publication.asp?pubID=34 Uninsured by Assembly and Senate districts
FHOP Community Assessment 1 October 2003 16

Alameda County MCAH Program Five Year Plan
I. Community Health Profile
A. Alameda County Profile
A.1 Geographic Features: Alameda County is located on the eastern side of San Francisco Bayextending from the urban northern region of the county, Berkeley and Albany, south to Fremont andthen east to the more sparsely populated communities in the Livermore valley. The countyencompasses a land area of 737.5 square miles, bounded on the north by Contra Costa County, on thesouth by Santa Clara County, on the southeast by Stanislaus County, on the east by San JoaquinCounty and on the west by the San Francisco Bay. The county has a varied geography, with woodedhills, vineyards, streams, and lakes. Elevations in Alameda County range from sea level to 3,817 ft.at Rose Peak in the southern part of the county. It is a highly industrialized county; an overwhelmingmajority (98%) of Alameda County residents live in urban or suburban areas, with only 2% residingin rural areas.
A.2 Population Demographics1: With an estimated population of 1,349,500, Alameda County is theseventh most populous county in California, and is honored to be one of the most ethnically diverseregions in the country. From 1990 to 1998, Alameda County has grown by 5.2%. The proportion offamilies has grown by 3.3%, about half the growth rate of California, 7.6%. In 1998, AlamedaCounty’s population is evenly divided by gender, with 50.7% females and 49.3% males. More thanhalf of the population is comprised of minority groups, with approximately one fifth each of Asians,Hispanics and African Americans. In terms of marital status, 48.9% of the residents are married,31.8% have never been married, and 18.9% are divorced, separated or widowed.
Table 1: Alameda County Population Demographics – 1998 Age (years) Race/ Ethnicity Gender
No. (%) No. (%) No. (%)
0-4 95516 (6.53%) White 46.60% Female 685,041 (50.7%)
5-14 190449 (13.0%) African-American 17.00% Male 664,498 (49.3%)
10-14 115082 (7.87%) Hispanic 17.90%
15-24 161919 (11.06%) Asian* 17.90%
25-34 215890 (14.76%) American-Indian 0.40%
35-44 246253 (16.84%) Other 0.30%
45-54 178257 (12.19%)
55-64 107107 (7.32%)
65-74 80538 (5.51%)
75-84 51257 (3.50%)
85+ 20439 (1.40%)
The proportion of women of childbearing age (15 to 44 years) of the total population in the county is23.5% in 1998. Alameda County has the seventh largest population of children in the State, with 25%of county residents under the age of 18 years. In 1990, the median age of Alameda County residents
1 1990 Census, Department of Finance; 1998 Claritas
FHOP Community Assessment 1 October 2003 17

Alameda County MCAH Program Five Year Plan
was 32.7 years. Children less than 5 years old account for 7.5% of the population, and young peoplebetween 6 and 20 years of age were 26.5%. From 1990 to 1998, considerable growth has beenobserved in elementary (15.2%) and middle school (20.3%) children, and among adults in their fortiesand fifties (30%).
The proportion of people living in poverty decreased slightly in Alameda County between 1993 to1995 from 12.3% to 11.3%, and the proportion of children under 18 years living in poverty decreasedfrom 18.5% to 17.3%.
A.3 Social-Economic Status: Alameda County has a bimodal income distribution – a large number ofpoor people, and a large number of wealthy people. Using 1998 Claritas, it is estimated that abouthalf of the county’s households earn less than $50,000 a year and approximately half earn more. The1990 Census reports that average annual income per person for residents of the county were $17,546.The median income of the county residents was $45,037.
The unemployment rate for Alameda County has remained below than that for California as a wholefor the entire decade, decreasing steadily from 6.6% in 1993 to 4.1% in 1998. The most recentfigures for Alameda County show an unemployment rate for February 1999 of 3.8%.2
A.4 Education Status: Alameda County residents have higher levels of education than do otherCalifornians. 81% of the county’s population aged 25 and over has graduated from high school. In1996-97, the overall graduation rate from Alameda County public schools was 66.0%. Although highschool dropout rates for the county are declining for all race/ethnic groups, they vary considerably byschool districts. For students in grades 9-12 during the 1993-94 school year, Oakland School Districthad the highest dropout rate (8.0%), followed by Hayward (5.7%). The overall dropout rate forAlameda County was 3.9%.3
A.5 Migration Trends :4 From 1990 to 1992, there were more people moving into the county thanleaving, but from 1993 to 1995, there were more people leaving, and since 1996 there has been a net
2 California Employment Development Department Website3 Alameda County Office of Education, 1994.4 California Department of Finance, Demographic Research Unit
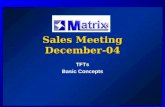
F i g u r e 1 . N e t m i g r a t i o n o v e r t i m e b y R a c e / E t h n i c i t y ,
A l a m e d a C o u n t y 1 9 9 0 - 1 9 9 6
- 1 2 , 0 0 0
- 1 0 , 0 0 0
- 8 , 0 0 0
- 6 , 0 0 0
- 4 , 0 0 0
- 2 , 0 0 0
0
2 , 0 0 0
4 , 0 0 0
6 , 0 0 0
8 , 0 0 0
1 0 , 0 0 0
1 9 9 0 1 9 9 1 1 9 9 2 1 9 9 3 1 9 9 4 1 9 9 5 1 9 9 6
Y e a r
Net
Num
ber
of M
igra
nts
W h i t e H i s p a n i c A s i a n / P I A f r i c a n - A m e r i c a n N a t i v e A m e r i c a n T o t a l
S o u r c e : C a l i f o r n i a D e p a r t m e n t o f F i n a n c e , D e m o g r a p h i c R e s e a r c h U n i t
FHOP Community Assessment 1 October 2003 18

Alameda County MCAH Program Five Year Plan
increase in the number of people moving into the county. During the period between 1990 to 1996,four to seven thousand Whites migrated out of the county annually. In contrast, thousands of variousethnic populations (especially Asians/Pacific Islanders) migrated into the county each year, andcontributed to the increase in the county’s population.
A.6 Racial/Ethnic Composition and Shift:
Racial/Ethnic Composition: Alameda County is honored to be one of the most ethnically diverseregions in the country, with at least 81 different languages spoken in the communities. The richnessand uniqueness of ethnic diversity and immigrant culture are valuable assets for the community.They also pose a challenge for Public Health professionals as they seek to develop a variety ofstrategies necessary to provide services that are culturally and linguistically competent.
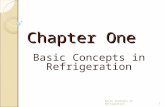
Racial/Ethnic Population Shift: The county continues to be a magnet for immigrants. Alameda Countyhas experienced significant demographic shifts in the last decade. In 1998, 46.6% of AlamedaCounty was Whites, decreasing from 61.6% in 1980; 17% African American, compared to 18.2% in1980; 18.6% Asian/Other, increasing significantly from 7.6% in 1980, and 17.9% Hispanic,compared to 11.7% in 1980. There were notable differences in rates of growth of the population byrace/ethnicity. The Asian population has been the fastest growing segment of the population (32.6%increase since 1990), followed by Hispanics (30.2% increase since 1990). The African Americanpopulation has stayed relatively stable in the 1990s, while the proportion of the White population hasdecreased by 24%.
A.7 Vital Statistics: The total number of births has been steadily declining in the county since 1990. In1996, the crude birth rate was 15.1 per 1,000 people and the general fertility rate was 66.3 births per1,000 women of childbearing age. In 1997, Alameda County recorded 20,761 live births, with Medi-Cal paying for 32.1% of these deliveries. The crude death rate was 7.1 per 1,000 people. There were6 infant deaths (under 1 year of age) per 1,000 live births, 3.5 per 1,000 births in the neonatal period(less than 28 days) and 2.6 per 1,000 in the post-neonatal period (28 days up to 1 year). There were6.1 fetal deaths per 1,000 live births plus fetal deaths. (See table 2)
F i g u r e 2 . R a c i a l / E t h n i c C o m p o s i t i o n S h i f t f r o m 1 9 8 0 t o 1 9 9 8A l a m e d a C o u n t y
6 1 . 6 %
1 8 . 2 %
7 . 6 %1 1 . 7 %
5 3 . 2 %
1 5 . 1 % 1 4 . 2 %1 7 . 9 %1 7 . 4 % 1 8 . 6 %
4 6 . 6 %
1 7 . 0 %
0 %
1 0 %
2 0 %
3 0 %
4 0 %
5 0 %
6 0 %
7 0 %
W h i t e A f r i c a n - A m e r i c a n A s i a n / O t h e r H i s p a n i c
Pe
rce
nt
ch
an
ge
in
po
pu
lati
on
1 9 8 0
1 9 9 0
1 9 9 8
D a t a s o u r c e : 1 9 9 0 C e n s u s , D e p a r t m e n t o f F i n a n c e
FHOP Community Assessment 1 October 2003 19

Alameda County MCAH Program Five Year Plan
Table 2: Population Distribution, Birth Distribution, Crude Birth rate and General FertilityRate by Race/ Ethnicity, California and Alameda County, 1996
AlamedaPopulation
California Births Alameda Births Crude BirthRate
General FertilityRate
CA Alameda CA AlamedaRace/ Ethnicity No. % No. % No. % per 1000 population per 1000 women aged 15-
45Non-Hispanic White 654,915 47.98 185,441 34.38 7,038 34.03 10.82 10.75 50.92 50.25
Hispanic White 21,7719 15.95 253,875 47.07 5,221 25.24 27.21 23.98 118.95 102.37
African-American 24,1363 17.68 38,001 7.05 3,715 17.96 16.70 15.39 69.51 63.07
American Indian 6,683 0.49 2,694 0.50 96 0.46 13.92 14.36 57.34 57.49
South East Asian 26,024 1.91 10,596 1.96 593 2.87 21.39 22.79 88.10 92.45
Other Asian 141,051 10.33 24,265 4.50 1,799 8.70 12.49 12.75 51.44 51.74
All other 77,286 5.66 22,667 4.20 1,984 9.59 22.34 25.67 91.98 104.15
Total 1,365,041 100.00 539,360 100.00 20,682 100.00 16.66 15.15 74.82 66.32
Source: Maternal and Infant Health Profile for Alameda County, University of California Berkeleyhttp://datamch.berkeley.edu/ipodm/cprs1997/poo1.htm
FHOP Community Assessment 1 October 2003 20

FHOP Community Assessment 1 October 2003 21
Working off the previous 5-year plan and the suggestions FHOP has made to update the profile and assessment, FHOP has created summary statements for a community health profile and community resources assessment. Please refer to Alameda County’s 1999 Community Health and Health Services Systems included earlier in this binder. The supporting data, graphics and/or maps should have been included in the profile and community resources assessment, in the future. Community Health Profile Summary The following are the major findings from the Community Health Profile for Alameda County, and need to be considered when identifying and responding to health problems.
• Alameda County is the seventh most populous county in California and growing, although at a rate lower than the State. It is a highly industrialized county with 98% of the population living in urban or suburban areas
• Has the largest population of children in the state with 25% of residents under the age of 18 years
• Is ethnically diverse, with at least 81 different languages spoken in the communities
• Over the past decade, there has been a significant demographic shift from 62% white in 1980 to 47% white in 1998, 17% African American compared to 18.6% in 1980. The growth in population has occurred amongst Hispanics who constitute 18% of the population (30.2% increase since 1990) and the Asian population (32.65 increase since 1990)
• The population is economically diverse with a large number of poor people and a large number of wealthy people. In 1997, approximately 1/3 of the 20,761 live birth deliveries in the county were paid for by Medi-Cal.
• County residents have a higher level of education than do other Californians, 81% of the county’s population, aged 25 and over has graduated from high school.
• The county has implemented the “Mobilization for Action through Planning and Partnership (MAPP)” planning process, which shows the county has strong assets in community organizing capacity, churches, etc. (added as an example of how the significant findings from an Assets Assessment might be included)
• The total number of births has been steadily declining in the county since 1990. In 1996, the crude birth rate was 15.1 per 1,000 people and the general fertility rate was 66.3 births per 1,000 women of childbearing age.
Community Resources Assessment Summary The following are the major findings from the Community Resources Assessment for 1999 :
• Alameda County has 13 not-for-profit and for-profit hospitals. The major sources of OB delivery for low-income women are Summit and Highland Hospitals in Oakland and Alta Bates Hospital in Berkeley where the highest concentration of low-income individuals live (as shown on Map ___)

FHOP Community Assessment 1 October 2003 22
• It has 2 Medi-Cal managed care plans: the county-operated Alameda Alliance for Health and the Private Blue Cross Medi-Cal managed Care plan. Providers of care to low income women are providers in both plans. (Map ___ shows the concentration of providers who 1) accept Medi-Cal or 2) are Healthy Families providers or 3) have sliding scale services to be located in the ____________neighborhoods. (hypothetical) (If Alameda County had included information in their profile about where the providers are located, in relation to need of the population, they should have drawn some conclusions about the accessibility of providers
• There are 394 persons per physician. In addition, there are 1,153 persons per dentist. In California, there are 400 persons per physician and 1,257 persons per dentist. This shows that Alameda County is providing has about the same ratio of providers to population as the State.(See Health Data Summaries for California Counties 2002)
• The county has implemented the “MAPP” planning process, which shows gaps in services in the following areas: (hypothetical)
o Staff that speak the appropriate languages for the population served o Lack of choice of providers for patients o Lack of transportation services is a problem for respondents in all towns,
but especially for those living in the rural towns.

COMMUNITY ASSESSMENT 1: BASIC CONCEPTS
Session Two
MCH Program Capacity Assessment
Presented by:
Judith A. Hager Belfiori, MA, MPH Director of Planning and Evaluation
Family Health Outcomes Project

PARTICIPANTS GUIDE
Session Two Assessing MCH Program Capacity
LEARNING OBJECTIVES By the end of the presentation and session, participants will be able to describe how to conduct an MCH capacity assessment including:
1. Define MCH capacity 2. Describe the purpose of the assessment 3. Describe how to use an assessment tool to assess MCH capacities 4. Describe possible MCH capacity assessment processes 5. List what should be included in the “Assessment of MCH Capacity” section of the
Title V 5 year MCH Needs Assessment Report REFERENCES FOR THIS SESSION
1. Developing an Effective Planning Process: A Guide to Local MCH Programs, Chapter 2 “Community Health Assessment: Identifying Maternal, Child Health Needs and Setting Priorities,” Component 2. Assess Capacity to Address Health Issues. 2nd edition, 2003
2. California MCH Five Year Needs Assessment Guidelines & Indicator List for MCAH Jurisdictions, August 2003
SESSION This session consists of a lecture/slide show presentation titled “MCH Program Capacity Assessment.” The presentation will include an interactive discussion of the process for assessing capacities and the use of a rating tool. Participants will be asked to discuss how they might conduct this assessment in their programs.
FHOP Community Assessment 1 October 2003 41

MCH Program CapacityAssessment
Judith A. Hager Belfiori, MA, MPH
Family Health Outcomes Project
October 8, 2003
Objectives for this Session
Par t i c ipan ts w i l l be ab le t o conduc t and
r e p o r t o n a n a s s e s s m e n t o f t h e i r l o c a l
M C H P r o g r a m c a p a c i t y :
ØP u r p o s e
ØR e v i e w c a p a c i t i e s / c o r e f u n c t i o n s
ØT o o l s
ØP r o c e s s
ØR e p o r t
MCH Capacity
Abi l i ty to C a r r y O u t
i t s Func t i ons t o
P r o m o t e a n d
Pro tec t t he Hea l th
o f M o t h e r s a n d
Ch i l d ren
++A ++
FHOP Community Assessment 1 October 2003 42

Purpose of Capacity Assessment
Ø Se l f -e x a m i n a t i o n ( P r o g r a m )
Ø Ass i s t p r i o r i t i za t i on o f p rob lems to be
a d d r e s s e d
Ø I n f o r m p l a n n i n g g r o u p s o f c a p a c i t y /
r e s o u r c e s
Ø D e v e l o p f u t u r e s t r a t e g i e s
Ø I n f o r m a t i o n f o r S t a t e ’ s a s s e s s m e n t
State’s Interests
l Coordinat ion on the
local level
l E m e r g i n g i s s u e s
l Ongo ing i s sues
Who Performs the Assessment?
l In terna l to MCH
(representative staff / key partners)
FHOP Community Assessment 1 October 2003 43

W h e r e D o e s i t F i t i n t o t h e T i t l e V 5
Y e a r A s s e s s m e n t P r o c e s s ?
Health Status Prof i le
Community ResourceAssessmen t
MCH Capac i t y
A s s e s s m e n t
Required Indicator Assessment
Community Selected Indicator Assessment
Prob lem
Ident i f icat ion,
Priori t izat ion,
Ana l ys i s
Part I. Assessment of MCH Capacity
• O r g a n i z a t i o n a l r e l a t i o n s h i p s
- - W i th in pub l i c hea l th
- - W i t h i n M C H
• R e s o u r c e s ( f u n d s , s t a f f , o t h e r )
• C u l t u r a l c o m p e t e n c y
• C o r e f u n c t i o n s
Core MCH Program Functions
F o r t h e M C H p o p u l a t i o n : (Re fer to handout )
Moni to r hea l th s ta tus
D i a g n o s e & I n v e s t i g a t e c o m m u n i t y p r o b l e m s
I n f o r m , E d u c a t e , E m p o w e r peop le
M o b i l i z e c o m m u n i t y pa r t ne r sh ips
FHOP Community Assessment 1 October 2003 44

Core Functions (more)
Deve lop po l i c i es and p lans
L i n k p e o p l e t o s e r v i c e s
Eva lua te e f f e c t i v eness ,
a ccess and qua l i t y o f p o p- b a s e d s e r v i c e s
Resea rch f o r i n s i gh t s /
so lu t i ons
Part II of the Assessment:
• I s sues i n pub l i c and p r i v a t e hea l t h ca re wh ich a re a f f ec t ing the ro le / capac i t y o f M C H ( e m e r g i n g , o n g o i n g )
• L o c a l c o l l a b o r a t i o n s ( c o n v e n e d b y M C H / in wh ich MCH par t i c ipa tes )
• ( I f appl ies) Par t ic ipat ion in / Impact o f a n y r e s e a r c h e f f o r t s
Capacity Assessment Tools
ØR e c o m m e n d e d t o o l
ØE x i s t i n g a s s e s s m e n t s
FHOP Community Assessment 1 October 2003 45

Let’s see how it works
Re lax , i t s easy
M C H C a p a c i t y R a t i n g a n d R e p o r t i n g T o o l
Par t I : Capac i t y Assessment
Summary of Challenges
1.
2.
Summary of Opportunities
1.
2.
Summary of Opportunities
1.
2.
Summary of Challenges
1.
13
13
Circle
24Organ iza t iona l re la t ionsh ips
24C u l t u r a l c o m p e t e n c y
S t r o n g WeakA s s e s s M C H c a p a c i t y i n e a c h o f
t h e a r e a s b e l o w
2 .
1 .
Summar i ze membersh ipList Col laborat ives / Networks in
which MCH par t ic ipates
2 .
1 .
2 .
1 .
Par t I I : Capac i ty Assessment
1
2 .
How MCH responded / its role / challenges
Lis t emerging issues a f fect ing MCH
M e m b e r s h i pList Col laborat ives / Networks c o n v e n e d b y M C H
How MCH responded / its role / challenges
L is t ongo ing i ssues a f fec t ing MCH
M C H C a p a c i t y R a t i n g a n d R e p o r t i n g T o o l
FHOP Community Assessment 1 October 2003 46

Assessment Process
l D e c i d e w h o s h o u l d p a r t i c i p a t e
l D i s c u s s a n d i n t r o d u c e p u r p o s e / f r a m e w o r k
l A s s e s s c a p a c i t i e s -- u s e w o r k s h e e t o r o t h e r
m e t h o d
l C o m p l e t e c a p a c i t y a s s e s s m e n t r a t i n g &
r e p o r t i n g t o o l
l S u m m a r i z e f o r r e p o r t / p l a n n i n g g r o u p
l Compare t o needs / ( l a t e r )
What belongs in the report?
Ø S u m m a r y o f a s s e s s m e n t p r o c e s s / m e t h o d s ( 1 ¶)
Ø S u m m a r y o f c o n c l u s i o n s a b o u t M C H c a p a c i t y ( c o n c i s e , i n c l u d e a s s e s s m e n t t o o l , M C H a n d D e p a r t m e n t o r g a n i z a t i o n c h a r t s )
Ø a ) A l i s t o f i ssues in pub l i c and p r i va te hea l t h ca re a f f ec t i ng MCH (÷ i n t o emerg ing / o n g o i n g ) a n d
b ) A s u m m a r y o f i m p a c t o n M C H a n d i t s r e s p o n s e
What belongs in the report?
Ø a ) A l i s t o f co l l abora t i ves , ne tworks i n w h i c h M C H p l a y s a r o l e ( ÷ i n t o t h o s e c o n v e n e d b y M C H a n d t h o s e i n w h i c h MCH pa r t i c i pa tes ) ,
b ) m e m b e r s h i p
Ø ( I f applies) A b r i e f s u m m a r y o f a n y r e s e a r c h a c t i v i t i e s M C H h a s b e e n i n v o l v e d i n a n d h o w t h e f i n d i n g s h a v e b e e n u s e d
FHOP Community Assessment 1 October 2003 47

ASSESSING LOCAL MCH PROGRAM CAPACITIES TITLE V FIVE YEAR NEEDS ASSESSMENT
Supplement to the MCH Capacity Rating and Reporting Tool and the Assessment Worksheets
Part I. Capacity Assessment. Assess and rate MCH program capacity on a scale of 4 to 1 (strong capacity to weak capacity) and identify opportunities and challenges in each of the following areas. A. Organizational Relationships Consider
• MCH participation in the leadership and overall strategic planning of the public health department
• relative authority / organizational influence within the department B. Adequacy of Cultural Competency Consider capacity to
• assess cultural needs • respond (within MCH and amongst partners / coalitions) to identified needs
C. Adequacy of MCH Resources Consider
• allocated program funding • ability to generate grants and other funding • adequacy of staffing and appropriate education / training of staff in relation to
responsibilities D/E Other MCH Capacities (Optional) Core Function #1: Monitor Health Status to Identify MCH Health Problems Consider capacity to
• accurately, periodically select and review indicators to assess community / maternal and child health status including adequacy of MIS and data collection capabilities
• utilize appropriate methods and technology, such as indicator data, geographic mapping, etc.
• collaborate with private providers, health plans, other departments to collect data Core Function #2: Diagnose and Investigate MCH Health Problems in the Community Consider capacity to
• analyze data – have expertise and understanding of how to manipulate the data to answer questions about it
• access expertise in epidemiology to investigate and look for causes and solutions • respond to emerging problems • coordinate with other county health and social service agencies and community
based agencies to diagnose and investigate these problems

ASSESSING LOCAL MCH PROGRAM CAPACITIES TITLE V FIVE YEAR NEEDS ASSESSMENT
Core Function #3: Inform, Educate and Empower People about MCH Health Issues Consider capacity to develop and implement:
• health Information, health education and health promotion activities designed to reduce health risk and promote better health
• health communication plans and activities appropriate to your communities, e.g., media advocacy, social marketing, community health workers
• accessible health information and education resources • health education and promotion program partnerships with schools, faith
communities, worksites, etc, to reinforce MCH health promotion programs and messages
Core Function #4: Mobilize Community Partnerships to Identify and Solve MCH Problems Consider capacity to
• identify and involve potential stakeholders • build networks, coalitions and collaborations to address MCH issues • convene, coordinate and facilitate partnerships among groups and associations
to undertake defined MCH programs / activities Core Function #5: Develop Policies and Plans that Support Individual and Community Health Efforts Consider capacity to
• develop and implement internal Departmental policies affecting the health/health care of women and children
• work with other agencies, CBOs, service providers, advocacy groups and others to develop plans and improve policies which affect health status and access to and quality of health services for women and children
• access and inform/educate local and state policy makers
Core Function #6: Link Women and Children to Needed Health Services and Assure the Provision of Health Care to the MCH population when Otherwise Unavailable Consider capacity to
• identify barriers to women’s and children’s health services and work with the public and private sectors to develop interventions to address barriers, e.g., culturally and linguistically appropriate staff and materials, transportation services, etc.
• connect women and children to health care including outreach, advocacy and linking to services, providing case management, linking to a source of insurance, etc.
• provide direct MCH health care services as needed in your county; e.g., family planning, school based services, immunizations, etc.

ASSESSING LOCAL MCH PROGRAM CAPACITIES TITLE V FIVE YEAR NEEDS ASSESSMENT
Core Function #7: Evaluate Effectiveness, Accessibility, and Quality of Personal and Population–Based Health Services Consider capacity to:
• conduct evaluation of MCH programs at the basic level of monitoring program process measures and monitoring program outcomes
• assist health care providers and plans to evaluate their MCH related services and programs
Core Function #8: Research for New Insights and Innovative Solutions to Health Problems Consider capacity to
• link to Universities, access researchers with knowledge and skill to design and conduct health-related studies
• participate in research projects such as those funded by CDC, HRSA, which contribute to health policy and improved health services, etc.
______________________________________________________________________ Part II. Capacity Assessment. Provide summary information for the following: Emerging issues/policies in the public or private health care sectors (or related sectors) that impact the local MCH program. List the emerging significant issues that impact or are anticipated to impact the role of the local MCH program in the community, its functions and/or its capacity to perform its functions. Briefly indicate in what ways the issue(s) are being addressed by MCH. Ongoing issues/policies in the public or private health care sectors (or related sectors) that impact the local MCH program. List the ongoing issues that affect MCH program capacity to perform its roles and functions. Briefly indicate in what ways the issue(s) are being addressed by MCH. Collaboratives/ Networks/ Partnerships. List the collaboratives, networks and partnerships that have 1) been convened by MCH and 2) in which MCH participates. If the focus of the collaborative or network is not obvious by its title, provide the focus. For the major MCH convened planning group(s) provide a full description of membership or include in an appendix. For others, summarize membership categories, e.g., child advocates, social services representatives, health plan representative, etc. (If Applies) Research activities and results. If your program is conducting or has conducted any MCH population research or health care service delivery research, briefly describe the area of research, any results and how the findings have been used by MCH or others to increase capacity or improve services.

MCH Capacity Rating and Reporting Tool
For assistance in using this form, see “Supplement/Guidance to Assist Use of the MCH Capacity Rating and Reporting Tool and the Assessment Worksheets”
Part I. Capacity Assessment
Assess MCH capacity in each of the areas below:
Rate capacity in each area by checking a number: 4 = strong, 3 = adequate 2 = inadequate, 1= weak Strong Weak
A. Organizational relationship within Health Department
Summary of Opportunities Summary of Challenges
B. Cultural competency
Summary of Opportunities Summary of Challenges
C. Resources
Summary of Opportunities Summary of Challenges
D. Coordination/Collaboration with other Agencies/CBOs
Summary of Opportunities Summary of Challenges
E. Other
Summary of Opportunities Summary of Challenges
3 2 14
3 2 14
3 2 14
3 2 14
3 2 14
FHOP10/30/03 1

MCH Capacity Rating and Reporting Tool
Core Public Health/ MCH Functions
Rate capacity in each area by checking a number: 4 = strong, 3 = adequate 2 = inadequate, 1= weak Strong Weak
1. Monitor health status
Summary of Opportunities Summary of Challenges
2. Diagnosis & investigate community problems
Summary of Opportunities Summary of Challenges
3. Inform, educate, empower people
Summary of Opportunities Summary of Challenges
4. Mobilize community partnerships
Summary of Opportunities Summary of Challenges
5. Develop policies and plans
Summary of Opportunities Summary of Challenges
4 13 2
4 3 12
4 3 12
4 3 12
4 3 12
FHOP10/30/03 2

MCH Capacity Rating and Reporting Tool
6. Link women and children to services
Summary of Opportunities Summary of Challenges 7. Evaluate effectiveness, access and quality of population
based services
Summary of Opportunities Summary of Challenges
8. Research for insights/solutions
Summary of Opportunities Summary of Challenges
Part II. Capacity Assessment List emerging issues/policies in the public or private health care sectors that impact the local MCH program
Briefly describe MCH impact and response
1.
2.
3.
List ongoing issues/policies in the public or private health care sectors that impact the local MCH program
Briefly describe MCH impact and response
1.
2.
3.
3 2 14
3 2 14
3 2 14
FHOP10/30/03 3

MCH Capacity Rating and Reporting Tool
FHOP10/30/03 4
List Collaboratives /
Networks that MCH convenes
For its major planning body or bodies, provide a full description of membership or include
roster/representation in an appendix. For others, summarize membership categories, e.g., child
advocates, social services representatives, etc. 1.
2.
3.
4.
5.
6.
List Collaboratives / Networks in which MCH participates as a member.
Summarize membership (see above)
1.
2.
3.
4.
5.
(If applies) Briefly highlight any research activities MCH is involved in and how the findings have been used to increase MCH capacity or affect policies.
1.
2.

MCH Program Capacity Assessment Worksheet For internal use as needed / Not to be included in Assessment Report
Area or Core Function: (List programs or activities if doing this as a group) Strengths: Weaknesses: Challenges: Opportunities:

COMMUNITY ASSESSMENT 1: BASIC CONCEPTS
Session Three
Measuring and Assessing Required Title V Indicators
Presented by:
Brianna Gass, MPH MCH Project Coordinator
Family Health Outcomes Project

PARTICIPANTS GUIDE
Session Three Measuring and Assessing
Required Title V Indicators
LEARNING OBJECTIVES By the end of the presentation and session, participants will be able to collect and evaluate indicator data. Sub-objectives include:
1. Identify data resources and use to accurately calculate values for required indicators 2. Use FHOP data templates and other resources to evaluate indicator data 3. Identify problem areas based on the evaluation of selected indicators 4. Understand when and how to select additional indicators of local interest
REFERENCES FOR THIS SESSION
1. Developing an Effective Planning Process: A Guide to Local MCH Programs, Chapter 2, “Community Health Assessment: Identifying Maternal, Child Health Needs and Setting Priorities,” Component 4. Collect, Analyze and Present Data for the Selected Indicators and Appendices II-B, II-C, II-D, and II-E. 2nd Edition, 2003
2. FHOP Website www.ucsf.edu/fhop under California MCH Data 3. Data sources for Indicators 4. FHOP Data Templates and Instructions 5. FHOP Tool for Summarizing Title V Indicators
OTHER MATERIALS FOR THIS SESSION
1. FHOP Perinatal Spreadsheet for county and CA state 2. Data tables for selected indicators 3. Data template for selected indicators 4. County profile for prenatal section (UC Berkeley) 5. County background summary
FHOP Community Assessment 1 October 2003 57

EXERCISE Scenario: You are part of an MCH staff group assigned to collecting and analyzing the required indicators for the Title V Needs Assessment process. You are asked to review the indicators selected and to present your conclusions based upon the data available. You have also been asked to discuss the next steps for data collection and problem analysis based on your findings.
For each of the following health indicators: 1. Examine the data provided 2. Discuss with the group what the data is showing in general 3. Discuss with the group how the county is doing compared to the state,
applicable Healthy People 2010 Objectives, and other counties in California 4. Based on what is discussed, which indicators seem to pose the biggest
problem for the county and why? 5. What other information might be useful in further evaluating each of the
above indicators?
Prepare a brief summary of your findings and present to the larger group your rationale for identifying the indicators that pose a problem for your county, and the next steps in the process of analyzing the Title V Indicators. Indicators being assessed in this exercise:
1. Number of teen births by age group 2. First trimester entry into prenatal care 3. Number of preterm births 4. Percent of children in poverty
FHOP Community Assessment 1 October 2003 58

Measuring and Assessing Required Title V Indicators
Brianna Gass, MPHFamily Health Outcomes Project
October 8, 2003
Objectives for this SessionDefine the required indicators for your Title V AssessmentsIdentify resources for locating data for Title V IndicatorsUnderstand how to evaluate the data for each indicatorEffectively use FHOP data templates and indicator rating tools
MCH Indicators
Provide baseline dataUniformly defined for comparabilityAllow for problem identificationAllow for tracking of changes over timeFunction as a performance measure
FHOP Community Assessment 1 October 2003 59

Background of Required Indicators
What drove the CA MCH selection and decision process?Why were these indicators chosen and others eliminated?How does this set of indicators support the Title V Assessment process?
Title V Required Indicators: Selection Process
Federal Title V RequirementMCH Directors survey identified prioritiesAvailability of county-level data sourceState MCH program staff additions
What can CA MCH learn from the Indicator Assessment?Summary of county performances on each indicatorHow many counties’ values are significantly better or worse than the State?Which indicators were identified as priorities in which counties?Which indicators pose the most widespread problem?
FHOP Community Assessment 1 October 2003 60

27 Required Indicators!Data Resources on the WebVital recordsSurvey dataOther community and government agencies
FHOP ResourcesWeb site: www.ucsf.edu/fhopCounty-level tables and spreadsheets for indicatorsData TemplatesData evaluation toolsEpi BCTechnical Assistance
Data Sources on the Web
FHOP Website: www.ucsf.edu/fhop•Data tables and spreadsheets•Links to other sites with relevant data
Other websites (refer to handout)•CA DHS Center for Health Statistics•UC Berkeley MCH project•UCLA/California Health Interview Survey•CA EPIC Center- Injury Data
FHOP Community Assessment 1 October 2003 61

Now that you have data for each of the indicators….
What does it all mean?
Evaluating Indicator Data
California State Other countiesHealthy People 2010 ObjectivesOther areas of your Needs Assessment (e.g. Community Health Profile)Government surveys and reportsMCH Literature
FHOP Data TemplatesAllow you to enter county data into pre-designed spreadsheetDisplay the comparison between your county data, the State and Healthy People 2010 ObjectivesMay indicate a basic trend in your county, if one exists— “are things getting better or worse?”
FHOP Community Assessment 1 October 2003 62

FHOP Data Templates exist for these indicators:
Fertility rates/number of birthsNumber of teen births by age groupNumber and percent low birth weightNumber and percent very low birth weightNumber and percent prenatal care in first trimesterNumber and proportion of women with adequate prenatal careNeonatal deaths and death rate for <28 daysPost-neonatal deaths 28 days to a yearInfant deaths and death rate birth to one yearPercent of women exclusively breastfeeding at dischargeBlank Template for rates and percentages
FHOP Tool for Summarizing Indicators
Allow counties to see their assessments of required indicators in summary form:
List values for each indicatorsShow comparison to State and Healthy People ObjectivesSpecify priority indicatorsExplain how conclusions were drawn
Allows for comparability across counties
GROUP EXERCISE
Measuring and Assessing Required Indicators
FHOP Community Assessment 1 October 2003 63

Identifying and Selecting Additional Maternal Child
Health IndicatorsJudith A. Hager Belfiori, MA, MPHFamily Health Outcomes Project
October 8, 2003
Where does this process fit into the overall assessment process?
MCH Mission Statement & Goals
Community AssessmentCommunity health profileAssess community resourcesAssess MCH program capacity Assess State required MCH indicatorsSelect / assess locally determined MCH indicatorsIdentification of Problems/Unmet needs
Select priority MCH problems/needs in the jurisdiction
Preliminary problem analysis for priority problems
Why / When is it necessary?
If required indicators do not includethe indicators of local interest (e.g., perinatal substance use, riskyteen behaviors)
FHOP Community Assessment 1 October 2003 64

Setting the Stage to Identify and Select among additional (locally
determined) MCH Indicators
Use planning group(inclusive)
Review mission and overall goals
Use the process appropriate to your needs
Selecting Additional Indicators
•For some, no problem
For others, not an easy process
Process of Selecting Additional Indicators
Review required indicators and discuss other assessment needs
Agree on selection method and whether there is a need for a process
Brainstorm / review list of additional indicators
Agree on indicators to be used. If a process is needed, refer to FHOP Planning Guide
FHOP Community Assessment 1 October 2003 65

Identify Additional Indicators
Group identifies indicators under each MCHgoal. These are in addition to--do not replacethe required indicators.__________________________________________
ExampleGoal 1. All pregnant women give birth to a
healthy child% of women who smoke during pregnancy% of women with an identified substance abuseproblem at delivery of their baby% of women with gestational diabetes
Talk About:Criteria for selection
________________________________________Example Criteria
The indicator is :– quantifiable– Data is easily available (e.g., FHOP
website)– Reflects high impact on local MCH
population
Construction of Indicator
Staff work:Develop precise definitionDefine numerator and denominatorIdentify data sourcesIdentify a standard for comparison or a comparison group or time period
FHOP Community Assessment 1 October 2003 66

Agree on Indicators to be used
If a formal process is needed, refer to FHOP Planning Guide / TA
Confirm the results of the informal / formal process with the group
Document the results
FHOP Community Assessment 1 October 2003 67

Data sources for Title V Indicators Definition Numerator
Denominator Data Source
1 Number of births & fertility rates
Number of live births Total population
http://www.ucsf.edu/fhop/dataport/perinatal/ (FHOP will update with latest data when available) http://datamch.berkeley.edu/ccpr.html (also includes trend tables and data maps)
2 Number and teen birth rate per 1000 females
Number of births among age group Total population in age group
http://www.ucsf.edu/fhop/dataport/perinatal/ (FHOP will update with latest data when available) http://datamch.berkeley.edu/ccpr.html (by age; also includes trend tables and data maps)
3 Number andpercent low birth weight (live births)
Number of live infants born weighing less than 2500 grams Total number of live births
http://www.ucsf.edu/fhop/dataport/perinatal/ (FHOP will update with latest data when available) http://datamch.berkeley.edu/ccpr.html#select (also includes trend tables and data maps)
4 Number andpercent very low birth weight (live births)
Number of live infants born weighing less than 1500 grams Total number of live births
http://www.ucsf.edu/fhop/dataport/perinatal/ (FHOP will update with latest data when available) http://datamch.berkeley.edu/ccpr.html#select (also includes trend tables and data maps)
5 Number andpercent preterm births (less than 37 weeks gestation)
Number of live births occurring before 37 weeks Total number of live births
http://www.dhs.ca.gov/hisp/chs/OHIR/vssdata/2002data/02Ch2Ex/2_24_2002c.xls http://www.dhs.ca.gov/hisp/chs/OHIR/vssdata/2001data/01Ch2Ex/2_24_2001.xls http://www.dhs.ca.gov/hisp/chs/OHIR/vssdata/2000data/00Ch2Excel/2_37_2000.xls http://www.dhs.ca.gov/hisp/chs/OHIR/vssdata/1999data/99Ch2Excel/2-37-99vJC.xls http://www.dhs.ca.gov/hisp/chs/OHIR/vssdata/1998data/chapter2/2-37-1998.xls
6 Number andpercent of births occurring within 24 months of a previous birth
Number of births occurring within 24 months of previous birth Total number of
http://datamch.berkeley.edu/ccpr.html#select (within 23 months of previous birth; also includes trend tables and data maps) FHOP is also preparing age specific data for this indicator and will post to website.
FHOP Community Assessment 1 October 2003 68

(entire population and by age)
live births
7 Number andpercent of teen births to women who were already mothers
Number of repeat teen births Total number of teen births
FHOP is preparing data for this indicator and will post to website.
8 Perinatal deathrate
Number of fetal deaths after 20 weeks gestation Total live births + number of fetal deaths
http://datamch.berkeley.edu/ccpr.html (also includes trend tables and data maps) Links to excel tables are on FHOP website under CA MCH data
9 Neonatal deathsand death rate (birth - <28 days)
Number of infant deaths 0-28 days Total number of live births
http://www.ucsf.edu/fhop/dataport/perinatal/ (FHOP will update with latest data when available) http://datamch.berkeley.edu/ccpr.html (also includes trend tables and data maps)
10 Post-neonatal deaths and death rate (>28 days – 1 year)
Number of infant deaths 28 days-1 year Total number of live births
http://datamch.berkeley.edu/ccpr.html (also includes trend tables and data maps) Links to excel tables are on FHOP website under CA MCH data
11 Infant deaths and death rate (birth – 1 year)
Number of infant deaths birth-1 yr Total number of live births
http://www.ucsf.edu/fhop/dataport/perinatal/ (FHOP will update with latest data when available) http://datamch.berkeley.edu/ccpr.html (also includes trend tables and data maps)
12 Deaths and death rate per 100000 age 1-14 and age 15-19
Number of deaths in age group Total population in age group
FHOP is preparing these data and will post to website when available
13 Number and percent prenatal
Number of births to women who
http://www.ucsf.edu/fhop/dataport/perinatal/ (FHOP will update with latest data when available)
FHOP Community Assessment 1 October 2003 69

care in first trimester (live births)
received prenatal care during the first trimesterTotal number of live births
14 Number and proportion of women (age 15-44) with adequate prenatal care (Kotelchuck index)
Number of women who received adequate prenatal care Total number of live births
http://datamch.berkeley.edu/ccpr.html (also includes trend tables and data maps) FHOP is preparing data for this indicator and will post to website.
15 Percent of women who were breastfeeding at the time of hospital discharge
Number of women who breastfeed at time of discharge Total number of postpartum women
MCH Epidemiology section is preparing these data and will post to website when available
16 Percent ofchildren and adolescents without health insurance
Number without health insurance Total number of children and adolescents
CHIS http://www.chis.ucla.edu/ (requires registration- username and password) Links to tables are on FHOP website under CA MCH data
17 Percent ofchildren without dental insurance (age 2-11)
Number without dental insurance Total children aged 2-11
CHIS http://www.chis.ucla.edu/ (requires registration- username and password) Links to tables are on FHOP website under CA MCH data
18 Percent ofchildren who have been to the dentist in the past year (age 2-11)
Number of children to dentist in year Total children aged 2-11
CHIS http://www.chis.ucla.edu/ (requires registration- username and password) Links to tables are on FHOP website under CA MCH data
FHOP Community Assessment 1 October 2003 70

19 Percent ofchildren and adolescents who are overweight (ages 5-11 and 12-19)
Number overweight in age group Total children in age group
http://www.dhs.cahwnet.gov/pcfh/cms/onlinearchive/pdf/chdp /informationnotices/2003/chdpin03j.pdf
20 Rate of children hospitalized for asthma per 10000 (age 0-4 and age 5-18)
Number of hospitalizations Number of children in age group
www.ucsf.edu/fhop/ (click on CA MCH data and go down to asthma) FHOP will be posting trend data to website
21 Rate per 1000 women aged 15-19 with a reported case of chlamydia
Number of cases among women in age group Number of women in age group
Links to tables are on FHOP website under CA MCH data The STD Branch is preparing tables with Confidence Intervals.
22 Rate of children hospitalized for mental health reason per 10000 (age 5-14, age 15-19)
Number of hospitalizations in age group Total number in age group
FHOP is preparing these data and will post to website when available
23 Number and rate of hospitalizations for all non-fatal injuries by age group 0-14, 15-24
Number of hospitalizations in age group Total number in age group
FHOP is preparing these data and will post to website when available
24 Rate of non-fatal injuries due to motor vehicle accidents (age 0-14, 15-24
Number of injuries in age group Total number in age group
http://www.applications.dhs.ca.gov/epicdata/content/sum_causebyage.htm FHOP is preparing these data and will post to website when available
FHOP Community Assessment 1 October 2003 71

25 Number of children living in foster care for selected month (July)
http://cssr.berkeley.edu/CWSCMSreports/pointintime/fostercare/childwel/prevalence.asp#year Links to tables are on FHOP website under CA MCH data
26 Percent ofchildren in poverty, aged 0-19
Number below poverty level Number of children in age group
Links to tables are on FHOP website under CA MCH data
27 Percent of women ages 18 or older reporting intimate partner physical abuse in last 12 months
http://justice.hdcdojnet.state.ca.us/cjsc_stats/prof99/index.htm http://justice.hdcdojnet.state.ca.us/cjsc_stats/prof00/index.htm http://justice.hdcdojnet.state.ca.us/cjsc_stats/prof01/index.htm FHOP is also preparing these data and will post to website when available
FHOP Community Assessment 1 October 2003 72

COMMUNITY ASSESSMENT 1: BASIC CONCEPTS
Session Four
Options for Collecting and Presenting Assessment Data
Presented by:
Geraldine Oliva, MD, MPH Director
Family Health Outcomes Project

PARTICIPANTS GUIDE
Session Four Options for Collecting and Presenting
Community Assessment Data
LEARNING OBJECTIVES: By the end of the presentation and session, participants will be able to:
1. Give at least two examples of the advantages and disadvantages of using quantitative vs. qualitative data
2. Identify at least three criteria for evaluating a quantitative data source 3. Select an appropriate data source for two sample indicators 4. Determine the most effective way to present data on a sample indicator
REFERENCES FOR THIS SESSION
1. Developing an Effective Planning Process: A Guide to Local MCH Programs, Chapter 2 “Community Health Assessment: Identifying Maternal, Child Health Needs and Setting Priorities,” Component 1. Compile the Community Health Profile and Component 4. Collect, Analyze and Present Data for the Selected Indicators and Appendices II-F, II-G, and II-H. 2nd edition, 2003
FHOP Community Assessment 1 October 2003 74

Options for Collecting and Presenting
Assessment Data
Geraldine Oliva, M.D. MPH
Family Health Outcomes ProjectOctober 8, 2003
12
34
56
0
20
40
60
80
100
-150
-100
-50
0
50
100
150
200
250
300
1 2 3 4 5 6 7 8 9 10
COUNTYREPORT
CARD
Title V Indicator HEALTHY PEOPLE2010
OBJECTIVES
Session Objectives
By the end of this session participants will be able to:n Give at least two examples of the
advantages and disadvantages of using quantitative data vs. qualitative data
n Identify at least three criteria for evaluating a quantitative data source
n Select an appropriate data source for two sample indicators
n Determine the most effective way to present data on a sample indicator
FHOP Community Assessment 1 October 2003 75

Choosing a Data Source
n Quantitative Data – numbers, rates, statisticsuPrimary- you collect ituSecondary – use an existing data
source
n Qualitative Data – words, thoughts, actions, intentions
Quantitative Data: Advantages
n Quantifies results
n Allows statistical comparisons
and multivariate analyses
n Allows comparisons with other groups and over
time using standard measures
n Conserves resources if secondary data source
available
Quantitative Data: Disadvantages
n Requires expertise in data analysis
n Limited use in situations where numbers are small
n Collecting primary data is expensive and time-consuming
n Can overlook emerging issues
FHOP Community Assessment 1 October 2003 76

Quantitative Data: Disadvantages
n Presupposes you to know the significant factors
n Often lacks important variables such as geographic markers or detailed race or ethnicity categories
n May not be timely
Qualitative Data: Advantages
n Rich data with more details and
contextual information
n Can provide new insights
n Can identify emerging issues
n Face-to-face contact allows opportunity to
clarify questions
n Can be timely and current
Qualitative Data: Disadvantages
n Requires expertise in staff and can be time consuming
n Possible inconsistency due to flexibility
n Difficult to make comparisons
n Transcribing and reduction of data costly
n Individuals may alter responses because of group environment
FHOP Community Assessment 1 October 2003 77

Factors to Consider in Choosing the Type of Data You Need
? Is this a well described and quantifiable
problem?
? Do I want to compare data with known
standards or other population groups?
? Do I have an evidenced based hypothesis about
the cause of a problem or am I searching for
new insights?
Factors to Consider in Choosing the Type of Data You Need (cont)
? Do I want to understand the perspective of the
community?
? Will quantitative data be meaningful? (i.e.
adequate numbers)
? Are there reliable secondary data sources
available?
? Are there adequate local resources for a
particular method?
Criteria for Assessing a Secondary Data Source
n Accuracy and Consistencyn Adequate sample size for local community
n Contains the specificity for local needs
n Timeliness
n Cost
n Availability over time
FHOP Community Assessment 1 October 2003 78

Data Accessibility
COMMISSAROF VITAL RECORDS
MCH DIRECTOR
Considerations for Primary Data Collection
n Existence of a validated instrument or
set of questions for area(s) of interest
n Potential sample size
n Potential for random sample
n Resource availability - $ and expertise
Choosing a Qualitative Method
n Determining the objectives for the study and identifying the type of information needed
n Identifying local expertise in both conducting the data collection and analyzing the data collected
n Identifying resources
FHOP Community Assessment 1 October 2003 79

Mini-Exercise: What is the Best Data Source for These Indicators?
n Infant mortality rate
n Barriers to early entry into prenatal care
n Use of infant car seats
n Prevalence of childhood obesity
Analyzing the Data
n Answer the who, what, where, when and why of epidemiology
n Describe the population affected (e.g. age, race/ethnicity, place of residence, income)
n Include at least 5 years to observe direction
n Compare to a standard such as HP 2010 n Make statistical comparisons where
possible
Z Z ZZ
ZZ
FHOP Community Assessment 1 October 2003 80

Addressing Methodological Issues
n Fewer than 10 cases over 3 years
n Only one year of data
n Unclear meaning of indicator
n Multiple indicator definitions
n Finding a denominator
Addressing Methodological Issues :Examples
n Infant mortality cases: 7 for 1999-2001
n Percent Uninsured from CHIS survey
n Rate per 1000 of children living in foster care
n Percent of teens 15-19 using alcohol
n Rate of mental health admissions by payor
source
Presenting the Data
n Identify key findingsn Select a graphic to convey your
message n Always show numbers as well as ratesn Indicate data sourcen Note statistical significancen Provide concise interpretationsn Discuss any lack of data
FHOP Community Assessment 1 October 2003 81

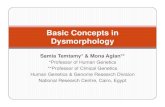
Infant Mortality Rates, Alameda County 1992-2000
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
1992
1993
1994
1995
1996
1997
1998
1999
2000
Year
Infa
nt
Death
s/1
,000 L
ive B
irth
s
County Point Estimate
State Point Estimate
Year 2010 Objective
Infant Mortality Rate, Alameda County
1997-1999
Percent of Infant Deaths by Race/ Ethnicity,
Alameda County 1995-1997 (N=362)
White28%
Asian Pacific/ Islander14%
African American41%
Native American0%
Hispanic17%
FHOP Community Assessment 1 October 2003 82

Infant Mortality Rate by Race/Ethnicity 1995-1997
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
Total White Black Hispanic Asian AmIndian
Race/Ethnicity
Death
Rate
/1,0
00 L
ive B
irth
s
Percent Low Birth Weight Babies, Alameda County 1992-2000
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
1992
1993
1994
1995
1996
1997
1998
1999
2000
Year
Perc
en
t L
ow
Bir
thw
eig
ht
County Point Estimate
State Point Estimate
Year 2010 Objective
Percent Low Birth Weight Births by Mother's Age and
Race/Ethnicity, Alameda County 1996-1998 (3-year
average)
11.2
6 6.9
4.95.3
17.1
12.3
7.25.3
7.46.1
8.4 10.1
8.26.6
0
246
810
1214
1618
19 and under 20-34 35 and above
Pe
rce
nt
of
Bir
ths
LB
W
White African American Hispanic Asian/PI Other
FHOP Community Assessment 1 October 2003 83

Percent of Low Birthweight Babies by Race/Ethnicity,Alameda County 1998
White32%
Black28%
Hispanic22%
Asian18%
AmIndian0%
White
Black
Hispanic
Asian
AmIndian
Percent of Babies Low Birth Weight by Race/Ethnicity,
Alameda County 1998
5.8%6.1%
12.6%
5.9%
0%
4%
8%
12%
16%
White AfricanAmerican
Hispanic Asian/ PacificIslander
Pe
rce
nt
of
Bir
ths
LB
W
Teen Birth Rate (10-19yrs), Alameda County 1992-2000
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
1992
1993
1994
.019
9519
9619
9719
9819
9920
00
Year
Ra
te/1
,00
0 F
em
ale
s 1
0-1
9
County Point Estimate
State Point Estimate
FHOP Community Assessment 1 October 2003 84

Percent of Births to Teens (ages 15-17), Alameda County 1998-2000
Percent of Teen Births (10-19yrs) by Race/Ethnicity, Alameda
County 1998
White19%
Black31%
Hispanic40%
Asian9%
AmIndian1%
White
Black
Hispanic
Asian
AmIndian
Teen Birth Rate (ages 15-17) by Race/Ethnicity, Alameda County 1998
10.112.6
41.245.3
0
10
20
30
40
50
White African American Hispanic Asian/ PacificIslander
Bir
ths
pe
r 1
,00
0 f
em
ale
s
FHOP Community Assessment 1 October 2003 85

Take Home Points
n Collect data that is meaningful for your jurisdiction
n Use quantitative data and qualitative data where feasible to tell your story
n Display data in a way that emphasizes the most important findings
RELAX !!!
FHOP Community Assessment 1 October 2003 86