
Community Acquired Pneumonia (CAP)
78
description
CAP. Community Acquired Pneumonia (CAP). CAP. Improving Outcomes Through Education. The New Treatment Paradigm – Selecting Appropriate Empiric Antibiotics. www.drsarma.in. CAP. Prof. Dr. Sarma VSN Rachakonda M.D., M.Sc., (Canada), FCGP, FIMSA, FICP, FRCP (G), FCCP (USA ), FACP(USA) - PowerPoint PPT Presentation
Transcript of Community Acquired Pneumonia (CAP)

The New Treatment Paradigm – The New Treatment Paradigm –
Selecting Appropriate Empiric AntibioticsSelecting Appropriate Empiric Antibiotics
Prof. Dr. Sarma VSN RachakondaM.D., M.Sc., (Canada), FCGP, FIMSA,
FICP, FRCP (G), FCCP (USA), FACP(USA)
Senior Consultant Physician & Cardio-metabolic & Chest Specialist
Adjunct Professor, The Tamilnadu Dr. MGR Medical University
Honorary National Professor of Medicine, IMA-CGP
www.drsarma.in
4
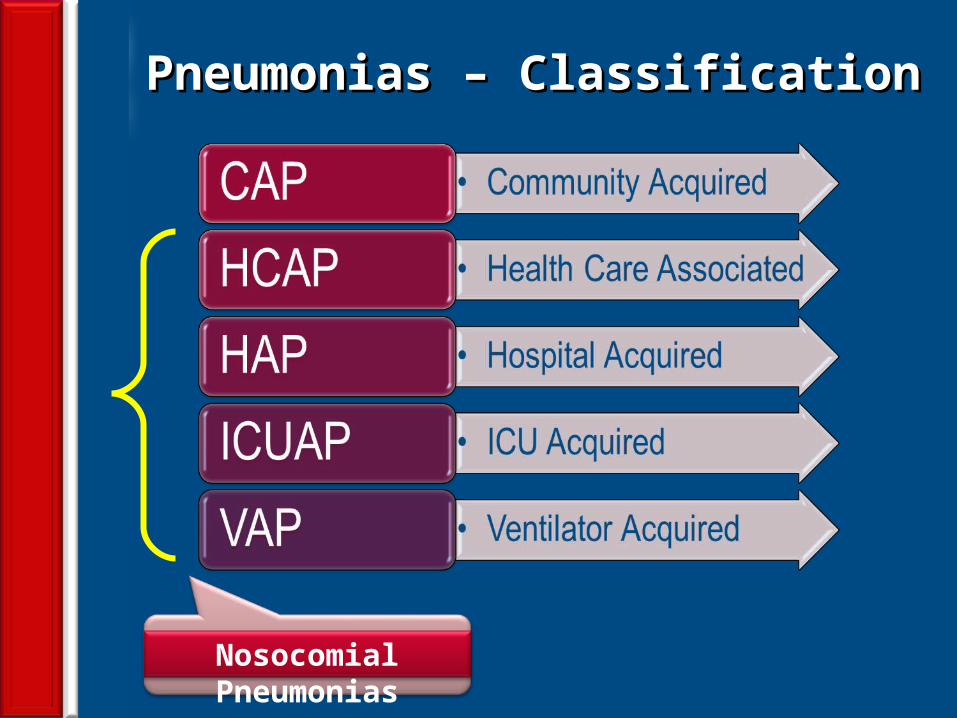
Pneumonias – ClassificationPneumonias – Classification
Nosocomial Pneumonias
5
Community Acquired Pneumonia (CAP)Community Acquired Pneumonia (CAP)
DefinitionDefinition… … an acute infection of the pulmonary parenchyma an acute infection of the pulmonary parenchyma
that is associated with at least some symptoms of that is associated with at least some symptoms of acute infection, accompanied by the presence of an acute infection, accompanied by the presence of an acute infiltrate on a chest radiograph, or auscultatory acute infiltrate on a chest radiograph, or auscultatory findings consistent with pneumonia, findings consistent with pneumonia, in a patient not in a patient not hospitalized or residing in a long term care facility hospitalized or residing in a long term care facility for for >> 14 days before onset of symptoms. 14 days before onset of symptoms.
Bartlett. Clin Infect Dis 2000;31:347-82.
6
Guidelines for CAPGuidelines for CAP
American Thoracic Society (ATS)American Thoracic Society (ATS) Guidelines - Management of Adults with CAP (2001)Guidelines - Management of Adults with CAP (2001)
Infectious Diseases Society of America (IDSA)Infectious Diseases Society of America (IDSA) Update of Practice Guidelines Management of CAP Update of Practice Guidelines Management of CAP
in in Immuno-competentImmuno-competent adults (2003) adults (2003) ATS and IDSA joint effort (we will follow this)ATS and IDSA joint effort (we will follow this)
IDSA/ATS Consensus Guidelines on the Management IDSA/ATS Consensus Guidelines on the Management
of CAP in of CAP in AdultsAdults ( (March 2007March 2007)) CAP – Consensus Statement on Indian ScenarioCAP – Consensus Statement on Indian Scenario
7
Evidence-based practiceEvidence-based practice Best outcome for patientsBest outcome for patients Best use of resourceBest use of resource Restricts idiosyncratic behaviourRestricts idiosyncratic behaviour
Legal protectionLegal protection Identify research needsIdentify research needs A tool for educationA tool for education Gain public confidenceGain public confidence
Why Guidelines?Why Guidelines?
8
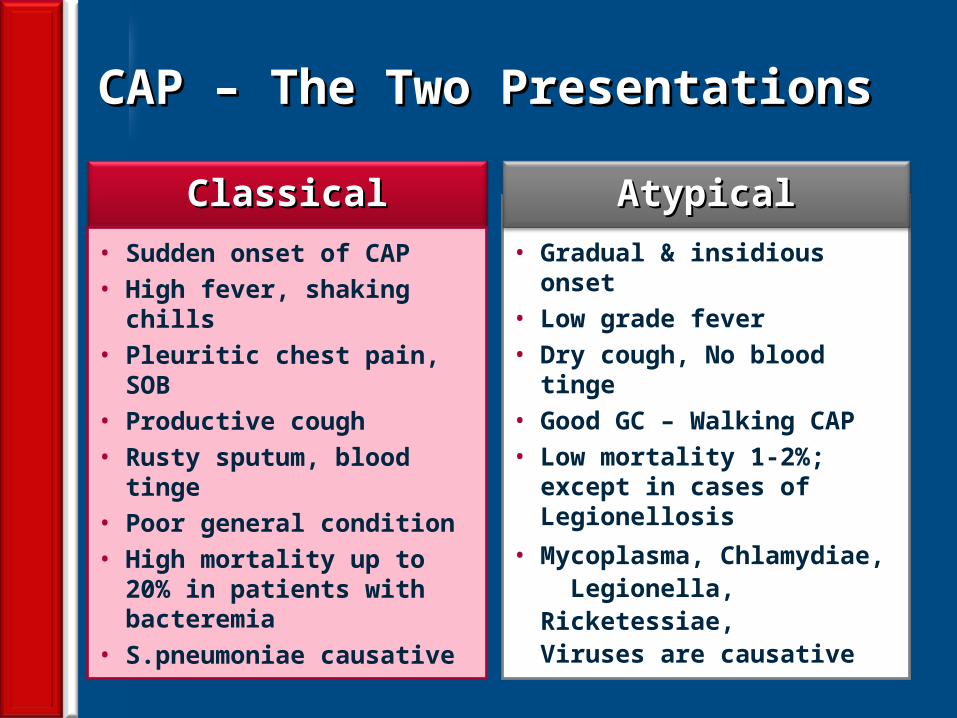
CAP – The Two PresentationsCAP – The Two Presentations
ClassicalClassical
• Sudden onset of CAP• High fever, shaking chills• Pleuritic chest pain, SOB• Productive cough• Rusty sputum, blood tinge• Poor general condition• High mortality up to 20% in
patients with bacteremia• S.pneumoniae causative
• Gradual & insidious onset• Low grade fever• Dry cough, No blood tinge• Good GC – Walking CAP• Low mortality 1-2%; except
in cases of Legionellosis• Mycoplasma, Chlamydiae,
Legionella, Ricketessiae, Viruses are causative
AtypicalAtypical
9
CAP – PathogenesisCAP – Pathogenesis
10
AgeAge Obesity; Exercise is protectiveObesity; Exercise is protective Smoking, PVD Smoking, PVD Asthma, COPDAsthma, COPD Immuno-suppression, HIVImmuno-suppression, HIV Institutionalization, Old age homes etcInstitutionalization, Old age homes etc DementiaDementia
CAP – Risk Factors for PneumoniaCAP – Risk Factors for Pneumonia
ID Clinics 1998;12:723. Am J Med 1994;96:313
11
Community Acquired Pneumonia (CAP)Community Acquired Pneumonia (CAP)
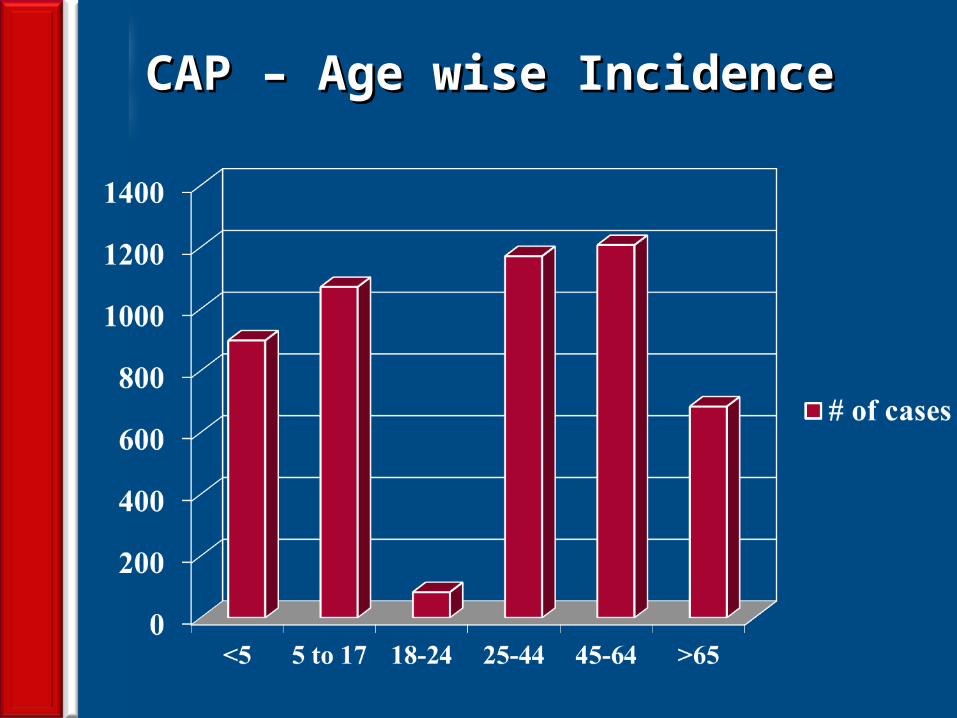
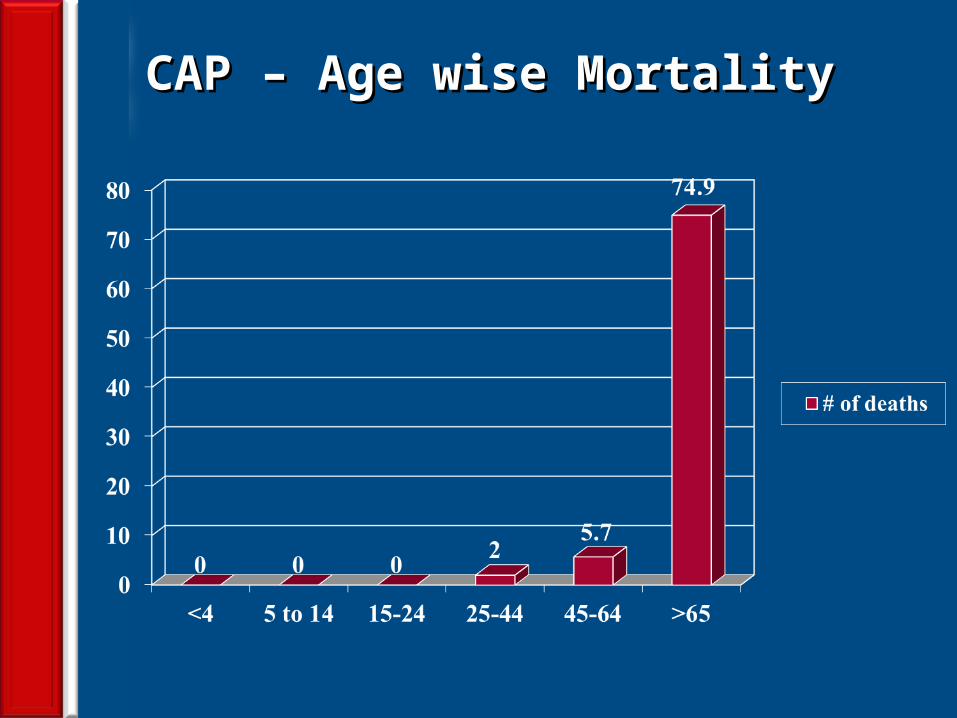
EpidemiologyEpidemiology 4-5 million cases annually4-5 million cases annually ~500,000 hospitalizations – 20% require admission~500,000 hospitalizations – 20% require admission ~45,000 deaths~45,000 deaths Fewest cases in 18-24 yr groupFewest cases in 18-24 yr group Probably highest incidence in <5 and >65 yrsProbably highest incidence in <5 and >65 yrs Mortality disproportionately high in >65 yrs Mortality disproportionately high in >65 yrs Over all mortality is 2-30%Over all mortality is 2-30% <1% for those not requiring hospitalization<1% for those not requiring hospitalization
Bartlett. CID 1998;26:811-38.
12
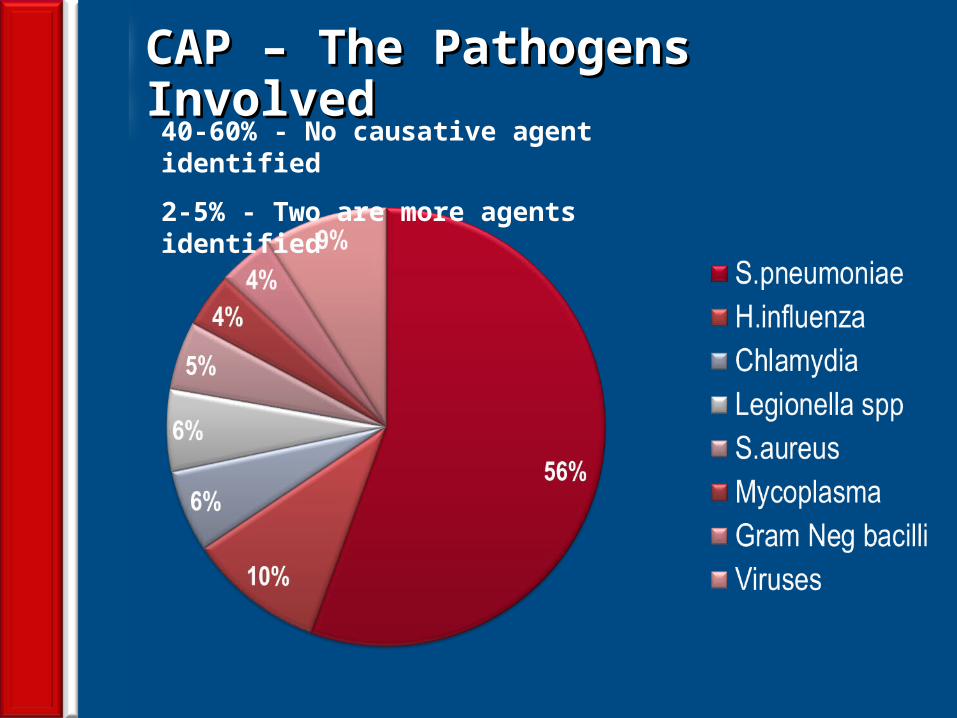
CAP – The Pathogens InvolvedCAP – The Pathogens Involved40-60% - No causative agent identified
2-5% - Two are more agents identified
13
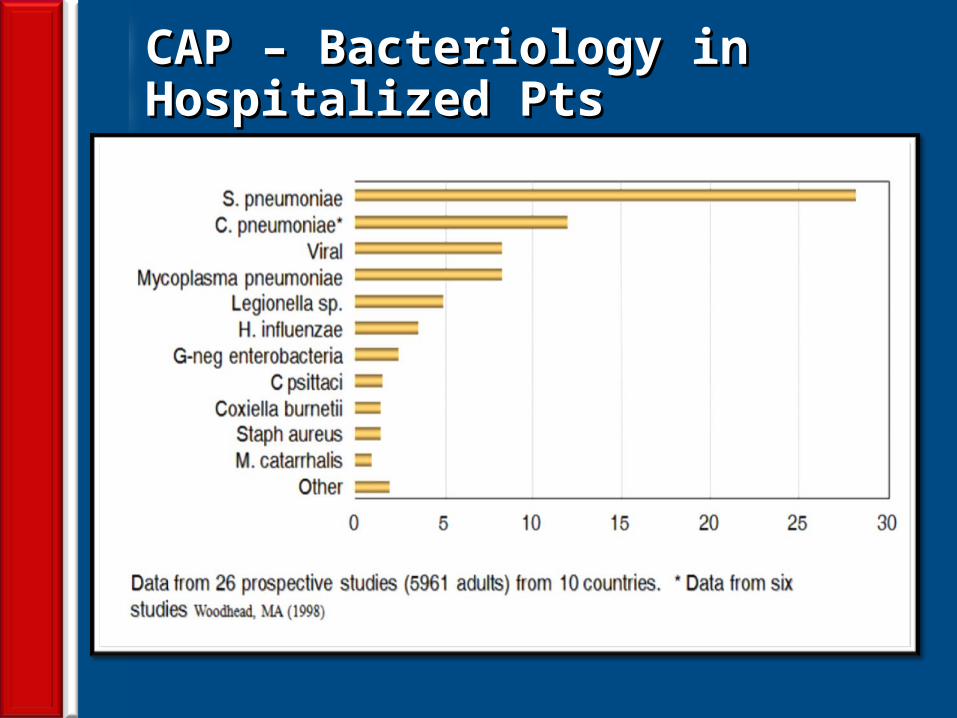
Streptococcus pneumonia Streptococcus pneumonia (Pneumococcus)Pneumococcus)
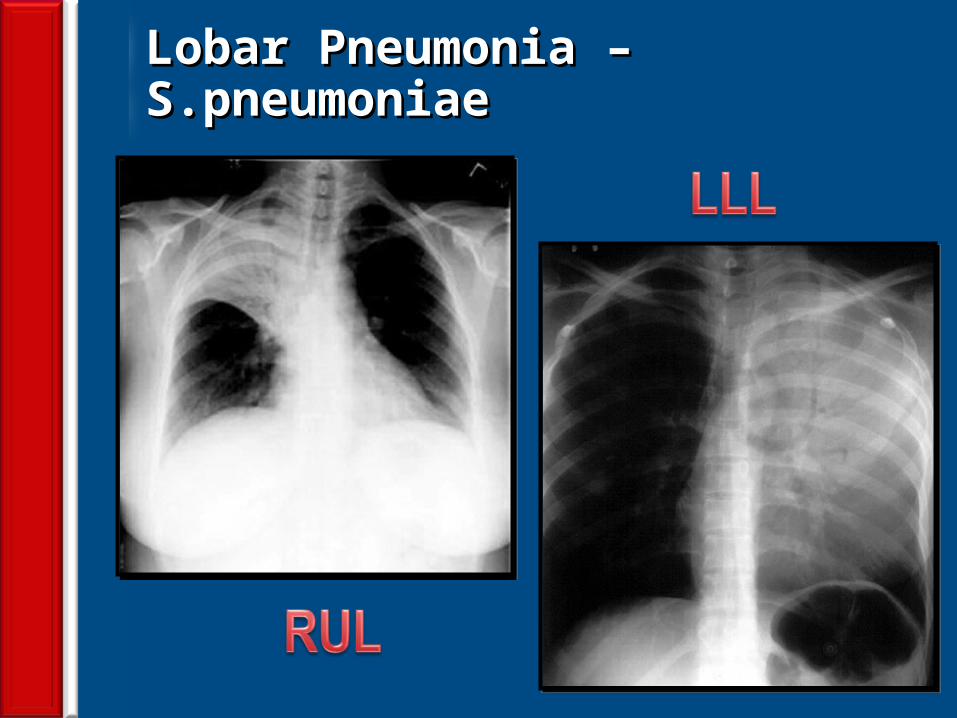
Most common cause of CAPMost common cause of CAP About 2/3 of CAP are due to S.pneumoniaeAbout 2/3 of CAP are due to S.pneumoniae These are gram positive diplococciThese are gram positive diplococci Typical symptoms (e.g. malaise, shaking chills Typical symptoms (e.g. malaise, shaking chills
fever, rusty sputum, pleuritic chest pain, cough)fever, rusty sputum, pleuritic chest pain, cough) Lobar infiltrate on CXRLobar infiltrate on CXR May be Immuno suppressed host*May be Immuno suppressed host* 25% will have bacteremia – serious effects25% will have bacteremia – serious effects
*Anorexia, ETOH, HIV, Sickle cell disease, Splenectomy, Hematologic diseases
14
CAP – Age wise IncidenceCAP – Age wise Incidence
15
CAP – Age wise MortalityCAP – Age wise Mortality
16
Older, Unemployed, UnmarriedOlder, Unemployed, Unmarried Recurrent common coldRecurrent common cold Asthma, COPD; Steroid or bronchodilator useAsthma, COPD; Steroid or bronchodilator use Chronic diseases, Diabetes, CHF, NeoplasiaChronic diseases, Diabetes, CHF, Neoplasia Amount of smoking Amount of smoking Alcohol is NOT related to increased risk for Alcohol is NOT related to increased risk for
hospitalizationhospitalization
CAP – Risk Factors for HospitalizationCAP – Risk Factors for Hospitalization
ID Clinics 1998;12:723. Am J Med 1994;96:313
17
Age > 65Age > 65 Bacteremia (for S. pneumoniae)Bacteremia (for S. pneumoniae) S. aureus, MRSA , Pseudomonas S. aureus, MRSA , Pseudomonas Extent of radiographic changesExtent of radiographic changes Degree of immuno-suppressionDegree of immuno-suppression Amount of alcohol consumptionAmount of alcohol consumption
CAP – Risk Factors for MortalityCAP – Risk Factors for Mortality
ID Clinics 1998;12:723. Am J Med 1994;96:313
18
CAP – Bacteriology in Hospitalized PtsCAP – Bacteriology in Hospitalized Pts
19
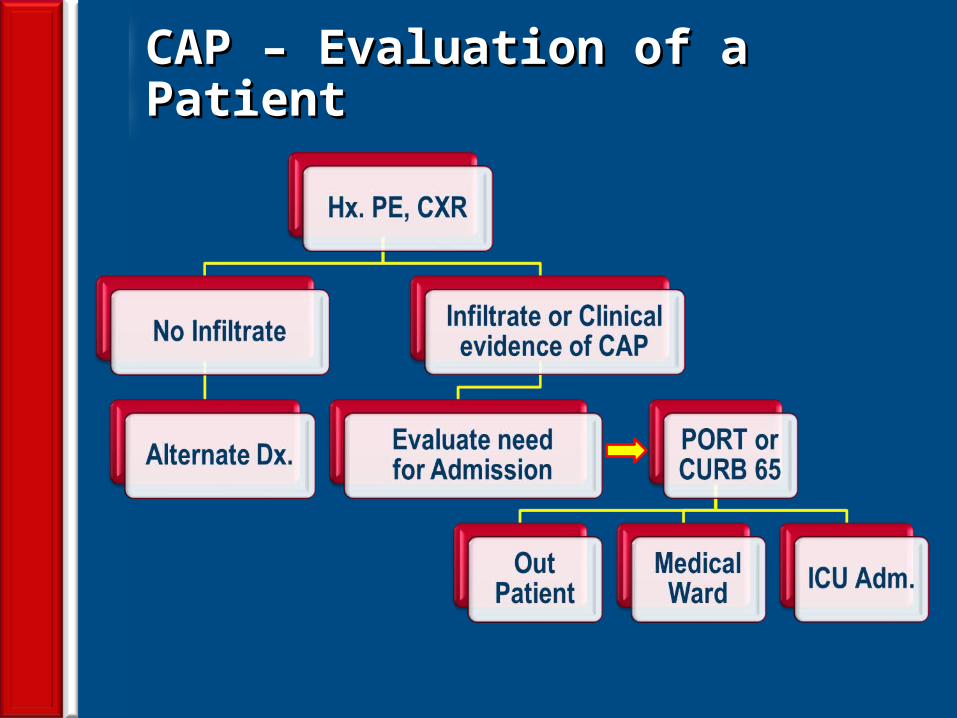
CAP – Evaluation of a PatientCAP – Evaluation of a Patient
20
CAP – Management Guidelines CAP – Management Guidelines
Rational use of microbiology laboratoryRational use of microbiology laboratory Pathogen directed antimicrobial therapy Pathogen directed antimicrobial therapy
whenever possiblewhenever possible Prompt initiation of Antibiotic therapyPrompt initiation of Antibiotic therapy Decision to hospitalize based on Decision to hospitalize based on
prognostic criteria - PORT or CURB 65prognostic criteria - PORT or CURB 65
21
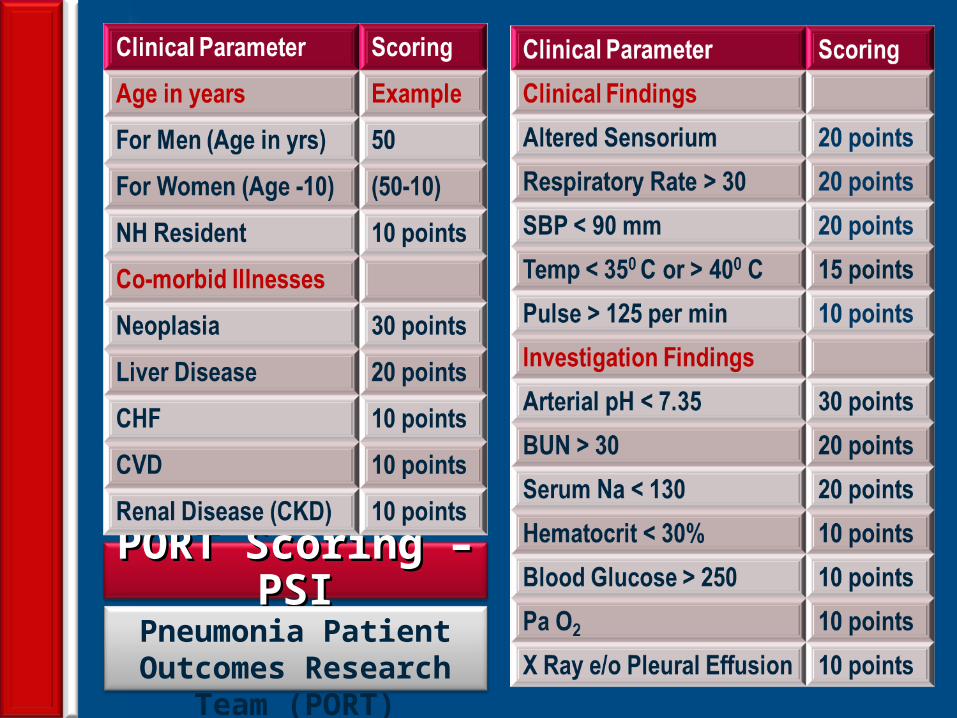
PORT Scoring – PSIPORT Scoring – PSIPneumonia Patient Outcomes
Research Team (PORT)
22
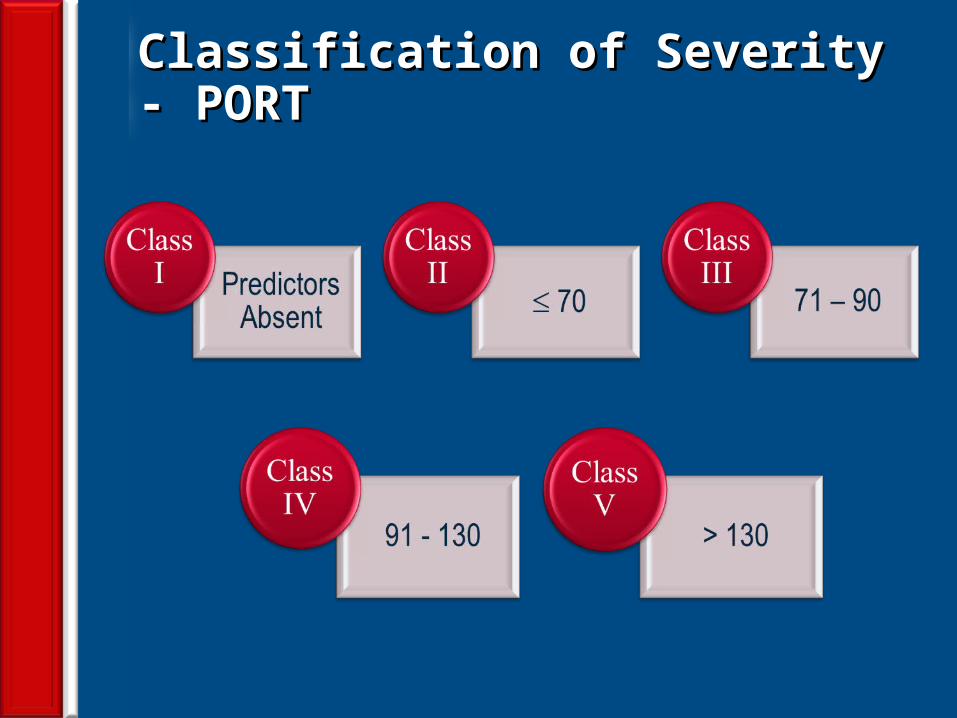
Classification of Severity - PORTClassification of Severity - PORT
23
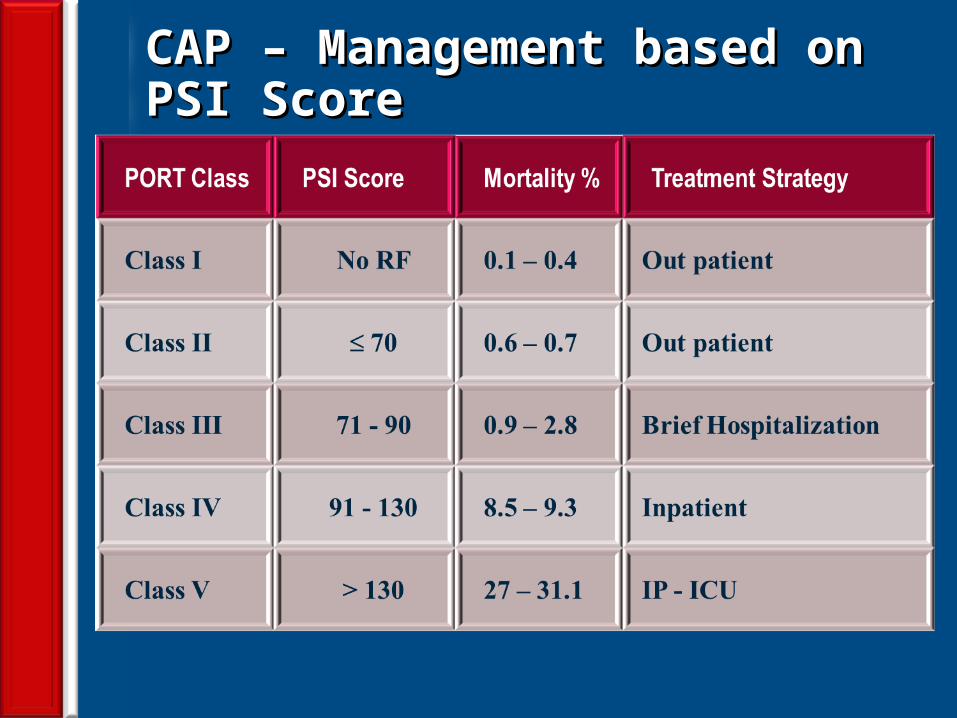
CAP – Management based on PSI ScoreCAP – Management based on PSI Score
24
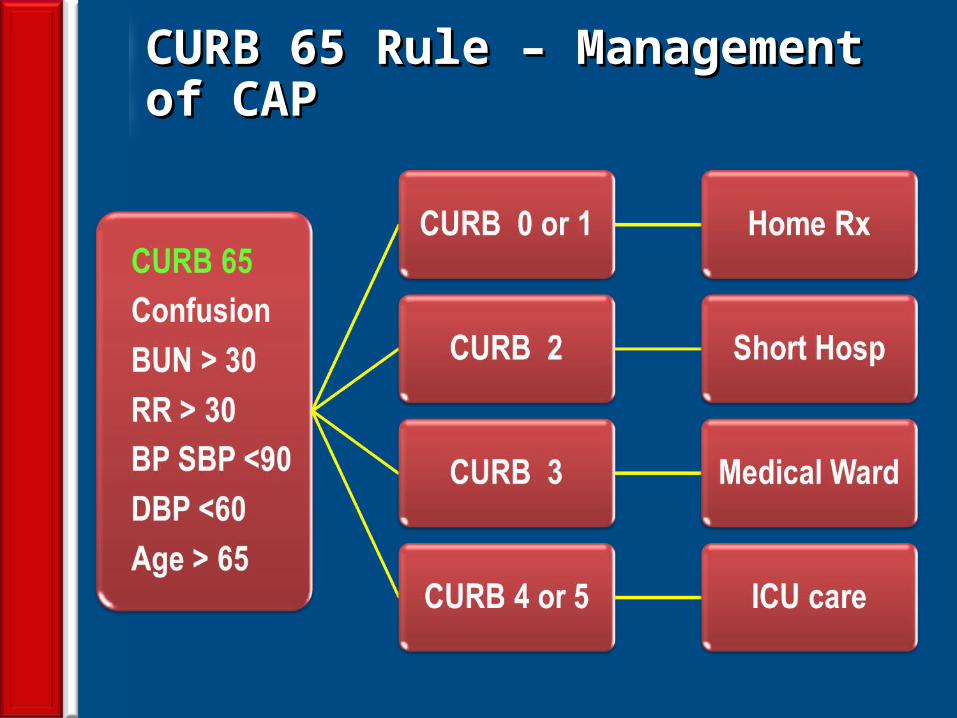
CURB 65 Rule – Management of CAPCURB 65 Rule – Management of CAP
25
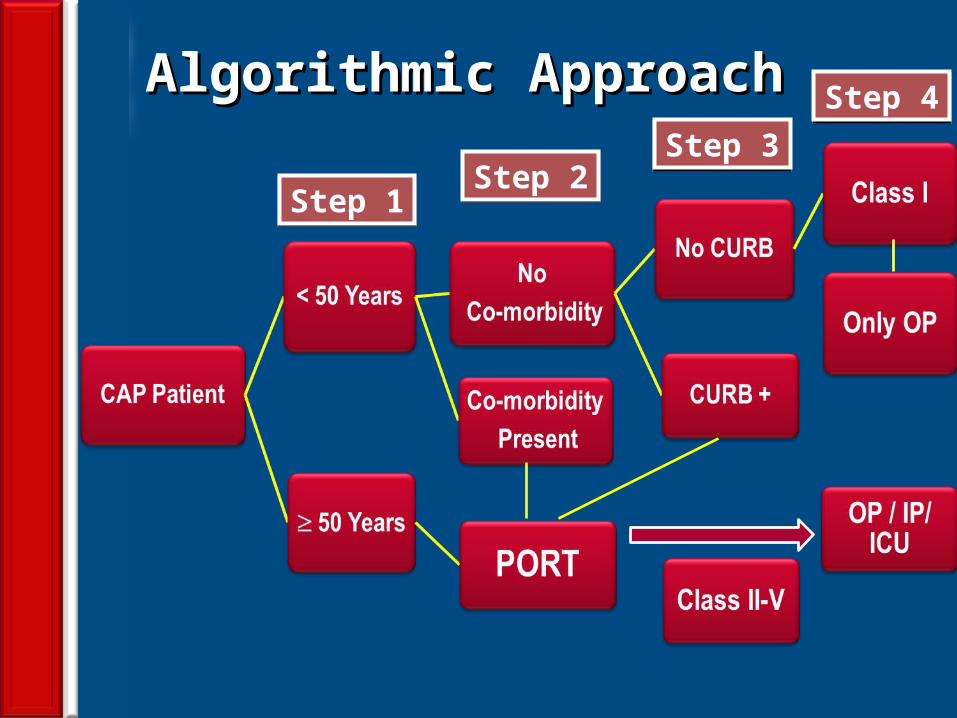
Algorithmic ApproachAlgorithmic Approach
Step 1Step 2
Step 3Step 4
26
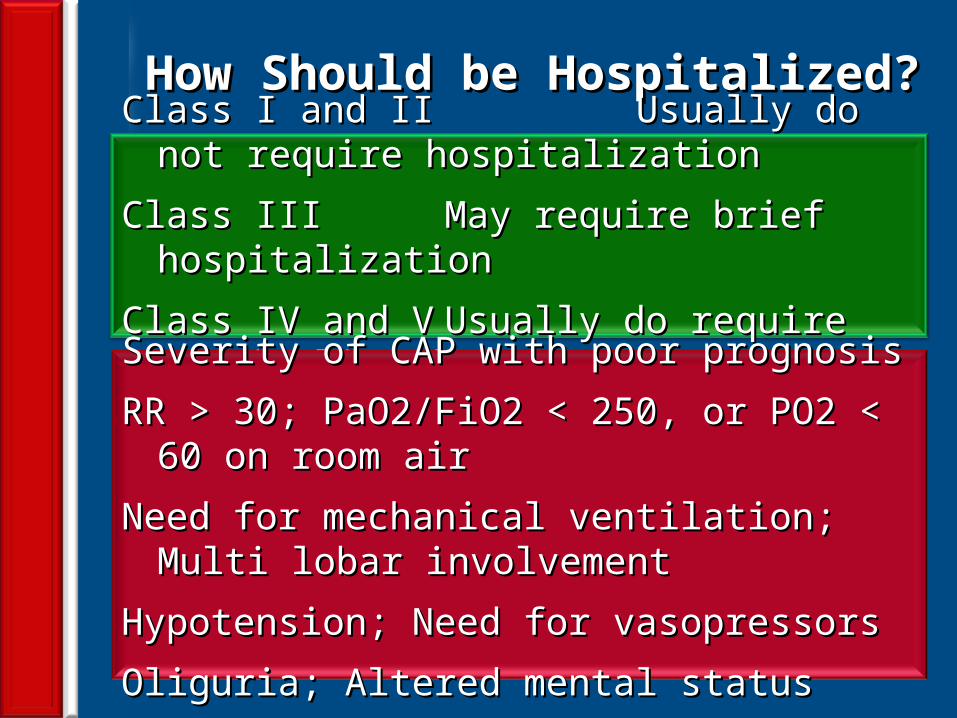
How Should be Hospitalized?How Should be Hospitalized?Class I and II Class I and II Usually do not require Usually do not require
hospitalizationhospitalization
Class IIIClass III May require brief hospitalizationMay require brief hospitalization
Class IV and VClass IV and V Usually do require hospitalizationUsually do require hospitalization
Severity of CAP with poor prognosis Severity of CAP with poor prognosis
RR > 30; PaO2/FiO2 < 250, or PO2 < 60 on room airRR > 30; PaO2/FiO2 < 250, or PO2 < 60 on room air
Need for mechanical ventilation; Multi lobar involvementNeed for mechanical ventilation; Multi lobar involvement
Hypotension; Need for vasopressorsHypotension; Need for vasopressors
Oliguria; Altered mental statusOliguria; Altered mental status
27
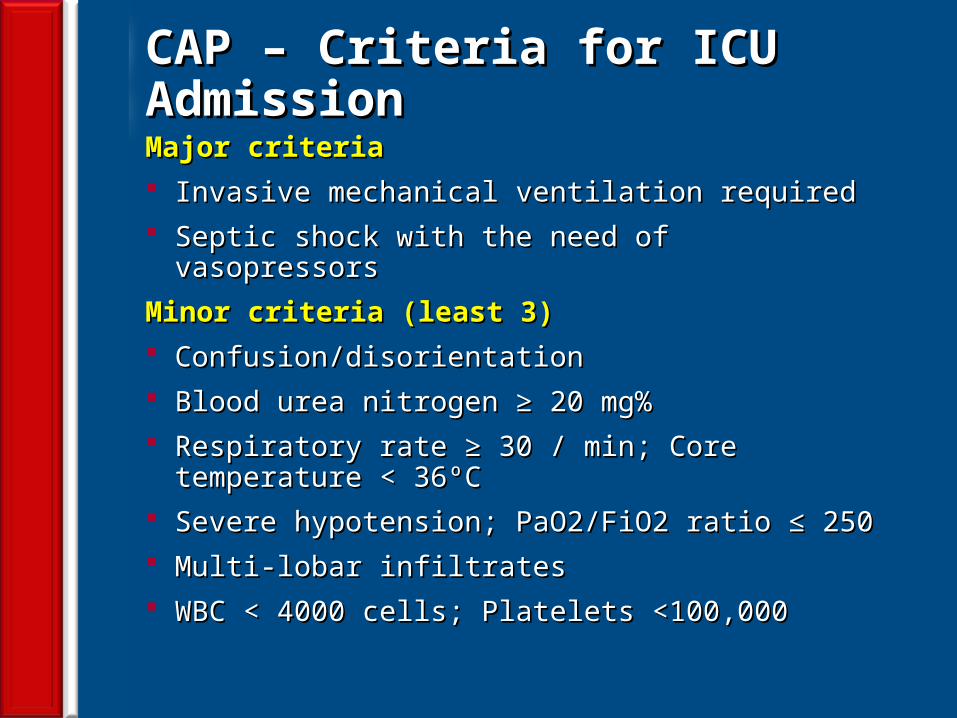
CAP – Criteria for ICU AdmissionCAP – Criteria for ICU AdmissionMajor criteriaMajor criteria Invasive mechanical ventilation requiredInvasive mechanical ventilation required Septic shock with the need of vasopressorsSeptic shock with the need of vasopressors
Minor criteria (least 3)Minor criteria (least 3) Confusion/disorientationConfusion/disorientation Blood urea nitrogen ≥ 20 mg%Blood urea nitrogen ≥ 20 mg% Respiratory rate ≥ 30 / min; Core temperature < 36ºCRespiratory rate ≥ 30 / min; Core temperature < 36ºC Severe hypotension; PaO2/FiO2 ratio ≤ 250Severe hypotension; PaO2/FiO2 ratio ≤ 250 Multi-lobar infiltratesMulti-lobar infiltrates WBC < 4000 cells; Platelets <100,000WBC < 4000 cells; Platelets <100,000
28
Limitation of Common InvestigationsLimitation of Common Investigations
• Quality of Sputum issuesQuality of Sputum issues
• Positivity rate of sputum smear/culture is 50%Positivity rate of sputum smear/culture is 50%
• Culture and smear correlationCulture and smear correlation
• Blood cultures very insensitive – poor positive ratesBlood cultures very insensitive – poor positive rates
• Serology needs raising titers – costly, time issuesSerology needs raising titers – costly, time issues
• Viral isolations not feasibleViral isolations not feasible
29
Scoring SystemsScoring Systems• Pneumonia Severity Index (PSI) - PORTPneumonia Severity Index (PSI) - PORT• CURB 65CURB 65• CRB 65CRB 65• ATS/IDSA CriteriaATS/IDSA Criteria• SMART-COP Rule (Systolic blood pressure, Multi-SMART-COP Rule (Systolic blood pressure, Multi-
lobar chest radiography involvement, Albumin level, lobar chest radiography involvement, Albumin level, Respiratory rate, Tachycardia, Confusion, Respiratory rate, Tachycardia, Confusion, Oxygenation, and arterial pH)Oxygenation, and arterial pH)
• SCAP Rule SCAP Rule
30
PSI v/s CURB 65: LimitationsPSI v/s CURB 65: Limitations• While the PSI is indicated for identifying low-risk patients, While the PSI is indicated for identifying low-risk patients,
the CURB65 is ideal for identifying high mortality risk the CURB65 is ideal for identifying high mortality risk patients with severe illness. patients with severe illness.
• The downside of PSI is it cannot predict need for ICU care.The downside of PSI is it cannot predict need for ICU care.• A recent meta-analysis by Chalmers et al. did not find any A recent meta-analysis by Chalmers et al. did not find any
significant differences in overall test performance between significant differences in overall test performance between PSI, CURB65 and CRB65 for predicting mortality of CAP.PSI, CURB65 and CRB65 for predicting mortality of CAP.
Both PSI and the CURB 65 have several limitations. These scoring systems are designed primarily to predict mortality. So, they are influenced by age and presence of co-morbid conditions. They are not very effective for predicting ICU admission
31
Why SCAP for CAP in Indian Context? Why SCAP for CAP in Indian Context? • The SCAP score needs only two additional parameters, The SCAP score needs only two additional parameters,
compared to CURB65 components - CXR and ABGcompared to CURB65 components - CXR and ABG• SCAP score cannot be as accurate in the absence of ABG. SCAP score cannot be as accurate in the absence of ABG. • Results of both these tests are available within an hour Results of both these tests are available within an hour
• CURB-65/CRB-65 is recommended over the PSI in the Indian context.
• Admission criteria should be based on CURB-65/CRB-65
• After the decision of hospital admission has been made , SCAP score (CURB-65 + CXR+ ABG) should be used to decide ward or ICU admission
• In patients admitted in ICU, in addition to SCAP, Procalcitonin levels may be used as prognostic marker for patients at intermediate risk.
32
CAP – Laboratory TestsCAP – Laboratory Tests
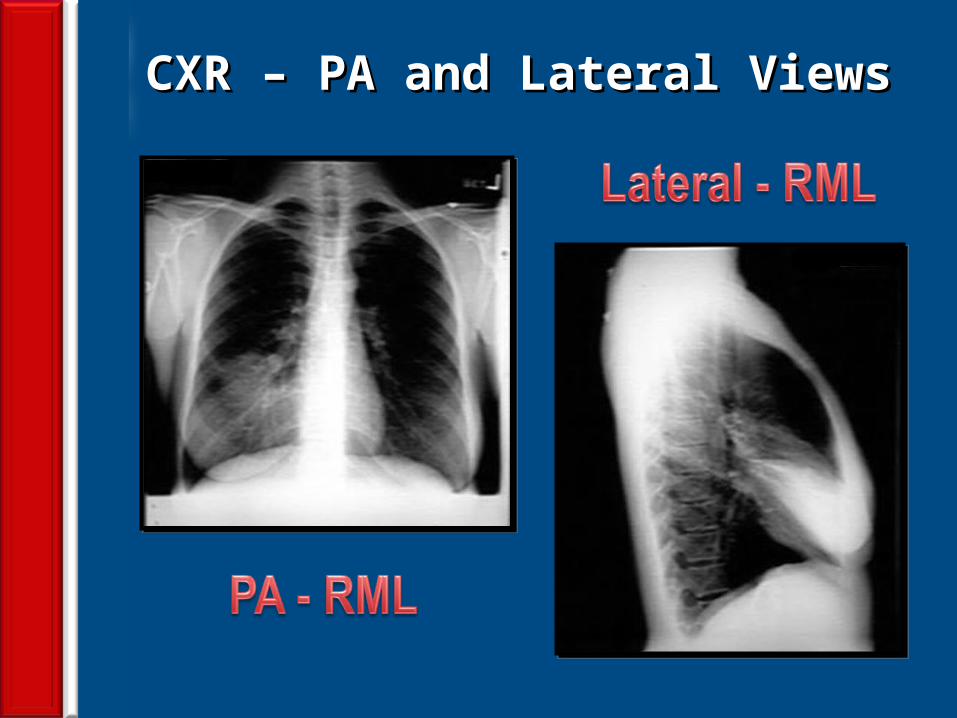
• CXR – PA & lateral• CBC with Differential• BUN and Creatinine• FBG, PPBG• Liver enzymes
• Serum electrolytes• Gram stain of sputum• Culture of sputum• Pre Rx. blood cultures• Oxygen saturation
33
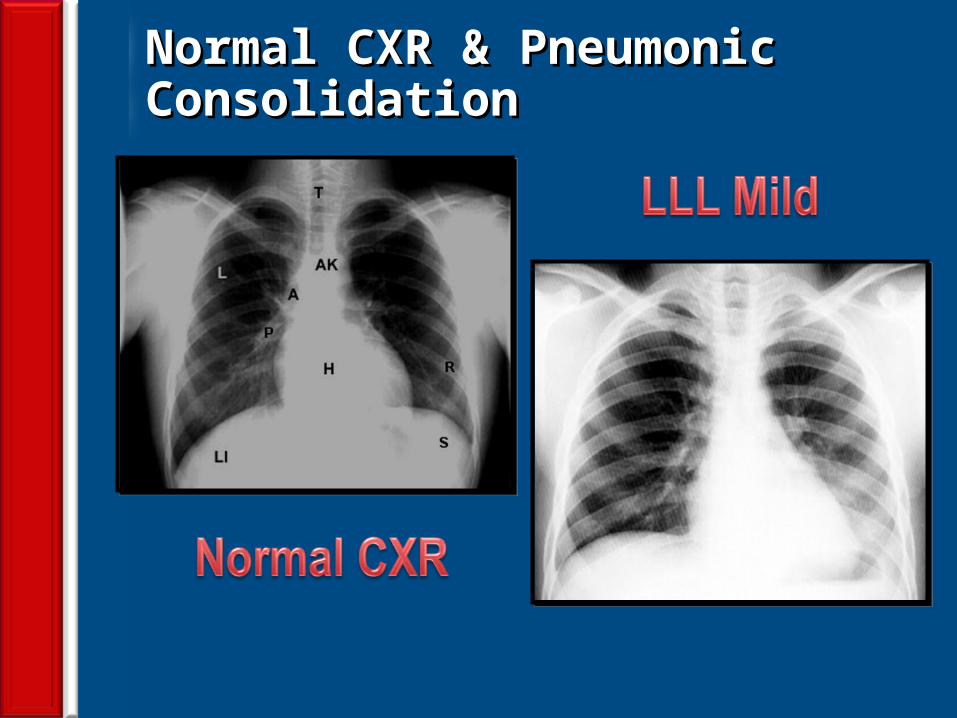
CAP – Value of Chest RadiographCAP – Value of Chest Radiograph
• Usually needed to establish diagnosis• It is a prognostic indicator • To rule out other disorders• May help in etiological diagnosis
J Chr Dis 1984;37:215-25
34
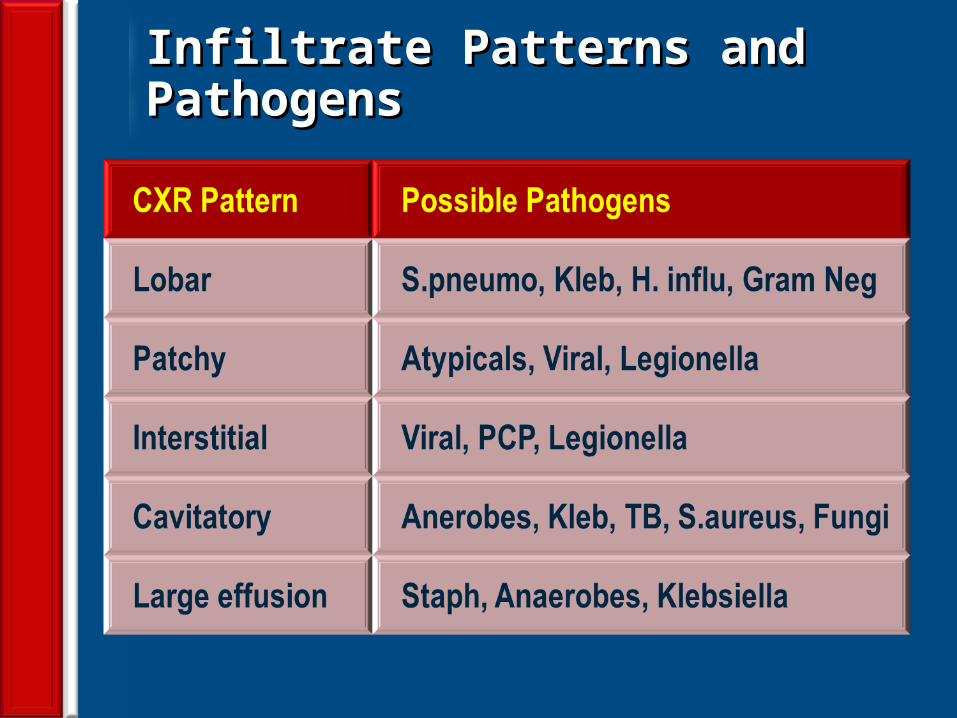
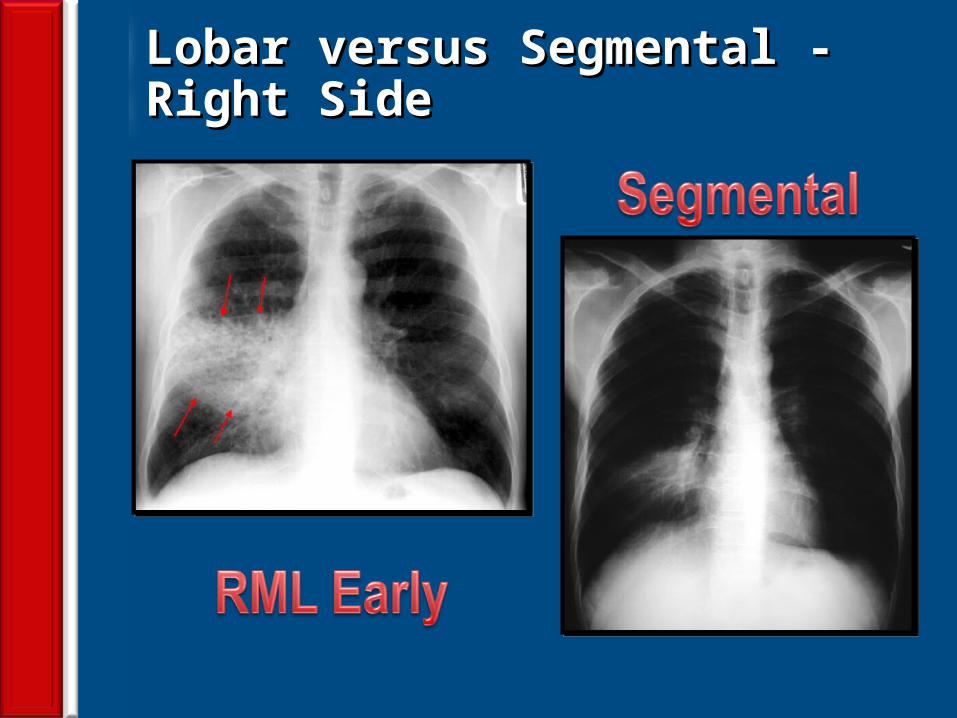
Infiltrate Patterns and PathogensInfiltrate Patterns and Pathogens
35
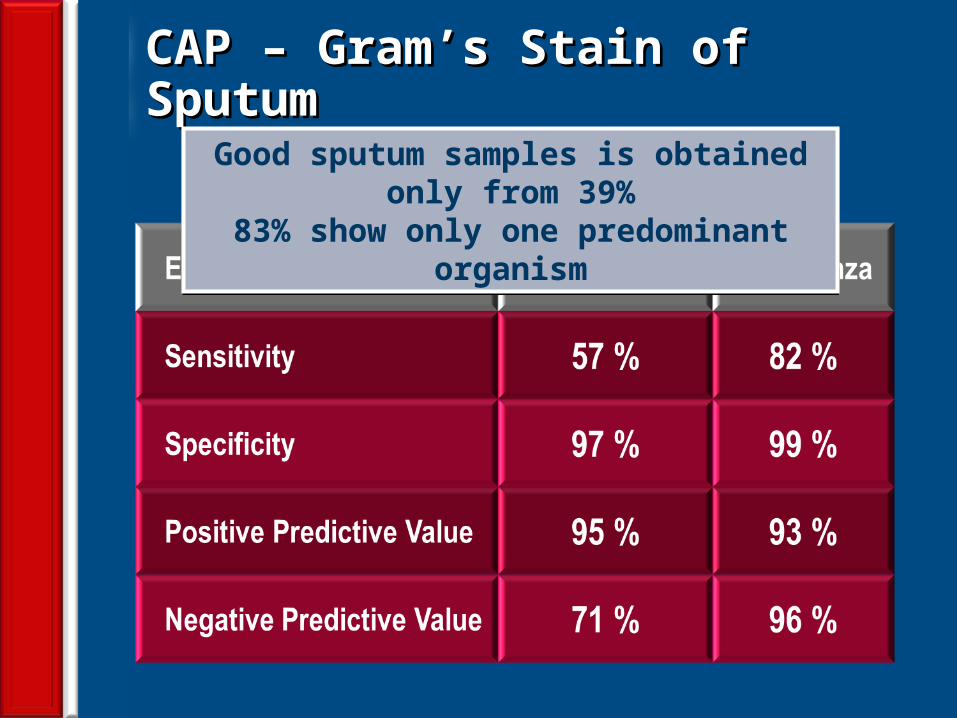
CAP – Gram’s Stain of SputumCAP – Gram’s Stain of SputumGood sputum samples is obtained only from 39%
83% show only one predominant organism
36
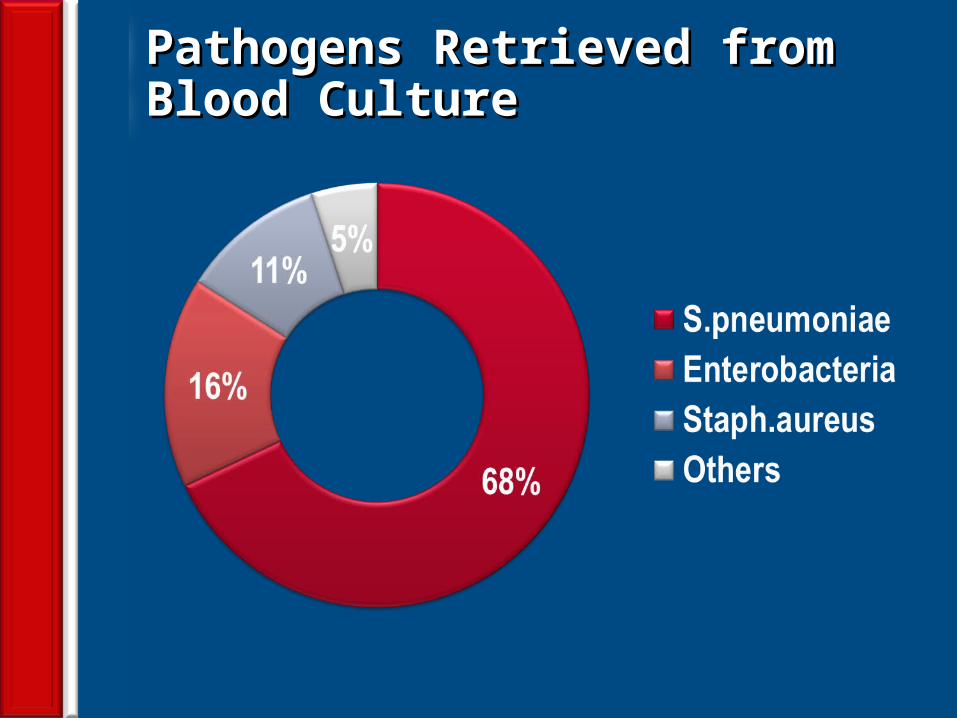
Pathogens Retrieved from Blood CulturePathogens Retrieved from Blood Culture
37
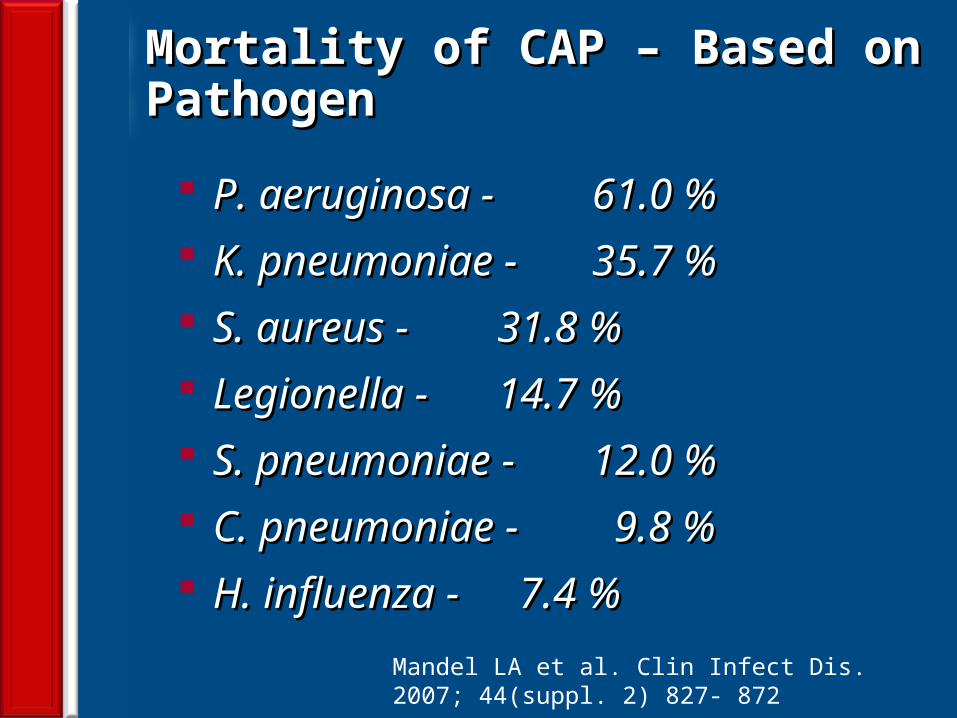
Mortality of CAP – Based on Pathogen Mortality of CAP – Based on Pathogen
P. aeruginosa - P. aeruginosa - 61.0 %61.0 % K. pneumoniae - K. pneumoniae - 35.7 %35.7 % S. aureus - S. aureus - 31.8 %31.8 % Legionella -Legionella - 14.7 %14.7 % S. pneumoniae - S. pneumoniae - 12.0 %12.0 % C. pneumoniae - C. pneumoniae - 9.8 % 9.8 % H. influenza - H. influenza - 7.4 % 7.4 %
Mandel LA et al. Clin Infect Dis. 2007; 44(suppl. 2) 827- 872
38
Traditional Treatment ParadigmTraditional Treatment Paradigm
Conservative start with ‘workhorse’ antibiotics
Reserve more potent drugs for non-responders
39
New Treatment ParadigmNew Treatment Paradigm
Hit hard and early with appropriate antibiotic(s)
Short Rx. Duration; De-escalate where possible
40
Objective 2Objective 2Objective 1Objective 1
Avoid emergence ofAvoid emergence ofmultidrug resistantmultidrug resistantmicroorganismsmicroorganisms Immediate Rx.Immediate Rx.
of patients with of patients with serious sepsisserious sepsis
The Therapy ConundrumThe Therapy Conundrum
41
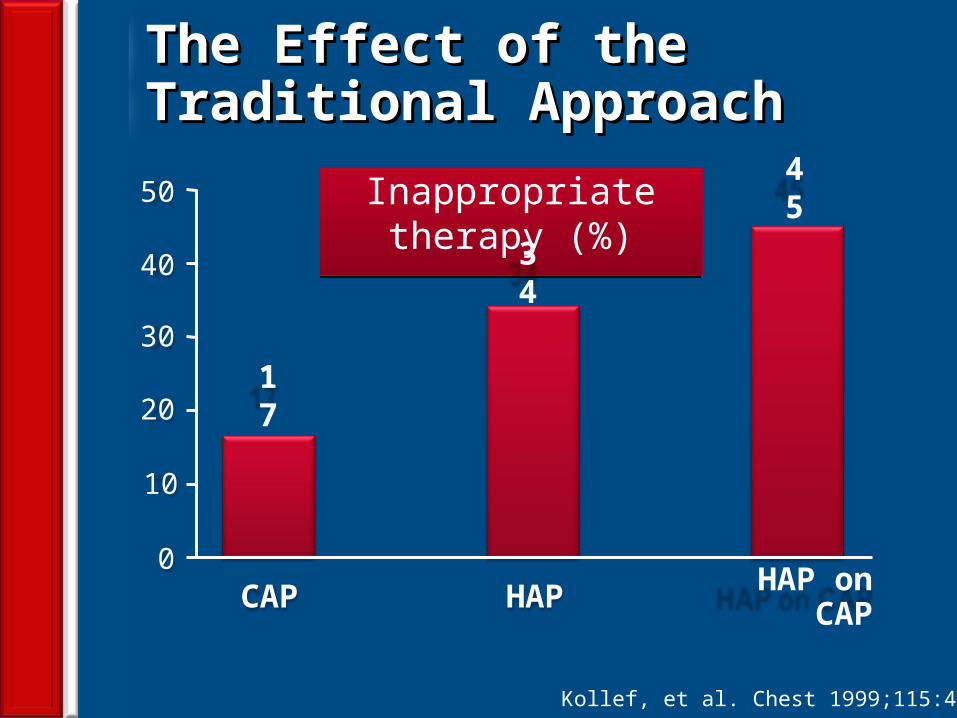
Inappropriate therapy (%)
0
30
50
10
CAP
20
40
HAP HAP on CAP
17
34
45
Kollef, et al. Chest 1999;115:462–474
The Effect of the Traditional ApproachThe Effect of the Traditional Approach
42
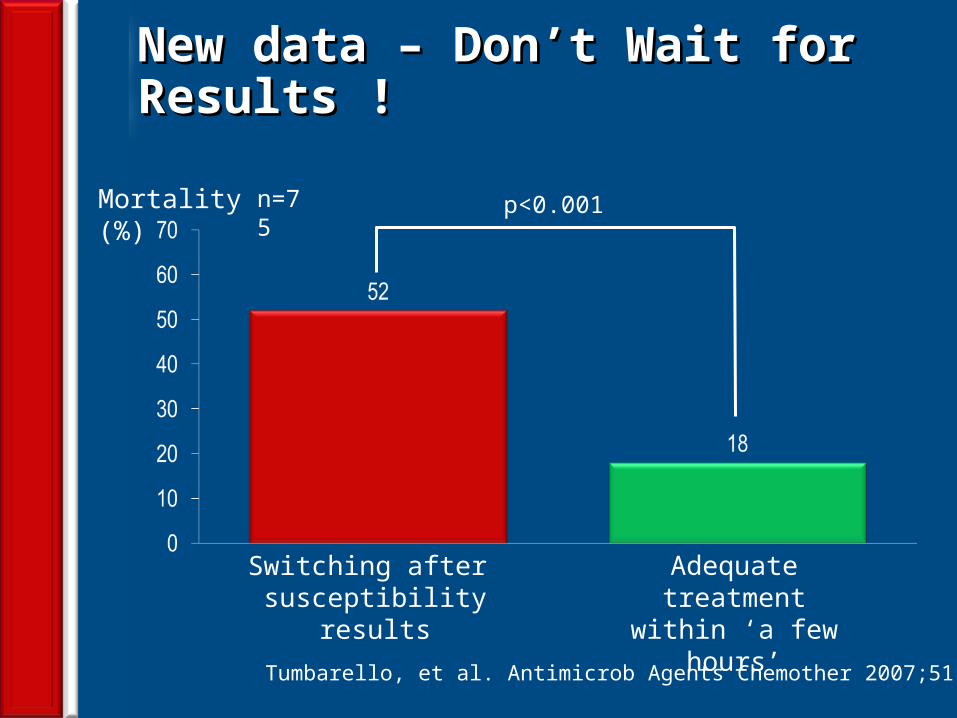
New data – Don’t Wait for Results !New data – Don’t Wait for Results !
Switching after susceptibility results
p<0.001
Adequate treatment within ‘a few hours’
Mortality (%) n=75
Tumbarello, et al. Antimicrob Agents Chemother 2007;51:1987–1994
43
Risk assessment approachRisk assessment approach Early Antibiotic selectionEarly Antibiotic selection Change treatment driven by local Change treatment driven by local
surveillancesurveillance Hit hard and hit earlyHit hard and hit early As short a duration as possibleAs short a duration as possible De-escalate when and where possibleDe-escalate when and where possible
CAP Treatment ConsensusCAP Treatment Consensus

44
OPAT – OP Parenteral Antimicrobial TherapyOPAT – OP Parenteral Antimicrobial Therapy
45
Antibiotics of choice for CAPAntibiotics of choice for CAP
46
Empiric Treatment – OutpatientEmpiric Treatment – Outpatient
Healthy and no risk factors for DR Healthy and no risk factors for DR S.pneumoniae S.pneumoniae 1. Macrolide or Doxycycline1. Macrolide or DoxycyclinePresence of co-morbidities, use of antimicrobialsPresence of co-morbidities, use of antimicrobialswithin the previous 3 months, and regions with a within the previous 3 months, and regions with a high rate (>25%) of infection with Macrolidehigh rate (>25%) of infection with Macrolideresistant resistant S. pneumoniaeS. pneumoniae1. Respiratory FQ – Moxiflox, Gemiflox or Levoflox1. Respiratory FQ – Moxiflox, Gemiflox or Levoflox2. Beta-lactam (High dose Amoxicillin,2. Beta-lactam (High dose Amoxicillin, Amoxicillin- Amoxicillin-
Clavulanate is preferred; Ceftriaxone, Cefpodoxime, Clavulanate is preferred; Ceftriaxone, Cefpodoxime, Cefuroxime) Cefuroxime) plus plus a Macrolidea Macrolide or Doxycycline or Doxycycline
47
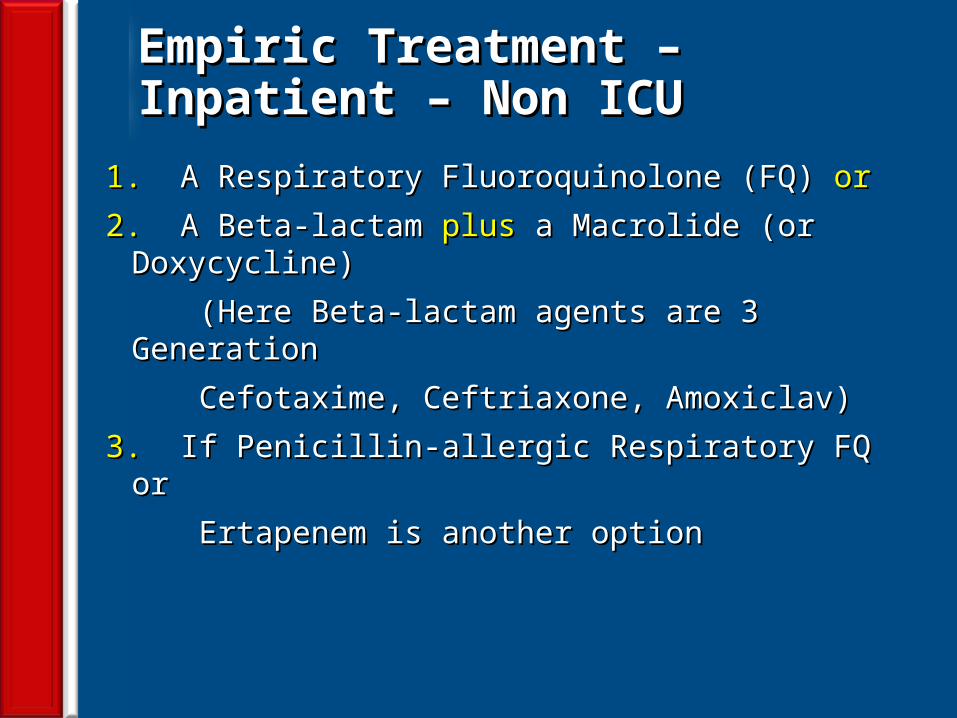
Empiric Treatment – Inpatient – Non ICUEmpiric Treatment – Inpatient – Non ICU
1. 1. A Respiratory Fluoroquinolone (FQ) A Respiratory Fluoroquinolone (FQ) oror
2. 2. A Beta-lactam A Beta-lactam plusplus a Macrolide (or Doxycycline) a Macrolide (or Doxycycline)
(Here Beta-lactam agents are 3 Generation (Here Beta-lactam agents are 3 Generation
Cefotaxime, Ceftriaxone, Amoxiclav)Cefotaxime, Ceftriaxone, Amoxiclav)
3. 3. If Penicillin-allergic Respiratory FQ orIf Penicillin-allergic Respiratory FQ or
Ertapenem is another optionErtapenem is another option
48
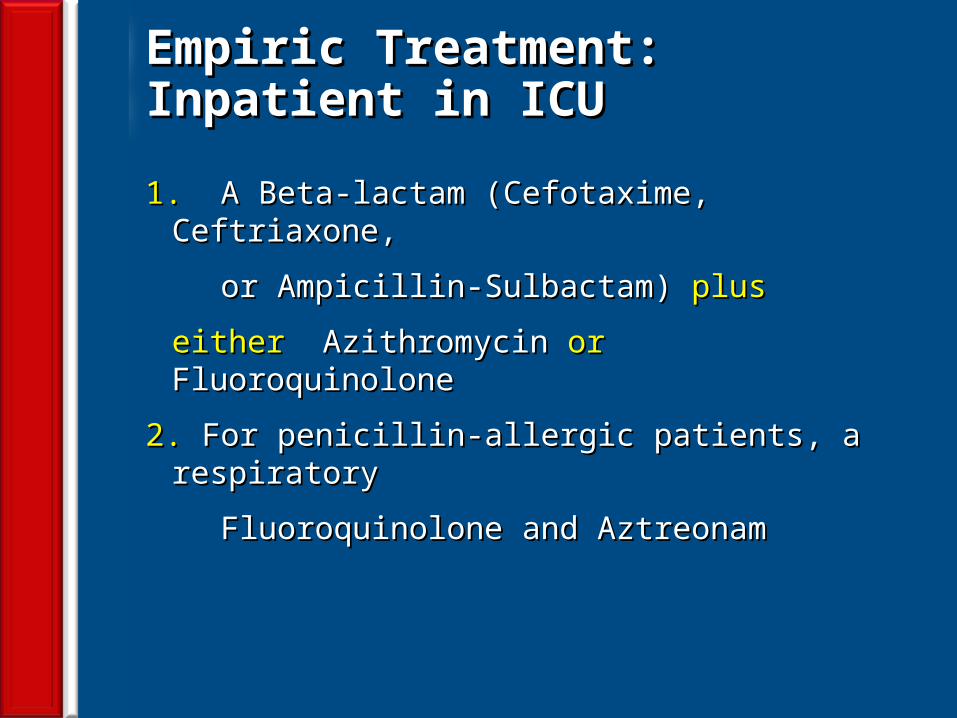
Empiric Treatment: Inpatient in ICUEmpiric Treatment: Inpatient in ICU
1. 1. A Beta-lactam (Cefotaxime, Ceftriaxone,A Beta-lactam (Cefotaxime, Ceftriaxone,
or Ampicillin-Sulbactam) or Ampicillin-Sulbactam) plusplus
eithereither Azithromycin Azithromycin oror Fluoroquinolone Fluoroquinolone
2. 2. For penicillin-allergic patients, a respiratoryFor penicillin-allergic patients, a respiratory
Fluoroquinolone and AztreonamFluoroquinolone and Aztreonam
49
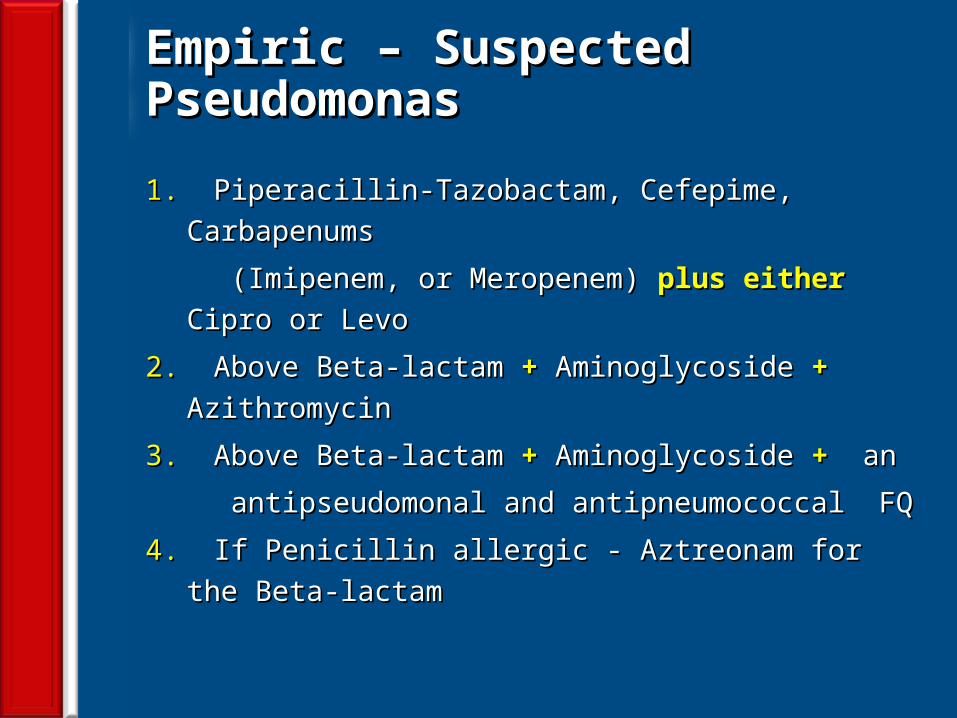
Empiric – Suspected PseudomonasEmpiric – Suspected Pseudomonas
1. 1. Piperacillin-Tazobactam, Cefepime, Carbapenums Piperacillin-Tazobactam, Cefepime, Carbapenums
(Imipenem, or Meropenem) (Imipenem, or Meropenem) plus either plus either Cipro or LevoCipro or Levo
2. 2. Above Beta-lactam Above Beta-lactam ++ Aminoglycoside Aminoglycoside ++ Azithromycin Azithromycin
3. 3. Above Beta-lactam Above Beta-lactam + + Aminoglycoside Aminoglycoside + + an an
antipseudomonal and antipneumococcal FQantipseudomonal and antipneumococcal FQ
4. 4. If Penicillin allergic - Aztreonam for the Beta-lactamIf Penicillin allergic - Aztreonam for the Beta-lactam
50
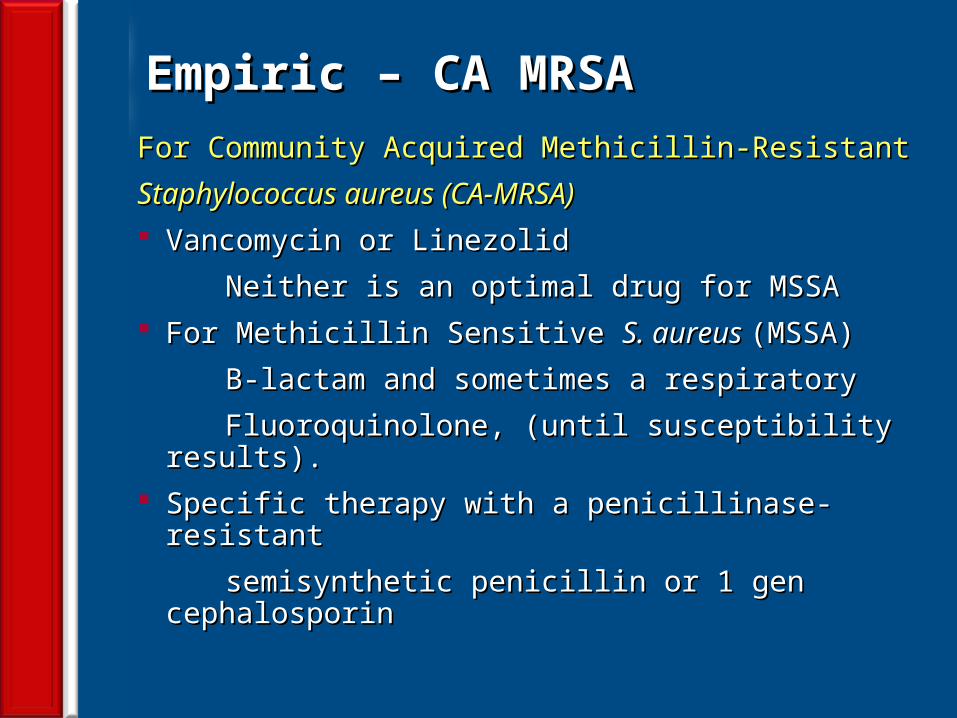
Empiric – CA MRSAEmpiric – CA MRSAFor Community Acquired Methicillin-ResistantFor Community Acquired Methicillin-Resistant
Staphylococcus aureus (CA-MRSA)Staphylococcus aureus (CA-MRSA) Vancomycin or LinezolidVancomycin or Linezolid
Neither is an optimal drug for MSSANeither is an optimal drug for MSSA For Methicillin Sensitive For Methicillin Sensitive S. aureus S. aureus (MSSA)(MSSA)
B-lactam and sometimes a respiratoryB-lactam and sometimes a respiratory
Fluoroquinolone, (until susceptibility results).Fluoroquinolone, (until susceptibility results). Specific therapy with a penicillinase-resistantSpecific therapy with a penicillinase-resistant
semisynthetic penicillin or 1 gen cephalosporinsemisynthetic penicillin or 1 gen cephalosporin
51
Duration of TherapyDuration of Therapy
• Minimum of 5 daysMinimum of 5 days• Afebrile for at least 48 to 72 hAfebrile for at least 48 to 72 h• No > 1 CAP-associated sign of clinical instabilityNo > 1 CAP-associated sign of clinical instability• Longer duration of therapy Longer duration of therapy
If initial therapy was not active against the identified If initial therapy was not active against the identified
pathogen or complicated by extra pulmonary infectionpathogen or complicated by extra pulmonary infection
52
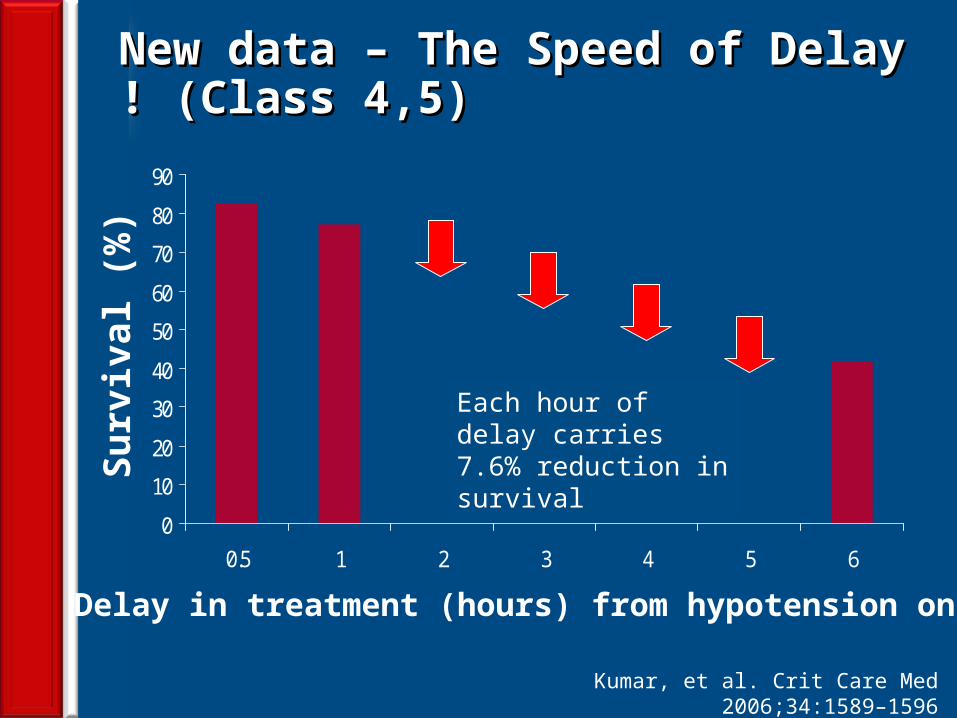
New data – The Speed of Delay ! (Class 4,5)New data – The Speed of Delay ! (Class 4,5)
0
10
20
30
40
50
60
70
80
90
0.5 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Surv
ival
(%)
Each hour of delay carries 7.6% reduction in survival
Kumar, et al. Crit Care Med 2006;34:1589–1596
53
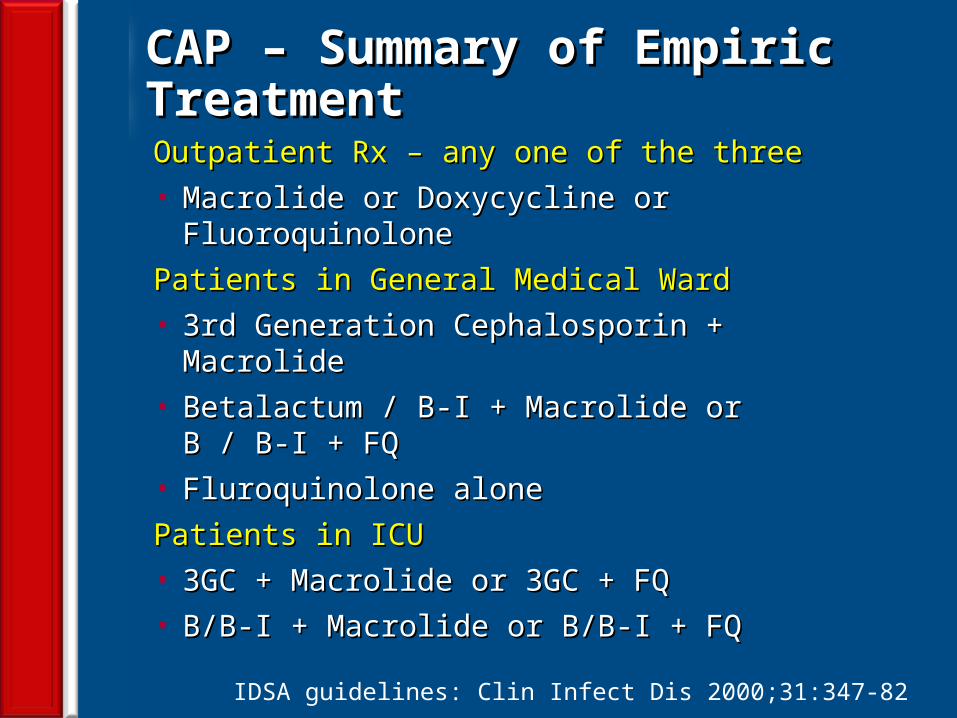
CAP – Summary of Empiric TreatmentCAP – Summary of Empiric Treatment
Outpatient Rx – any one of the threeOutpatient Rx – any one of the three• Macrolide or Doxycycline or FluoroquinoloneMacrolide or Doxycycline or Fluoroquinolone
Patients in General Medical WardPatients in General Medical Ward• 3rd Generation Cephalosporin + Macrolide3rd Generation Cephalosporin + Macrolide• Betalactum / B-I + Macrolide or B / B-I + FQBetalactum / B-I + Macrolide or B / B-I + FQ• Fluroquinolone aloneFluroquinolone alone
Patients in ICUPatients in ICU• 3GC + Macrolide or 3GC + FQ3GC + Macrolide or 3GC + FQ• B/B-I + Macrolide or B/B-I + FQB/B-I + Macrolide or B/B-I + FQ
IDSA guidelines: Clin Infect Dis 2000;31:347-82
54
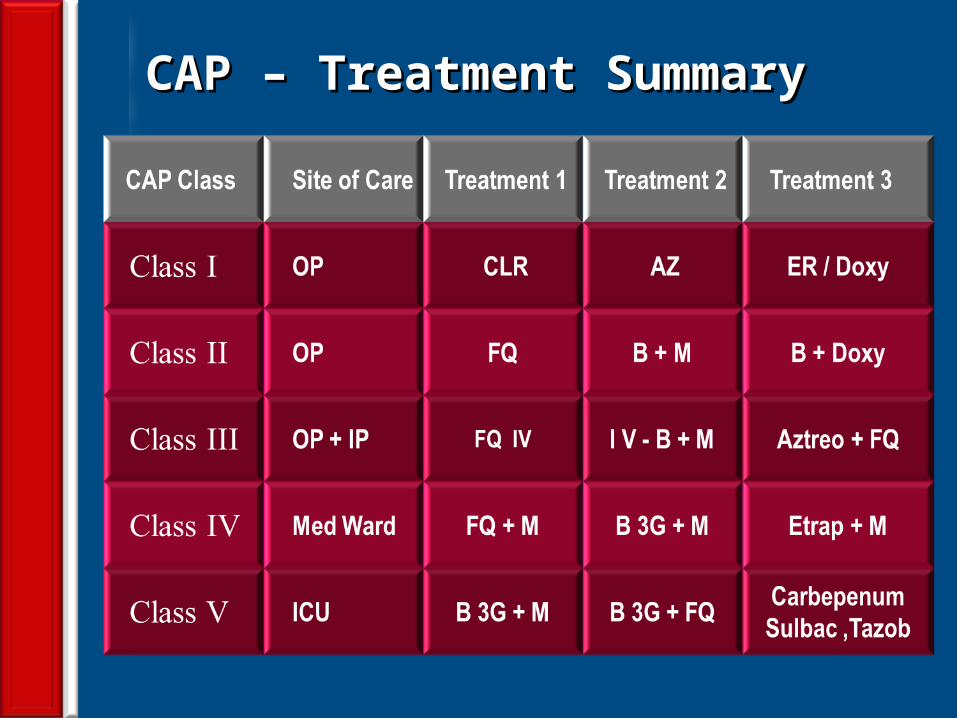
CAP – Treatment SummaryCAP – Treatment Summary
55
Recommendations: Empirical antibiotic Recommendations: Empirical antibiotic choice for CAP treated in the communitychoice for CAP treated in the community
• Amoxicillin is the preferred agent to initiate empiric antibiotic OP Rx.
• Macrolides, Clarithromycin and Azithromycin for pts hypersensitive to Penicillin.
• TB is endemic in India - Macrolides such as Clarithromycin and Azithromycin may be preferred to quinolones/doxycycline as the initial empiric therapy.
• Pathogens causing CAP are resistant to Doxycycline. Hence it is not recommended.
• If co-morbidities are present a respiratory Fluoroquinolone or a β-lactam plus a macrolide or Amoxicillin–Clavulanate is preferred.
56
Strategies for Prevention of CAPStrategies for Prevention of CAP• Cessation smokingCessation smoking• Influenza Vaccine (Flu shot – Oct through Feb)Influenza Vaccine (Flu shot – Oct through Feb)
It offers 90% protection and reduces mortality by 80%It offers 90% protection and reduces mortality by 80%• Pneumococcal Vaccine (Pneumonia shot)Pneumococcal Vaccine (Pneumonia shot)
It protects against 23 types of PneumococciIt protects against 23 types of Pneumococci
70% of us have Pneumococci in our RT70% of us have Pneumococci in our RT
It is not 100% protective but reduces mortalityIt is not 100% protective but reduces mortality
Age 19-64 with co morbidity of high for pneumoniaAge 19-64 with co morbidity of high for pneumonia
Above 65 all must get it even without high riskAbove 65 all must get it even without high risk
• Starting first dose of antibiotic with in 4 h & OStarting first dose of antibiotic with in 4 h & O22 status status
57
Switch to Oral TherapySwitch to Oral Therapy
Four criteriaFour criteria Improvement in cough, dyspnea & clinical signsImprovement in cough, dyspnea & clinical signs Afebrile on two occasions 8 h apartAfebrile on two occasions 8 h apart WBC decreasing towards normalWBC decreasing towards normal Functioning GI tract with adequate oral intakeFunctioning GI tract with adequate oral intake
If overall clinical picture is otherwise favorable, If overall clinical picture is otherwise favorable, hemodynamically stable; can switch to oral hemodynamically stable; can switch to oral therapy while still febrile.therapy while still febrile.
58
Management of Poor RespondersManagement of Poor Responders
Consider non-infectious illnessesConsider non-infectious illnesses Consider less common pathogensConsider less common pathogens Consider TuberculosisConsider Tuberculosis Consider serologic testingConsider serologic testing Broaden antibiotic therapyBroaden antibiotic therapy Consider bronchoscopyConsider bronchoscopy
59
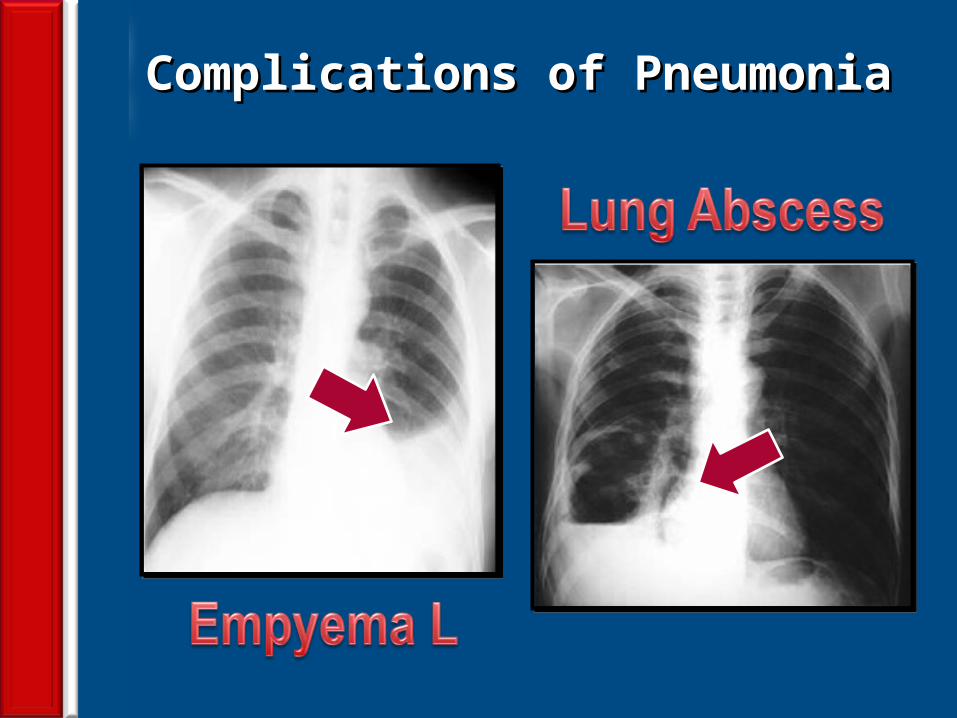
CAP – ComplicationsCAP – Complications
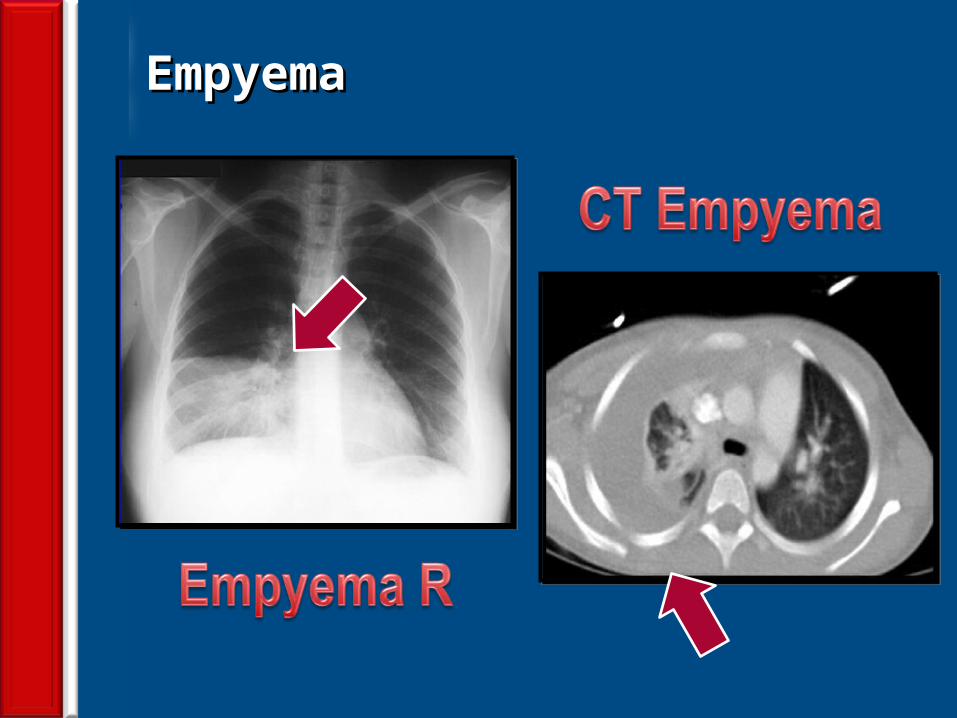
Hypotension and septic shockHypotension and septic shock 3-5% Pleural effusion; Clear fluid + pus cells3-5% Pleural effusion; Clear fluid + pus cells 1% Empyema thoraces pus in the pleural space 1% Empyema thoraces pus in the pleural space Lung abscess – destruction of lung - CSLDLung abscess – destruction of lung - CSLD Single (aspiration) anaerobes, Single (aspiration) anaerobes, PseudomonasPseudomonas Multiple (metastatic) Multiple (metastatic) Staphylococcus aureusStaphylococcus aureus Septicemia – Brain abscess, Liver AbscessSepticemia – Brain abscess, Liver Abscess Multiple Pyemic AbscessesMultiple Pyemic Abscesses
60
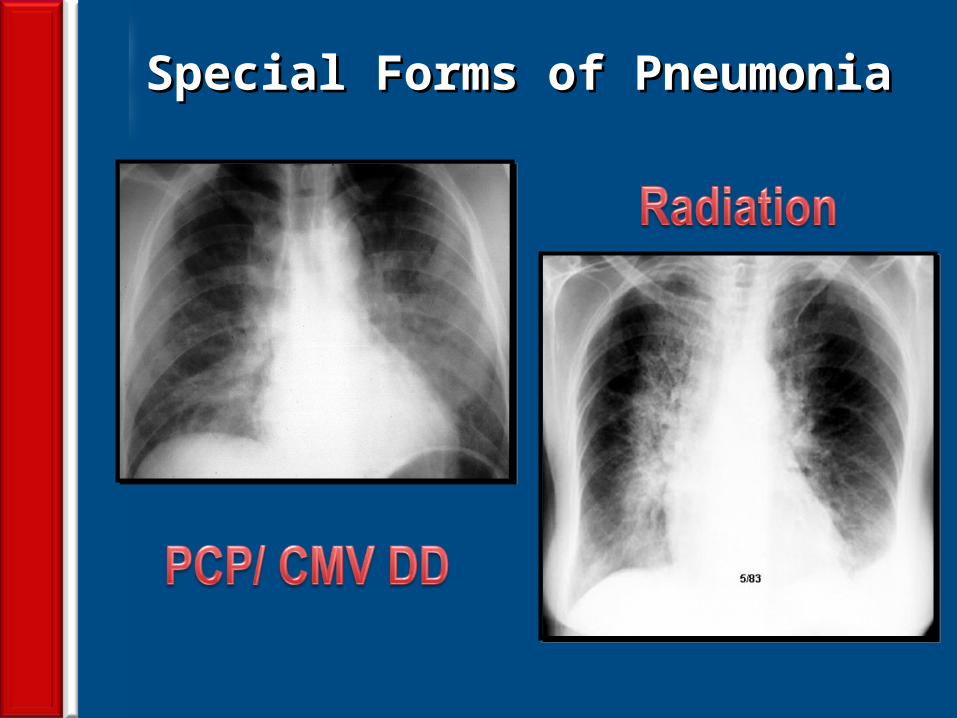
Pneumocystis carinii (PCP)Pneumocystis carinii (PCP)
Important cause of pneumonia in the severelyImportant cause of pneumonia in the severely
immuno-compromised, i.e. not a “primary atypicalimmuno-compromised, i.e. not a “primary atypical
pneumonia”.pneumonia”. Classically PCP pneumonia presents with slight fever,Classically PCP pneumonia presents with slight fever,
dyspnea and non-productive coughdyspnea and non-productive cough Diagnosis – usually histological (silver staining).Diagnosis – usually histological (silver staining). Treatment – Co-trimoxazole or Pentamidine.Treatment – Co-trimoxazole or Pentamidine.
61
Viruses and PneumoniaViruses and Pneumonia
Pneumonia in the normal hostPneumonia in the normal host
• Adults or ChildrenAdults or Children
• Influenza A and B, RSV, Adenovirus Para InfluenzaInfluenza A and B, RSV, Adenovirus Para Influenza
Pneumonia in the immuno-compromisedPneumonia in the immuno-compromised
• Measles, HSV, CMV, HHV-6, Influenza virusesMeasles, HSV, CMV, HHV-6, Influenza viruses
• Can cause a primary viral pneumonia. Cause partial Can cause a primary viral pneumonia. Cause partial paralysis of “mucociliary escalator” - increased risk of paralysis of “mucociliary escalator” - increased risk of secondary bacterial LRTI. secondary bacterial LRTI. S.aureus pneumonia S.aureus pneumonia is a is a known complication following influenza infection.known complication following influenza infection.
62
CAP – So How Best to Win the War?CAP – So How Best to Win the War?
Early antibiotic administration within 4-6 hoursEarly antibiotic administration within 4-6 hours Empiric antibiotic Rx. as per guidelines (IDSA / ATS)Empiric antibiotic Rx. as per guidelines (IDSA / ATS) PORT or CURB scoring and Classification of casesPORT or CURB scoring and Classification of cases Early hospitalization in Class IV and VEarly hospitalization in Class IV and V Change Abx. as per pathogen & sensitivity patternChange Abx. as per pathogen & sensitivity pattern Decrease smoking cessation advice / counselingDecrease smoking cessation advice / counseling Arterial oxygenation assessment in the first 24 hArterial oxygenation assessment in the first 24 h Blood culture collection in the first 24 h prior to Abx.Blood culture collection in the first 24 h prior to Abx. Pneumococcal & Influenza vaccination; Smoking Pneumococcal & Influenza vaccination; Smoking XX
63
Normal CXR & Pneumonic ConsolidationNormal CXR & Pneumonic Consolidation
64
Lobar Pneumonia – S.pneumoniaeLobar Pneumonia – S.pneumoniae
65
CXR – PA and Lateral ViewsCXR – PA and Lateral Views
66
Lobar versus Segmental - Right SideLobar versus Segmental - Right Side
67
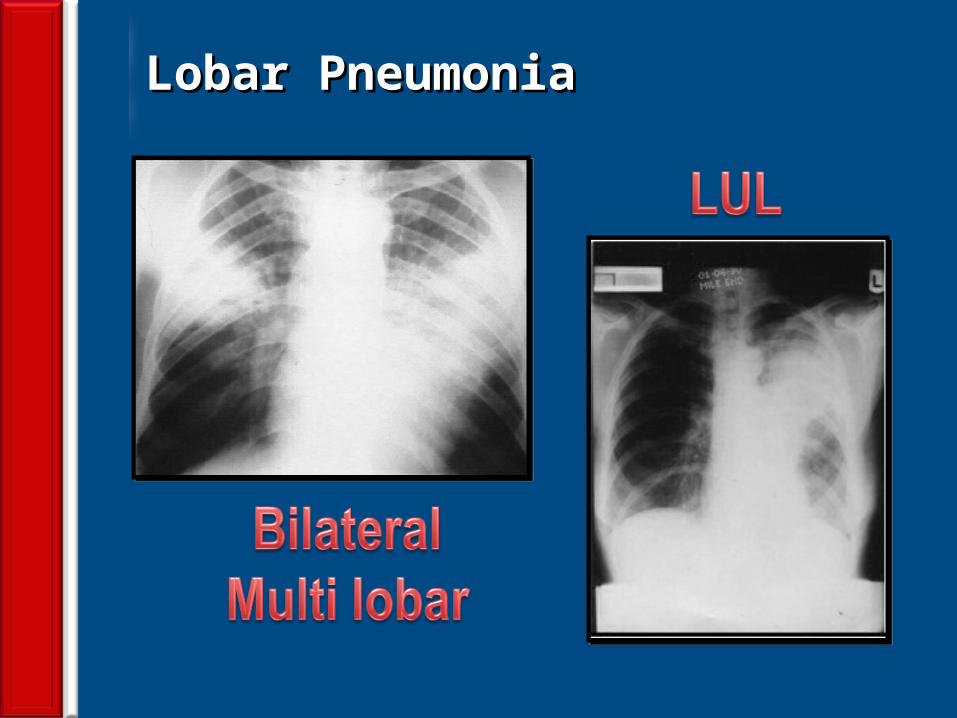
Lobar PneumoniaLobar Pneumonia
68
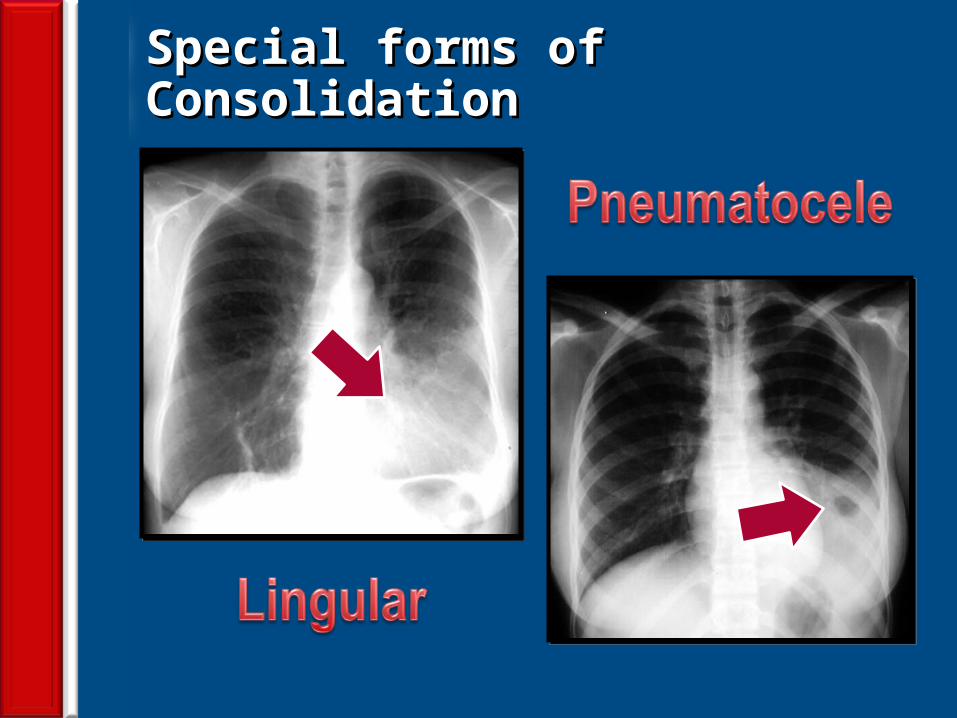
Special forms of ConsolidationSpecial forms of Consolidation
69
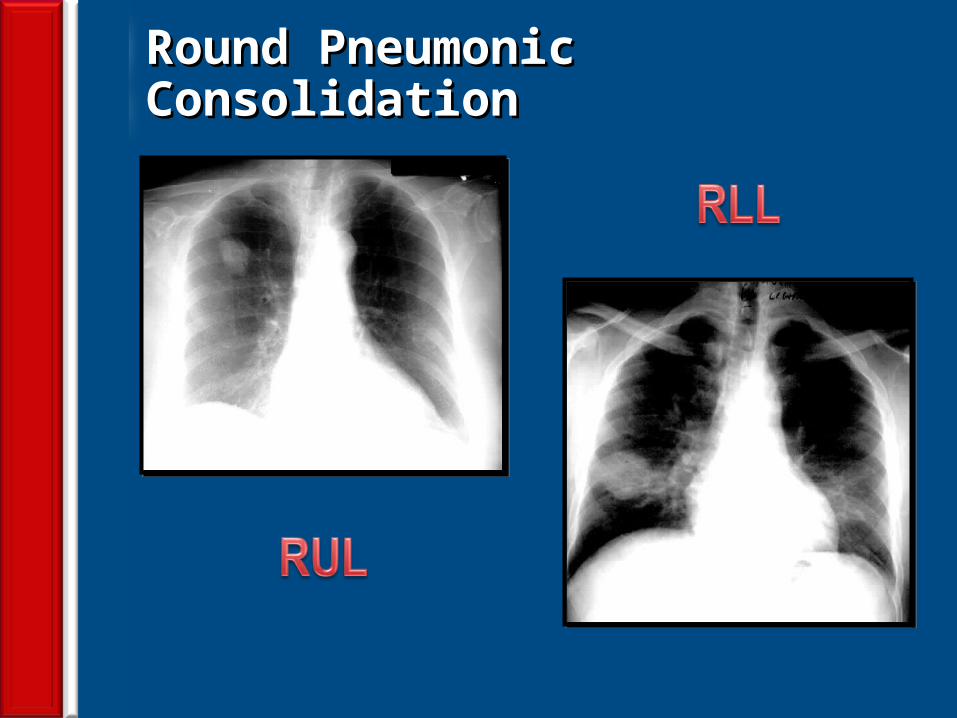
Round Pneumonic ConsolidationRound Pneumonic Consolidation
70
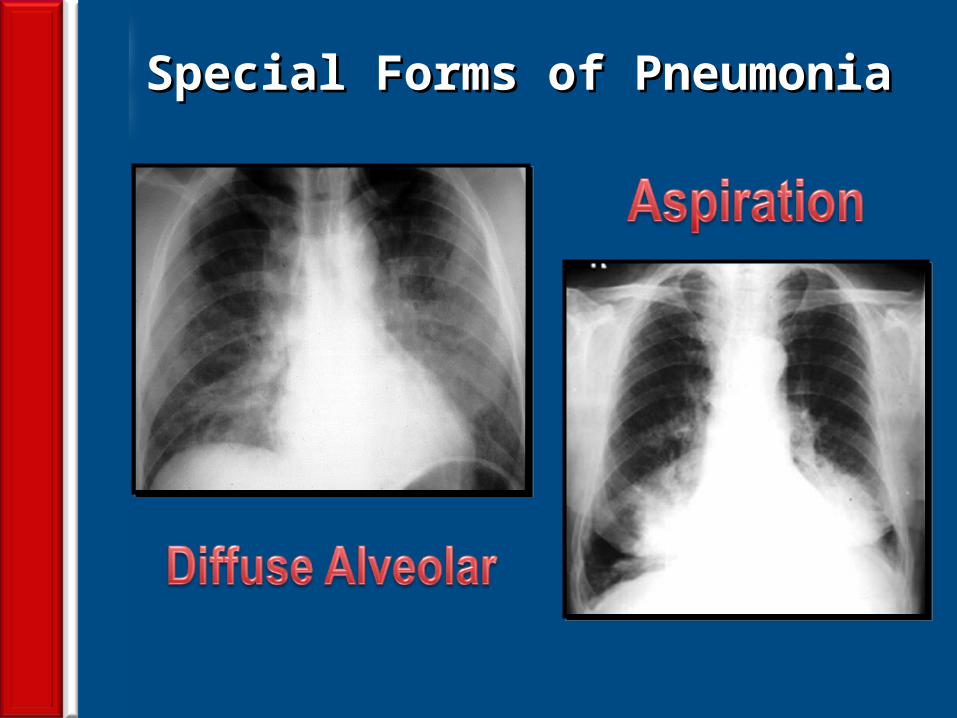
Special Forms of PneumoniaSpecial Forms of Pneumonia
71
Special Forms of PneumoniaSpecial Forms of Pneumonia
72
Complications of PneumoniaComplications of Pneumonia
73
EmpyemaEmpyema
74
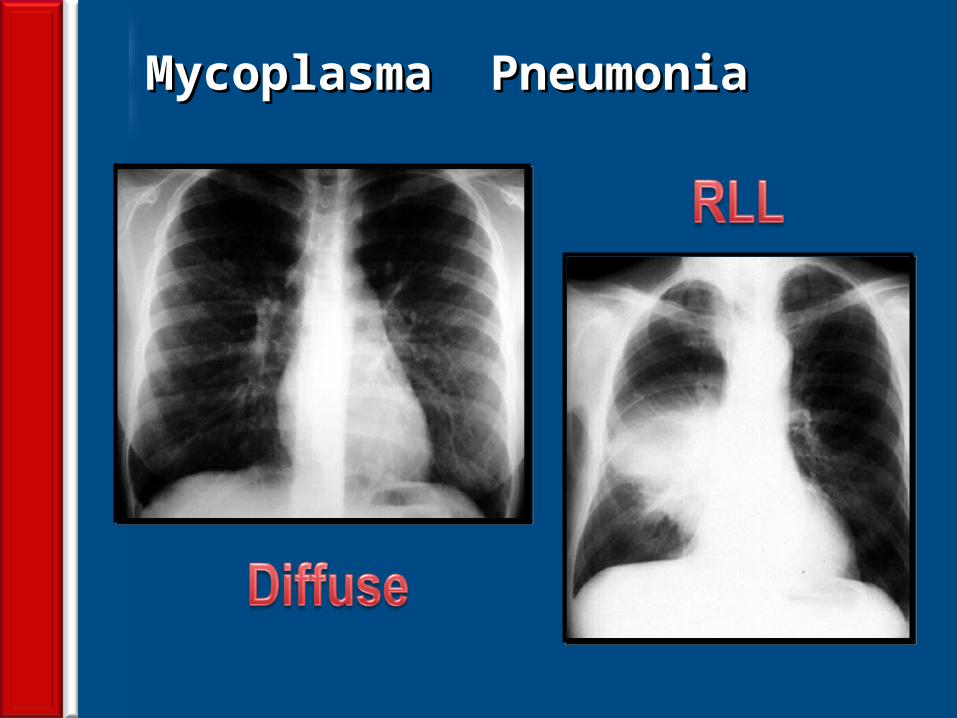
Mycoplasma Pneumonia Mycoplasma Pneumonia
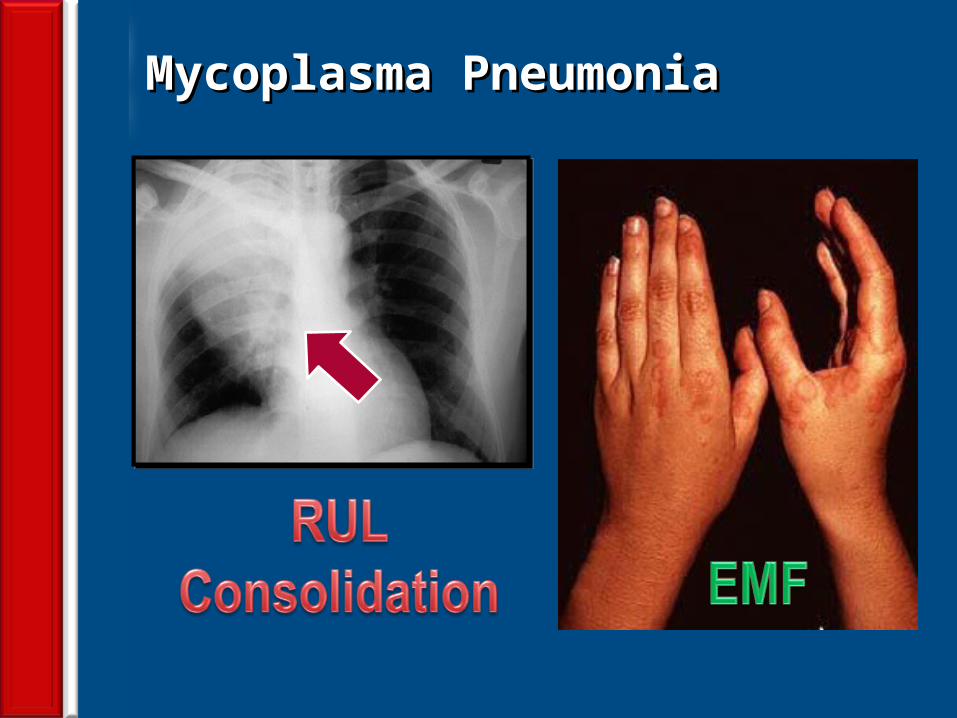
75
Mycoplasma PneumoniaMycoplasma Pneumonia
76
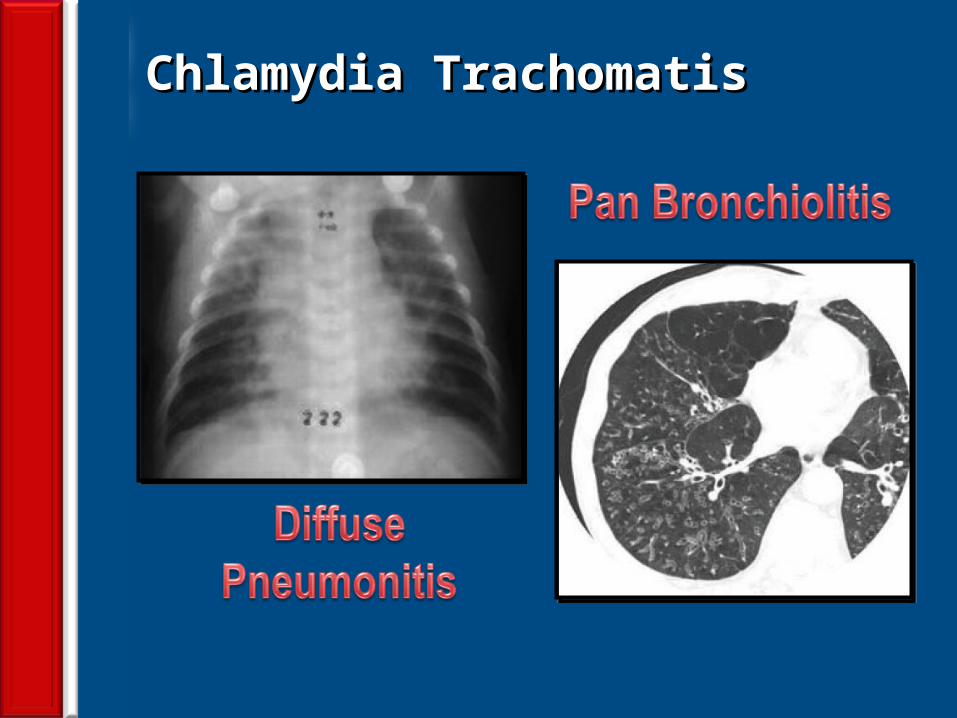
Chlamydia TrachomatisChlamydia Trachomatis
77
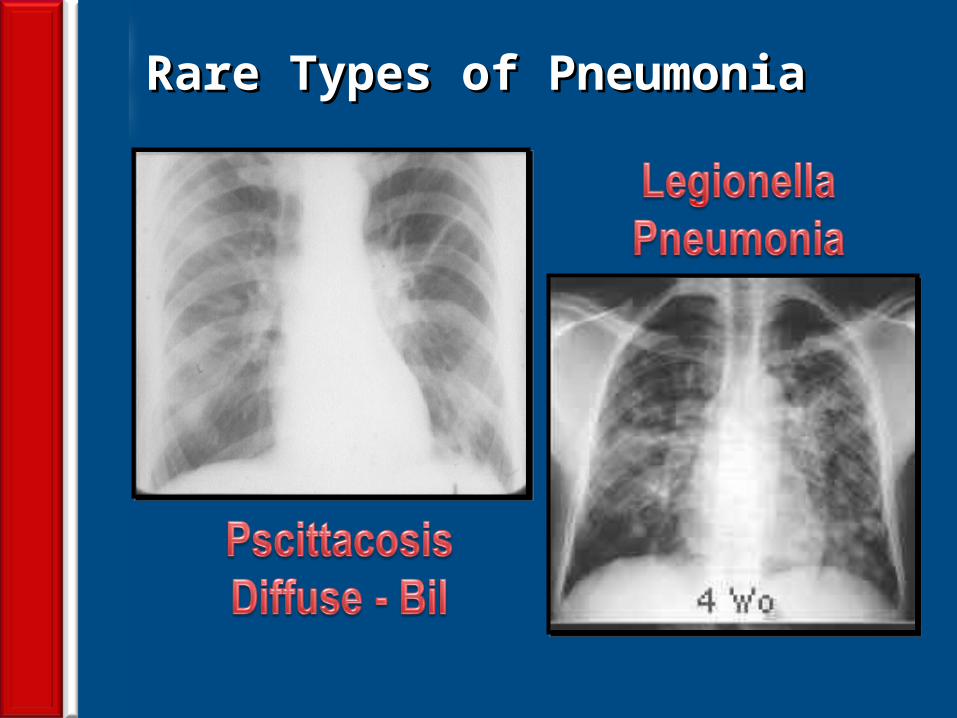
Rare Types of PneumoniaRare Types of Pneumonia
Visit our website: www.drsarma.inVisit our website: www.drsarma.in
YouTube: drsarmajiYouTube: drsarmaji





![Community acquired pneumonia [cap] in children](https://static.fdocuments.in/doc/165x107/5454e4c4af795946778b8712/community-acquired-pneumonia-cap-in-children.jpg)












