COMMON SHOULDER PROBLEMS IN THE 21ST … · · 2014-08-22COMMON SHOULDER PROBLEMS IN THE 21ST...
69
COMMON SHOULDER PROBLEMS IN THE 21 ST CENTURY Mr Ali Noorani MBBS BSc (Hons) MRCS FRCS (Trauma & Orth) Consultant Trauma & Orthopaedic Surgeon at St Bartholomew’s & The Royal London Hospital Upper Limb Service The London Sports Injury Clinic, 108 Harley Street
Transcript of COMMON SHOULDER PROBLEMS IN THE 21ST … · · 2014-08-22COMMON SHOULDER PROBLEMS IN THE 21ST...

COMMON SHOULDER PROBLEMS IN THE 21ST CENTURY
Mr Ali Noorani MBBS BSc (Hons) MRCS FRCS (Trauma & Orth)
Consultant Trauma & Orthopaedic Surgeon at
St Bartholomew’s & The Royal London Hospital
Upper Limb Service
The London Sports Injury Clinic, 108 Harley Street

• Upper Limb Surgery & Rehabilitation is a “team sport” & requires a MDT approach
2

3

Common Shoulder Problems
• Common Shoulder Problems
– Instability – Impingement – Frozen Shoulder – Rotator Cuff Disease – Arthritis
• Assessment & Diagnosis
• Treatment in 1° and 2° care
4

Shoulder Symptoms
5
PAIN
STIFF
WEAK
INSTABILITY

Age & Diagnosis
• 10 to 30 Instability
Internal & Secondary Impingement
• 30 to 50 Primary Impingement Syndrome
Frozen Shoulder
• 50 to 80 Full Thickness Cuff Tears
Arthritis
6

Young Age
7

AMBRI
TUBS
Muscle
Patterning
I
II III
Matsen classification
Shoulder Instability & Stanmore Classification

Type 1 “The Rugby Player”
• Traumatic Instability
• Bankart Lesion
• Detachment of the Anteroinferior Labrum & Anterior Band of IGHL ( & MGHL)

Known Risk Factors for Recurrence
• Age ( younger at greater risk)
•16yr 85%
•21yr 69%
•30yr 40%
• Male gender ( controversial)
• Contact sports ( trending towards statistical significance)

Is there a consequence of Recurrent Dislocations?
Early
Late
Progressive Capsular Elongation
with Recurrent Dislocations
Urayama, AJSM, 2003
MRI Study
Pollack, JSES, 2000
Biomechanics study
Habermeyer
Longitudinal Study of Tissue
Trauma
Progressive damage to Labrum,
Cartilage, Glenoid Rim & Capsule
Yanniakopoulos et al (2007)
Acute (A) vs
Chronic (C)
Hill-Sachs Lx: A= 65% C= 93%
Bankart: A= 78% C= 97%
Capsular Laxity: A= 9% C= 30%
Inverted Pear
(Glenoid Erosion): A= 0% C- 15%

Bankart Lx ALPSA Lx
67 patients
3.2 anchors used
F/U 46 Months
Recurrence rate = 7%
26 patients
3.6 anchors used
F/U 48 Months
Recurrence rate = 19%
Chronicity affects tissue & Recurrence rate….
Ozbaydar M et al: Results of Arthroscopic Capsulolabral Repair: Bankart
Lesion Versus anterior labroligamentous
Periosteal sleeve avulsion lesion.
Arthroscopy, 2008

Early Intervention Rationale
• 3 major concerns established:
• Risk of Recurrence Unacceptably High in Young, Male, Athletic population
• Significant Soft Tissue & Bone Trauma
sustained with Instability Episodes • Quality of Life improved with early
stabilization vs. non-operative group

Clinical Evaluation
• History

Clinical Evaluation
• History – Direction of Instability – Aetiology (Trauma at 1st Dislocation & Subsequent
Instability – Frequency – Degree of Instability – Arm position that elicits Instability & Pain – AGE
–< 40 Bankart/ Hill-Sachs –> 40 Cuff Tear / GT Fracture

Clinical Evaluation
• History
• Examination

Clinical Evaluation
• History
• Examination
– Beighton score
– Sulcus
– Anterior and Posterior Apprehension Test
– Jobe relocation test
– Anterior/Posterior drawer
– Gagey hyperabduction test
– Load-shift test

“Hyperlaxity” > 90o ER
Rev Chir Orthop 1995
105° 130°
Hyperabduction test of Gagey (JBJS 2001) > 20o between sides (Boileau Rev Chir Orthop 1999)

Clinical Evaluation
• History
• Examination
• Investigations

Clinical Evaluation
• History
• Examination
• Investigations
– Plain radiographs – AP/Velpeau /Stryker/ Bernageau view
– MRI A
– CT (3D)

Treatment
• Non-surgical

Treatment
• Non-surgical
– Acute – Reduce & Immobilsation – IR or ER
• Miller AOSSM 2006 IR 25% vs ER 26% recurrence
• Itoi JBJS 2007 (Level 1) IR 42% vs ER 26% recurrence)
– Dynamic Rotator Cuff / Periscapular Strengthening

Treatment
• Non-surgical
• Surgical

Treatment
• Non-surgical
• Surgical
– Arthroscopic ( mainly soft tissue Bankart Repair)
Vs
– Open ( mainly Bone work e.g Latarjet )

Middle Age
25

Middle Age
• Frozen Shoulder
• Primary Impingement Syndrome
26

“Frozen Shoulder” Codman 1934
• Slow onset ( Freezing/Frozen/Thawing Phases)
• Pain in the Deltoid Region
• Stiff ( Adhesive Capsulitis)
• Painful and Restricted External Rotation and Elevation (Passive)
• Associated with Diabetes & Dupuytrens
• Normal X ray » Consider Osteoarthritis & Dislocation

Frozen Shoulder Non Operative Treatment
• ?Physiotherapy
• GHJ Injection if very early in Disease Process

Arthroscopic Rotator Interval Release

The Impingement Syndrome Neer:JBJS 54A:41-50,1972.
• Stage 1 - Reversible oedema
• Stage 2 - Fibrosis & Tendinitis
• Stage 3 – Bone Spurs & Tendon Rupture

Classification of Impingement
• Primary – Collagen Degeneration, Vascular
Damage, Subacromial Spur, Calcium
• Secondary- Hypermobility, Muscle Imbalance,
Repeated Overhead Movements, Frozen Shoulder

Classification of Impingement

Primary Impingement Syndrome
• Symptoms • Age>35
• Pain
• Overhead Activities
• Signs • Painful Arc
• Hawkins Test Positive
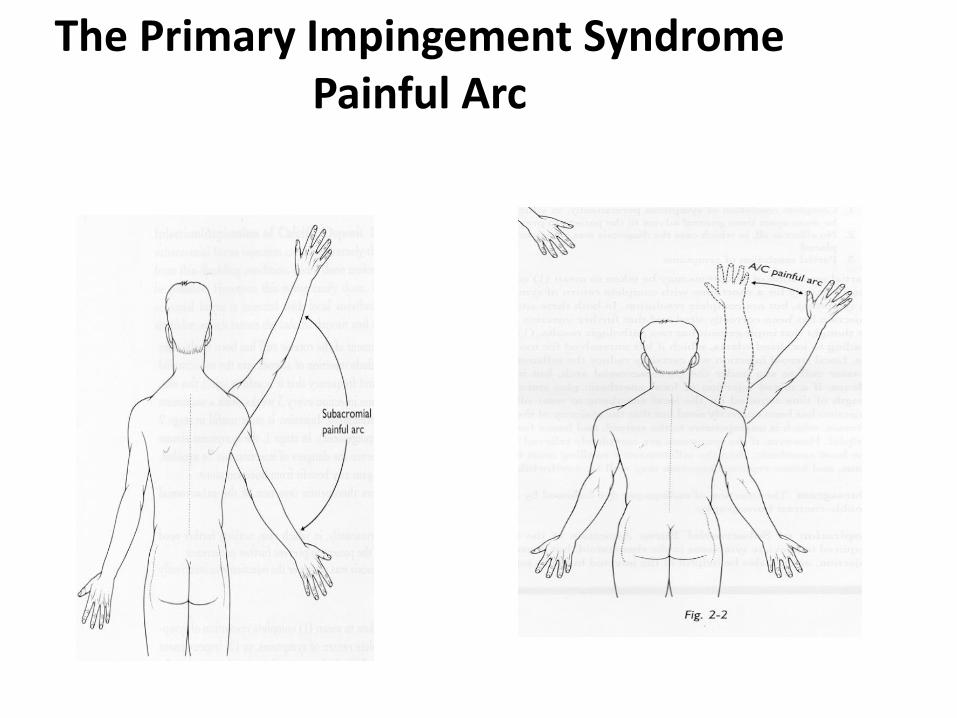
The Primary Impingement Syndrome Painful Arc

The Primary Impingement Syndrome The Hawkins Test

The Primary Impingement Syndrome Non-Operative Management
• Rehabilitation Programme
• Avoidance of Repeated Injury
• Restore Flexibilty
• Restore Strength
• Modify Work/Sport
• Steroid Injection
• One Diagnostic & Therapeutic

The Primary Impingement Syndrome Injection Technique
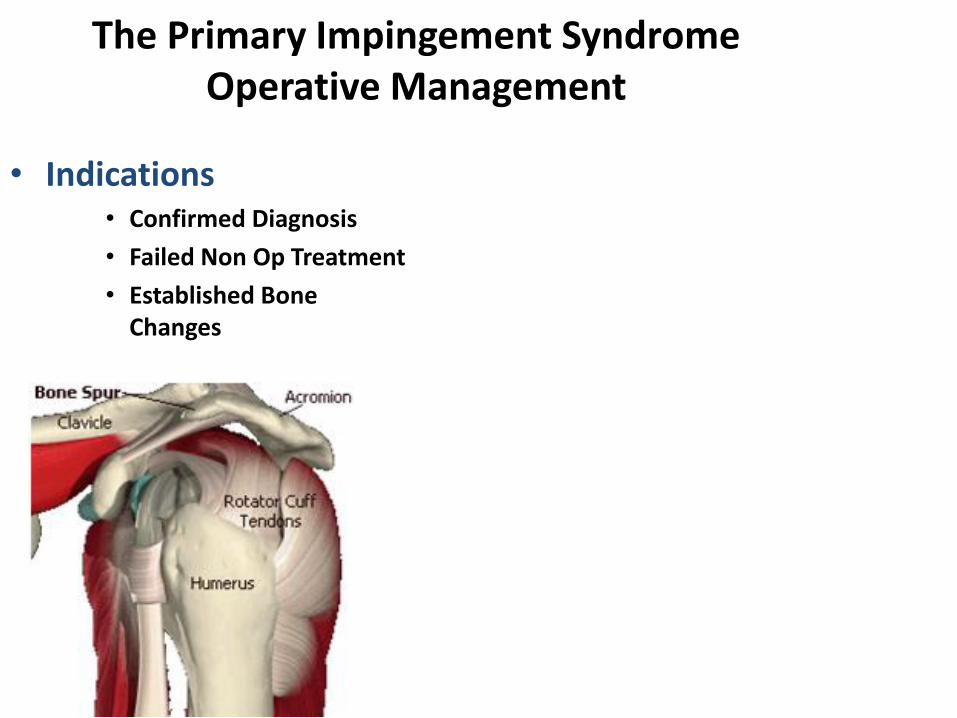
The Primary Impingement Syndrome Operative Management
• Indications • Confirmed Diagnosis
• Failed Non Op Treatment
• Established Bone Changes

Randomised Controlled Trials
• Principle Investigator in Multicentre RCTs
• Arthroscopic Subacromial Decompression with PRP
• Arthroscopic Release in Frozen Shoulder with ASAD
39

“Older” Age
40

Older Age
• Rotator Cuff Disease
• Arthritis
41

Surgical Management of the Rotator Cuff When to Repair?

The Main Ingredients

The Incidence of Rotator Cuff Tears
• Lehman et al 1995
• 235 cadavers
• Age 27y-102y
• Full thickness cuff tears present in 17%
• <60y 6%
• >60y 30%

The Incidence of Rotator Cuff Tears
• Sher et al 1995
• MRI study
• 96 Asymptomatic shoulders
• Wide age range
• 15% Full Thickness tears
• 20% Partial Thickness tears
– >60 years 54% (28% FT 26% PT)
– 40–60 years 28% (4% FT 28% PT)
– 19-39 years 4% (0% FT 4% PT

Cuff defects become increasingly common after the age of 40
years and many of these occur without substantial symptoms

Acute Tears are more likely to be Repairable and Early Repair
appears to be Advantageous in this situation

Full Thickness Rotator Cuff Tears Operative Repair
Examination
• Postacchini et al 1992
• 73 cuff repairs
• 73% satisfactory results
• Almost always successful in patients with more than 60 degrees active flexion pre operatively and either small or medium tears
• Unsatisfactory results associated with reduced motion and especially with muscle atrophy pre-operatively

Full Thickness Rotator Cuff Tears Operative Repair
Steroids
• Watson et al 1985
• 89 patients
• No steroid injection assoc with good cuff tissue
• 1- 4 steroid injections assoc with weak cuff tissue
• > 4 steroid injections assoc with very poor tissue
• Shoulders with weak cuff tissue had poorer results after repair

Full Thickness Rotator Cuff Tears Operative Repair
Litigation
• Misamore et al 1995
• 107 repairs
• 24 patients on workers compensation 79 not
• All other factors were comparable
• 54% good or excellent results in those claiming compensation
• 94% good or excellent results in those Not claiming compensation

Surgical Repair of Chronic Rotator Cuff Tears A prospective long term study
(Tear size) Cofield et al JBJS 83A Jan 2001
• 105 shoulders
• One surgeon
• Mean follow up 13 years
• Result
– excellent 68
– satisfactory 16
– unsatisfactory 21
Surgical repair of chronic rotator cuff tears A prospective long term study
Cofield et al JBJS 83A Jan 2001
• Conclusions • Tear size was the most important determinant of
outcome with regard to active motion, strength, patient satisfaction & end result
• Older age, less preoperative active motion & preoperative weakness were all associated with larger tear size

Full Thickness Rotator Cuff Tears Operative Repair
(Integrity of repair) Harryman et al JBJS 73A 1991
• Study to correlate integrity of the cuff with functional status after 105 cuff repairs
• Ultrasound based study
• 57% cuffs intact at 4 years when 2 tendons involved
• 30% cuffs intact at 4 years when 3 tendons involved
• Patients generally satisfied with surgery

Full Thickness Rotator Cuff Tears Operative Repair
Harryman et al JBJS 73A 1991
• Conclusions
• Integrity of the cuff at the time of follow up was the major determinant of functional outcome and not the size of tear
• Chances of a large tear remaining intact were less than for a small tear
• Older patients tend to have larger tears

• Many factors affect the functional outcome following repair
• Tear size appears very important
• Repairs which remain intact are associated with a good outcome
• Larger tears are less likely to remain intact

Prognostic Factors in Rotator Cuff Repair The Shoulder Rockwood & Matsen 1998
Encouraging Discouraging
• <55 Years
• Acute traumatic onset
• No relation to work
• Weakness < 6 months
• No steroid injections
• Mild/mod weakness
• No atrophy
• Normal x-ray
• >65 years
• Insidious onset
• Compensation
• Weakness >6months
• Repeated injections
• Severe weakness
• Severe atrophy
• Cuff Arthropathy

Recipe for Rotator Cuff Tears
• Assessment of the patient
• History
–Age
–Onset
–Duration
– Injections
–Compensation

• Assessment of the patient
• Examination
–Muscle wasting
–Active/Passive ROM
–Weakness
–Pain
Recipe for Rotator Cuff Tears

Recipe for Rotator Cuff Tears
• Assessment of the patient
• Investigation
• AP, Axial & Outlet X-ray views
• US

• The Asymptomatic Cuff Tear DOES NOT require Treatment
• < Active ROM
• < Strength
• Pain
Recipe for Rotator Cuff Tears

• The Chronic Symptomatic Cuff Tear may be Managed Non-Operatively for 3 to 6 months
• Advice, physiotherapy, NSAID
• One or Two steroid injections only (?)
Recipe for Rotator Cuff Tears

Recipe for Rotator Cuff Tears
• Patients with Inoperable Tears are treated with a non Operative Programme or RSA

Recipe for Rotator Cuff Tears
• Patients presenting with a Traumatic History, Sudden or Progressive Weakness, are managed more Expeditiously
• Evaluate “Acute” nature of Cuff Tear
• Consider Early Repair

Recipe for Rotator Cuff Tears
• Assess each patient individually
• Consider all factors and estimate the likelihood of a successful outcome
• Explain the Nature of the Surgery and Subsequent Rehabilitation
• Give a Guarded Prognosis

Arthroscopic v Open • Pros
• Less Deltoid Disrupt
• Full Diagnosis
• ?More Rapid Recovery
• ?Improved Function
• Improved Cosmesis
• Less Infection
• Cons
• ?Technical Difficulty
• The Learning Curve
• ?Reduced security

“The Case for Surgery to Prevent Future
Problems in the Asymptomatic Patient with a Rotator Cuff Tear has Not been Convincingly
made” The Shoulder, Rockwood & Matsen,1998

Age & Diagnosis
• 10 to 30 Instability
Internal & Secondary Impingement
• 30 to 50 Primary Impingement Syndrome
Frozen Shoulder
• 50 to 80 Full Thickness Cuff Tears
Arthritis
67

1° to 2° Referral
• Early Referral for Most Shoulder Problems = Better Outcomes
• Shoulder Problems need a Diagnosis and a MDT approach
• X-ray useful in 1° ( MRI/US not so useful)
• Inject with Caution

Thank You
Mr Ali Noorani MBBS BSc (Hons) MRCS FRCS (Trauma & Orth)
Consultant Trauma & Orthopaedic Surgeon at
St Bartholomew’s & The Royal London Hospital
Upper Limb Service
The London Sports Injury Clinic, 108 Harley Street