Common Neurologic Emergencies Tamer Belal, MD,PHD Lecturer of Neurology Mansoura University...
54
-
Upload
gordon-wilcox -
Category
Documents
-
view
226 -
download
0
Transcript of Common Neurologic Emergencies Tamer Belal, MD,PHD Lecturer of Neurology Mansoura University...



Common Neurologic
EmergenciesTamer Belal, MD ,PHDLecturer of Neurology
Mansoura University Hospitals
19 April 2012
These are time sensitive situations in which effective therapy may lessen or completely reverse a potentially catastrophic insult to the central nervous system
Coma
Stroke
Status Eepilepticus

Coma

Disturbance of consciousness characterised by impaired capacity to think clearly and to perceive, respond to and remember current stimuli; there is also disorientation.
A state of much disturbed consciousness with motor restlessness, transient hallucinations, disorientation and delusions.”
A disturbance of alertness associated with psychomotor retardation.
Definitions
A state in which the patient, though not unconscious, exhibits little or no spontaneous activity.
A state of unrousable psychologic unresponsiveness in which the subject lies with eyes closed and shows no psychologically understandable response to external stimulus or inner need.
Confusion.
Delirium
Obtundation
Stupor
Coma
A 50-year-old man is found unconscious in the street. The patient is transported to the emergency department. The paramedics report that the patient is comatose with a Glasgow Coma Scale of 7 (no eye opening = 1; unintelligible sounds = 2; nonspecific withdrawal movements = 4).
His breathing was noisy, but improved with a jaw thrust maneuver. He has been placed on a backboard with spine precautions. His C-spine has been immobilized. Vital signs are 140/90, 90 pulse, 24 respiratory rate, pulsoximetry 94%.
Oxygen at 6L/min by nasal cannula has been applied. An IV line is initiated. Serum glucose level is 80. Cardiac monitor shows sinus rhythm. There was no response to intravenous naloxone.
There is a nearly empty bottle of Thunderbird wine in his jacket along with a full bottle of (phenytoin) Dilantin® capsules dated two weeks earlier
Case Report: Part 1

The patient smells of alcohol and his pants are urine stained. There are numerous healed scars about the head with encrusted sutures along his right parieto-occipital scalp.
His right pupil is 6 mm and does not appear to react, while the left is 3 mm reactive. According to his buddies, he had been drinking more than usual recently to alleviate a headache. He has been lying on the ground for several hours.
Although the patient is a known alcoholic and appears to be in an alcoholic stupor or perhaps in a postictal state, the history and physical examination point to a more urgent situation.
The pupil asymmetry (presumably not due to a previous insult) suggests thatcoma is due to brainstem compromise with herniation. Because acute or chronic intracranial hematoma is the likely cause, the trauma team is notified.
Case Report: Part 1

A careful history, along with timely and appropriate interventions is necessary in the management of patients presenting with an altered level of consciousness
Obtain history from witnesses, friends, and family keeping in mind that certain interventions must be performed while gathering information. Is there any history of trauma, seizures, diabetes, allergies or medical problem?
How long has the patient been unconscious? Were there any bottles or medication containers at the scene?Is the patient taking prescribed medications? Is there anything special about the environment in which the patient was found?Indoors or outdoors?Any unusual odors?Any others in the vicinity in a similar state?Is the patient wearing a Medical Alert bracelet?
History
Interventions
Always assume there is a C-spine fractureEnsure a patent airway maintaining C-spine precautions
If respirations are inadequate, a jaw-thrust or chin-lift maneuver may assist respirations initially
Oxygen – Initially high- flow oxygen by nasal cannula or mask
Repeat and monitor vital signs including temperature
Intravenous line
ECG monitor
Thiamine –Wernicke’s encephalopathy may present as comaIn such patients, administer 100 mg of thiamine by intravenous injection before giving glucose

Glucose – If the patient is hypoglycemic, administer 50 cc D50%W intravenously. In children give 2 cc/kg of D25W
NB: If the patient is not hypoglycemic, giving a glucose load to a patient with a stroke or other brain injury may aggravate the brain damage
Naloxone - Give 2 mg. intravenously. Be prepared for the patient who is a narcotic overdose individual to awaken in response to the naloxone and to become combative and resist further medical evaluation.
Review responses to glucose, thiamine, naloxone and oxygen
With the airway protected, an orogastric tube for gastric lavage is inserted and activated charcoal is instilled when there is a possibility of a toxic ingestion
Interventions

If meningitis is suspected, perform a lumbar puncture
If a unilaterally dilated pupil (sluggish or unresponsive to light) is present, suggesting uncal cerebral herniation, the patient is hyperventilated to a pCO2 of about 30 to 35mmHg and given mannitol IV at 1 gram/kg as a temporizing measure for the increased intracranial pressure. Obtain a head CT scan while neurosurgery consultation is requested emergently
A Foley catheter is inserted for obtaining urine for laboratory tests and monitoring urine output.
Observe for status epilepticus . A rhythmical twitching of some of the digits of either hand or a rhythmical small amplitude horizontal jerking of the eyes may be the only clue that the patient is in status epilepticus.
Interventions

Physical Examination
Confirm the comatose state
Use the Glasgow Coma Scale to assess the degree of coma prior to intubation and the use of paralytic or sedative agents.
Components Of The Physical Examination
Vital Signs
Head
Neck
·Eyes
Motor System
Skin
Lungs, Cardiac, Abdomen
Extremities
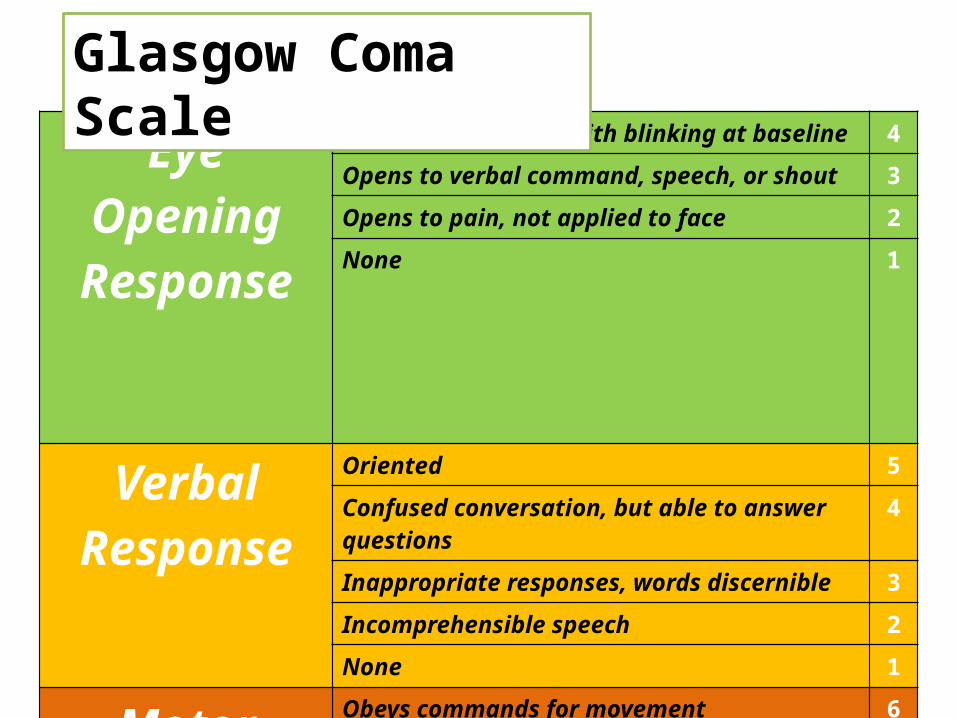
Eye Opening Response
Spontaneous--open with blinking at baseline 4
Opens to verbal command, speech, or shout 3
Opens to pain, not applied to face 2
None 1
Verbal Response
Oriented 5
Confused conversation, but able to answer questions
4
Inappropriate responses, words discernible 3
Incomprehensible speech 2
None 1
Motor Response
Obeys commands for movement 6
Purposeful movement to painful stimulus 5
Withdraws from pain 4
Abnormal (spastic) flexion, decorticate posture 3
Extensor (rigid) response, decerebrate posture 2
None 1
Glasgow Coma Scale
Case Report: Part 2
On arrival at the emergency department, the rescue squad's findings were confirmed. The patient was comatose with a nonreactive 6mm right pupil. In response to noxious stimuli, his left side moved much less than the right.
Immediately, the C-spine was examined radiologically and the patient was intubated, slightly hyperventilated, and placed on a ventilator with 100% oxygen.
Mannitol 100 grams was given intravenously and a CT of the head obtained.
The neurosurgeon was at the bedside and the operating room staff were notified of possible emergent surgery.
Preoperative laboratory and X-ray studies were performed

Differential Diagnosis
Is the coma due to a primary central nervous system disease or the consequence of a systemic illness?
The first 10 items in the differential diagnosis list below are the most life- and function threatening.
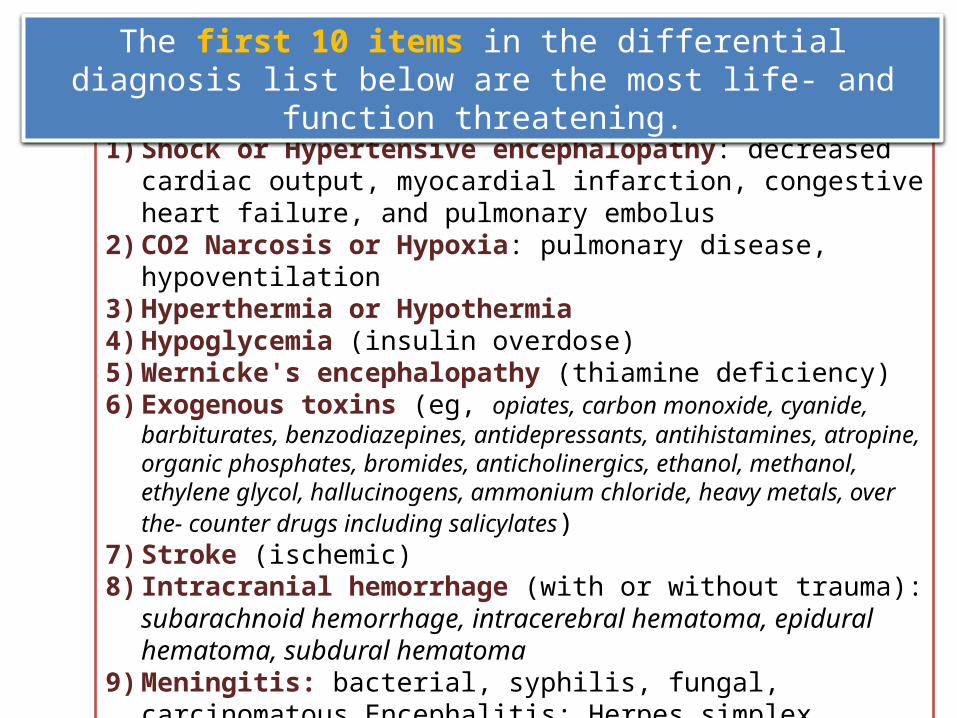
1) Shock or Hypertensive encephalopathy: decreased cardiac output, myocardial infarction, congestive heart failure, and pulmonary embolus
2) CO2 Narcosis or Hypoxia: pulmonary disease, hypoventilation3) Hyperthermia or Hypothermia4) Hypoglycemia (insulin overdose)5) Wernicke's encephalopathy (thiamine deficiency)6) Exogenous toxins (eg, opiates, carbon monoxide, cyanide, barbiturates,
benzodiazepines, antidepressants, antihistamines, atropine, organic phosphates, bromides, anticholinergics, ethanol, methanol, ethylene glycol, hallucinogens, ammonium chloride, heavy metals, over the- counter drugs including salicylates)
7) Stroke (ischemic)8) Intracranial hemorrhage (with or without trauma): subarachnoid
hemorrhage, intracerebral hematoma, epidural hematoma, subdural hematoma
9) Meningitis: bacterial, syphilis, fungal, carcinomatous Encephalitis: Herpes simplex
10)Reye's syndrome (pediatric )
The first 10 items in the differential diagnosis list below are the most life- and function threatening.

11) Trauma: diffuse axonal injury to the brain without significant intracranial hemorrhage
12) Tumor: CNS meningioma, glioma, and remote effects (e.g., lung cancer)13) Toxin: mercury, arsenic, lead, and magnesium.14) Infections: sepsis, any infection outside of CNS especially in elderly, AIDS,
subacute bacterial endocarditis (SBE).15) CNS Infections: progressive multifocal leukoencephalopathy, Creutzfeldt-
Jakob disease16) Seizures: status epilepticus, including non-convulsive; prolonged postictal state17) Blood: anemia, sickle cell disease18) Vascular: systemic lupus erythematosis (SLE)19) Metabolic: hypercalcemia ,uremic encephalopathy , hepatic encephalopathyhyperosmolar state, thyrotoxicosis or myxedema coma, Cushing's diseasepituitary apoplexy, porphyria20) Psychiatric: especially depression; hysterical conversion reaction21) Other: migraine, basilar (especially in children) intussusception in children
The first 10 items in the differential diagnosis list below are the most life- and function threatening.

Diagnostic Adjuncts
Laboratory Evaluation
CBC, differential, plateletsSerum glucose, electrolytes, calcium, magnesium, phosphorusRenal function testsHepatic function testsArterial blood gases; carboxyhemoglobin levelUrine for urinalysis and toxicology studies, myoglobin and porphobilinogenECGCT scanThyroid function studiesLumbar puncture for CSF cells, protein, sugar, India ink prep, fungal cultures, and extra tubes as neededEEG (immediately if suspect status epilepticus) Alcohol level

Case Report: Part 3
The CT scan showed a large right parieto-occipital chronic subdural hematoma, which probably explains the patient's recent headaches.
There was fresh blood within the chronic subdural. This recent bleeding probably resulted in the patient's acute decompensation.
The patient was taken immediately to the operating room to have the subduralhematoma evacuated
Case Report: Part 4
After evacuation of the subdural hematoma, the patient had an uneventful course and recovered completely

ReferralTransfer should be considered when
The patient is stable enough to be transferred and definitive care exists which your facility does not offer
If there is uncertainty regarding the diagnosis or management
If the clinician does not have privileges to provide the type of care needed (e.g., surgery),
The clinician is ethically opposed to providing care (e.g., hospice care, or the opposite, definitive care at the patient’s/ family’s request when it would be futile).
Referral
Transfer should be considered when
If the patient requests a consultation.
There is inadequate equipment (e.g., no dialysis, CT or EEG) or facilities (e.g., limited ICU) in your hospital
As a second opinion may be wise when the diagnosis is unexpected (e.g., young person with severe injury), serious, the prognosis is grim or the patient is not getting better
When there is a conflict (e.g., personality conflict or the patient is a close friend or family member) and the clinician feels they cannot be objective.
All neurologic emergencies requiring surgery,
Status epilepticus requiring general anesthesia,
For rehabilitation for neurological emergencies with sequelae if the clinician is not comfortable.
Specific examples of consultation for neurologic emergencies include

Psychosocial Impact
Surviving a neurological emergency can be very stressful for the patient and/or family members.
Survivors of neurologic emergencies with risk of recurrence go through many of the same stages of any patient receiving bad news:
denial, anger, bargaining, (depression )resolution.
caregiver burnout

ISCHEMIC STROKE

Incidence of Ischemic Stroke by Subtype
Stroke Subtype Incidence
Cardioembolic 30%
Atherothrombotic (large vessel) disease 30%
Lacunar (small vessel) disease 25%
Other (vasculitis, dissection, hypercoagulable state) 10%
Cryptogenic 5%
Succinct Approach to the Stroke Patient
WHERE – Neuroanatomical localization
WHERE – Vascular localization
WHEN – Profile of onset
HOW – Vascular mechanism
Common conditions mimicking acute stroke
Hypoglycemia
Mass Lesion
Complex Migraine
Seizure with postical Todd’s paralysis
Ion channels dysfunctions (channelopathies)
Psychiatric disorders with functional focal defi cits
Is this a vascular event
Are the neurological symptoms focal rather than non-focal?
Are the focal neurological symptoms negative (that is, lossof function) rather than positive (for example, pins andneedles rather than numbness)?
Was the onset of the focal symptoms sudden?
Were the focal symptoms maximal at onset (that is, comingon over minutes to hours) rather than progressive (that is,evolving over hours to days)?
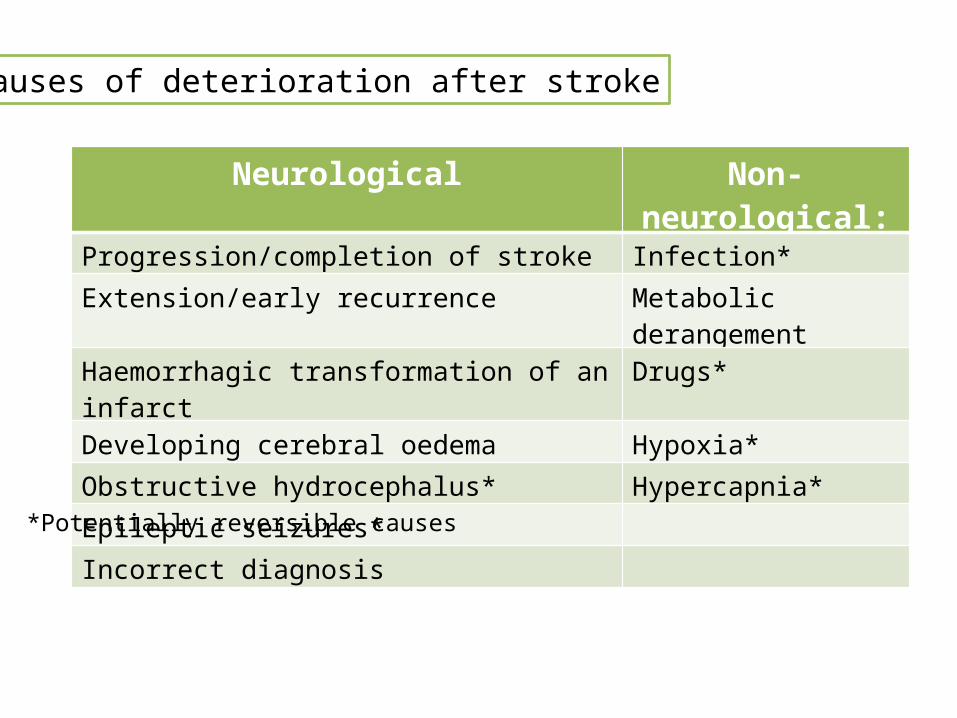
Causes of deterioration after stroke
Neurological Non-neurological:Progression/completion of stroke Infection*
Extension/early recurrence Metabolic derangement
Haemorrhagic transformation of an infarct Drugs*
Developing cerebral oedema Hypoxia*
Obstructive hydrocephalus* Hypercapnia*
Epileptic seizures*
Incorrect diagnosis
*Potentially reversible causes

HistoryTime of onset (for patients who cannot provideinformation, use the time when they were lastseen normal) and circumstancesHistoryTime of onset (for patients who cannot provideinformation, use the time when they were lastseen normal) and circumstancesRecent events: strokes, chest pain, MI, trauma, surgery, bleeding Comorbidities: HTN, DM, Cardiac disease,hyperlipidemia, smoking, allergies (iodine)Medications: anticoagulants, antihypertensives, antiplatelets, antidiabetics, antiarrhythmics
Clinical Evaluation
ExamGENERAL:ABC, Oxg Sat, temperature, signs of trauma or seizures, carotid bruits, CHF, arrhythmias, abdominal and skin exam to identify comorbities (hepatic dysfunction, coagulopathies and etc)Use NIH Stroke ScaleNEUROLOGICAL:Localize and Identify Stroke Syndrome
All PatientsBrain imaging: CT or MRI (preferably multimodal)Fingerstick glucose, CBC, BMPECGCardiac enzymesPT/PTT/INROxygen saturation
Candidate for Recanalization? > refer to recanalization algorithm
Labs/Imaging Evaluation
Selected PatientsLFTCXRUrinalysisTox ScreenBlood ETOH levelsAED levelsABGCSF (if SAH is suspected and HCT is negative)B-HCG (for all women of child bearing potential)
Algorithm for Management of Acute Ischemic Stroke

Algorithm for Management of Acute Ischemic Stroke
Contact Acute Stroke team and proceed perrecanalization algorithm
Candidate for Recanalization? > refer to recanalization algorithm
Recanalization performed?
Admit to Neuro ICU and follow early subacute stagealgorithm plus specific instructions from Neuro ICU team
Pt stable for stroke unit (no risk of malignant edema, not intubated and no severe comorbidities)?
Admit to telemetry bed and follow early subacute stage algorithm
Yes No
No
NoYes
Yes
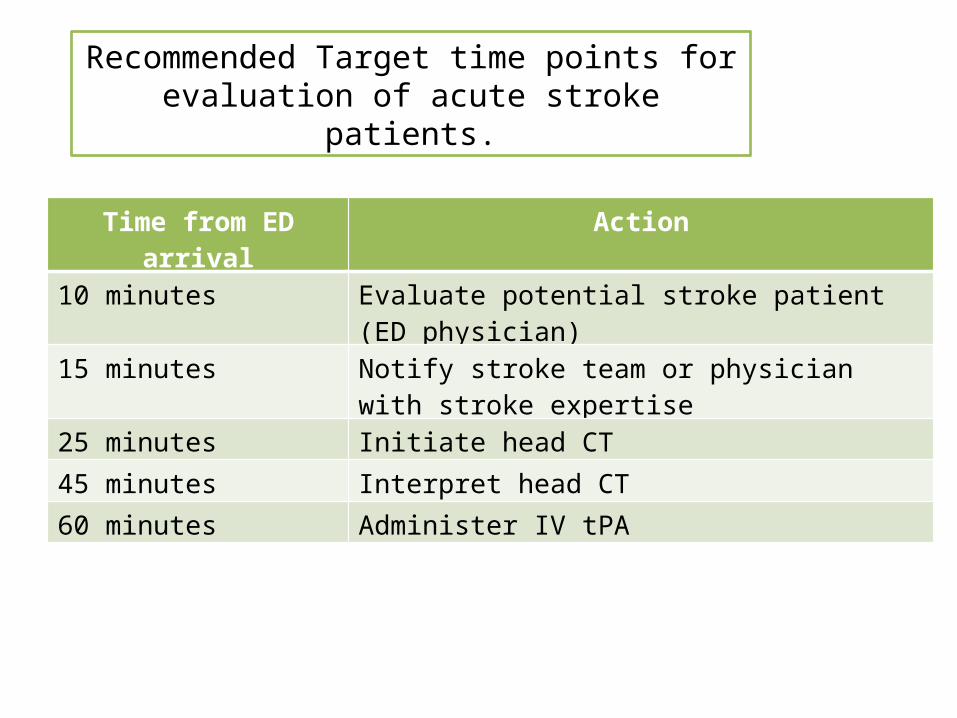
Recommended Target time points for evaluation of acute stroke patients.
Time from ED arrival Action
10 minutes Evaluate potential stroke patient (ED physician)
15 minutes Notify stroke team or physician with stroke expertise
25 minutes Initiate head CT
45 minutes Interpret head CT
60 minutes Administer IV tPA
Case Report
You have just completed your morning rounds at the hospital, and are informedthat a long-time patient has notified your office that her husband (a 65-year-old man who has always been in excellent health and on no medications) is en route to the Emergency Department (ED).
You go directly to the ED where the paramedics arrive at 8AM. They report that the patient’s wife called 911 when she noticed upon awakening at 7:30 AM her husband was having difficulty speaking, his face was crooked and his right arm was limp at his side.
They had established an intravenous line, obtained a blood glucose measurement of 120 mg/dL, and placed the patient on low-flow oxygen by nasal canulae. Blood pressure in the field was 200/100 mm Hg, and it was the same in the ED, heart rate was 82 and regular, with a respiratory rate of 18. The patient's temperature was recorded along with the initial vital signs in the ED as 37°C.
Case Report
You examine the patient and the key findings are neurologic.
There is no speech output but he seems to follow some simple commands (close your eyes, lift up your arm),
There is right facial asymmetry, a right field cut to threat, a flaccid right arm with no withdrawal to a painful stimulus to the nailbed digits of the right hand, and spontaneous weak movement of the right leg compared to the left.
You join the Emergency Physician in providing care.
Question 1
Your initial management includes
Sublingual nifedipine
Chewable aspirin
Obtain an emergency head computerized tomography (CT) scan
All of the above
The patient goes to CT scan, monitored, with a nurse, and returns from the CT scan 15 minutes later.
The radiologist's preliminary report is that the CT scan is negative.
Reassessment shows that there is no change in the patient's clinical state, except the BP is now 150/80 mmHg

Ordering tissue plasminogen activator (t-PA) at 0.9 mg/kg
Ordering a heparin infusion at 10 units/kg/hour
Performing a lumbar puncture before either 1 or 2
None of the above
None of the above
Question 2
Your management includes
Case Report
Minutes later the patient’s wife arrives. She states that she and her husband had arisen early that morning, awakening in time to catch a beautiful sunrise. At that time her husband was perfectly normal. They returned to bed at 6:30 AM, and when they awoke at 7:30 AM, he was noted to have the neurologic deficit. She knows he's having a stroke and is asking that you do something.
You re-evaluate the patient. He's neurologically the same.
The radiologist states the CT scan shows no hemorrhage and there are no early infarct signs.
The nurse provides you with the blood test results from clinical laboratory. A complete blood count including platelets, glucose, electrolytes, renal function tests, prothrombin time and partial thromboplastin time are all within normal limits.
Ordering t-PA at 0.9 mg/kg, 10% initial bolus, and the remainder over an hour becausethe patient has a greater likelihood of functionally independent recovery with minimal or no disability than without t-PA therapy, despite a 6% increase in the likelihood of asymptomatic intracerebral hemorrhage.
Ordering 1,000,000 units of streptokinase (SK) since SK is minimally more effectivecompared to t-PA for acute stroke and is less expensive
Withholding thrombolytic therapy for the acute ischemic stroke since the patient cannot give informed consent
Withholding thrombolytic therapy for acute ischemic stroke until the patient's privatephysician arrives since it is now only just over 2 hours from stroke onset and the patient may still be suffering only a transient ischemic attack.
Question 3
Your management includes

Case 1A 72-year-old woman with a past medical history of arthritis, diabetes mellitus, coronary artery disease, and stroke presented to the ICU in a coma. Apparently, she had been found slumped over in a chair earlier in the day by her husband.
At the time he found her, she was confused and combative. By the time emergency medical services arrived at the home, she was comatose. They quickly intubated her, supported her low blood pressure, and transported her to the ICU.
The neurologist was called to see the patient to determine the cause of the coma.In further discussion, the husband denied that the patient had hit her head, complained of chest pain, or had an obvious seizure. He claimed she had been feeling ill for a few days and had not had much of an appetite. According to him, she had never had an episode like this before.
Review of her medications showed medicines appropriate for her disease history without any narcotics. The husband denied any illegal drug use.The neurologist was asked to comment on the cause of the coma and order more tests if necessary.
Case 1Comment
This type of coma, preceded by an episode of combativeness and delirium, is commonly associated with seizures or metabolic problems.
The most important entity to rule out here is hypoglycemia. Since the patient is taking hypoglycemic medications for her diabetes and she has had a suppressed appetite, it is likely she is hypoglycemic.
It is critical to search for this condition because the correction of the bloodglucose level can lead to significant recovery.
Hypoxia is the second derangement that could lead to rapid recovery.
Other entities, including seizures, encephalitis, stroke, intracerebral hemorrhage, and metabolic derangements, can be investigated in turn after hypoglycemia and hypoxia are ruled out.
STATUS EPILEPTICUS

Patient does not recover to a normal alert state between two or more tonic clonic seizures or duration of seizures greater than 20 minutes.
Although most epileptic seizures are self-limited, some go on for prolonged periods, whereas others recur so rapidly that the condition is referred to as status epilepticus.
The most serious form of this disorder is generalized convulsive status epilepticus, in which convulsive seizures are repeated without return of consciousness in between.
Definition

Treatment of the premonitory stages is likely to be more successful than treatment in the later stages and so treatment should commence as soon as it is apparent that the seizure is persisting (a tonic-clonic seizure of more than five minutes duration) or there is a significant worsening of a patient’s normal seizure pattern
Status epilepticus to account for about 4% of admissions to neurological intensive care, and 5% of all visits to a university hospital casualty department
The mortality of status epilepticus is about 20%.
Permanent neurological and mental deterioration may result from status epilepticus, particularly in young children, the risks of morbidity being greatly increased the longer the duration of the status epilepticus episode
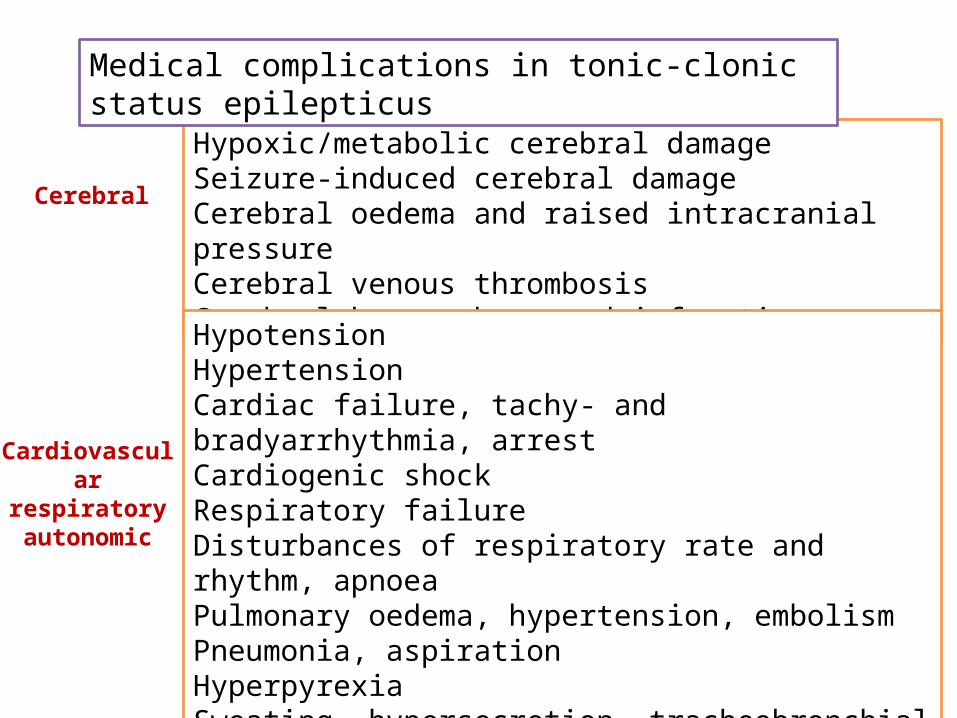
Hypoxic/metabolic cerebral damageSeizure-induced cerebral damageCerebral oedema and raised intracranial pressureCerebral venous thrombosisCerebral haemorrhage and infarction
HypotensionHypertensionCardiac failure, tachy- and bradyarrhythmia, arrestCardiogenic shockRespiratory failureDisturbances of respiratory rate and rhythm, apnoeaPulmonary oedema, hypertension, embolismPneumonia, aspirationHyperpyrexiaSweating, hypersecretion, tracheobronchial obstructionPeripheral ischaemia
Medical complications in tonic-clonic status epilepticus
Cerebral
Cardiovascular respiratory autonomic

DehydrationElectrolyte disturbance (especially hyponatraemia, hyperkalaemia,hypoglycaemia)Acute renal failure (especially acute tubular necrosis)Acute hepatic failureAcute pancreatitis
Disseminated intravascular coagulopathy/multiorgan failureRhabdomyolysisFracturesInfections (especially pulmonary, skin, urinary)Thrombophlebitis, dermal injury
Medical complications in tonic-clonic status epilepticus
Metabolic
Other
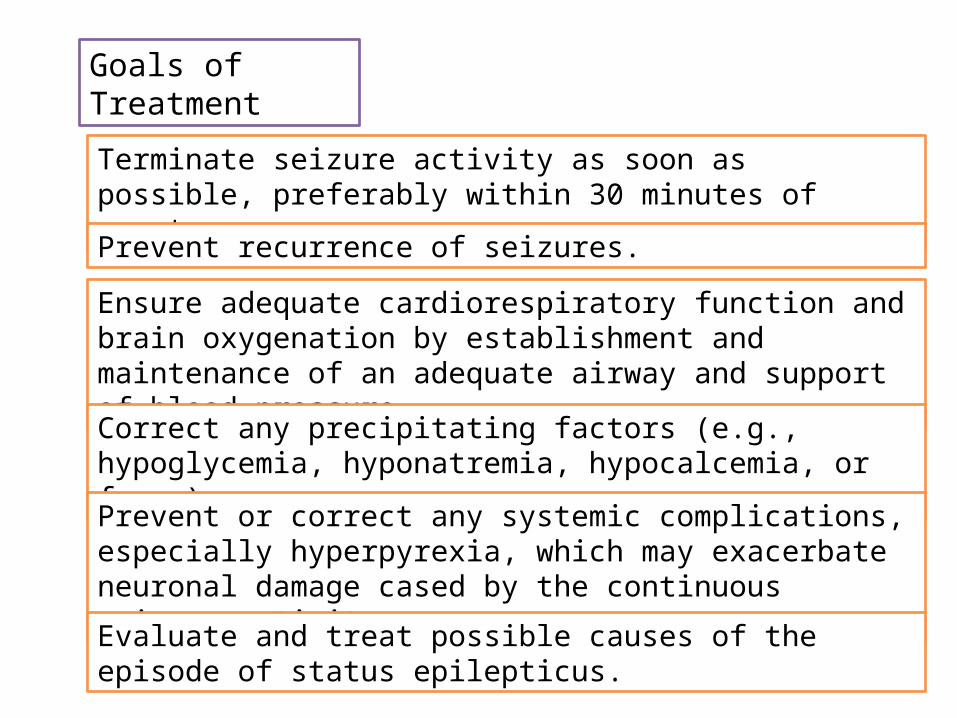
Terminate seizure activity as soon as possible, preferably within 30 minutes of onset
Prevent recurrence of seizures.
Ensure adequate cardiorespiratory function and brain oxygenation by establishment and maintenance of an adequate airway and support of blood pressure.
Correct any precipitating factors (e.g., hypoglycemia, hyponatremia, hypocalcemia, or fever).
Prevent or correct any systemic complications, especially hyperpyrexia, which may exacerbate neuronal damage cased by the continuous seizure activity.
Evaluate and treat possible causes of the episode of status epilepticus.
Goals of Treatment

Assess cardiorespiratory functionSecure airway and resuscitateAdminister oxygen
Institute regular monitoring (see text)Emergency antiepileptic drug therapy (see text)Set up intravenous linesEmergency investigations (see text)Administer glucose (50 ml of 50% solution) and/or intravenous thiamine (250 mg) as high potency intravenous Pabrinex where appropriateTreat acidosis if severe
Management of tonic-clonic status epilepticus (General measures)
First stage (0–10 minutes)
Second stage (0–60 minutes)
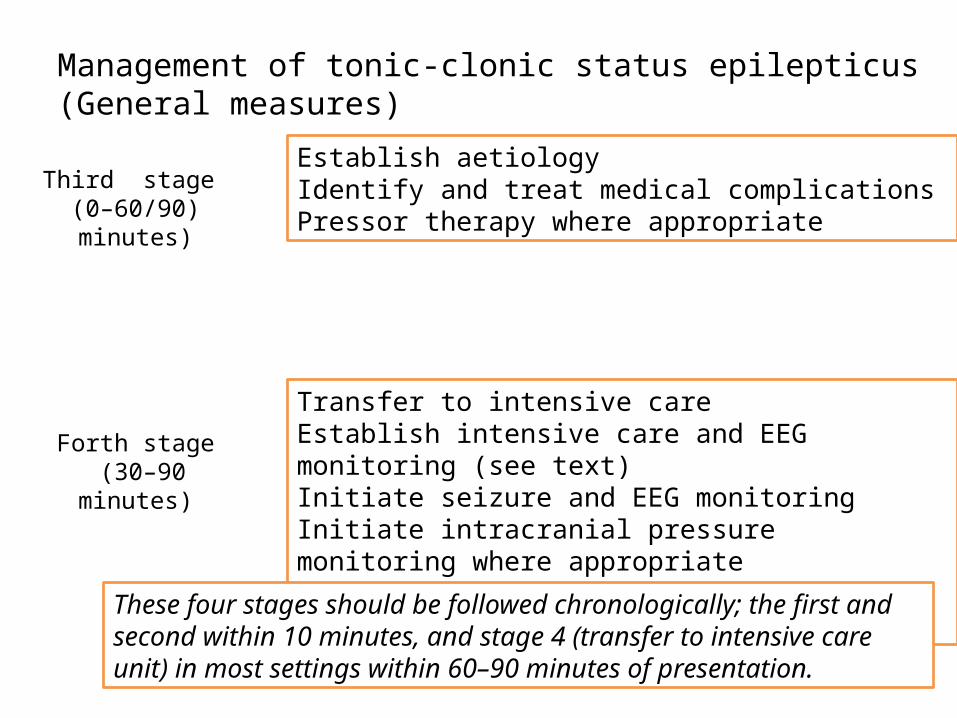
Establish aetiologyIdentify and treat medical complicationsPressor therapy where appropriate
Transfer to intensive careEstablish intensive care and EEG monitoring (see text)Initiate seizure and EEG monitoringInitiate intracranial pressure monitoring where appropriateInitiate long term, maintenance, antiepileptic therapy
Third stage (0–60/90) minutes)
Forth stage (30–90 minutes)
Management of tonic-clonic status epilepticus (General measures)
These four stages should be followed chronologically; the first and second within 10 minutes, and stage 4 (transfer to intensive care unit) in most settings within 60–90 minutes of presentation.

Have no active metabolites (diazepam, midazolam, lidocaine (lignocaine), and thiopentone have active metabolites)
Not interact with other medication
Not have saturable metabolism (both phenytoin and thiopentone have saturable pharmacokinetics at therapeutic levels)
Not be unduly affected by hepatic or renal blood flow or disease (chlormethiazole is an example of a drug whose metabolism is greatly affected by both hepatic disease and changes in hepatic blood flow)
An ideal antiepileptic drug should
Show no tendency to autoinduction (thiopentone, phenobarbitone, and phenytoin are all subject to strong autoinduction)
Have strong antiepileptic action (the non-barbiturate anaesthetics have little or no intrinsic antiepileptic action – a conundrum for their use in status epilepticus, the implications of which have not been fully considered)
Be stable in solution and unreactive with giving sets (a problem with paraldehyde, diazepam, and thiopentone).
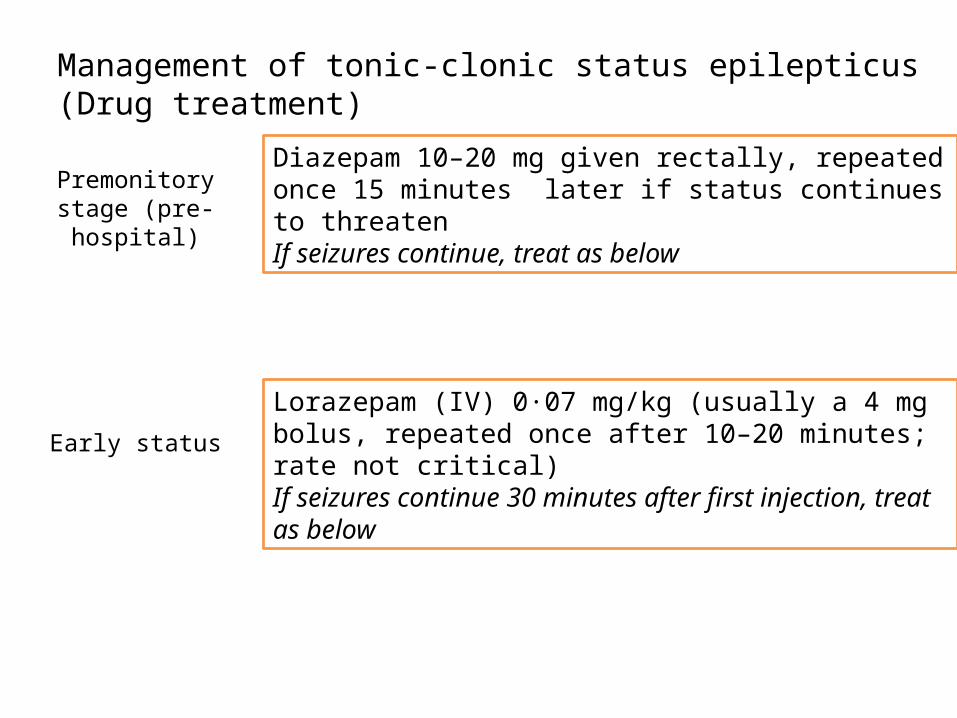
Diazepam 10–20 mg given rectally, repeated once 15 minutes later if status continues to threatenIf seizures continue, treat as below
Lorazepam (IV) 0·07 mg/kg (usually a 4 mg bolus, repeated once after 10–20 minutes; rate not critical)If seizures continue 30 minutes after first injection, treat as below
Premonitory stage (pre-hospital)
Early status
Management of tonic-clonic status epilepticus (Drug treatment)

Phenytoin infusion at a dose of 15–18 mg/kg at a maximum rate of 50 mg/min or fosphenytoin infusion at a dose of 15–20 mg PE/kg at a maximum rate of 100 mg PE/minuteand/orPhenobarbitone bolus of 10 mg/kg at a rate of 100 mg/min(usually 700 mg over seven minutes in an adult)
General anaesthesia, with propofol, midazolam, or thiopentone.Anaesthetic continued for 12–24 hours after the last clinical or electrographic seizure, then dose tapered
Established status
Refractory status
Management of tonic-clonic status epilepticus (Drug treatment)
In the above scheme, the refractory stage (general anaesthesia) is reached 60/90 minutes after the initial therapy. This scheme is suitable for usual clinical hospital settings. In some situations, general anaesthesia should be initiated earlier and, occasionally, should be delayed.
Inadequate emergency antiepileptic drug therapy (especially the administration of drugs at too low a dose)
Failure to initiate maintenance antiepileptic drug therapy (seizures will recur as the effect of emergency drug treatment wears off)
Hypoxia, hypotension, cardiorespiratory failure, metabolic disturbance
Failure to identify the underlying cause
Failure to identify other medical complications (including hyperthermia, disseminated intravascular coagulation, hepatic failure)
Misdiagnosis (Pseudostatus epilepticus is a common differential diagnosis that is often missed)
Common reasons for the failure of emergency drug therapy to control seizures in status epilepticus


Thank you