
Common Ailments of the foot - c.ymcdn.com · If you only treat tinea pedis and patient ... MPJ and...
58
Transcript of Common Ailments of the foot - c.ymcdn.com · If you only treat tinea pedis and patient ... MPJ and...



PLANTAR FASCIITIS
Symptoms:
Stabbing sensation in the heel
Pain worse in the morning when getting out of bed or after prolonged seating and decreases after the first several steps.
Limping, tenderness, swelling, stiff sensation
Can be caused by prolonged standing

PLANTAR FASCIITIS

PLANTAR FASCIITIS
One of the most common causes of heel pain.
Caused by inflammation, micro tearing of the fascia

PLANTAR FASCIITIS RISKS
Obesity
Working long hours on hard surfaces
Age
Exercise with repetitive stress to the heels
Foot mechanics ie. Pes planus, pes cavus
Can be caused by pronation, tight achilles.

PLANTAR FASCIITIS
Can get xray but will commonly see a heel spur. These are common and often blamed for plantar fascial symptoms but can also be seen on xrays in people who do not have plantar fasciitis.
Stress fracture
Pinched nerve
Calcaneal bursitis

PLANTAR FASCIITIS
Differential diagnosis
1. pinched nerve
2. Calcaneal stress fracture
3. Calcaneal bursitis
PLANTAR FASCIITIS TREATMENT
Anti-inflammatories
Physical therapy
Night splints
Orthotics
Steroid shots.
ECSWT, Tenex, etc
Surgery
Prolotherapy

PLANTAR FASCIITIS TREATMENT CONTINUED
Weight loss
Supportive shoe gear, changing shoes frequently if a runner
Changing exercises
Icing
Stretching
Wedges in shoes
Shortening stride and increasing cadence during running

FREIDBERG’S
Avascular necrosis of the metatarsal head. Most commonly affects the 2nd metatarsal head.
Can be difficult to diagnose on plain radiographs
Diagnosis primarily made on H& P

FREIDBERG’S

FREIGBERG’S SYMPTOMS
Swelling
Pain upon ROM of the 2nd MPJ
Pain with compaction of the MPJ
Pain with ambulation

FREIBERG’S DIAGNOSIS
Xray- may not show anything initially but can eventually see osteopenia in the metatarsal head, flattening of metatarsal head, loose bodies, arthritic changes
MRI- can be used to diagnose in the early stages will show increase signal intensity on T-2 images

FREIBERG’S TREATMENT
Conservative: immobilization in boot or cast with or without crutches for 4-6 weeks, or until symptoms resolve then gradual return to normal activity. Orthotics, shoes modifications.
Surgical: cleaning up the joint, cartilage replacement, implants, resection of the metatarsal head.

HALLUX LIMITUS DEFINITION
Hallux limitus:-A degenerative process of the joint characterized by decreased Range of Motion of the Hallux. Over a period of time this jamming forms a dorsal bump on the head of the 1st Metatarsal and is often referred to as a dorsal bunion. Eventually can lead to joint ankyloses and loss of motion.

HALLUX LIMITUS
Several etiologies including Biomechanical, Neuromuscular, Iatrogenic, traumatic, metabolic, anatomic/structural. Four common factors is: 1) Systemic dz (Gout, RA), 2)Injury to the joint (turf toe, jamming etc.) 3)Metatarsus primus elevatus 4) Long 1st metatarsal

HALLUX LIMITUS
Stage I – No symptoms to vague joint pain, decreased dorsiflexion of the 1st MPJ. X-rays show no changes, can show mild dorsal enlargement. One or more etiologic factors.

HALLUX LIMITUS
Stage II – Decreased dorsiflexion, pain with end ROM, increased frequency of pain. x-ray finding such as subchondral sclerosis, mild joint space narrowing with asymmetry, mild dorsal exostosis.

HALLUX LIMITUS

HALLUX LIMITUS
Stage III- Inflammatory arthritis, pain with activity, Limited ROM which is very noticeable. Impingement with nerve type symptoms with shoe gear. Increased dorsal exostosis, subchondral cyst, irregular narrowing with practical obliteration.

HALLUX LIMITUS

HALLUX LIMITUS
Stage IV- Significant pain with attempted ROM of the joint to no pain within the joint just with bony protrusions of joint. Joint is enlarged. X-ray findings can show flattening of the joint with surrounding spurring of the joint to ankyloses with no joint space visible.

HALLUX LIMITUS

HALLUX LIMITUS

HALLUX LIMITUS
STAGE I- Orthotics with reverse morton’s extension or padding, rigid rocker bottom type shoes

HALLUX LIMITUS/HALLUX RIGIDUS

PLANTAR WARTS
Caused by Human papillomavirus (HPV) which enters the body via tiny abrasions in the skin. These can cause discomfort and pain.
PLANTAR WARTS
Black pinpoints which are small clotted vessels
Disrupts normal lines and ridges of the skin in the foot.

PLANTAR WARTS
Treatment:
Most clear up on their own but laser therapy, cryotherapy, acid treatments ( Salicyclicacid, cantharone) surgical excision. No single treatment is 100% effective
Imiquimod
5-Flurouracil
Bleomycin sulphate
Candida antigen
Interferon-alpha

PLANTAR WARTS
Oral medication (Retinoids, Cimetidine, Diindolymethane)
Laser
Surgical excision

ONYCHOMYCOSIS
A fairly common disease of the toenail . The two most common causes of Onychomycosis are Trichophyton mentagrophytes and Trichophyton rubrum. Less commonly it can be caused by molds or yeast as well. Some families have a genetic predisposition for T. rubrum.

ONYCHOMYCOSIS

ONYCHOMYCOSIS
Test that can be ordered to confirm onychomycosis are Periodic acid-Schiff (PAS), KOH, PCR. Fungal cultures are more difficult to obtain, hard to culture and takes weeks to grow cultures.

ONYCHOMYCOSIS
Tinea pedis is linked to onychomycosis. Onychomycosis often starts as Tinea pedis. Important that you treat both of these. If you only treat tinea pedis and patient has onychomycosis, onychomycosis can re-infect the skin.
Onychomycosis is more common in diabetic than those who are non-diabetic.

ONYCHOMYCOSIS
Lasers: has become quite popular very little data to determine if this is effective . The FDA approved it because it can cause “temporary improvement of the appearance of the toenail” and not actually labelled for treatment of Onychomycosis.

ONYCHOMYCOSIS CONTROLLING RECURRENCE
Use maintenance regimens of antifungal agents (Limits growth of fungi on nails)
Discard old shoes (removes fungal reservoir)
Alternate wearing different pairs of shoes (allows shoes to dry, reduces fungal load in footwear.
Wash feet regularly ( minimizes fungal presence on the feet.
Alert provider at first sign of infection (minimizes progression of infection)

ONYCHOMYCOSIS (TREATMENT)
Topical (Efinaconazole- 53-55% effective)
Oral (Itraconazole 54% , Terbinafine 70%)
% of Mycologic cure

STRESS FRACTURES
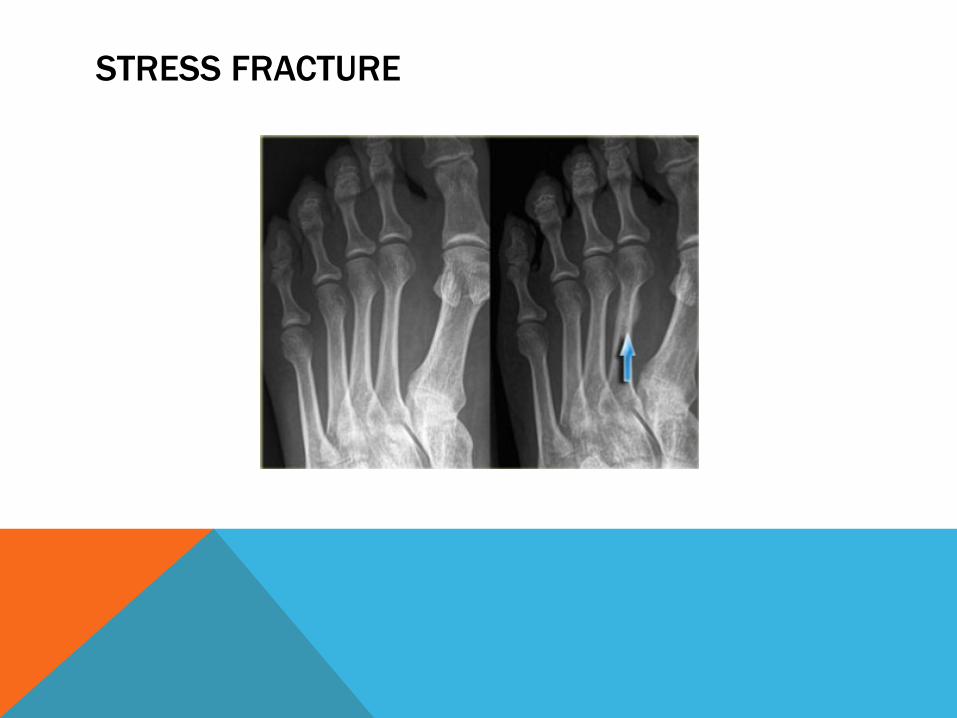
Overuse injury of bone. The more the load the more calcium will be placed at the site . Increased overloads can overwhelm repair and small cracks can occur within the bone structure.
STRESS FRACTURE

STRESS FRACTURE -SYMPTOMS
Pain
Swelling
Inability to bear weight

STRESS FRACTURE DIAGNOSIS
Plain film may not initially show fracture should plan to treat as a fracture and see patient back in 2 weeks to repeat xrays.
MRI
CT Scan

STRESS FRACTURE (TREATMENT)
Rest, Ice , compression, elevation
Immobilize (cast or boot) sometimes for at least 6-8 weeks depending on bone fractured.
PT once healing has occurred and in athletes to try and prevent future injury.

PLANTAR PLATE INJURY
Common in over pronators and in middle aged women.
Plantar plate is a thick ligament which inserts into the base of the phalanges plantarly. It protects the head of the metatarsal from pressure and prevents over extension of our toes also spreading or splaying.

PLANTAR PLATE INJURY

PLANTAR PLATE SYMPTOMS
Swelling under the ball of the foot extending into the toes seen commonly in the 2nd
MPJ and sometimes on the dorsum of the foot.
Sensation of walking on bones
Positive Lachman’s test
Splaying of toes and clawing

PLANTAR PLATE INJURY DIAGNOSIS
Careful history
Xrays
Diagnostic ultrasound
MRI

PLANTAR PLATE INJURY TREATMENT
Conservative (anti-inflammatories, strapping of toe, offloading padding, altering activity, changing shoe gear, determining biomechanical cause, orthotics)
Surgical ( plantar plate repair, osteotomy)
Can take 3-4 months to improve symptoms in some cases.

INTERMETATARSAL NEUROMA
Commonly occurring between the 3rd and 4th metatarsals called “Morton’s neuroma”
Thickening/enlargement of the nerve as a result of irritation of the nerve

INTERMETATARSAL NEUROMA

INTERMETATARSAL NEUROMA
Causes:
1. Compression from shoe gear
2. Activities such as running, court sports, any activity that involve repetitive irritation to the ball of the foot.

INTERMETATARSAL NEUROMA
Symptoms:
1. Pain
2. Feeling of “bunched up sock”
3. Feeling of a “pea”
4. Burning numbness, tingling sensation

INTERMETATARAL NEUROMA
Treatment:
1. Activity modifications
2. Padding
3. Anti-inflammatories, icing
4. Orthotics
5. Wide toe box shoes
6. Injection therapy –cortisone, injections, alcohol sclerosing injection therapy


REFERENCES:
Dananberg HJ. Sagittal plane biomechanics. In: Subotnick SI, ed. Sports Medicine of the lower extremity. New York: Churchill Livingstone; 1999: 137-156
Hetherington VJ, Carnett J, Patterson BA. Motion of the first metatarsophalangeal joint. J Foot Surgery 1989;28(1):13-19.
Clough JG. Functional hallux limitus and lesser metatarsal overload. J Am Podiatric Med Assoc 2005;95(6):593-601
Photos: Myfootshop.com, fdafac.com
Video: www.drglass.org http://www.youtube.com/watch?v=1gPcoRVuF9I

REFERENCES:
Levy LA. Epidemiology of onychomycosis in special risk populations. J AM Podiatr Med Assoc. 1997: 87 (12):546-50
Bodman, M. Keys to managing severe Onychomycosis. Podiatry today. Volume 25-Issue 5-May 2013
Gupta AK. Simpson FC. New therapeutic options for onychomycosis. Expert OpinPharmacothera. 2012 Jun;13 (8):1131-42
Weber C, Hoffman K. How to treat recalcitrant plantar warts. Podiatry today. Volume 26- issuey- July 2013
Leung L. Recalcitrant nongenital warts. Aust Family Physician. 2011;40(1-2):40-2.

REFERENCES
Jacobs, A. An Evidence-Based Medicine approach to plantar fasciitis. Podiatry Today. Volume 26-Issue11-Nov 2013
Mahowald S, LeggeBS, Grady JF. The correlation between plantar fascia thickness and symptoms of plantar fasciitis. J AM PodiatrMed Assoc. 2011;101(5):385-9
Cerrato RA. Freiberg’s disease. Foot Ankle Clin N AM. 2011; 16(4):647-58.
Joseph. W. Onychomycosis and the Role of Topical Antifungals. (table1:Preventative strategies to control recurrence of Onychomycosis). Podiatry today: Nov 2013

REFERENCES:Leung L. Recalcitrant nongenital warts. Aust Family Physician. 2011: 40 (1-2):40-2James WD, Berger TG, et al. Andrews’ Diseases of the Skin:Clinical Dermatology.
Saunders Elsevier, Philadelphia, 2006.Fullem, B. Managing Stress Fractures in Athletes. Podiatry Today. Volume 25-Issue 1-
January 2012.Cruveilhier J. The Anatomy of the Human Body Harper& Bros, New York, 1844, pp.176Coughlin MJ. Second metatarsophalangeal joint instability in the athlete. Foot Ankle.
1993;14:309-319.DeHeer, P. A Practical approach to Morton’s Neuroma. Podiatry today. Sept 2010. Br.
J. Sports Med., Sonographically guided intratendinous injections for the treatment of chronic plantar fasciitis of hyperosmolar dextrose/lidocaine: a pilot study.
M B Ryan, A D Wong, J H Gillies, J Wong and J E Taunton. Br. J. Sports Med., Sonographicallyguided intratendinous injections for the treatment of chronic plantar fasciitis of hyperosmolar dextrose/lidocaine: a pilot study. 2009;43;303-306; originally published online 19 Nov 2008; doi:10.1136/bjsm.2008.050021


















