Combined Analysis of Concordance between Liquid and ......2021/02/17 · Lilly, Merck Serono, Ni...
19
1 Article type: Research article 1 Combined Analysis of Concordance between Liquid and Tumor Tissue Biopsies for RAS Mutations 2 in Colorectal Cancer with a Single Metastasis Site: The METABEAM Study 3 Yoshinori Kagawa 1 , Elena Elez Fernandez 2 , Jesus Garcia-Foncillas 3 , Hideaki Bando 4 , Hiroya Taniguchi 5 , 4 Ana Vivancos 6 , Kiwamu Akagi 7 , Ariadna Garcia 2 , Tadamichi Denda 8 , Javier Ros 2 , Tomohiro Nishina 9 , 5 Iosune Baraibar 2 , Yoshito Komatsu 10 , Davide Ciardiello 2,11 , Eiji Oki 12 , Toshihiro Kudo 13 , Takeshi Kato 14 , 6 Takeharu Yamanaka 15 , Josep Tabernero 2 , Takayuki Yoshino 5 7 8 1 Department of Surgery, Kansai Rosai Hospital, Amagasaki, Hyogo, Japan 9 2 Department of Medical Oncology, Vall d’Hebron University Hospital (HUVH), Vall d’Hebron Institute 10 of Oncology (VHIO); IOB-Quiron, UVic-UCC, Barcelona, Spain 11 3 Oncology Department, Fundacion Jimenez Diaz University Hospital, Autonomous University; Madrid, 12 Spain 13 4 Department of Clinical Oncology, Aichi Cancer Center Hospital, Nagoya, Japan 14 5 Department of Gastrointestinal Oncology, National Cancer Center Hospital East, Kashiwa, Chiba, 15 Japan 16 6 Cancer Genomics Group, Vall d’Hebron Institute of Oncology, Barcelona, Barcelona, Spain 17 7 Division of Molecular Diagnosis and Cancer Prevention, Saitama Cancer Center, Ina, Saitama, Japan 18 8 Division of Gastroenterology, Chiba Cancer Center, Chiba, Chiba, Japan 19 9 Department of Gastrointestinal Medical Oncology, National Hospital Organization Shikoku Cancer 20 Center, Matsuyama, Ehime, Japan 21 10 Department of Cancer Chemotherapy, Hokkaido University Hospital Cancer Center, Sapporo, 22 Hokkaido, Japan 23 11 Department of Precision Medicine, University of Campania Luigi Vanvitelli, Naples, Italy 24 12 Department of Surgery and Science, Graduate School of Medical Science, Kyushu University, 25 Fukuoka, Fukuoka, Japan 26 13 Department of Frontier Science for Cancer and Chemotherapy, Graduate School of Medicine, 27 Osaka University, Suita, Osaka, Japan 28 14 Department of Surgery, National Hospital Organization Osaka National Hospital, Osaka, Osaka, 29 Japan. 30 15 Department of Biostatistics, Yokohama City University School of Medicine, Yokohama, Kanagawa, 31 Japan 32 33 Running title: RAS Mutations in CRC Tested by Liquid and Tumor Biopsies 34 35 Keywords 36 Research. on August 16, 2021. © 2021 American Association for Cancer clincancerres.aacrjournals.org Downloaded from Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677
Transcript of Combined Analysis of Concordance between Liquid and ......2021/02/17 · Lilly, Merck Serono, Ni...

1
Article type: Research article 1
Combined Analysis of Concordance between Liquid and Tumor Tissue Biopsies for RAS Mutations 2
in Colorectal Cancer with a Single Metastasis Site: The METABEAM Study 3
Yoshinori Kagawa1, Elena Elez Fernandez2, Jesus Garcia-Foncillas3, Hideaki Bando4, Hiroya Taniguchi5, 4
Ana Vivancos6, Kiwamu Akagi7, Ariadna Garcia2, Tadamichi Denda8, Javier Ros2, Tomohiro Nishina9, 5
Iosune Baraibar2, Yoshito Komatsu10, Davide Ciardiello2,11, Eiji Oki12, Toshihiro Kudo13, Takeshi Kato14, 6
Takeharu Yamanaka15, Josep Tabernero2, Takayuki Yoshino5 7
8
1Department of Surgery, Kansai Rosai Hospital, Amagasaki, Hyogo, Japan 9
2Department of Medical Oncology, Vall d’Hebron University Hospital (HUVH), Vall d’Hebron Institute 10
of Oncology (VHIO); IOB-Quiron, UVic-UCC, Barcelona, Spain 11
3Oncology Department, Fundacion Jimenez Diaz University Hospital, Autonomous University; Madrid, 12
Spain 13
4Department of Clinical Oncology, Aichi Cancer Center Hospital, Nagoya, Japan 14
5Department of Gastrointestinal Oncology, National Cancer Center Hospital East, Kashiwa, Chiba, 15
Japan 16
6Cancer Genomics Group, Vall d’Hebron Institute of Oncology, Barcelona, Barcelona, Spain 17
7Division of Molecular Diagnosis and Cancer Prevention, Saitama Cancer Center, Ina, Saitama, Japan 18
8Division of Gastroenterology, Chiba Cancer Center, Chiba, Chiba, Japan 19
9Department of Gastrointestinal Medical Oncology, National Hospital Organization Shikoku Cancer 20
Center, Matsuyama, Ehime, Japan 21
10Department of Cancer Chemotherapy, Hokkaido University Hospital Cancer Center, Sapporo, 22
Hokkaido, Japan 23
11Department of Precision Medicine, University of Campania Luigi Vanvitelli, Naples, Italy 24
12Department of Surgery and Science, Graduate School of Medical Science, Kyushu University, 25
Fukuoka, Fukuoka, Japan 26
13Department of Frontier Science for Cancer and Chemotherapy, Graduate School of Medicine, 27
Osaka University, Suita, Osaka, Japan 28
14Department of Surgery, National Hospital Organization Osaka National Hospital, Osaka, Osaka, 29
Japan. 30
15Department of Biostatistics, Yokohama City University School of Medicine, Yokohama, Kanagawa, 31
Japan 32
33
Running title: RAS Mutations in CRC Tested by Liquid and Tumor Biopsies 34
35
Keywords 36
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

2
Colorectal cancer, circulating tumor DNA, liquid biopsy, organ specificity, RAS mutations 37
38
Funding 39
This work was funded and sponsored by Sysmex Corporation. 40
41
Correspondence to: Dr. Takayuki Yoshino 42
Department of Gastrointestinal Oncology, National Cancer Center Hospital East 43
6-5-1 Kashiwanoha, Kashiwa-shi, Chiba 277-8577, Japan 44
Tel: +81-4-7133-1111 45
Fax: +81-4-7131-9960 46
E-mail: [email protected] 47
48
Disclosure of Conflict of Interest 49
Y Kagawa reports personal fees received from Bayer, Chugai, Eli Lilly, Merck, Ono, and Taiho, grants 50 and personal fees from Takeda, and personal fees from Yakult Honsha outside the submitted work. E 51 Elez reports personal financial interests in the form of a scientific consultancy role for AbbVie, 52 Amgen, Array BioPharma, Boehringer Ingelheim, Bristol-Myers Squibb, GSK, Roche, MedImmune, 53 Merck Serono, MSD, Novartis, Pierre-Fabre, Sanofi-Aventis, and Servier. J Garcia-Foncillas reports 54 consultancies/advisories undertaken for Abbott, Amgen, Astellas, AstraZeneca, Bayer, Biocartis, 55 Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eisai, Foundation Medicine, GSK, Hospira, 56 Janssen, Eli Lilly, Merck Serono, MSD, Novartis, Pfizer, Pharmamar, Roche, Sanofi, Servier, Sysmex, 57 and Tesaro. H Bando reports honoraria received from Chugai, Eli Lilly, Merck Serono, Taiho, Takeda, 58 Sanofi, and Yakult Honsha. H Taniguchi reports honoraria received from Bayer, Bristol-Myers Squibb, 59 Chugai, Daiichi Sankyo, Eli Lilly, MBL, Merck Serono, Mitsubishi Tanabe Pharma, MSD, Nippon 60 Kayaku, Novartis, Sanofi, Taiho, Takeda, and Yakult Honsha; research funding received from Array 61 BioPharma, Daiichi Sankyo, Dainippon Sumitomo Pharma, MSD, Novartis, Ono, Sysmex, and Takeda. 62 K Akagi reports honoraria received from MSD and Taiho. T Denda reports lecture fees received from 63 Sysmex; honoraria received from Sawai; research funding received from MSD and Ono. T Nishina 64 reports honoraria received from Bristol-Myers Squibb, Chugai, Eli Lilly, Merck Serono, Nippon Kayaku, 65 Taiho, and Takeda; research funding received from Chugai, Daiichi Sankyo, Dainippon Sumitomo 66 Pharma, Eisai, Eli Lilly, Merck Serono, MSD, Ono, and Taiho. Y Komatsu reports research funding 67 received from Astellas, A2 Healthcare, Bayer, Daiichi Sankyo, Dainippon Sumitomo Pharma, Eisai, Eli 68 Lilly, EP-CRSU, EPS, Incyte, IQVIA, Kyowa Kirin, Linical, Mediscience Planning, MSD, NanoCarrier, Ono, 69 Parexel, QuintilesIMS, Sanofi-Aventis, Syneos Health, Sysmex, Taiho, and Yakult Honsha; lecture fees 70 from Asahi Kasei Pharma, Bayer, Bristol-Myers Squibb, Chugai, CROee, Daiichi Sankyo, EA Pharma, Eli 71 Lilly, Kyowa Kirin, Mitsubishi Tanabe Pharma, Moroo, Nippon Kayaku, Nipro, Ono, Otsuka, Pfizer, 72 Sanofi-Aventis, Sanofi, Taiho, Takeda, and Yakult Honsha; honoraria received from Asahi Kasei, Bayer, 73 Chugai, Daiichi Sankyo, Eli Lilly, Kyowa Kirin, Medical Review, Merck, MSD, Nippon Kayaku, Nipro, 74 Novartis, Ono, Pfizer, Sanofi-Aventis, Sanofi, Sawai, Shiseido, Taiho, Takeda, and Yakult Honsha. E 75 Oki reports lecture fees received from Bayer, Chugai, Eli Lilly, Merck, Ono, Taiho, Takeda, and Yakult 76 Honsha. T Kato reports honoraria received from Bayer, Boehringer Ingelheim, Chugai, Ono, Taiho, 77 and Takeda; research funding from Chugai and Takeda. J Tabernero reports personal financial 78 interest in the form of scientific consultancy role for Array Biopharma, AstraZeneca, Bayer, BeiGene, 79
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

3
Biocartis, Boehringer Ingelheim, Chugai, Foundation Medicine, Roche, Genentech, Genmab, HalioDX 80 SAS, Halozyme, Imugene, Inflection Biosciences, Ipsen, Kura, Eli Lilly, Menarini, Merck Serono, 81 Merrimack, Merus, Molecular Partners, MSD, Novartis, Peptomyc, Pfizer, Pharmacyclics, 82 ProteoDesign SL, Rafael Pharmaceuticals, Roche Diagnostics, Sanofi, SeaGen, Seattle Genetics, 83 Servier, Symphogen, Taiho, and VCN Biosciences. T Yoshino reports research funding received from 84 Chugai, Daiichi Sankyo, Dainippon Sumitomo Pharma, GSK, MSD, Novartis, Ono, Parexel, and Sanofi. 85 All remaining authors have declared no conflicts of interest. 86 87
Word count (main text): 2747 88
Number of Figures: 4 89
Number of Tables: 1 90
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

4
Translational Relevance 91
The BEAMing technology with the OncoBEAMTM RAS CRC Kit can detect the plasma RAS status in 92
patients with metastatic colorectal cancer (mCRC). However, the concordance rate in circulating 93
tumor DNA (ctDNA) and tumor tissue RAS status varies by metastatic site. We conducted the first 94
international collaboration study on the concordance rate of liquid and tumor biopsy RAS status by 95
metastatic site. The utility of OncoBEAMTM may depend on tumor burden and/or the metastatic site. 96
There is no need to consider the cut-off for patients with only liver metastases. The baseline longest 97
diameter and number of lesions are associated with the concordance rate. Peritoneal metastases 98
alone with a lesion diameter <20 mm, lung metastases alone with a lesion diameter <20 mm, and 99
<10 lesions are discordant for ctDNA testing. Careful consideration should be given to patients with 100
mCRC with lung or peritoneal metastases only when using liquid biopsy. 101
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

5
Abstract 102
Background: OncoBEAMTM is a circulating tumor DNA (ctDNA) test that uses the BEAMing digital 103
polymerase chain reaction technology. We clarified the association between the baseline tumor 104
burden and discordance in the RAS status by metastatic sites in patients with a single metastatic site. 105
Patients and methods: Data from previous Spanish and Japanese studies investigating the 106
concordance of the RAS status between OncoBEAMTM and tissue biopsy in 221 patients with 107
metastatic colorectal cancer (mCRC) were used. We collected data from patients with liver, 108
peritoneal, or lung metastases and evaluated the concordance rates according to the metastatic site 109
and the association between the concordance rate and tumor burden. 110
Results: Patients had metastases in the liver (n=151), peritoneum (n=25), or lung (n=45) with 111
concordance rates of 91% (95% confidence interval, 85–95%), 88% (68–97%), and 64% (49–78%), 112
respectively. Factors associated with concordance included the baseline longest diameter and lesion 113
number (P=0.004), and sample collection interval (P=0.036). Concordance rates ≥90% were observed 114
in the following groups: liver metastases alone, regardless of the baseline longest diameter and 115
lesion number; peritoneal metastases alone in patients with a baseline longest diameter ≥20 mm; 116
and lung metastases alone in patients with a baseline longest diameter ≥20 mm and/or number of 117
lesions ≥10. 118
Conclusion: Plasma ctDNA-based liquid biopsy in patients with mCRC may be useful depending on 119
the metastatic site. The maximum diameter and lesion number should be carefully considered when 120
determining patients' RAS status with only peritoneal or lung metastases. 121
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

6
Introduction 122
Colorectal cancer (CRC) is the third most common cause of cancer death, and the fourth most 123
diagnosed cancer worldwide (1). Substantial progress has been made in treating metastatic CRC 124
(mCRC) through the development of anti-vascular endothelial growth factor and anti-epidermal 125
growth factor receptor (anti-EGFR) monoclonal antibodies (mAbs) (2, 3). However, several studies 126
have reported that patients with mCRC with tumors harboring RAS mutations are unlikely to benefit 127
from anti-EGFR antibodies (2, 3); therefore, such therapies are not recommended (4). 128
Almost all patients with mCRC have low but detectable levels of cell-free circulating tumor DNA 129
(ctDNA), in which tumor mutations can be characterized (5). Liquid biopsy is highly sensitive for 130
detecting mutations present at low frequencies. 131
The OncoBEAMTM RAS CRC Kit, which uses highly sensitive BEAMing digital polymerase chain 132
reaction (PCR) technology (6–8), is an in vitro diagnostic tool that has been CE-marked (conformity 133
with health, safety, and environmental protection standards for products sold within the European 134
Economic Area) and approved by the Pharmaceuticals and Medical Devices Agency in Japan for 135
detecting plasma RAS mutations in patients with mCRC. This kit has been widely used for patients 136
whose tissues are difficult to collect and who are planned to be treated with anti-EGFR antibody re-137
challenge. A comparison between the use of BEAMing technology to determine the RAS mutational 138
status in plasma ctDNA and the reference method of tumor tissue DNA in previous clinical trials 139
revealed concordance rates between 86% and 93% in all patients with mCRC regardless of the 140
metastatic sites (9–13). 141
Previous studies of small numbers of patients suggested that the concordance rates in ctDNA and 142
tissue RAS mutational status varied by metastatic site (9, 10). An adequate concordance between 143
the plasma and tissue RAS mutational status was observed in patients with mCRC with liver 144
metastases alone (9, 10). Although they were thought to be associated with a significant discordance 145
in patients with only lung metastases, the baseline longest diameter and number of lesions in the 146
lungs were significantly associated with concordance (9). Moreover, a range of concordance rates 147
depending on the metastatic site was suggested in previous studies (9, 10). 148
We integrated individual patient data from cases evaluated in previous studies (9–11) wherein the 149
RAS status in ctDNA using the OncoBEAMTM RAS CRC Kit was examined. Through a combined analysis, 150
we investigated the clinical factors associated with concordance between the plasma and tissue RAS 151
mutational status in patients with mCRC with liver, peritoneal, or lung metastases only to identify 152
individuals eligible for liquid biopsy analysis. 153
Materials and Methods 154
Study design and patients 155
Individual patient data from one Japanese (9) and two Spanish studies (10, 11) (n=659), which 156
examined the concordance rates between plasma and tissue RAS mutational status using the 157
OncoBEAMTM RAS CRC Kit and tissue reference method, respectively, were integrated. Patients who 158
met the following criteria were selected (n=261, CONSORT diagram, Supplementary Fig. S1): (1) 159
patients with pathologically confirmed metastatic colorectal adenocarcinoma; (2) patients who were 160
chemo-naïve or confirmed to have a progressive disease without having initiated subsequent 161
treatment; (3) patients with no prior treatment with anti-EGFR mAb or regorafenib; (4) patients with 162
only liver metastases, peritoneal metastases, or lung metastases; and (5) patients with no tumor 163
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

7
removal before blood sample collection. The interval between plasma collection and CT was ≤ 3 164
months. 165
166
Tumor burden data for post-hoc analysis was obtained by investigating the baseline longest 167
diameter of the largest lesion and number of tumor lesions on computerized tomography (CT) within 168
three months before or after ctDNA sample collection. Scatterplots of concordant and discordant 169
cases based on the tumor burden data were used to confirm the significance of the cut-offs. This 170
combined study was approved by the ethics & review committees at each institution, and all 171
patients provided written informed consent. All procedures related to the study were performed in 172
accordance with the Helsinki Declaration and the Ethical Guidelines for Medical Health Research 173
Involving Human Subjects in Japan and Spain. 174
Study outcomes 175
This study's primary outcome was to investigate the clinical factors associated with concordance 176
between the plasma and tissue RAS mutational status. The secondary outcome was to determine 177
the optimal cut-offs for clinical factors to maintain a sufficient concordance greater than 90% at each 178
metastatic site. 179
Statistical analysis 180
Continuous variables were described using medians and ranges, whereas categorical variables were 181
presented as percentages. The concordance between the plasma and tissue RAS mutational status in 182
the overall cohort, RAS mutant concordance based on tissue RAS mutant cohort, and RAS wild 183
concordance based on tissue RAS wild cohort were calculated with 95% confidence intervals (CIs) 184
and tested using Fisher's exact test. 185
Factors associated with concordance were calculated using univariate and multivariate logistic 186
regression models. Multivariate analysis was performed for factors with P<0.1 based on univariate 187
analysis. Variables were entered directly if P<0.1 in the univariate analysis. Statistical analyses were 188
performed using R version 3.6.1. 189
Results 190
Of the 261 patients with mCRC who were initially enrolled (CONSORT diagram, Supplementary Fig. 191
S1), 40 were excluded because of missing measurements for the baseline longest diameter or 192
number of lesions (n=15) or due to an interval of more than three months between plasma 193
collection and CT (n=25). The full analysis set comprised 221 patients who had liver metastases 194
alone (n=151), peritoneal metastases alone (n=25), and lung metastases alone (n=45). Patient 195
characteristics categorized by metastatic sites are shown in Supplementary Table S1. The cut-offs for 196
the baseline longest diameter and number of lesions were provisionally set to 20 mm and 10 lesions, 197
respectively, based on a previous report (9). 198
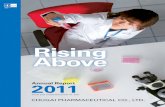
The overall concordance rate in liver metastases alone was 91% (95% Cl 85–95), whereas those of 199
peritoneal and lung metastases alone were 88% (95% CI 68–97) and 64% (95% CI 49–78), 200
respectively. Similar trends were observed in the European and Asian subsets (Fig. 1). The 201
concordance rate of lung metastases alone was relatively low compared with that of liver or 202
peritoneal metastases alone. The mean of mutation allele fraction (MAF) of liver, peritoneum, and 203
lung was 6.8%, 7.2%, and 2.6%, respectively. The MAF is relatively low in lung metastases alone, as 204
shown in Supplementary Fig. S2. 205
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

8
RAS mutations were detected in 39% and 47% of plasma and tissue samples, respectively. The 206
overall concordance between plasma- and tissue-based analyses was 85% (188/221; 95% CI 80–89), 207
with 76% (79/104; 95% CI 66–84) RAS mutant concordance based on tissue RAS mutant cohort and 208
93% (109/117; 95% CI 87–97) RAS wild concordance based on tissue RAS wild cohort. The RAS 209
mutant concordance was significantly lower than the RAS wild concordance(p<0.001). Almost no 210
difference in the concordance rate for each codon of RAS was observed (data not shown). 211
Univariate/multivariate analysis of the clinical findings between concordant and discordant cases 212
was conducted. The analysis for identifying factors associated with discordance is described in 213
Supplementary Table S2. On multivariate analysis, the most significant factor associated with 214
concordance was the baseline longest diameter of the lesion and the number of lesions (P=0.004) 215
(Table 1). Both factors are related to tumor burden and are evaluable factors in clinical practice; thus, 216
these values were adopted as cut-offs to select concordant cases in this study. 217
Furthermore, univariate and multivariate analyses of the clinical findings by tissue RAS mutational 218
status between concordant and discordant cases were conducted (Supplementary Tables S3 and S4). 219
In the tissue RAS mutant cohort, the analysis for identifying factors associated with discordance is 220
described in Supplementary Table S3. In multivariate analysis of the tissue RAS mutant cohort, the 221
significant factors associated with the RAS mutant concordance were collection interval (P=0.004), 222
baseline longest diameter, and number of lesions (P=0.005) as it is with the overall cohort. On the 223
other hand, there was no significant factor in univariate analysis of the tissue RAS wild cohort 224
(Supplementary Table S4). 225
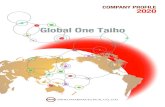
The concordance rate in the liver metastases alone was over 90%, with any cut-off value used (Fig. 2). 226
Using the baseline longest diameter of lesion ≥20 mm as a cut-off, the concordance rate of 227
peritoneal metastases alone was 94%, providing a sufficient concordance and indication for 228
OncoBEAMTM testing, with a coverage of 68%, that is, this cut-off covered 68% of patients with liver 229
metastases. The reliability of using the cut-off of a baseline longest diameter ≥20 mm for patients 230
with mCRC with peritoneal metastases alone was reflected by a high RAS mutant concordance of 86% 231
(95% CI 42–99), along with 100% (95% CI 66–100) RAS wild concordance. Using 20 mm as the cut-off 232
value for the baseline longest diameter in peritoneal metastases alone, 67% (2/3) of discordant 233
cases were below the cut-off value, and 73% (16/22) of concordant cases were above the cut-off 234
(Supplementary Fig. S3). 235
The concordance rate for lung metastases alone using the cut-off of the baseline longest diameter 236
≥20 mm alone was 90%, but the coverage was poor (22%) (Fig. 2). Similarly, when the number of 237
lesions ≥10 alone was used as a cut-off, the concordance rate for lung metastases alone was 89%, 238
with poor coverage of 20% (Supplementary Fig. S4). However, the concordance rate of lung 239
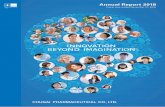
metastases alone increased to 94%, with improved coverage of 38% when using the cut-off of a 240
baseline longest diameter ≥20 mm and ≥10 lesions (Fig. 3) with 88% RAS mutant concordance. Most 241
discordant cases (94%, 15/16) occurred in the baseline longest diameter of lung lesions<20 mm and 242
<10 lesions (Fig. 4, as shown in the black square). Concordance within and without the cut-offs were 243
46% (95% CI 28–66) and 94% (95% CI 69–100), respectively, showing a significant difference 244
(P<0.001). 245
Discussion 246
This is the first combined analysis of individual patient data from Europe and Asia on the 247
concordance of RAS mutational status by metastatic site between plasma ctDNA and tumor tissue 248
DNA testing (14). There were no differences between the European and Asian data. We found that 249
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

9
the concordance rates differed by the metastatic site. Although there is currently no clear 250
explanation for this result, the effects may have been organ-specific. Therefore, it is necessary to 251
investigate the clinical factors associated with high concordance in each metastatic site so that 252
patients with these clinical factors can be selected for OncoBEAMTM-based detection of their RAS 253
mutational status. 254
In our multivariate statistical model, the most significant concordance factors were the baseline 255
longest diameter and the number of lesions (P=0.004), followed by the sample collection interval 256
(P=0.036). Tumor burden (that is, baseline longest diameter and number of lesions) impacts the 257
amount of ctDNA released into plasma (15). Thus, an increasing amount of ctDNA results in 258
increased concordance rates. The baseline longest diameter and number of lesions can be easily 259
measured and implemented in clinical practice. Additionally, the sample collection interval has been 260
associated with discordance, in which longer intervals between plasma and tissue collections may 261
contribute to clonal evolution (9, 16). 262
For patients with liver metastases alone, the concordance rate was high in Europe and Asia. As such, 263
the lesion diameter and number are not necessary to select patients for testing using the 264
OncoBEAMTM RAS CRC Kit. The median mutant allele fraction (MAF) was higher in liver metastases 265
than in peritoneal and lung metastases (9, 10, 12, 17). Bachet et al. reported that primary tumor 266
resection and the presence of liver metastases were significantly associated with the presence of 267
ctDNA, although liver metastases appeared to be the key factor (18). Elez et al. observed a high MAF 268
burden in liver metastases, which was not related to the volume and number of lesions in liver 269
metastases (17). ctDNA is thought to be easily released into the circulation regardless of the tumor 270
size or lesion number in the liver. 271
In previous studies, patients with peritoneal metastases alone showed a low MAF burden (12, 17). 272
MAF from patients with only peritoneal metastases was lower than in patients with peritoneal 273
metastases and at least one other metastatic site (12). The discordance was associated with the 274
presence of peritoneal metastases (18). However, our combined study revealed considerable high 275
concordance (88%) without setting a cut-off value. This may be because we enrolled cases in which 276
lesions could be detected by CT; a total of 68% (17/25) peritoneal metastases with the longest lesion 277
diameter ≥20 mm were included. Additionally, sufficient concordance and good coverage were 278
observed when we selected cases with the RAS wild concordance longest diameter ≥20 mm, with 279
high RAS mutant concordance and RAS wild concordance. In peritoneal metastases alone, the 280
maximum size may be related to the amount of ctDNA release. 281
In contrast, the concordance in patients with lung metastasis alone was extremely low in Europe and 282
Asia (9, 10), likely because of the low MAF (9, 10, 12, 17). Like previous studies, this study's results 283
also showed that the MAF with lung metastases tended to be lower than for other metastatic sites 284
(Supplementary Fig. S2). The release of ctDNA from lung metastases is thought to be extremely low; 285
thus, tumor burden plays a more important role in lung metastases. As such, the lesion size and 286
number must be determined to select appropriate patients with lung metastases alone for 287
OncoBEAMTM testing; that is, a closer evaluation of the tumor burden is required. These two factors 288
were also selected as cut-offs for patients with lung metastases alone in the Japanese study (9). 289
Under the cut-off value, a liquid biopsy may not detect RAS mutations in lung metastases. In such 290
cases, the tissue-based analysis would be the preferred choice. 291
In a post-hoc analysis, we reviewed the size and number of metastatic tumors of baseline CT in each 292
case. This is the first international collaborative study to evaluate the relationship between the 293
tumor burden and concordance by metastatic site between plasma- and tissue-based RAS 294
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

10
mutational analysis. This study reveals the impact of the tumor burden and organ specificity on 295
concordance rates. 296
In our study, the presence of previous chemotherapy was significantly associated with a higher 297
discordance than its absence for the overall cohort (P=0.045) (Supplementary Table S2). In univariate 298
analysis of clinical findings between concordant and discordant in overall and tissue RAS mutant 299
cohorts, previous chemotherapy was indicated to be one of the significant factors, as described in 300
Table1 and Supplementary Table S3 (P=0.032 and P=0.019, respectively); however, it was not a 301
significant factor in multivariate analysis for overall and RAS mutant cohorts (P=0.500 and P=0.214, 302
respectively). This study included 50 patients who received chemotherapy between tissue and 303
plasma collection. The mutational state was changed in 12 cases, including 10 cases (1 case in the 304
liver, 3 in the peritoneum, and 6 in the lung), which changed from mutant to wild type, suggesting 305
below limit-of-detection level (called NeoRAS) (19). All of the 10 cases had tumors with sizes <20 mm, 306
and each case had <10 lesions, indicating a low tumor burden. The collection interval between tissue 307
and plasma sampling is also a significant factor in the multivariate analysis for the overall and tissue 308
RAS mutant cohorts shown in Table1 and the Supplementary Table S3 (p=0.036 and p=0.004, 309
respectively), indicating that the tumor volume reduction as a result of chemotherapy may affect the 310
discordance of the tissue RAS mutant. Only 2 cases (1 case each in the lung and the liver) changed 311
from wild type to mutant during chemotherapy. These might be due to clonal evolution or tumor 312
heterogeneity, even in cases that did not receive targeting agents such as an anti-EGFR antibody 313
and/or a regorafenib. 314
In conclusion, the OncoBEAMTM RAS CRC Kit's utility in patients with mCRC may depend on the 315
metastatic site. Although no further selection is required for patients with liver metastases alone, 316
careful attention should be given to patients with peritoneal metastases alone with lesion size <20 317
mm, as well as those with lung metastases alone with lesion size <20 mm and <10 metastatic lesions 318
when determining the RAS mutational status using the ctDNA-based assay. 319
Acknowledgments 320
We would like to express our special gratitude to all participating patients, their families, and all 321
participating investigators. The authors thank P4 Statistics Co. Ltd., Tokyo, for providing support 322
during the statistical analyses, and Celestina Chin and Yen May Ong of MIMS Pte Ltd., Singapore, for 323
providing medical writing support/editorial support. We also thank Editage (www.editage.com) for 324
English language editing, which was funded by Sysmex Corporation, Japan, in accordance with Good 325
Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). 326
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

11
References 327
1. Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: incidence, mortality, survival, 328 and risk factors. Prz Gastroenterol 2019;14:89–103. 329 2. Bokemeyer C, Köhne CH, Ciardiello F, Lenz H-J, Heinemann V, Klinkhardt U, et al. FOLFOX4 plus 330 cetuximab treatment and RAS mutations in colorectal cancer. Eur J Cancer 2015;51:1243–52. 331 3. Van Cutsem E, Lenz H-J, Köhne C-H, Heinemann V, Tejpar S, Melezínek I, et al. Fluorouracil, 332 leucovorin, and irinotecan plus cetuximab treatment and RAS mutations in colorectal cancer. J Clin 333 Oncol 2015;33:692–700. 334 4. Yoshino T, Arnold D, Taniguchi H, Pentheroudakis G, Yamazaki K, Xu R-H, et al. Pan-Asian adapted 335 ESMO consensus guidelines for the management of patients with metastatic colorectal cancer: a 336 JSMO-ESMO initiative endorsed by CSCO, KACO, MOS, SSO and TOS. Ann Oncol 2018;29:44–70. 337 5. Bettegowda C, Sausen M, Leary RJ, Kinde I, Wang Y, Agrawal N, et al. Detection of circulating 338 tumor DNA in early- and late-stage human malignancies. Sci Transl Med 2014;6:224ra24. 339 6. Diehl F, Li M, He Y, Kinzler KW, Vogelstein B, Dressman D. BEAMing: single-molecule PCR on 340 microparticles in water-in-oil emulsions. Nat Methods 2006;3:551–9. 341 7. Diehl F, Schmidt K, Choti MA, Romans K, Goodman S, Li M, et al. Circulating mutant DNA to assess 342 tumor dynamics. Nat Med 2008;14:985–90. 343 8. Vivancos A, Aranda E, Benavides M, Élez E, Gómez-España MA, Toldeano M, et al. Comparison of 344 the clinical e of the Idylla platform and the OncoBEAM RAS CRC assay for KRAS mutation detection in 345 liquid biopsy samples. Sci Rep 2019;9:8976. 346 9. Bando H, Kagawa Y, Kato T, Akagi K, Denda T, Nishina T, et al. A multicentre, prospective study of 347 plasma circulating tumour DNA test for detecting RAS mutation in patients with metastatic 348 colorectal cancer. Br J Cancer 2019;120:982–6. 349 10. García-Foncillas J, Tabernero J, Élez E, Aranda E, Benavides M, Camps C, et al. Prospective 350 multicenter real-world RAS mutation comparison between OncoBEAM-based liquid biopsy and 351 tissue analysis in metastatic colorectal cancer. Br J Cancer 2018;119:1464–70. 352 11. Grasselli J, Elez E, Caratù G, Matito J, Santos C, Macarulla T, et al. Concordance of blood- and 353 tumor-based detection of RAS mutations to guide anti-EGFR therapy in metastatic colorectal cancer. 354 Ann Oncol 2017;28:1294–301. 355 12. Vidal J, Muinelo L, Dalmases A, Jones F, Edelstein D, Iglesias M, et al. Plasma ctDNA RAS mutation 356 analysis for the diagnosis and treatment monitoring of metastatic colorectal cancer patients. Ann 357 Oncol 2017;28:1325–32. 358 13. Schmiegel W, Scott RJ, Dooley S, Lewis W, Medlrum CJ, Pockney P, et al. Blood-based detection 359 of RAS mutations to guide anti-EGFR therapy in colorectal cancer patients: concordance of results 360 from circulating tumor DNA and tissue-based RAS testing. Mol Oncol 2017;11:208–19. 361 14. Galvano A, Taverna S, Badalamenti G, Incorvaia L, Castiglia M, Barraco N, et al. Detection of RAS 362 mutations in circulating tumor DNA: a new weapon in an old war against colorectal cancer. A 363 systematic review of literature and meta-analysis. Ther Adv Med Oncol 2019;11:1–15. 364 15. Thierry AR, Mouliere F, Gongora C, Ollier J, Robert B, Ychou M, et al. Origin and quantification of 365 circulating DNA in mice with human colorectal cancer xenografts. Nucleic Acid Res 2010;38:6159–75. 366 16. Siravegna G, Mussolin B, Buscarino M, Corti G, Cassingena A, Crisafulli G, et al. Clonal evolution 367 and resistance to EGFR blockade in the blood of colorectal cancer patients. Nat Med 2015;21:795–368 801. 369 17. Elez E, Chianese C, Sanz-García E, Martinelli E, Noguerido A, Mancuso FM, et al. Impact of 370 circulating tumor DNA mutant allele fraction on prognosis in RAS-mutant metastatic colorectal 371 cancer. Mol Oncol 2019;13:1827–35. 372 18. Bachet JB, Bouché O, Taieb J, Dubreuil O, Garcia ML, Meurisse A, et al. RAS mutation analysis in 373
circulating tumor DNA from patients with metastatic colorectal cancer: the AGEO RASANC 374
prospective multicenter study. Ann Oncol 2018;29:1211–9. 375
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

12
19. Henry J, Willis J, Parseghian CM, Raghav KPS, Johnson B, Dasari A, et al. NeoRAS: incidence of 376
RAS reversion from RAS mutated to RAS wild type. J Clin Oncol 2020;38(4_suppl):180. 377
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

13
Table 378
Table 1. Univariate and multivariate analyses of clinical findings between concordant and discordant 379
cases in the overall cohort. 380
Categorical variablesa
Univariate analysis Multivariate analysis
Odds ratio [95% CI] P value
b
Odds ratio [95% CI] P value
b
Age
1.0 [0.6, 1.7]
0.869 NA NA
Sex Male/female 1.4 [0.6, 3.3]
0.383 NA NA
Previous chemotherapy Yes/no 2.4 [1.1, 5.2]
0.032 0.7 [0.2, 2.0]
0.500
Location of primary tumorc Left/right 2.9
[1.0, 8.6] 0.059
2.0 [0.6, 6.8]
0.261
Metastatic site
Liver/other 0.3 [0.1, 0.6]
<0.001 0.9 [0.2, 3.9]
0.897
Peritoneum/other 0.8 [0.2, 2.7]
0.663 NA NA
Lung/other 5.2 [2.3, 11.4]
<0.001 1.8 [0.4, 8.1]
0.443
Collection interval (tissue vs. plasma)
2.2 [1.5, 3.3]
<0.001 1.9 [1.0, 3.3]
0.036
Source of tissue samples Metastasis/primary 1.9 [0.7, 5.7]
0.237 NA NA
Baseline longest diameter and number of lesions
<20 mm and <10, or ≥20 mm and ≥10
5.0 [2.3, 10.9]
<0.001 3.8 [1.5, 9.5]
0.004
Resection of primary tumor
Yes/no 3.8 [1.1, 13.1]
0.032 1.4 [0.3, 5.6]
0.633
CEA <5 ng/mL or ≥5 ng/mL 1.6 [0.7, 3.6]
0.296 NA NA
aThe second category for each variable was used as reference in the model to calculate the odds ratio.
381
bP values were derived using Fisher's exact test for categorical variables and the Kruskal–Wallis test 382
for continuous variables. 383 cLeft includes splenic flexure to rectum; right includes caecum to transverse colon. 384 CEA, carcinoembryonic antigen: NA, not available. 385 386
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

14
Figure Legends 387
388
Fig. 1. Combined analysis of concordance in the RAS mutational status between plasma- and tumor 389
tissue-based analyses for individual metastatic sites: (A) single-organ limited; (B) liver metastases 390
alone, (C) peritoneal metastases alone, and (D) lung metastases alone. CI, confidence interval. 391
392
Fig. 2. Concordance and coverage with an optimal cut-off of the baseline longest diameter of lesions 393
alone. Coverage refers to the percentage of patients having the specific metastatic lesions 394
(liver/peritoneal/lung) covered or included in the categories specified by lesion size, as defined by 395
computerized tomography. 396
397
Fig. 3. Concordance and coverage with optimal cut-offs of the baseline longest diameter of lesions 398
and number of lesions in lung metastases alone. The concordance rate of lung metastases increased 399
to 94%, with an improved coverage rate of 38%, when using the cut-off of baseline longest diameter 400
of ≥20 mm or ≥10 lesions. Coverage refers to the percentage of patients having the specific 401
metastatic lesions (liver/peritoneal/lung) covered or included in the categories specified by lesion 402
size and numbers, as defined by computerized tomography. 403
404
Fig. 4. Scatterplot of concordant and discordant cases based on baseline longest diameter and 405
number of lesions to confirm the optimal cut-offs in lung metastases alone. 406
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677

Published OnlineFirst February 18, 2021.Clin Cancer Res Yoshinori Kagawa, Elena Elez Fernandez, Jesús García-Foncillas, et al. Cancer with a Single Metastasis Site: The METABEAM Study
Mutations in ColorectalRASTumor Tissue Biopsies for Combined Analysis of Concordance between Liquid and
Updated version
10.1158/1078-0432.CCR-20-3677doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2021/02/16/1078-0432.CCR-20-3677.DC1
Access the most recent supplemental material at:
Manuscript
Authorbeen edited. Author manuscripts have been peer reviewed and accepted for publication but have not yet
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2021/02/17/1078-0432.CCR-20-3677To request permission to re-use all or part of this article, use this link
Research. on August 16, 2021. © 2021 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 18, 2021; DOI: 10.1158/1078-0432.CCR-20-3677