Colorectal Screening FOBT
12
Colorectal Screening Using Hemocult II Slides (FOBT) Annual Physical Exam Ages 50-75 Thomas Desnoyers, Terri Hupfer, Elyssa Lakich, Nancy Moua, Elaine Reyes-Simmons, and Travis Whitson
-
Upload
dmfreedom1 -
Category
Documents
-
view
213 -
download
0
Transcript of Colorectal Screening FOBT

Colorectal Screening Using Hemocult II
Slides (FOBT)Annual Physical Exam Ages 50-75
Thomas Desnoyers, Terri Hupfer, Elyssa Lakich, Nancy Moua, Elaine Reyes-Simmons, and Travis Whitson
Demographics• U.S. Preventative Task Force recommended for annual
colorectal screening of adults between 50-75 years old. • California is home to more than 37 million people.(1)
• The U.S. Census Bureau estimates that about 22 percent of California’s population will be over age 60 by the year 2030, an increase of 34 percent from 2012.(1)
• 49.7% males and 50.3% females(2)
• Racial/Ethnic breakdown of : 57.6% whites; 37.6 % Latino; 17.5% some other race or two or more races; 13.4% Asian, Native Hawaiian and other Pacific Native; 6.2% black, and 1% American Indian and Alaska Native.(2)
Demographics• Though incidence rates have dropped over the past few years
(a decrease of 25-30% from 1988-2007) colorectal cancer still affects approximately 14,000 Californians a year. Colorectal cancer is responsible for nearly 5000 deaths per year, second only to lung cancer as a cause of cancer death in California.
• Though screening tests such as the fecal occult blood test are available, more than half of the cases in California are still diagnosed at a late stage, after it has spread from the colon, making the morbidity and mortality much higher than it would be if the cancer was found at a time of precancerous polyps.
• Five year survival rate for those diagnosed prior to spread from the colon is 90%. This drops to 66% once it spreads to the regional lymph glands and 10% if it has spread to distal organs, making early diagnosis crucial.
Frame Criteria• Effect on quality and quantity of life
o Colorectal Cancer is the third most common cancer and the second leading cause of general death (1)
o Screening with any of the three recommended tests reduces colorectal cancer mortality (1)
o Death from colorectal cancer are preventable by combo of screening and early treatment of precursor lesions (2)
• Screening detects early stage cancer and adenomatous polyps (1)
o Colonoscopy is reference standard but significant morbidity is associated – perforation, major bleeding, diverticulitis, severe abdominal pain, and even death(1)
o Less invasive screening (Hemoccult II) decreases need for colonoscopy and associated morbidity• Harm assessed by US Preventative Services Task Force is no greater than
small(1)
• Available Acceptable Methods of Screening – USPSTF recommendationo High-Sensitivity Fecal Occult Blood Testing (FOBT) – annuallyo Flexible Sigmoidoscopy – every 5 years with FOBT every 3 yearso Colonoscopy – every 10 yearso Colorectal Cancer Screening is identified as high-impact, cost-effective service (3)
Frame Criteria• Asymptomatic Period for Detection and Treatment
o Most patients remain asymptomatic until advanced disease (2)
• Advanced disease symptoms vague (abdominal cramping, changes in bowel habits) (2)
• Many patients do not seek medical attention until rectal bleeding (late sign) (2)
• Asymptomatic Treatment Yields Superior Results Compared to Delay Until Treatment for Symptomso Survival Rates correlate to stage at time of discovery (2)
• Early, localized - 5 yr survival rate 90% (2)
• Regional metastasis to adjacent organs/lymph nodes - 5 yr rate 68% (2)
Frame Criteria• Acceptable Tests Available at Reasonable Cost
o “Fecal occult blood tests are the most affordable and least invasive of the various screening tests available for colorectal cancer.” (1)
o Hemoccult II costs about $5 per test (1)
o Flexible Sigmoidoscopyo Colonoscopy
• Incidence Sufficient to Justify Cost of Screeningo >142,000 persons diagnosed and >53,000 died of colorectal cancer in
2007(2)
• 10,000 could be prevented each year if all adults >50 were offered screening ($11,900 per life year saved) (2)
• Increasing screening would have greatest impact on reducing mortality vs reducing risk factors or increasing treatment (2)

Evidence Based Practice – Recommendation and Rationale• Recommendation
o Strongly recommended that clinicians routinely provide guaiac-based FOBT for asymptomatic individuals older than 50 years at least annually to reduce mortality from colorectal cancer. FOBT is easy and inexpensive and poses no risk to the patient.
o Individuals should be informed that annual testing is necessary to achieve the fullest potential of this test and that they will need follow-up colonoscopy if test results are positive.
• Rationaleo There is convincing evidence that screening reduces colorectal cancer
mortality in adults age 50 to 75 years. Follow-up of positive screening test results requires colonoscopy regardless of the screening test used. Because of the harms of colonoscopy, the chief benefit of less invasive screening tests is that they may reduce the number of colonoscopies required and their attendant risks.

Reliability and Validity• The relative sensitivity and specificity of the
different colorectal screening tests with adequate data to assess cancer detection—colonoscopy, flexible sigmoidoscopy, and fecal tests—can be depicted as follows:o Sensitivity: Hemoccult II < fecal immunochemical tests <
Hemoccult SENSA < flexible sigmoidoscopy < colonoscopyo Specificity: Hemoccult SENSA < fecal immunochemical tests ≈
Hemoccult II < flexible sigmoidoscopy = colonoscopy
Characteristics of High Quality FOBT Screening (Implications for Practice)• Never use in office FOBT at the time of digital rectal exam as a
screening test for colorectal cancero Rationale: Studies have shown that a guaiac FOBT obtained on a single
stool sample obtained at the time of in- office digital rectal exam may miss up to 95% of cancers and significant adenomas.
• Perform tests only on stool specimens collected by patients at their home; the number of specimens to be collected and the collection process should follow manufacturers’ recommendations. o Rationale: Studies that demonstrated decreases in incidence and
mortality with FOBT screening utilized home collection and analysis of specimens based on manufacturers’ instructions.
• Repeat stool tests annually.o Rationale: Annual testing significantly improves lesion detection over
time.• Any positive test should be followed up with colonoscopy.
o Rationale: Stool-based screening results in decreased colorectal cancer incidence and mortality only when screen-detected abnormalities are assessed and managed appropriately.
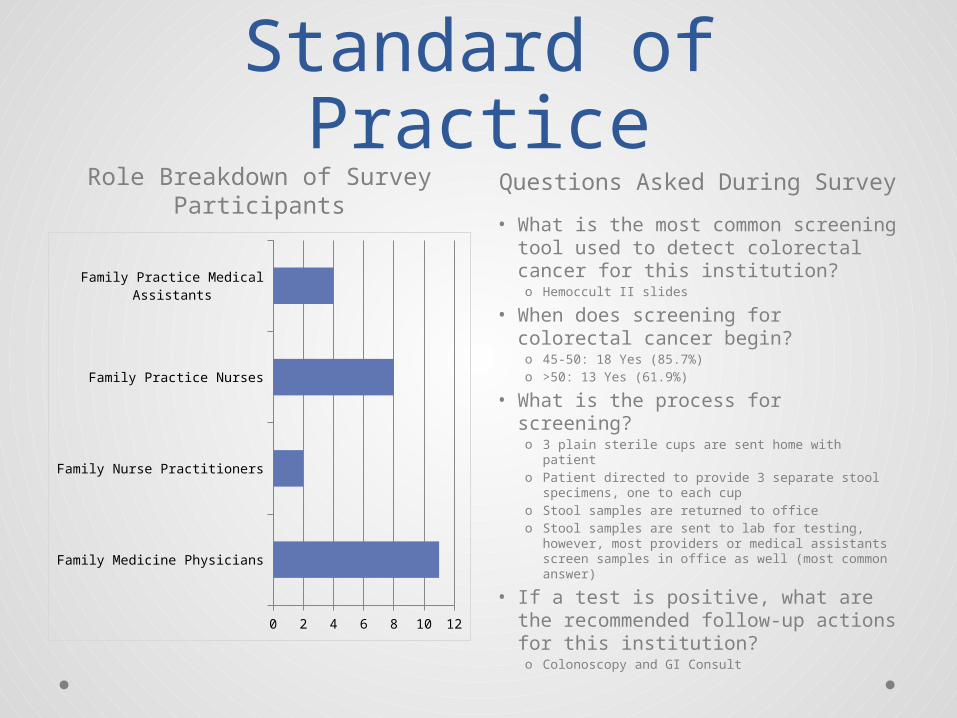
Assessment of Standard of PracticeRole Breakdown of Survey
ParticipantsQuestions Asked During Survey
Family Medicine Physicians
Family Nurse Practitioners
Family Practice Nurses
Family Practice Medical Assistants
0 2 4 6 8 10 12
• What is the most common screening tool used to detect colorectal cancer for this institution?o Hemoccult II slides
• When does screening for colorectal cancer begin?o 45-50: 18 Yes (85.7%)o >50: 13 Yes (61.9%)
• What is the process for screening?o 3 plain sterile cups are sent home with patiento Patient directed to provide 3 separate stool
specimens, one to each cup o Stool samples are returned to officeo Stool samples are sent to lab for testing,
however, most providers or medical assistants screen samples in office as well (most common answer)
• If a test is positive, what are the recommended follow-up actions for this institution?o Colonoscopy and GI Consult
Ethical and Economic Issues
Colonoscopy Hemoccult II Screening• Evidence is adequate to estimate
the harms of colonoscopy. In the U.S. perforation of the colon occurs in an estimated 3.8 per 10,000 procedures. Serious complications defined as deaths attributable to colonoscopy or adverse events requiring hospital admission, including perforation, major bleeding, diverticulitis, severe abdominal pain, and cardiovascular events are more common, 25 per 10000 procedures.
• Cost: Deductible for colorectal cancer screening waived for Medicare patients. Patients responsible for copay if screening colonscopy results in removal of polyp, thus becoming “therapeutic procedure.”
• Evidence about the harms of fecal tests is lacking (inadequate), but the USPSTF assesses them to be no greater than small.
• Cost: $4.50 as part of annual screening covered twice per year per Medicare, regardless if the screening procedure leads to a “therapeutic procedure.”
Legal Issues• The USPSTF found evidence of harms associated with different colorectal
screening programs. With all colorectal cancer screening modalities, a positive test result leads to follow-up testing, specifically colonoscopy, to resolve the diagnosis. This invasive procedure can result in serious morbidity as well as anxiety, inconvenience, discomfort, and additional medical expenses.
• Colonoscopyo Perforation from colonoscopy occurs in an estimated 3.8 per 10,000 procedures in the
United States; major bleeding is estimated to occur in 12.3 per 10,000 procedures (95% CI, 7.8 to 19.3 per 10,000 procedures). Serious complications—deaths from colonoscopies in asymptomatic populations or events requiring hospital admission, including perforation, major bleeding, diverticulitis, severe abdominal pain, and cardiovascular events—are estimated at 25 per 10,000 procedures (CI, 12 to 76 per 10,000 procedures).
• Flexible Sigmoidoscopyo Serious complications—deaths from flexible sigmoidoscopy in asymptomatic populations
or events requiring hospital admission, including perforation, major bleeding, severe abdominal symptoms, and syncope—were fewer than with colonoscopy. The rate of serious complications is estimated at 3.4 per 10,000 procedures (CI, 0.6 to 19 per 10,000 procedures). Perforation from flexible sigmoidoscopy was relatively uncommon, with a point estimate of 4.6 per 100,000 procedures (CI, 0.36 to 59 per 100,000 procedures). Proportions for other complications were not calculated because of a lack of reliable data.