Colorectal OR CUSPweb2.facs.org/download/Makary-Wick.pdf• SSI is the most common complication...
38
Colorectal OR CUSP Elizabeth C. Wick, M.D. Acknowledgement to the entire CUSP Team
Transcript of Colorectal OR CUSPweb2.facs.org/download/Makary-Wick.pdf• SSI is the most common complication...

Colorectal OR CUSP
Elizabeth C. Wick, M.D.
Acknowledgement to the entire CUSP Team

Background
• SSI is the most common nosocomial infection in the surgical patient
• SSI is the most common complication after colorectal abdominal surgery
• SSI is associated with increased mortality, length of stay and readmission
• An SSI costs between $6,200-15,000/per patient*
• Approximately 320,000 colorectal operations per year, national cost in the 100s of millions of dollars
*Smith et al, Ann Surg, 2004Wick et al, Archives Surg, 2011

BackgroundNSQIP report 2009
8/7/2012 3
Johns Hopkins

CUSP Goals
1. Improve team work and work place safety culture in the perioperative setting with the goal of improving surgical outcomes
2. Integrate safety practices into daily work

CUSP for Surgery:Applied to SSI prevention
Comprehensive Unit Based Safety Program
Component Method
1. Science of safety education Introductory talk to explain the approach to addressing safety at a local level
2. Staff Safety Assessment Two question survey to team members asking: 1) How will the next patient develop an SSI? 2) What can we do to prevent an SSI?
3. Senior executive partnership Senior executive attends CUSP meetings, making resources available to address safety concerns and assist with system-wide barriers
4. Learning from defects Teams are trained to use a structured tool to learn from defects
5. Implement teamwork and communication tools Review unit-level safety data (e.g. SSI) monthly and develop local quality improvement initiatives to improve teamwork, communication and address identified hazards

Team
Leadership:• Surgeon Champion• Anesthesiologist Champion• CRNA Champion• Nursing Champion• Coach• Hospital Executive• NSQIP SCR
Members:• 5 surgeons (>90% of
colorectal surgery at hospital)
• 20-30 GI RNs and techs• 6 CRNAs• 1 Anesthesiologist• 2 PACU/post-op RNs• 1 inpatient ward NP

Results of the two-question survey identifying local staff safety concerns and areas for improvement
Safety Issue Identified(% response)
Opportunities to Improve
Infection Control (68%) Skin preparation; hypothermia; contamination of bowel contents into the wound, antibiotic timing, selection and redosing; length of case;
Coordination of Care (12%) Increase utilization of preoperative evaluation center, improve surgical posting accuracy (case name and duration), computer assistance for antibiotic selection and redosing
Communication and Teamwork (12%) Improve communication throughout perioperative period, empower team members to speak up, improve compliance with briefings/debriefings, implement teamwork tools
Equipment/ Supplies (2%) Accurate temperature probes, point of care glucose monitoring, under body warmers, and sanitizing wipes near anesthesia machine
Policies/Protocols (2%) Standardize care/protocols/policies (5) , monitor sterile technique policies
Education/Training (2%) Ongoing education (with supportive data), development of a SSI prevention checklist
Journal of the American College of Surgeons, 2012, in press

Initial Areas of Focus
• Problem 1: Penicillin-allergic patients were not receiving proper prophylactic antibiotics
• Problem 2: Despite intra-op warmers patients were hypothermic in the recovery room
• Problem 3: Skin preparation was inconsistent
• Problem 4: Bowel instruments were used on skin

Kevin Driscoll CRNACRNA Lead
Deb Hobson RN“Coach”
Tracie Cometa RNLead RN
Mary Grace Hensel RNManager OR
Sean Berenholtz MDAnesthesia Lead
Lucy Mitchell RNNSQIP SCR
Elizabeth Wick MDSurgery Lead
Renee Demski MBASenior Director QualityJohns Hopkins Medicine
Executive
CoachNSQIPOutcomes
Steph Mullens CSTLead Tech

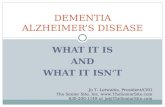
Gentamicin
Problem 1: Penicillin-allergic patients were not receiving proper prophylactic antibiotics
Stakeholders:Anesthesia, Surgery
Administrat ion IV push IV push 10-20 min. infusion 60 min. infusion prior to incision 30 min. infusion 60 min infusion per gram Redosing Interval During Surgery CrCl >60 Q4H (Cardiac Q2H) Q8H Q8H N/A Q8H Do not redose Q8H Q12H CrCl 30-60 Q6H (Cardiac Q4H) Q8H Q8H N/A Q8H Do not redose Q8H Q12H CrCl 10-29 Q8H (Cardiac Q6H) Q12H Q8H N/A Q12H Do not redose Q8H Q24H CrCl <10 or HD No redose (Cardiac Q6H) No redose Q8H N/A Do not redose Do not redose Q12H Do not redose FOR CEFOT ETAN AND CE FAZOL IN, RE-DOSE FOR EVERY 1500 CC OF BLOOD LOSS IF CrCl > 60
Pa tients receiving pre-op prophylactic antibiotics do not need additional antibiotics for prophylaxis for endocarditis or for existing orthopedic hardware. Call the Antibiotic Management Program (7-4570, pager 3-9229) or the pharmacy (5-6505) for assistance.
Procedure Prophylaxis Recommendations P CN Allergy Alter nate Prophylaxis Urologic surgery Transrectal prostate biopsy Cefotetan Ciprofloxacin
Transurethral surgery (e.g. TURP, TURBT, ureteroscopy, cystouretoscopy)
Cefazolin Gentamicin
Lithotr ipsy Cefazolin Gentamicin Nephrectomy or radical prostatectomy Cefazolin Clindamycin Radical cystectomy, cystoprostatectomy or anterior exenteration
Cefotetan Clindamycin PLUS Gentamicin
Penile or other prostheses Cefazolin OR [Vancomycn ± Gentamicin] [Clindamycin OR Vancomycn] ± Gentamicin Head and neck sur gery Major procedure with incision of oral or pharyngeal or sinus mucosa
Cefotetan Clindamycin
Major neck dissection or pa rotid dissection Cefazolin Clindamycin Thyroid/parathyroid surgery Prophylaxis not r ecommended Prophylaxis not recommended Tonsillectomy Clindamycin Clindamycin Cardiac surgery* Median sternotomy/uncomplicated heart transplant Cefazolin Vancomycin
Heart transplant – previous VAD or MRSA colonization/infection
Cefazolin PLUS Vancomycin Vancomycin
Pacemaker placement Cefazolin Clindamycin
Lung transplant Piperacillin/tazobactam 4.5 g IV Q6H If CF pa tient: please confirm with transplant surgery
Vancomycin PLUS Ciprofloxacin I f CF patient: please conf irm with tr ansplant surgery
LVAD/BIVAD placement Vancomycin PLUS Ciprof loxacin PLUS Fluconazole Vancomycin PLUS Ciprofloxacin PLUS Fluconazole
Vascular surgery All procedure s
Cefazolin Prophylaxis not r ecommended for carotid surgery unless risk of infection thought to be high
Vancomycin Prophylaxis not recommended for carotid surgery unle ss risk of infection thought to be high
Thoracic surgery All cases except esophageal Cefazolin Clindamycin
Esophageal cases Cefotetan Clindamycin
Neurosurgery Craniotomy (including shunt placement) Cefazolin Clindamycin
Spinal fusion Cefazolin Clindamycin OR Vancomycin
Laminectomy Cefazolin Clindamycin Gynecologic surgery Cesarean section Cefazolin Clindamycin
Hysterectomy (abdominal or vaginal) Uncomplicated:Cefazolin Complicated: Cefotetan Clindamycin
Repair of cystoce le or rectocele Cefazolin Clindamycin Dilation and curettage Uncomplicated: Prophylaxis not recommended
Complicated: Cefazolin Uncomplicated: Prophylaxis not r ecommended Complicated: Clindamycin
Orthopedic surgery Joint replacement Cefazolin Vancomycin Open reduction of fracture Cefazolin Vancomycin
Lower limb a mputation Cefotetan Clindamycin PLUS Gentamicin
Spinal fusion Cefazolin Clindamycin OR Vancomycin
Laminectomy Cefazolin Clindamycin
Arthroscopic surgery No data to support prophylaxis No data to support prophylaxis General surgery Inguinal hernia repair Uncomplicated: Prophylaxis not recommended
Complicated, recurrent or emergent: Cefotetan Uncomplicated: Prophylaxis not r ecommended Complicated, recur rent or emergent: Clindamycin ± Ge ntamicin
PEG Cefazolin OR Cefotetan Clindamycin ± Gentamicin
Gastrectomy/hepatectomy/cholecystectomy Cefotetan Clindamycin ± Gentamicin
Small bowel or colon surgery Cefotetan Clindamycin PLUS Gentamicin
Whipple procedure or pancreatectomy Cefotetan Clindamycin PLUS Ciprofloxacin Appendectomy (uncomplicated), if complicated or perfora ted, treat as peritonitis
Cefotetan Clindamycin PLUS Gentamicin
Penetrating abdominal trauma Cefotetan Clindamycin PLUS Gentamicin
Mastec tomy Prophylaxis not r ecommended Prophylaxis not recommended

Gentamicin
33%
92%
0
25
50
75
100
Before After
% o
f Pat
ient
s C
ompl
iant
Correct Dose of Gentamicin Received
Interventions:• Increased amount of
gentamicin available in the room
• Added dose calculator in anesthesia record
• Educated surgery, anesthesia and nursing in grand rounds
Despite >95% compliance on SCIP

Normothermia
Problem 2: Despite intra-op warmers patients were hypothermic in the recovery room
Stakeholders:Anesthesia, Nursing (Surgery)
• Frequent operating room delays result in 2nd and 3rd cases waiting in prep for hours
• Individual operating rooms do not have thermostat

Normothermia
83%95%
0
25
50
75
100
Before After
% o
f Pat
ient
s C
ompl
iant
Temperature > 36 °C post-op
Interventions:• Confirmed that
temperature probes were accurate (trial comparing foley and esophageal sensors)
• Initiated forced air warming in the pre-operative area

Skin Preparation
Problem 3: Skin preparation was inconsistent
Stakeholders:Nursing, Surgery
• No standardization of operating room skin preparation (no reference document or policy)
• Prep done by residents and medical students

Skin Preparation
Interventions:• Chlorhexidine wash cloths given to patients pre-
operatively
• Surgical skin preparation standardized to chloraprep(even in patients with ostomies)
• Prep responsibility shifted to circulating nurse from resident
• All nurses trained on chloraprep application

Instruments
Problem 4: Bowel instruments were used on skin
Stakeholders:Nursing/Techs, Surgery
• No “team members”• Nurses and techs
frequently not familiar with cases
• No education on contamination

Separation of “Dirty” and “Clean” Instruments
Intervention:• Built separate tray of
instruments used for bowel anastomosis
• Extra suction and bovie tip and gloves opened and changed after anastomosis
• Educational sessions with scrub techs and nurses about instrument separation
• Audits and education on the spot

CUSP Intervention Checklist
8/7/2012 18CompletedBy: Date:
ColorectalSSIProjectInterventionChecklist
1. CHLORAPREPWASHCLOTHSATHOME
2. PRE‐OPWARMING:Bairhuggerplacedonpatientinpre‐op.TemponadmissiontoPREP=_________________
TempwhenleavingPREP=___________________3. ROOMTEMPERATURE:warmedto72degreespriortopatientarrival4. ANTIBIOTICSELECTION
Standard:Cefotetan2gmorCefoxitin2gmPenicillinAllergy:Clindamycinplus
Gentamicin5mg/kg
5. SKINPREPARATION:ChloraprepcompletedbyRN6. INSTRUMENTS:Cleananddirtyinstrumentsseparated
Placecompletedformin“ColorectalEnvelope”atControlDesk
PatientStickerCompleteforSurgeons:Wick,S.Gearhart,J.Efron,Marohn

0
5
10
15
20
25
30
35
40
45
Q3 2009 Q4 2009 Q1 2010 Q2 2010 Q3 2010 Q4 2010 Q1 2011 Q2 2011
Col
orec
tal S
SI ra
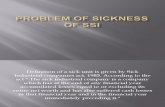
teSSI Rate and Interventions
Quarter 3Skin preparation protocolPre-op wash clothes
Quarter 4CUSP kickoffAntibiotic deficiencies addressed
Quarter1Pre-op warmingEnhanced sterile techniqueIntervention checklist
42 %
17 %
29 %26 %
16 %
20 % 19 % 18 %

Pre and Post Colorectal SSI Rates
Pre-intervention Post-intervention
Total OperationsOverall SSI
27827.3%
32418.2%*
Superficial SSI 16.9% 13.6%Deep SSI 1.4% 0.6%Organ Space 9.0% 4.0%*
* p<0.05Journal of the American College of Surgeons, 2012, in press

Johns Hopkins Colorectal TeamSAQ results (Fall 2011)
8/7/2012 21
Bottomline:We still have work to do

YEAR 2
8/7/2012 22

Building Capacity:Armstrong Institute Patient Safety Fellowship
Tracie Cometa, RN Kevin Driscoll, CRNA
• 16 hrs per week (Jan-June 2012)• 8 hrs classroom training on patient safety• 8 hrs protected time for quality improvement projects
8/7/2012 23

Briefing/Debriefing Form
The Johns Hopkins Hospital Operating Room Briefing/ Debriefing Tool©
Attending Surgeon to utilize this tool is to prompt open interdisciplinary communication before and after surgery to promote a clear understanding of specifics for each case.
ORMIS Case #___________________ Date ________________
Briefing – Before Every Procedure Team introductions – first and last names including roles (Circulator writes on board) Do the following match:
Patient ID band, Informed Consent (read out loud), Site Marking, OR posting, patient’s verbalization of procedure (if patient awake), other clinically relevant documentation (H&P, clinic note)
Do we have any safety, equipment, instrument, implant or other questions or concerns? Have antibiotics been given, if indicated? What are the anticipated times of antibiotic redosing? Is glycemic control/ beta blockers indicated? Is the patient positioned to minimize injury? Has the Prep been applied properly, without pooling and allowed to dry? Have the goals and critical steps of the procedure been discussed? Is the appropriate amount of blood available? Is DVT prophylaxis indicated? If so, what? Has the patient received anticoagulants? Any Special Precautions? If yes, describe. Are warmers on the patient? Is the time allotted for this procedure an accurate estimate? Has Attending reviewed latest/ final test results for Lab/ Radiology? Are Intraoperative X rays indicated?
____________________ _____________________ ________________________ Circulating Nurse Anesthesia Provider Attending Surgeon
Debriefing – After every procedure Could anything have been done to make this case safer or more efficient? Has the SSI data collection form been completed? Are the patient name/ history number and the surgical specimen name and laterality
on the paperwork? (Paperwork/ labeling to be independently verified by Surgeon) Did we have problems with instruments? Plan for transition of care to post-op unit discussed? To include:
Fluid Management/ blood (all slips in chart) Antibiotics – continue post-op (dose/interval) PACU tests/ Xrays Pain/ PCA plan New meds needed (immediate periop) Beta blockers (as required) Glycemic control (as required) DVT prophylaxis
_________________ ________________________ ________________________ Circulating Nurse Anesthesia Provider Attending Surgeon
Addressograph here
• No follow-up on comments
• Too long• Same form used in
all OR’s (neurosurgery, ortho, general surgery)
Staff had lostfaith

Briefing and Debriefing
• Team developed new form based on needs
• RN given protected time to address concerns raised during briefing and debriefing
• Candid discussion with surgeons about effective strategies for briefing/debriefing
• Ongoing observations of briefing to address defects

% A
gree
“I know the names of the personnel I worked with during my last shift.”
SAQ question And Results:

Roles Assigned for Briefing/Debriefing
• Surgeon initiates dialogue– Introduction all team members– Discussion of dirty/clean instruments
• Nursing takes over– Equipment– Heparin– Steroids– Antibiotics– Etc.

Examples of Defects Addressed by Debriefing
• Surgical scheduler taught to note if “bottom table” is needed during the case
• Pyxis in new clinical building operating rooms stocked with GI peel packs and disposables
• Clarified procedures which should receive chlorhexidine washcloths pre-op
• Developed work flow for inpatients to get appropriate bowel prep and washcloths pre-op
• Surgeon preference cards revised and instrument trays refined– Instruments still on cards from retired and departed surgeons

Revision of Laparoscopic GI Surgery Trays
137 instruments
54 instruments
Outcome:Fewer instruments to count and turnoverSave money and time
Few surgeons knew that the major 1 and 2were opened for lap cases

Collaboration with Infection Control
• OR observations• Noted circulating
nurse left the room between 30 and 50 times during case for equipment not on case carts
• “Stapler Cart”
Lucy Mitchell RN, SCR, Patricia Lawson RN, ICP, Tracie Cometa RN, Steph Mullens CST

Standardization of perioperative steroid use
• Lucy Mitchell RN SCR– Noted 50% SSI rate in patients on steroids
• Pharmacy led audit of perioperative steroid use demonstrated 50-200mg hydrocortisone administered intra-op
Table 4. Mean Postoperative Total Daily Dose
Patient population n (%) Hydrocortisone Equivalents (mg)*
No Steroids Upon Admission (n=16)
Received postoperative steroids 7 (44%) 62
Budesonide (n=10)
Received postoperative steroids 3 (30%) 77
Prednisone (n=24)
Received postoperative steroids 23 (96%) 87
*Calculated based on a dose equivalence of 1:4 (prednisone: hydrocortisone)
Raymon Lamore Pharm D.

Standardized Steroid Intra and Post-op Orders
Roberto Salvatori, MDEndocrinology
• Standardized to 50mg hydrocortisone intra-op (surgeon and anesthesia education, included in briefing)
• POE-based post-op ordersetwith rapid taper

Engaging Other Providers: Peer Outcome Reports
Armstrong Institute for Patient Safety and Quality
33
• Provider specific data compared to peers• All surgeons performing > 10 colorectal procedures per year• Sets the stage that problem is preventable and a social problem
Surgeon ID
ACS NSQIP (defined
variables) 30-Day Mortality
Rate
Superficial Incisional
SSI
Deep Incisional
SSIOrgan/Space
SSIWound
DisruptionPulmonary Embolism
Urinary Tract Infection
Transfusion Intraop/ Postop Sepsis
Septic Shock
1
2
3
Dr. Wick
5
6
7
8
Site Total 9 2.3% 61 15.4% 2 0.5% 21 5.3% 5 1.3% 10 2.5% 20 5.0% 69 17.4% 13 3.3% 9 2.3%
Comparison480 3.3% 1,049 7.2% 206 1.4% 649 4.5% 206 1.4% 130 0.9% 572 3.9% 2,448 16.8% 755 5.2% 384 2.6%
TARGETTED PROCEDURE MODULEColon and Rectal Combined

Barriers and Challenges
• Implementing pre-operative warming– Greater than 100 emails (April 2011 to present)
and still not enough warmers available to warm all patients undergoing colon surgery
• No consistent reporting of process measures (antibiotic compliance, selection, temperature etc)– All available data manually abstracted by medical
student– 5 separate electronic records with different aspect
of perioperative informationArmstrong Institute for Patient Safety and Quality
34

Barriers and Challenges
• Poor moral in operating room (increased workload and opening new clinical building/operating rooms)
• Management resistant to developing team of providers and scheduling designated providers in rooms
• No sustainable plan for maintaining frontline providers protected time after completion of patient safety fellowship
• Lack of pre operative education

Recent Initiatives
• Pre-operative SSI education– Audit of intervention checklist demonstrated poor compliance
with chlorhexidine wash clothes– Applied for grant funding to trial nurse-led pre-operative
education
• Mechanical bowel preparation with oral antibiotics (rapid implementation of new national guidelines)

Johns Hopkins Hospital Motto
Our experience: hospital level interventions(SCIP) pale in comparison to interventions at the work unit level (CUSP)
We embrace local wisdom in the Colorectal OR ‘s
37© JHU and JHHS, 2009

Lessons Learned
• Harm is preventable
• Science of the implementation of quality improvement is under appreciated
CUSP is one tool for implementation
• CUSP sends a clear message, all provider opinions and ideas are important and essential for improvement
• Better teamwork better outcomes better culture and teamwork
• Positive culture empowers frontline staff to take ownership of patient safety and achieve unprecedented improvements