ColoradoCare Amendment 69 Vote YES
24
Vote for A69, ColoradoCare, because: - Businesses will pay 7% of payroll, much less than current aver age of 15%. - Overhead Cost of Insurance Industry reduced from 30% to 10% - 90% of residents will pay less than current system (individual s with 80k or less, families with 180k or less) - Residents will be insured no matter who their employer, or bet ween jobs; businesses no longer fiddle with insurance plans - Patients will not be limited to narrow networks and Providers will be compensated fairly for quality services - Benefits will be comprehensive, 94% actuarial value (eg the Pl atinum Plan, required to get the Waiver) - Improved care with Quality Transparency (required to get the C MS Waiver) - 30-30-30 Solution to the 30-30-30 Problem (Cost, Waste, Best P ractice) - Overall reduction from current 17% of GDP (in Colorado) to 15% of GDP or less (vs 19% of GDP nationally) - Waiver Oversight guarantees valid pro forma and full fed fundi ng, with incentives for improving Colorado's Health Equity Ind ex Read article For further discussion or to arrange a group presentation, contact: George Swan, MPH 303-406-8009 gswan@ emPoweredDecisions.us
-
Upload
jhealth-unlimited -
Category
Healthcare
-
view
31 -
download
0
Transcript of ColoradoCare Amendment 69 Vote YES

Vote for A69, ColoradoCare, because:- Businesses will pay 7% of payroll, much less than current average of 15%.- Overhead Cost of Insurance Industry reduced from 30% to 10%- 90% of residents will pay less than current system (individuals with 80k or less, families with
180k or less)- Residents will be insured no matter who their employer, or between jobs; businesses no lon
ger fiddle with insurance plans - Patients will not be limited to narrow networks and Providers will be compensated fairly for
quality services- Benefits will be comprehensive, 94% actuarial value (eg the Platinum Plan, required to get th
e Waiver)- Improved care with Quality Transparency (required to get the CMS Waiver)- 30-30-30 Solution to the 30-30-30 Problem (Cost, Waste, Best Practice)- Overall reduction from current 17% of GDP (in Colorado) to 15% of GDP or less (vs 19% of G
DP nationally)- Waiver Oversight guarantees valid pro forma and full fed funding, with incentives for improvi
ng Colorado's Health Equity Index
Read article
For further discussion or to arrange a group presentation, contact:
George Swan, [email protected]

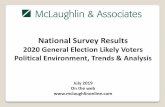
National Health Expenditures = $4,020B: 19.1% GDP, $12,113 per Capita
Amendment 69* = $50.3B: 14.7% GDP, $9,142 per Capita
Colorado State Health Expense = $60.1B: 17.0% GDP, $10,558 per Capita
30 – 30 – 30 Problem: Current System, ObamaCare- 30% Administrative Overhead due to Complex Insurance
and Complex Billing.- 30% Fraud, Waste, Inappropriate, Contra-indicated and
Harmful healthcare delivery.- 30% Shortfall of Appropriate and Necessary Healthcare as
indicated by Best Practice Guidelines.
30 – 30 – 30 Promise: Amendment 69, ColoradoCare- 10% Administrative Overhead – Single Payer Model- 10% Fraud, Waste and Inappropriate Care achievable
from data availability, transparency and accountability- 10% Shortfall of Appropriate Healthcare, according to
Best Practice Guidelines, due to integrated healthcare system, communication and accountability.
30% Admin Expense Overhead
30% Shortfall of Appropriate and Medically Indicated Care
30% Expense due to Waste, Fraud and InappropriateCare
Economic Analysis of ColoradoCareUpdate 2015.03, by Ivan Miller
30 – 30 – 30 Analysis by George Swan, MPH
“Independent Financial Analysis”by Colorado Health Institute (CHI)
Effective Year, 2019
International Comparisons of Admin Cost in Healthcare, 2012Health Affairs: Reducing Waste in Healthcare, 2011Health Affairs: Reducing Shortfall in Healthcare, 2009 Health Affairs: Patients with Problems in Six Countries, 2005
19%
17%
15%
Vote “Yes” on Amendment 69!

Forbes: Greatest Heist in American Healthcare by Dave Chase
Current System (ACA, ObamaCare)vs ColoradoCare: Frequently Asked Questions
For further discussion or to arrange a group presentation, contact:
George Swan, [email protected]
Triple Aim:-Lower Cost per Capita-Better Personal Care-Community Health

Economic Analysis of Healthcare – Colorado- Voters will have three choices in November:
HillaryCare (continuation of ACA), TrumpCare (repeal of ACA) or ColoradoCare (Amendment69)
- Before any analysis can begin, what is the foundational situation, the key data, as a baseline?
- What are the NHE (National Health Expenditures) and CHE (Colorado - State Health Expenditures) data, historical and projected?
- Valid Source of Data should be at CDPHE!- What factors are important determinants of
NHE/CHE going forward? Payer Mix?- What are the key assumptions that will affect the
NHE/CHE going forward?- Population growth- Benefits Package (Platinum for All)- Utilization of Services (fraud/waste/evidence)- Pricing of Services (negotiation of rates)- Deductibles, Co-pays and Co-Insurance (OOP)- Administrative Overhead (Payers & Providers)- Algorithms/Paradigms for Services (Quality)- Capacity and Productivity of Providers- Health and Demand for Services by Patients
Economic Analysis of ColoradoCareUpdate 2015.03, by Ivan Miller
“Independent Financial Analysis”by Colorado Health Institute (CHI)
ColoradoCare: Frequently Asked Questions


National Health Expenditures = $4,020B: 19.1% GDP, $12,113 per Capita
Amendment 69* = $50.3B: 14.7% GDP, $9,142 per Capita
Colorado State Health Expense = $60.1B: 17.0% GDP, $10,558 per Capita
30 – 30 – 30 Problem: Current System, ObamaCare- 30% Administrative Overhead due to Complex Insurance
and Complex Billing.- 30% Fraud, Waste, Inappropriate, Contra-indicated and
Harmful healthcare delivery.- 30% Shortfall of Appropriate and Necessary Healthcare as
indicated by Best Practice Guidelines.
30 – 30 – 30 Promise: Amendment 69, ColoradoCare- 10% Administrative Overhead – Single Payer Model- 10% Fraud, Waste and Inappropriate Care achievable
from data availability, transparency and accountability- 10% Shortfall of Appropriate Healthcare, according to
Best Practice Guidelines, due to integrated healthcare system, communication and accountability.
30% Admin Expense Overhead
30% Shortfall of Appropriate and Medically Indicated Care
30% Expense due to Waste, Fraud and InappropriateCare
Economic Analysis of ColoradoCareUpdate 2015.03, by Ivan Miller
30 – 30 – 30 Analysis by George Swan, MPH
“Independent Financial Analysis”by Colorado Health Institute (CHI)
Effective Year, 2019
International Comparisons of Admin Cost in Healthcare, 2012Health Affairs: Reducing Waste in Healthcare, 2011Health Affairs: Reducing Shortfall in Healthcare, 2009 Health Affairs: Patients with Problems in Six Countries, 2005
19%
17%
15%
Vote “Yes” on Amendment 69!

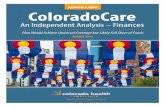
Total 35%
Harvard Business Review

Individuals Businesses
State-wide Health Services Trust
Governing Board:A Trust Fund administered by the Board of Trustees – with regional representation of consumers and providers
Private Providers
Colorado Regional Healthcare Information Organization (CoRHIO)
Trust Fund
Single Payer Database
ClaimsPayments
Fed/State Financing
Single PayerUniversal CoverageInformed ChoicesPrivate PracticeQuality Data TransparencyComprehensive BenefitsIncreased EfficiencyQuality Healthcare DeliveryInsurance Disconnected from Employment
Tax
3PMP*
3PMP = 3rd Party, Multi-Payer Health Insurance
Dept of RevenueTripleAim
“It’s easier done than said.”
LegislativeOversight
CMS Waiver
Oversight

Atul Gawande: Overkill(New Yorker, 2015)
Vote “Yes” on Amendment 69!
Current System (ObamaCare)is not working.
ColoradoCare: Frequently Asked Questions
Triple Aim:- Lower Cost- Better Care- Community Health

Gallup Surveys: Healthcare Satisfaction, Well-Being, Happiness

Context for Colorado Care (Amendment 69):
- Valid Source of Data- Health Expenditures- Pivot Table Link - NHE- Pivot Table Data Sets- Context of ACA- Context of Insured- Key Ratios:
- % of GSP- Per Capita- Income Level- OOP- Insurance
- Timely Updates- Authority, Reliability- Accountability
- Same Assumptions- Triple Aim Objectives- Winners and Losers- Pros and Cons- Critical Success Factors

National and State-level Health Expenditures:- Single, authoritative “Valid Source of Data”- Pivot Table Links and Holarchy of Pivot Tables (Categories/Levels)
ColoradoCare: Frequently Asked Questions

Simply put, CHI’s analysis is invalid. Amendment 69 is null and void if the required actuarial analysis is not viable; for example, if full federal funding or state funding is not agreed. In that case, CHI analysis is irrelevant.
More importantly, CHI should provide a “best-case scenario” of ColoradoCare, assuming that the trustees selected and local community leaders can better work with healthcare providers to over-come the “30-30-30 problem” of the current system, as highlighted for the 208 Commission:- 30% cost overhead, from insurance administration complexities and requirements;- 30% cost of unnecessary, contra-indicated or inappropriate healthcare services, or fraud; and- 30% cost of failing to provide medically appropriate care to patients, according to best-practice guidelines.It should be made clear, if CHI is truly independent in their analysis, that the major benefits of ColoradoCare, compared to the current healthcare system (Obamacare), will include the following:- Healthcare costs significantly less than the 18-19% of GDP cost of the current system, as predicted by Lewin
Group time and time again, which the required actuarial analysis will show.- Employers freed from managing health care insurance for their employees, and employees are released from
their “golden handcuffs”. Employers will be able to focus on their business success and employees can work without any concern for their healthcare insurance benefits, even between jobs or working at home.
- Everyone covered, no one left out. The industry associated with insurance, under-insured or non-insured virtually disappears. All the means testing and disparity analysis for the uninsured will vanish. The conversation will shift to “value-based healthcare” and metrics associated with Triple Aim (eg total population health and well-being, quality healthcare services and affordable health services for everyone.
- Pricing of healthcare services will be transparent and providers will be incentivized by various payment agreements to work together, with community stakeholders, to facilitate value-for-money.
- Quality measures will be transparent and timely, for clinically-appropriate services and outcomes, according to best-practice guidelines.
- Community leaders and stakeholders will monitor, and be accountable for, community health and well-being through the full life course, from pre-natal to death, from “womb to tomb”.
Triple Aim:- Lower Cost- Better Care- Community Health

Colorado Health Institute “Three Minute Expert”
Additional Questions:- If providers do not accept a negotiated payment for services, can they see patients anyway?- What actions/policies are needed to ensure capacity and quality of healthcare providers?- How will payments be determined, knowing that cost of resources and services have nuances?- What is the meaning of “value-based payments” or “bundled payments”? Relate to billing.- How will ColoradoCare integrate Kaiser (HMO model) or Medicare Advantage beneficiaries?
“Safeguards to ensure effective implementation?”“Safeguards to ensure effective Board members?”
ColoradoCare: Frequently Asked Questions

Commonwealth Fund: The Healthcare Affordability Index“…40% of adults with high deductibles reported not getting needed care because of their deductible…”

Additional Questions:- How do Colorado residents access out of state providers? Emergencies and Specialties?- Can hospitals/physicians/healthcare providers care for non-state visitors/patients? Charges?- How do healthcare providers bill for non-ColoradoCare patients?- How are healthcare provider charges negotiated?- What if there are insufficient providers to obtain timely appointments? Or lacking rural services?- Does Dept of Regulatory Affairs (DORA) still oversee/monitor/require adherence to standards?
ColoradoCare: Frequently Asked Questions

ColoradoCareYes: Individual Calculator

Calculate Current vs ColoradoCare
- When Premium Tax is a credit/exemption for individuals as well as businesses?- Health status of employees and/or family members no longer an issue to hiring?- Freedom of employees to seek best opportunities, insurance benefits no longer an issue.- How does ColoradoCare reconcile high-hazard occupations and business risks?

Medicare (65yo and over):- 10% of net income,
after exemptions.- Replaces Supplement
(Avg $4,046 value)- Eliminates deductibles
and majority of OOP- Insurance against
$300,000 Medicare risk
, 2010ColoradoCare:Frequently Asked Questions

Cost of Healthcare per Employee (Aon Hewitt)ACA (Current System), 2016 = Premium + OOP = $11,484 + $2,433 = $13,917Vs (10% of $139,170)ColoradoCare (Amendment 69) = 10% of Income (20% of $69,985)
* Does not include employer cost of administration

Question: What is the current percentage of income paid by Colorado residents ….. compared to 10% of income for ColoradoCare, Platinum Plan for ALL?

David Chase, Forbes: The Healthcare Mess
David Chase, Forbes:65X Larger Healthcare Cost
ColoradoCare is Alexander’s Sword over the Gordian Knot!
19%
17%
15%
Slides
ColoradoCare: Frequently Asked QuestionsTriple Aim:- Lower Cost- Better Care- Community Health

emPowered Decisions
ColoradoCare?
Insurance Profits
30 – 30 – 30 Problem
Current Healthcare System
Vote “Yes” on Amendment 69!
For further discussion or to arrange a group presentation, contact: 303-406-8009
George Swan, [email protected]

National Health Expenditures = $4,020B: 19.1% GDP, $12,113 per Capita
Amendment 69* = $50.3B: 14.7% GDP, $9,142 per Capita
Colorado State Health Expense = $60.1B: 17.0% GDP, $10,558 per Capita
30 – 30 – 30 Problem: Current System, ObamaCare- 30% Administrative Overhead due to Complex Insurance
and Complex Billing.- 30% Fraud, Waste, Inappropriate, Contra-indicated and
Harmful healthcare delivery.- 30% Shortfall of Appropriate and Necessary Healthcare as
indicated by Best Practice Guidelines.
30 – 30 – 30 Promise: Amendment 69, ColoradoCare- 10% Administrative Overhead – Single Payer Model- 10% Fraud, Waste and Inappropriate Care achievable
from data availability, transparency and accountability- 10% Shortfall of Appropriate Healthcare, according to
Best Practice Guidelines, due to integrated healthcare system, communication and accountability.
30% Admin Expense Overhead
30% Shortfall of Appropriate and Medically Indicated Care
30% Expense due to Waste, Fraud and InappropriateCare
Economic Analysis of ColoradoCareUpdate 2015.03, by Ivan Miller
30 – 30 – 30 Analysis by George Swan, MPH
“Independent Financial Analysis”by Colorado Health Institute (CHI)
Effective Year, 2019
International Comparisons of Admin Cost in Healthcare, 2012Health Affairs: Reducing Waste in Healthcare, 2011Health Affairs: Reducing Shortfall in Healthcare, 2009 Health Affairs: Patients with Problems in Six Countries, 2005
19%
17%
15%
Vote “Yes” on Amendment 69!