
Colorado Review of Anesthesia for SurgiCenters and ... · Tetralogy of Fallot Tricuspid atresia...
6
Anesthetic considerations in Adults with Congenital Heart Disease Dr. Mark Twite MA MB BChir FRCP Director of Congenital Cardiac Anesthesiology Associate Professor Department of Anesthesiology University of Colorado, Anschutz Medical Campus & Children’s Hospital Colorado CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals and Ski Holiday! No Financial Disclosures CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals Page 2 xxx00.#####.ppt 2/9/2018 10:23:41 AM Page 2 Ameristar Casino, Blackhawk, CO Page 3 xxx00.#####.ppt 2/9/2018 10:23:41 AM Page 3 Objectives Understand and Discuss the: 1. Changing epidemiology of congenital heart disease (CHD) 2. Current outcomes for patients with CHD 3. Perioperative anesthetic approach to adults with CHD undergoing non- cardiac surgery Page 4 xxx00.#####.ppt 2/9/2018 10:23:41 AM Page 4 • 37yr old female in Atrial Flutter presents for TEE, EP study and ablation • Tricuspid Atresia s/p Fontan ‐ Non-alcoholic cirrhosis (elevated LFTs and low albumin) ‐ Protein losing enteropathy ‐ Hypoxia. Baseline Sats 75-85% in air. Polycythemia Hct 65 ‐ Pacemaker Dual Chamber DDD at 70bpm • Medications ‐ Apixaban, Aspirin ‐ L-Arginine ‐ Digoxin, Quinapril, Sotalol ‐ Furosemide, Spironolactone ‐ Melatonin, Valium, Ambien, Tramadol Case Page 5 xxx00.#####.ppt 2/9/2018 10:23:41 AM Page 5 • 37yr old female in Atrial Flutter presents for TEE, EP study and ablation • Echocardiogram 9/2016 TTE 1. History of Tricuspid atresia, status post initial class (RA to PA)Fontan, with subsequent Fontan conversion to intra-cardiac lateral tunnel Fontan through the RA body 2. Subjectively there remains normal LV systolic function. 3. Dilated IVC without respiratory collapse. Low velocity flow within IVC suggests IVC pressure is greater than 15 mm Hg . 4. The Glenn anastomosis is not well visualized, though there is normal respiratory variation in SVC flow suggestive of no obstruction within the Fontan pathway. 5. Trivial mitral regurgitation, mild mitral stenosis (mean gradient 5.6 mmHg). 6. Mildly dilated left ventricle with subjectively normal function. Hypoplastic right ventricle is not well seen. 7. No pericardial effusion. Case Mark Twite, MB Anesthetic Considerations in Adults with Congenital Heart Disease
Transcript of Colorado Review of Anesthesia for SurgiCenters and ... · Tetralogy of Fallot Tricuspid atresia...

Anesthetic considerations in Adults with Congenital Heart Disease
Dr. Mark Twite MA MB BChir FRCP
Director of Congenital Cardiac Anesthesiology
Associate Professor
Department of Anesthesiology
University of Colorado, Anschutz Medical Campus &
Children’s Hospital Colorado
CRASH Vail, Colorado 2018
Colorado Review of Anesthesia for SurgiCenters and Hospitalsand Ski Holiday!
No Financial Disclosures
CRASH Vail, Colorado 2018
Colorado Review of Anesthesia for SurgiCenters and Hospitals
Page 2
xxx00.#####.ppt 2/9/2018 10:23:41 AMPage 2
Ameristar Casino, Blackhawk, CO
Page 3
xxx00.#####.ppt 2/9/2018 10:23:41 AMPage 3
Objectives
Understand and Discuss the:
1. Changing epidemiology of congenital heart disease (CHD)
2. Current outcomes for patients with CHD
3. Perioperative anesthetic approach to adults with CHD undergoing non-cardiac surgery
Page 4
xxx00.#####.ppt 2/9/2018 10:23:41 AMPage 4
• 37yr old female in Atrial Flutter presents for TEE, EP study and ablation
• Tricuspid Atresia s/p Fontan
‐ Non-alcoholic cirrhosis (elevated LFTs and low albumin)
‐ Protein losing enteropathy
‐ Hypoxia. Baseline Sats 75-85% in air. Polycythemia Hct 65
‐ Pacemaker Dual Chamber DDD at 70bpm
• Medications
‐Apixaban, Aspirin
‐L-Arginine
‐Digoxin, Quinapril, Sotalol
‐Furosemide, Spironolactone
‐Melatonin, Valium, Ambien, Tramadol
Case
Page 5
xxx00.#####.ppt 2/9/2018 10:23:41 AMPage 5
• 37yr old female in Atrial Flutter presents for TEE, EP study and ablation
• Echocardiogram 9/2016 TTE
1. History of Tricuspid atresia, status post initial class (RA to PA)Fontan, with subsequent Fontan conversion to intra-cardiac lateral tunnel Fontan through the RA body
2. Subjectively there remains normal LV systolic function.
3. Dilated IVC without respiratory collapse. Low velocity flow within IVC suggests IVC pressure is greater than 15 mm Hg .
4. The Glenn anastomosis is not well visualized, though there is normal respiratory variation in SVC flow suggestive of no obstruction within the Fontan pathway.
5. Trivial mitral regurgitation, mild mitral stenosis (mean gradient 5.6 mmHg).
6. Mildly dilated left ventricle with subjectively normal function. Hypoplastic right ventricle is not well seen.
7. No pericardial effusion.
Case
Mark Twite, MB Anesthetic Considerations in Adults with Congenital Heart Disease
Page 6
xxx00.#####.ppt 2/9/2018 10:23:41 AMPage 6
• 37yr old female in Atrial Flutter presents for TEE, EP study and ablation
• Cardiac Cath
CATH (Denver, 2010) no fenestration, unobstructed PA's, Fontan 11-12 mmHg, no change with volume challenge, small angiographic right to left shunt seen likely from the suture line of the lateral tunnel.
CATH (Denver, 2013) Fontan pressures 18 mmHg, PCWP 14 mmHg, small veno-venous collaterals off left innominate embolized, 100% FiO2 and improved Fontan pressure to 11 mmHg
CATH (Denver, 2016) hepatic wedge 19 mmHg, hepatic vein 15 mmHg (transhepaticgradient 4 mmHg), Fontan 13, RPA 11, LPA 12, PCWP 9. Fick CO 5.06. S/P 10ml/kg bolus PA increased to 17, PCWP to 14, Fick CO 5.74. With 100% O2, PA pressure decreased to 13, PCWP to 12, Fick CO 5.69, with 40 ppm iNO PA pressure 14 , PCWP 13, CO 5.64
Case
Page 7
xxx00.#####.ppt 2/9/2018 10:23:41 AMPage 7
?
Page 8
xxx00.#####.ppt 2/9/2018 10:23:41 AMPage 8
• Most common congenital disorder of newborns‐ 1% of live births‐ Leading cause of infant deaths in the USA‐ Accounts for more than half of all deaths from congenital anomalies worldwide
• Estimated 1.5 million adults living in USA with CHD
• NIH funded CHD research from 2005 – 2015‐ 663 CHD research projects for a total cost of $991 million
• 70% Basic science (Cardiac developmental biology most common)• 27% Clinical• 3% Both
Congenital Heart Disease
Van der Bom Nat Rev Cardiol 2011Burns Pediatr Cardiol 2017
Page 9
xxx00.#####.ppt 2/9/2018 10:23:41 AMPage 9
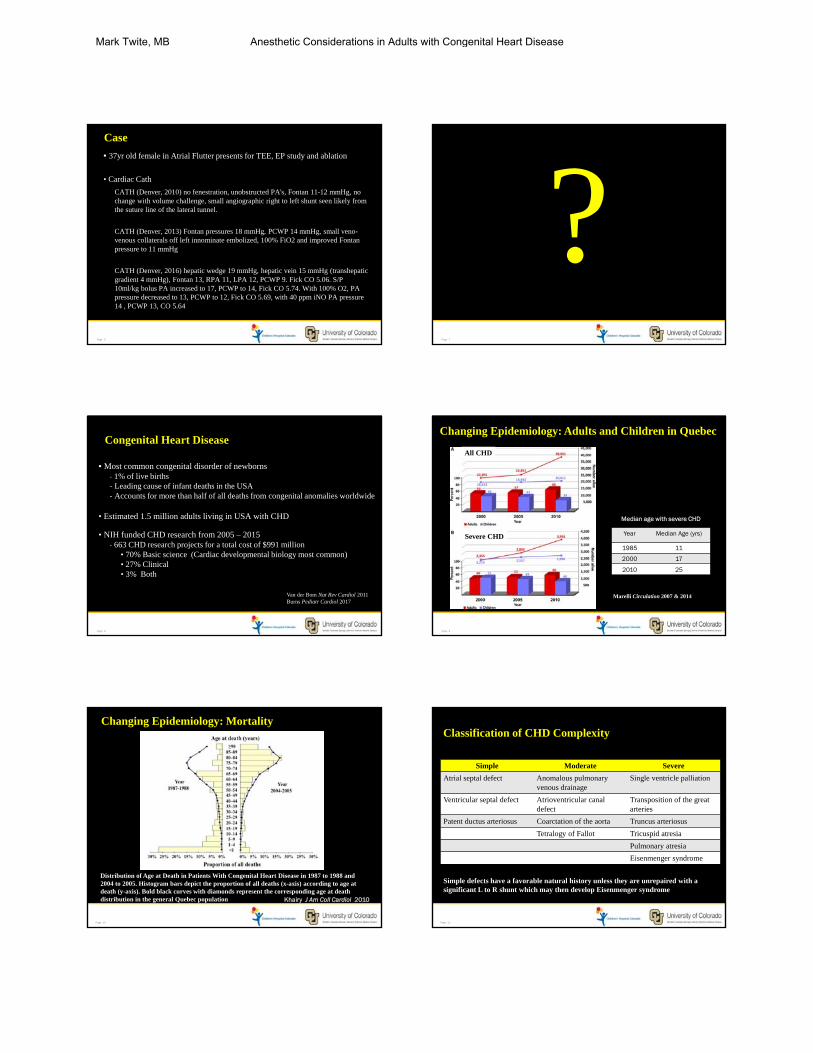
Changing Epidemiology: Adults and Children in Quebec
Marelli Circulation 2007 & 2014
Median age with severe CHD
Year Median Age (yrs)
1985 11
2000 17
2010 25
All CHD
Severe CHD
Page 10
xxx00.#####.ppt 2/9/2018 10:23:41 AMPage 10
Changing Epidemiology: Mortality
Distribution of Age at Death in Patients With Congenital Heart Disease in 1987 to 1988 and 2004 to 2005. Histogram bars depict the proportion of all deaths (x-axis) according to age at death (y-axis). Bold black curves with diamonds represent the corresponding age at death distribution in the general Quebec population Khairy J Am Coll Cardiol 2010
Page 11
xxx00.#####.ppt 2/9/2018 10:23:41 AMPage 11
Classification of CHD Complexity
Simple Moderate Severe
Atrial septal defect Anomalous pulmonary venous drainage
Single ventricle palliation
Ventricular septal defect Atrioventricular canal defect
Transposition of the great arteries
Patent ductus arteriosus Coarctation of the aorta Truncus arteriosus
Tetralogy of Fallot Tricuspid atresia
Pulmonary atresia
Eisenmenger syndrome
Simple defects have a favorable natural history unless they are unrepaired with a significant L to R shunt which may then develop Eisenmenger syndrome
Mark Twite, MB Anesthetic Considerations in Adults with Congenital Heart Disease
Page 12
xxx00.#####.ppt 2/9/2018 10:23:42 AMPage 12
Long term Survival by complexity of CHD
95% 90% 80%
Simple Moderate Severe
Atrial septal defect Anomalous pulmonary venous drainage
Single ventricle palliation
Ventricular septal defect Atrioventricular canal defect
Transposition of the great arteries
Patent ductus arteriosus Coarctation of the aorta Truncus arteriosus
Tetralogy of Fallot Tricuspid atresia
Pulmonary atresia
Eisenmenger syndrome
Long term survival > 20 years Warnes J Am Coll Cardiol 2008
Page 13
xxx00.#####.ppt 2/9/2018 10:23:42 AMPage 13
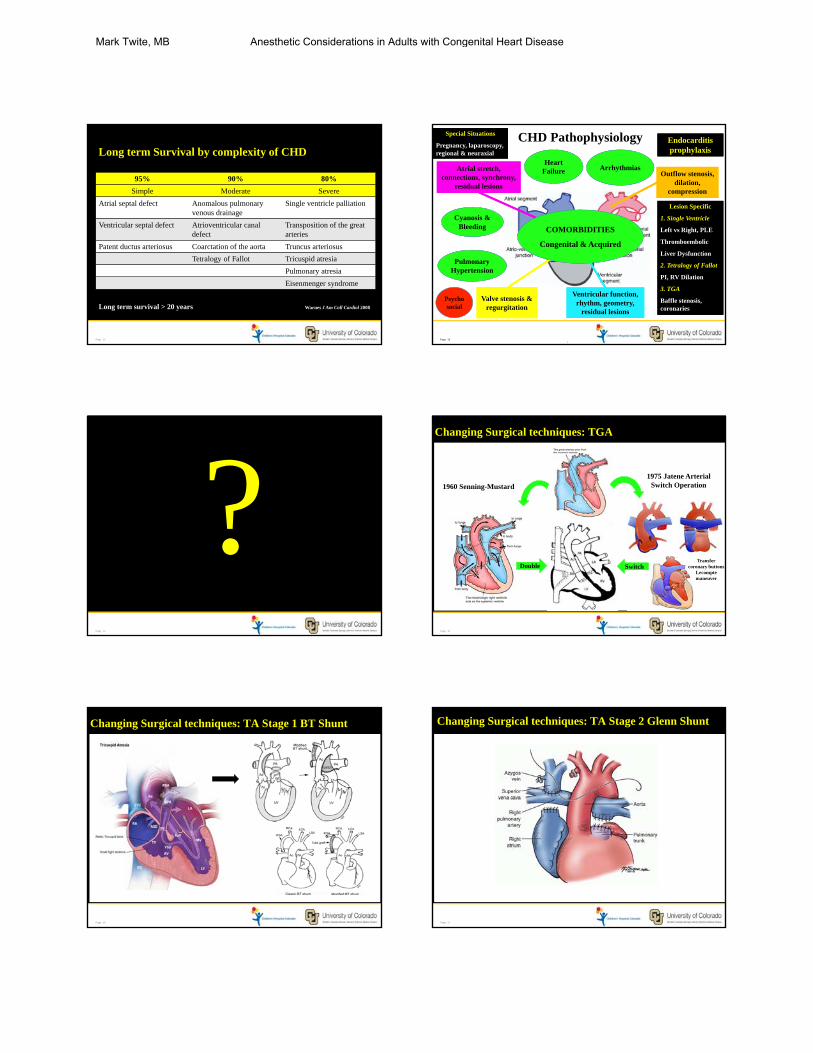
CHD Pathophysiology
Valve stenosis & regurgitation
Atrial stretch, connections, synchrony,
residual lesions
Outflow stenosis, dilation,
compression
Ventricular function, rhythm, geometry,
residual lesions
Heart Failure Arrhythmias
Pulmonary Hypertension
Cyanosis & Bleeding COMORBIDITIES
Congenital & Acquired
Lesion Specific
1. Single Ventricle
Left vs Right, PLE
Thromboembolic
Liver Dysfunction
2. Tetralogy of Fallot
PI, RV Dilation
3. TGA
Baffle stenosis, coronaries
Lesion Specific
1. Single Ventricle
Left vs Right, PLE
Thromboembolic
Liver Dysfunction
2. Tetralogy of Fallot
PI, RV Dilation
3. TGA
Baffle stenosis, coronaries
Special Situations
Pregnancy, laparoscopy, regional & neuraxial
Special Situations
Pregnancy, laparoscopy, regional & neuraxial
Endocarditis prophylaxisEndocarditis prophylaxis
Psychosocial
Page 14
xxx00.#####.ppt 2/9/2018 10:23:42 AMPage 14
?Page 15
xxx00.#####.ppt 2/9/2018 10:23:42 AMPage 15
Changing Surgical techniques: TGA
1975 Jatene Arterial Switch Operation
DoubleDouble SwitchSwitchTransfer
coronary buttonsLecomptemaneuver
1960 Senning-Mustard
Page 16
xxx00.#####.ppt 2/9/2018 10:23:44 AMPage 16
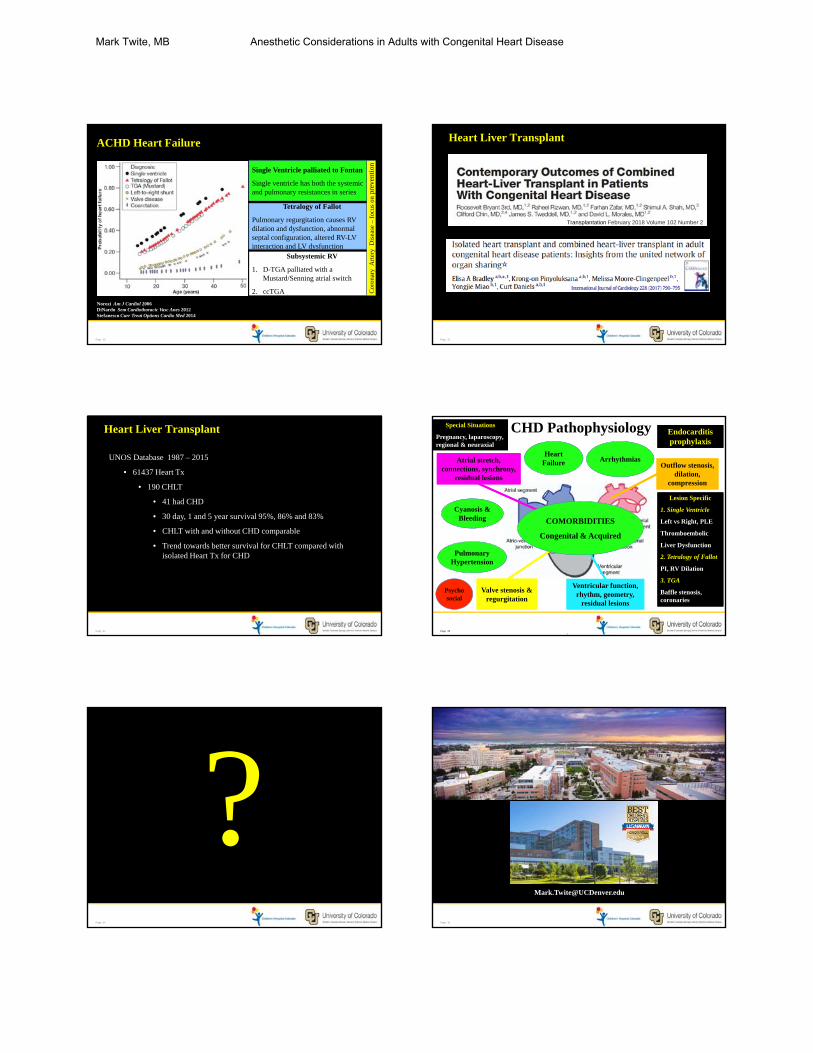
Changing Surgical techniques: TA Stage 1 BT Shunt
Page 17
xxx00.#####.ppt 2/9/2018 10:23:44 AMPage 17
Changing Surgical techniques: TA Stage 2 Glenn Shunt
Mark Twite, MB Anesthetic Considerations in Adults with Congenital Heart Disease

Page 18
xxx00.#####.ppt 2/9/2018 10:23:44 AMPage 18
Changing Surgical techniques: TA Stage 3 Fontan
AtrioPulmonary Lateral Tunnel Extracardiac
Page 19
xxx00.#####.ppt 2/9/2018 10:23:44 AMPage 19
Effects of anesthetic agents
aKetamine can depress contractility in vitro and in catecholamine depleted patients.
bDexmedetomidinecan increase MAP during loading dose administration.
Friesen SCVA 2017
Page 20
xxx00.#####.ppt 2/9/2018 10:23:44 AMPage 20
Consensus Statements
Circulation, October 2017
Circulation, January 2017
Page 21
xxx00.#####.ppt 2/9/2018 10:23:44 AMPage 21
Time-series analysis: referral to specialized ACHD
centers and ACHD patient mortality
Mylotte Circulation 2014
Page 22
xxx00.#####.ppt 2/9/2018 10:23:45 AMPage 22
Studied 482 adults with CHD from 12 centers in the USA• Most common presenting arrhythmia:
‐ Intra-atrial re-entrant tachycardia (IART) 61.6% (increased with CHD complexity)‐ Atrial fibrillation (AF) 28.8% increased with age to surpass IART at 50yrs of age‐ Focal atrial tachycardia 9.5%
Atrial Arrhythmias
Page 23
xxx00.#####.ppt 2/9/2018 10:23:45 AMPage 23
Risk factors for developing atrial arrhythmias: ‐ single ventricle‐ previous intracardiac repair‐ systemic right ventricle‐ pulmonary hypertension
Mark Twite, MB Anesthetic Considerations in Adults with Congenital Heart Disease

Page 24
xxx00.#####.ppt 2/9/2018 10:23:45 AMPage 24
Adults with CHD and atrial arrhythmias:• x 4 increase of heart failure• x 2 increase in death
Page 25
xxx00.#####.ppt 2/9/2018 10:23:45 AMPage 25
Atrial arrhythmias frequent cause of sudden cardiac death (43%)Increasing incidence with complexity of CHD
‐ Eisenmenger‐ Transposition of great arteries (atrial switch)‐ Single ventricles lesions palliated to Fontan circulation
Page 26
xxx00.#####.ppt 2/9/2018 10:23:45 AMPage 26
Single Center study in USA of Fontan patients• 10, 20 and 30 year freedom from arrhythmias of 71%, 42% and 24%• SCD 52 of 1052 Fontan patients (5%) with 65% due to arrhythmias
Congenital Heart Disease 2017 (12) 17‐23
Page 27
xxx00.#####.ppt 2/9/2018 10:23:45 AMPage 27
Factors leading to arrhythmias in CHD
Escudero Can J Cardiol 2013
Page 28
xxx00.#####.ppt 2/9/2018 10:23:45 AMPage 28
Risk estimates for arrhythmias across CHD
PACES / HRS Expert Consensus Statement on the Recognition and Management of Arrhythmias in ACHD Heart Rhythm 2014
Sim
ple
Mod
erat
eS
ever
e
Page 29
xxx00.#####.ppt 2/9/2018 10:23:45 AMPage 29
Majority of SCD victims unrecognized with an area under the curve of 0.6 for the discriminative ability of current guidelines Critical clinical reasoning essential when deciding on ICD placement in adult CHD patients
Implantable Cardioverter-Defibrillator
Mark Twite, MB Anesthetic Considerations in Adults with Congenital Heart Disease
Page 30
xxx00.#####.ppt 2/9/2018 10:23:46 AMPage 30
ACHD Heart Failure
Norozi Am J Cardiol 2006DiNardo Sem Cardiothoracic Vasc Anes 2012Stefanescu Curr Treat Options Cardio Med 2014
Single Ventricle palliated to Fontan
Single ventricle has both the systemic and pulmonary resistances in series
y
Tetralogy of Fallot
Pulmonary regurgitation causes RV dilation and dysfunction, abnormal septal configuration, altered RV-LV interaction and LV dysfunction
Subsystemic RV
1. D-TGA palliated with a Mustard/Senning atrial switch
2. ccTGA Cor
onar
y A
rter
y D
isea
se –
focu
s on
prev
enti
on
Page 31
xxx00.#####.ppt 2/9/2018 10:23:46 AMPage 31
Heart Liver Transplant
Transplantation February 2018 Volume 102 Number 2
Page 32
xxx00.#####.ppt 2/9/2018 10:23:46 AMPage 32
Heart Liver Transplant
UNOS Database 1987 – 2015
• 61437 Heart Tx
• 190 CHLT
• 41 had CHD
• 30 day, 1 and 5 year survival 95%, 86% and 83%
• CHLT with and without CHD comparable
• Trend towards better survival for CHLT compared with isolated Heart Tx for CHD
Page 33
xxx00.#####.ppt 2/9/2018 10:23:46 AMPage 33
CHD Pathophysiology
Valve stenosis & regurgitation
Atrial stretch, connections, synchrony,
residual lesions
Outflow stenosis, dilation,
compression
Ventricular function, rhythm, geometry,
residual lesions
Heart Failure Arrhythmias
Pulmonary Hypertension
Cyanosis & Bleeding COMORBIDITIES
Congenital & Acquired
Lesion Specific
1. Single Ventricle
Left vs Right, PLE
Thromboembolic
Liver Dysfunction
2. Tetralogy of Fallot
PI, RV Dilation
3. TGA
Baffle stenosis, coronaries
Lesion Specific
1. Single Ventricle
Left vs Right, PLE
Thromboembolic
Liver Dysfunction
2. Tetralogy of Fallot
PI, RV Dilation
3. TGA
Baffle stenosis, coronaries
Special Situations
Pregnancy, laparoscopy, regional & neuraxial
Special Situations
Pregnancy, laparoscopy, regional & neuraxial
Endocarditis prophylaxisEndocarditis prophylaxis
Psychosocial
Page 34
xxx00.#####.ppt 2/9/2018 10:23:46 AMPage 34
?Page 35
xxx00.#####.ppt 2/9/2018 10:23:46 AMPage 35
Thank you
Mark Twite, MB Anesthetic Considerations in Adults with Congenital Heart Disease


















