
Colonoscopy screening in the elderly: when to stop?
5
Colonoscopy Screening in the Elderly: When to Stop? Tyler Stevens, M.D., and Carol A. Burke, M.D. Department of Gastroenterology and Hepatology, Cleveland Clinic Foundation, Cleveland, Ohio OBJECTIVES: The age to begin colorectal cancer (CRC) screening is based on the risk of neoplasia and is published in screening guidelines. The age to stop screening is un- known but should be based, in part, on the same principle. The purpose of this study was to establish whether the prevalence of neoplasia detected by colonoscopy dimin- ished with advancing age, to warrant ceasing colonoscopic screening. METHODS: The endoscopic and pathology reports of all asymptomatic subjects undergoing colonoscopy for the pur- pose of CRC screening or an evaluation of abdominal pain or change in bowel habits between 1997 and 2000 were reviewed. A multivariate logistic regression analysis was used to assess the effect of age, gender, and indication for examination on the prevalence of neoplasia, as well as on having more than two adenomas, advanced adenomas (tu- bulovillous, villous, severe dysplasia, or size 1 cm), and invasive cancers. RESULTS: A total of 915 patients were included. Of these, 50% were male, with a mean age of 65 yr (range 50 –100). Neoplasia peaked in the seventh decade, with a fall there- after (p 0.009). Numerous adenomas, advanced adeno- mas, and invasive cancers increased with age. The yield for overall neoplasia, advanced adenomas, and more than two adenomas was higher in the screening group than in the symptomatic group. More invasive cancers were found in the symptomatic group compared with the asymptomatic group, but this did not achieve statistical significance (4 vs 1, p 0.44). CONCLUSIONS: The prevalence of advanced neoplasia con- tinues to increase with age. Subjects undergoing colonos- copy for screening had a greater risk for neoplasia than did subjects with symptoms. There is no decline in yield of advanced neoplasia to justify stopping screening colonos- copy in the elderly. (Am J Gastroenterol 2003;98: 1881–1885. © 2003 by Am. Coll. of Gastroenterology) INTRODUCTION Colonoscopy is gaining acceptance as the preferred strategy for colorectal cancer (CRC) screening. It has the greatest sensitivity and specificity for the detection of neoplasia compared with other modalities (1, 2). Evidence for its effectiveness comes from cohort studies, which show a de- crease in the incidence and mortality of CRC in subjects who have had adenomas removed (3–7). Colonoscopy has been found to be comparable in cost-effectiveness to other methods of screening (8 –10). Multiple guidelines include colonoscopy as an option for screening average risk patients (11, 12). Screening is initiated at age 50 yr because the incidence of CRC rises precipitously after age 50 yr, from 26 cases per 100,000 at age 45– 49 yr to 49 cases at age 50 –54 yr and 85 cases at age 55–59 yr (13). Additionally, CRC is uncommon in asymptomatic persons 40 – 49 yr old, and advanced neo- plasia have been reported in less than 3.5% (14). In contrast to recommendations of the age to begin screening, no guidelines exist regarding the age to stop screening. Part of such a decision depends on the clinical judgment of the physician, desires of the patient, presence of other life-limiting comorbidities, projected lifespan, and the length of protective benefit from screening. The decision should also be based on evidence of the prevalence of colorectal neoplasia with advancing age. A recent study of screening flexible sigmoidoscopy found the risk of distal neoplasia to significantly decrease from 19% at age 65–69 yr to 14% at age 70 yr and suggested stopping colorectal cancer screening after age 70 yr (15). Establishing the prevalence of neoplasia in elderly pa- tients undergoing colonoscopy would be helpful in guiding physicians and counseling patients as to the risk of neoplasia and potential benefit of colonoscopy. The purpose of our study was to assess the effect of age on the prevalence of neoplasia detected by colonoscopy. In doing this, we hoped to determine whether there is an age at which the prevalence of advanced neoplasia is low enough to cease screening. We also sought to determine whether gender or indication for examination had an effect on the prevalence of neoplasia. MATERIALS AND METHODS The endoscopy reports of all colonoscopies performed in the Department of Gastroenterology and Hepatology at the Presented at the American College of Gastroenterology Annual Meeting October 21–24, 2001, Las Vegas, Nevada. THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 98, No. 8, 2003 © 2003 by Am. Coll. of Gastroenterology ISSN 0002-9270/03/$30.00 Published by Elsevier Inc. doi:10.1016/S0002-9270(03)00425-8
-
Upload
tyler-stevens -
Category
Documents
-
view
213 -
download
1
Transcript of Colonoscopy screening in the elderly: when to stop?

Colonoscopy Screening in the Elderly:When to Stop?Tyler Stevens, M.D., and Carol A. Burke, M.D.Department of Gastroenterology and Hepatology, Cleveland Clinic Foundation, Cleveland, Ohio
OBJECTIVES: The age to begin colorectal cancer (CRC)screening is based on the risk of neoplasia and is publishedin screening guidelines. The age to stop screening is un-known but should be based, in part, on the same principle.The purpose of this study was to establish whether theprevalence of neoplasia detected by colonoscopy dimin-ished with advancing age, to warrant ceasing colonoscopicscreening.
METHODS: The endoscopic and pathology reports of allasymptomatic subjects undergoing colonoscopy for the pur-pose of CRC screening or an evaluation of abdominal painor change in bowel habits between 1997 and 2000 werereviewed. A multivariate logistic regression analysis wasused to assess the effect of age, gender, and indication forexamination on the prevalence of neoplasia, as well as onhaving more than two adenomas, advanced adenomas (tu-bulovillous, villous, severe dysplasia, or size� 1 cm), andinvasive cancers.
RESULTS: A total of 915 patients were included. Of these,50% were male, with a mean age of 65 yr (range 50–100).Neoplasia peaked in the seventh decade, with a fall there-after (p � 0.009). Numerous adenomas, advanced adeno-mas, and invasive cancers increased with age. The yield foroverall neoplasia, advanced adenomas, and more than twoadenomas was higher in the screening group than in thesymptomatic group. More invasive cancers were found inthe symptomatic group compared with the asymptomaticgroup, but this did not achieve statistical significance (4vs1, p � 0.44).
CONCLUSIONS: The prevalence of advanced neoplasia con-tinues to increase with age. Subjects undergoing colonos-copy for screening had a greater risk for neoplasia than didsubjects with symptoms. There is no decline in yield ofadvanced neoplasia to justify stopping screening colonos-copy in the elderly. (Am J Gastroenterol 2003;98:1881–1885. © 2003 by Am. Coll. of Gastroenterology)
INTRODUCTION
Colonoscopy is gaining acceptance as the preferred strategyfor colorectal cancer (CRC) screening. It has the greatestsensitivity and specificity for the detection of neoplasiacompared with other modalities (1, 2). Evidence for itseffectiveness comes from cohort studies, which show a de-crease in the incidence and mortality of CRC in subjects whohave had adenomas removed (3–7). Colonoscopy has beenfound to be comparable in cost-effectiveness to other methodsof screening (8–10). Multiple guidelines include colonoscopyas an option for screening average risk patients (11, 12).Screening is initiated at age 50 yr because the incidence ofCRC rises precipitously after age 50 yr, from 26 cases per100,000 at age 45–49 yr to 49 cases at age 50–54 yr and 85cases at age 55–59 yr (13). Additionally, CRC is uncommonin asymptomatic persons 40–49 yr old, and advanced neo-plasia have been reported in less than 3.5% (14).
In contrast to recommendations of the age to beginscreening, no guidelines exist regarding the age to stopscreening. Part of such a decision depends on the clinicaljudgment of the physician, desires of the patient, presence ofother life-limiting comorbidities, projected lifespan, and thelength of protective benefit from screening. The decisionshould also be based on evidence of the prevalence ofcolorectal neoplasia with advancing age.
A recent study of screening flexible sigmoidoscopy foundthe risk of distal neoplasia to significantly decrease from19% at age 65–69 yr to 14% at age� 70 yr and suggestedstopping colorectal cancer screening after age 70 yr (15).
Establishing the prevalence of neoplasia in elderly pa-tients undergoing colonoscopy would be helpful in guidingphysicians and counseling patients as to the risk of neoplasiaand potential benefit of colonoscopy. The purpose of ourstudy was to assess the effect of age on the prevalence ofneoplasia detected by colonoscopy. In doing this, we hopedto determine whether there is an age at which the prevalenceof advanced neoplasia is low enough to cease screening. Wealso sought to determine whether gender or indication forexamination had an effect on the prevalence of neoplasia.
MATERIALS AND METHODS
The endoscopy reports of all colonoscopies performed in theDepartment of Gastroenterology and Hepatology at the
Presented at the American College of Gastroenterology Annual Meeting October21–24, 2001, Las Vegas, Nevada.
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 98, No. 8, 2003© 2003 by Am. Coll. of Gastroenterology ISSN 0002-9270/03/$30.00Published by Elsevier Inc. doi:10.1016/S0002-9270(03)00425-8

Cleveland Clinic Foundation between 1997 and 2000 werereviewed. Examinations done for colorectal cancer screen-ing in asymptomatic, average or increased risk patients, or insubjects with a change in bowel habit or abdominal painwere included. Exclusion criteria included incomplete ex-amination, poor bowel preparation, known history of pre-vious colon polyps, previous colonoscopy, hereditary colo-rectal cancer syndromes, or GI bleeding (overt or occult).Demographic information (age, gender, and indication forexamination) was obtained. Subject age was stratified bydecade: 50–60, 61–70, 71–80, and 81–100 yr. The preva-lence of overall neoplasia, numerous adenomas (more thantwo), advanced adenomas (size � 1 cm, tubulovillous, vil-lous, carcinoma in situ/severe dysplasia), and invasive can-cer was determined.
Descriptive data for the demographic characteristics ofage, gender, indication, and outcomes are reported as per-centages. Chi-square or Fisher exact tests were used toassess the association between age group, indication forexamination, and gender and neoplasia. Logistic regressionmodels were used to assess the association between age andprevalence of overall neoplasia, advanced adenomas, morethan two adenomas, and invasive cancer, adjusting for gen-der and indication for examination.
RESULTS
A total of 915 patients were included; 456 (49.8%) weremale (Table 1). The mean age was 65.2 yr (range 50–100yr); 340 patients were aged 50–60 yr, 251 were aged 61–70yr, 271 were aged 71–80 yr, and 53 were older than 80 yr.Fifty-two percent of colonoscopies (472) were done forCRC screening (30% for average risk and 22% for increasedrisk), 37% (337) were done for change in bowel habit, and12% (106) were done for abdominal pain (Table 2). The
elder age groups had relatively more examinations per-formed for symptom investigation. One hundred eighty-onepatients (20%) were found to have neoplasia (Table 3).Thirty-six patients (3.9%) had advanced adenomas, 23 pa-tients (2.5%) had more than two adenomas, and five patients(0.6%) were found to have invasive cancer.
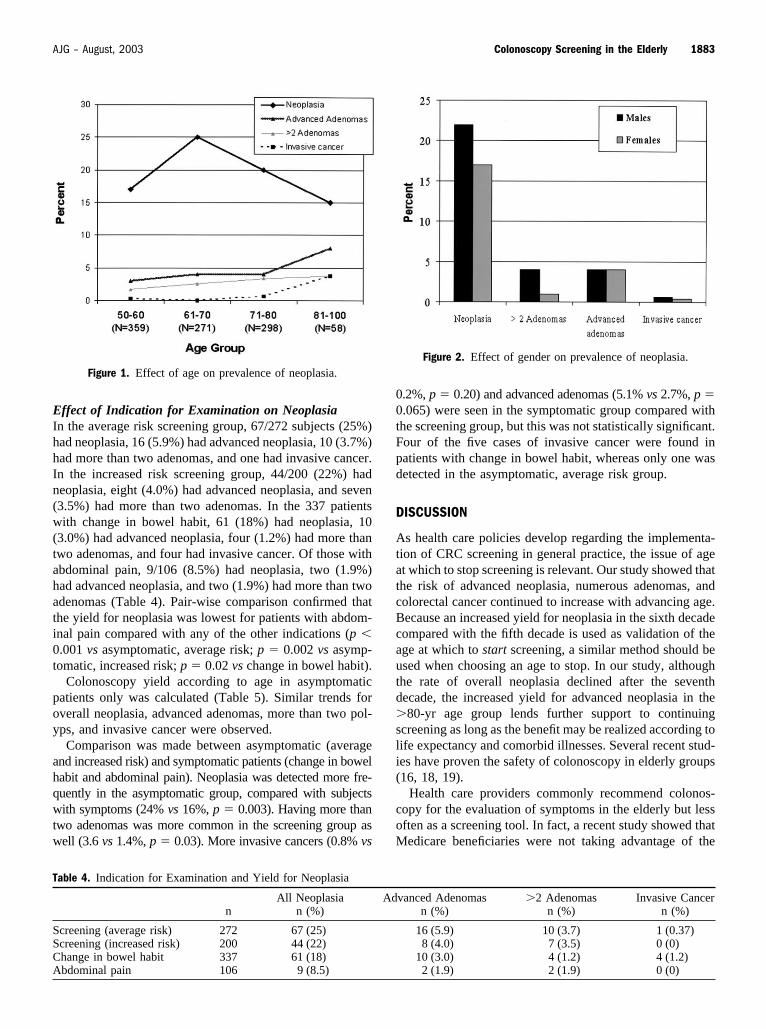
Effect of Age on NeoplasiaThe prevalence of neoplasia peaked in the sixth decade at25%, with a fall to 19% at ages 71–80 yr and 15% at ages81–100 yr (p � 0.009) (Fig. 1). The prevalence of advancedadenomas increased with age, from 3.2% at age 50–60 yr to4.4% at age 61–70 yr, 3.7% at age 71–80 yr, and 7.6% atage 81–100 yr, although this did not achieve statisticalsignificance (p � 0.16). The detection of more than twoadenomas increased from a rate of 1.8% at age 50–60 yr to2.8% at ages 61–70 yr, 3.0% at ages 71–80 yr, and 3.8% atages 81–100 yr (p � 0.017). The incidence of invasivecancers also increased with age (p � 0.019): one case(0.3%) in the sixth decade, two cases (0.7%) in the eighthdecade, and two cases (3.8%) in the oldest age group (age �80 yr).
Effect of Gender on NeoplasiaTwenty-two percent of men (101/456) and 17% of women(80/459) were found to have neoplasia (p � 0.20, Fig. 2).Men were more likely than women to have more than twoadenomas (4.0% vs 1.1%, p � 0.015). No gender differencewas seen in the prevalence of advanced adenomas or inva-sive cancer. Eighteen men and 18 women had advancedadenomas (4.0% vs 3.9%, p � 0.72). Three cases of invasivecancer were found in men and two cases in women (0.7% vs0.4%, p � 0.59).
Table 1. Patient Demographics
n %
Total 915Gender
Male 456 50Female 459 50
Age groups (yr)50–60 340 3761–70 251 2771–80 271 3081–100 53 6
Table 2. Indication for Examination
Indication n %
Age Group (Yr) n (%)
50–60 61–70 71–80 81–100
Average risk, screening 272 30 133 (49) 71 (26) 60 (22) 8 (3)Increased risk, screening 200 22 87 (43) 54 (27) 54 (27) 5 (3)Change in bowel habit 337 37 92 (27) 97 (29) 118 (35) 30 (9)Abdominal pain 106 12 28 (26) 29 (27) 40 (38) 10 (9)
Table 3. Colonoscopy Findings According to Most AdvancedLesion
Classification n %
Overall adenomas 181 20Tubular adenomas 145 16Advanced adenoma* 36 3.9
Size � 1 cm 27 2.9Tubulovillous adenomas 21 2.3Villous adenomas 1 0.1Carcinoma in situ 4 0.5Size � 1 cm and advanced
histology17 1.8
�2 Adenomas 23 2.5Invasive cancer 5 0.6
* Advanced adenoma: tubulovillous, villous, carcinoma in situ, or size � 1 cm.
1882 Stevens and Burke AJG – Vol. 98, No. 8, 2003
Effect of Indication for Examination on NeoplasiaIn the average risk screening group, 67/272 subjects (25%)had neoplasia, 16 (5.9%) had advanced neoplasia, 10 (3.7%)had more than two adenomas, and one had invasive cancer.In the increased risk screening group, 44/200 (22%) hadneoplasia, eight (4.0%) had advanced neoplasia, and seven(3.5%) had more than two adenomas. In the 337 patientswith change in bowel habit, 61 (18%) had neoplasia, 10(3.0%) had advanced neoplasia, four (1.2%) had more thantwo adenomas, and four had invasive cancer. Of those withabdominal pain, 9/106 (8.5%) had neoplasia, two (1.9%)had advanced neoplasia, and two (1.9%) had more than twoadenomas (Table 4). Pair-wise comparison confirmed thatthe yield for neoplasia was lowest for patients with abdom-inal pain compared with any of the other indications (p �0.001 vs asymptomatic, average risk; p � 0.002 vs asymp-tomatic, increased risk; p � 0.02 vs change in bowel habit).
Colonoscopy yield according to age in asymptomaticpatients only was calculated (Table 5). Similar trends foroverall neoplasia, advanced adenomas, more than two pol-yps, and invasive cancer were observed.
Comparison was made between asymptomatic (averageand increased risk) and symptomatic patients (change in bowelhabit and abdominal pain). Neoplasia was detected more fre-quently in the asymptomatic group, compared with subjectswith symptoms (24% vs 16%, p � 0.003). Having more thantwo adenomas was more common in the screening group aswell (3.6 vs 1.4%, p � 0.03). More invasive cancers (0.8% vs
0.2%, p � 0.20) and advanced adenomas (5.1% vs 2.7%, p �0.065) were seen in the symptomatic group compared withthe screening group, but this was not statistically significant.Four of the five cases of invasive cancer were found inpatients with change in bowel habit, whereas only one wasdetected in the asymptomatic, average risk group.
DISCUSSION
As health care policies develop regarding the implementa-tion of CRC screening in general practice, the issue of ageat which to stop screening is relevant. Our study showed thatthe risk of advanced neoplasia, numerous adenomas, andcolorectal cancer continued to increase with advancing age.Because an increased yield for neoplasia in the sixth decadecompared with the fifth decade is used as validation of theage at which to start screening, a similar method should beused when choosing an age to stop. In our study, althoughthe rate of overall neoplasia declined after the seventhdecade, the increased yield for advanced neoplasia in the�80-yr age group lends further support to continuingscreening as long as the benefit may be realized according tolife expectancy and comorbid illnesses. Several recent stud-ies have proven the safety of colonoscopy in elderly groups(16, 18, 19).
Health care providers commonly recommend colonos-copy for the evaluation of symptoms in the elderly but lessoften as a screening tool. In fact, a recent study showed thatMedicare beneficiaries were not taking advantage of the
Figure 2. Effect of gender on prevalence of neoplasia.
Table 4. Indication for Examination and Yield for Neoplasia
nAll Neoplasia
n (%)Advanced Adenomas
n (%)�2 Adenomas
n (%)Invasive Cancer
n (%)
Screening (average risk) 272 67 (25) 16 (5.9) 10 (3.7) 1 (0.37)Screening (increased risk) 200 44 (22) 8 (4.0) 7 (3.5) 0 (0)Change in bowel habit 337 61 (18) 10 (3.0) 4 (1.2) 4 (1.2)Abdominal pain 106 9 (8.5) 2 (1.9) 2 (1.9) 0 (0)
Figure 1. Effect of age on prevalence of neoplasia.
1883AJG – August, 2003 Colonoscopy Screening in the Elderly

screening colonoscopy benefit (20). It may be thought that,because an elderly patient has reached a certain age withoutdeveloping CRC, they may be in some way protected fromit. Our data refutes this idea: the yield for numerous adenomas,advanced adenomas, and invasive cancer increases with age.
The yield for neoplasia, numerous adenomas, and ad-vanced adenomas is surprisingly higher in asymptomaticthan in symptomatic subjects. This may be assumed to bebecause of our high sampling of increased risk patients, butno difference in the yield of neoplasia was seen betweenaverage and high risk screening groups. A recent study ofcolonoscopy in octogenarians by Sardinha et al. showed asimilar incidence of cancer in patients with abdominal painor constipation as in asymptomatic patients (16). Cancerwas detected in 11.5% of patients with bleeding, comparedwith 1.9% for all other indications. Furthermore, a review ofthe literature of yield of colonoscopy done for variousindications found a low yield in examinations done fornonbleeding symptoms (17). Although our results confirmthat colonoscopies done for nonbleeding symptoms have ayield comparable to those done for screening, it is notablethat 80% of our subjects with invasive cancer had a changein bowel habit.
Previous studies have shown an increased rate of neopla-sia in men compared with women (21, 22). We did not finda gender difference in the prevalence of neoplasia, advancedadenomas, and invasive cancer. Interestingly, men did havea slightly higher rate of numerous adenomas. Based on ourdata, gender should not effect decision to screen, becauseboth men and women have similar rates of advanced neo-plasia and CRC.
A recent study by David et al. reviewed 775 screeningflexible sigmoidoscopies (15). Adenomas were detected in19% of subjects 65–69 yr old, 14% of 70–74-yr-olds, and14% of �74-yr-olds. Because the yield of neoplasiadropped after age 70 yr, the authors concluded that endo-scopic screening for CRC should stop at age 75 yr. Althoughour study of colonoscopy demonstrated a similar decline inoverall neoplasia after age 70 yr, the incidence of advancedadenomas, multiple adenomas, and invasive cancer contin-ued to increase with age. Because these lesions portend thegreatest risk for CRC, our findings imply that CRC screen-ing should continue until life expectancy precludes a benefitof screening.
The life expectancy of the American population continuesto increase because of improved health care, nutrition, life-
style, and other factors. As the risk of advanced neoplasiaincreases, it seems appropriate to screen patients into theireighties and nineties, provided no obvious life-limiting co-morbidities exist. Further prospective studies are needed toprove a mortality benefit for the use of screening colonos-copy in older patients.
Reprint requests and correspondence: Carol A. Burke, M.D.,Cleveland Clinic Foundation, Gastroenterology A-30, 9500 EuclidAvenue, Cleveland, OH 44195.
Received Sep. 11, 2002; accepted Feb. 11, 2003.
REFERENCES
1. Lieberman DA, Smith FW. Screening from colon malignancywith colonoscopy. Am J Gastroenterol 1991;86:946–51.
2. Inadomi JM, Sonnenberg A. The impact of colorectal cancerscreening on life expectancy. Gastrointest Endosc 2000;51:517–23.
3. Selby JV, Friedman GD, Quesenberry CP, et al. A case-control study of screening sigmoidoscopy and mortality fromcolorectal cancer. N Engl J Med 1992;326:653–7.
4. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colo-rectal cancer by colonoscopic polypectomy. N Engl J Med1993;329:1977–81.
5. Muller AD, Sonnenberg A. Protection by endoscopy againstdeath from colorectal cancer. Arch Intern Med 1995;155:1741–8.
6. Muller AD, Sonnenberg A. Prevention of colorectal cancer byflexible endoscopy and polypectomy. Ann Intern Med 1995;123:904–10.
7. Citarda F, Tomaselli G, Capocaccia R, et al. Efficacy instandard clinical practice of colonoscopic polypectomy in re-ducing colorectal cancer incidence. Gut 2001;48:812–5.
8. Wagner JL, Herdman RC, Wadhwa S. Cost effectiveness ofcolorectal cancer screening in the elderly. Ann Intern Med1991;115:807–17.
9. Sonnenberg A, Delco F, Inadomi JM. Cost-effectiveness ofcolonoscopy in screening for colorectal cancer. Ann InternMed 2000;133:573–84.
10. Leiberman D. Cost-effectiveness model for colon cancerscreening. Gastroenterology 1995;109:1781–90.
11. Winawer SJ, Fletcher RH, Miller L, et al. Colorectal cancerscreening: Clinical guidelines and rationale. Gastroenterology1997;112:594–642.
12. Smith RA, Mettlin CJ, Johnston-Davis KJ, et al. AmericanCancer Society guidelines for early detection of cancer. CAJ Clin 2000;50:34–49.
13. Ries LAG, Eisner MP, Kosary CL, et al, eds. SEER cancerstatistics review, 1973–1999. Bethesda, MD: National CancerInstitute.
Table 5. Yield of Colonoscopy for Asymptomatic Patients Only
Age Group(Yr) n
All Neoplasian (%)
AdvancedAdenomas
n (%)�2 Adenomas
n (%)Invasive Cancer
n (%)
50–60 220 46 (21) 9 (4.0) 6 (2.7) 1 (0.5)61–70 125 38 (30) 7 (5.6) 4 (3.2) 071–80 114 25 (22) 6 (5.2) 6 (5.2) 081–100 13 2 (14) 1 (8) 1 (8) 0
1884 Stevens and Burke AJG – Vol. 98, No. 8, 2003

14. Imperiale TF, Wagner DR, Lin CY, et al. Results of screeningcolonoscopy among persons 40 to 49 years of age. N EnglJ Med 2002;346:1781–5.
15. David J, Totta F, Shaukat M, et al. At what age is it appropriateto stop screening flexible sigmoidoscopy? Am J Gastroenterol2000;95:2531 (abstract).
16. Sardinha TC, Nogueras JJ, Ehrenpreis ED. Colonoscopy inoctogenarians: A review of 428 cases. Int J Colorectal Dis1999;14:172–6.
17. Rex D. Colonoscopy. A review of its yield for cancers andadenomas by indication. Am J Gastroenterol 1995;90:353–63.
18. Bae L, Pines A, Shemesh E, et al. Colonoscopy in patientsaged 80 years or older and its contribution to the evaluation ofrectal bleeding. Postgrad Med J 1992;68:355–8.
19. Ure T, Dhghan K, Vernava AM, et al. Colonoscopy in theelderly. Low risk, high yield. Surg Endosc 1995;9:505–8.
20. Mansley EC, Straus WL, Pshos CL. Many medicare recipientslack awareness of colorectal cancer screening coverage: Anopportunity for intervention? Am J Gastroenterol 2001;96:S274 (abstract).
21. Cannon-Albright LA, Skolnick MH, Bishop DT, et al. Com-mon inheritance of susceptibility to colonic adenomatous pol-yps and associated colorectal cancers. N Engl J Med 1988;319:533–7.
22. Johnson DA, Gurney MS, Volpe RJ, et al. A prospective studyof the prevalence of colonic neoplasms in asymptomatic pa-tients with an age-related risk. Am J Gastroenterol 1991;86:941–5.
1885AJG – August, 2003 Colonoscopy Screening in the Elderly


















