Cognitive Outcomes and Positional Plagiocephaly · Scales, Second Edition and Wechsler Individual...
11
Cognitive Outcomes and Positional Plagiocephaly Brent R. Collett, PhD, a,b Erin R. Wallace, PhD, b Deborah Kartin, PT, PhD, c Michael L. Cunningham, MD, PhD, d,e,f Matthew L. Speltz, PhD a,b abstract BACKGROUND: Studies have revealed an association between positional plagiocephaly and/or brachycephaly (PPB) and development, although little is known about long-term outcomes. We examined cognition and academic achievement in children with and without PPB, testing the hypothesis that children who had PPB as infants would score lower than controls. METHODS: We enrolled 187 school-aged children with a history of PPB and 149 controls. Exposures were the presence or absence and severity of infancy PPB (mild, moderate to severe). Cognitive and academic outcomes were assessed by using the Differential Ability Scales, Second Edition and Wechsler Individual Achievement Test, Third Edition, respectively. RESULTS: Children with PPB scored lower than controls on most scales of the Differential Ability Scales, Second Edition (standardized effect sizes [ESs] = 20.38 to 20.20) and the Wechsler Individual Achievement Test, Third Edition (ESs = 20.22 to 20.17). Analyses by PPB severity revealed meaningful differences among children with moderate to severe PPB (ESs = 20.47 to 20.23 for 8 of 9 outcomes), but few differences in children with mild PPB (ESs = 20.28 to 0.14). CONCLUSIONS: School-aged children with moderate to severe PPB scored lower than controls on cognitive and academic measures; associations were negligible among children with mild PPB. The findings do not necessarily imply that these associations are causal; rather, PPB may serve as a marker of developmental risk. Our findings suggest a role for assessing PPB severity in clinical practice: providing developmental assessment and intervention for infants with more severe deformation and reassurance and anticipatory guidance for patients with mild deformation. WHAT’S KNOWN ON THIS SUBJECT: Infants and toddlers with positional plagiocephaly and/or brachycephaly (PPB) exhibit mild developmental delays relative to unaffected children. It is not known whether these developmental differences persist in school-aged children. WHAT THIS STUDY ADDS: School-aged children who had moderate to severe PPB as infants scored lower on measures of cognition and academic achievement than unaffected children. Differences between children who had mild PPB versus unaffected controls were negligible. To cite: Collett BR, Wallace ER, Kartin D, et al. Cognitive Outcomes and Positional Plagiocephaly. Pediatrics. 2019; 143(2):e20182373 a Center for Child Health, Behavior, and Development and d Center for Developmental Biology and Regenerative Medicine, Seattle Children’ s Research Institute, Seattle, Washington; b Departments of Psychiatry and Behavioral Sciences, c Rehabilitation Medicine, and e Pediatrics, School of Medicine, University of Washington, Seattle, Washington; and f Seattle Children’ s Craniofacial Center, Seattle, Washington Drs Collett and Speltz conceptualized and designed the study, supervised data collection, and drafted the manuscript; Dr Wallace completed the data analyses and drafted the analyses and results sections of the manuscript; Dr Kartin assisted with the selection of outcome measures; Dr Cunningham assisted with the design of the study and helped to develop the methods for measuring positional plagiocephaly and/or brachycephaly severity in the earlier phase of this research; and all authors reviewed and revised the final manuscript. DOI: https://doi.org/10.1542/peds.2018-2373 Accepted for publication Oct 30, 2018 Address correspondence to Brent R. Collett, PhD, Center for Child Health, Behavior, and Development, Seattle Children’ s Research Institute, 2001 8th Ave, Mailstop CW8-6, Seattle, WA 98121. E-mail: [email protected] PEDIATRICS Volume 143, number 2, February 2019:e20182373 ARTICLE by guest on June 22, 2020 www.aappublications.org/news Downloaded from
Transcript of Cognitive Outcomes and Positional Plagiocephaly · Scales, Second Edition and Wechsler Individual...

Cognitive Outcomes andPositional PlagiocephalyBrent R. Collett, PhD,a,b Erin R. Wallace, PhD,b Deborah Kartin, PT, PhD,c Michael L. Cunningham, MD, PhD,d,e,f
Matthew L. Speltz, PhDa,b
abstractBACKGROUND: Studies have revealed an association between positional plagiocephaly and/orbrachycephaly (PPB) and development, although little is known about long-term outcomes.We examined cognition and academic achievement in children with and without PPB, testingthe hypothesis that children who had PPB as infants would score lower than controls.
METHODS: We enrolled 187 school-aged children with a history of PPB and 149 controls.Exposures were the presence or absence and severity of infancy PPB (mild, moderate tosevere). Cognitive and academic outcomes were assessed by using the Differential AbilityScales, Second Edition and Wechsler Individual Achievement Test, Third Edition, respectively.
RESULTS: Children with PPB scored lower than controls on most scales of the Differential AbilityScales, Second Edition (standardized effect sizes [ESs] = 20.38 to 20.20) and the WechslerIndividual Achievement Test, Third Edition (ESs = 20.22 to 20.17). Analyses by PPB severityrevealed meaningful differences among children with moderate to severe PPB (ESs =20.47 to20.23 for 8 of 9 outcomes), but few differences in children with mild PPB (ESs = 20.28to 0.14).
CONCLUSIONS: School-aged children with moderate to severe PPB scored lower than controls oncognitive and academic measures; associations were negligible among children with mild PPB.The findings do not necessarily imply that these associations are causal; rather, PPB may serveas a marker of developmental risk. Our findings suggest a role for assessing PPB severity inclinical practice: providing developmental assessment and intervention for infants with moresevere deformation and reassurance and anticipatory guidance for patients with milddeformation.
WHAT’S KNOWN ON THIS SUBJECT: Infants andtoddlers with positional plagiocephaly and/orbrachycephaly (PPB) exhibit mild developmentaldelays relative to unaffected children. It is not knownwhether these developmental differences persist inschool-aged children.
WHAT THIS STUDY ADDS: School-aged children whohad moderate to severe PPB as infants scored loweron measures of cognition and academic achievementthan unaffected children. Differences between childrenwho had mild PPB versus unaffected controls werenegligible.
To cite: Collett BR, Wallace ER, Kartin D, et al. CognitiveOutcomes and Positional Plagiocephaly. Pediatrics. 2019;143(2):e20182373
aCenter for Child Health, Behavior, and Development and dCenter for Developmental Biology and RegenerativeMedicine, Seattle Children’s Research Institute, Seattle, Washington; bDepartments of Psychiatry and BehavioralSciences, cRehabilitation Medicine, and ePediatrics, School of Medicine, University of Washington, Seattle,Washington; and fSeattle Children’s Craniofacial Center, Seattle, Washington
Drs Collett and Speltz conceptualized and designed the study, supervised data collection, anddrafted the manuscript; Dr Wallace completed the data analyses and drafted the analyses andresults sections of the manuscript; Dr Kartin assisted with the selection of outcome measures; DrCunningham assisted with the design of the study and helped to develop the methods formeasuring positional plagiocephaly and/or brachycephaly severity in the earlier phase of thisresearch; and all authors reviewed and revised the final manuscript.
DOI: https://doi.org/10.1542/peds.2018-2373
Accepted for publication Oct 30, 2018
Address correspondence to Brent R. Collett, PhD, Center for Child Health, Behavior, andDevelopment, Seattle Children’s Research Institute, 2001 8th Ave, Mailstop CW8-6, Seattle, WA 98121.E-mail: [email protected]
PEDIATRICS Volume 143, number 2, February 2019:e20182373 ARTICLE by guest on June 22, 2020www.aappublications.org/newsDownloaded from

Positional skull deformation ininfancy is common in the UnitedStates and other countries wheresupine sleep positioning isrecommended to prevent suddeninfant death syndrome (SIDS).Although these efforts reduced theincidence of SIDS, an unanticipatedconsequence was an increase in therate of positional plagiocephaly and/or brachycephaly (PPB).1,2 Prevalencestudies are limited, although the bestestimates suggest that 20% to 30%of infants have noticeable skulldeformation, and PPB has becomea common reason for referral tocraniofacial and neurosurgeryclinics.3–6
Although PPB is considered a benigncosmetic condition, associationsbetween PPB and development havebeen described. Miller and Clarren7
first reported on PPB andneurodevelopmental outcomes ina retrospective study of 63 school-aged children with a history of PPBand 91 unaffected siblings. Childrenwith PPB were much more likely tohave received developmental andeducational interventions thansiblings. Several others have sincereported developmental deficits inchildren with PPB relative to testnorms or controls. In a recent review,most of the studies reviewed revealedan association between PPB anddevelopmental outcomes.8 Aside fromthe Miller and Clarren7 study, nearlyall of this research involved infantsand toddlers.
We have previously reported on thedevelopment of 235 children withPPB and 237 children without PPB ina cohort recruited in infancy andreevaluated at ages 18 and 36months.6,9,10 At each assessment,children with PPB scored lower thancontrols on the Bayley Scales of Infantand Toddler Development, ThirdEdition. The nature of groupdifferences changed over time: ininfancy, PPB was most stronglyassociated with motor development.By age 3, motor differences were
reduced and differences in cognitionand language were the mostprominent.10
The goals of this study were toevaluate development in school-agedchildren with and without a history ofPPB, testing the hypothesis thatchildren with PPB would score lowerthan controls and examiningdifferences as a function of PPBseverity.
METHODS
Study Design
We used a prospective cohort designto assess development in childrenwith and without a history of PPB. Inphase 1 of this research, infants withPPB (cases) were recruited at thetime of their diagnosis in the SeattleChildren’s Craniofacial Center.6 Thefirst 8 controls were recruitedthrough area pediatricians, andremaining controls were recruitedthrough an infant participant registry.To confirm the presence or absence ofskull deformation, we used a 4-pod3dMD digital camera to collect three-dimensional (3D) surface images ofparticipants' head shapes in infancy.6
Images were deidentified, randomlysorted, and rated by 2 pediatriciansfrom the Seattle Children’sCraniofacial Center who wereunaware of the infants’ PPB diagnosis.Ratings of deformation were made ona scale of 0 = none, 1 = mild, 2 =moderate, and 3 = severe by usinga scale based on a measure describedby Argenta et al.1,11 Interrateragreement was excellent for thepresence or absence of deformation(k = 0.80) and good for severityrating (weightedk = 0.72). We usedthe average of the 2 ratings tocategorize infants as having PPB(diagnosed PPB, severity rating$0.5), unaffected controls (nodiagnosed PPB, severityrating = 0),and affected controls (no diagnosedPPB, severity rating $0.5). Theresulting samples included 233children with confirmed PPB, 167
unaffected controls, and 70 affectedcontrols.
We reapproached children withconfirmed PPB and unaffectedcontrols from the infant cohort whenthey were age $7 years. Familiesreceived $200 for their participationas well as a written summary of theirchild’s evaluation results. The studywas approved by the SeattleChildren’s Hospital InstitutionalReview Board.
Children With PPB
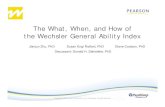
Phase 1 inclusion criteria for childrenwith PPB were diagnosis of PPB bya clinician in the Seattle Children’sCraniofacial Center, confirmed byusing independent ratings of 3Dimages by 2 pediatricians who wereunaware of the children’s PPB status;age 4 to 11 months at the time ofdiagnosis; English reported as theprimary language spoken in thehome; and the child’s biologic motherwas available for participation.Exclusions were prematurity (,35weeks’ gestation); diagnosedneurodevelopmental conditions (eg,Down syndrome); and severe sensoryimpairments (eg, deafness orblindness). We enrolled 235 infantswith PPB, representing 52% of thoseapproached.6 No discernibledeformation was observed on 3Dimaging for 2 children with clinicalPPB diagnoses, and they were notreapproached for phase 2 follow-up.Significant neurodevelopmentalconditions were diagnosed afterenrollment for 7 participants (eg,22q11 deletion, Chiari malformation),who were not approached for follow-up, and 1 child with PPB died. Thisleft a total of 225 potentially eligibleparticipants with PPB (see Fig 1). Tenfamilies could not be located, 9declined participation, and 19 wereunresponsive to outreach efforts. Atotal of 187 families consented toparticipate between August 2014 andMarch 2018, representing 83% ofthose eligible.
2 COLLETT et al by guest on June 22, 2020www.aappublications.org/newsDownloaded from

Unaffected Controls
In addition to the exclusions listed forchildren with PPB, controls wereexcluded if they had evidence ofdeformation on the 3D imagingcompleted in phase I. Specifically,although they had not been diagnosedwith PPB, we excluded the 70“affected control” children found tohave some skull deformation ininfancy (63 mild, 7 moderate). Onechild in the control sample diedbefore phase 2. Out of 164 unaffectedcontrols eligible for follow-up, 3families could not be located, 1 familydeclined participation, and 11families were unresponsive. In total,149 unaffected control familiesconsented to participate betweenDecember 2014 and February 2018,representing 91% of those eligible.
Study Measures
Participants completed anindividually-administered
neuropsychological assessmentbattery including the DifferentialAbility Scales, Second Edition(DAS-2),12 a measure of cognitiveability, and the Wechsler IndividualAchievement Test, Third Edition(WIAT-3),13 a measure of academicachievement. Outcomes from theDAS-2 were the composite scales forglobal cognitive ability (GCA), verbalability, nonverbal reasoning, spatialability, working memory, andprocessing speed. From the WIAT-3,outcomes included composite totalreading, written expression, andmathematics scores. Standardized,norm-referenced scores aregenerated for all DAS-2 and WIAT-3indices, with an averagestandardscore = 100,SD = 15. Testswere administered by trainedpsychometrists and video recordedfor coding of inter-examinerreliability. Approximately 30% of thetests administered were reviewed byone of the study psychologists (B.R.C.,
M.L.S.). Average item-level agreementranged from 95% to 100% for theDAS-2 and 94% to 100% for theWIAT-3.
We used clinician ratings of 3Dhead shape images describedearlier to quantify PPB severity. Onthe basis of their infant data,children with PPB were categorizedas having mild PPB (averageseverityrating = 0.5–1.0) ormoderate to severe PPB (averageseverityrating = 1.5–3.0).
Caregivers completed asemistructured interview, whichconfirmed and updated familydemographic information;categorized the child’s participationin developmental interventions (eg,occupational therapy, physicaltherapy, speech and/or languagetherapy); and documented anynewly diagnosed medicalconditions.
FIGURE 1Participants with and without PPB in the infant cohort (phase 1) and school-age follow-up (phase 2).
PEDIATRICS Volume 143, number 2, February 2019 3 by guest on June 22, 2020www.aappublications.org/newsDownloaded from

Statistical Analyses
Descriptive statistics (ie, means, SDs,frequencies) were used to summarizeparticipant demographic and clinicalcharacteristics separately for childrenwith PPB and unaffected controls.We also used descriptive statisticsto compare participants andnonparticipants on demographicinformation from phase 1. We usedlinear regression analyses with robuststandard errors to compare childrenwith PPB and unaffected controls onprimary outcomes. Analyses wereadjusted for demographics, includingsocioeconomic status (SES) basedon the total Hollingshead14 score(continuous), age at assessment, sex,and race and/or ethnicity (white,non-Hispanic versus people of coloror Hispanic). Because of theexploratory nature of these analyses,we did not adjust P values formultiple comparisons and did notconsider P values alone to bedichotomous tests of significance.Instead, we evaluated the magnitude,precision, and consistency of effectsacross outcomes.15 To determine themagnitude of group differences, wecalculated standardized meandifference effect sizes (ESs) using theadjusted group difference dividedby the root mean square error.To evaluate for attrition bias, werepeated these analyses using inverseprobability weighting (IPW).16 Forthese analyses, we determinedpropensity scores for phase 2participation based on phase 1characteristics (SES, sex, race and/orethnicity, PPB severity, and BayleyScales of Infant and ToddlerDevelopment, Third Edition scores atage 36 months). We then used thesescores to generate propensity weightsfor linear regression analyses. Inessence, these analyses giveadditional “weight” to participantswho were retained in the studyand were similar to participantswho were lost to follow-up. Wealso evaluated the effects ofdevelopmental intervention on
achievement and cognitive scoresusing censored normal regression.17
This approach assumes that thescores of children who receivedintervention are “left censored” and,although their true scores in theabsence of intervention are unknown,they are presumed to be at least aslow as the scores observed.
To evaluate case-control differencesby severity of skull deformation, werepeated these analyses for childrenwho had mild PPB in infancy versuscontrols and those who had moderateto severe PPB versus controls. Wealso ran sensitivity analyses forclinically relevant characteristics,including history of orthotic helmettreatment, torticollis, twin status, andprematurity (ie, delivery #38 weeks’gestation).
RESULTS
A total of 336 children (N = 187children with PPB,N = 149 unaffectedcontrols) were re-enrolled forparticipation. Participants andnonparticipants were similar in mostrespects, although nonparticipatingfamilies tended to be lower in SES,more likely to have moderate tosevere PPB in infancy (90% versus72% among participants), and tohave had developmental delays asinfants or toddlers (53% versus 38%among participants). Sixteenparticipants (n = 8 children with PPB,n = 8 controls) were unable tocomplete an in-person assessment(eg, because of family relocationout of the country) and completedonly a caregiver interview.Neuropsychological assessment datawere considered invalid for 1 controlbecause of child refusal, resulting inavailable test data for 1 or moreoutcomes for 179 children with PPBand 140 unaffected controls.
Children in both groups werepredominately boys (66% childrenwith PPB, 57% unaffected controls),white and non-Hispanic (69%children with PPB, 60% unaffected
controls), and from middle to upperSES families (ie, Hollingshead14
categories I–II; 80% children withPPB, 78% unaffected controls)(Table 1). Mean age at participationwas 9.0 years (SD = 0.8) for childrenwith PPB and 8.8 years (SD = 0.6) forunaffected controls. Children who hadPPB in infancy were much more likelythan controls to have received someform of developmental intervention(66% children with PPB, 21%unaffected controls). Among childrenwith PPB, 52 (28%) had mild PPB asinfants and 135 (72%) had moderateto severe PPB. Sixty-four (34%)children received orthotic helmettreatment of their skull deformation,and 84 (45%) had a history oftorticollis.
Mean cognitive and academicachievement scores for both childrenwith PPB and controls were generallywithin the “average” range relativeto test norms (Table 2). Afteradjustment for demographiccharacteristics, children with PPBscored lower than unaffected controlson most scales of the DAS-2 withESs ranging from 20.38 to 20.20(P = .001–.09). Processing speed wasthe only exception (ES = 0.04, P =.72). Children with PPB also scoredlower than unaffected controls onthe WIAT-3, although differenceswere smaller and statisticallynonsignificant (ESs = 20.22 to20.17,P = .06–.16). The magnitude of groupdifferences increased when adjustingfor attrition by using IPW analysesand when adjusting for interventionparticipation by using censorednormal regression (SupplementalTable 3). For example, the ES for DAS-2GCA scores increased from 20.38 to20.42 in the primary and IPW-adjusted analyses, respectively,suggesting that the magnitude ofgroup differences is slightly largerwhen accounting for differentialattrition.
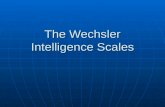
In analyses stratified by PPB severity,we found that case-controldifferences were consistently larger
4 COLLETT et al by guest on June 22, 2020www.aappublications.org/newsDownloaded from

for children who had moderate tosevere PPB than for those witha history of mild PPB (Fig 2). Forexample, on the DAS-2, case-controldifferences ranged from ESs = 20.47to 20.32 (P , .001–.02) on mostsubscales when comparing childrenwith moderate to severe PPB tounaffected controls. Processing speedwas the only subtest on whichmoderate to severe cases did notscore significantly lower thancontrols (ES = 0.01, P = .71). On theWIAT-3, case-control differenceswere ESs = 20.25 to 20.23(P = .04–.07) for children who hadmoderate to severe PPB. Whencomparing children with mild PPB tocontrols, ESs ranged from 20.28 to
0.14 (P = .06–.48) on the DAS-2 and20.13 to 0.00 (P = .44–.99) on theWIAT-3.
In sensitivity analyses, we found thatgroup differences were similar forchildren with and without a history oforthotic helmet treatment and inanalyses excluding children withtorticollis, those born #38 weeks’gestation, and twins (SupplementalTables 4 and 5).
DISCUSSION
This is the first study to trackdevelopmental outcomes for school-aged children with and withouta history of PPB. Strengths include
a large, longitudinal cohort ofchildren with and without PPB; theuse of “blinded” clinician ratings of3D images to document the presenceand severity of PPB several yearsbefore the collection of the outcomedata reported here; a low rate ofattrition; and a broad, standardizedneuropsychological test battery. Ourfindings are consistent with thoseobserved in early childhood6,9,10 andsuggest that children with PPB scorelower than controls on measures ofcognition and, to a lesser extent,academic achievement. There wasa gradient in these differences asa function of the severity of PPB ininfancy, with children who had mildPPB showing few if any differences
TABLE 1 Characteristics of Children With and Without Deformational Plagiocephaly at School Age
Characteristic Controls Children With PPB
N or Mean % or SD N or Mean % orSD
Total 149 100.0 187 100.0SexGirls 64 43.0 64 34.2Boys 85 57.0 123 65.8
Age, y 8.8 0.6 9.0 0.8Race and/or ethnicityWhite, non-Hispanic 89 59.7 130 69.5Asian American or Pacific Islander 4 2.7 9 4.8African American 5 3.4 0 0.0Hispanic or Latino 20 13.4 22 11.8Mixed race or ethnicity 31 20.8 26 13.9
SESI, highest 39 26.2 69 36.9II 77 51.7 80 42.8III 24 16.1 27 14.4IV 8 5.4 10 5.3V, lowest 1 0.7 1 0.5
Child delivered #38 wkNo 139 93.3 146 78.1Yes 10 6.7 41 21.9
Developmental interventions, ever receivedOccupational or physical therapy 15 10.1 106 56.7Speech or language therapy 23 15.4 56 29.9Any intervention 31 20.8 123 65.8
TorticollisNo 146 98.0 103 55.1Yes 3 2.0 84 44.9
Helmet treatmentNo — — 122 65.2Yes — — 64 34.2
Severity of plagiocephalyMild — — 52 27.8Moderate — — 101 54.0Severe — — 34 18.2
—, not applicable.
PEDIATRICS Volume 143, number 2, February 2019 5 by guest on June 22, 2020www.aappublications.org/newsDownloaded from

relative to controls and those whohad moderate to severe PPBexhibiting robust differences (eg,ESs = 20.47 to 20.32 on the DAS-2,representing ∼4 to 7 standard scorepoints in IQ). Other factors that couldmodify group differences (eg, historyof torticollis, orthotic helmettreatment) had little effect.
Some of the observed case-controldifferences were modest, and mostchildren in both groups scored withinthe average range compared with testnorms. However, as Bellinger18 haspointed out, even a modest effect canhave significant cumulative publichealth consequences when anexposure or condition is highlyprevalent. In addition, our findingswere observed in a low risk samplewith respect to both biological andsocial factors, making it unsurprisingthat both groups scored within theaverage range relative to test norms.Specifically, in the earlier phaseof this research, we excludedchildren delivered at ,35 weeks’gestation and those with knownneurodevelopmental conditions.Although overall retention wasexcellent, there was differentialattrition among children from lowSES households, those with moresevere PPB in infancy, and childrenwho exhibited developmental delays.Developmental risk was furtherattenuated by a high rate ofintervention. Children with PPBwere more likely than unaffectedcontrols to receive developmentalintervention (66% versus 21%), andtheir rate of intervention was higherthan is typically observed in thegeneral population.19 All of thesefactors could result in higher scoresthan might be observed in the generalpopulation, and, if anything, ourresults may be an underestimate ofgroup differences.
In addition to differential attrition,study limitations include clinic-basedrecruitment of children with PPB andrecruitment of unaffected controlsthrough a participant registry.TA
BLE2Comparisonof
MeanIQ
andAchievem
entScores
inChildrenWith
andWithoutPPB
Test
andScale
Controls
ChildrenWith
PPB
ChildrenWith
PPBVersus
Controls
Unadjusted
Adjusted
a
NMean(SD)
NMean(SD)
MeanDifference
95%
CIES
PMeanDifference
95%
CIES
P
DAS-2
GCA
140
106.9(11.9)
179
103.5(12.9)
23.46
26.18
20.74
20.28
.01
24.26
26.89
21.63
20.38
.002
Nonverbalreasoning
140
104.4(14.0)
179
101.2(13.6)
23.23
26.28
20.19
20.24
.04
24.00
27.03
20.97
20.31
.01
Spatial
140
105.7(10.9)
179
104.2(12.3)
21.55
24.10
1.01
20.13
.24
22.19
24.73
0.34
20.20
.09
Processing
speed
140
101.7(12.5)
177
102.4(13.1)
0.64
22.20
3.47
0.05
.66
0.53
22.41
3.47
0.04
.72
Verbal
140
107.4(12.9)
179
103.5(13.1)
23.94
26.82
21.06
20.30
.01
24.66
27.51
21.81
20.38
.001
Working
mem
ory
140
104.0(11.1)
179
101.2(11.0)
22.86
25.31
20.41
20.26
.02
23.33
25.74
20.93
20.32
.01
WIAT-3
Mathematics
140
106.4(15.5)
176
104.9(15.4)
21.44
24.88
2.00
20.09
.41
22.75
26.14
0.63
20.19
.11
Totalreading
137
107.4(15.7)
171
104.9(13.1)
22.51
25.97
0.96
20.16
.16
23.19
26.47
0.10
20.22
.06
Written
expression
139
101.6(14.8)
169
99.6(15.1)
22.02
25.32
1.27
20.14
.23
22.29
25.50
0.92
20.17
.16
aAdjusted
forsex,SES(continuous),race
(white
orpeople
ofcolor),age
inmonths(continuous).
6 COLLETT et al by guest on June 22, 2020www.aappublications.org/newsDownloaded from

Although our case and control groupswere demographically similar,children referred to a specialty clinicmay differ from nonreferred children.For example, referral may beassociated with a higher level ofconcern and vigilance among parentsregarding their child’s health, orbetter access to health care. Similarly,control families participating ina research registry may differ inways that influence their child’sdevelopment (eg, parents’ curiosityor interest in research) but areinadequately captured bydemographic measures. Ideally, ourfindings would be replicated in
a study in which population-basedsampling of children with andwithout PPB is used. Anotherlimitation relates to our assessmentof academic achievement at a youngage, when measures may not besensitive enough to detectdifferences.
As we have written previously,10
the association between PPBand neurodevelopment does notnecessarily indicate a causalrelationship. That is, we cannot saythat PPB causes developmentaldisadvantage. Determining causality isalways problematic in observational
research. However, future prospective,population-based studies that trackearly development and head shapefrom birth would help to clarifywhether motor deficits precede orfollow skull deformation. We havehypothesized that PPB may, in fact,serve as a marker for developmentalvulnerability. For example, infantswith subtle neuromotor deficits maybe less able to reposition themselvesand more likely to develop PPB,particularly in the context of routinesupine positioning. As childrenmature, these motor deficits may havea cascading effect on other areas ofdevelopment.20,21 If this were true,
FIGURE 2Standardized mean difference ESs and confidence intervals for case-control comparisons, stratified by PPB severity: mild PPB versus unaffected controlsand moderate to severe PPB versus unaffected controls.
PEDIATRICS Volume 143, number 2, February 2019 7 by guest on June 22, 2020www.aappublications.org/newsDownloaded from

treating the skull deformationassociated with PPB may be lessimportant than evaluating thedevelopmental progress of affectedinfants and providing earlyintervention as needed. Sensitivityanalyses adjusting for developmentaltreatments such as physical therapyand occupational therapy suggest theirpossible benefit for most outcomes.
Our findings reveal that the severityof skull deformation is importantwhen considering developmental riskfor infants with PPB, implying theneed for reliable measures of PPB toguide pediatricians’ decisions toeither refer a child for furtherevaluation or provide caregiverreassurance and anticipatoryguidance. Such measures have beendescribed in the literature11;however, they are not widely used inclinical practice. Rather, we suspectthat the decision to refer a child forfurther evaluation of positional skulldeformity or its developmentalimplications often depends on lessdata-driven factors such as the degreeof expressed caregiver concern,clinicians’ perceptions of caregivers’
potential to benefit from specialtyservices, or clinicians’ beliefs aboutthe importance of infant skulldeformation.
Among infants with moderate tosevere deformation, we recommenddevelopmental assessment,monitoring, and intervention. Forexample, infants with more noticeableskull deformation might receivedevelopmental assessment in primarycare with a low threshold for referralto a developmental specialist (eg,physical therapist or occupationaltherapist). In addition to ruling outother etiologies for head shapeanomalies (eg, craniosynostosis), animportant function for specialtyclinics within tertiary care centerswould be to provide developmentalassessment and parent coaching tooptimize early motor development. Incontrast, given that children withmild PPB as infants did not differfrom controls (at least in the currentstudy), caregiver reassurance andanticipatory guidance would seem tobe most appropriate. Randomizedclinical trials for children withvarying degrees of skull deformation
are needed to confirm theseimpressions.
ACKNOWLEDGMENTS
We thank all of the families whoparticipated in this research for theirtime and dedication to our project.We also thank Tristen Nash, projectcoordinator, and the psychometristsand research staff who assisted withdata collection.
ABBREVIATIONS
3D: three-dimensionalDAS-2: Differential Ability Scales,
Second EditionES: effect sizeGCA: global cognitive abilityIPW: inverse probability weightingPPB: positional plagiocephaly and/
or brachycephalySES: socioeconomic statusSIDS: sudden infant death
syndromeWIAT-3: Wechsler Individual
Achievement Test, ThirdEdition
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2019 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Funded by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Development (R01HD080462; Dr Collett, Principal Investigator).
Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Argenta LC, David LR, Wilson JA, Bell WO.An increase in infant cranial deformitywith supine sleeping position.J Craniofac Surg. 1996;7(1):5–11
2. Turk AE, McCarthy JG, Thorne CH, WisoffJH. The “back to sleep campaign” anddeformational plagiocephaly: is therecause for concern? J Craniofac Surg.1996;7(1):12–18
3. Hutchison BL, Hutchison LA, ThompsonJM, Mitchell EA. Plagiocephaly and
brachycephaly in the first two years oflife: a prospective cohort study.Pediatrics. 2004;114(4):970–980
4. Kane AA, Mitchell LE, Craven KP, MarshJL. Observations on a recent increase inplagiocephaly without synostosis.Pediatrics. 1996;97(6 pt 1):877–885
5. McKinney CM, Cunningham ML, Holt VL,Leroux B, Starr JR. Characteristics of2733 cases diagnosed withdeformational plagiocephaly and
changes in risk factors over time. CleftPalate Craniofac J. 2008;45(2):208–216
6. Speltz ML, Collett BR, Stott-Miller M,et al. Case-control study ofneurodevelopment in deformationalplagiocephaly. Pediatrics. 2010;125(3).Available at: www.pediatrics.org/cgi/content/full/125/3/e537
7. Miller RI, Clarren SK. Long-termdevelopmental outcomes in patientswith deformational plagiocephaly.
8 COLLETT et al by guest on June 22, 2020www.aappublications.org/newsDownloaded from

Pediatrics. 2000;105(2). Available at:www.pediatrics.org/cgi/content/full/105/2/e26
8. Martiniuk A, Jacob J, Faruqui N, Yu W.Positional plagiocephaly reducesparental adherence to SIDS guidelinesand inundates the health system.Child Care Health Dev. 2016;42(6):941–950
9. Collett BR, Starr JR, Kartin D, et al.Development in toddlers with andwithout deformational plagiocephaly.Arch Pediatr Adolesc Med. 2011;165(7):653–658
10. Collett BR, Gray KE, Starr JR, Heike CL,Cunningham ML, Speltz ML.Development at age 36 months inchildren with deformationalplagiocephaly. Pediatrics. 2013;131(1).Available at: www.pediatrics.org/cgi/content/full/131/1/e109
11. Spermon J, Spermon-Marijnen R,Scholten-Peeters W. Clinicalclassification of deformationalplagiocephaly according to Argenta:
a reliability study. J Craniofac Surg.2008;19(3):664–668
12. Elliott CD. Differential Ability Scales. 2nded. San Antonio, TX: PsychologicalCorporation; 2007
13. Wechsler D. Wechsler IndividualAchievement Test. 3rd ed. San Antonio,TX: Psychological Corporation; 2009
14. Hollingshead AB. Four Factor Index ofSocial Status. New Haven, CT: YaleUniversity; 1975
15. Rothman KJ. Six persistent researchmisconceptions. J Gen Intern Med.2014;29(7):1060–1064
16. Heyting A, Tolboom JTBM, Essers JGA.Statistical handling of drop-outs inlongitudinal clinical trials. Stat Med.1992;11(16):2043–2061
17. Tobin MD, Sheehan NA, Scurrah KJ,Burton PR. Adjusting for treatmenteffects in studies of quantitative traits:antihypertensive therapy and systolicblood pressure. Stat Med. 2005;24(19):2911–2935
18. Bellinger DC. A strategy for comparingthe contributions of environmentalchemicals and other risk factors toneurodevelopment of children.Environ Health Perspect. 2012;120(4):501–507
19. Rice CE, Naarden Braun KV, Kogan MD,et al; Centers for Disease Control andPrevention (CDC). Screening fordevelopmental delays among youngchildren–National Survey of Children’sHealth, United States, 2007. MMWRSuppl. 2014;63(2):27–35
20. Bornstein MH, Hahn CS, Suwalsky JTD.Physically developed and exploratoryyoung infants contribute to their ownlong-term academic achievement.Psychol Sci. 2013;24(10):1906–1917
21. Viholainen H, Ahonen T, Lyytinen P,Cantell M, Tolvanen A, Lyytinen H. Earlymotor development and later languageand reading skills in children at risk offamilial dyslexia. Dev Med Child Neurol.2006;48(5):367–373
PEDIATRICS Volume 143, number 2, February 2019 9 by guest on June 22, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-2373 originally published online January 11, 2019; 2019;143;Pediatrics
Matthew L. SpeltzBrent R. Collett, Erin R. Wallace, Deborah Kartin, Michael L. Cunningham and
Cognitive Outcomes and Positional Plagiocephaly
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/143/2/e20182373including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/143/2/e20182373#BIBLThis article cites 18 articles, 5 of which you can access for free at:
Subspecialty Collections
rning_disorders_subhttp://www.aappublications.org/cgi/collection/cognition:language:leaCognition/Language/Learning Disordersal_issues_subhttp://www.aappublications.org/cgi/collection/development:behaviorDevelopmental/Behavioral Pediatricsfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 22, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2018-2373 originally published online January 11, 2019; 2019;143;Pediatrics
Matthew L. SpeltzBrent R. Collett, Erin R. Wallace, Deborah Kartin, Michael L. Cunningham and
Cognitive Outcomes and Positional Plagiocephaly
http://pediatrics.aappublications.org/content/143/2/e20182373located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2019/01/09/peds.2018-2373.DCSupplementalData Supplement at:
ISSN: 1073-0397. 60007. Copyright © 2019 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on June 22, 2020www.aappublications.org/newsDownloaded from