Coelioscopic surgery in children: the anesthesiologist’s
36
Coelioscopic Coelioscopic surgery surgery in in children children : : the the anesthesiologist’s anesthesiologist’s point point of of view view
Transcript of Coelioscopic surgery in children: the anesthesiologist’s

CoelioscopicCoelioscopic surgerysurgeryin in childrenchildren : :
thethe anesthesiologist’s anesthesiologist’spoint point ofof viewview

PlanPlan
Indications Indications PhysiologicPhysiologic consequencesconsequences AdditionalAdditional riskrisk : CO : CO22 embolismembolism MedicalMedical contraindicationscontraindications AnestheticAnesthetic management management New New crisiscrisis situations situations

IndicationsIndications•• diagnostic : impalpable diagnostic : impalpable testistestis,, contralateralcontralateral herniahernia stagingstaging•• therapeutictherapeutic : :-- appendicectomyappendicectomy, , cholecystectomycholecystectomy,,
splenectomysplenectomy, , fundoplicationfundoplication, , adhesiolysisadhesiolysis-- nephrectomynephrectomy, , pyeloplastypyeloplasty, , adrenalectomyadrenalectomy-- pyloricpyloric stenosisstenosis, , pull-throughpull-through-- ductusductus arteriosusarteriosus, , TOFistulaTOFistula … …

CoelioscopicCoelioscopic vsvs open open surgerysurgery+ + :: lessless postoperativepostoperative pain ? pain ? betterbetter cosmeticcosmetic resultresult quickerquicker functionalfunctional recoveryrecovery shortershorter hospitalhospital staystay-- :: increasedincreased costcost : : equipmentequipment,,disposablesdisposables unfamiliarunfamiliar physiologicphysiologic consequencesconsequences new new anestheticanesthetic crisiscrisis situations situations

PhysiologicPhysiologic consequencesconsequencesmodelmodel : : laparoscopylaparoscopy = insufflation = insufflation intointo peritonealperitoneal cavitycavity increasedincreased intraabdominalintraabdominal pressure pressure absorption absorption ofof exogenousexogenous CO CO22 + + positioningpositioning ofof thethe childchild
retroperitonealretroperitoneal intrathoracicintrathoracic intravesicalintravesical

IncreasedIncreased IAP IAP
respiratoryrespiratory mechanicsmechanics1) 1) cephaladcephalad shift shift ofof diaphragmdiaphragm thoracicthoracic compliancecompliance functionalfunctional residualresidual capacitycapacity airwayairway resistanceresistance2) 2) peakpeak inspiratoryinspiratory pressure pressure leakleak andand VtVt if if uncuffeduncuffed tube tube P PETETCOCO2 2 && PaCO PaCO22 –– P PETETCOCO22

PigPig: insufflation : insufflation upup to to 10 10 mmHgmmHg IAP IAP withwith CO CO22 or or HeHe
13.0 13.0 ±± 2 24.8 4.8 ±± 1 112.5 12.5 ±± 1 15.2 5.2 ±± 1 1pIVCpIVC
6.7 6.7 ±±1.51.52.7 2.7 ±±1.51.54.7 4.7 ±± 1.5 1.53.0 3.0 ±± 1.7 1.7RAPRAP
36.8 36.8 ±± 3 327.8 27.8 ±± 5 547.2 47.2 ±± 5 529.0 29.0 ±± 2 2PPETETCOCO22
43.5 43.5 ±± 4 432.8 32.8 ±± 1 157.9 57.9 ±± 6 635.0 35.0 ±± 1 1paCOpaCO22
212 212 ±± 21 21266 266 ±± 30 30189 189 ±± 33 33261 261 ±± 49 49paOpaO22
HeHe 10 10 HeHe base baseCOCO22 1010COCO2 2 basebase

IncreasedIncreased IAP IAP hemodynamicshemodynamics : :
-- IAP < RAP (6 IAP < RAP (6 mmHgmmHg) : ) : venousvenous return return CO CO-- IAP > RAP (12 IAP > RAP (12 mmHgmmHg): ): venousvenous return return CO CO-- systemicsystemic resistanceresistance ( (vasopressinvasopressin, , NepiNepi))-- falselyfalsely elevatedelevated CVP CVP hypovolemiahypovolemia ! !

IncreasedIncreased IAP IAP
fluidfluid balance balance - - lessless sensible & insensible sensible & insensible losseslosses ? ?
splanchnicsplanchnic organsorgans - - renalrenal & & splanchnicsplanchnic bloodblood flowflow urine output urine output - - or or flowflow in portal in portal veinvein hepatichepatic arterialarterial bufferbuffer responseresponse ? ?

AdultAdult: portal : portal veinvein flowflow vsvs IAP IAP

IncreasedIncreased IAP IAP intracranialintracranial pressure pressure
- - cerebralcerebral bloodblood volume & volume & velocityvelocity - - reducedreduced venousvenous drainage drainage - - reducedreduced outflowoutflow fromfrom VP shunt ? VP shunt ? checkcheck freefree flowflow ofof CSF CSF monitoring monitoring ofof ICP ? ICP ? e.g.e.g., , transcranialtranscranial doppler doppler postoperativepostoperative clinicalclinical monitoring monitoring

Absorption Absorption ofof CO CO22
1) varies 1) varies withwith intraabdominalintraabdominal pressure : pressure : in in thethe pigpig modelmodel ((AnesthesiologyAnesthesiology 1994; 80: 129-36) 1994; 80: 129-36)
* if < 10 * if < 10 mmHgmmHg : absorption : absorption ofof CO CO22 withwith insufflation pressure ( insufflation pressure (recruitmentrecruitment))** if > 10 if > 10 mmHgmmHg : : absorption absorption ofof CO CO22 stable stable but but increasedincreased deadspacedeadspace ventilation ventilation ( ( PaCOPaCO22))

ExcretionExcretion ofof CO CO22 vs IAP vs IAP

paCOpaCO22 vs IAP ( vs IAP (pigletpiglet !) !)

Absorption Absorption ofof CO CO22
2) 2) effectseffects ofof hypercarbiahypercarbia : :•• systemicsystemic : : sympatheticsympathetic tonetone vasoconstriction, vasoconstriction, increasedincreased BP BP•• regionalregional : : vasodilationvasodilation e.g.e.g., , mesentericmesenteric vesselsvessels partial compensation partial compensation ofof portal portal flowflow ? ?

Absorption Absorption ofof CO CO22
3) portal hypertension :3) portal hypertension : absorption absorption ofof CO CO22
4)4) a large a large amountamount ofof absorbedabsorbed CO CO22 isisbufferedbuffered in in bonebone, muscles , muscles andand tissues tissuesandand eliminatedeliminated throughthrough thethe lungslungs afterafterthethe procedureprocedure
if if poorpoor respiratoryrespiratory functionfunction

RetroperitonealRetroperitoneal insufflation insufflation+ + ** nono increaseincrease in P in PETETCOCO2 2 inin childrenchildren * * nono increaseincrease in in airwayairway pressures pressures
-- * * ventilatoryventilatory effectseffects ofof position position * * increasedincreased riskrisk ofof subcutaneoussubcutaneous diffusion to pleura, diffusion to pleura, mediastinummediastinum… ?… ? * * increasedincreased absorption absorption ofof CO CO22 ? ? ( (adultsadults >< >< childrenchildren?)?)

ThoracoscopyThoracoscopy
usuallyusually : : one-lung-ventilationone-lung-ventilation bronchial bronchial blockerblocker
if if nono OLV : OLV : lowlow insufflation pressure insufflation pressure pleural absorption pleural absorption ofof CO CO22

VesicalVesical insufflation insufflation
* to correct * to correct vesico-ureteralvesico-ureteral reflux reflux
* * stillstill experimentalexperimental
* absorption * absorption ofof CO CO22 ? ?* * riskrisk ofof embolismembolism ? ?

GaslessGasless laparoscopylaparoscopy

Child’s positionChild’s position
head-downhead-down : : respiratoryrespiratory effectseffects ofof increasedincreased IAP IAP
head-uphead-up:: hemodynamichemodynamic effectseffects ofof increasedincreased IAP IAP
laterallateral decubitusdecubitus : : V/Q V/Q mismatchmismatch proneprone: : COCO
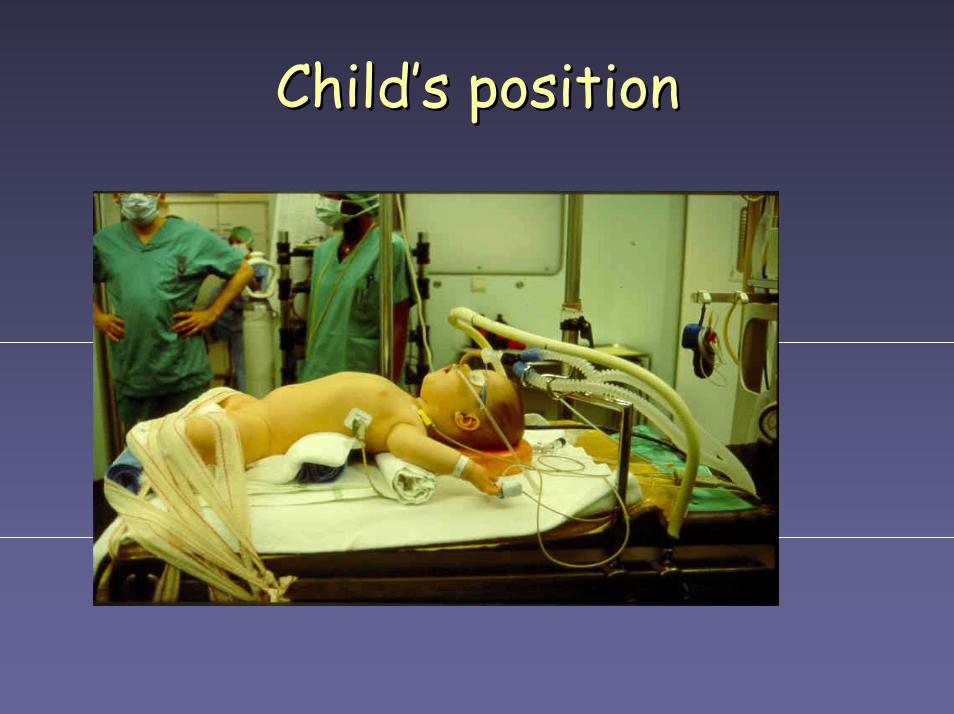
Child’s positionChild’s position
COCO22 embolisationembolisation
probablyprobably frequentfrequent but but nono clinicalclinical signssigns
pigletpiglet modelmodel ofof 0.6L/min 0.6L/min iviv CO CO22 : : mortalitymortality withwith insufflation pressure insufflation pressure 0% if 5 0% if 5 mmHgmmHg 50% if 15 50% if 15 mmHgmmHg

COCO22 embolisationembolisation
« « drivingdriving pressure » pressure » = = IApressureIApressure – – intravascularintravascular pressure pressure IAP > IVIAP > IV : : vesselvessel collapse collapse IAP < IV :IAP < IV : bleedingbleeding IAP IAP ≅≅ IV : IV : bubblesbubbles cancan enter enter vesselvessel cancan remainremain trappedtrapped embolismembolism atat exsufflation !! exsufflation !!

MedicalMedical contraindicationscontraindications•• severesevere cardiaccardiac diseasedisease - - physiologicphysiologic effectseffects on CO on CO - - paradoxicalparadoxical embolismembolism throughthrough shunt shunt•• severesevere pulmonarypulmonary diseasedisease - - increasedincreased CO CO22 loadload•• reducedreduced intracranialintracranial compliancecompliance•• liverliver diseasedisease ? ?•• historyhistory ofof spontaneousspontaneous pneumothorax pneumothorax•• acute trauma : acute trauma : volemiavolemia, , vesselvessel damage damage

PreoperativePreoperative evaluationevaluation
•• samesame as for as for anyany pediatricpediatric patient patient Cave : Cave : cholecystetomycholecystetomy & & HbHb SS SS•• PremedicationPremedication : : - - accordingaccording to age, to age, emotionalemotional statusstatus,, local habits … local habits … - atropine for - atropine for preventionprevention ofof vasovagalvasovagal reflex reflex atat insufflation ? insufflation ?

MonitoringMonitoring
usualusual : ECG, NIBP, SpO : ECG, NIBP, SpO22, P, PETETCOCO22
airwayairway pressures, pressures, compliancecompliance
PaCOPaCO22 - P - PETETCOCO22 : varies : varies duringduring procedureprocedure cancan becomebecome negativenegative ! ! P PTCTCCOCO2 2 ??
fragile patient: fragile patient: TEEchocardigraphyTEEchocardigraphy

Minimal invasive Minimal invasive surgerysurgery cancan meanmeanminimal minimal accessaccess anesthesiaanesthesia ! !

AnestheticAnesthetic management management cuffedcuffed ETtubeETtube gastricgastric emptyingemptying venousvenous accessaccess in in upperupper limblimb controlledcontrolled ventilation ventilation IV IV fluidsfluids : ? : ? volume volume loadingloading priorprior to insufflation? to insufflation? slow slow andand progressive progressive tiltingtilting ! ! preventionprevention ofof hypothermiahypothermia

AnestheticAnesthetic management management monitoring monitoring ofof insufflation pressure insufflation pressure ! !
- - itit shouldshould bebe keptkept as as lowlow as possible as possible additionnaladditionnal intracavitaryintracavitary pressure if pressure if a a gasgas coagulatorcoagulator isis usedused e.g.e.g.: Argon : Argon beambeam = 4L/min ! = 4L/min !
NN22O ?O ? cancan support combustion if support combustion ifintestinal perforationintestinal perforation muscle relaxation ?muscle relaxation ?

VideohypnosisVideohypnosis

UnusualUnusual crisiscrisis situations situations
CO CO22 or or coagulatorcoagulator gasgas embolismembolism bronchial intubation bronchial intubation pneumothorax (« pneumothorax (« capnothoraxcapnothorax ») ») subcutaneoussubcutaneous emphysemaemphysema hemorrhagehemorrhage

« « CapnothoraxCapnothorax » »

DifferentialDifferential diagnosisdiagnosis
capnothoraxcapnothorax PPETETCOCO2 2 PawPaw SpO SpO22
subcutaneoussubcutaneous emphysemaemphysema P PETETCOCO2 2 PawPaw SpOSpO22
endobronchialendobronchial intubation intubation PPETETCOCO2 2 PawPaw SpO SpO22

PostoperativePostoperative care care Pain : Pain :
- exsufflation - exsufflation ofof CO CO22 - infiltration - infiltration ofof trocartrocar ports ports withwith LA LA - - NSAID’sNSAID’s for for shouldershoulder pain pain - IV - IV opioidsopioids or or locoregionallocoregional blockadeblockade
Vital Vital signssigns : : - - breathingbreathing : : accumulatedaccumulated CO CO22 loadload ! ! - vital - vital signssigns : : delayeddelayed hemorrhagehemorrhage ? ?

ConclusionConclusion
betterbetter understandingunderstanding ofof physiologicphysiologicconsequencesconsequences ofof CO CO22 insufflation in insufflation ininfants infants andand childrenchildren
reliablereliable non-invasivenon-invasive monitoring monitoring
betterbetter postoperativepostoperative pain pain treatmenttreatment