
CODE BURNCODE BURN CODE BURN.pdf · Julie-Ann Airth RN, BA Mafalda Concordia, RN ... o Heals:...
31
CODE BURN CODE BURN The First 48 Hours The First 48 Hours By By Julie-Ann Airth RN, BA Mafalda Concordia, RN Donna Wood, RRT, BSc. Hon J li K i ht RN MS N Julie Knighton, RN, MScN Karen Smith, RN, MHS Rimona Natanson, pharmacist Melissa Adamson, RN, BScN Anita Au RN MN CNCC(C) Anita, Au, RN, MN, CNCC(C) Ross Tilley Burn Center Sunnybrook Health Sciences
Transcript of CODE BURNCODE BURN CODE BURN.pdf · Julie-Ann Airth RN, BA Mafalda Concordia, RN ... o Heals:...
CODE BURNCODE BURNThe First 48 HoursThe First 48 Hours
ByBy
Julie-Ann Airth RN, BAMafalda Concordia, RN
Donna Wood, RRT, BSc. HonJ li K i ht RN MS NJulie Knighton, RN, MScN
Karen Smith, RN, MHSRimona Natanson, pharmacistMelissa Adamson, RN, BScNAnita Au RN MN CNCC(C)Anita, Au, RN, MN, CNCC(C)
Ross Tilley Burn CenterSunnybrook Health Sciences

Objectives: 48 hours Post InjuryObjectives: 48 hours Post Injury
oo Nurse to ADVOCATE Nurse to ADVOCATE for the burn patientso Shatter the Silence
o Aims:
A case review
Current standard of careCurrent standard of care
2
O tliOutline1. Case Scenario
2. What to doA t Assessment
o Primary Survey (ABC)o Secondary Survey (Burn)
Interventionso Fluid Resuscitationo Fluid Resuscitation
o Dressing the Burn
3 Transfer3
3. Transfer

Case ScenarioCase Scenario55♂ presents to emergency room after a ball of flames erupted while
attempting to light his barbeque with lighter fluidattempting to light his barbeque with lighter fluid
4

Case ScenarioCase Scenario
INJURY b t th f tINJURY: burns to the face, upper torso, bilateral arms and left upper leg
5

Primary SurveyPrimary Survey
o COMMON: Use ABCDE approach as with any new trauma A: airway B: breathing C: circulation D di bilit D: disability E: exposure
Id tif d t li h i l th l l t i l to Identify and neutralize any chemical, thermal, or electrical agents which might pose a threat to health care team
6

Airway and BreathingAirway and Breathing
o Evaluate upper airway for patency
Inhalational injury
Stridor or dysphagia
Airway compromise Airway compromise
7

Airway and Breathingo Evaluate lower airway for comprise
Inhalational injury: increase in secretions, bronchospasm, or
Airway and Breathing
j y , p ,pulmonary edema
o History of injury reveals special considerations Enclosed vs. open space Risk factor for carbon monoxide poisoning
8 10/5/2013
Airway and BreathingAirway and Breathingo Intubation
Place largest possible uncut ETT
9
Airway and BreathingAirway and Breathingo Airway monitoring and work up
Monitor: breathing and chest wall expansion Comorbidities Carboxyhemoglobiny g ABG
10
CirculationCirculationo Prepare for extensive fluid resuscitation
2 large PIVs 2 large PIVs Central line
o Check all extremities for pulses
o Elevate! Elevate! Elevate!o Elevate! Elevate! Elevate!
o Check for circumferential burns Risk: compartment syndrome May require escharotomy
11
o BP cuff readings may be unreliable Consider arterial line

Secondary Survey: Assess the Burn
o Degree of the Burn
o The Total Body Surface Area (TBSA) affected
12

First Degree/Superficial g po Layer: the epidermiso Look: SUNBURNo Feel: Painfulo Heals: 2-7dayso NOT calculated in totalo NOT calculated in total
burn surface area
13

Second Degree - Partial Thickness go Layer: epidermis into upper dermiso Look:
• Blister/BullaeBlister/Bullae• Bright red/mottled, moist and
weepingo Feel: extremely painfulo Feel: extremely painfulo Healing: 4-6 weeks
14

Second Degree - Deep Dermal g po Layers: epidermis into the dermiso Look: Red with patchy white/yellow
area, and typically dry(usually no blister)
o Feel: Painfulo Heal: up 6 weekso Heal: up 6 weeks
15

Third Degree-Full thickness go Layers: Allo Look: Pale white, charred, red or brown,
leathery appearanceo Surface dry o Unblanchable
o Feel: Painless and insensitive o Heal: surgical excision and debridement
Really no pain?
16

Total Body Surface Area (TBSA)Total Body Surface Area (TBSA)o an estimate of the extent of burns which are at least 2nd degree or
greatergreaterPalm only, no finger!
17

Fluid Resuscitationo Parkland Formula in the first 24 hours post injury (ABLS consensus
Guidelines, 2011)
o Fluid: Ringer’s Lactateo 2-4mL x body weight (kg) x %TBSA
50% l l t d t 1 t 8 h t i j
RATE OF ADMINISTRATION(2 X kg X %burn) [2nd & 3rd Burn added together]
o50% calculated amount 1st 8 hours post injury
o25% second 8 hourstogether]
First 8 hours ½
o25% third 8 hours
½Second8 hours
1/4
Third8 hours
1/4
18
1/4 1/4

Case Scenario Part 2
o Audience to apply: TALK TO MY HAND!
Case Sce a o a t
pp y Face Anterior upper torso Both anterior upper limbs Both anterior upper limbs Anterior left upper leg
o Apply the formula RATE OF ADMINISTRATIONpp yo Total TBSA: 40.5%o Weight: 70kg
RATE OF ADMINISTRATION(2 X kg X %burn) [2nd & 3rd Burn added together]
o Fluid required in first 8 hrs: (2mL x 70kg x 40.5%)/2
First 8 hours ½
Second Third
19
= 2.84L in 8 hours= 354cc/hr
8 hours1/4
8 hours1/4
Monitoring the ResuscitationMonitoring the Resuscitation
o Guide Fluid Resuscitation: insert a urinary catheter
o Urine output targetsoo Adult Thermal and Chemical burns: 30Adult Thermal and Chemical burns: 30 -- 50 ml urine/hour50 ml urine/houroo Adult Thermal and Chemical burns: 30 Adult Thermal and Chemical burns: 30 -- 50 ml urine/hour50 ml urine/houro Adult High Voltage Electrical burns: 75 - 100 ml urine/hour
20
Fluid Shift and EdemaFluid Shift and Edema
• Fluid shift and edema formation peaks 24-48hrs post injury
• Fluid mobilization (18-36hrs post injury)
• Fluid resuscitation– General/Localized edema – 20% weight gain from retained resuscitation fluid g g– Interstitial fluid volume may lead to an in compartment pressures
– Pay close attention to circumferential burns and regularly assess CSM and pulsePay close attention to circumferential burns and regularly assess CSM and pulse
21

Analgesia in Burns
o Assess
Analgesia in BurnsUNIVERSAL: inadequate pain treament
o Assess Visual Analogue Scale Numeric Rating Scale Critical Care Pain Observation Tool Critical Care Pain Observation Tool
oNon-PharmacologicDistractionDistractionGuided ImageryRelaxation Virtual Reality
oPharmacologic Opioid analgesicsAdj t
22
Adjuncts
Dressing The Burn: COMPLICATED?Dressing The Burn: COMPLICATED?
o 1. Clean
o 2. Debride nonviable sloughing tissue.
o 3.Dress Silver Sulfadiazine-topical antimicrobial agent
4 Wo 4.Wrap wrap the affected area with NS wet to dry gauze and secure with kling. Wrapping distal to proxmial
23 October 5, 2013

Dressing The Burn: SIMPLEDressing The Burn: SIMPLE
oo CleanClean Clean wound with warm Normal Saline
oo Normal Saline Soaked Normal Saline Soaked Wet to dry dressing
24 October 5, 2013
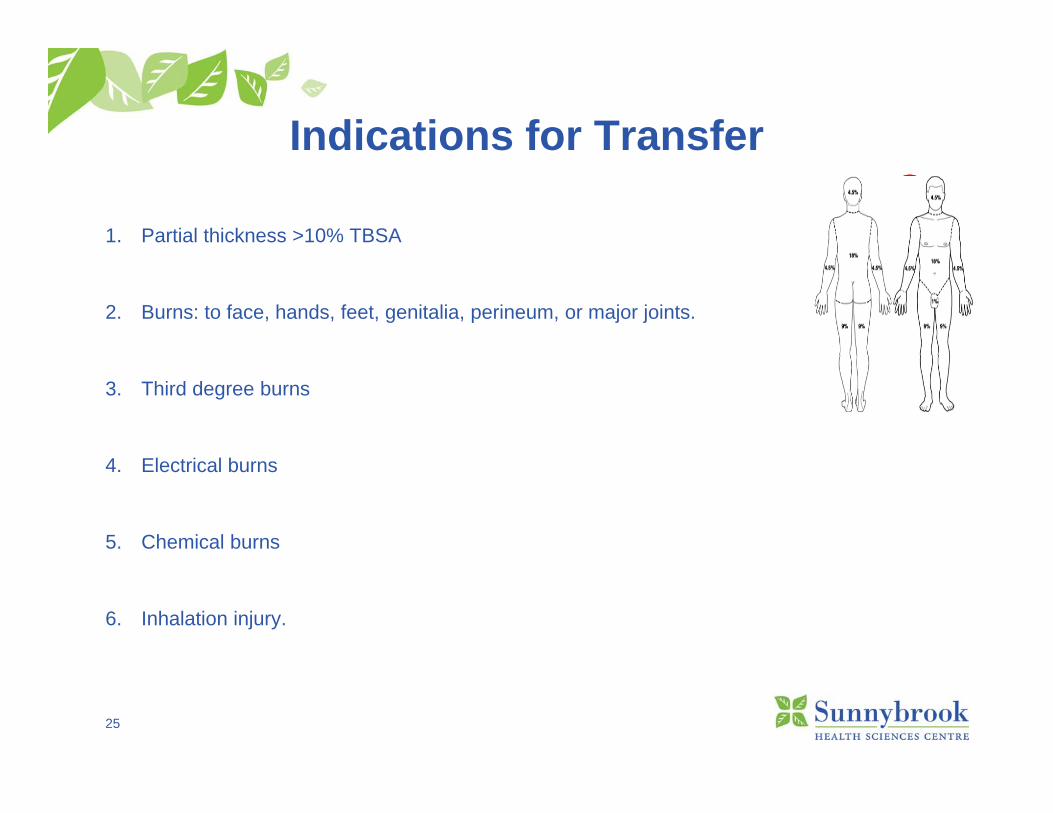
Indications for Transferd cat o s o a s e
1. Partial thickness >10% TBSA
2. Burns: to face, hands, feet, genitalia, perineum, or major joints.
3. Third degree burns
4 El i l b4. Electrical burns
5. Chemical burns
6. Inhalation injury.
25
Indications for Transfer (cont’d)Indications for Transfer (cont d)7. Pre-existing medical disorders that complicates management
8. Burn & Trauma (such as fractures)
9. Burned children in hospitals WITHOUT qualified personnel/equipment
10. Burn patients requiring social, emotional, or rehabilitative intervention.
26 Handout available!!!Handout available!!!

Case ScenarioCase Scenario
55♂ presents to emergency room after a ball of flames erupted p g y pwhile attempting to light his barbeque with lighter fluid
INJURY: burns to the face, upper torso, bilateral arms and left upper leg
27

Case Scenario Part 3Case Scenario Part 3INJURY: burns to the face, upper torso, bilateral arms and left upper leg
GOAL: Stabilize, Monitor and Dress
Airway
What do we need to do or assess?Intubate
Breathing
Circulation (and lines)
Pulse check q1h (U/S doppler)Lines(Arterial and CVL/PIV’s)VS q1htemp. q4h
Fluid
Dressing
Fluid:Parkland formulaU/O q1hCVP q1h
Dress: NS soaked wet to dryOthers
Dress: NS soaked wet to drypain control
OtherBladder pressures q4hNG/OG/Post-pyloric
28
Transfer
10/5/2013
Bloodwork: lactate, carboxyhemaglobin, and ABG
Arrangement for transport to burn unit
AchievementAchievementCare of burn patients prior to transfer to the Burn Centre
Main Goal
• Quick Review/Sharing our knowledge with our fellow colleagues
• Break the barrier between Critical Care and “Burn Care”• Break the barrier between Critical Care and Burn Care
• Always available, CALL
29 10/5/2013

QUESTIONS?QUESTIONS?
30 10/5/2013
Referencese e e ces
1. ABLS 2011 Provider Manual Ch. 9 Stabilization, Transfer and Transport. P. 97-103.2 B D C t htt // h lth lb t /h lth/P / diti ?h id b A d2. Burn Degree Cartoons. https://myhealth.alberta.ca/health/Pages/conditions.aspx?hwid=burns. Accessed
June 11, 2013.3. Cartotto, R. (2009). Fluid Resuscitation of the Thermally Injured Patient. Journal of Clinical Plastic Surgery
36. p. 569-5814 Connor Ballard P (2009) Understanding and managing burn pain: Part I American Journal of Nursing4.Connor-Ballard, P. (2009). Understanding and managing burn pain: Part I. American Journal of Nursing,
109(4), p. 48-56. 5. Herndon, D. (2007). Total Burn Care. Philadelphia, Elsevier Saunders.Latenser, B (2009). Critical care of the burn patient: The first 48 hours. Critical Care Medicine, 37(10),
2819-2826.6. Oliver, R., del la Torre, J. (2012). Burn resuscitation and early management.
http://emedicine.medscape.com/ article/1277360-overview7. Urder, L., Stacy. K, & Lough, M. (2010). Critical Care Nursing: Diagnosis and Mangagement. Chapter 41:
Burns. Elsevier, St. Louis, Missouri.
31 10/5/2013












![[PPT]Emergency Care of Burn Injuries - Home | UW Health ... · Web viewInitial Care of Burns Connie Handel RN University of Wisconsin Hospital and Clinics * * * * * * * * * * Burn](https://static.fdocuments.in/doc/165x107/5b1d78e07f8b9af05b8c16c5/pptemergency-care-of-burn-injuries-home-uw-health-web-viewinitial.jpg)




