Coagulation Final

of 70
-
Upload
abhyuday-kumar -
Category
Documents
-
view
236 -
download
0
Transcript of Coagulation Final
-
7/30/2019 Coagulation Final
1/70
HEMOSTASIS
& ANTICOAGULATION
-
7/30/2019 Coagulation Final
2/70
Components of blood clotting1) Intact Endothelial Cells
Inhibit blood clotting by antiplatelet, anticoagulant andprofibrolytic effects.
Negatively charged vascular endothelium repel platelets and
produce prostacycline and NO which are potent plateletinhibitors. Vascular endothelium further expresses several inhibitors of
plasma-mediated hemostasis, including thrombomodulin (anindirect thrombin inhibitor), heparin-like glycosaminoglycans, andtissue factor pathway inhibitor (TFPI).
Vascular endothelium synthesizes tissue plasminogen activator (t-PA), which is responsible for activating fibrinolysis
Store von Willebrand factor in cytop. granules. Make prostacyclin ~ inhibits platelet aggregation
-
7/30/2019 Coagulation Final
3/70
2) Subendothelial Cells
Contain membrane prots and extracellularmatrix prots (collagen) that normally do notcontact blood
When exposed after injury, platelets aggregateat the site by mediation of von Willebrand factor(vWF) that binds to both platelet receptors andcollagen/subendo cells
-
7/30/2019 Coagulation Final
4/70
3) Platelets After injury to vascular endothelium platelets undergo alterations
characterised by three phases.a) Adhesion - Exposure of subendothelial matrix proteins (i.e.,
collagen, vWF, fibronectin) allows for platelet adhesion to thevascular wall. Deficiency of either vWF (von Willebrand disease) orglycoprotein Ib/factor IX/factor V receptors (Bernard-Soulier
syndrome) results in a clinically significant bleeding disorder.b) Activation- platelets release granular contents (alpha bodies &
dense granules), resulting in recruitment and activation of additional platelets as well as propagation of plasma-mediatedcoagulation.
c) Aggregation- Newly active glycoprotein IIb/IIIa receptors on theplatelet surface bind fibrinogen to provide for cross-linking withadjacent platelets (platelet aggregation). Bleeding disorderassociated with hereditary deficiency these receptors: Glanzmann
thrombasthenia.
-
7/30/2019 Coagulation Final
5/70
Cell surface glycoprotein receptors on platelets
that mediate hemostatic response GPIb receptor von Willebrand Factor
GPIa/IIa or GPIV receptors collagen GPIc/IIa laminin or fibronectin GPIV receptor thrombospondin
GPIIb/IIIa receptor - fibrinogen
-
7/30/2019 Coagulation Final
6/70
4) Clotting Factors Soluble plasma proteins
Mostly made in liver
Most are serine proteases and circulate as zymogens(inactive precursors)
Cascade in which clotting factors are activated by selective
proteolytic cleavage must have an enzyme (activatedcoagulation factor), substrate (inactive precursorzymogen), cofactor (accelerator/ catalyst), and calcium.
-
7/30/2019 Coagulation Final
7/70
CLOTTING FACTORS
I Fibrinogen
II Prothrombin
III Platelet Factor 3
IV Calcium ionV Pro accelerin , Labile factor
VII Pro convertin . Stable factor
VIII Anti Haemophilic A
IX Anti Haemophilic B , Christmas factorX Stuart Power factor
XI Anti Haemophilic C
XII Hageman factor
XIII Fibrin Stabilizing factor
-
7/30/2019 Coagulation Final
8/70
Blood Vessel Injury
IX IXa
XI XIa
X Xa
XII XIIa
Tissue Injury
Tissue Factor
Thromboplastin
VIIa VII
X
Prothrombin Thrombin
Fibrinogen Fribrin monomer
Fibrin polymerXIII
Intrinsic Pathway Extrinsic Pathway
-
7/30/2019 Coagulation Final
9/70
-
7/30/2019 Coagulation Final
10/70
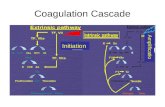
Coagulation cascade has 2 steps1) Initiation
2) Propagation Initiation Phase :
TF VIIa small amount X to Xa small amount II to IIaIf II a not neutralized by Antithrombin 3 then triggerspropogation phase.
Propogation Phase :IIa ramps up its own formation by activating platelets andfactors (FV, FVIII), setting the stage for formation of the FVIIIa IXa complex.Formation of this FVIIIa IXa complex allows FXa generation toswitch from a TF-VIIa complex catalyzed reaction to oneproduced by the intrinsic Xase pathway.
-
7/30/2019 Coagulation Final
11/70
The intrinsic Xase complex exhibiting 50-fold higherefficiency at Xa generation.Hemophilia is characterised by intact initiation phase andabsent propagation phase.The intrinsic or contact pathway of coagulation has no role inthe earliest clotting events.The commonly used laboratory tests of soluble coagulationonly measure the kinetics of the initiation phase. Theprothrombin time (PT) and activated partial thromboplastintime (aPTT) both have as endpoints the first appearance of
fibrin gel, which occurs after completion of less than 5% of the total reaction.
-
7/30/2019 Coagulation Final
12/70
Antithrombotic mechanisms
Antiplatelet effects : Intact endothelium- prevent platelet adhetion. Prostacyclin (PGI 2) and nitric oxide Inhibits adhetion & aggregation.
Anticoagulant effects : Heparin-like molecules - Activates antithrombin 3. Antithrombin is a serine protease inhibitor (serpin ) that degrades the serine
proteases: thrombin , FIXa, FXa, FXIa, and FXIIa. Protein C - inhibits clotting by inactivating factors Va and VIIIa. Protein S - a co-factor for protein C. Thrombomodulin Activates protein C. Tissue factor pathway inhibitor (TFPI)- a cell surface protein that directly
inhibits tissue factor factor VIIa and factor Xa activities.
Fibrinolytic effects : Plasminogen activator ( t-PA ) - a protease that cleaves plasminogen to form
plasmin; plasmin, in turn, cleaves fibrin to degrade thrombi .
http://en.wikipedia.org/wiki/Antithrombinhttp://en.wikipedia.org/wiki/Serine_protease_inhibitorhttp://en.wikipedia.org/wiki/Serpinhttp://en.wikipedia.org/wiki/Serpinhttp://en.wikipedia.org/wiki/Serine_protease_inhibitorhttp://en.wikipedia.org/wiki/Antithrombin -
7/30/2019 Coagulation Final
13/70
Prothrombotic mechanism
Platelet effects : von Willebrand factor (vWF) - essential cofactor for platelet
binding to matrix elements.
Procoagulant effects : tissue factor- expressed by fibroblast in ECM & is produced in
response to cytokines (e.g., tumor necrosis factor [TNF] orinterleukin-1 [IL-1]) or bacterial endotoxin and major contributorin extrinsic pathway.
Antifibrinolytic effects : Endothelial cells secrete inhibitors of plasminogen activator
(PAIs), which limit fibrinolysis and tend to favor thrombosis.
-
7/30/2019 Coagulation Final
14/70
Testing of coagulation Blood plasma after the addition of Tissue Factor forms a
gel-like structure (Test for prothrombin time). Numerous tests are used to assess the function of the
coagulation system: Common: aPTT, PT (also used to determine INR),
fibrinogen testing (often by the Clauss m ethod ), platelet
count, platelet function testing (often by PFA-100 ). Other: TCT, bleeding time , mixing test (whether an
abnormality corrects if the patient's plasma is mixed withnormal plasma), coagulatio n factor assays,antiphosholipid antibodies , D-dimer , genetic tests (e.g.
factor V Leiden , prothromb in mutation G20210A), diluteRussell's viper venom t ime (dRVVT), miscella neousplatelet fu nction tests, thrombo elastography (TEG orSonoclot), euglobulin lysis time (ELT).
http://en.wikipedia.org/wiki/Fibrinogenhttp://en.wikipedia.org/wiki/Partial_thromboplastin_timehttp://en.wikipedia.org/wiki/Prothrombin_timehttp://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/wiki/Platelethttp://en.wikipedia.org/wiki/Fibrinogenhttp://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/wiki/PFA-100http://en.wikipedia.org/wiki/PFA-100http://en.wikipedia.org/wiki/PFA-100http://en.wikipedia.org/wiki/Platelethttp://en.wikipedia.org/wiki/PFA-100http://en.wikipedia.org/wiki/Thrombin_clotting_timehttp://en.wikipedia.org/wiki/Bleeding_timehttp://en.wikipedia.org/wiki/Mixing_testhttp://en.wikipedia.org/wiki/Antiphospholipid_antibodyhttp://en.wikipedia.org/wiki/D-dimerhttp://en.wikipedia.org/wiki/Factor_V_Leidenhttp://en.wikipedia.org/wiki/Antiphospholipid_antibodyhttp://en.wikipedia.org/wiki/Prothrombinhttp://en.wikipedia.org/wiki/Prothrombinhttp://en.wikipedia.org/wiki/Prothrombinhttp://en.wikipedia.org/wiki/D-dimerhttp://en.wikipedia.org/wiki/Dilute_Russell's_viper_venom_timehttp://en.wikipedia.org/wiki/Dilute_Russell's_viper_venom_timehttp://en.wikipedia.org/wiki/Dilute_Russell's_viper_venom_timehttp://en.wikipedia.org/wiki/Dilute_Russell's_viper_venom_timehttp://en.wikipedia.org/wiki/Prothrombinhttp://en.wikipedia.org/wiki/Dilute_Russell's_viper_venom_timehttp://en.wikipedia.org/wiki/Dilute_Russell's_viper_venom_timehttp://en.wikipedia.org/wiki/Thromboelastographyhttp://en.wikipedia.org/wiki/Thromboelastographyhttp://en.wikipedia.org/wiki/Euglobulin_lysis_timehttp://en.wikipedia.org/wiki/Euglobulin_lysis_timehttp://en.wikipedia.org/wiki/Thromboelastographyhttp://en.wikipedia.org/wiki/Euglobulin_lysis_timehttp://en.wikipedia.org/wiki/Euglobulin_lysis_timehttp://en.wikipedia.org/wiki/Euglobulin_lysis_timehttp://en.wikipedia.org/wiki/Euglobulin_lysis_timehttp://en.wikipedia.org/wiki/Euglobulin_lysis_timehttp://en.wikipedia.org/wiki/Euglobulin_lysis_timehttp://en.wikipedia.org/wiki/Thromboelastographyhttp://en.wikipedia.org/wiki/Dilute_Russell's_viper_venom_timehttp://en.wikipedia.org/wiki/Dilute_Russell's_viper_venom_timehttp://en.wikipedia.org/wiki/Prothrombinhttp://en.wikipedia.org/wiki/Factor_V_Leidenhttp://en.wikipedia.org/wiki/D-dimerhttp://en.wikipedia.org/wiki/D-dimerhttp://en.wikipedia.org/wiki/D-dimerhttp://en.wikipedia.org/wiki/Antiphospholipid_antibodyhttp://en.wikipedia.org/wiki/Antiphospholipid_antibodyhttp://en.wikipedia.org/wiki/Antiphospholipid_antibodyhttp://en.wikipedia.org/wiki/Mixing_testhttp://en.wikipedia.org/wiki/Bleeding_timehttp://en.wikipedia.org/wiki/Thrombin_clotting_timehttp://en.wikipedia.org/wiki/PFA-100http://en.wikipedia.org/wiki/PFA-100http://en.wikipedia.org/wiki/PFA-100http://en.wikipedia.org/wiki/Platelethttp://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/wiki/Fibrinogenhttp://en.wikipedia.org/wiki/International_normalized_ratiohttp://en.wikipedia.org/wiki/Prothrombin_timehttp://en.wikipedia.org/wiki/Partial_thromboplastin_time -
7/30/2019 Coagulation Final
15/70
The contact activation (intrinsic) pathway is initiated by
activation of the "contact factors" of plasma, and can bemeasured by the activated partial thromboplastin time (aPTT)test.
The tissue fa ctor (extrinsic) pathway is initiated by release of tissue factor (a sp ecific cellular lipo protein), and can bemeasured by the prothr om bin time (PT) test. PT results areoften reported as ratio (INR value) to monitor dosing of oralanticoagulants such as warfarin .
The quantitative and qualitative screeni ng of fibrinogen ismeasured by the thrombin clotting time (TCT). Measurementof the exact amount of fi brinogen prese nt in the blood isgenerally done using the Clauss method for fibrinogen testing.Many analysers are capable of measuring a "derivedfibrinogen" level from the graph of the Prothrombin time clot.
Deficiencies of fibrinogen (quantitative or qualitative) willaffect all screening tests.
http://en.wikipedia.org/wiki/Partial_thromboplastin_timehttp://en.wikipedia.org/wiki/Partial_thromboplastin_timehttp://en.wikipedia.org/wiki/Tissue_factorhttp://en.wikipedia.org/wiki/Tissue_factorhttp://en.wikipedia.org/wiki/Prothrombin_timehttp://en.wikipedia.org/wiki/Prothrombin_timehttp://en.wikipedia.org/wiki/International_normalized_ratiohttp://en.wikipedia.org/wiki/Prothrombin_timehttp://en.wikipedia.org/wiki/Warfarinhttp://en.wikipedia.org/wiki/Warfarinhttp://en.wikipedia.org/wiki/Warfarinhttp://en.wikipedia.org/wiki/Warfarinhttp://en.wikipedia.org/wiki/Thrombin_clotting_timehttp://en.wikipedia.org/wiki/Thrombin_clotting_timehttp://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Clauss_method&action=edit&redlink=1http://en.wikipedia.org/wiki/Thrombin_clotting_timehttp://en.wikipedia.org/wiki/Warfarinhttp://en.wikipedia.org/wiki/International_normalized_ratiohttp://en.wikipedia.org/wiki/Prothrombin_timehttp://en.wikipedia.org/wiki/Prothrombin_timehttp://en.wikipedia.org/wiki/Prothrombin_timehttp://en.wikipedia.org/wiki/Tissue_factorhttp://en.wikipedia.org/wiki/Partial_thromboplastin_timehttp://en.wikipedia.org/wiki/Partial_thromboplastin_time -
7/30/2019 Coagulation Final
16/70
Deficiencies of factor XII, high molecular
weight kininogen, and prekallikrein are notassociated with clinical bleeding but are ass.with prolongation of aPTT.
Factor XIII deficiency should be considered ina patient with a severe bleeding diathesiswho has otherwise normal coagulationscreening tests, including PT, PTT, fibrinogenlevel, platelet count, and bleeding time. Clotdissolution in 5M urea can be used as ascreen.
-
7/30/2019 Coagulation Final
17/70
Thrombus Formation
Clot is a Thrombus formed in an arterial or
venous vessel Thrombophlebitis - Both inflammation and
clots are present
Some thrombus can be superficial but itsthe DVT thats a concern embolism tolungs.
-
7/30/2019 Coagulation Final
18/70
Arterial formation - begins with platelet adhesion toarterial vessel wall Adenosine diphosphate (ADP)released from platelets more platelet aggregation
Bld. flow inhibited fibrin, platelets & RBCssurround clot build up of size structure occludesbld vessels tissue ischemia
The result of Arterial Thrombus is localized tissueinjury from lack of perfusion
-
7/30/2019 Coagulation Final
19/70
Venous Formation - Usually from slow bld flow
- Can occur rapidly. Stagnation of the blood flow initiate thecoagulation cascade production of fibrin enmeshesRBCs & platelets to form the thrombus. Venous thrombushas a long tail that can break off to produce an embolus.
These travel to faraway sites then lodge in lung (capillarylevel) inadequate O2 & CO2 exchange occur (ie.pulmonary embolism & cerebral embolism)
Oral & parenteral anticoagulants (Heparin/Warfarin)
primarily act by preventing venous thrombosis Antiplatelet drugs primarily act by preventing arterial
thrombosis
-
7/30/2019 Coagulation Final
20/70
Anticoagulants
Heparin Composition : mixture of sulfated glycosaminoglycans Mechanism of action : binds to anti thrombin and enhances its
effects by 1000 times to inactivate coagulation enzymes.
Antithrombin inhibits clotting factor proteases, especially thrombin(IIa), IXa, and Xa.
Heparin functions as a cofactor for the antithrombin-proteasereaction without being consumed.
Molecular weight : 5000-30000 Half life: IV 1 hr.
IM 3hr.
-
7/30/2019 Coagulation Final
21/70
-
7/30/2019 Coagulation Final
22/70
Prepared from a. bovine lung
b. bovine or porcine gi mucosa Endogenously present in a. basophils
b. mast cellsc. liver
1 Unit of Heparin volume of heparin containing
solution that will prevent clotting of 1 ml of sheeps blood from clotting for 1 hour afteraddition of 0.2 ml of 1:100 calcium chloride.
-
7/30/2019 Coagulation Final
23/70
Pharmacokinetics Poorly lipid soluble not useful orally : does not cross
placenta Routes : iv or sc Not given im : hematoma formation
Metabolism pathway not known No suitable chemical assay Extensively bound to plasma proteins Decrease in body temp below 37C prolongs elimination
half time Hepatic and renal dysfunction prolong elimin half time Nitroglycerin increases required dose of heparin
-
7/30/2019 Coagulation Final
24/70
Lab evaluation :aPTT: Used usually to monitor heparin treatment Maintain the ratio of APTT to approx 1.5 to 2.5
times the pre drug value(approx 30-35 secs) If >120 secs omit single dose as heparin is
short acting.TCT (Thrombin clotting time): For conforming heparin induced prolongation of aPTT.
-
7/30/2019 Coagulation Final
25/70
ACT (Activated clotting time) Mainstay of heparin anti coagulation monitoring. Easy to use and reliable for high heparin conc. Influenced by hypothermia, pre existing coag defects ,
presence of contact activation inhibitors (aprotinin),thrombocytopenia.
Baseline value determineda. before heparin administrationb. 3mins afterc. every 30 mins after that
Control ACT : 90 120 secs Cardio pulm bypass : adeq ACT- >300 secs: inadeq ACT -
-
7/30/2019 Coagulation Final
26/70
Clinical uses of heparin
Prevention of venous thrombosis and pulmonaryembolism Prevention of mural thrombosis after MI Treatment of unstable angina and acute MI Prevention of coronary re thrombosis after
thrombolysis Prevent extra corporeal thrombosis during bypass Treat selected cases of DIC Treat retarded fetal growth in pregnant women
-
7/30/2019 Coagulation Final
27/70
For prophylaxis : Enoxaparin better than low dose heparin (5000 U) This dose of heparin has a risk of forming wound haematoma
but no major bleeding Prophylaxis very imp for Hip surg bcoz 1. kinking of femoral vein
and 2. altered leg vein haemodynamics
For treatment : Heparin better Treatment : 5000U iv followed by infusion of 30,000 U every 24
hrs. After an initial bolus injection of 80-100 units/kg, a continuous
infusion of about 15-22 units/kg/h is required to maintain the
aPTT at 2-2.5 times control. Heparin is anticoagulant of choice in pregnancy and patientswith prosthetic heart valves
For treatment : duration 3- 6 months For treatment of MI : 5000 U followed by infusion of 24,000 U
over 24 hrs
-
7/30/2019 Coagulation Final
28/70
Side effects
Hemorrhage most common side effect Thrombocytopenia 2 types Allergic reactions CVS changes Altered protein binding displacement of alkaline
drugs like Propranolol and diazepam. Altered cell morphology distorts morphology of
RBC & WBC.(Hct , WBC Count and ESR not altered)
Decreased anti thrombin concentrations /activity paradoxical thrombotic tendency
-
7/30/2019 Coagulation Final
29/70
HAEMORRHAGE :
Most common serious side effect Increased risk : pre existing coag defects,
other drugs(eg aspirin), need forinstrumentation, chronic alchoholism.
Advantages : easy assessment (APTT, TT),shortelimin half time , availability of antagonist
Increased incidence of epidural haematoma inpatients receiving spinal and epiduralanesthetic followed by heparinanticoagulation.
-
7/30/2019 Coagulation Final
30/70
Thrombocytopenia
THROMBOCYTOPENIA MILD SEVERE
more common Life threatning
INCIDENCE seen in 30-40% patients seen in 0.5-6% patients
PLATELET COUNT
-
7/30/2019 Coagulation Final
31/70
ALLERGIC REACTIONS: Esp seen in patients with pre existing allergies d/t animal protein. Fever , utricaria
CARDIOVASCULAR CHANGES: Occurs with rapid infusion of large dose (300 U/Kg)
before bypass Modest decrease in MAP and pulm art pr D/t heparin mediated relaxation of vasc sm musc fall
in SVR
-
7/30/2019 Coagulation Final
32/70
Contraindication HIT Hypersensitivity to the drug Active bleeding Hemophilia Significant thrombocytopenia Purpura Severe hypertension Intracranial hemorrhage Infective endocarditis
Active tuberculosis Ulcerative lesions of the gastrointestinal tract Threatened abortion Visceral carcinoma
Advanced hepatic or renal disease.
-
7/30/2019 Coagulation Final
33/70
Protamine Specific antagonist of heparin. Strongly alkaline (d/t arginine) ; positively charged. Polycationic LMW protein found in salmon sperm. Positively charged alk Protamine combines with negatively
charged acidic heparin to form a complex that is devoid of anticoagulant activity.
The complex is removed by reticuloendothelial systemwithin 20 mins.
Dose reqd : 1 - 1.3 mg for every 100U of circulatingheparin.
If given in absence of heparin interacts with platelets andproteins including fibrinogen anti coag effect
CVS S/E hypotension , pulm hypertension , allergic
reactions
-
7/30/2019 Coagulation Final
34/70
HYPOTENSION : Rapid IV histamine release facial flushing , tachycardia ,
hypotension The rate of infusion should not exceed 50 mg in any 10-minute period.
Also influenced by site of injection in dogs hist release andsubseq effects seen if injected in RA but not in LA or
peripheral vein.
PULMONARY HTN : Hep-Prot complex secr of thromboxane and serotonin
pulm vasoconstic , pulm htn , pulm edema VQ mismatchart hypoxaemia
Also broncho constriction Pre treatment with COX inhibitors eg indomethacin or aspirin
blunts increase in pulm vasc resistance.
-
7/30/2019 Coagulation Final
35/70
Alternative to protaminePLATELET FACTOR 4 stored in the alpha granules of platelets. prevents formation of active thrombin inhibitor
from heparin and anti-thrombin III. Released during platelet aggregation May be an alternative to protamine
HEPARINASE I Specific heparin degrading enzyme Lyses heparin at its alpha-glycoside linkage
-
7/30/2019 Coagulation Final
36/70
LOW MOLECULAR WEIGHT HEPARINS Enoxaparin, Dalteparin , tinzaparin Derived by chemical depolymerization of unfractionated heparin Approx one third the size of heparin Heterogenous , mean mol wt 4000 5000 daltons have equal efficacy as heparin Superior bioavailability at lower doses More predictable anti coagulant responses Less binding to endothelial cells hence..longer elimin half life Once daily dosing Therapeutic doses do not affect PT and APTT. LMW heparin levels are not generally measured except in the
setting of renal insufficiency, obesity, and pregnancy. LMWheparin levels can be determined by anti-Xa units.
Protamine neutralises 65% of anti Xa activity of LMW heparin.
-
7/30/2019 Coagulation Final
37/70
Half life : 4.5 hrs. Prophylactic enoxaparin is given
subcutaneously in a dosage of 30 mg twicedaily or 40 mg once daily. Full-dose
enoxaparin therapy is 1 mg/kg subcutaneouslyevery 12 hours. This corresponds to atherapeutic anti-factor Xa level of 0.5-1unit/mL.
-
7/30/2019 Coagulation Final
38/70
LMWHUFH
1000-100003000-30000Mol Wt range
4000-500012000-15000Mo Wt average
2:1-4:11:1 Anti Xa: anti IIa activity
No YesaPTT monitoring required
NoYesInactivation by platelet factor 4
YesNoCapable of inactivation of plateletbound factor Xa
++++++Inhibition of platelet function
No YesIncrease vascular permeability+++++Protein binding
-+++Endothelial cell binding
No YesDose dependent clearance
2-5 times longer 50-90 minElimination half life
-
7/30/2019 Coagulation Final
39/70
Activated factor X inhibitor
FONDAPARINUX Interacts with antithrombin & increases its activity 300
times. Inhibits activated factor X. Eliminated through kidney. Half life- 17-21 hrs. Monitoring not required unlesss CKD.
-
7/30/2019 Coagulation Final
40/70
DIRECT ACTIVATED FACTOR XINHIBITOR
RIVAROXABAN Oral Half life- 7-11 hrs Used in HIT Contraindicated in hepatic diseses with coagulopathy
& CKD. No antidote.
0ral anticoagulants
-
7/30/2019 Coagulation Final
41/70
0ral anticoagulants
CHEMISTRY Derivatives of 4-hydroxy coumarin. (Wisconsin Alumni Research Foundation, with"arin" from coumarin added)
Warfarin most commonly usedAdvantages : predictable onset and duration of action
Excellent bioavailability after oral administrationDisadvantages: Delayed onset of action Require regular lab monitoring Difficulty in reversing effect
-
7/30/2019 Coagulation Final
42/70
Mechanism of action Inhibits Vit K epoxide reductase blocks conversion of Vit K epoxide
to Vit K depletion of Vit K block gamma-carboxylation of severalglutamate residues in prothrombin and factors VII, IX, and X as wellas the endogenous anticoagulant proteins C and S.
Platelet activity not affected.
Pharmacokinetics
Onset 8 12 hrs Rapidly and completely absorbed Peak conc 1 hr after ingestion 97% bound to albumin hence minimal renal excretion
long elimination half time
prevents diffusion into RBC , CSF , breast milk Crosses placenta with extensive effects on fetus Metabolized to inactive metabolites and conjugated with glucuronic
acid Excreted in bile and urine
-
7/30/2019 Coagulation Final
43/70
COMPARISON OF ORAL ANTICOAGULANTS
WARFARIN DICOUMAROL PHENINDIONE
PEAK EFFECT 36 72 hrs 36-48hrs 18-24hrs
DUR AFTERDISCONT
2-5 days 2-6 days 1-2 days
INITIAL ADULTDOSE
1st day- 15mg2nd day 10 mg
1st day 200-300mg
1st day 300mg2nd day 200 mg
MAINT ADULT DOSE 2.5-10mg 25-200mg 25-200mg
-
7/30/2019 Coagulation Final
44/70
LAB EVALUATIONProthrombin time (PT) should be increased to a level
representing a reduction of prothrombin activity to 25% of normal and maintained there for long-term therapy. Whenthe activity is less than 20%, the warfarin dosage should bereduced or omitted until the activity rises above 20%.
Therapeutic range for oral anticoagulant therapy is defined interms of an international normalized ratio (INR). The INR isthe prothrombin time ratio (patient prothrombin time/meanof normal prothrombin time for lab) ISI, where the ISIexponent refers to the International Sensitivity Index, and isdependent on the specific reagents and instruments used forthe determination.
-
7/30/2019 Coagulation Final
45/70
USE : Prevent venous thrombo embolism Prevent systemic embolization in pats with prosth
heart valves or atrial fibrillation Prevent stroke , recurrent MIINCREASED EFFECT: Drugs that inhibit clearance phenylbutazone and
amiodarone Inhibit conv of Vit K 2nd and 3 rd gen cephalosporins
Added effect heparin , aspirin and NSAIDsDECREASED EFFECT: Drugs that impair gi absorption cholestyramine Drugs that increase clearance barbiturates ,
rifampicin ,
-
7/30/2019 Coagulation Final
46/70
SIDE EFFECT: Bleeding main complication Treatment Vit K 10-20 mg orally or 1-5 mg IV @
1mg/min.PT returns to normal in 4 to 24 hrs. Skin necrosis occurs between 3-8 days d/t
extensive thrombosis of venules and capillarieswithin subcut fat.
Cross placenta embryopathy , CNS damage ,fetal bleeding
Embyopathy only in 1 st trimester nasalhypoplasia,stippled epiphyses
CNS damage any trimester blindness ,agenesis of corpus callosum
-
7/30/2019 Coagulation Final
47/70
Reversal of warfarin effect : Oral or parenteral vitamin K 1 (phytonadione) Fresh-frozen plasma Prothrombin complex concentrates such as
Bebulin and Proplex T, and recombinant factorVIIa (rFVIIa).
-
7/30/2019 Coagulation Final
48/70
THROMBOLYTIC DRUGS(fibrinolytics )
Streptokinase , alteplase , anistreplase MOA convert endogenous plasminogen to plasmin that causes
fibrinolysis Goal restore circulation through a previously occluded artery or
vein Acts best on newly formed clot (platelet rich and formed by weaker
fibrinogen bonds) Since reocclusion is common hence heparin also used for 1 st 24hrs Most common side effect bleeding ( M/C ICH) Most common in patients with recent trauma or recent surgery Disadvantage not fibrin specific
-
7/30/2019 Coagulation Final
49/70
CONTRAINDICATIONS
ABSOLUTE RELATIVE
Active internal bleeding Trauma/surg > 14 days
Trauma or surgery in last 14 days Chronic severe htn
Recent head trauma or KCO IC aneurysm Active peptic ulcer disease
H/O haemorrhagic CVA Treatment with anti coagulantsSBP > 200/120 mm Hg Known bleeding diathesis
Previous allergy Sig. liver ds
Traumatic CPR Prior exposure to Streptokinase oranistreplase
Suspected aortic dissection
Diabetic hgic retinopathy
pregnancy
-
7/30/2019 Coagulation Final
50/70
STREPTOKINASE Protein produced by beta hemolytic streptococci
Does not directly convert plasminogen to plasmin Binds non covalently to p.gen formation of p.gen activator
complex acts on other p.gen mols gen of plasmin Elimin half life 23 mins Infusion decreases SVR hypotension May stimulate Ab produc subsequent allergic reactions If anti strepto Abs present then induces amnestic response Lab monitoring TT If TT not prolonged within a few hrs resistance to streptokinase
d/t high titre of anti strepto Abs. Streptokinase is administered by intravenous infusion of a loading
dose of 250,000 units, followed by 100,000 units/h for 24-72hours in acute MI.
-
7/30/2019 Coagulation Final
51/70
ANISTREPLASE ( ANISOYLATED PLASMINOGEN STREPTOKINASE ACTIVATOR COMPLEX) Synthesized with aim of longer dur of action . allows for rapid intravenous injection, greater clot selectivity (ie, more activity on
plasminogen associated with clots than on free plasminogen in the blood), and morethrombolytic activity.
Tissue plasminogen activators (t-PAs) preferentially activate plasminogen that is bound to fibrin.
Alteplase, Reteplase, Tenecteplase(Longer half life).Alteplase Synth by endothelial cells More expensive and more effective than Streptokinase in opening an infarct
related artery esp if started in 3hrs Clearance by liver Elimin half life
-
7/30/2019 Coagulation Final
52/70
COMPARISONTHROMBOLYTIC DRUGS
STREPTOKINASE ALTEPLASE ANISTREPLASE
DOSE 1.5 million U..1 hr 1.25mg/kg over 3hrs
30 U over 2-5 mins
USES ACS,PE ACS,PE ACS,PE
SITE OF ACTION P.gen P.gen P.gen
ELIMIN T 23 mins
-
7/30/2019 Coagulation Final
53/70
DIRECT THROMBIN INHITOR (anti thrombotic)
Directly binds to the active site of thrombin, thereby inhibitingthrombin's downstream effects. Suppress platelet function. Use arterial and venous thrombotic disease
Used in treatment of art thrombi and preven of venthr.emb
Inhibit free and clot bound thrombin HIRUDIN- derived from leech saliva. Recombinant Lepirudin and Desirudin Alternative to heparin in pats who req anti coag but have hep
resist or heparin induced thrombocytopenia.
-
7/30/2019 Coagulation Final
54/70
HIRUDIN XIMELAGATRAN
ARGATROBAN BIVALIRUDIN
ROUTE IV Oral IV IVEXCRETION Renal Renal hepatic hepatic
USE Hep inducedthr cytopenia
thromboPxt/t of DVT
Hep ind thrcytopenia
Coronaryinterventions
STOP B4 SURG 8hrs 24 hrs 4-6hrs 2-3 hrs
PROLONGPT/PTT
+/+ +/+ +/+ +/+
ANTIDOTE haemodialysis (-) (-) (-)
-
7/30/2019 Coagulation Final
55/70
Antiplatelet drugs Targets for platelet inhibitory drugs:(a) inhibition of prostaglandin metabolism through inhibition of
cyclooxygenase (aspirin): COX is a key enzyme involved in the synthesis of thromboxane 2
(prostaglandins). Inhibits platelet aggregation long acting because new proteins must be synthesizedDose: Low dose daily (180 mg/day): Prevents ischemic attack
(ministroke) and MI 325 mg/d for primary prophylaxis of myocardial infarction
-
7/30/2019 Coagulation Final
56/70
(b) inhibition of ADP-induced platelet aggregation (ticlopidine,
clopidogrel) no effect on PG metabolism used as alternative for patients intolerant to aspirin expensive
(c)BLOCKADE OF PLATELET GLYCOPROTEIN IIB/IIIA RECEPTORS(Abciximab, Eptifibatide, Tirofiban)
(d) Additional antiplatelet drugs (Dipyridamole , cilostazol)
DRUGS USED IN BLEEDING DISORDERS
-
7/30/2019 Coagulation Final
57/70
DRUGS USED IN BLEEDING DISORDERS
VITAMIN K Vitamin K 1 is available clinically in oral and parenteral forms. Onset of effect is delayed for 6 hours but the effect is complete by 24
hours. Treatment of depression of prothrombin activity by excess warfarin or
vitamin K deficiencyPLASMA FRACTIONS FFP Cryoprecipitate- It is used to treat deficiencies or qualitative
abnormalities of fibrinogen, such as that which occurs withdisseminated intravascular coagulation and liver disease. Alsouseful in factor VIII deficiency.
Desmopressin acetate- increases the factor VIII activity of patients with mild hemophilia A or von Willebrand disease
-
7/30/2019 Coagulation Final
58/70
FIBRINOLYTIC INHIBITORS:Aminocaproic acid (EACA)
synthetic inhibitor of fibrinolysis. It competitively inhibits plasminogen activation. It is rapidly absorbed orally and is cleared from the body by
the kidney. The usual oral dosage of EACA is 6 g four times a day. When
the drug is administered intravenously, a 5 g loading doseshould be infused over 30 minutes to avoid hypotension.
Tranexamic acid analog of aminocaproic acid and has the same properties. It is administered orally with a 15 mg/kg loading dose
followed by 30 mg/kg every 6 hours. Iv dose is 10 mg/kg followed by infusion of 1
mg/kg/hour
-
7/30/2019 Coagulation Final
59/70
SERINE PROTEASE INHIBITORS :APROTININ inhibits fibrinolysis by free plasmin.
It also inhibits the plasmin-streptokinase complex inpatients who have received that thrombolytic agent. currently approved for use in patients undergoing
coronary artery bypass grafting who are at high risk
of excessive blood loss.
-
7/30/2019 Coagulation Final
60/70
-
7/30/2019 Coagulation Final
61/70
-
7/30/2019 Coagulation Final
62/70
-
7/30/2019 Coagulation Final
63/70
-
7/30/2019 Coagulation Final
64/70
-
7/30/2019 Coagulation Final
65/70
RISK STRATIFICATION OF TEHIGH RISK : Mitral or aortic valve prosthosis Stroke or TIA AF CHADS 2 > 4
VTE < 3 months Known thrombophilia
MODERATE RISK: Aortic valve (new)
CHADS 2 >2 VTE 6-12 months
LOW RISK: CHADS 2 12 MONTHS
CHADS-2 SCORINGSYSTEM
POINTS
CHF 1
HTN 1
AGE >75 1
DM 1
PRIOR STROKE OR TIA 2
A h i id i
-
7/30/2019 Coagulation Final
66/70
Anaesthetic considerationsPatient on warfarinPreoperative Discontinue warfarin at least 5 d before elective procedure. Assess INR 1 to 2 d before surgery, if >1.5, consider 1-2 mg of oral vitamin K. Reversal for urgent surgery/procedure, consider 2.5-5 mg of oral or intravenous vitamin K; for immediate
reversal, considerfresh-frozen plasma
Patients at high risk for thromboembolism Bridge with therapeutic subcutaneous LMWH (preferred) to be given 36 hrs after stopping warfarin
(eonoxaparin 1.5mg/kg BD or 1mg/kg OD) or intravenous UFH. Last dose of preoperative LMWH administered (BD- morning dose only., OD- 24 hrs before surgery, administerhalf of the daily dose)
Intravenous heparin discontinued 4 hrs before surgery No bridging necessary for patients at low risk for thromboembolism
PostoperativePatients at low risk for thromboembolism
Resume warfarin on postoperative dayPatients at high risk for thromboembolism (who received preoperative bridging therapy)
Minor surgical procedure - resume therapeutic LMWH 24 hrs postoperatively Major surgical procedure - resume therapeutic LMWH 48-72 hrs postoperatively or administer low-dose LMWH Restart warfarin on the evening of post operative day. Discontinue LMWH when INR Is therapeutic for 2 consequitive day.
l l d
-
7/30/2019 Coagulation Final
67/70
Patient on antiplatelet drugsPatients with coronary stents (on aspirin/ clopidogrel) Elective surgery postponed for the following duration
Bare metal stents: 4-6 wkDrug-eluting stents: 12 months
If surgery cannot be postponed, continue aspirin throughoutperioperative period
Patients at high risk for cardiac events (exclusive of coronarystents)
Continue aspirin throughout the perioperative period Discontinue clopidogrel at least 5 d (and preferably 10 d) before
surgery Resume clopidogrel 24 hrs postoperativelyPatients at low risk of cardiac events Discontinue antiplatelet therapy 7-10 d before surgery Resume antiplatelet therapy 24 hrs postoperatively
l h & l
-
7/30/2019 Coagulation Final
68/70
Regional anaesthesia & anticoagulationPatient on unfractionated heparinProphylactic subcutaneous UFH 5000 U twice daily No contraindication to the use of neuraxial techniques.
Doses >10,000 U of UFH daily or more than twice daily
Safety not established . Needle placement 1 hr Heparin
Heparin 2-4 hrs Catheter removal 1hr Heparin
P ti t LMWH
-
7/30/2019 Coagulation Final
69/70
Patient on LMWHPreoperative
LMWH thromboprophylaxis doses :LMWH 10-12 hrs Needle placementHigher (treatment) doses :
LMWH 24hr Needle placementPostoperative
Twice daily dose :
NP 24hrs 1st
dose LMWHCatheter removal 2hrs
-
7/30/2019 Coagulation Final
70/70
once daily dose:
NP 6-8hrs 1 st dose 24 hrs 2 nd dose
LMWH 10-12 hrs Cath. rem. 2hrs LMWH
Patient on warfarin Warfarin should be stopped 4-5 days before planned proc. Catheter removed when INR > 1.5.