CO Strongyloides stercoralisin solid organ transplantation ... Mobley... · disseminated...
9
Copyright © 2017 Wolters Kluwer Health, Inc. All rights reserved. C URRENT O PINION Strongyloides stercoralis in solid organ transplantation: early diagnosis gets the worm Constance M. Mobley a,b , Atiya Dhala a , and Rafik Mark Ghobrial a,b Purpose of review Strongyloidiasis is a parasitic infection affecting millions of people worldwide. Complications of infection are strongly associated with alcoholism, immunosuppression, and organ transplantation. Delayed diagnosis results in hyperinfection syndrome and disseminated strongyloidiasis leading to mortality rates approaching 80%. Early detection, and prevention of infection and transmission are key to diminish this illness. Recent findings In this review, we cover the basic concepts in immunity, immunosuppression, and disorder necessary for understanding the infectious syndromes associated with Strongyloides stercoralis infection. Focused discussion on donor-derived transmission and recipient risk in solid organ transplantation is presented. Current methodology for diagnosis, screening algorithms, and treatment are also reviewed. Summary Strongyloidiasis complicated by hyperinfection and dissemination remains associated with a poor outcome. The poor outcome pleads for a high level of suspicion and aggressive treatment in at-risk patients. As the population of transplant patients continues to increase, the risk of infection also increases, compelling us to address this highly fatal infectious complication in solid organ transplantation (SOT). Here we review the pathology, immunology, diagnosis, and treatment of strongyloides infection in the immunosuppressed SOT population. Keywords disseminated strongyloidiasis, posttransplant infections, solid organ transplantation, Strongyloides hyperinfection syndrome, Strongyloides stercoralis INTRODUCTION Strongyloidiasis is a chronic parasitic infection spread by the nematode, Strongyloides stercoralis. This soil-transmitted helminth is the only parasite that secretes larvae in feces and alternates between free-living cycles (rhabditiform larvae) and parasitic cycles (filariform infective larvae). The rhabditiform larvae in the stool can either become filariform larvae or free-living adult worms. These free-living adult worms produce eggs that develop into infec- tive filariform larvae, which can penetrate the intact human skin through contact with contaminated soil. The larvae finally settle in the small intestine via the hematogenous spread or through the skin. The female adults produce eggs within the epi- thelium of the small intestine. During the auto- infective stage, the infective filariform larvae per- petuates the infection leading to chronic stages of this disease (Fig. 1). Infection with these intestinal helminths cause microbial translocation from the leaky intestinal epithelium, leading to sepsis and multiorgan failure [1–5]. Strongyloidiasis is very difficult to diagnose as the infected patients are generally asymptomatic while carrying the dormant parasite for decades. Among the infected population, certain susceptible patients with impaired cellular immunity may develop strongyloides hyperinfection syndrome (SHS), an amplification of the normal life cycle of the nematode leading to excessive worm burden within the traditional reproductive route. The other serious manifestation of this infection results in disseminated strongyloidiasis, where the larvae spread through abnormal pathways outside the a Department of Surgery, Division of Surgical Critical Care and b Sherrie & Alan Conover Center for Liver Disease & Transplantation, Houston Methodist Hospital, Houston, Texas, USA Correspondence to Constance M. Mobley, MD, PhD, FACS, 6550 Fannin Street, SM1601, Houston, TX 77030, USA. Tel: +1 713 441 1590; fax: +1 713 790 6470; e-mail: [email protected] Curr Opin Organ Transplant 2017, 22:336–344 DOI:10.1097/MOT.0000000000000428 www.co-transplantation.com Volume 22 Number 4 August 2017 REVIEW
Transcript of CO Strongyloides stercoralisin solid organ transplantation ... Mobley... · disseminated...

REVIEW
CURRENTOPINION Strongyloides stercoralis in solid organ
transplantation: early diagnosis gets the worm
Copyright
www.co-transplantation.com
a,b a a,b
Constance M. Mobley , Atiya Dhala , and Rafik Mark GhobrialPurpose of review
Strongyloidiasis is a parasitic infection affecting millions of people worldwide. Complications of infectionare strongly associated with alcoholism, immunosuppression, and organ transplantation. Delayed diagnosisresults in hyperinfection syndrome and disseminated strongyloidiasis leading to mortality rates approaching80%. Early detection, and prevention of infection and transmission are key to diminish this illness.
Recent findings
In this review, we cover the basic concepts in immunity, immunosuppression, and disorder necessary forunderstanding the infectious syndromes associated with Strongyloides stercoralis infection. Focuseddiscussion on donor-derived transmission and recipient risk in solid organ transplantation is presented.Current methodology for diagnosis, screening algorithms, and treatment are also reviewed.
Summary
Strongyloidiasis complicated by hyperinfection and dissemination remains associated with a poor outcome.The poor outcome pleads for a high level of suspicion and aggressive treatment in at-risk patients. As thepopulation of transplant patients continues to increase, the risk of infection also increases, compelling us toaddress this highly fatal infectious complication in solid organ transplantation (SOT). Here we review thepathology, immunology, diagnosis, and treatment of strongyloides infection in the immunosuppressed SOTpopulation.
Keywords
disseminated strongyloidiasis, posttransplant infections, solid organ transplantation, Strongyloideshyperinfection syndrome, Strongyloides stercoralis
aDepartment of Surgery, Division of Surgical Critical Care and bSherrie &Alan Conover Center for Liver Disease & Transplantation, HoustonMethodist Hospital, Houston, Texas, USA
Correspondence to Constance M. Mobley, MD, PhD, FACS, 6550Fannin Street, SM1601, Houston, TX 77030, USA.Tel: +1 713 441 1590; fax: +1 713 790 6470;e-mail: [email protected]
Curr Opin Organ Transplant 2017, 22:336–344
DOI:10.1097/MOT.0000000000000428
INTRODUCTION
Strongyloidiasis is a chronic parasitic infectionspread by the nematode, Strongyloides stercoralis.This soil-transmitted helminth is the only parasitethat secretes larvae in feces and alternates betweenfree-living cycles (rhabditiform larvae) and parasiticcycles (filariform infective larvae). The rhabditiformlarvae in the stool can either become filariformlarvae or free-living adult worms. These free-livingadult worms produce eggs that develop into infec-tive filariform larvae, which can penetrate the intacthuman skin through contact with contaminatedsoil. The larvae finally settle in the small intestinevia the hematogenous spread or through the skin.The female adults produce eggs within the epi-thelium of the small intestine. During the auto-infective stage, the infective filariform larvae per-petuates the infection leading to chronic stages ofthis disease (Fig. 1). Infection with these intestinalhelminths cause microbial translocation from theleaky intestinal epithelium, leading to sepsis andmultiorgan failure [1–5].
© 2017 Wolters Kluwer
Strongyloidiasis is very difficult to diagnose asthe infected patients are generally asymptomaticwhile carrying the dormant parasite for decades.Among the infected population, certain susceptiblepatients with impaired cellular immunity maydevelop strongyloides hyperinfection syndrome(SHS), an amplification of the normal life cycle ofthe nematode leading to excessive worm burdenwithin the traditional reproductive route. The otherserious manifestation of this infection results indisseminated strongyloidiasis, where the larvaespread through abnormal pathways outside the
Health, Inc. All rights reserved.
Volume 22 � Number 4 � August 2017

Copyright © 2017 Wolters Kluwe
KEY POINTS
� The risks associated with S. stercoralis infectionincreases with immunosuppressive therapy, particularlycorticosteroids, which is used in solid organtransplantation.
� Most posttransplant infections with Strongyloides resultfrom reactivation of a chronic infection; however, thefrequency of donor-derived strongyloidiasis is becomingan increasingly recognized phenomena.
� Strongyloides hyperinfection syndrome anddisseminated strongyloides remain highly lethalinfections with mortality rates approaching 80%.
� The mainstay of strongyloides management remainsutilizing appropriate screening and maintaining a highindex of suspicion in at-risk patients.
FIGURE 1. The life cycle of S. stercoralis. Source: https://wwPublished Online].
Strongyloides stercoral is in solid organ transplantation Mobley et al.
1087-2418 Copyright � 2017 Wolters Kluwer Health, Inc. All rights rese
intestines and the lungs, often involving but notlimited to the liver, central nervous system, heart,and the urinary tract. The group most susceptible tosuch hyperinfection and dissemination includepatients who have received corticosteroid therapyincluding organ transplant recipients, patients withHIV, human T-cell lymphotropic virus type 1(HTLV-1) coinfected patients, hematological malig-nancies, chronic kidney disease [6], and chronicalcoholics among others.
PREVALENCE
Strongyloides is endemic in Africa, Southeast Asia,the West Indies, South America, Bangladesh, andPakistan [7]. In tropical and subtropical countries,S. stercoralis infections affect between 10 and 40% ofthe population. However, prevalence of strongyloi-diasis globally is underestimated because of the lowsensitivity of reference methods [3], and prevalencerates vary widely with estimates varying between
r Health, Inc. All rights reserved.
w.cdc.gov/parasites/strongyloides/biology.html. [Previously
rved. www.co-transplantation.com 337

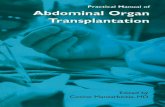
FIGURE 2. Prevalence of S. stercoralis infection by country-based community-based studies. Reproduced with permission [8].
Infectious complications in transplantation
30 and 100 million patients affected globally (Fig. 2).In underdeveloped countries where socioeconomicconditions promote the spread of S. stercoralis, highinfection rates of up to 60% can be expected. In S.stercoralis endemic countries, such as Thailand andBrazil, where more accurate data on infection isavailable, prevalence rates vary between 13 and17% and 23.7 and 34.7%, respectively, dependingon methodology used for data acquisition [8].
S. stercoralis has a very low prevalence insocieties where fecal contamination of soil is rare.Hence, it is a very rare infection in developedcountries and is less prevalent in urban than in ruralareas of resource poor countries. In the UnitedStates, the prevalence of strongyloidiasis variesgreatly between the native-born population andthe immigrant population, which has significantlyhigher rates of infection, and infection tends tooccur in pockets and predominantly affects indivi-duals pursuing farming activities or miners [8].
CLINICAL MANIFESTATIONS
Patients with acute strongyloides infection oftenhave only mild waxing and waning symptoms, incontrast to chronically infected patients who oftenremain asymptomatic. Clinical manifestations ofacute infection consist of localized skin irritationat the site of larvae penetration, followed by pul-monary symptoms of dry cough, dyspnea, wheezing
Copyright © 2017 Wolters Kluwer
338 www.co-transplantation.com
and hemoptysis, and gastrointestinal distress, suchas abdominal pain from duodenitis, diarrhea, orconstipation. Some infected patients may only havea mild or moderate eosinophilia. Symptoms canpersist for years and even decades and remainundiagnosed. In cases of immunosuppressive treat-ment, patients have the potential to develop fatalhyperinfection and dissemination. Proper screeningof potentially infected individuals prior to begin-ning immunosuppressive treatment (coprologicallyover several days and/or serologically) is essential.
Hyperinfection syndrome
The cycle of autoinfection can lead to increasedparasite burden without spread of the larvae outsideof their normal migration pattern in the gastro-intestinal and respiratory tracts. The incidence ofSHS in patients chronically infected is approxi-mately 2% [9
&&
]. Common clinical manifestationsof SHS include fever, nausea, vomiting, anorexia,diarrhea, abdominal pain, dyspnea, wheezing,hemoptysis and cough. Chest radiograph revealspulmonary infiltrates that consist of foci of hemor-rhage, pneumonitis, and edema [10]. In a reviewconcerning clinical manifestations and outcomes ofSHS, Guillaume Geri et al. retrospectively analyzed atotal of 133 cases over a 14-year period (2000–2013).According to their findings, fever (80.8%), respirat-ory (88.6%), and gastrointestinal (71.2%) symptoms
Health, Inc. All rights reserved.
Volume 22 � Number 4 � August 2017

Strongyloides stercoral is in solid organ transplantation Mobley et al.
were the most common clinical manifestations.The same study found the following clinical andlaboratory manifestations: shock in 57.3% ofpatients, hypereosinophilia in 34.3%, mechanicalventilation in 67.9%, and bacterial infection in38.4%. The predictive factors of the ICU mortality(rate¼60.3%) included shock, mechanical venti-lation, and concomitant bacterial infection [9
&&
].
Disseminated strongyloidiasis
Disseminated infection results from parasitic spreadto organs other than the pulmonary system andgastrointestinal tract. Disseminated strongyloidiasisrefers to the widespread dissemination of the para-sites from the gut to any organ and is associated withimpairment of the normal intestinal wall barrier andconcomitant bacterial translocation [11]. Given therarity of the disease, only case reports and small caseseries are available. In one study, the clinical courseand outcome of disseminated strongyloidiasistreated in one hospital over a 10-year period wasreviewed. Of the seven cases identified, the mostcommon presenting symptoms were seven patientwith fever (100%), five patients (71%) had gastro-intestinal symptoms, three (42%) patients had asignificant drop in hemoglobin, and six (85%)patients had bronchoalveolar infiltrates on chestradiographs. Most patients were immunosuppressedby means of steroid treatment for their underlyingprimary disease. Five (71%) of the patients with lunginvolvement progressed to respiratory failure anddied. Two (29%) cases were complicated by gram-negative bacterial infection. Despite aggressivetherapy, the mortality rate in the cohort was 71%[10].
Chronic infection predisposes immunosup-pressed patients to shock because of microbial trans-location whenever there is a violation of theintestinal epithelium. Studies of circulating levelsof bacterial translocation markers have foundincreased levels of lipopolysaccharide, acute phaseproteins, and several proinflammatory cytokinesamong infected patients [12].
IMMUNOLOGY
Chronic strongyloidiasis profoundly modulates thehost’s innate and adaptive immune system, whichprevents the development of hyperinfection syn-drome and disseminated strongyloidiasis. A numberof situations can disrupt the host immune systemwith loss of granulocyte function or Th-2 cytokinerelease, reducing the immune regulation of adultworm density, which can trigger hyperinfectionsyndrome and disseminated strongyloidiasis [13].
Copyright © 2017 Wolters Kluwe
1087-2418 Copyright � 2017 Wolters Kluwer Health, Inc. All rights rese
Immunosuppressive therapy use in solidorgan transplantationGlucocorticoids are the most commonly usedimmunosuppressive therapy associated withincreased risk for SHS and disseminated strongyloi-diasis. Corticosteroids affect the immunity in thefollowing ways: suppression of eosinophil prolifer-ation and inhibition of mast cell response, increas-ing the apoptosis of Th-2 lymphocytes, increasingecdysteroid-like substances that act as moltingsignals and lead to increased production of auto-infective filariform larvae, and a direct effect on theparasite – either accelerating the transformation ofrhabditiform to invasive filariform larvae or rejuve-nating asexual reproduction of latent adult females[13,14]. Interestingly, calcineurin inhibitor cyclo-sporine has been demonstrated to be toxic to thisnematode and maybe associated with reduced riskof infection in patients receiving this drug. Figure 3provides an overview of the immunology and path-ology of strongyloidiasis.
Innate immunity
Eosinophils are one of the major components of theimmune system responsible for combating infec-tions, specifically helminth infections. Eosinophilsare believed to play an essential role in the interfacebetween innate and adaptive responses. In indivi-duals with severe strongyloidiasis, eosinophil levelswere found to be lower than in asymptomatic indi-viduals. Thus, eosinophilia may play a preventiverole in strongyloides infection [15]. Strongyloidesantigens activate eosinophils, and these activatedeosinophils then act as antigen-presenting cells(APC) and stimulate the production of antigen-specific Th-2 cytokines, including interleukin (IL)-4 and IL-5. Larval killing is aided by neutrophils,mediated by IL-4 which in turn induces the pro-duction of immunoglobulin E (IgE) and immuno-globulin G4 antibodies and IL-8 by a class-switch ofactivated B lymphocytes. IgE production causesmast cell degranulation and increases eosinophilmigration, whereas IL-5 prompts further eosinophilgrowth and activation [13].
Adaptive immunity
The adaptive immune response involves robusttype-2 responses. In contrast, the regulatory T cellsdampen Th-2 responses and it is the critical inter-actions between the Th-1 and Th-2 and regulatory Tcells, which function as the defense mechanism forthis nematode. The Th-2 responses are composed oftwo compartments – one characterized by increasedproduction of type 2 cytokines including IL-4, IL-5,
r Health, Inc. All rights reserved.
rved. www.co-transplantation.com 339

FIGURE 3. Immunology of hyperinfection syndrome and disseminated strongyloidiasis. This figure provides an overview of theimmunology and pathology of strongyloidiasis leading to hyperinfection syndrome and disseminated strongyloidiasis. The blueboxes represent the precipitating factors whereas the grey box describes the different mechanisms by which corticosteroidsmay affect the immunity. The pink boxes list the clinical manifestations of hyperinfection syndrome and disseminatedstrongyloidiasis.
Infectious complications in transplantation
IL-9, and IL-13 and second increased expression ofregulatory cytokines IL-10 and transforming growthfactor-ß. In helminth infections, it is believed thatthe proinflammatory responses including type-1and type-17 responses are downregulated andtype-2 and anti-inflammatory responses are upregu-lated. Anuradha et al., confirmed these findings inboth animal models and human infections forwhich predominant type-2 and regulatory cytokinesresponses are reported in the settings of chronicstrongyloidiasis. Both type-2 cytokines and regulat-ory cytokines were increased markedly in infectedindividuals and their levels decreased followingtreatment. In addition, two other immunoregula-tory, anti-inflammatory cytokines IL-27 and IL-37were found to be elevated in infected patientswith similarly decreasing levels following therapy[16,17
&
].
STRONGYLOIDIASIS IN SOLID ORGANTRANSPLANT POPULATION
Strongyloidiasis in SOT recipients can occur bytransmission from an infected donor or from reac-tivation of latent infection in the recipient. The
Copyright © 2017 Wolters Kluwer
340 www.co-transplantation.com
diagnosis should be considered in immunocompro-mised patients who experience nonspecific gastro-intestinal or cardiopulmonary symptoms or whosuffer from unexplained sepsis caused by gramnegative bacilli.
Donor-derived Infection
Donor-transmitted S. stercoralis infections in trans-plant recipients are rare. The rarity of the phenom-enon is evident in two recent studies where review ofcase reports spanning nearly two decades identifiedonly 27 patients with confirmed donor-derivedstrongylodiasis. Donor-derived infection has beenmost compelling in cases of renal allograft recipi-ents, with 18 of the 27 (66.7%) cases identifiedoccurring in kidney transplant recipients, andwhy renal recipients may be more susceptible totransmission is not clear [18–20]. However, trans-mission has been documented in cardiac, liver, pul-monary, pancreatic, and intestinal transplants aswell [21,22]. Onset of symptoms and presentationis typically around 6 weeks, but has been reported upto 9 months posttransplant [19]. As expected, pre-senting symptoms were vague, and diarrhea, fever,
Health, Inc. All rights reserved.
Volume 22 � Number 4 � August 2017

Strongyloides stercoral is in solid organ transplantation Mobley et al.
and abdominal pain predominated. All patientsexcept one were on corticosteroids for immuno-suppression therapy. Of the patients who werediagnosed early, survival was good. Patients whoprogressed to hyperinfection and disseminationhad predictably poor outcomes.
Donor derivation is difficult to prove andusually only confirmed after infection is docu-mented from organs received from a commondonor. Although the incidence of transmissionremains unknown, a review of CDC data, from2009 to 2013, identified seven donor-derived infec-tions. In this group, six out of seven (86%) of donorstended to be from high-risk areas where strongy-loides is endemic [23
&
,19].
Recipient infection and reactivation
Unlike donor-derived strongyloidiasis, activation ofdormant disease in transplant patients is compara-tively common. Indeed, most strongyloides infec-tions in organ transplant recipients are thought tobe caused by reactivation of chronic infection afterinitiation of immunosuppressive therapy. The typeof immunotherapy can affect the risk of infectionand reactivation. T-cell depleting therapies, such assteroids, increase the host risk for reactivation.Alternatively, cyclosporine has some antiparasiticeffects. Most patients present symptomatic withinthe first 6 months posttransplant, but diagnosis isoften delayed because of nonspecific symptoms.After an immunocompromised patient developsSHS or disseminated strongyloidiasis, mortality ishigh.
Posttransplant patients with SHS and dissemi-nated disease generally have a very high mortalityrate (�87%), underscoring the need for carefulscreening of both donor and recipient populationsand treatment of these patients prior to transplan-tation [22].
DIAGNOSTIC TESTING
Eosinophilia
Eosinophilia is a common but not confirmatoryfinding in strongyloides infection. It is more pro-nounced in acute infections, but less so with chronicinfections. Hays et al. [24] showed that eosinophiliaalone cannot be used to confirm the presence ofstrongyloides infection in patients from endemicareas. Hypereosinophilia is encountered in about70% of patients with strongyloides infection butonly 20% of patients with SHS. Therefore, it shouldnot be used as a single criterion for screening inimmunocompromised patients because it is not
Copyright © 2017 Wolters Kluwe
1087-2418 Copyright � 2017 Wolters Kluwer Health, Inc. All rights rese
always evident that it can be associated withmigratory phase of infection and thus transient innature [9
&&
].
Microscopic observation of larvae in stool
A traditional microscopy-based diagnostic test, thestool test is considered to be the gold standard fordiagnosis of strongyloides in serial stool examin-ation. Seven consecutive cultures are required toreach 100% sensitivity. The disadvantage of this testis that there is intermittent larval excretion duringchronic infection. The Baermann method and Kogaagar plate culture are preferable, although they arecumbersome and not routinely used. An interestingimprovement in the sensitivity of stool microscopyfor strongyloides has been obtained with a verysimple concentration method called spontaneoustube sedimentation [25
&
].
Serological
Serological diagnostic testing is highly sensitive incases of chronic infection. However, it is less reliableamong immunocompromised patients, includingthose from endemic areas. This test also cannotdistinguish between recent versus past infections.The key types of serological testing include in-houseimmunofluorescence antibody test (IFAT), NIE-ELISA, and NIE-LIPS. The most sensitive test wasIFAT with 94.6% sensitivity, followed by IVD-ELISA(97.4%). However, the sensitivity of ELISA drops inimmunocompromised hosts. Commercially avail-able ELISAs reach a negative predictive value of upto 99%, providing some utility in ruling out thediagnosis [26].
Real-time polymerase chain reaction
Recent advances in molecular techniques have pro-vided an important diagnostic tool. Real-time PCR(RT-PCR) can detect DNA of the parasite in stoolsamples. Using RT-PCR on two serial stool samplesfrom the same patient, studies have shown highsensitivity and negative predictive value [25
&
,27].RT-PCR may be used not only as a screening testfor donors, but can also provide early diagnosis inpatients receiving SOT from infected donors, facil-itating early treatment and prevention of SHS anddisseminated strongyloidiasis [28–32]. AlthoughRT-PCR is not widely available, especially inendemic countries, it remains a promising tech-nique to improve early detection.
Other diagnostic tools
Another test using duodenal aspirate is more sensi-tive than stool examination. Duodenal fluid can be
r Health, Inc. All rights reserved.
rved. www.co-transplantation.com 341

Infectious complications in transplantation
examined using techniques such as the Enteroteststring or duodenal aspiration. Duodenal biopsy mayreveal parasites in the gastric crypts, in the duodenalglands or eosinophilic infiltration in the laminapropria. The pulmonary sample test uses a simplewet-mount in fluid from a bronchoalveolar lavage(BAL). Frequently, the larvae can be identified in wetpreparations of sputum, BAL fluid, bronchial wash-ings and brushings, lung biopsies, or examination ofpleural fluid.
Screening methodology
Screening tests have limitations, so clinicalsuspicion remains an important component ofthe pretransplantation evaluation. Recipientsand donors from endemic areas should be screenedfor Strongyloides by serology. The American Societyof Transplantation recommends screening byserum ELISA. Although current practice guidelinesrecommend screening for strongyloides, cliniciansoften fail to identify patients with chronicinfections. Recommended protocol for screeningand early detection of strongyloidiasis entails astep-by-step approach. The initial step involvesconducting interviews with patients or theirfamily members to identify individuals at higherrisk of contracting the infection. A full diagnostic
Copyright © 2017 Wolters Kluwer
FIGURE 4. Step-by-step recommended protocol for screening, eawith data compiled from [5,33&&].
342 www.co-transplantation.com
work-up may be conducted as a second step, usingtools such as RT-PCR among others. Prior to theuse of any immunosuppressive therapy, promptinitiation of treatment is highly recommended.Figure 4 summarizes the recommended steps forscreening and early detection of strongyloidiasis[33
&&
].
TREATMENT
Treatment of hyperinfection syndrome and dis-semination includes ivermectin and albendazoletherapy. Broad-spectrum antibiotics are initiatedif bacteremia, meningitis, or pneumonitis issuspected, and reduction in immunosuppressionis necessary.
The benzimidazoles (albenadazole and thiaben-dazole) and ivermectin are the drugs most com-monly used to treat strongyloidiasis. Ivermectin isan extremely potent, broad spectrum, antihel-minthic drug. As a semisynthetic macrocyclic lac-tone, ivermectin causes paralysis of intestinalparasites through its effect on ion channels in cellmembranes.
Ivermectin in available in the oral, rectal, andsubcutaneous routes. The only route licensed forhuman use is oral, however, in SHS and dissemi-nated strongyloidiasis where there might be small
Health, Inc. All rights reserved.
rly detection and treatment of strongyloidiasis. Original figure
Volume 22 � Number 4 � August 2017

Strongyloides stercoral is in solid organ transplantation Mobley et al.
bowel involvement, enteral treatment is poorlytolerated. There is limited data on the unlicenseduse of subcutaneous route of ivermectin. If oraland/or rectal administration are not possible, theninvestigational new drug (IND) exemptions forveterinary subcutaneous form of ivermectin canbe granted by the FDA [34].
Data covering seven randomized controltrials in adults with chronic strongyloides infec-tion taken from Cochrane Review comparedivermectin with albendazole or thiabendazole.Results showed treatment with ivermectin curedmore people than albendazole and may be bettertolerated [35
&&
].
CONCLUSION
Strongyloides is a global health challenge particu-larly in the transplant population where infectioncarries a high mortality rate. Diagnosis is oftendelayed due to the nonspecific nature of presentingsymptoms, and early diagnosis relies on a high indexof clinical suspicion to prevent death. Posttrans-plant patients with SHS and disseminated diseasehave a very high mortality rate of about 87%, under-scoring the need for both donor and recipientscreening and treatment of these patients. Trans-plant teams should be aware that strongyloidiasis iswidely distributed in many tropical and subtropicalareas of the world.
Migrants from these regions are expected topresent with high infection rates. The AmericanSociety of Transplantation recommends screeningof S. stercoralis in donors and recipients fromendemic areas with or without eosinophilia. Ifthese guidelines are followed rigorously, rapiddetection can prompt anthelminthic treatmentand decrease the risk of severe strongyloidiasis.As S. stercoralis infection is mostly chronic andasymptomatic, and as there is no ideal diagnostictest, strongyloidiasis still tends to be a diagnosti-cally elusive disease, even in the present era.However, newer diagnostic modalities, such asRT-PCR can be an effective tool for the earlydetection of transmission among solid organtransplant recipients.
Acknowledgements
None.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
Copyright © 2017 Wolters Kluwe
1087-2418 Copyright � 2017 Wolters Kluwer Health, Inc. All rights rese
REFERENCES AND RECOMMENDEDREADINGPapers of particular interest, published within the annual period of review, havebeen highlighted as:
& of special interest&& of outstanding interest1. Kikuchi T, Hino A, Tanaka T, et al. Genome-wide analyses of individualStrongyloides stercoralis (Nematoda: Rhabditoidea) provide insights intopopulation structure and reproductive life cycles. PLoS Negl Trop Dis2016; 10:e0005253.
2. Beknazarova M, Whiley H, Ross K. Strongyloidiasis: a disease of socio-economic disadvantage. Int J Environ Res Public Health 2016; 13:. doi:10.3390/ijerph13050517.
3. Kandi V, Bhatti A. Human strongyloidiasis: an insight in to a neglected tropicalparasitic disease. Transl Biomed 2015; 6:31.
4. Viney M. Strongyloides. Parasitology 2017; 144:259–262.5. CDC - DPDx - Strongyloidiasis. http://www.cdc.gov/dpdx/strongyloidiasis/
index.html. [Accessed 3 May 2016]6. Qu T, Yang Q, Yu M, et al. A fatal Strongyloides Stercoralis hyperinfection
syndrome in a patient with chronic kidney disease: a case report and literaturereview. Medicine (Baltimore) 2016; 95:e3638.
7. Segarra-Newnham M. Manifestations, diagnosis, and treatment of Strongy-loides stercoralis infection. Ann Pharmacother 2007; 41:1992–2001.
8. Schar F, Trostdorf U, Giardina F, et al. Strongyloides stercoralis: globaldistribution and risk factors. PLoS Negl Trop Dis 2013; 7:e2288.
9.&&
Geri G, Rabbat A, Mayaux J, et al. Strongyloides stercoralis hyperinfectionsyndrome: a case series and a review of the literature. Infection 2015;43:691–698.
A retrospective multicenter study of patients admitted to the ICU with SHS over a14-year period, this article identified clinical and biological characteristics as wellas key predictive factors of ICU mortality.10. Lam C, Tong M, Chan K, et al. Disseminated strongyloidiasis: a retrospective
study of clinical course and outcome. Eur J Clin Microbiol Infect Dis 2006;25:14–18.
11. Plata-Menchaca E, de Leon V, Pena-Romero A, et al. Pulmonary hemorrhagesecondary to disseminated strongyloidiasis in a patient with systemic lupuserythematosus. Case Rep Crit Care 2015; 2015:310185.
12. Rajamanickam A, Munisankar S, Bhootra Y, et al. Microbial translocationassociated with an acute-phase response and elevations in MMP-1, HO-1,and proinflammatory cytokines in Strongyloides stercoralis infection. InfectImmun 2017; 85:e00772–e00816.
13. Weatherhead J, Mejia R. Immune response to infection with Strongyloidesstercoralis in patients with infection and hyperinfection. Curr Trop Med Rep2014; 1:229–233.
14. Vadlamudi R, Chi D, Krishnaswamy G. Intestinal strongyloidiasis and hyper-infection syndrome. Clin Mol Allergy 2006; 4:8.
15. Iriemenam N, Sanyaolu A, Oyibo W, et al. Strongyloides stercoralis and theimmune response. Parasitol Int 2010; 59:9–14.
16. Anuradha R, Munisankar S, Dolla C, et al. Parasite antigen-specific regulationof Th1, Th2, and Th17 responses in Strongyloides stercoralis infection. JImmunol 2015; 195:2241–2250.
17.&
Anuradha R, Munisankar S, Bhootra Y, et al. Systemic cytokine profiles inStrongyloides stercoralis infection and alterations following treatment. InfectImmun 2015; 84:425–431.
This article discusses the role of innate and adaptive immunity in mediatingresistance to infection and provides insight into the profound alterations in thesystemic cytokine responses in patients with asymptomatic strongyloidiasis.18. Kim J, Kim D, Yoon Y, et al. Donor-derived strongyloidiasis infection in solid
organ transplant recipients: a review and pooled analysis. Transplant Proc2016; 48:2442–2449.
19. Le M, Ravin K, Hasan A, et al. Single donor-derived strongyloidiasis in threesolid organ transplant recipients: case series and review of the literature. Am JTransplant 2014; 14:1199–1206.
20. Vilela E, Clemente W, Mira R, et al. Strongyloides stercoralis hyperinfectionsyndrome after liver transplantation: case report and literature review. TransplInfect Dis 2009; 11:132–136.
21. Hamilton K, Abt P, Rosenbach M, et al. Donor-derived Strongyloides stercor-alis infection in renal transplant recipients. Transplantation 2011; 91:1019–1024.
22. Lichtenberger P, Doblecki-Lewis S. Strongyloidiasis in transplant recipients.http://www.antimicrobe.org/new/t31_dw.html.
23.&
Abanyie F, Gray E, Delli Carpini K, et al. Donor-derived Strongyloidesstercoralis infection in solid organ transplant recipients in the United States,2009–2013. Am J Transplant 2015; 15:1369–1375.
Providing a perspective on donor-derived strongyloidiasis and targeted donorscreening, the authors discuss in detail the experience of major organ procurementorganizations.24. Hays R, Thompson F, Esterman A, et al. Strongyloides stercoralis, eosino-
philia, and type 2 diabetes mellitus: the predictive value of eosinophilia in thediagnosis of S. stercoralis infection in an endemic community. Open ForumInfect Dis 2016; 3:ofw029.
r Health, Inc. All rights reserved.
rved. www.co-transplantation.com 343

Infectious complications in transplantation
25.&
Buonfrate D, Formenti F, Perandin F. Novel approaches to the diagnosis ofStrongyloides stercoralis infection. Clin Microbiol Infect 2015; 21:543–552.
In this article, the authors present a wide range of strategies to screen anddiagnose strongyloidiasis in individual patients and for at-large endemic regions.The study also provides insight on monitoring of the cure in clinical cases and trials.26. Bisoffi Z, Buonfrate D, Sequi M, et al. Diagnostic accuracy of five serologic
tests for Strongyloides stercoralis infection. PLoS Negl Trop Dis 2014;8:e2640.
27. Dacal E, Saugar J, Soler T, et al. Parasitological versus molecular diagnosis ofstrongyloidiasis in serial stool samples: how many? J Helminthol 2017; 1–5.[Epub ahead of print]
28. Saugar J, Merino F, Martın-Rabadan P, et al. Application of real-time PCR forthe detection of Strongyloides spp. in clinical samples in a reference center inSpain. Acta Trop 2015; 142:20–25.
29. Becker S, Piraisoody N, Kramme S, et al. Real time PCR for detection ofStrongyloides stercoralis in human stool samples from Cote d’Ivoire: diag-nostic accuracy, inter-laboratory comparison and patterns of hookworm co-infection. Acta Trop 2015; 150:210–217.
30. Paula F, Malta F, Corral M, et al. Diagnosis of Strongyloides stercoralisinfection in immunocompromised patients by serological and molecularmethods. Rev Inst Med Trop Sao Paulo 2016; 58:63.
Copyright © 2017 Wolters Kluwer
344 www.co-transplantation.com
31. Pilotte N, Papaiakovou M, Grant J, et al. Improved PCR-based detection of soiltransmitted helminth infections using a next-generation sequencing approachto assay design. PLoS Negl Trop Dis 2016; 10:e0004578.
32. Gomez-Junyent J, Paredes-Zapata D, de las Parras ER, et al. Real-timepolymerase chain reaction in stool detects transmission of Strongyloidesstercoralis from an infected donor to solid organ transplant recipients. Am JTrop Med Hyg 2016; 94:897–899.
33.&&
Repetto S, Ruybal P, Solana M, et al. Comparison between PCR and larvaevisualization methods for diagnosis of Strongyloides stercoralis out of en-demic area: a proposed algorithm. Acta Trop 2016; 157:169–177.
An important article that proposes an early diagnostic algorithm for immunocom-promised patients at risk of developing SHS and DS.34. Barrett J, Newsholme W. Subcutaneous ivermectin use in the treatment of
severe Strongyloides stercoralis infection: two case reports and a discussionof the literature-authors’ response. J Antimicrob Chemother 2016; 71:220–225.
35.&&
Henriquez-Camacho C, Gotuzzo E, Echevarria J, et al. Ivermectin versusalbendazole or thiabendazole for Strongyloides stercoralis infection.Cochrane Database Syst Rev 2016; 1:1–50.
This article provides a comprehensive comparative review of various treatmentmodalities in strongyloidiasis in over 1100 patients, spanning more than 15 years.
Health, Inc. All rights reserved.
Volume 22 � Number 4 � August 2017