CNS INFECTION
41
CNS INFECTIONS Meningitis Encephalitis Brain Abscess BY : VISHRANT AMIN & FRIENDS
-
Upload
vishrant-amin -
Category
Education
-
view
108 -
download
1
Transcript of CNS INFECTION

CNS INFECTIONS
MeningitisEncephalitis
Brain Abscess
BY : VISHRANT AMIN & FRIENDS

COMMON CNS INFECTIONS BACTERIAL INFECTIONS
Bacterial meningitis Tuberculosis Brain abscess Lysteriosis Neurosyphilis
FUNGAL INFECTIONS Cryptococcal meningitis
VIRAL INFECTIONS
Viral meningitis Herpes simplex encephalitis Rabies
PARASITIC INFECTIOS Neurocysticercosis Toxoplasmosis

CASE• A seven year old boy presented to emergency department with high
grade fever on the previous day. He complained of headache, was disoriented and had projectile vomiting. On examination, the neck was found to be rigid and kerning’s sign was positive. A lumbar puncture was carried out along with complete blood counts and serum biochemistry. Cytology showed polymorphs at 1000/cumm,protein 250 mg/dl and glucose20 mg/dl. Blood glucose level normal.
• On gram stain, gram negative cocci seen in pairs, most of them inside polymorphs.
• The latex agglutination test was positive for N.Meningitidis antigen.

NORMAL ANATOMY OF MENINGIES

MENINGITISINTRODUCTION
Meningitis is an acute inflammation of the protective membranes ( collectively known as meninges) covering the brain and spinalcord.
Meningitis can be life threatening condition because of the inflammation proximity to the brain and spinal cord, therefore the condition is termed as MEDICAL EMERGENCY.

TYPES OF MENINGITIS
Bacterial meningitis Tuberculous meningitis Viral meningitisFungal meningitisParasitic meningitisNon-Infectious meningitis
MENINGITIS MAY BE
Acute meningitis < 4 weeksChronic meningitis > 4 weeks

CAUSATIVE ORGANISMS
BACTERIA
IN PREMATURE BABIES AND NEW BORNS(UPTO 3 MONTHS )
• Group B streptococci• Listeria Monocytogen
OLDER CHILDREN• N.Meningitidis• S.Pneumoniae• H.Influenzae type B
ADULTS• N.Meningitidis• S.Pneumoniae• Listeria Monocytogens
OTHER BACTERIA• Staphylococci• Mycobacterium Tuberculosis• Pseudomonas• Treponema Pallidium

VIRUSES• Enterovirus• Herpes simplex virus• Varicella-zoster virus• Mumps
PARASITE
• E.Histolytica• Naegleria• Acanthamoeba• T.gondii
FUNGI• Cryptococcus Neoformans• Coccidioides Immitis• Histoplasma Capsulatum• Blastomyces Dermatitidis• Candida Spp.
NON-INFECTIOUS CAUSES
• Malignant condition (cancer)• Certain Drugs(NSAIDS,Antibiotics)• SLE• Inflammatory conditions(sarcoidosis)
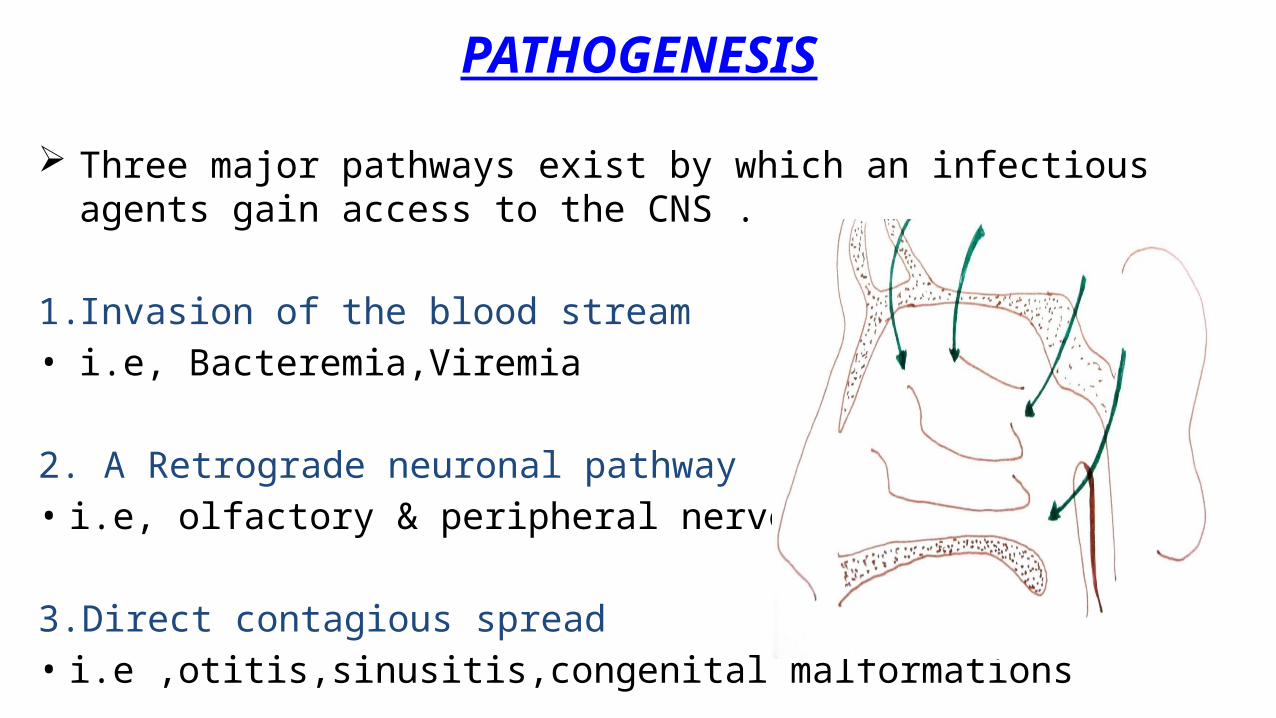
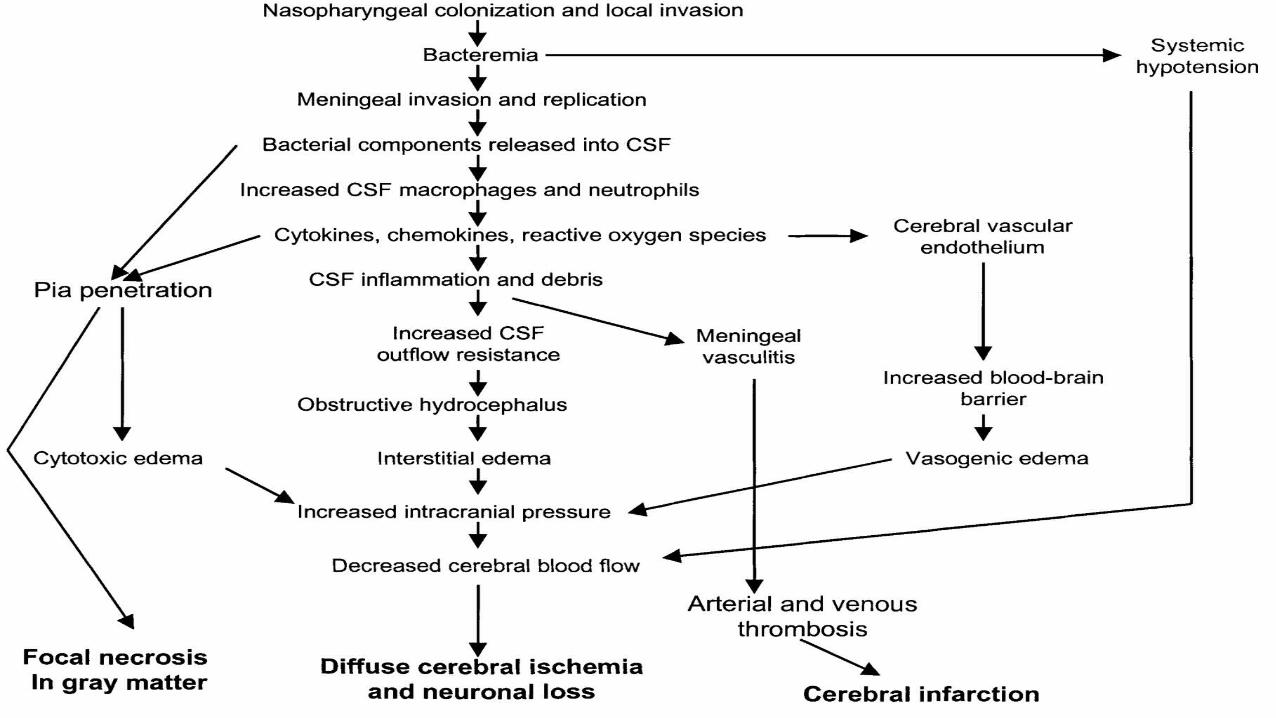
PATHOGENESIS
Three major pathways exist by which an infectious agents gain access to the CNS .
1. Invasion of the blood stream• i.e, Bacteremia,Viremia
2. A Retrograde neuronal pathway• i.e, olfactory & peripheral nerves
3.Direct contagious spread• i.e ,otitis,sinusitis,congenital malformations
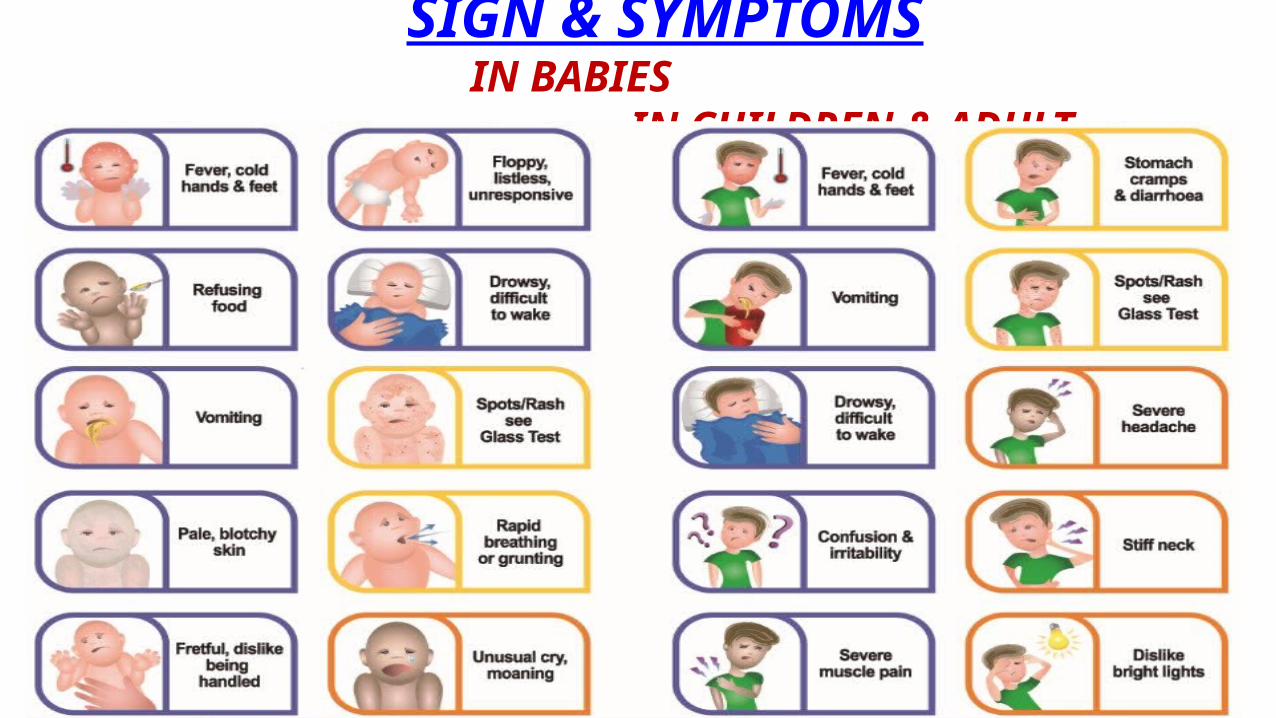
SIGN & SYMPTOMS IN BABIES IN CHILDREN & ADULT

KERNIG’S SIGN:It is assessed with the patient lying supine, with the hip and knee flexed to 90 degrees. In a patient with a positive kerning’s sign, pain limits passive extensions of the knee.
BRUDZINSKI SIGN:A positive brudzinki sign occurs when flexion of the neck causes involuntary flexion of the knee and hip.
COMPLICATIONS
Encephalitis Deafness Epilepsy Hydrocephalus Cognitive Deficits Loss of pupillary reflex Abnormal posture Decreased level of consciousness

LABORATORY DIAGNOSISSPECIMEN
CSF : By Lumbar puncture (L3-L4 level) See for the turbidity
Divide into 4 parts
For Microbiological Test For Pathological Test For Biochemical Test For Preservation
BLOOD serology & culture
URINE For antigen detection• S.Pneumoniae• C.Neoformans
MICROSCOPY STAINING GRAM’S STAIN:• N.Meningitidis : Intracellular, gram negative, diplococci• S.Pneumoniae : gram positive, diplococci(lanceolated shaped)• H.Influenzae : gram negative, pleomorphic, coccobacilli Z-N STAIN:• To demonstrate AFB along with LYMPHOCYTE (tuberculous meningitis) INDIAN INK: ( For demonstration of capsule of organisms)• C.Neoformans• S.Pneumoniae WET-MOUNT & GIEMSA STAIN : For Parasite QUELLANG REACTION:• C.Neoformans• S.Pneumoniae

CULTURE FOR BACTERIA: N.MENINGITIDIS: (1)ON SOLID MEDIA: - Blood agar Small,Translucent,Round,Convex, - Chocolate agar Bluish-Grey colour, Weak haemolysis - Muller-Hinton Agar - Thayer-Martin agar : selective media
(2) ON LIQUID MEDIA: - Turbidity with little or no surface growth
S.PNEUMONIAE: - BA Small,Dome-Shaped,Glistening with - CA an area of green discolouration ( α- haemolysis)
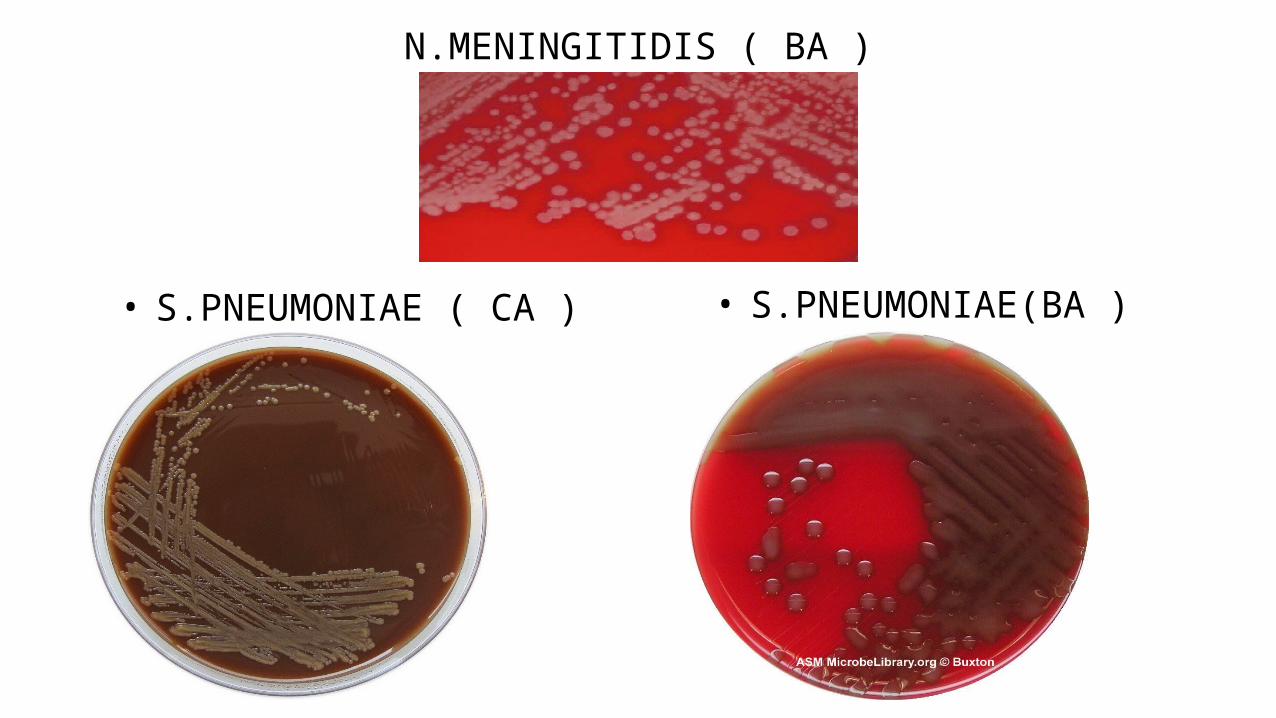
N.MENINGITIDIS ( BA )
• S.PNEUMONIAE ( CA ) • S.PNEUMONIAE(BA )

H.INFLUENZAE TYPE B• BA : Shows “SATELLITISM”• CHOCOLATE AGAR• LEVINTHAL’S AGAR: -Translucent colonies with distinctive
iridescence - Produced by capsulated strains • FIELD’S AGAR : Small, Opaque ,Short colonies
MYCOBACTERIUM TUBERCULOSIS : (TUBERCULOUS MENINGITIS)
L-J MEDIA : Dry,Rough,Irregular colonies
FOR VIRAL CULTURE : - Tissue culture - Egg Inoculation - Animal inoculation
FOR FUNGAL CULTURE - SDA - BHI - BIRD SEED AGAR

• L-J MEDIUM • H.INFLUENZAE

BIOCHEMICAL & PATHOLOGICAL FINDINGS IN CSF

BIOCHEMICAL REACTION
ORGANISM Catalase
TEST Oxidase TEST
Nitrate.R TEST
SUGARFERMENTATION
N.MENINGITIDIS + ve +ve -- ve
Glucose/maltose:Acid+NO GasLactose/Sucrose:NO Reaction
S.PNEUMONIAE -- Ve --ve -- -----
H.INFLUENZAE +ve +ve + ve Glucose/Xylose: AcidOther sugar : NO Acid
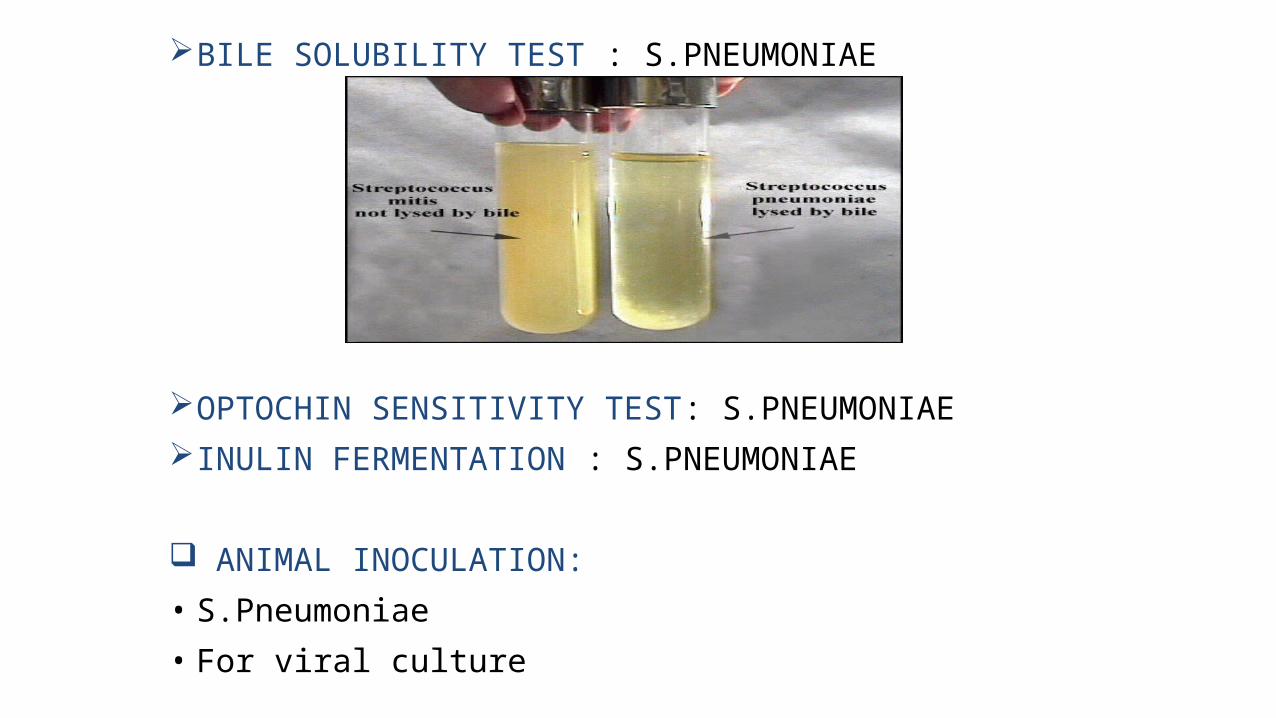
BILE SOLUBILITY TEST : S.PNEUMONIAE
OPTOCHIN SENSITIVITY TEST: S.PNEUMONIAE INULIN FERMENTATION : S.PNEUMONIAE
ANIMAL INOCULATION: • S.Pneumoniae • For viral culture

SEROLOGYFOR N.MENINGITIDIS (1)Slide Agglutination Test (2)Latex Agglutination Test (3)Haemagglutination Test
FOR S.PNEUMONIAE : (1) Latex Agglutination Test (2) Demonstration of SSS (3) Immunochromatography (4) CRP Test (biomarker) (5) Procalcitonin Level (biomarker)
FOR H.INFLUENZAE Latex agglutination testFOR L.MONOCYTOGENSC.NEOFORMANS
MOLECULAR METHOD : CSF- PCR
LIMULUS TEST : Test for rapid detection of meningitis that
is caused by Gram negative bacteria, which detects bacterial endotoxin.
PRINCIPLE: LAL( Limulus amebocyte lysate) is an aqueous extract of amoebocytes from horse shoe crab (Limulus polyphemus)
LAL reacts with bacterial endotoxin/ LPS which is membrane component of Gram negative bacteria.

ENCEPHALITIS
Encephalitis is defined as acute, diffuse inflammation of brain parenchyma, which leads to cerebral dysfunction.
Sometimes, it is associated with meningitis, which is known as Meningoencephalitisinfection may result in one of the two conditions affecting the brain.
PRIMARY ENCEPHALITIS
Occurs when a virus / other infectious agent infects the brain.
May be reactivation after previous illness
SECONDARY ENCEPHALITIS (POST INFECTIONAL ENCEPHALITIS)
It is faulty immune system reaction in response to a infection elsewhere in body.
Occurs 3 weeks after initial infection.

CAUSATIVE ORGANISM VIRUSES
HERPES VIRUS : HSV, EBV, VZV ENTEROVIRUS : Poliovirus & Coxsackievirus ARBOVIRUS - Japanese B virus - Western & Eastern equine virus - St. Louis virus - West Nile virus - La crosse virus RABIES VIRUS PARAMYXO VIRUS - Measles - Mumps
BACTERIA Legionella Pneumophilia Mycoplasma Pneumoniae Listeria Monocytogens
FUNGI Candida Spp. Cryptococcus Spp. Mucor
PARASITE Toxoplasma gondii Naegleria

SIGNS AND SYMPTOMS MILD ENCEPHALITIS - Fever - Poor Appetite - Headache - Weakness SEVERE ENCEPHALITIS - Stiff Neck - Mental confusion - High Fever - Disorientation - Severe headache - Convulsion - Memory loss - Problems with Speech - Hallucination - Coma IN INFANTS -Vomiting - Poor Appetite - Body stiffness - Poor memory
BRUDZINSKI SIGN: KERNING’S SIGN :

COMPLICATION
Paralysis Hearing & Vision defectsMemory Problems Speech impairment Lack of Muscle coordination Coma & Death

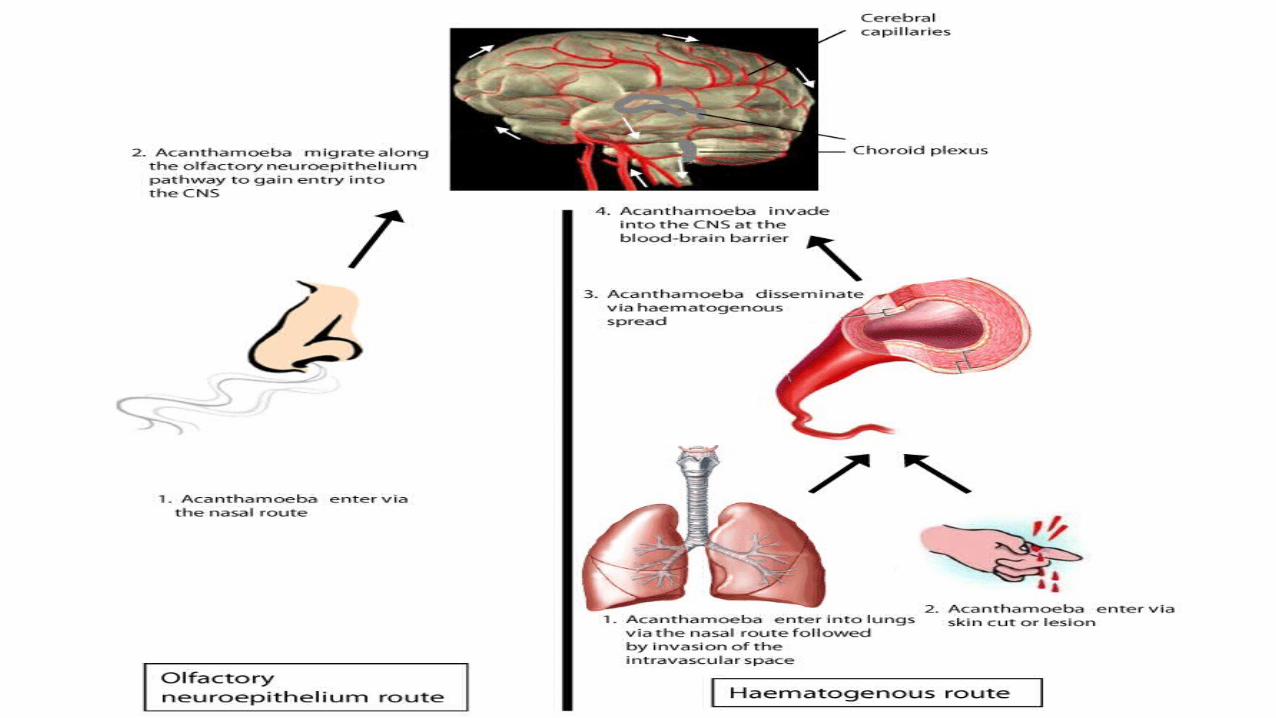
PATHOGENESIS Transmission into human depend on causative organism :• HSV & NAEGLERIA : Respiratory Tract• ARBOVIRUS : Vector ( Mosquito & Tick )• ACANTHAMOEBA : Eye & Nasal route• RABIES : Dog bite Spread to CNS : ( 3 Routes )1. Haematogenous Route2. Neuronal Route3. Contagious Route Damage to the Brain Parenchyma Causes Encephalitis

ENTEROVIRUS: JAPANESE ENCEPHALITIS:
Pathogenesis : Entry via aerosol or ingestion-> replicate in oro-pharynx-> replicate in Peyer's patches-> 1° viremia-> 2° viremia in tissues-> virus in feces

LABORATORY DIAGNOSISSPECIMENS: CSF 4. THROAT SWAB BLOOD 5. NASOPHARYNGEAL SWAB URINE
MICROSCOPY: VIRAL: Herpes virus: Tzank smear Multinucleated giant cells and Ground glass chromatin and giemsa stained smears and flurescent antibody techniqe Rabies virus: Negri bodies Measles: multinucleated giant cells in Giemsa stained smears BACTERIAL: Legionella pneumophilia: Legionella stains poorly with Gram stain, stains positive with silver Mycoplasma pneumoniae: Giemsa stain

3. FUNGAL: Candida spp.: Gram stain +ve Cryptococcus: India ink stain capsulated budding yeast cells
4.PARASITIC: Naegleria fowleri : wright or giemsa stain pink nuclei and blue cytoplasm Toxoplasma gondii: Periodic acid Schiff Bradyzoites are PAS +ve
CULTURE: VIRAL: Limited utility as culture may be insensitive BACTERIAL: Listeria monocytogens: Listeria grows on media such as Mueller-Hinton agar.
Identification is enhanced if the primary cultures are done on agar containing sheep blood, because the characteristic small zone of hemolysis can be observed around and under colonies.
Legionella pneumophilia: Cultured on charcoal yeast extract with iron & cysteine FUNGAL: Candida spp. & Cryptococcus: Sabouraud agar creamy white, smooth colony. PARASITIC: Naegleria fowleri: Non nutrient agar Plaques formation

SPINAL TAP: A spinal tap is done by inserting a needle into the spinal column. Another name for a spinal tap is a lumbar puncture. The CSF fluid taken during a spinal tap will also be tested to find the cause of encephalitis. It may show which type of virus or germ is causing the inflammation.
ISOLATION OF VIRUS: HSV : Human Diploid Fibroblast – Typical CPE ( 24-48 hrs) RABIES : CPE is minimal so by Immunofluorescence ARBOVIRUS : Vero,BHK-21 & Mosquito cell line ( Immunofluorescence)
SEROLOGY: DEMONSTRATION OF IgM ANTIBODY IMMUNOFLUORESCENCE ELISA LATEX AGGLUTINATION TESTMOLECULAR METHOD: PCR.

BRAIN ABSCESS Brain abscess (or cerebral abscess) is an abscess caused by inflammation and
collection of infected material, coming from local or remote infectious sources, within the brain tissue.
A).LOCAL SOURCES B). REMOTE SOURCES Ear infection, Dental abscess Lung, heart, kidney Infection of Paranasal sinuses Infection of the Mastoid air cells of the temporal bone, Epidural abscess
The infection may also be introduced through a skull fracture following a headtrauma or surgical procedures.
Brain abscess is usually associated with congenital heart disease in young children. It may occur at any age but is most frequent in the third decade of life.
CAUSATIVE ORGANISMSBACTERIA
• S.Aureus• S.Intermidius• Bacteroides• Fusobacterium• Enterobacteriaceae• Pseudomonas spp
LESS COMMON• N.Meningitidis• S.Pneumoniae• H.Influenzae
FUNGI
• Aspergillus• Candida• Cryptococcus• Mucor• Coccidioides• Histoplasma capsulatum• Blastomyces dermatitidis
PARASITE• Toxoplasma gondii• Entamoeba histolytica• Trypanosoma cruzi• Schistosoma

SIGN & SYMPTOMS
• Headache• Drowsiness• Fever• Confusion• Seizures• Speech difficulties• Hemiparesis

STAGES OF BRAIN ABSCESS
1. Early cerebritis2. Late cerebritis3. Early Capsule4. Late Capsule

RADIOLOGY IS IMPORTANT FOR DIAGNOSISOF ALL CNS INFECTION
CT-SCAN MRI CHEST X-RAY


![Pedia - CNS Infection, Seizures, NMD [Agrava]](https://static.fdocuments.in/doc/165x107/577cc6031a28aba7119d7e1e/pedia-cns-infection-seizures-nmd-agrava.jpg)