CMV infection of transplant recipients fileJournal of Hepatology ISSN 0168.8278 Liver...
11
Copyright 0 European Association for the Sfudy of the Liver 1996 Journal of Hepatology ISSN 0168.8278 Liver Transplantation: Special Article CMV infection of transplant recipients David Mutimer Condtant Physician, Liver and Hepatobiliary Unit, Queen Elizabeth Hospital, Birmingham, UK C YTOMEGALOVIRUS (CMV) LlSUdly CiXlSeS ZiSyIllptO- matic or clinically insignificant infection in the immunocompetent host. Thereafter, the virus persists in a latent state, but may be reactivated by immuno- suppression. Reactivation of latent infection most commonly occurs in the context of Human Immunodeficiency Virus (HIV) infection and allogeneic organ transplan- tation, but has also been described in other settings. Chronic liver disease may be associated with reac- tivation of CMV. Tanaka et al. detected CMV DNA by polymerase chain reaction (PCR) in the blood of 77/122 (63.1%) patients with hepatic cirrhosis, but only l/40 normal controls was PCR-positive (1). In the same study, PCR-positive patients with cirrhosis were antigenaemia assay-negative (the antigenaemia assay employs immunological methods to detect CMV-encoded antigens in peripheral blood smears). In cirrhotic patients, PCR-positivity was associated with worse liver dysfunction and with greater sup- pression of cellular immune responses. Using PCR, CMV DNA has also been detected in the blood of 23/25 septic patients on an Intensive Care Unit (ICU), but not in controls (2). Despite virological evidence of CMV reactivation in these patient groups (cirrhotic patients and septic patients), symptomatic infection did not develop. This suggests that other factors are required for the development of CMV-associated disease. Donor vi- rus is clearly the most important factor. Symptomatic infection of transplant recipients is usually associated with donor seropositivity, and is a consequence of the acquisition of donor CMV strain in the context of im- munosuppression. When the recipient is seronega- Correspondence: David Mutimer, Consultant Physician, Liver and Hepatobiliary Unit, Queen Elizabeth Hospital, Birmingham, UK. Tel. 0121 627 2337. tive, then primary infection occurs on a background of immunosuppression, and this infection is likely to be symptomatic. In seropositive recipients, symptomatic infection is usually associated with excretion of the donor strain. The importance of donor CMV strain in deter- mining the manifestations of CMV infection in trans- plant recipients was shown by Grundy et al. and by Chou. Of 74 renal transplant recipients in the study of Grundy et al., 51 were seropositive pre-transplant, and symptomatic infection only developed in those with seropositive donors (3). Consistent with this ob- servation, CMV strains with identical restriction en- zyme analyses have been isolated from organ recipi- ents with a common donor (3,4). Primary exposure to CMV does not, however, in- variably result in infection. Chou examined nine pairs of seronegative transplant recipients who were ex- posed to nine seropositive donors. Four pairs sero- converted (and excreted virus), but five pairs re- mained uninfected (4). This observation supports the hypothesis that donor strain is the principal determi- nant of recipient infection, and also suggests that all seropositive donors are not equally infectious. CMV infection in liver transplantation - inci- dence and risk factors CMV infection has been reported in 30% to 50% of liver transplant recipients. In the same series, 12% to 25% of patients had symptomatic infection (also known as CMV disease) (refs. 5-13). A higher inci- dence of infection will be reported if prospective virological surveillance is undertaken. In Birming- ham, the incidence of symptomatic infection is 12%. The incidence of CMV infection (including sympto- matic and asymptomatic) in Birmingham recipients is 50%. The likelihood of infection and disease depends on 259
Transcript of CMV infection of transplant recipients fileJournal of Hepatology ISSN 0168.8278 Liver...
Copyright 0 European Association
for the Sfudy of the Liver 1996
Journal of Hepatology ISSN 0168.8278
Liver Transplantation: Special Article
CMV infection of transplant recipients
David Mutimer
Condtant Physician, Liver and Hepatobiliary Unit, Queen Elizabeth Hospital, Birmingham, UK
C YTOMEGALOVIRUS (CMV) LlSUdly CiXlSeS ZiSyIllptO-
matic or clinically insignificant infection in the immunocompetent host. Thereafter, the virus persists in a latent state, but may be reactivated by immuno- suppression.
Reactivation of latent infection most commonly occurs in the context of Human Immunodeficiency Virus (HIV) infection and allogeneic organ transplan- tation, but has also been described in other settings.
Chronic liver disease may be associated with reac- tivation of CMV. Tanaka et al. detected CMV DNA by polymerase chain reaction (PCR) in the blood of 77/122 (63.1%) patients with hepatic cirrhosis, but only l/40 normal controls was PCR-positive (1). In the same study, PCR-positive patients with cirrhosis were antigenaemia assay-negative (the antigenaemia assay employs immunological methods to detect CMV-encoded antigens in peripheral blood smears). In cirrhotic patients, PCR-positivity was associated with worse liver dysfunction and with greater sup- pression of cellular immune responses.
Using PCR, CMV DNA has also been detected in the blood of 23/25 septic patients on an Intensive Care Unit (ICU), but not in controls (2).
Despite virological evidence of CMV reactivation in these patient groups (cirrhotic patients and septic patients), symptomatic infection did not develop.
This suggests that other factors are required for the development of CMV-associated disease. Donor vi- rus is clearly the most important factor. Symptomatic infection of transplant recipients is usually associated with donor seropositivity, and is a consequence of the acquisition of donor CMV strain in the context of im- munosuppression. When the recipient is seronega-
Correspondence: David Mutimer, Consultant Physician, Liver and Hepatobiliary Unit, Queen Elizabeth Hospital, Birmingham, UK. Tel. 0121 627 2337.
tive, then primary infection occurs on a background of immunosuppression, and this infection is likely to be symptomatic.
In seropositive recipients, symptomatic infection is usually associated with excretion of the donor strain. The importance of donor CMV strain in deter- mining the manifestations of CMV infection in trans- plant recipients was shown by Grundy et al. and by Chou. Of 74 renal transplant recipients in the study of Grundy et al., 51 were seropositive pre-transplant, and symptomatic infection only developed in those with seropositive donors (3). Consistent with this ob- servation, CMV strains with identical restriction en- zyme analyses have been isolated from organ recipi- ents with a common donor (3,4).
Primary exposure to CMV does not, however, in- variably result in infection. Chou examined nine pairs of seronegative transplant recipients who were ex- posed to nine seropositive donors. Four pairs sero- converted (and excreted virus), but five pairs re- mained uninfected (4). This observation supports the hypothesis that donor strain is the principal determi- nant of recipient infection, and also suggests that all seropositive donors are not equally infectious.
CMV infection in liver transplantation - inci- dence and risk factors CMV infection has been reported in 30% to 50% of liver transplant recipients. In the same series, 12% to 25% of patients had symptomatic infection (also known as CMV disease) (refs. 5-13). A higher inci- dence of infection will be reported if prospective virological surveillance is undertaken. In Birming- ham, the incidence of symptomatic infection is 12%. The incidence of CMV infection (including sympto- matic and asymptomatic) in Birmingham recipients is 50%.
The likelihood of infection and disease depends on
259

D. Mutimer
the serological status of donor and recipient. Infec- tion is principally dependent on organ donor seropos- itivity. When the donor is seropositive, then disease is more likely to develop in a seronegative recipient. The incidence of symptomatic infection in recipients with primary exposure ranges from 50% to 90% (1 l- 13). The seronegative recipient of a liver from a se- ronegative donor has the lowest risk of symptomatic infection (13% to 22% in the same series).
Other risk factors for CMV infection and disease are detailed in Table 1.
Conventional diagnostic techniques Viral culture
Human fibroblasts (MRC-5) cells are most com- monly used for viral culture. Following inoculation, classic cytopathic effect is usually recognised within 2 to 3 weeks, but may take as long as 6 weeks to develop. This delay limits the application of conven- tional viral culture to clinical practice.
Early detection of CMV in cell culture can be achieved by modifications of the traditional tech- nique. Such modifications include the use of immun- ofluorescence to identify viral antigens in cell culture. DEAFF (detection of early antigen fluorescent foci) detects CMV prior to development of classic cytopa- thy. DEAFF and conventional viral culture appear to have equivalent sensitivities for CMV detection (14).
Centrifugal enhancement of viral culture is a rela- tively specific property of CMV. Centrifugation cul- ture and immunohistology have been combined (in a technique known as “shell vial culture”) to confirm CMV infection at a very early stage. It has been sug- gested that shell vial culture is more sensitive for vi- ral detection than conventional culture (15), but in other laboratories the converse has been found (16).
When viral culture is employed for CMV surveil- lance following transplantation, then blood and urine are most often examined. Isolation of CMV prior to the development of symptoms requires a rapid cul- ture technique. Urine specimens are more frequently culture positive, but the predictive value of urine cul-
TABLE 1
Risk factors for CMV infection and disease (and references)
Pretransplant diagnosis of fuhninant hepatic failure (7,ll) Pretransplant diagnosis of malignancy when pre-operative treatment includes chemotherapy and radiotherapy (11) High operative requirement for blood and plasma (8) Acute cellular rejection (9) High dose corticosteroids (8) The use of OKT3 (7,10,13) Hepatic artery thrombosis (7)
ture positivity (for the development of symptomatic infection) is inferior to that of blood culture positivity (17). Isolation of CMV from blood is strongly associ- ated with symptomatic infection (8,16-l 9).
There is a tendency for virus to be isolated at an earlier stage from the specimens of symptomatic pa- tients than from asymptomatic patients (16,17,20). Nevertheless, and despite the application of rapid cul- ture techniques, many patients present with symp- toms prior to the isolation of CMV from surveillance specimens (8,16,17,19,21-23).
These observations explain the poor sensitivity (for identification of potentially symptomatic patients at a presymptomatic stage) of those strategies which target pre-emptive therapy at asymptomatic culture positive patients (21-23).
Serology Primary CMV infection may be associated with the development of an IgM antibody response. Reactiva- tion of CMV (or infection by another CMV strain) in a seropositive recipient may be associated with an increase in IgG titre. Seropositive organ recipients frequently exhibit an IgM response in association with CMV reactivation or superinfection. The suita- bility of IgM assays for surveillance and diagnosis of CMV infection in transplant recipients has been addressed in a number of studies. The following char- acteristics of the IgM response have been described. Despite concurrent immunosuppression, an IgM response is observed in nearly all patients with pri- mary CMV infection. An IgM response is observed in 26% to 55% of patients with reactivation or super- infection (24-27). An IgM response is observed in as many as 88% of patients with asymptomatic infection (16). The IgM response may be absent in patients with severe and overwhelming CMV infection (24) (28). IgM usually appears after the development of symptoms, and the interval from symptom onset to IgM positivity is characteristically 1 to 3 weeks (24) (29). IgM may appear earlier in reactivation infection than in primary infection (26). Viral culture positivity usually precedes the IgM response (assuming the application of rapid culture techniques). The timing of IgM appearance does not differ significantly between symptomatic and asymptomatic infection
(24).
Alternative diagnostic techniques Recognising the inadequacy of conventional virolog- ical techniques, two alternative diagnostic methods were introduced in the late 1980’s, and have been refined in the 1990’s.
260

CMV infection of transplant recipients
The “antigenaemia assay” is now routinely used by many diagnostic laboratories for the management of transplant recipients.
The antigenaemia assay detects and quantitates CMV-infected leukocytes in the peripheral blood. Buffy-coat smears are examined, and CMV-infected cells are identified by immunoperoxidase or APAAP (alkaline phosphatase/anti-alkaline phosphatase) la- belling after incubation with a mixture of CMV-spe- cific monoclonal antibodies. More than 80% of anti- gen-positive cells are polymorphs. As the number of antigen-positive cells increases, the development of symptoms becomes more likely.
The results of the antigenaemia assay are generally concordant with the results of blood viral culture (30,31), though discordance may be observed during antiviral therapy (30,32).
The assay is highly sensitive and specific for the diagnosis of CMV infection (as defined by culture and serology), but specificity and positive predictive value for the diagnosis of CMV disease are less im- pressive. In other words, patients with asymptomatic infection (who do not subsequently develop symp- toms) are frequently antigenaemia-positive.
Symptomatic infection is nearly always associated with a positive assay, and a negative assay effectively excludes CMV as the cause of symptoms (in evalua- tion of a pyrexial transplant patient). For this reason, the antigenaemia assay now has an established role for the confirmation of symptomatic CMV infection.
The antigenaemia assay is usually positive 1 to 2 weeks before a serological response is observed (3 1,33-36).
Unfortunately, the antigenaemia assay appears to have no role for surveillance of patients after trans- plantation. Surveillance specimens are frequently negative prior to the onset of symptoms, even when weekly monitoring is performed.
The antigenaemia assay cannot be recommended for routine surveillance of liver transplant recipients. Surveillance might, however, be appropriate in spe- cial circumstances e.g. monitoring the occasional pa- tient who requires prolonged hospitalisation for man- agement of septic complications.
PCR shares many of the assets and shortfalls of the antigenaemia assay. PCR is a sensitive and specific means of detecting viral nucleic acid, and has been applied to the detection of CMV DNA (and mRNA) in biological specimens.
CMV DNA has been detected by PCR in the blood of non-immunosuppressed seropositive blood donors (37,38). CMV DNA has also been detected in the blood of some ELISA-negative blood donors (50),
suggesting that ELISA might fail to identify some la- tently infected individuals. The sensitivity of the PCR varies enormously, and is dependent on: (a) method of substrate preparation, (b) primer selection and con- stitution, (c) thermal cycling conditions including cy- cle number, and (d) post-PCR detection steps. Nested PCR is more sensitive than single-round PCR. For example, exquisite sensitivity will be achieved when nested PCR is combined with a post-PCR detection technique such as Southern blotting or ELISA. In these circumstances it is often possible to detect a single copy of target DNA. When an extremely sensi- tive PCR is used for CMV detection, then the tech- nique will not differentiate immunosuppressed from non-immunosuppressed patients, and will not segre- gate immunosuppressed patients into non-infected, infected asymptomatic, and infected symptomatic groups. Therefore, the PCR assay required by the cli- nician managing transplant recipients must be rela- tively insensitive, and its ability to segregate these patient groups will be a direct function of that sensi- tivity. Disparate conclusions concerning the useful- ness of PCR in this clinical setting reflect the applica- tion of assays with different detection sensitivities.
This concept assumes that the PCR has a detection threshold for any given set of substrates and condi- tions. It also assumes that the detection threshold is relatively constant, and therefore reproducible. Un- fortunately the second assumption is untrue, and there is significant interassay variation in amplifica- tion efficiency. Problems of interpretation stemming from variable reaction efficiency can be partially overcome by the co-amplification of a known amount of standard DNA. An “internal” standard DNA may be used. The internal standard DNA sequence is near- ly identical to that of the substrate target DNA, but differs in such a way (e.g. introduction of a restriction site or a short unique sequence) that amplified stand- ard and amplified wild-type DNA can be differentiat- ed in a post-PCR step. A known amount of internal standard DNA is added to each PCR reaction. Re- duced PCR efficiency should result in a proportionate reduction of the two amplified species, so the ratio should be unchanged. This accounts for variable re- action efficiency, and most quantitative PCR assays are based on this principle.
Clinical studies of PCR in liver allograf recipients For the majority of published studies, buffy-coat has been separated from blood, and used as substrate for the PCR reaction (29,3944).
Plasma (29) and serum (42,44) have also been
261
D. Mutimer
used as substrate for the PCR. For detection of viral DNA in serum and plasma, nested PCR was used by Nyberg et al. (42), and by Schmidt et al. (29). Schmidt compared the results of serum nested ampli- fication with buffy-coat single round amplification (for evaluation of the same blood specimen), and found 97% concordance. The detection of CMV DNA in serum clearly requires the use of a more sen- sitive PCR (such as nested PCR), or the addition of a post-PCR detection step such as hybridisation with a radiolabelled probe (44).
PCR is clearly more sensitive than viral culture, and culture-positive buffy-coats are invariably PCR- positive (40,43,44). Schmidt et al. examined 264 specimens with both the antigenaemia assay and PCR, and found concordant results in 249 (94%) (29).
Buffy-coat PCR is nearly always positive at the time of symptom onset. Since false-negative results are not obtained at that time, sensitivity and negative predictive value of the PCR for the diagnosis of symptomatic infection are 100% (39,40,42). A posi- tive result may be obtained up to 3 weeks prior to symptom onset (44). As assay sensitivity increases, then specificity and positive predictive value (for the diagnosis of symptomatic infection) decrease. In the study of Nyberg et al., most (24/25) patients had at least one PCR-positive buffy-coat (42). The specifici- ty of the PCR (for symptomatic infection) in this study was only 8%.
Quantitation of CMV DNA by PCR CMV DNA can be quantified by PCR including a competitive internal standard CMV DNA sequence (45-48).
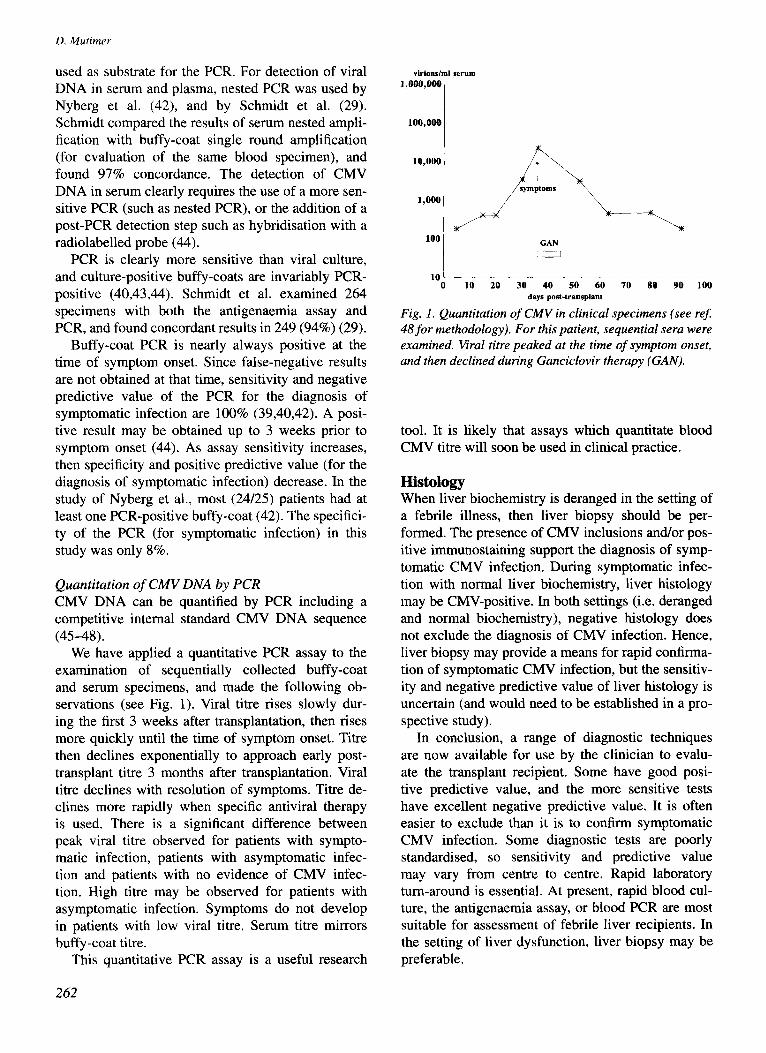
We have applied a quantitative PCR assay to the examination of sequentially collected buffy-coat and serum specimens, and made the following ob- servations (see Fig. 1). Viral titre rises slowly dur- ing the first 3 weeks after transplantation, then rises more quickly until the time of symptom onset. Titre then declines exponentially to approach early post- transplant titre 3 months after transplantation. Viral titre declines with resolution of symptoms. Titre de- clines more rapidly when specific antiviral therapy is used. There is a significant difference between peak viral titre observed for patients with sympto- matic infection, patients with asymptomatic infec- tion and patients with no evidence of CMV infec- tion. High titre may be observed for patients with asymptomatic infection. Symptoms do not develop in patients with low viral titre. Serum titre mirrors buffy-coat titre.
This quantitative PCR assay is a useful research
vkions/ml serum
1,000,000
100,000
10,000
1,000
GAN
1
10’ 0 10 20 30 40 50 60 70 80 90 100
days post-transplant
Fig. 1. Quantitation of CMV in clinical specimens (see rej
48 for methodology). For this patient, sequential sera were examined. Viral titre peaked at the time of symptom onset,
and then declined during Ganciclovir therapy (GAN).
tool. It is likely that assays which quantitate blood CMV titre will soon be used in clinical practice.
Histology When liver biochemistry is deranged in the setting of a febrile illness, then liver biopsy should be per- formed. The presence of CMV inclusions and/or pos- itive immunostaining support the diagnosis of symp- tomatic CMV infection. During symptomatic infec- tion with normal liver biochemistry, liver histology may be CMV-positive. In both settings (i.e. deranged and normal biochemistry), negative histology does not exclude the diagnosis of CMV infection. Hence, liver biopsy may provide a means for rapid confirma- tion of symptomatic CMV infection, but the sensitiv- ity and negative predictive value of liver histology is uncertain (and would need to be established in a pro- spective study).
In conclusion, a range of diagnostic techniques are now available for use by the clinician to evalu- ate the transplant recipient. Some have good posi- tive predictive value, and the more sensitive tests have excellent negative predictive value. It is often easier to exclude than it is to confirm symptomatic CMV infection. Some diagnostic tests are poorly standardised, so sensitivity and predictive value may vary from centre to centre. Rapid laboratory turn-around is essential. At present, rapid blood cul- ture, the antigenaemia assay, or blood PCR are most suitable for assessment of febrile liver recipients. In the setting of liver dysfunction, liver biopsy may be preferable.
262
Prevention of CMV infection (strategies employed for liver transplant recipients) Passive immunoprophylaxis with polyvalent or high- titre anti-CMV (hyperimmune) human immunoglob- ulin, Acyclovir, and Ganciclovir have been used to prevent CMV infection in liver ~anspl~t recipients. These agents have also been used in combination. Approaches to prophylaxis include: l treatment of all recipients (excluding seronegative
recipients of seronegative organs in some studies) from the time of transplantation,
l treatment of high-risk patients, such as those with primary CMV exposure (49-5 1) and those receiv- ing 0KT3 (52), and
l pre-emptive treatment targeted by surveillance cultures (22).
Passive immunoprophylaxis Snydman et al. conducted a randomised, placebo- controlled, double-blind study of CMV hyperim- mune globulin prophylaxis for liver recipients (10). In that study, treatment with hyperimmune globulin was associated with a reduced incidence (compared with placebo) of symptomatic CMV infection, and with fewer CMV-associated deaths (however, the magnitude of these beneficial effects did not achieve statistical significance). Prophylaxis was also associ- ated with a statistically significant reduction in the incidence of CMV-associated fungal infection. Compared with other donor/recipient serological pairings, the study demonstrated little beneficial effect for seronegative recipients of seropositive organs.
Saliba et al, conducted a prospective, randomised, controlled study of CMV hyperimmune globulin prophylaxis for seronegative liver recipients (50). Prophylaxis was associated with a reduced incidence of CMV disease in recipients of seropositive organs
TABLE 2
CMV infection of transplant recipients
(4/15), but primary exposure was associated with a very high incidence of symptomatic infection in the control group of this study (6/7).
Recently, the use of immune globulin to prevent symptomatic infection was examined by meta-analy- sis (53). The analysis concluded that: l published results suggest that immune globulin
reduces the incidence of symptomatic infection, l a beneficial effect is observed in recipients with
primary exposure, and l hyperimmune products are not clearly superior to
the polyvalent preparations. I~unoglobulin has been used in combination
with Acyclovir (51-56), and with Ganciclovir (56,57).
In conclusion, a reduction of symptomatic CMV infection can be achieved by passive i~unoprophy- laxis. The mechanism of protection is unclear, and may be independent of the titre of neutralising anti- CMV antibodies. The observed reduction of severe CMV-associated disease (principally CMV-associat- ed fungal infection) is intriguing, but may be inde- pendent of the anti-CMV activity of the preparation.
Acyclovir Compared with Herpes Simplex Virus (HSV), CMV is resistant to Acyclovir. CMV does not encode the thymidine kinase required for monophosphorylation of Acyclovir. Thus, acyclovir should not be used for treatment of established symptomatic infection, but the work of Balfour et al. suggested that high-dose Acyclovir (800 mg qid for patients with normal renal function) may provide effective prophylaxis against CMV in solid organ recipients (58).
Prospective analyses in liver recipients suggest that prophylaxis with high-dose Acyclovir is: l more effective than the combination of short-term
Ganciclovir and i~unoglobulin (57),
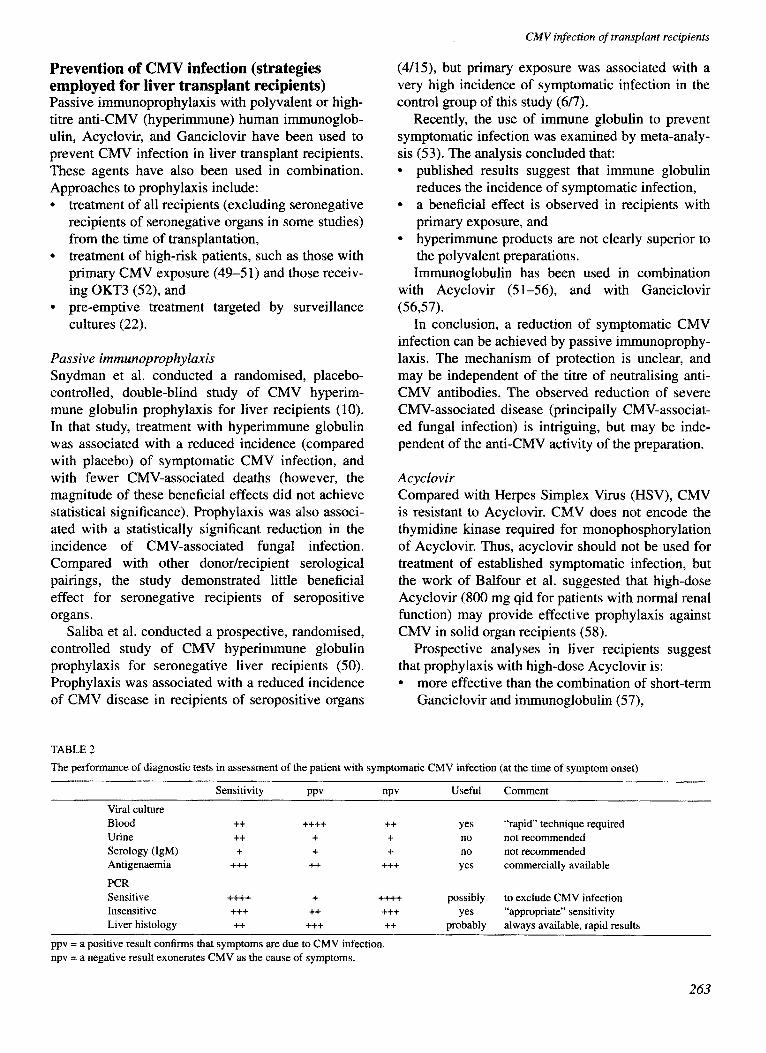
The performance of diagnostic tests in assessment of the patient with symptomatic CMV infection (at the time of symptom onset)
Sensitivity PPV uPv
Viral culture Blood ++ ++++ * Urine ++ + + Serology (IgM) + + + Antigenaemia +++ ++ +++
PCR Sensitive ++++ f ++++ Insensitive +++ ++ +++ Liver histology ++ +++ ++
ppv = a Positive result confirms that symptoms are due to CMV infection. npv = a negative result exonerates CMV as the cause of symptoms.
Useful Comment
yes “rapid” t~hnique required no not recommended no not recommended
yes commercially available
Possibly to exclude CMV infection
yes “appropriate” sensitivity probably always available, rapid results
263

D. Mutimer
l less effective than prolonged Ganciclovir prophy- laxis (59),
l inferior to a strategy based on pre-emptive Ganci- clovir treatment of asymptomatic culture-positive recipients (22).
Retrospective analyses suggest that high-dose Acy- clovir prophylaxis is: l better than no prophylaxis (54,55), l superior to low-dose Acyclovir (60), and l inferior to sequential GanciclovirYhigh-dose Acy-
clovir prophylaxis (56,60). When combined with immunoglobulin, low-dose
Acyclovir may decrease the incidence of symptomat- ic CMV infection in patients with primary CMV ex- posure (5 1).
Ganciclovir
Ganciclovir prophylaxis can prevent symptomatic CMV infection in liver transplant recipients (59). Winston et al. compared Ganciclovir with high-dose Acyclovir. Ganciclovir was given at a dose of 6 mg/ kg, starting on the first post-transplant day, then daily until day 30. The same dose was then administered 5 times per week until day 100. CMV infection was observed in 6/124 Ganciclovir-treated patients (cf. 48/126 Acyclovir-treated patients), and only one patient developed symptomatic infection (cf. 12 Acy- clovir-treated patients). Central venous access was required for Ganciclovir administration for the dura- tion of prophylaxis. One assumes that this therapy was administered and monitored in outpatients and at home. The strategy is remarkable for the lack of mor- bidity associated with maintenance of venous access for this duration. In the United Kingdom, the cost of Ganciclovir required for this protocol is nearly &3,000 per 70-kg patient. The cost of administering the protocol is probably significantly greater.
Despite this convincing demonstration that symp- tomatic CMV infection is a preventable disease, few transplant groups are likely to adopt this protocol. Nevertheless, this study would have implications for CMV prophylaxis if oral Ganciclovir proves to be ef- ficacious
In a prospective, randomised study including sero- positive recipients and recipients with seropositive donors, Cohen et al. failed to reduce the incidence of symptomatic infection by administration of prophy- lactic Ganciclovir during the third and fourth post- transplant weeks (61).
More selective prescription of intravenous Ganci- clovir can reduce the incidence of symptomatic infec- tion. In the only study of its type conducted in liver recipients, Singh et al. targeted asymptomatic pa-
tients with positive surveillance cultures for pre-emp- tive treatment with Ganciclovir (22). Consistent with the results of similar studies performed in bone mar- row recipients (21,23), this approach lacks sensitivity for the presymptomatic identification of potentially symptomatic patients. The results of the study sug- gest that symptomatic infection can be reduced by approximately 50%, and that one patient receives un- necessary pre-emptive treatment for each patient cor- rectly targeted (i.e. positive predictive value of a pos- itive surveillance culture is approximately 50%). These remarkable results were achieved despite rela- tively infrequent surveillance sampling (only four samples in the first 8 post-transplant weeks) required by protocol. The strategy needs independent valida- tion.
The potential of other surveillance techniques to target high-risk patients correctly should also be ex- plored.
In conclusion, no prophylactic strategy can be rec- ommended. The strategy adopted by a Unit should be commensurate with the incidence of symptomatic CMV infection observed in that Unit. For most Units, the incidence of serious CMV infection is decreasing. In Birmingham, the incidence of symptomatic infec- tion is 12%, and pneumonitis affects fewer than 2% (and mechanical ventilation has not been required for many years). This low incidence of infection is ob- served without prophylaxis. The protocol of Winston et al. is clearly unsuitable for our programme.
The medical literature will be biased by the publi- cation of studies with positive results. Strategies should be validated by controlled study before being adopted. Cost-benefit analysis should be an integral part of any strategy development.
Association of CMY infection with bacterial and fungal sepsis An association of CMV infection with bacterial and fungal sepsis in renal (62) and cardiac (63) transplan- tation was recognised in the 1970’s, before the wide- spread application of liver transplantation.
More recently, Smyth et al. confirmed this associa- tion of pulmonary bacterial infection with CMV in- fection and CMV pneumonitis in heart/lung recipi- ents (64).
In an early report of the Pittsburgh experience, Singh et al. recognised the association of disseminat- ed CMV infection with serious bacterial and fungal infection in patients who died after liver transplanta- tion (13).
Bronsther et al. reported 17 cases of CMV hepatitis, and 8/17 died with bacterial and fungal sepsis (65).
264

CMV infection of transplant recipients
George et al. analysed the results of Ganciclovir treatment of 17 liver recipients with CMV pneumoni- tis (66). In this series 11 patients died, and six died with fungal and bacterial sepsis. Four patients had he- patic artery thrombosis.
In a carefully performed prospective study, Paya et al. also found an association of hepatic artery throm- bosis with CMV infection in liver transplant recipi- ents (7).
Stratta et al. reported their experience with Ganci- clovir treatment of CMV disease complicating liver transplantation (67). One hundred and three patients were treated, and 22 died. Seventeen of these died with bacterial and fungal sepsis.
Harbison et al. also reported their initial experi- ence with Ganciclovir treatment of nine liver recipi- ents (68). Six of nine patients had bacterial infection of the abdominal cavity and/or biliary tree. Three of nine patients had persistent CMV infection despite Ganciclovir treatment. Refractory CMV infection was associated with persistent abdominal abscess for- mation.
Mor et al. examined the results of high dose Acy- clovir and immunoglobulin prophylaxis for liver re- cipients (54). CMV infection was associated with the deaths of seven patients in that study, and all seven died with invasive Can&da infection.
CMV infection is clearly associated with serious bacterial and fungal infection, and this association merits further examination.
Does viral infection predispose to bacterial and fungal infection? Paya et al. undertook a multivariate time-dependent analysis of risk factors for bacterial and CMV infection (7). In multivariate analysis, asymptomatic CMV infection was a risk factor for bacterial infection, though the mechanism of this as- sociation was unclear.
In that study, risk factors for symptomatic CMV infection included thrombosis of the hepatic artery. Arterial thrombosis is almost invariably associated with severe and refractory bacterial biliary (intrahe- patic and extrahepatic) sepsis.
Other studies suggest that bacterial sepsis pre- cedes (and predisposes to) CMV infection. For in- stance, Harbison et al. described six patients with bacterial infection of the biliary tree and abdominal cavity preceding the onset of symptomatic CMV in- fection (68). Indeed, serious bacterial complications usually involve the biliary anastomosis, and fre- quently have an ischaemic basis. Biliary complica- tions usually present in the first post-operative month, and symptomatic CMV infection usually de- velops in the second and third post-operative
months. It is easier to reconcile these observations with the hypothesis that bacterial infection predis- poses to CMV infection and not vice versa. Alterna- tively, bacterial and viral sepsis may be associated but not causally related.
At least two groups of investigators have sug- gested that bacterial infection predisposes to CMV infection, and that tumour necrosis factor alpha (TNF-alpha) may mediate that predisposition (69- 71). Stein et al. used a transfected human monocyte cell line to demonstrate that TNF-alpha acts on an enhancer sequence to stimulate transcription of the CMV immediate early gene (72). The same investi- gators later showed an association of raised serum TNF-alpha with the subsequent development of CMV antigenaemia in solid organ transplant recipi- ents (70).
Bacterial sepsis has also been associated with evi- dence of CMV replication in non-immunosuppressed patients (2).
CMV infection in patients with fulminant hepatic failure undergoing liver transplanta- tion A pre-transplant diagnosis of fulminant hepatic fail- ure may also predispose liver recipients to the subse- quent development of CMV infection. Paya et al. examined risk factors for CMV infection in a cohort of 79 consecutive liver recipients (7). A diagnosis of FHF emerged as a significant risk factor for CMV infection. That cohort included seven patients with FHF due to seronegative hepatitis, and 5/7 developed symptomatic infection.
In a preliminary report of Ganciclovir treatment for symptomatic CMV infection complicating liver transplantation, 4/9 patients were grafted for FHF (68). One of these recipients had CMV isolated from blood culture 2 days prior to transplantation. Stratta et al. observed an increased incidence of CMV infec- tion in patients transplanted for FHF (11). The inci- dence of CMV infection in patients transplanted at their centre was 34.6%, but in patients grafted for FHF the incidence was 57.9% (1 l/19).
TNF-alpha might also mediate the association of FHF with CMV infection. Sheron et al. observed very high levels of TNF-alpha in the serum of pa- tients with FHF (73). The highest levels of TNF-al- pha were observed in patients who subsequently died (a group similar to those who would be considered candidates for liver transplantation).
An inverse correlation between TNF-alpha and in- terleukin-2 production by monocytes was also ob- served. IL-2 is required for clonal expansion of T and
265

D. Mutimer
B cells. Impaired immune responses to CMV infec- tion might be observed in the setting of conditions as- sociated with enhanced secretion of TNF-alpha.
CMV infection and liver graft dysfunction The patient with symptomatic CMV infection is febrile, and disease may affect a single system (e.g. pneumonitis or colitis). The liver may appear to be the principal focus of infection, and symptomatic infection with deranged liver function is usually labelled CMV hepatitis. Biochemical derangement is usually mild, and CMV hepatitis does not cause acute liver failure.
During symptomatic infection, liver biopsy fre- quently contains CMV inclusions and microabscess- es, even when liver biochemistry is normal. In a pa- tient with graft dysfunction, the presence of inclu- sions does not imply that dysfunction is due to CMV infection, and does not necessarily predict the subse- quent development of symptomatic CMV infection.
Retrospective studies have suggested that donor/ recipient HLA-DR matching is associated with an in- creased incidence of CMV hepatitis (74) and with the development of a form of chronic graft rejection known as the vanishing bile duct syndrome (VBDS) (74,75). CMV infection (defined by serology) (75) and primary CMV exposure (seropositive donor for seronegative recipient) (76) may also be associated with an increased incidence of VBDS. However, analysis of prospectively collected virological data by Paya et al. failed to confirm the association of CMV infection with HLA matching and development of VBDS (77).
The development of VBDS might be determined by a reduction of immunosuppression consequent up- on the diagnosis of symptomatic CMV infection. Most physicians reduce immunosuppression in this setting, and azathioprine is frequently stopped in re- sponse to leukopenia. Candinas et al. observed an in- creased incidence of VBDS in patients who stopped azathioprine within the first 3 months (76).
Conclusions CMV infection causes significant morbidity in a minority of patients. CMV rarely causes the death of liver transplant recipients. Instead, the patient who dies after liver transplantation usually succumbs to infection with multiple organisms (viral, bacterial and fungal) in the setting of multiple organ failure. Such patients frequently had poor preoperative condition, with advanced cirrhosis or fulminant hepatic failure.
Post-transplant CMV surveillance should only be undertaken if a positive result precipitates pre-emp-
266
tive therapy. Despite the encouraging results of a sin- gle study, a role for routine surveillance and pre-emp- tive therapy remains unproven. Evaluation of a fe- brile patient requires the application of rapid diagnos- tic tests, such as the antigenaemia assay or PCR. These tests are sensitive, and have good negative pre- dictive value. A negative result effectively excludes significant CMV infection. A positive result must be interpreted in the context of clinical features and oth- er microbiology.
At present, antiviral prophylaxis should be re- served for high-risk patients, and probably requires the prolonged administration of Ganciclovir.
References 1.
2.
3.
4.
5.
6.
7.
8.
9
10.
11.
Tanaka S, Toh Y, Minagawa H, Mori R, Sugimachi K, Mina- mishima Y. Reactivation of Cytomegalovirus in patients with cirrhosis: analysisof 122cases.Hepatology 1992; 16: 1409-14. Docke WD, Prosch S, Fietze E, Kimel V, Zuckerman H, Klug C, Syrbe U, Kruger DH, von Baebr R, Volk HD. Cy- tomegalovirus reactivation and tumour necrosis factor. Lan- cet 1994; 343: 268-9. Grundy JE, Lui SF, Super M, Berry NJ, Sweny P, Fernando ON, Moorhead J, Griffiths PD. Symptomatic Cytomegalovi- rus infection in seropositive kidney recipients: reinfection with donor virus rather than reactivation of recipient virus. Lancet 1988; ii: 132-5. Chou S. Acquisition of donor strains of Cytomegalovirus by renal-transplant recipients. NEJM 1986; 314: 1418-23. Breinig MK, Zitelli B, Starzl TE, Ho M. Epstein-Barr virus, Cytomegalovirus, and other viral infections in children after liver transplantation. J Infect Dis 1987; 156: 273-9. Gorensek MJ, Carey WD, Vogt D, Goormastic M. A multi- variate analysis of risk factors for Cytomegalovirus infection in liver transplant recipients. Gastroenterology 1990; 98: 1326-32. Paya CV, Wiesner RH, Hermans PE, Larson-Keller JJ, Il- strup DM, Krom RAF, Rettke S, Smith TF. Risk factors for Cytomegalovirus and severe bacterial infections following liver transplantation: a prospective multivariate time-de- pendent analysis. J Hepatol 1993; 18: 185-95. Pillay D, Charman H, Burroughs AK, Smith M, Rolles K, Griffiths PD. Surveillance for CMV infection in orthotopic liver transplant recipients. Transplantation 1992; 53: 1261-5. Savage LH, Gonwa TA, Goldstein RM, Husberg BS, Klint- malm GB. Cytomegalovirus infection in orthotopic liver transplantation. Transplant Int 1989; 2: 96-101. Snydman DR, Werner BG, Dougherty NN, Griffith J, Rubin RH, Dienstag JL, Rohrer RH, Freeman R, Jenkins R, Lewis D, Hammer S, O’Rourke E, Grady GF, Fawaz K, Kaplan MM, Hoffman MA, Katz AT, Doran M. Cytomegalovirus immune globulin prophylaxis in liver transplantation. Ann Intern Med 1993; 119: 984-91. Stratta RJ, Shaefer MS, Markin RS, Wood RP, Kennedy EM, Langnas AN, Reed EC, Woods GL, Donovan JP, Pillen TJ, Duckworth RM, Shaw Jr BW. Clinical patterns of Cytomeg- alovirus disease after liver transplantation. Arch Surg 1989; 124: 1443-50.

CMV infection of transplant recipients
12. Wiens M, Lefebre B, Blumhardt G, Schmidt CA, Lohmann R, Neuhaus P. Incidence and therapy of Cytomegalovirus disease after liver transplantation. Transplant Proc 1993; 25:
1985-6. 13. Singh N, Dummer JS, Kusne S, Breinig MK, Armstrong JA,
Makowka L, Starzl TE, Ho M. Infections with Cytomegalo- virus and other Herpes viruses in 121 liver transplant recipi- ents: transmission by donated organ and the effect of OKT3 antibodies. J Infect Dis 1988; 158: 124-31.
14. Pillay D, Griffiths PD. Diagnosis of Cytomegalovirus infec- tion: a review. Genitourinary Med 1992; 68: 183-8.
15. Miller MJ, Bovey S, Pado K, Bruckner DA, Wagar EA. Ap- plication of PCR to multiple specimen types for diagnosis of Cytomegalovirus infection: comparison with cell culture and shell vial assay. J Clin Microbial 1994; 32: 5-10.
16. Marsano L, Perrillo RP, Flye MW, Hanto DW, Spitzer ED, Thomas JR, Murray PR, Windus DW, Brunt EM, Starch GA. Comparison of culture and serology for the diagnosis of Cy- tomegalovirus infection in kidney and liver transplant recipi- ents. J Infect Dis 1990; 161: 454-61.
17. Pillay D, Ali AA, Liu SF, Kops E, Sweny P, Griffiths PD. The prognostic significance of positive CMV cultures during surveillance of renal transplant recipients. Transplantation 1993; 56: 103-8.
18. Martin M, Manez R, Linden P, Estores D, Torre-Cisneros J, Kusne S, Ondick L, Ptachcinski R, Irish W, Kisor D, Felser I, Rinaldo C, Stieber A, Fung J, Ho M, Simmons R, Starzl T. A prospective randomised trial comparing sequential Ganciclo- vir-high dose Acyclovir to high dose Acyclovir for preven- tion of Cytomegalovirus disease in adult liver transplant re- cipients. Transplantation 1994; 58: 779-785.
19. Meyers JD, Ljungman P, Fisher LD. Cytomegalovirus excre- tion as a predictor of Cytomegalovirus disease after marrow transplantation: importance of Cytomegalovirus viraemia. J Infect Dis 1990; 162: 373-80.
20. Paya CV, Smith TF, Ludwig J, Hermans PE. Rapid shell vial culture and tissue histology compared with serology for the rapid diagnosis of Cytomegalovirus infection in liver trans- plantation. Mayo Clinic Proc 1989; 64: 670-5.
21. Goodrich JM, Mori M, Gleaves CA, Du Mond C, Cays M, Ebeling DF, Buhles WC, De Armond B, Meyers JD. Early treatment with Ganciclovir to prevent Cytomegalovirus dis- ease after allogeneic bone marrow transplantation. NEJM 1991; 325: 1601-7.
22. Singh N, Yu VL, Mieles L, Wagener MM, Miner RC, Gay- owski T. High-dose Acyclovir compared with short-course pre-emptive Ganciclovir therapy to prevent Cytomegalovirus disease in liver transplant recipients. Ann Intern Med 1994; 120: 375-81.
23. Schmidt GM, Horak DA, Niland JC, Duncan SR, Forman SJ, Zaia JA. A randomised, controlled trial of prophylactic Gan- ciclovir for Cytomegalovirus pulmonary infection in recipi- ents of allogeneic bone marrow transplants. NEJM 1991; 324: 1005-11.
24. Pass RF, Griffiths PD, August AM. Antibody response to Cytomegalovirus after renal transplantation: comparison of patients with recurrent and primary infections. J Infect Dis 1983; 147: 40-6.
25. Kangro HO, Griffiths PD, Huber TJ, Heath RB. Specific IgM class antibody production following infection with Cytomeg- alovirus. J Med Virol 1982; 10: 203-12.
26. Basson J, Tardy JC, Aymard M. Pattern of anti-Cytomegalo-
virus IgM antibodies determined by immunoblotting. A study of kidney graft recipients developing a primary or re- current CMV infection. Arch Virol 1989; 108: 259-70.
27. Chou S, Kim DY, Scott KM, Sewell DL. Immunoglobulin M to Cytomegalovirus in primary and reactivation infections in renal transplant recipients. J Clin Microbial 1987; 25: 52-5.
28. Rasmussen L, Kelsall D, Nelson R, Camey W, Hirsch M, Winston D, Preiksaitis J, Merigan TC. Virus-specific IgG and IgM antibodies in normal and immunocompromised subjects infected with Cytomegalovirus. J Infect Dis 1982; 145: 191-9.
29. Schmidt CA, Oettle H, Peng R, Neuhaus P, Blumhardt G, Lohmarm R, Wilbom F, Osthoff K, Oertel J, Timm H, Sieg- ert W. Comparison of polymerase chain reaction from plasma and buffy coat with antigen detection and occurrence of immunoglobulin M for the detection of Cytomegalovirus infection after liver transplantation. Transplantation 1995; 59: 1133-8.
30. Revello MG, Percivalle E, Zavattoni M, Parea M, Grossi P, Gema G. Detection of human Cytomegalovirus immediate early antigen in leukocytes as a marker of viraemia in immu- nocompromised patients. J Med Virol 1989; 29: 88-93.
3 1. van der Bij W, Torensma R, van Son WJ, Anema J, Schirm J, Tegzess AM, The TH. Rapid immunodiagnosis of active Cy- tomegalovirus infection by monoclonal antibody staining of blood leucocytes. J Med Virol 1988; 25: 179-88.
32. van den Berg AP, Tegzess AM, Scholten-Sampson A, Schirm J, van der Giessen M, The TH, van Son WJ. Monitor- ing antigenaemia is useful in guiding treatment of severe Cy- tomegalovirus disease after organ transplantation. Transplant Int 1992; 5: 101-7.
33. Bein G, Bitsch A, Hoyer J, Steinhoff J, Fricke L, Machnik H, Dennin R, Kirchner H. A longitudinal prospective study of Cytomegalovirus pp65 antigenaemia in renal transplant re- cipients. Transplant Int 1993; 6: 185-90.
34. van den Berg AP, Klompmaker IJ, Haagsma EB, Scholten- Sampson A, Bijleveld CMA, Schirm J, van der Giessen M, Sloof MJH, The TH. Antigenaemia in the diagnosis and monitoring of active Cytomegalovirus infection after liver transplantation. J Infect Dis 1991; 164: 265-70.
35. Boland GJ, Ververs C, Hene RJ, Jambroes G, Donckerwol- eke RAMG, de Gast GC. Early detection of primary Cy- tomegalovirus infection after heart and kidney transplanta- tion and the influence of hyperimmune prophylaxis. Trans- plant Int 1993; 6: 34-8.
36. van den Berg AP, van der Bij W, van Son WJ, Anema J, van der Giessen M, Schirm J, Tegzess AM, The TH. Cytomega- lovirus antigenaemia as a useful marker of symptomatic Cy- tomegalovirus infection after renal transplantation: a report of 130 consecutive patients. Transplantation 1989; 48: 991- 995.
37. Bevan IS, Daw RA, Day PJR, Ala FA, Walker MR. Polymer- ase chain reaction for detection of human Cytomegalovirus infection in a blood donor population. Br J Haematol 1991; 78: 4-9.
38. Smith KL, Kulski JK, Cobain T, Dunstan RA. Detection of Cytomegalovirus in blood donors by the polymerase chain reaction. Transfusion 1993; 33: 497-503.
39. Schmidt CA, Oettle H, Neuhaus P, Wiens M, Timm H, Wilbom F, Siegert W. Demonstration of Cytomegalovirus by polymerase chain reaction after liver transplantation. Trans- plantation 1993; 56: 8724.
267
D. Mutimer
40. Delgado R, Lumbreras C, Alba C, Pedraza MA, Otero JR, Gomez R, Moreno E, Noriega AR, Paya CV. Low predictive value of polymerase chain reaction for diagnosis of Cytome- galovirus disease in liver transplant recipients. J Clin Micro- biol 1992; 30: 1876-8.
41. Kidd IM, Fox JC, Pillay D, Charman H, Griffiths PD, Emery VC. Provision of prognostic information in immunocompro- mised patients by routine application of the polymerase chain reaction for Cytomegalovirus. Transplantation 1993; 56: 867-71.
42. Nyberg G, Bergstrom T, Blohme I, Norden G, Olofsson S, Ricksten A. Clinical evaluation in organ transplant patients of a polymerase chain reaction test for CMV DNA applied on white cells and serum. Transplant Int 1994; 7: 428-33.
43. Prosch S, Kimel V, Dawydowa I, Kruger DH. Monitoring of patients for Cytomegalovirus after organ transplantation by centrifugation culture and PCR. J Med Virol1992; 38: 246-5 1.
44. Pate1 R, Smith TF, Espy M, Portela D, Wiesner RH, Krom RAF, Paya CV. A prospective comparison of molecular diag- nostic techniques for the early detection of Cytomegalovirus in liver transplant recipients. J Infect Dis 1995; 171: 1010-4.
45. Gerdes JC, Spees EK, Fitting K, Hi&i J, Sheehan M, Duda D, Jarvi T, Roehl C, Robertson AD. Prospective study utilis- ing a quantitative polymerase chain reaction for detection of Cytomegalovirus DNA in the blood of renal transplant recip- ients.Transplant Proc 1993; 25: 1411-13.
46. Schafer P, Braun RW, Mohring K, Hence K, Kang J, Wend- land T, Kuhn JE. Quantitative determination of human Cy- tomegalovirus target sequences in peripheral blood leuko- cytes by nested polymerase chain reaction and temperature gradient gel electrophoresis. J Gen Virol 1993; 74: 2699- 707.
47. Fox JC, Griffiths PD, Emery VC. Quantification of human Cytomegalovirus DNA using the polymerase chain reaction. J Gen Virol 1992; 73: 2405-8.
48. Mutimer DJ, Matyi-Toth A, Elias E, Shaw J, O’Donnell K, Kilgariff H, Neuberger J, Gunson B, McMaster P, Stalhand- ske P. Quantitation of Cytomegalovirus in the blood of liver transplant recipients. Liver Transplant Surg 1995; 1: 395-
400. 49. Bell R, Sheil AGR, McDonald JA, McCaughan GW. The
role of CMV immune prophylaxis in patients at risk of pri- mary CMV infection following orthotopic liver transplanta- tion. Transplant Proc 1989; 21: 3781-2.
50. Saliba F, Arulnaden JL, Gugenheim J, Serves C, Samuel D, Bismuth A, Mathieu D, Bismuth H. CMV hyperimmune globulin prophylaxis after liver transplantation: a prospective randomised controlled study. Transplant Proc 1989; 21: 2260-2.
51. Stratta RJ, Shaefer MS, Cushing KA, Markin RS, Wood RP, Langnas AN, Reed EC, Woods GL, Donovan JP, Pillen TJ, Li S, Duckworth RM, Shaw Jr BW. Successful prophylaxis of Cytomegalovirus disease after primary CMV exposure in liver transplant recipients. Transplantation 1991; 5 1: 90-7.
52. Stratta RJ, Shaefer MS, Cushing KA, Markin RS, Reed EC, Langnas AN, Pillen TJ, Shaw Jr BW. A randomised prospec- tive trial of Acyclovir and immune globulin prophylaxis in liver transplant recipients receiving 0KT3 therapy. Arch Surg 1992; 127: 55-64.
53. Glowacki LS, Smaill FM. Use of immune globulin to pre- vent symptomatic Cytomegalovirus disease in transplant re- cipients - a meta-analysis. Clin Transplant 1994; 8: 10-18.
54. Mor E, Meyers BR, Yagmur 0, Kishikawa K, Sheiner PA, Emre S, Schwartz ME, Miller CM. High-dose Acyclovir and intravenous immune globulin reduce the incidence of CMV disease after liver transplantation. Transplant Int 1995; 8: 152-6.
55. Mollison LC, Richards MJ, Johnson PDR, Hayes K, Munck- hof WJ, Jones RM, Dabkowski PD, Angus PW. High-dose Acyclovir reduces the incidence of Cytomegalovirus infec- tion in liver transplant recipients. J Infect Dis 1993; 168: 721-4.
56. Nakazato PZ, Bums W, Moore P, Garcia-Kennedy R, Cox K, Esquivel C. Viral prophylaxis in hepatic transplantation: pre- liminary report of a randomised trial of Acyclovir and Ganci- clovir. Transplant Proc 1993; 25: 1935-7.
57. Dunn DL, Gillingham KJ, Kramer MA, Schmidt WJ, Erice A, Balfour Jr HH, Gores PF, Gruessner RWG, Matas AJ, Payne WD, Sutherland DER, Najarian JS. A prospective ran- domised study of Acyclovir versus Ganciclovir plus human immune globulin prophylaxis of Cytomegalovirus infection after solid organ transplantation. Transplantation 1994; 57: 876-884.
58. Balfour HH, Chace BA, Stapleton JT, Simmons RL, Fryd DS. A randomised, placebo-controlled trial of oral acyclovir for the prevention of Cytomegalovirus disease in recipients of renal allografts. NEJM 1989; 320: 1381-7.
59. Winston DJ, Wirin D, Shaked A, Bus&l RW. Randomised comparison of Ganciclovir and high-dose Acyclovir for long-term Cytomegalovirus prophylaxis in liver transplant recipients. Lancet 1995; 346: 69-74.
60. Freise CE, Pons V, Lake J, Burke E, Ascher NL, Roberts JP Comparison of 3 regimens for Cytomegalovirus prophylaxis in 147 liver transplant recipients. Transplant Proc 1991; 23: 1498-50.
61. Cohen AT, O’Grady JG, Sutherland S, Sallie R, Tan K-C, Williams R. Controlled trial of prophylactic versus therapeu- tic use of Ganciclovir after liver transplantation in adults. J Med Virol 1993; 40: 5-9.
62. Chatterjee SN, Fiala M, Weiner J, Stewart JA, Stacey B, Warner N. Primary Cytomegalovirus and opportunistic in- fections. Incidence in renal transplant patients. JAMA 1978; 240: 2446-9.
63. Rand KH, Pollard RB, Merigan TC. Increased pulmonary su- perinfections in cardiac transplant patients undergoing pri- mary Cytomegalovirus infections. NEJM 1978; 298: 951-3.
64. Smyth RL, Scott JP, Borysiewicz LK, Sharples LD, Stewart S, Wreghitt TG, Gray JJ, Higenbottam TW, Wallwork J. Cy- tomegalovirus infection in heart-lung transplant recipients: risk factors, clinical associations, and response to treatment. J Infect Dis 1991; 164: 1045-50.
65. Bronsther 0, Makowka L, Jaffe R, Demetris AJ, Breinig MK, Ho M, Esquivel CO, Gordon RD, Iwatsuki S, Tzakis A, Marsh Jr JW, Mazzaferro V, Van Thiel D, Starzl TE. Occur- rence of Cytomegalovirus hepatitis in liver transplant pa- tients. J Med Virol 1988; 24: 423-34.
66. George MJ, Snydman DR, Werner BG, Dougherty NN, Grif- fith J, Rohrer RH, Freeman R, Jenkins R, Lewis WD. Use of Ganciclovir plus Cytomegalovirus immune globulin to treat CMV pneumonia in orthotopic liver transplant recipients. Transplant Proc 1993; 25: 22-4.
67. Stratta RJ, Shaefer MS, Markin RS, Cushing KA, Donovan JP, Wood RP, Langnas AN, Reed EC, Woods GL, Zetterman RK, Sorrel1 MF, Pillen TJ, Shaw BW Jr. Ganciclovir therapy
268
CMV infection of transplant recipients
for viral disease in liver transplant recipients. Clin Transplant 1991; 5: 287-93.
68. Harbison MA, De Girolami PC, Jenkins RL, Hammer SM. Ganciclovir therapy of severe Cytomegalovirus infections in solid-organ transplant recipients. Transplantation 1988; 46: 82-8.
69. Bitsch A, Kirchner H, Dennin R, Hoyer J, Fricke L, Stein- hoff J, Sack K, Bein G. The long persistence of CMV DNA in the blood of renal transplant patients after recovery from CMV infection. Transplantation 1993; 56: 108-13.
70. Fietze E, Prosch S, Reinke P, Stein J, Docke W-D, Staffa G, Loning S, Devaux S, Emmrich F, von Baehr R, Kruger DH, Volk HD. Cytomegalovirus infection in transplant recipients. Transplantation 1994; 58: 675-80.
71. Tilg H, Vogel W, Aulitzky WE, Herold M, Konigsrainer A, Margreiter R, Huber C. Evaluation of cytokines and cy- tokine-induced secondary messages in sera of patients after liver transplantation. Transplantation 1990; 49: 1074-80.
72. Stein J, Volk HD, Liebenthal C, Kruger DH, Prosch S. Tu- mour necrosis factor alpha stimulates the activity of the hu- man Cytomegalovirus major immediate early enhancer/pro- moter in immature monocytic cells. J Gen Virol 1993; 74: 2333-8.
73. Sheron N, Goka J, Wendon J, Keays R, Keane H, Alexander
G, Williams R. Highly elevated plasma cytokines in fuhni- nant hepatic failure: correlations with multiorgan failure and death. Hepatology 1990; 12: 939.
74. Manez R, White LT, Linden P, Kusne S, Martin M, Kramer D, Demetris AJ, Van Thiel DH, Starzl TE, Duquesnoy RJ. The influence of HLA matching on Cytomegalovirus hepati- tis and chronic rejection after liver transplantation. Trans- plantation 1993; 55: 1067-71.
75. O’Grady JG, Alexander GJM, Sutherland S, Donaldson PT, Harvey F, Portmann B, Calne RY, Williams R. Cytome- galovirus infection and donor/recipient HLA antigens: in- terdependent co-factors in pathogenesis of vanishing bile- duct syndrome after liver transplantation. Lancet 1988; ii: 302-5.
76. Candinas D, Gunson BK, Nightingale P, Hubscher S, Mc- Master P, Neuberger JM. Sex mismatch as a risk factor for chronic rejection of liver allografts. Lancet 1995; 346: 1117- 21.
77. Paya CV, Wiesner RH, Hermans PE, Larson-Keller JJ, Il- strup DM, Krom RAF, Moore SB, Ludwig J, Smith TF. Lack of association between Cytomegalovirus infection, HLA matching and the vanishing bile duct syndrome after liver transplantation. Hepatology 1992; 16: 66-70.
269