cme asthma
55
G IN A lobal itiative for sthma
-
Upload
samah-sahak -
Category
Documents
-
view
137 -
download
6
Transcript of cme asthma

G INA
G INA
lobal
itiative for
sthma
lobal
itiative for
sthma

GINA Program Objectives
GINA Program Objectives
Increase appreciation of asthma as a global public health problem
Present key recommendations for diagnosis and management of asthma
Provide strategies to adapt recommendations to varying health needs, services, and resources
Identify areas for future investigation of particular significance to the global community
Increase appreciation of asthma as a global public health problem
Present key recommendations for diagnosis and management of asthma
Provide strategies to adapt recommendations to varying health needs, services, and resources
Identify areas for future investigation of particular significance to the global community

Global Strategy for Asthma Management and Prevention Global Strategy for Asthma Management and Prevention
Definition and Overview Diagnosis and
Classification Asthma Medications Asthma Management and
Prevention Program
Definition and Overview Diagnosis and
Classification Asthma Medications Asthma Management and
Prevention Program
Updated 2007Updated 2007

Apa itu Asthma ?
Adalah penyakit paru paru melibatkan radangan ( inflamasi) yang kronik pada saluran.
Apa yang berlaku pada saluran tersebut
• Radang pada saluran pernafasan
• Saluran pernafasan terlalu sensitif
• Penyempitan saluran pernafasan (Bronchoconstriction)

Source: Peter J. Barnes, MDSource: Peter J. Barnes, MD
Asthma Inflammation: Cells and Mediators

PERUBAHAN PERUBAHAN YANG BERLAKU PADA SALURAN
PERNAFASAN
RADANG SALURAN
Penyempitan saluran
pernafasan
Faktor Sekitaran dan Biologi ( Penyebab )
Tanda / gejalaFaktor pencetus serangan
Saluran pernafasan terlalu sensitif

hidungtekak
farink
Trakea
bronkiol
Bronkus
alveolus
diafragm

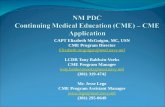
The picture below shows what your lungs look like when everything is working normally. The muscles that are wrapped around the airways are very thin and loose, and the airway is wide open. This makes it easy to move air in and out of the air sacs.
During an asthma attack, the muscles around the airways tighten, or "spasm" (like when you make a fist) and the lining inside the airways swell or thicken, and get clogged with lots of thick mucous. This makes the airways much skinnier than usual so it is harder to move air in and out of the air sacs. This makes it hard to breathe! The picture below shows what
your lungs would look like during an asthma attack.
SALURAN PERNAFASAN
NORMAL
SALURAN PERNAFASAN
ASTHMA
OTOT
KERATAN RENTAS
KERATAN RENTAS
SEMPIT SEMPIT & BENGKAK
SEMPIT,BENGKAK & LENDIR

This animation shows normal breathing. As you breathe in, red air that contains lots of oxygen is pulled into the lungs. The oxygen slowly moves out of the lungs and into the blood, and then blue air that contains carbon dioxide is pushed out of the lungs. When
things are working normally, the amount of air we breathe in is about the same as the amount of air we breathe out.

This animation shows breathing during an asthma attack. Notice that the airways are narrowed so less air can move in and out of the lungs. When things are working normally, the amount of air we breathe in is about the same as the amount of air we breathe out however during an asthma attack air gets trapped inside
the lungs making it harder and harder to breathe.
During an asthma attack, it is actually harder to breathe out than it is to breathe in. This means that during an asthma attack, it takes much longer to breathe out (expire) than it does to breathe in (inspire

Burden of Asthma
Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals
Prevalence increasing in many countries, especially in children
A major cause of school/work absence
Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals
Prevalence increasing in many countries, especially in children
A major cause of school/work absence

Risk Factors for Asthma
Host factors: predispose individuals to, or protect them from, developing asthma
Environmental factors: influence susceptibility to development of asthma in predisposed individuals, precipitate asthma exacerbations, and/or cause symptoms to persist
Host factors: predispose individuals to, or protect them from, developing asthma
Environmental factors: influence susceptibility to development of asthma in predisposed individuals, precipitate asthma exacerbations, and/or cause symptoms to persist

Factors that Exacerbate AsthmaFactors that Exacerbate Asthma
Allergens Respiratory infections Exercise and hyperventilation Weather changes Sulfur dioxide Food, additives, drugs

Factors that Influence Asthma Development and Expression
Host Factors Genetic - Atopy - Airway
hyperresponsiveness Gender Obesity
Host Factors Genetic - Atopy - Airway
hyperresponsiveness Gender Obesity
Environmental Factors Indoor allergens Outdoor allergens Occupational sensitizers Tobacco smoke Air Pollution Respiratory Infections Diet
Environmental Factors Indoor allergens Outdoor allergens Occupational sensitizers Tobacco smoke Air Pollution Respiratory Infections Diet

Is it Asthma?Is it Asthma?
Recurrent episodes of wheezing Troublesome cough at night Cough or wheeze after exercise Cough, wheeze or chest tightness after
exposure to airborne allergens or pollutants
Colds “go to the chest” or take more than 10 days to clear

Asthma Diagnosis
History and patterns of symptoms
Measurements of lung function
- Spirometry - Peak expiratory flow
Measurement of airway responsiveness
Measurements of allergic status to identify risk factors
Extra measures may be required to diagnose asthma in children 5 years and younger and the elderly
History and patterns of symptoms
Measurements of lung function
- Spirometry - Peak expiratory flow
Measurement of airway responsiveness
Measurements of allergic status to identify risk factors
Extra measures may be required to diagnose asthma in children 5 years and younger and the elderly

Clinical Control of Asthma
No (or minimal)* daytime symptoms
No limitations of activity
No nocturnal symptoms
No (or minimal) need for rescue medication
Normal lung function
No exacerbations_________* Minimal = twice or less per week

Levels of Asthma Control
CharacteristicControlled
(All of the following)Partly controlled
(Any present in any week)Uncontrolled
Daytime symptomsNone (2 or less / week)
More than twice / week
3 or more features of partly controlled asthma present in any week
Limitations of activities
None Any
Nocturnal symptoms / awakening
None Any
Need for rescue / “reliever” treatment
None (2 or less / week)
More than twice / week
Lung function (PEF or FEV1)
Normal< 80% predicted or
personal best (if known) on any day
Exacerbation None One or more / year 1 in any week

1. Develop Patient/Doctor Partnership
2. Identify and Reduce Exposure to Risk Factors
3. Assess, Treat and Monitor Asthma
4. Manage Asthma Exacerbations
5. Special Considerations
1. Develop Patient/Doctor Partnership
2. Identify and Reduce Exposure to Risk Factors
3. Assess, Treat and Monitor Asthma
4. Manage Asthma Exacerbations
5. Special Considerations
Asthma Management and PreventionProgram: Five ComponentsAsthma Management and PreventionProgram: Five Components
Revised 2006

Asthma Management and Prevention Program: Five Interrelated Components
1. Develop Patient/Doctor Partnership
2. Identify and Reduce Exposure to Risk Factors
3. Assess, Treat and Monitor Asthma
4. Manage Asthma Exacerbations
5. Special Considerations
1. Develop Patient/Doctor Partnership
2. Identify and Reduce Exposure to Risk Factors
3. Assess, Treat and Monitor Asthma
4. Manage Asthma Exacerbations
5. Special Considerations

Asthma Management and Prevention Program
Goals of Long-term Management
Achieve and maintain control of symptoms
Maintain normal activity levels, including exercise
Maintain pulmonary function as close to normal levels as possible
Prevent asthma exacerbations Avoid adverse effects from asthma
medications Prevent asthma mortality
Achieve and maintain control of symptoms
Maintain normal activity levels, including exercise
Maintain pulmonary function as close to normal levels as possible
Prevent asthma exacerbations Avoid adverse effects from asthma
medications Prevent asthma mortality

Asthma Management and Prevention Program
Asthma can be effectively controlled in most patients by intervening to suppress and reverse inflammation as well as treating bronchoconstriction and related symptoms
Early intervention to stop exposure to the risk factors that sensitized the airway may help improve the control of asthma and reduce medication needs.
Asthma can be effectively controlled in most patients by intervening to suppress and reverse inflammation as well as treating bronchoconstriction and related symptoms
Early intervention to stop exposure to the risk factors that sensitized the airway may help improve the control of asthma and reduce medication needs.
.

Asthma Management and Prevention Program
Although there is no cure for asthma, appropriate management that includes a partnership between the physician and the patient/family most often results in the achievement of control

Example Of Contents Of An Action Plan To Maintain Asthma Control
Your Regular Treatment: 1. Each day take ___________________________ 2. Before exercise, take _____________________
WHEN TO INCREASE TREATMENTAssess your level of Asthma ControlIn the past week have you had: Daytime asthma symptoms more than 2 times ? No Yes Activity or exercise limited by asthma? No Yes Waking at night because of asthma? No Yes The need to use your [rescue medication] more than 2 times? No Yes If you are monitoring peak flow, peak flow less than________? No YesIf you answered YES to three or more of these questions, your asthma is uncontrolled and you may need to step up your treatment.
HOW TO INCREASE TREATMENTSTEP-UP your treatment as follows and assess improvement every day:____________________________________________ [Write in next treatment step here] Maintain this treatment for _____________ days [specify number]
WHEN TO CALL THE DOCTOR/CLINIC.Call your doctor/clinic: _______________ [provide phone numbers]If you don’t respond in _________ days [specify number]______________________________ [optional lines for additional instruction]
EMERGENCY/SEVERE LOSS OF CONTROLIf you have severe shortness of breath, and can only speak in short sentences,If you are having a severe attack of asthma and are frightened,If you need your reliever medication more than every 4 hours and are not improving.1. Take 2 to 4 puffs ___________ [reliever medication] 2. Take ____mg of ____________ [oral glucocorticosteroid]3. Seek medical help: Go to _____________________; Address___________________ Phone: _______________________4. Continue to use your _________[reliever medication] until you are able to get medical help.

Asthma Management and Prevention Program
Factors Involved in Non-AdherenceAsthma Management and Prevention Program
Factors Involved in Non-Adherence
Medication Usage Difficulties associated
with inhalers
Complicated regimens
Fears about, or actual side effects
Medication Usage Difficulties associated
with inhalers
Complicated regimens
Fears about, or actual side effects
Non-Medication Factors
Misunderstanding/lack of information
Fears about side-effects
Inappropriate expectations
Underestimation of severity
Attitudes toward ill health
Cultural factors
Poor communication
Non-Medication Factors
Misunderstanding/lack of information
Fears about side-effects
Inappropriate expectations
Underestimation of severity
Attitudes toward ill health
Cultural factors
Poor communication

Asthma Management and Prevention Program
Component 2: Identify and Reduce Exposure to Risk Factors
Asthma Management and Prevention Program
Component 2: Identify and Reduce Exposure to Risk Factors
Measures to prevent the development of asthma, and asthma exacerbations by avoiding or reducing exposure to risk factors should be implemented wherever possible.
Asthma exacerbations may be caused by a variety of risk factors – allergens, viral infections, pollutants and drugs.
Reducing exposure to some categories of risk factors improves the control of asthma and reduces medications needs.

Reduce exposure to indoor allergens Avoid tobacco smoke Avoid vehicle emission Identify irritants in the workplace Explore role of infections on asthma
development, especially in children and young infants
Asthma Management and Prevention Program
Component 2: Identify and Reduce Exposure to Risk Factors
Asthma Management and Prevention Program
Component 2: Identify and Reduce Exposure to Risk Factors

Asthma Management and Prevention Program
Component 3: Assess, Treat and Monitor Asthma
Asthma Management and Prevention Program
Component 3: Assess, Treat and Monitor Asthma
The goal of asthma treatment, to achieve and maintain clinical control, can be achieved in a majority of patients with a pharmacologic intervention strategy developed in partnership between the patient/family and the health care professional
The goal of asthma treatment, to achieve and maintain clinical control, can be achieved in a majority of patients with a pharmacologic intervention strategy developed in partnership between the patient/family and the health care professional

Asthma Management and Prevention Program
Component 3: Assess, Treat and Monitor Asthma
Asthma Management and Prevention Program
Component 3: Assess, Treat and Monitor Asthma
Depending on level of asthma control, the patient is assigned to one of five treatment steps
Treatment is adjusted in a continuous cycle driven by changes in asthma control status. The cycle involves:
- Assessing Asthma Control
- Treating to Achieve Control
- Monitoring to Maintain Control

Levels of Asthma Control
Characteristic Controlled Partly controlled(Any present in any week)
Uncontrolled
Daytime symptomsNone (2 or less / week)
More than twice / week
3 or more features of partly controlled asthma present in any week
Limitations of activities
None Any
Nocturnal symptoms / awakening
None Any
Need for rescue / “reliever” treatment
None (2 or less / week)
More than twice / week
Lung function (PEF or FEV1)
Normal< 80% predicted or
personal best (if known) on any day
Exacerbation None One or more / year 1 in any week

Component 4: Asthma Management and Prevention Program
Controller MedicationsComponent 4: Asthma Management and Prevention Program
Controller Medications
Inhaled glucocorticosteroids Leukotriene modifiers Long-acting inhaled β2-agonists Systemic glucocorticosteroids Theophylline Long-acting oral β2-agonists Anti-IgE Systemic glucocorticosteroids
Inhaled glucocorticosteroids Leukotriene modifiers Long-acting inhaled β2-agonists Systemic glucocorticosteroids Theophylline Long-acting oral β2-agonists Anti-IgE Systemic glucocorticosteroids

Estimate Comparative Daily Dosages for Inhaled Glucocorticosteroids by AgeEstimate Comparative Daily Dosages for Inhaled Glucocorticosteroids by Age
Drug Low Daily Dose (g) Medium Daily Dose (g) High Daily Dose (g)
> 5 y Age < 5 y > 5 y Age < 5 y > 5 y Age < 5 y
Drug Low Daily Dose (g) Medium Daily Dose (g) High Daily Dose (g)
> 5 y Age < 5 y > 5 y Age < 5 y > 5 y Age < 5 y
Beclomethasone 200-500 100-200 >500-1000 >200-400 >1000 >400
Budesonide 200-600 100-200
600-1000 >200-400 >1000 >400
Budesonide-Neb Inhalation Suspension
250-500
>500-1000
>1000
Ciclesonide 80 – 160 80-160 >160-320 >160-320 >320-1280 >320
Flunisolide 500-1000 500-750
>1000-2000 >750-1250 >2000 >1250
Fluticasone 100-250 100-200
>250-500 >200-500 >500 >500
Mometasone furoate 200-400 100-200
> 400-800 >200-400 >800-1200 >400
Triamcinolone acetonide 400-1000 400-800
>1000-2000 >800-1200 >2000 >1200

Component 4: Asthma Management and Prevention Program
Reliever MedicationsComponent 4: Asthma Management and Prevention Program
Reliever Medications
Rapid-acting inhaled β2-agonists
Systemic glucocorticosteroids
Anticholinergics
Theophylline
Short-acting oral β2-agonists
Rapid-acting inhaled β2-agonists
Systemic glucocorticosteroids
Anticholinergics
Theophylline
Short-acting oral β2-agonists

controlled
partly controlled
uncontrolled
exacerbation
LEVEL OF CONTROLLEVEL OF CONTROL
maintain and find lowest controlling step
consider stepping up to gain control
step up until controlled
treat as exacerbation
TREATMENT OF ACTIONTREATMENT OF ACTION
TREATMENT STEPSREDUCE INCREASE
STEP
1STEP
2STEP
3STEP
4STEP
5
RE
DU
CE
INC
RE
AS
E







Treating to Maintain Asthma Control
When control as been achieved, ongoing monitoring is essential to:
- maintain control
- establish lowest step/dose treatment
Asthma control should be monitored by the health care professional and by the patient

Treating to Maintain Asthma Control
Stepping down treatment when asthma is controlled
When controlled on medium- to high-dose inhaled glucocorticosteroids: 50% dose reduction at 3 month intervals (Evidence B)
When controlled on low-dose inhaled glucocorticosteroids: switch to once-daily dosing (Evidence A)

Exacerbations of asthma are episodes of progressive increase in shortness of breath, cough, wheezing, or chest tightness
Exacerbations are characterized by decreases in expiratory airflow that can be quantified and monitored by measurement of lung function (FEV1 or PEF)
Severe exacerbations are potentially life-threatening and treatment requires close supervision
Exacerbations of asthma are episodes of progressive increase in shortness of breath, cough, wheezing, or chest tightness
Exacerbations are characterized by decreases in expiratory airflow that can be quantified and monitored by measurement of lung function (FEV1 or PEF)
Severe exacerbations are potentially life-threatening and treatment requires close supervision
Asthma Management and Prevention Program
Component 4: Manage Asthma Exacerbations
Asthma Management and Prevention Program
Component 4: Manage Asthma Exacerbations

Primary therapies for exacerbations:
• Repetitive administration of rapid-acting inhaled β2-agonist
• Early introduction of systemic glucocorticosteroids
• Oxygen supplementation
Closely monitor response to treatment with serialmeasures of lung function
Primary therapies for exacerbations:
• Repetitive administration of rapid-acting inhaled β2-agonist
• Early introduction of systemic glucocorticosteroids
• Oxygen supplementation
Closely monitor response to treatment with serialmeasures of lung function
Asthma Management and Prevention Program
Component 4: Manage Asthma Exacerbations
Asthma Management and Prevention Program
Component 4: Manage Asthma Exacerbations

Asthma can be effectively controlled in most patients by intervening to suppress and reverse inflammation as well as treating bronchoconstriction and related symptoms
Although there is no cure for asthma, appropriate management that includes a partnership between the physician and the patient/family most often results in the achievement of control
Asthma can be effectively controlled in most patients by intervening to suppress and reverse inflammation as well as treating bronchoconstriction and related symptoms
Although there is no cure for asthma, appropriate management that includes a partnership between the physician and the patient/family most often results in the achievement of control
Asthma Management and Prevention Program: SummaryAsthma Management and Prevention Program: Summary

A stepwise approach to pharmacologic therapy is recommended. The aim is to accomplish the goals of therapy with the least possible medication
The availability of varying forms of treatment, cultural preferences, and differing health care systems need to be considered
A stepwise approach to pharmacologic therapy is recommended. The aim is to accomplish the goals of therapy with the least possible medication
The availability of varying forms of treatment, cultural preferences, and differing health care systems need to be considered
Asthma Management and Prevention Program: SummaryAsthma Management and Prevention Program: Summary

A. PERSEDIAAN PERALATAN• Kad pesakit asthma• Buku pendaftaran pesakit luar• Peralatan ukur timbang/ tinggi• Blood Pressure set• Peak flow meter (adult/ paediatric)• Pulse oxymeter• Nebuliser and face mask• Inhaler placebo - ( untuk tujuan pendidikan kesihatan)• Ubatan reliever- Salbutamol MDI/ Bricanyl MDI • Ubatan controller – Budesonide/ Beclomethasone MDI, Budesonide Turbohaler• Ubatan bronchodilator – untuk acute case ( Salbutamol, Bricanyl, Combivent, Atrovent)• Oxygen supply• Oral steroids prednisolone, Intravenous Steroids ( hydrocortisone)• Flow chart untuk management of acute asthma• Flow chart untuk asthma assessment• Carta pengkelasan asthma control• Bahan pendidikan kesihatan asthma• Written asthma plan•

Alternate Slides for Alternate Slides for Asthma TreatmentAsthma Treatment

Characteristic Controlled(All of the following)
Partly Controlled(Any measure present in any week)
Uncontrolled
Daytime symptoms None (twice or less/week)
More than twice/week
Three or more features of partly controlled asthma present in any week
Limitations of activities
None Any
Nocturnal symptoms/awakening
None Any
Need for reliever/ rescue treatment
None (twice or less/week)
More than twice/week
Lung function (PEF or FEV1)
Normal < 80% predicted or personal best (if known)
Exacerbations None One or more/year* One in any week†
Levels of Asthma Control
* Any exacerbation should prompt review of maintenance treatment to ensure that it is adequate.† By definition, an exacerbation in any week makes that an uncontrolled asthma week.





Asthma Control: Treatment StepsChildren Older than Five Years, Adolescents, Adults

Example Of Contents Of An Action Plan To Maintain Asthma Control
Your Regular Treatment: 1. Each day take ___________________________ 2. Before exercise, take _____________________
WHEN TO INCREASE TREATMENTAssess your level of Asthma ControlIn the past week have you had: Daytime asthma symptoms more than 2 times ? No Yes Activity or exercise limited by asthma? No Yes Waking at night because of asthma? No Yes The need to use your [rescue medication] more than 2 times? No Yes If you are monitoring peak flow, peak flow less than________? No YesIf you answered YES to three or more of these questions, your asthma is uncontrolled and you may need to step up your treatment.
HOW TO INCREASE TREATMENTSTEP-UP your treatment as follows and assess improvement every day:____________________________________________ [Write in next treatment step here] Maintain this treatment for _____________ days [specify number]
WHEN TO CALL THE DOCTOR/CLINIC.Call your doctor/clinic: _______________ [provide phone numbers]If you don’t respond in _________ days [specify number]______________________________ [optional lines for additional instruction]
EMERGENCY/SEVERE LOSS OF CONTROLIf you have severe shortness of breath, and can only speak in short sentences,If you are having a severe attack of asthma and are frightened,If you need your reliever medication more than every 4 hours and are not improving.1. Take 2 to 4 puffs ___________ [reliever medication] 2. Take ____mg of ____________ [oral glucocorticosteroid]3. Seek medical help: Go to _____________________; Address___________________ Phone: _______________________4. Continue to use your _________[reliever medication] until you are able to get medical help.