Clostridium sordellii as a cause of constrictive pericarditis with pyopericardium and tamponade
10
1 Clostridium sordellii as a cause of constrictive pericarditis with 1 pyopericardium and tamponade 2 Rama Chaudhry, 1 * Nishant Verma, 1 Tej Bahadur, 1 Parul Chaudhary, 1 Pallavi Sharma, 1 and 3 Nidhi Sharma 1 4 All India Institute of Medical Sciences, New Delhi, India 1 5 *Corresponding author. Mailing address. Department of Microbiology, All India Institute 6 of Medical Sciences, New Delhi 110029, India. Phone: 91-11-2659 4795. Fax: 91-11-2658 7 8641. Email id: [email protected] . 8 Abstract 9 Systemic infections caused by Clostridium sordellii is a rare entity. They are usually 10 reported in skin, soft tissue infections and sometimes toxic shock syndrome involving 11 exotoxins. We report here, the first case of Clostridium sordellii infection associated with 12 acute constrictive pericarditis with pyopericardium and tamponade. 13 Case Report 14 The patient, an eight months old infant, was admitted in a local hospital with history of fever 15 of about 2 months and an abscess in right thigh which had developed following hepatitis-B 16 vaccination. The abscess was drained and the pus culture revealed Staphylococcus aureus for 17 which the patient was given vancomycin intravenously as per the antimicrobial susceptibility 18 report. The abscess subsequently healed, however, the patient continued to remain sick with 19 development of dry cough and swelling of legs. Echocardiography and chest x-ray showed 20 pericardial effusion with increased cardio-thoracic ratio and the patient was referred to our 21 institute. On admission, the patient was afebrile with mild pedal edema, tender hepatomegaly, 22 and liver palpable till 4 cm below costal margin. Routine investigations showed 23 Copyright © 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved. J. Clin. Microbiol. doi:10.1128/JCM.00933-11 JCM Accepts, published online ahead of print on 3 August 2011 on April 3, 2019 by guest http://jcm.asm.org/ Downloaded from
Transcript of Clostridium sordellii as a cause of constrictive pericarditis with pyopericardium and tamponade

1
Clostridium sordellii as a cause of constrictive pericarditis with 1
pyopericardium and tamponade 2
Rama Chaudhry,1* Nishant Verma,
1 Tej Bahadur,
1 Parul Chaudhary,
1 Pallavi Sharma,
1 and 3
Nidhi Sharma1 4
All India Institute of Medical Sciences, New Delhi, India1
5
*Corresponding author. Mailing address. Department of Microbiology, All India Institute 6
of Medical Sciences, New Delhi 110029, India. Phone: 91-11-2659 4795. Fax: 91-11-2658 7
8641. Email id: [email protected]. 8
Abstract 9
Systemic infections caused by Clostridium sordellii is a rare entity. They are usually 10
reported in skin, soft tissue infections and sometimes toxic shock syndrome involving 11
exotoxins. We report here, the first case of Clostridium sordellii infection associated with 12
acute constrictive pericarditis with pyopericardium and tamponade. 13
Case Report 14
The patient, an eight months old infant, was admitted in a local hospital with history of fever 15
of about 2 months and an abscess in right thigh which had developed following hepatitis-B 16
vaccination. The abscess was drained and the pus culture revealed Staphylococcus aureus for 17
which the patient was given vancomycin intravenously as per the antimicrobial susceptibility 18
report. The abscess subsequently healed, however, the patient continued to remain sick with 19
development of dry cough and swelling of legs. Echocardiography and chest x-ray showed 20
pericardial effusion with increased cardio-thoracic ratio and the patient was referred to our 21
institute. On admission, the patient was afebrile with mild pedal edema, tender hepatomegaly, 22
and liver palpable till 4 cm below costal margin. Routine investigations showed 23
Copyright © 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.J. Clin. Microbiol. doi:10.1128/JCM.00933-11 JCM Accepts, published online ahead of print on 3 August 2011
on April 3, 2019 by guest
http://jcm.asm
.org/D
ownloaded from

2
haemoglobin-12.8 g/dL; total leukocyte count-14,100/µL; differential leukocyte count of 24
Neutrophils 50 , Lymphocytes 46, Eosinophils 3, Monocytes 1; erythrocyte sedimentation 25
rate-5 mm in first hour; blood urea-35 mg/dL; serum creatinine-0.4 mg/dL; serum sodium- 26
128 mEq/L; serum potassium-4.3 mEq/L; SGOT-115 U/L; SGPT-235 U/L; total bilirubin-1.8 27
mg/dL; total protein-5.1 g/dL; serum albumin-2.8 g/dL. The urine output was within normal 28
limits. Central nervous system and respiratory system examination showed no abnormalities. 29
Heart rate was 128 beats per minute. Electrocardiogram showed low voltage complexes and 30
echocardiography revealed organized pericardial effusion with features of tamponade. The x-31
ray of chest showed a cardio-thoracic ratio of 0.65. Computerized tomography (CT) scan of 32
chest showed features suggestive of effusive constrictive pericarditis and a diagnosis of 33
constrictive pericarditis with pyopericardium and tamponade was made. Pigtail drainage of 34
pericardial pus was performed and patient was administered empirically with intravenous 35
piperacillin-tazobactam and linezolid. On examination, pericardial fluid was turbid with 36
protein-40 mg/dL; sugar-45 mg/dL; total leukocyte count of 2600/µL; differential leukocyte 37
count of Neutrophils 90 and Lymphocytes 10. Gram staining on direct smear showed no 38
organisms and Ziehl-Neelsen staining showed no acid fast bacilli. Aerobic cultures of 39
pericardial fluid and blood were sterile, however, pericardial fluid was not sent for anaerobic 40
culture. Meanwhile the patient had stabilized. Follow-up Computerized tomography-41
angiogram showed a localized constriction at atrio-ventricular groove and pericardiectomy 42
was performed. Post-operative period was uneventful and the patient was discharged with 43
oral amoxycillin-clavulanic acid. 44
The excised pericardial tissue was sent for both aerobic and anaerobic culture. Aerobic 45
culture showed no growth. On anaerobic culture, odourless, flat, greyish, non-hemolytic 46
colonies were seen with irregular margin. They were metronidazole sensitive. Gram staining 47
on April 3, 2019 by guest
http://jcm.asm
.org/D
ownloaded from

3
showed gram-positive bacilli with sub terminal non-bulging spores. The isolate was further 48
identified biochemically, and tested positive for lecithinase, urease, gelatin liquefaction, 49
indole production, glucose fermentation, and esculin hydrolysis. The isolate was identified as 50
C. sordellii. The isolate was also tested using API 20A (Biomeurix, France) and was 51
identified as C. sordellii. 52
A polymerase chain reaction (PCR) using published primers for 16S ribosomal RNA was 53
also done. Briefly, DNA was extracted from the culture by QIAmp kit (QIAGEN, Germany) 54
and was amplified using broad range PCR primers i.e., forward primer (F8) 5’-55
AGTTTGATCCTGGCTCAG-3’ and reverse primer (357R) 5’-CTGCTGCCTCCCGTA-3’ 56
(6, 14) and C. sordellii specific forward primer (C1SOR-F) 5’-TCGAGCGACCTTCGG-3’ 57
and reverse primer (C1SOR-R) 5’-CACCACCTGTCACCAT-3’ respectively, targeting the 58
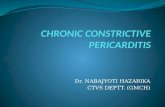
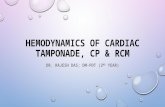
16S ribosomal RNA (rRNA) gene (10). Amplified products i.e., 330 bp (Fig. 1) for broad 59
range and 944 bp (Fig. 2) for Clostridium sordellii specific PCR, were purified by using 60
QIAGEN Gel extraction kit. The purified products were commercially sequenced and 61
compared with sequences available in the Gene Bank database by Basic Local Alignment 62
Search Tool (BLAST). The 16S rRNA gene sequences amplified from isolate showed 99% 63
identity with C. sordellii (Accession no. dbj|AB448946.1|) sequence available in the 64
database. Thus, C. sordellii was identified as the cause of constrictive pericarditis with 65
pyopericardium and tamponade. Patient responded favourably to the therapy. 66
______________________________________________________ 67
Anaerobes are now being recognized as etiological agents for infections of almost any body 68
site including pericardium (4). Pericarditis refers to inflammation of the pericardium and the 69
proximal part of great blood vessels. It may either be asymptomatic or may present as a 70
fulminating, life threatening condition. Brahan et al (3), Francois et al (8), and Pigrau et al 71
on April 3, 2019 by guest
http://jcm.asm
.org/D
ownloaded from

4
(12) have reported the association of C. septicum infection with pericarditis in patients with 72
underlying carcinoma. Skiest et al (13) have given a brief review of anaerobic pericarditis 73
occurring in children in which Bacteroides species was highlighted as the predominant cause. 74
Pericarditis was also associated with C. perfringens (9). C. difficile pericarditis complicating 75
pseudomembranous colitis in patient hospitalized after multiple trauma was first reported by 76
Koehler et al (11). It is to be noted that C. difficile resembles C. sordellii phenotypically and 77
since more virulent strains of C. difficile such as NAP1 are being reported worldwide, there is 78
a need to carefully differentiate between them genotypically (7). Although few other cases of 79
pericarditis caused by genus clostridia have been reported, to our knowledge, this is the first 80
case where Clostridium sordellii infection is associated with pericarditis. C. sordellii is a 81
gram-positive anaerobe; an infrequent human pathogen associated with skin and soft tissue 82
infections. The exotoxins produced by the bacteria are associated with toxic shock syndrome 83
with high mortality rate following childbirth, medically induced abortion, and routine 84
gynaecological procedures (1, 2). Recently, C. sordellii has been reported as a cause of brain 85
abscess (15). 86
In the case reported here, there was no clinical suspicion of anaerobic infection initially. 87
Since all other reasons were ruled out systematically the clinicians finally decided to send the 88
excised pericardial tissue for anaerobic culture. The sample was transported in anaerobic 89
transport medium with sterile precautions. A pure culture of C.sordellii was confirmed 90
phenotypically and genotypically. 91
Prevailing local conditions, host factors, and rapid administration of appropriate antimicrobial 92
treatment could have decreased the clinical severity of the infection which led to good 93
prognosis in the case reported here. The possibility of low virulence of the pathogen could 94
not be ruled out (5). 95
on April 3, 2019 by guest
http://jcm.asm
.org/D
ownloaded from

5
Present case demonstrates that C.sordellii can cause acute constrictive pericarditis. Moreover, 96
expanding clinical spectrum of C. sordellii necessitates application of rapid identification 97
methods such as PCR and gene sequencing and increased clinical awareness of this 98
unrecognized human pathogen. 99
References 100
1. Aldape, M. J., A. E. Bryant, and D. L. Stevens. 2006. Clostridium 101
sordellii infections: epidemiology, clinical findings, and current perspectives on 102
diagnosis and treatment. Clin. Infect. Dis. 43:1436-1446. 103
2. Aronoff, D. M., and J. D. Ballard. 2009. Clostridium sordellii toxic shock 104
syndrome. Lancet Infect. Dis. 9:725-726. 105
3. Brahan, R. B., and R. C. Kahler. 1990. Clostridium septicum as a cause of 106
pericarditis and mycotic aneurysm. J. Clin. Microbiol. 28:2377-2378. 107
4. Brook, I., 2009. Pericarditis caused by anaerobic bacteria. Int. J. Antimicrob. 108
Agents. 33:297-300. 109
5. Brüggemann, H., 2005. Genomics of clostridial pathogens: implication of 110
extrachromosomal elements in pathogenicity. Curr. Opin. Microbiol. 8:601-605. 111
6. Daly, J. S., M. G. Worthington, D. J. Brenner, C. W. Moss, D. G. Hollis, R. S. 112
Weyant, A.G. Steierwalt, R. E. Weaver, M. I. Daneshvar, and S. P. O’Connor. 113
1993. Rochalimaea elizabethae sp. nov. isolated from a patient with endocarditis. J. 114
Clin. Microbiol. 31:872-881. 115
7. Elsayed, S., and K. Zhang. 2006. Positive Clostridium difficile Stool Assay in a 116
Patient with Fatal C. sordellii Infection. N. Engl. J. Med. 355:1284-1285. 117
on April 3, 2019 by guest
http://jcm.asm
.org/D
ownloaded from

6
8. Francois, B. L., P. Delare, L. Vignon, Niquet R, Gobeaux F, and Gay R. 1994. 118
Gas gangrene and purulent pericarditis during Clostridium septicemia revealing a 119
cecal carcinoma. Intensive Care Med. 20:309. 120
9. Ivey, M. J., and B. H. Gross. 1993. Back pain and fever in an elderly patient. Chest. 121
103:1851-1853. 122
10. Kikuchi, E., Y. Miyamoto, S. Narushima, and K. Itoh. 2002. Design of species-123
specific primers to identify 13 species of Clostridium harboured in human intestinal 124
tracts. Microbiol. Immunol. 46:353-358. 125
11. Koehler, R., M. Mone, E. Kimball , D. Vargo, N. Leonardo , and R. Barton. 126
2003. Clostridium difficle pericarditis complicating pseudomembranous colitis in a 127
trauma patient. J. Trauma. 55:771-773. 128
12. Pigrau, C. M., P. Ruiz, and J. Sagrista. 1995. Purulent pericarditis due to 129
Clostridium septicum associated with carcinoma of the colon. Clin. Infect. Dis. 130
20:202-203. 131
13. Skiest, D. J., D. Steiner, M. Werner, and J. G. Garner. 1994. Anaerobic 132
pericarditis: case report and review. Clin. Infect. Dis. 19:435-440. 133
14. Stackebrandt, E., and O. Charfreitag. 1990. Partial 16S rRNA primary structure of 134
five Actinomyces species: phylogenetic implications and development of an 135
Actinomyces israelii-specific oligonucleotide probe. J. Gen. Microbiol. 136:37-43. 136
15. Valour, F. S., Boisset, S. Lebras, B. Martha, A. Boibieux, T. Perpoint, C. 137
Chidiac, T. Ferry, and D. Peyramond. 2010. Clostridium sordellii Brain Abscess 138
diagnosed by 16S rRNA Gene Sequencing. J. Clin. Microbiol. 48:3443-344. 139
on April 3, 2019 by guest
http://jcm.asm
.org/D
ownloaded from

Figure 1:
Broad range PCR assay showing 330 bp sequence of 16S rRNA gene of genus clostridia.
Lane 1: 100 bp ladder
Lane 2: Pericardial isolate
Lane 3: C. sordellii lab isolate
Lane 4: C. difficile ATCC 9689
Lane 5: C. perfringens lab solate
Lane 6: Negative control
on April 3, 2019 by guest
http://jcm.asm
.org/D
ownloaded from

FIGURE 2:
Clostridium sordellii specific PCR showing 944 bp sequence of 16S rRNA gene.
Lane 1: 100 bp ladder
Lane 2: Negative control
Lane 3: C.sordellii pericardial isolate
Lane 4 and 5: C.sordellii lab isolate
Lane 6: 100 bp ladder
on April 3, 2019 by guest
http://jcm.asm
.org/D
ownloaded from