Describe relationship between neuromodulation, rehabilitation…

Closed-Loop Neuromodulation in Physiologicaland Translational Research
Stavros Zanos
Translational Neurophysiology Laboratory, Center for Bioelectronic Medicine, Feinstein Institute for MedicalResearch, Northwell Health, Manhasset, New York 11030
Correspondence: [email protected]
Neuromodulation, the focused delivery of energy to neural tissue to affect neural or physio-logical processes, is a commonmethod to study the physiologyof the nervous system. It is alsosuccessfully used as treatment for disorders in which the nervous system is affected or impli-cated. Typically, neurostimulation is delivered in open-loop mode (i.e., according to a pre-determined schedule and independently of the state of the organ or physiological systemwhose function is sought to be modulated). However, the physiology of the nervous systemor the modulated organ can be dynamic, and the same stimulus may have different effectsdepending on the underlying state. As a result, open-loop stimulation may fail to restore thedesired function or cause side effects. In such cases, a neuromodulation intervention may bepreferable to be administered in closed-loop mode. In a closed-loop neuromodulation (CLN)system, stimulation is delivered when certain physiological states or conditions are met(responsive neurostimulation); the stimulation parameters can also be adjusted dynamicallyto optimize the effect of stimulation in real time (adaptive neurostimulation). In this review, thereasons and the conditions for using CLN are discussed, the basic components of a CLNsystem are described, and examples of CLN systems used in physiological and translationalresearch are presented.
Typically, in a physiology experiment, the sub-ject is exposed to a set of controlled condi-
tions and interventions, while the investigatortakes functional measurements. These measure-ments are recorded during the experiment to beanalyzed at a later time, offline (Fig. 1A). How-ever, in some cases, the timing and other aspectsof the intervention need to be linked to one ormore physiological events and physiological pa-rameters and tightly controlled, especially whenthose parameters change rapidly. In such cases,the intervention is delivered on the occurrenceof certain physiological states, defined a priori
by the investigator and inferred by an automatedsystem that analyzes measurements taken si-multaneously, in real time (Fig. 1B). This exper-imental model can be useful in the study of thenervous system owing to the inherently dynamicnature of neural activity because the same stim-ulus delivered against a different physiologicalstate may have completely different physiologi-cal effects. It can also be used as a method forcontrolling dynamic neural processes, as wellas other physiological functions that are them-selves modulated by the nervous system, in aresponsive and adaptivemanner. In recent years,
Editors: Valentin A. Pavlov and Kevin J. TraceyAdditional Perspectives on Bioelectronic Medicine available at www.perspectivesinmedicine.org
Copyright © 2018 Cold Spring Harbor Laboratory Press; all rights reservedAdvanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314
1
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

the term neuromodulation has been adapted torefer to these neural control systems, although inthe more traditional usage, neuromodulation isthe physiological process by which a neuron useschemicals to regulate the activity of large, oftendistant, populations of neurons.
Here we will discuss the most common rea-sons for using a closed-loop neuromodulation(CLN) approach and describe the basic compo-nents of closed-loop systems. Examples of CLNsystems in the context of basic and translationalphysiological research will be presented. Finally,future directions of this line of research will bediscussed.
REASONS AND CONDITIONS FOR THE USEOF CLOSED-LOOP NEUROMODULATION
There are two main reasons why one wouldwant to use a closed-loop approach in a neuro-modulation setting.
Need for Responsive Neuromodulation
The requirement for responsive interaction withthe nervous system arises when neural processesthat depend on precise timing between a phys-iological event or state and an intervention are
studied, or when an intervention needs to hap-pen during a certain physiological state for it tobe successful.
In principle, the state dependency of the ef-fects of neurostimulation on a dynamic neural orphysiological process could be studied in eitherof twoways in a given experiment: (1) open-loopdelivery of stimuli across different physiologicalstates and registration of physiological effectsseparately for each state, and (2) closed-loop de-liveryof stimuli in response to a specific state andregistration of the effects for that state only. Incases when the effects of neurostimulation arenonstationary and, more importantly, whenthey are affected by the history of neurostimula-tion itself, a closed-loop approach will more ac-curately address state-dependent effects.
One successful use of responsive CLN sys-tems in physiological research has been in invivo studies of synaptic plasticity. For spiketiming-dependent synaptic potentiation to beinduced, the detection of a spontaneous presyn-aptic action potential needs to be followed byelectrical or sensory stimulation that elicits post-synaptic depolarization within a short windowof time, typically, <50 msec (Dan and Poo 2004;Jackson et al. 2006a; Nishimura et al. 2013a).There are several examples of CLN systems
CPU
A B
Figure 1. Principles of open-loop and closed-loop experiments or interventions. (A) In an open-loop context, apredetermined intervention is applied to an animal according to a hypothesis, a set of measurements are taken tocharacterize the response of the animal to that intervention, and those measurements are analyzed at a later timeby the investigator. (B) In a closed-loop context, the investigator starts by defining a set of rules that will determinethe conditions at which an intervention will be applied to the animal. An automated system (CPU) observes a setofmeasurements taken from the animal at regular intervals and delivers the intervention according to the definedrules, in real time.
S. Zanos
2 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

that, in real time, monitor neural or physiolog-ical activity, detect relevant signal signatures in it(e.g., spikes, field potentials or muscle activity),and deliver neurostimulation to successfully in-duce neural plasticity (Rebesco et al. 2010; Gug-genmos et al. 2013; Ethier et al. 2015; Fetz 2015;Oweiss and Badreldin 2015). Such systems havebeen used to investigate plasticity mechanismsin vivo (e.g., Jackson et al. 2006a; Carrillo-Reidet al. 2016), as well as to facilitate adaptive plas-ticity after neural injury (Edwardson et al. 2013;Nudo 2014; McPherson et al. 2015). ResponsiveCLN systems have also been used in experimen-tal efforts to restore disrupted communicationbetween brain regions in the context of a cogni-tive prosthesis (e.g., Deadwyler et al. 2017), be-tween the brain and the spinal cord (Nishimuraet al. 2013b; Zimmermann and Jackson 2014;Capogrosso et al. 2016) or the peripheral ner-vous system (Moritz et al. 2008; Bouton et al.2016) in the context of restoration of motormovement is patients with paraplegia or quad-riplegia.
On amore translational front, “on-demand”delivery of a neurostimulation-based therapyduring certain physiological states, inferred byphysiological and other biomarkers, has twomain advantages over open-loop delivery: (1)higher probability of attaining desirable, state-specific effects, while minimizing the chance ofundesirable side effects, and (2) more efficientoperation of the stimulus generator becausestimulation happens only when it is needed. Forexample, brain stimulation delivered throughsubdural electrodes in response to detection ofabnormal brain activity can suppress the onset ofepileptic seizures (Ramgopal et al. 2014; Gelleret al. 2017). Closed-loop left cervical vagus nervestimulation (VNS) triggered from seizure-relat-ed increases in heart rate (HR) reduces the fre-quency and severity of seizures more effectivelythan open-loop VNS (Fisher et al. 2016; Hamil-ton et al. 2018). Deep brain stimulation (DBS)delivered in response to pathologic brain activityor to the onset of hand tremor is at least as effec-tive as and at least as safe as open-loop DBS,while consuming less power, hence significantlyextending the battery life of the implantable gen-erator (Gilat 2018; Kuo et al. 2018). Finally, a
number of preliminary human studies suggestthat closed-loop stimulation of the auricularbranch of the vagus nerve (VN), triggeredfrom the expiratory phase of the respiratoryrhythm, which is known to strongly modulatevagal tone, can effectively induce analgesia inindividuals with pelvic pain and reduce bloodpressure (BP) in hypertensive patients (Na-padow et al. 2012; Sclocco et al. 2017).
Need for Adaptive Neuromodulation
The requirement for adaptive neuromodula-tion arises when a neuromodulation interven-tion leads to physiological or clinical effects thatare not entirely predictable and that need tobe monitored for the parameters of the inter-vention to be optimized with regard to thoseeffects.
In physiological research, an important ap-plication of CLN systems is determining stimu-lus-response characteristics of a sensory neuralcircuit by the iso-responsemethod (Gollisch andHerz 2012). Iso-response curves are trajectoriesin the stimulus parameter space that elicit simi-lar neural responses. To explore the parameterspace while no significant changes in the neuralresponse occur, aCLN system records and quan-tifies neural activity in real time, then selects thenext stimuli so that the neural response remainson the iso-response curve. This adaptive selec-tion of iso-response stimuli can significantly re-duce experiment time (Benda et al. 2007) andreveal nonlinearities in the stimulus–responsefunction, would be missed had the experimentbeen performed in an open-loop manner (Gol-lisch andHerz 2012). A proof-of-concept designof an adaptive CLN system has recently beenexplored in the context of VNS for HR control;in this system, VNS parameters are adjusted in away that minimizes the difference between anobserved physiological variable (i.e., HR) and adesired target value of that variable (Romero-Ugalde et al. 2017).
A more translational example of an adaptiveCLN system is closed-loop spinal stimulationthat aims to restore locomotion in paralyzed an-imals by activating sensory and motor spinalcircuits; this system is dynamically adapted to
Closed-Loop Neuromodulation
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314 3
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

maximize the precision or fluidity of the result-ing motor movement by monitoring and ana-lyzing the resulting movements themselves, inreal time (Wenger et al. 2014). Closed-loop spi-nal stimulation is also used to relieve pain andassociated symptoms in patients with back orleg pain; in this case, the recruitment of fibersin the dorsal columnviamonitoring of stimulus-evoked compound actional potentials is used toadjust stimulation parameters and maintainstimulationwithin an individualized therapeuticrange (Russo et al. 2018).
In translational closed-loop applications,the choice of biomarkers used in the adaptationprocess warrants special consideration. Whenthe entire range of physiological, desirable,and undesirable effects is well characterized, thenthe choice of biomarkers that “reward” and “pe-nalize” a given set of stimulation parametersduring the adaptation process is straightfor-ward. However, this is not always the case, asthe nonobvious effects of most neuromodula-tion therapies are incompletely understood, es-pecially because they involve multiple organsystems and at different timescales. This situa-tion is not unlike the unpredictable effects ofdrug therapies, often recognized years after thetherapies are introduced clinically. More com-prehensive characterization of the varied effectsof neuromodulation therapies in relevant ani-mal models and data collection from as manysensors and clinical and laboratory tests as it isfeasible during their clinical application are thebest ways to build more confidence in the selec-tion of biomarkers for therapy optimization.Moreover, in clinical applications, the processof adaptation itself ought to be more conserva-tive, because of the potential for undesirable,even catastrophic, events (e.g., Ali et al. 2004).A blind trial-and-error strategy to discover thedirections in parameter space that minimize thediscrepancy between current and desirable ef-fects may not be ideal in terms of safety; how-ever, it is one of the few options when no robustmodels relating stimulation parameters andphysiological effects exist. In such cases, evensmall increases in the magnitude of unwantedeffects in response to a new set of stimulationparameters could be heavily penalized and the
change in stimulation parameters reversed im-mediately.
The potential clinical application of suchadaptive approaches is significant, as it allowssubject- and state-specific therapy to be “pre-scribed” without a priori knowledge of the var-iable, complex, and inherently dynamic effects,both desired and undesired, of neurostimulationon the target organs.
Conditions for the Use of a CLN System
Three conditions need to be met for a closed-loop approach to be meaningful and successful,at least in principle.
First, the physiology of the target organ andthe mechanism of action of the interventionneed to be relatively fast. A targeted physiolog-ical process that is inherently slow (e.g., the ap-plication of electrical fields for accelerating bonefracture or wound healing) is unlikely to benefitfrom a closed-loop approach that emphasizesrapid action and feedback, unless that is an in-herently slow process that relies on fast physiol-ogy (e.g., fast synaptic plasticity that underlieslearning). For that reason, physiological pro-cesses that benefit from CLN interventionsinclude those that are under the modulatorycontrol of the central or peripheral nervous sys-tem, such as restoration of motor movement inparalysis (Nishimura et al. 2013b; Wenger et al.2014; Alam et al. 2016; Ganzer et al. 2018), al-leviation of chronic pain (Russo et al. 2018),suppression of epileptic seizures (Ramgopal etal. 2014; Parastarfeizabadi and Kouzani 2017;Thomas and Jobst 2018), augmentation of brainplasticity after neural injury (Hays et al. 2013;Pruitt et al. 2016), improvement of movementdeficits in Parkinson’s disease ([PD]; Hebb et al.2014; Meidahl et al. 2017; Parastarfeizabadi andKouzani 2017), and even psychiatric disease (Loand Widge 2017).
Second, the feedback signals that inform theCLN system of the relevant aspects of the dy-namic state of the target organ need to be rep-resentative of that state. For example, althougharm accelerometry may be an excellent feedbacksignal for the detection of the onset or the mon-itoring of an ongoing epileptic seizure, it may
S. Zanos
4 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

not be as useful for the prediction of an upcom-ing seizure with the intent of suppressing itbefore it becomes clinically evident (Ramgopalet al. 2014). In that regard, it is important todefine appropriate signals as biomarkers thatare reliably quantifiable, track the targeted phys-iological process in a timescale congruent withits dynamics, and correlate well with the clinicalmanifestations and the treatment results (Hebbet al. 2014; Thomas and Jobst 2018).
Finally, from a translational perspective, aCLN system ought to be used instead of anopen-loop system only when the latter, becauseof its nonresponsive nature, cannot attain thedesired effect or causes unwanted effects thatclosed-loop stimulation would minimize. Phar-macotherapy of human diseases is a good illus-tration of this dichotomy. For many diseases, wehave a working model of the pathophysiologyand its dependency on physiological state; wealso have a good understanding of the timecourse and magnitude of the drug’s physiologi-cal effects. Consequently, we can come upwith astandardized, open-loop, daily delivery schedulethat works well when it is adhered to, as is thecase with antibiotics in infectious diseases.However, there are numerous diseases in whichan intervention is successful only when it is de-livered under the right circumstances and po-tentially deleterious when delivered outside ofthem: glycemic control in diabetes, heartrhythm control in arrhythmias, control of vas-cular resistance in hypertension, control of air-way resistance in asthma, etc. Given that all theseare examples of diseases in which pathogenesisinvolves the nervous system, closed-loop pe-ripheral neuromodulation would be a meaning-ful therapeutic approach (Sharma and Weber2018).
BASIC COMPONENTS OF A CLOSED-LOOPNEUROMODULATION SYSTEM
A CLN system comprises a few basic compo-nents: sensors, acquisition system, processingunit, and output device. When the system ischronically implanted, it also includes a case, apower source, and, in some cases, wireless trans-mission.
Sensors
The set of sensors are needed to obtain physio-logical measurements from the nervous systemor other organ systems. These sensors need tohave a relatively fast response time and be able totake repeated measurements, to provide an ad-equate representation of the dynamic biologicalsystem that is being monitored. The outputs ofthese sensors comprise the physiological signalsthat the closed-loop system uses to infer the sta-tus of the organ or the organism. Many of thesesensors are invasive, meaning they require a sur-gical procedure to be implanted. Typically, thesesensors need to be implanted chronically, andthey need to be appropriately interfaced withthe acquisition system and the rest of theclosed-loop system. The surgical techniquesand challenges, as well as the special engineeringdemands associated with chronic, invasive sen-sors, depend on the type and the anatomicallocation of the sensor and the connected deviceand are outside the scope of this work (Arle2011). Sensors that measure electrical activityof neurons and other excitable cells are inexpen-sive, readily available, and they can be interfacedwith a variety of amplification and acquisitionsystems. For all those reasons, they represent thefirst choice for sensing in CLN systems.
Sensors used in neuromodulation systemsinclude:
• Sensors for electrical neural activity. These aretypically conductive elements (microelec-trodes, microwires, pads, etc.) placed nearthe source of activity. Noninvasive sensorsare those that are placed on the skin or onthe scalp surface (Lopez-Gordo et al. 2014).However, most sensors are invasive as they areimplanted subdermally (Young et al. 2006),subdurally (Schalk and Leuthardt 2011), in-tracortically (Gunasekera et al. 2015), in deepbrain structures (Lewis et al. 2016), on thesurface of the spine or intraspinally (Tatoret al. 2012), or on peripheral nerves (Fammet al. 2013; Rijnbeek et al. 2018). Measuringelectrical brain activity has the overall advan-tage of high temporal resolution (down toa submillisecond scale, if needed); spatialresolution can also be high, albeit only with
Closed-Loop Neuromodulation
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314 5
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

invasive, high-channel count implants com-prising microscale sensors. Invasive sensorsgenerally give rise to better signal-to-noise ra-tio signals, as they typically lie closer to thesource of the electrical signals and tend to pickup less ambient noise (Fig. 2).
• Sensors for electrical activity of nonneuronalexcitable cells. These include sensors for elec-trocardiography (ECG), electromyography(EMG), electrooculography (EOG), and dif-ferent forms of electrodermal activity, includ-ing the galvanic skin response. These sensorscan be noninvasive, typically placed on the
skin surface in predetermined locations, orinvasive (e.g., subcutaneous or epicardialECG, intramuscular EMG).
• Invasive sensors for other physiological mea-surements. These include pressure sensorsplaced in vessels or body cavities (e.g., ventri-cles of the brain), blood flow sensors, temper-ature sensors, biochemical sensors measuringblood glucose, pH, blood CO2, etc. Althoughthe physical process involved in such mea-surements is different for different sensors,the output of these sensors is generally anelectrical potential that can be registered in
0.2 msec
Window 2
Window 1
Threshold
50 msec
50 msec
25 msec
Rawsignal
LFP
50 μ
V
50 μ
V
A B
250
μV
30 μ
V
Figure 2.Digital signal processing (DSP) and event detection examples in a closed-loop neuromodulation (CLN)system. (A) In the top panel, a short snippet of neuronal activity is shown, acquired from an intracorticalmicroelectrode, after high-pass filtering of the raw electrical signal to isolate fast spiking activity. Red arrowsdenote spiking events detected by a double time-window discriminatorDSP chain operating on the filtered signalin real time, using the Neurochip CLN system (Jackson et al. 2006b). The graphical representation of that DSPchain is shown in the bottom panel: The filtered signal has to cross a voltage threshold, then go through both of thetwo voltage windows that are set in such a way to detect spikes with a certain waveform (black traces) and ignorethreshold crossingswith non-spikelikewaveforms (gray traces). (B) In the top panel, a snippet of electrical activityfrom another intracortical microelectrode is shown, this time with no filtering applied; slow oscillatory activity(representing the local field potential [LFP]), as well as fast spiking events riding on top of it are shown. Arrowsdenote spiking events, just like in panel A; red arrows denote spiking events that occurred during a depolarizing(negative) phase of the oscillatory field potential, and black arrows denote the remaining spiking events. (Middlepanel) The discrimination between the two populations of spikes happened through implementation of a secondDSP chain, in addition to the spike detection, that gates the acceptance of spikes on negative values of the low-frequency band-filtered field potential (shown in the red trace). (Bottom panel) Average raw signal during theoperation of the CLN system, in which single-pulse electrical stimuli were triggered from the accepted (red)spiking events. The triggered stimulus artifact is blanked by the gray vertical line. The average spikewaveform thatlead to triggering of neurostimulation events is shown just before the artifact (open arrow); that spike is riding onthe trough of a slow, oscillatory field potential (filled arrow). This detection system was implemented on theNeurochip-2 CLN system (Zanos et al. 2011).
S. Zanos
6 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

real time by a standard acquisition system, justlike with neural signals. For that reason, theseare also excellent sensors for CLN systems.
• Noninvasive, wearable, and ambient sensors.This heterogeneous group of sensors includeswearable systems that capture acceleration ofthe torso, head or limbs, respiration, temper-ature, oxygen saturation, etc. (Patel et al.2012). There are also ambient sensor systemsthat use light sensing, motion sensing, andvideo to monitor a space in which a patientoperates daily. Signals from these sensors re-quire special digital acquisition systems and,therefore, individualized CLN system design.
Acquisition System
The acquisition system amplifies, if needed, anddigitizes the output of the sensors, and makesthe digitized signals available to the processingunit. In some cases, the acquisition system isembedded in the sensors (active sensors) (Ra-ducanu et al. 2017). The acquisition systemmayinclude wireless transmission if the processingunit is physically separated from the acquisitionsystem (Won et al. 2018).
The acquisition system may include analogcomponents (bioamplifiers), when electricalphysiological activity that needs to be amplifiedis monitored (all neural signals, ECG, EMG,etc.). A detailed discussion of the properties ofbioamplifiers and how those relate to the differ-ent sensor/signal/implant scenarios is beyondthe scope of this review (Holleman 2016). Ana-log circuits for signal preconditioning are some-times deployed (e.g., ac coupling, notch filteringof 60 Hz noise, low-pass or high-pass filtering,etc.) to ensure signals are within the require-ments for digitization.
The analog-to-digital converter (ADC) op-erates on the analog signals (amplified or not)and converts them to digital signals of appropri-ate sampling rate, accuracy, and bitrate resolu-tion. Different input signals have different ADCrequirements. For example, neuronal spiking ac-tivity (Fig. 2) requires a much higher samplingrate than ECG and that, in turn, requires a high-er sampling rate than BP signals.
Finally, the acquisition system may be usedto suppress stimulation artifacts in neural orphysiological recordings, arising from the oper-ation of the stimulation device. Artifacts areorders of magnitude larger than physiologicalsignals and introduce epochs during which nomeaningful data can be recorded. Various ana-log- and digital-based methods have been devel-oped for artifact suppression; however, this issuehas not been fully resolved (Erez et al. 2010).
Processing Unit
The digitized signals are streamed, in individualsamples or in a packet of more than one sample,to the processing unit, which is essentially acomputer. The computer performs, in realtime, several functions.
Function 1
It implements digital signal processing (DSP)functions (blue box labeled “A,” Fig. 3). Inmany cases, the digitized signals need to be fur-ther processed for relevant features to be extract-ed. For example, a voltage threshold crossingfollowed by a comparison with two consecutivevoltage windows is a typical DSP chain that isused to detect neuronal spike waveforms in asignal from a single intracortical microelectrode(Fig. 2A). When the signal meets all these con-ditions, a spike is detected; the time stamps ofoccurrence of individual spikes, or the frequencyof spiking are common features used in closed-loop systems (Franke et al. 2010). Similar DSPchains can be applied to ECG to extract normalor abnormal QRS complexes (Maheshwari et al.2013) to arterial BP signals to measure systolicpressure, etc.
Function 2
The computer combines different features fromone or more input signals, estimates the physi-ological state of the system, and compares thatstate with a number of preprogramed physiolog-ical conditions, which should generate a certainoutput (the so-called “intervention rules” in thered box labeled “B,” Fig. 3). For example, in
Closed-Loop Neuromodulation
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314 7
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from
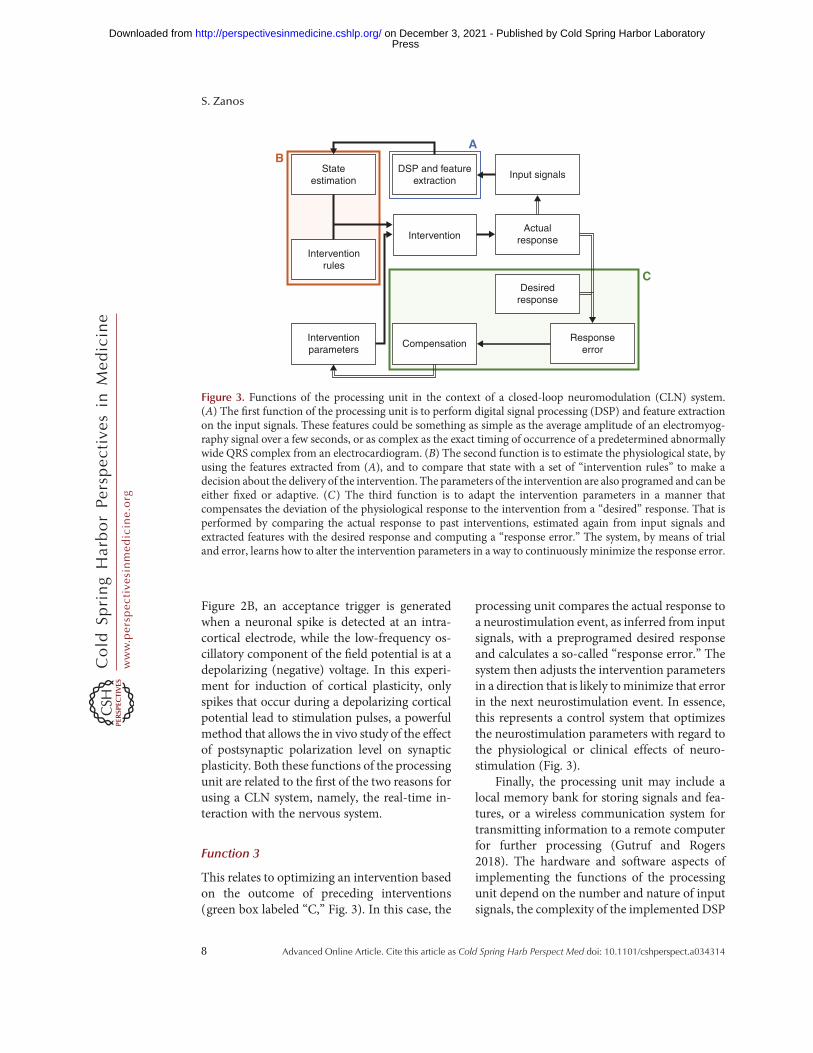
Figure 2B, an acceptance trigger is generatedwhen a neuronal spike is detected at an intra-cortical electrode, while the low-frequency os-cillatory component of the field potential is at adepolarizing (negative) voltage. In this experi-ment for induction of cortical plasticity, onlyspikes that occur during a depolarizing corticalpotential lead to stimulation pulses, a powerfulmethod that allows the in vivo study of the effectof postsynaptic polarization level on synapticplasticity. Both these functions of the processingunit are related to the first of the two reasons forusing a CLN system, namely, the real-time in-teraction with the nervous system.
Function 3
This relates to optimizing an intervention basedon the outcome of preceding interventions(green box labeled “C,” Fig. 3). In this case, the
processing unit compares the actual response toa neurostimulation event, as inferred from inputsignals, with a preprogramed desired responseand calculates a so-called “response error.” Thesystem then adjusts the intervention parametersin a direction that is likely tominimize that errorin the next neurostimulation event. In essence,this represents a control system that optimizesthe neurostimulation parameters with regard tothe physiological or clinical effects of neuro-stimulation (Fig. 3).
Finally, the processing unit may include alocal memory bank for storing signals and fea-tures, or a wireless communication system fortransmitting information to a remote computerfor further processing (Gutruf and Rogers2018). The hardware and software aspects ofimplementing the functions of the processingunit depend on the number and nature of inputsignals, the complexity of the implemented DSP
Stateestimation
BA
C
DSP and featureextraction
Input signals
Actualresponse
Desiredresponse
Responseerror
CompensationInterventionparameters
Interventionrules
Intervention
Figure 3. Functions of the processing unit in the context of a closed-loop neuromodulation (CLN) system.(A) The first function of the processing unit is to perform digital signal processing (DSP) and feature extractionon the input signals. These features could be something as simple as the average amplitude of an electromyog-raphy signal over a few seconds, or as complex as the exact timing of occurrence of a predetermined abnormallywide QRS complex from an electrocardiogram. (B) The second function is to estimate the physiological state, byusing the features extracted from (A), and to compare that state with a set of “intervention rules” to make adecision about the delivery of the intervention. The parameters of the intervention are also programed and can beeither fixed or adaptive. (C) The third function is to adapt the intervention parameters in a manner thatcompensates the deviation of the physiological response to the intervention from a “desired” response. That isperformed by comparing the actual response to past interventions, estimated again from input signals andextracted features with the desired response and computing a “response error.” The system, by means of trialand error, learns how to alter the intervention parameters in a way to continuously minimize the response error.
S. Zanos
8 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

chain, whether the state estimation process andintervention rules are fixed or adaptive, the re-quired frequency of computing the response er-ror, the algorithm for minimizing the responseerror, and the complexity of the interventionparameter space (Denison and Litt 2014).
Output Device
The output device in a CLN system delivers theintervention and it is typically a programmableand triggerable neurostimulator or drug deliverysystem.
Neurostimulators are devices that delivertargeted energy to neural tissue by means ofelectrical current (van Dongen and Serdijn2016), magnetic fields (Malmivuo and Plonsey1995), ultrasound waves (Bystritsky et al. 2011),or light (Bolus et al. 2018). That energy caneither excite or suppress activity of neural tis-sue, with concomitant effects on physiology.Neural tissues that are typically the target ofneurostimulation include the cerebral cortex,deep brain regions, the spinal cord, and periph-eral nerves. The energy is delivered throughappropriate stimulation probes, placed in theproximity of the neural tissue of interest eitherinvasive or noninvasively. Similar anatomicaland surgical principles apply to stimulationprobes as with signal sensors and, in fact,many of the sensors discussed above also serveas stimulation probes (Cogan 2008). The closerto neural tissue a probe lies, the smaller theenergy required to excite (or inhibit) the tissue;also, the smaller the contact area between theprobe and the tissue is, the more focused and,therefore, the more physiologically specific themodulation effect is (McCreery et al. 1986).Two additional considerations for invasiveneurostimulation probes are the thermal andelectrochemical effects of stimulation, whichneed to observe strict safety requirements(Merrill et al. 2005). Electromechanical micro-infusion pumps and microfluidic probes arechemical delivery systems that can be electrical-ly or remotely triggered or programmed andcan locally administer neuroactive agents toneural tissue via an implantable channel (Simet al. 2017).
EXAMPLES OF CLOSED-LOOPNEUROMODULATION SYSTEMS
In this section, we will discuss in some moredetail a few examples of currently used CLNsystems, from basic and translational physiologyto more mature clinical systems, to showcasesome practical implementations of this technol-ogy and its applications.
Induction of Neuroplasticity via Closed-LoopCortical Stimulation
One of the first bidirectional CLN systems thatallowed bidirectional interaction with the cen-tral and the peripheral nervous system was theNeurochip brain–computer interface (BCI)platform, developed by Eberhard Fetz’s groupat the University of Washington (Jackson et al.2006b; Zanos et al. 2011). It features sensing of avariety of neural and behavioral signals, custom-izable DSP and feature extraction modules,programmable logic for the delivery of neuro-stimulation, and a multichannel neurostimula-tion output. The two main applications for theNeurochip BCI are the in vivo study of activity-dependent neural plasticitymechanisms and therestoration of transmission of motor signalsacross an interrupted neural pathway (Fetz2015). Both these applications depend on real-time detection of specific signatures of neuralactivity and delivery of contingent electricalstimulation, continuously during unrestrainedbehavioral conditions, hence the need for animplantable CLN system.
The Neurochip BCI has been successfullyused to induce spike-timing-dependent plastic-ity (STDP) between motor cortical sites (Jack-son et al. 2006a) and between the motor cortexand the spinal cord (Nishimura et al. 2013a) infreely behavingmonkeys, using penetrating wireimplants, with important implications for mo-tor recovery after stroke or spinal cord injury.Because of the challenges for maintaining stablerecordings of spiking activity with penetratingwires over long periods of time, surface corticaland spinal probes have recently attracted atten-tion among basic and translational researchers(Schalk and Leuthardt 2011). In a series of stud-
Closed-Loop Neuromodulation
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314 9
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from
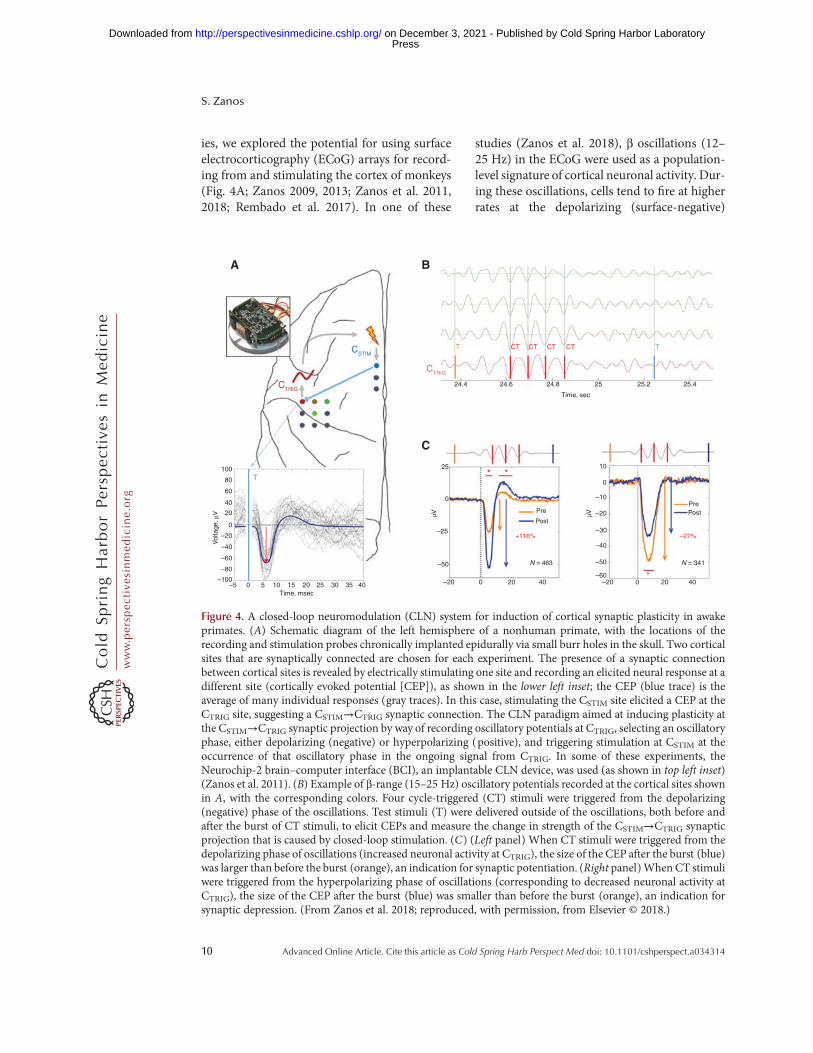
ies, we explored the potential for using surfaceelectrocorticography (ECoG) arrays for record-ing from and stimulating the cortex of monkeys(Fig. 4A; Zanos 2009, 2013; Zanos et al. 2011,2018; Rembado et al. 2017). In one of these
studies (Zanos et al. 2018), β oscillations (12–25 Hz) in the ECoG were used as a population-level signature of cortical neuronal activity. Dur-ing these oscillations, cells tend to fire at higherrates at the depolarizing (surface-negative)
–20–60
–50
–40
–30
–20
–10PrePostPre
Post
+116% –27%
0
1025100T80
60
40
20
–20
Vol
tage
, µV
–40
–60
–80
–100–5 0 5 10 15 20
Time, msec25 30 35 40
0
* *
0
–25
µV
–50
–20
25.22524.8
Time, sec
24.4
CTRIG
A B
C
CSTIM
CTRIG
T CT CT CT CT T
24.6 25.4
0 20 400 20 40
N = 341
*
N = 463
µV
Figure 4. A closed-loop neuromodulation (CLN) system for induction of cortical synaptic plasticity in awakeprimates. (A) Schematic diagram of the left hemisphere of a nonhuman primate, with the locations of therecording and stimulation probes chronically implanted epidurally via small burr holes in the skull. Two corticalsites that are synaptically connected are chosen for each experiment. The presence of a synaptic connectionbetween cortical sites is revealed by electrically stimulating one site and recording an elicited neural response at adifferent site (cortically evoked potential [CEP]), as shown in the lower left inset; the CEP (blue trace) is theaverage of many individual responses (gray traces). In this case, stimulating the CSTIM site elicited a CEP at theCTRIG site, suggesting a CSTIM→CTRIG synaptic connection. The CLN paradigm aimed at inducing plasticity atthe CSTIM→CTRIG synaptic projection by way of recording oscillatory potentials at CTRIG, selecting an oscillatoryphase, either depolarizing (negative) or hyperpolarizing (positive), and triggering stimulation at CSTIM at theoccurrence of that oscillatory phase in the ongoing signal from CTRIG. In some of these experiments, theNeurochip-2 brain–computer interface (BCI), an implantable CLN device, was used (as shown in top left inset)(Zanos et al. 2011). (B) Example of β-range (15–25 Hz) oscillatory potentials recorded at the cortical sites shownin A, with the corresponding colors. Four cycle-triggered (CT) stimuli were triggered from the depolarizing(negative) phase of the oscillations. Test stimuli (T) were delivered outside of the oscillations, both before andafter the burst of CT stimuli, to elicit CEPs and measure the change in strength of the CSTIM→CTRIG synapticprojection that is caused by closed-loop stimulation. (C) (Left panel) When CT stimuli were triggered from thedepolarizing phase of oscillations (increased neuronal activity at CTRIG), the size of the CEP after the burst (blue)was larger than before the burst (orange), an indication for synaptic potentiation. (Right panel)When CT stimuliwere triggered from the hyperpolarizing phase of oscillations (corresponding to decreased neuronal activity atCTRIG), the size of the CEP after the burst (blue) was smaller than before the burst (orange), an indication forsynaptic depression. (From Zanos et al. 2018; reproduced, with permission, from Elsevier © 2018.)
S. Zanos
10 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

oscillatory phase, and at lower rates during thehyperpolarizing (surface-positive) phase (Fig.4B). Using the Neurochip BCI, the depolarizingphase at one cortical site triggered electricalstimulation at a second site, creating the condi-tions for spike-timing-dependent synaptic po-tentiation. That led to an increase in the strengthof the synaptic projection between the two sites(Fig. 4C). In separate experiments, the hyperpo-larizing oscillatory phase of one site triggeredstimulation at a second site, and that led to adecrease in the strength of the synaptic projec-tion (Fig. 4C). These findings indicate thatinduction of bidirectional cortical synaptic plas-ticity is possible through the operation of aCLN system, using oscillatory signals recordedthrough minimally invasive neural probes. Al-though these plasticity effects last only for a fewseconds, they do represent activity-dependentsynaptic changes that may have a range of im-plications for the role of cortical oscillations inshort-term plasticity, attention and learning,and for their role in movement brain disorderslike PD (for a more detailed discussion, see Za-nos et al. 2018).
Treatment of Parkinson’s Disease via Closed-Loop Deep Brain Stimulation
PD is caused by depletion of the dopamine neu-rons in the nigrostriatal pathway, resulting indysregulation of the glutamatergic projectionfrom the striatum to the motor cortex and anabnormal level of oscillatory activity in the re-ciprocal connections between the motor cortex,the thalamus, and the striatum (Caligiore et al.2016). Patients with PD experience slowness ofmotor movement and tremor, among othersymptoms, both of which have been correlatedwith abnormal neuronal activity in those cir-cuits (Stein and Bar-Gad 2013). DBS delivershigh-frequency electrical stimulation to the sub-thalamic nucleus, believed to create a reversible,functional suppression of the circuit, therebystopping aberrant neuronal activity and allevi-ating symptoms (Little and Brown 2014; Tink-hauser et al. 2017).
DBS is delivered in an open-loop mode (i.e.,in preprogramed “on” and “off” periods), irre-
spective of the level of neural dysfunction orsymptoms. This results in neurological side ef-fects arising from disruption of neuronal com-munication between other affected circuits.Delivering DBS in closed-loop mode (or adap-tively), only when it is needed or when it ismaximally efficient, would increase the thera-peutic window and reduce the power drain onthe battery of the pulse generator (Hebb et al.2014; Meidahl et al. 2017).
Two types of biomarkers, related to the se-verity and time course of PD symptoms, can beused to optimize the timing of stimulation inadaptive DBS: brain activity and peripheralmotor signals. Brain activity related to PDsymptoms can be recorded invasively throughthe DBS electrode or ECoG electrodes implant-ed during the procedures, or noninvasivelythrough electroencephalography (EEG) elec-trodes on the scalp (Morishita and Inoue2017; Swann et al. 2018). Of these signals, in-vasively recorded local field potentials (LFPs)are the most widely used in closed-loop DBSsystems, typically focusing on the amplitudeand phase of oscillatory activity in the subtha-lamic nucleus or the motor cortex (Parastarfei-zabadi and Kouzani 2017; Swann et al. 2018).Peripheral motor activity, captured throughEMG electrodes or arm-mounted accelerome-ters, can be used alone or in combination withbrain signals to infer the presence and severityof motor symptoms for adaptive DBS (Para-starfeizabadi and Kouzani 2017). In terms ofeffectiveness, compared with open-loop DBS,adaptive DBS has been shown to provide anadditional clinical improvement of ∑25%–30%, a 20% reduction in side effects and a40%–55% reduction in stimulation time (Mei-dahl et al. 2017). Two commercial systems arecurrently Food and Drug Administration(FDA) approved and can provide closed-loopDBS: the responsive neurostimulation (RNS)System by NeuroPace, which is also used totreat epilepsy through cortical stimulation,and the Activa PC+S system by Medtronic.They both respond with appropriately timedneural stimulation pulses to either brain or pe-ripheral signals indicative of motor symptomsin PD.
Closed-Loop Neuromodulation
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314 11
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Control of Hemodynamic Function viaClosed-Loop Vagus Nerve Stimulation
The cardiovascular (CV) system is physiologi-cally regulated by the autonomic nervous systemin a responsive, dynamic fashion. In addition, ina variety of conditions, it shows complex time-dependent pathophysiology, with the autonom-ic nervous system implicated in it. Therefore, asis the case with the brain, it is appropriate toconsider treating CV disorders within a CLNframework. Although closed-loop control ofheart rhythm using pacing technology hasbeen a mainstay of clinical cardiology, neuro-modulation-based control of CV physiologyand treatment of CV disorders have only recent-ly received attention. Autonomic, sympathetic,or parasympathetic nerve stimulation has beensuccessfully used in experimental animals tocontrol systemic BP (Plachta et al. 2014), HR(Ardell et al. 2017), atrial fibrillation (Choiet al. 2017), ventricular arrhythmias (Brueg-mann et al. 2016), heart failure (Premchandet al. 2014), etc. The main advantage of neuro-modulation-based over traditional drug-basedtherapies in CV diseases is the potential forhighly selective modulation of different hemo-dynamic parameters in a responsive and adap-tive manner. However, no CLN system respond-ing to changes inCVphysiologic parameters hasbeen implemented yet beyond some theoreticaldesigns (Romero-Ugalde et al. 2017, 2018).
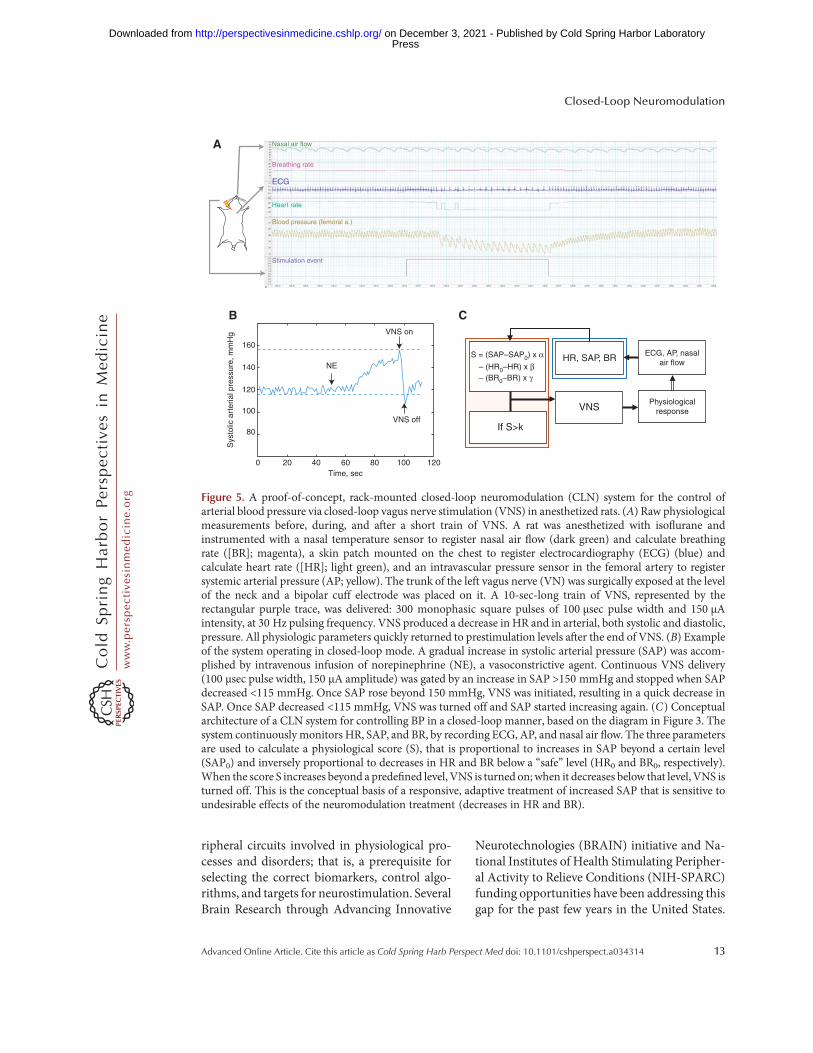
In a proof-of-concept experiment, we usedresponsive, closed-loop cervical VNS to controlsystemic BP in rats. Rats anesthetized with iso-flurane were instrumented with ECG sensors, anasal flow sensor, and a BP sensor in the femoralartery, which allowed us to monitor their HR,breathing rate (BR), and arterial BP (Fig. 5).After exposing the carotid sheath at the neckand separating the VN from its vascular ele-ments, we placed a flexible cuff around the leftVN and connected the cuff to a rack-mountedstimulator. In constant current mode, trains ofmonophasic rectangular pulses (100 µsec pulsewidth, 30 Hz, 300 pulses) were delivered to theVN, in increasing amplitudes, until a physio-logical response, defined as a stimulus-elicitedchange in HR, BR or BP, was noted; that ampli-
tudewas considered the physiological threshold.Delivery of similar VNS trains at supra-thresh-old amplitudes was associated with a rapid de-crease in HR and in systolic arterial pressure(SAP); a similarly swift return of these parame-ters to prestimulation levels occurred once VNSwas discontinued (Fig. 5A). Once all physiolog-ical parameters had stabilized, continuous intra-venous administration of norepinephrine, anagent that causes vasoconstriction, was initiatedand a gradual increase in SAP was noted (Fig.5B). At the same time, the stimulator was pro-gramed to deliver continuous VNS (constantcurrent, monophasic rectangular pulses, 100µsec pulse width, 30 Hz, at current amplitudeequal to 1.5 times the physiological threshold)while SAP exceeded 150 mmHg; it was alsoprogramed to discontinue VNS when SAP de-creased below 115 mmHg. While the closed-loop VNS system was in operation, and despitethe continuous delivery of norepinephrine,“normal” levels of SAP, within the 115–150mmHg range, were maintained, without any oc-currences of hypotension (Fig. 5B).
Although there is evidence that VNS causesdirect vasodilation in different vascular beds(McMahon et al. 1992; Feliciano and Henning1998), which would explain the elicited decreasein SAP, the mechanism of action in this caselikely also involves a decrease in HR, reductionin cardiac contractility, inhibition of sympa-thetic tone, reflexive changes in the centralautonomic drive as a result of afferent vagal ac-tivation, and, finally, extraneural hemodynamiceffects from the spread of current beyond theVN to surrounding muscles and vessels. Takena step further, a CLN system that also takes intoaccount additional undesirable effects of VNS(e.g., significant decreases in HR or in BR) couldcontrol AP in a safer manner (Fig. 5C).
CHALLENGES AND OPPORTUNITIES FORCLOSED-LOOP NEUROMODULATION
There are several challenges for the wider use ofCLN systems in basic and translational physiol-ogy and, more importantly, in clinical medicine.First, there is urgent need for understanding theanatomy and physiology of the central and pe-
S. Zanos
12 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from
ripheral circuits involved in physiological pro-cesses and disorders; that is, a prerequisite forselecting the correct biomarkers, control algo-rithms, and targets for neurostimulation. SeveralBrain Research through Advancing Innovative
Neurotechnologies (BRAIN) initiative and Na-tional Institutes of Health Stimulating Peripher-al Activity to Relieve Conditions (NIH-SPARC)funding opportunities have been addressing thisgap for the past few years in the United States.
0 20 40 60Time, sec
80 100
VNS offIf S>k
VNS
ECG, AP, nasalair flow
S = (SAP–SAP0) x α– (HR0–HR) x β– (BR0–BR) x γ
HR, SAP, BR
Physiologicalresponse
VNS on
B C
NE
160
140
120
100
80
Sys
tolic
art
eria
l pre
ssur
e, m
mH
g
120
A
Stimulation event
Blood pressure (femoral a.)
Heart rate
ECG
Breathing rate
Nasal air flow
Figure 5. A proof-of-concept, rack-mounted closed-loop neuromodulation (CLN) system for the control ofarterial blood pressure via closed-loop vagus nerve stimulation (VNS) in anesthetized rats. (A) Raw physiologicalmeasurements before, during, and after a short train of VNS. A rat was anesthetized with isoflurane andinstrumented with a nasal temperature sensor to register nasal air flow (dark green) and calculate breathingrate ([BR]; magenta), a skin patch mounted on the chest to register electrocardiography (ECG) (blue) andcalculate heart rate ([HR]; light green), and an intravascular pressure sensor in the femoral artery to registersystemic arterial pressure (AP; yellow). The trunk of the left vagus nerve (VN) was surgically exposed at the levelof the neck and a bipolar cuff electrode was placed on it. A 10-sec-long train of VNS, represented by therectangular purple trace, was delivered: 300 monophasic square pulses of 100 µsec pulse width and 150 µAintensity, at 30 Hz pulsing frequency. VNS produced a decrease in HR and in arterial, both systolic and diastolic,pressure. All physiologic parameters quickly returned to prestimulation levels after the end of VNS. (B) Exampleof the system operating in closed-loop mode. A gradual increase in systolic arterial pressure (SAP) was accom-plished by intravenous infusion of norepinephrine (NE), a vasoconstrictive agent. Continuous VNS delivery(100 µsec pulse width, 150 µA amplitude) was gated by an increase in SAP >150 mmHg and stopped when SAPdecreased <115 mmHg. Once SAP rose beyond 150 mmHg, VNS was initiated, resulting in a quick decrease inSAP. Once SAP decreased <115 mmHg, VNS was turned off and SAP started increasing again. (C) Conceptualarchitecture of a CLN system for controlling BP in a closed-loop manner, based on the diagram in Figure 3. Thesystem continuously monitors HR, SAP, and BR, by recording ECG, AP, and nasal air flow. The three parametersare used to calculate a physiological score (S), that is proportional to increases in SAP beyond a certain level(SAP0) and inversely proportional to decreases in HR and BR below a “safe” level (HR0 and BR0, respectively).When the score S increases beyond a predefined level, VNS is turned on; when it decreases below that level, VNS isturned off. This is the conceptual basis of a responsive, adaptive treatment of increased SAP that is sensitive toundesirable effects of the neuromodulation treatment (decreases in HR and BR).
Closed-Loop Neuromodulation
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314 13
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Second, additional progress is needed in the fab-rication of tissue-friendly sensors, stimulationprobes, and implantable generators as well asin the design and implementation of energy-efficient and computationally powerful proces-sors that able to handle more complex detectionand optimization algorithms. Third, the special-ized physician training requirements and theregulatory steps involved in bringing such de-vices into the market are more complex and ex-pensive to navigate compared with open-loopstimulators, which make commercialization ef-forts riskier (Meidahl et al. 2017). However, asscientists, engineers, and physicians continue todefine the principles, methods, and applicationsfor CLN systems in physiological and transla-tional research, in animalmodels, and in humansubjects, it is expected that CLN systems willcomprise a significant portion of the growthforecasted for the neuromodulation market,from approximately $2.8 billion in 2016 tomore than $7 billion in 2025 (Accuray Research2018).
REFERENCES
Accuray Research. 2018. Global neuromodulation devicesmarket analysis and trends—Industry forecast to 2025.Accuray Research, Noida, Uttar Pradesh, India.
AlamM, RodriguesW, Pham BN, Thakor NV. 2016. Brain–machine interface facilitated neurorehabilitation viaspinal stimulation after spinal cord injury: Recent prog-ress and future perspectives. Brain Res 1646: 25–33.doi:10.1016/j.brainres.2016.05.039
Ali II, PirzadaNA,Kanjwal Y,Wannamaker B,MedhkourA,Koltz MT, Vaughn BV. 2004. Complete heart block withventricular asystole during left vagus nerve stimulationfor epilepsy. Epilepsy Behav 5: 768–771. doi:10.1016/j.yebeh.2004.05.008
Ardell JL, Nier H, Hammer M, Southerland EM, Ardell CL,Beaumont E, KenKnight BH, Armour JA. 2017. Definingthe neural fulcrum for chronic vagus nerve stimulation:Implications for integrated cardiac control. J Physiol 595:6887–6903. doi:10.1113/JP274678
Arle J. 2011. Surgical techniques in neuromodulation. InEssential neuromodulation (ed. Arle J, Shils JL), pp.269–282. Elsevier, Amsterdam.
Benda J, Gollisch T, Machens CK, Herz AVM. 2007. Fromresponse to stimulus: Adaptive sampling in sensory phys-iology. Curr Opin Neurobiol 17: 430–436. doi:10.1016/j.conb.2007.07.009
Bolus MF, Willats AA, Whitmire CJ, Rozell CJ, Stanley GB.2018. Design strategies for dynamic closed-loop optoge-netic neurocontrol in vivo. J Neural Eng 15: 026011.doi:10.1088/1741-2552/aaa506
Bouton CE, Shaikhouni A, Annetta NV, Bockbrader MA,Friedenberg DA, Nielson DM, Sharma G, Sederberg PB,Glenn BC, Mysiw WJ, et al. 2016. Restoring cortical con-trol of functional movement in a human with quadriple-gia. Nature 533: 247–250. doi:10.1038/nature17435
Bruegmann T, Boyle PM, Vogt CC, Karathanos TV, ArevaloHJ, Fleischmann BK, Trayanova NA, Sasse P. 2016. Op-togenetic defibrillation terminates ventricular arrhythmiain mouse hearts and human simulations. J Clin Invest126: 3894–3904. doi:10.1172/JCI88950
Bystritsky A, Korb AS, Douglas PK, Cohen MS, MelegaWP,Mulgaonkar AP, DeSalles A, Min BK, Yoo SS. 2011. Areview of low-intensity focused ultrasound pulsation.Brain Stimul 4: 125–136. doi:10.1016/j.brs.2011.03.007
CaligioreD,HelmichRC,HallettM,Moustafa AA, Timmer-mann L, Toni I, Baldassarre G. 2016. Parkinson’s diseaseas a system-level disorder. NPJ Parkinsons Dis 2: 16025.doi:10.1038/npjparkd.2016.25
Capogrosso M, Milekovic T, Borton D, Wagner F, MoraudEM,Mignardot JB, Buse N, Gandar J, Barraud Q, Xing D,et al. 2016. A brain–spine interface alleviating gait deficitsafter spinal cord injury in primates.Nature 539: 284–288.doi:10.1038/nature20118
Carrillo-Reid L, Yang W, Bando Y, Peterka DS, Yuste R.2016. Imprinting and recalling cortical ensembles. Science353: 691–694. doi:10.1126/science.aaf7560
Choi EK, Zhao Y, Everett TH, Chen PS. 2017. Ganglionatedplexi as neuromodulation targets for atrial fibrillation. JCardiovasc Electrophysiol 28: 1485–1491. doi:10.1111/jce.13319
Cogan SF. 2008. Neural stimulation and recording elec-trodes. Annu Rev Biomed Eng 10: 275–309. doi:10.1146/annurev.bioeng.10.061807.160518
Dan Y, Poo MM. 2004. Spike timing-dependent plasticity ofneural circuits. Neuron 44: 23–30. doi:10.1016/j.neu-ron.2004.09.007
Deadwyler SA, Hampson RE, Song D, Opris I, GerhardtGA, Marmarelis VZ, Berger TW. 2017. A cognitive pros-thesis for memory facilitation by closed-loop functionalensemble stimulation of hippocampal neurons in pri-mate brain. Exp Neurol 287: 452–460. doi:10.1016/j.expneurol.2016.05.031
Denison T, Litt B. 2014. Advancing neuromodulationthrough control systems: A general framework and casestudy in posture-responsive stimulation. Neuromodula-tion 17 (Suppl. 1): 48–57. doi:10.1111/ner.12170
Edwardson MA, Lucas TH, Carey JR, Fetz EE. 2013. Newmodalities of brain stimulation for stroke rehabilitation.Exp Brain Res 224: 335–358. doi:10.1007/s00221-012-3315-1
Erez Y, Tischler H, Moran A, Bar-Gad I. 2010. Generalizedframework for stimulus artifact removal. J NeurosciMeth-ods 191: 45–59. doi:10.1016/j.jneumeth.2010.06.005
Ethier C, Gallego JA, Miller LE. 2015. Brain-controlled neu-romuscular stimulation to drive neural plasticity andfunctional recovery. Curr Opin Neurobiol 33: 95–102.doi:10.1016/j.conb.2015.03.007
FammK, Litt B, Tracey KJ, Boyden ES, SlaouiM. 2013. Drugdiscovery: A jump-start for electroceuticals. Nature 496:159–161. doi:10.1038/496159a
S. Zanos
14 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Feliciano L, Henning RJ. 1998. Vagal nerve stimulationreleases vasoactive intestinal peptide which significantlyincreases coronary artery blood flow. Cardiovasc Res 40:45–55. doi:10.1016/S0008-6363(98)00122-9
Fetz EE. 2015. Restoring motor function with bidirectionalneural interfaces. Prog Brain Res 218: 241–252.doi:10.1016/bs.pbr.2015.01.001
Fisher RS, Afra P, Macken M, Minecan DN, Bagic A, Ben-badis SR, Helmers SL, Sinha SR, Slater J, Treiman D, et al.2016. Automatic vagus nerve stimulation triggered byictal tachycardia: Clinical outcomes and device perfor-mance—The U.S. E-37 Trial. Neuromodulation 19:188–195. doi:10.1111/ner.12376
Franke F, Natora M, Boucsein C, MunkMHJ, Obermayer K.2010. An online spike detection and spike classificationalgorithm capable of instantaneous resolution of overlap-ping spikes. J Comput Neurosci 29: 127–148. doi:10.1007/s10827-009-0163-5
Ganzer PD,DarrowMJ,Meyers EC, Solorzano BR, Ruiz AD,Robertson NM, Adcock KS, James JT, Jeong HS, BeckerAM, et al. 2018. Closed-loop neuromodulation restoresnetwork connectivity and motor control after spinal cordinjury. eLife 7: e32058. doi:10.7554/eLife.32058
Geller EB, Skarpaas TL, Gross RE, Goodman RR, BarkleyGL, Bazil CW, Berg MJ, Bergey GK, Cash SS, Cole AJ, etal. 2017. Brain-responsive neurostimulation in patientswith medically intractable mesial temporal lobe epilepsy.Epilepsia 58: 994–1004. doi:10.1111/epi.13740
Gilat M. 2018. Towards closed-loop deep brain stimulationfor freezing of gait in Parkinson’s disease. Clin Neuro-physiol 129: 2448–2450. doi:10.1016/j.clinph.2018.08.012
Gollisch T, Herz AVM. 2012. The iso-response method:Measuring neuronal stimulus integration with closed-loop experiments. Front Neural Circuits 6: 104.doi:10.3389/fncir.2012.00104
GuggenmosDJ, AzinM, Barbay S,Mahnken JD, DunhamC,Mohseni P, Nudo RJ. 2013. Restoration of function afterbrain damage using a neural prosthesis.ProcNatl Acad Sci110: 21177–21182. doi:10.1073/pnas.1316885110
Gunasekera B, Saxena T, Bellamkonda R, Karumbaiah L.2015. Intracortical recording interfaces: Current chal-lenges to chronic recording function.ACS ChemNeurosci6: 68–83. doi:10.1021/cn5002864
Gutruf P, Rogers JA. 2018. Implantable, wireless device plat-forms for neuroscience research.Curr Opin Neurobiol 50:42–49. doi:10.1016/j.conb.2017.12.007
Hamilton P, Soryal I, Dhahri P, Wimalachandra W, Leat A,Hughes D, Toghill N, Hodson J, Sawlani V, Hayton T, etal. 2018. Clinical outcomes of VNS therapywithAspireSR(including cardiac-based seizure detection) at a largecomplex epilepsy and surgery centre. Seizure 58: 120–126. doi:10.1016/j.seizure.2018.03.022
Hays SA, Rennaker RL, Kilgard MP. 2013. Targeting plastic-ity with vagus nerve stimulation to treat neurological dis-ease. Prog Brain Res 207: 275–299. doi:10.1016/B978-0-444-63327-9.00010-2
Hebb AO, Zhang JJ, Mahoor MH, Tsiokos C, Matlack C,Chizeck HJ, Pouratian N. 2014. Creating the feedbackloop: Closed-loop neurostimulation. Neurosurg Clin NAm 25: 187–204. doi:10.1016/j.nec.2013.08.006
Holleman J. 2016. Design considerations for neural ampli-fiers. Conf Proc IEEE Eng Med Biol Soc 2016: 6331–6334.
Jackson A, Mavoori J, Fetz EE. 2006a. Long-term motorcortex plasticity induced by an electronic neural implant.Nature 444: 56–60. doi:10.1038/nature05226
Jackson A, Moritz CT, Mavoori J, Lucas TH, Fetz EE. 2006b.The neurochip BCI: Towards a neural prosthesis for up-per limb function. IEEETrans Neural Syst Rehabil Eng 14:187–190. doi:10.1109/TNSRE.2006.875547
Kuo CH, White-Dzuro GA, Ko AL. 2018. Approaches toclosed-loop deep brain stimulation for movement disor-ders. Neurosurg Focus 45: E2.
Lewis PM, Thomson RH, Rosenfeld JV, Fitzgerald PB. 2016.Brain neuromodulation techniques: A review. Neurosci-entist 22: 406–421. doi:10.1177/1073858416646707
Little S, Brown P. 2014. The functional role of β oscillationsin Parkinson’s disease. Parkinsonism Relat Disord 20(Suppl. 1): S44–S48. doi:10.1016/S1353-8020(13)70013-0
Lo MC, Widge AS. 2017. Closed-loop neuromodulationsystems: Next-generation treatments for psychiatric ill-ness. Int Rev Psychiatry 29: 191–204. doi:10.1080/09540261.2017.1282438
Lopez-Gordo MA, Sanchez-Morillo D, Pelayo Valle F. 2014.Dry EEG electrodes. Sensors (Basel) 14: 12847–12870.doi:10.3390/s140712847
Maheshwari S, Acharyya A, Puddu PE, Mazomenos EB,Leekha G,Maharatna K, SchiaritiM. 2013. An automatedalgorithm for online detection of fragmented QRS andidentification of its various morphologies. J R Soc Inter-face 10: 20130761. doi:10.1098/rsif.2013.0761
Malmivuo J, Plonsey R. 1995.Magnetic stimulation of neuraltissue. In Bioelectromagnetism—Principles and applica-tions of bioelectric and biomagnetic fields, pp. 375–381.Oxford University Press, New York.
McCreery DB, Bullara LA, Agnew WF. 1986. Neuronal ac-tivity evoked by chronically implanted intracortical mi-croelectrodes. Exp Neurol 92: 147–161. doi:10.1016/0014-4886(86)90131-7
McMahon TJ, Hood JS, Kadowitz PJ. 1992. Pulmonary va-sodilator response to vagal stimulation is blocked by Nω-nitro-L-arginine methyl ester in the cat. Circ Res 70: 364–369. doi:10.1161/01.RES.70.2.364
McPherson JG, Miller RR, Perlmutter SI. 2015. Targeted,activity-dependent spinal stimulation produces long-last-ing motor recovery in chronic cervical spinal cord injury.Proc Natl Acad Sci 112: 12193–12198. doi:10.1073/pnas.1505383112
Meidahl AC, Tinkhauser G, Herz DM, Cagnan H, DebarrosJ, Brown P. 2017. Adaptive deep brain stimulation formovement disorders: The long road to clinical therapy.Mov Disord 32: 810–819. doi:10.1002/mds.27022
Merrill DR, Bikson M, Jefferys JG. 2005. Electrical stimu-lation of excitable tissue: Design of efficacious andsafe protocols. J Neurosci Methods 141: 171–198. doi:10.1016/j.jneumeth.2004.10.020
Morishita T, Inoue T. 2017. Need for multiple biomarkers toadjust parameters of closed-loop deep brain stimulationfor Parkinson’s disease. Neural Regen Res 12: 747–748.doi:10.4103/1673-5374.206642
Moritz CT, Perlmutter SI, Fetz EE. 2008. Direct control ofparalysed muscles by cortical neurons. Nature 456: 639–642. doi:10.1038/nature07418
Closed-Loop Neuromodulation
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314 15
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Napadow V, Edwards RR, Cahalan CM, Mensing G, Green-baum S, Valovska A, Li A, Kim J, Maeda Y, Park K, et al.2012. Evoked pain analgesia in chronic pelvic pain pa-tients using respiratory-gated auricular vagal afferentnerve stimulation. Pain Med 13: 777–789. doi:10.1111/j.1526-4637.2012.01385.x
Nishimura Y, Perlmutter SI, Eaton RW, Fetz EE. 2013a.Spike-timing-dependent plasticity in primate corticospi-nal connections induced during free behavior.Neuron 80:1301–1309. doi:10.1016/j.neuron.2013.08.028
Nishimura Y, Perlmutter SI, Fetz EE. 2013b. Restoration ofupper limb movement via artificial corticospinal andmusculospinal connections in a monkey with spinalcord injury. Front Neural Circuits 7: 57. doi:10.3389/fncir.2013.00057
Nudo R. 2014. Plasticity of cerebral motor functions: Impli-cations for repair and rehabilitation. InTextbook of neuralrepair and rehabilitation, 2nd ed. (ed. Selzer ME, et al.),pp. 99–113. Cambridge University Press, Cambridge.
Oweiss KG, Badreldin IS. 2015. Neuroplasticity subservingthe operation of brain–machine interfaces. Neurobiol Dis83: 161–171. doi:10.1016/j.nbd.2015.05.001
ParastarfeizabadiM, Kouzani AZ. 2017. Advances in closed-loop deep brain stimulation devices. J Neuroeng Rehabil14: 79. doi:10.1186/s12984-017-0295-1
Patel S, ParkH, Bonato P, ChanL, RodgersM. 2012.A reviewof wearable sensors and systems with application in reha-bilitation. J Neuroeng Rehabil 9: 21. doi:10.1186/1743-0003-9-21
Plachta DT, Gierthmuehlen M, Cota O, Espinosa N, BoeserF, Herrera TC, Stieglitz T, Zentner J. 2014. Blood pressurecontrol with selective vagal nerve stimulation and mini-mal side effects. J Neural Eng 11: 036011. doi:10.1088/1741-2560/11/3/036011
Premchand RK, Sharma K, Mittal S, Monteiro R, Dixit S,Libbus I, DiCarlo LA, Ardell JL, Rector TS, Amurthur B,et al. 2014. Autonomic regulation therapy via left or rightcervical vagus nerve stimulation in patients with chronicheart failure: Results of the ANTHEM-HF trial. J CardFail 20: 808–816. doi:10.1016/j.cardfail.2014.08.009
Pruitt DT, Schmid AN, Kim LJ, Abe CM, Trieu JL, Choua C,Hays SA, Kilgard MP, Rennaker RL. 2016. Vagus nervestimulation delivered with motor training enhances re-covery of function after traumatic brain injury. J Neuro-trauma 33: 871–879. doi:10.1089/neu.2015.3972
Raducanu BC, Yazicioglu RF, Lopez CM, Ballini M, PutzeysJ, Wang S, Andrei A, Rochus V, Welkenhuysen M, vanHelleputte N, et al. 2017. Time multiplexed active neuralprobe with 1356 parallel recording sites. Sensors (Basel)17: E2388. doi:10.3390/s17102388
Ramgopal S, Thome-Souza S, Jackson M, Kadish NE, Sán-chez Fernández I, Klehm J, Bosl W, Reinsberger C,Schachter S, Loddenkemper T. 2014. Seizure detection,seizure prediction, and closed-loop warning systems inepilepsy. Epilepsy Behav 37: 291–307. doi:10.1016/j.ye-beh.2014.06.023
Rebesco JM, Stevenson IH, Kording KP, Solla SA, Miller LE.2010. Rewiring neural interactions by micro-stimulation.Front Syst Neurosci 4: 39. doi:10.3389/fnsys.2010.00039
Rembado I, Zanos S, Fetz EE. 2017. Cycle-triggered corticalstimulation during slow wave sleep facilitates learning a
BMI task: A case report in a non-human primate. FrontBehav Neurosci 11: 59. doi:10.3389/fnbeh.2017.00059
Rijnbeek EH, EleveldN,OlthuisW. 2018. Update on periph-eral nerve electrodes for closed-loop neuroprosthetics.Front Neurosci 12: 350. doi:10.3389/fnins.2018.00350
Romero-Ugalde HM, Le Rolle V, Bonnet JL, Henry C, Bel A,Mabo P, Carrault G, Hernández AI. 2017. A novel con-troller based on state-transition models for closed-loopvagus nerve stimulation: Application to heart rate regula-tion. PLoS ONE 12: e0186068.
Romero-Ugalde HM, Le Rolle V, Bonnet JL, Henry C, MaboP, Carrault G, Hernández AI. 2018. Closed-loop vagusnerve stimulation based on state transition models.IEEE Trans Biomed Eng 65: 1630–1638. doi:10.1109/TBME.2017.2759667
Russo M, Cousins MJ, Brooker C, Taylor N, Boesel T, Sulli-van R, Poree L, Shariati NH, Hanson E, Parker J. 2018.Effective relief of pain and associated symptoms withclosed-loop spinal cord stimulation system: Preliminaryresults of the Avalon Study. Neuromodulation 21: 38–47.doi:10.1111/ner.12684
Schalk G, Leuthardt EC. 2011. Brain–computer interfacesusing electrocorticographic signals. IEEE Rev BiomedEng 4: 140–154. doi:10.1109/RBME.2011.2172408
Sclocco R, Garcia RG, Gabriel A, Kettner NW, Napadow V,Barbieri R. 2017. Respiratory-gated auricular vagal affer-ent nerve stimulation (RAVANS) effects on autonomicoutflow in hypertension. Conf Proc IEEE Eng Med BiolSoc 2017: 3130–3133.
Sharma G, Weber D. 2018. Closing the loop for bioelectron-ic medicine. MedDevice Online, www.meddeviceonline.com.
Sim JY, Haney MP, Park SI, McCall JG, Jeong JW. 2017.Microfluidic neural probes: In vivo tools for advancingneuroscience. Lab Chip 17: 1406–1435. doi:10.1039/C7LC00103G
Stein E, Bar-Gad I. 2013. β oscillations in the cortico-basalganglia loop during parkinsonism. Exp Neurol 245: 52–59. doi:10.1016/j.expneurol.2012.07.023
Swann NC, de Hemptinne C, ThompsonMC,Miocinovic S,Miller AM, Gilron R, Ostrem JL, Chizeck HJ, Starr PA.2018. Adaptive deep brain stimulation for Parkinson’sdisease using motor cortex sensing. J Neural Eng 15:046006. doi:10.1088/1741-2552/aabc9b
Tator CH, Minassian K, Mushahwar VK. 2012. Spinal cordstimulation: Therapeutic benefits and movement genera-tion after spinal cord injury.HandbClinNeurol 109: 283–296. doi:10.1016/B978-0-444-52137-8.00018-8
Thomas GP, Jobst BC. 2018. Feedback-sensitive and closed-loop solutions. In Innovative neuromodulation (ed. Arle J,Shils J), pp. 41–59. Elsevier, Amsterdam.
Tinkhauser G, Pogosyan A, Little S, Beudel M, Herz DM,Tan H, Brown P. 2017. The modulatory effect of adaptivedeep brain stimulation on β bursts in Parkinson’s disease.Brain 140: 1053–1067. doi:10.1093/brain/awx010
van Dongen M, Serdijn W. 2016. Design of efficient andsafe neural stimulators: A multidisciplinary approach.Springer, New York.
Wenger N, Moraud EM, Raspopovic S, Bonizzato M, Di-Giovanna J, Musienko P, Morari M, Micera S, CourtineG. 2014. Closed-loop neuromodulation of spinal sensori-
S. Zanos
16 Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

motor circuits controls refined locomotion after com-plete spinal cord injury. Sci Transl Med 6: 255ra133.doi:10.1126/scitranslmed.3008325
Won SM, Song E, Zhao J, Li J, Rivnay J, Rogers JA. 2018.Recent advances in materials, devices, and systems forneural interfaces. Adv Mater 30: e1800534. doi:10.1002/adma.201800534
Young GB, Ives JR, Chapman MG, Mirsattari SM. 2006. Acomparison of subdermal wire electrodes with collodion-applied disk electrodes in long-term EEG recordings inICU. Clin Neurophysiol 117: 1376–1379. doi:10.1016/j.clinph.2006.02.006
Zanos S. 2009. Neural correlates of high-frequency intra-cortical and epicortical field potentials. J Neurosci 29:3673–3675. doi:10.1523/jneurosci.0009-09.2009
Zanos S. 2013. “Cortical surface recurrent brain-computerinterfaces.”PhD thesis, University ofWashington, Seattle.
Zanos S, Richardson AG, Shupe L, Miles FP, Fetz EE. 2011.The Neurochip-2: An autonomous head-fixed computerfor recording and stimulating in freely behavingmonkeys.IEEE Trans Neural Syst Rehabil Eng 19: 427–435.doi:10.1109/tnsre.2011.2158007
Zanos S, Rembado I, Chen D, Fetz EE. 2018. Phase-lockedstimulation during cortical β oscillations produces bidi-rectional synaptic plasticity in awake monkeys. Curr Biol28: 2515–2526.e4. doi:10.1016/j.cub.2018.07.009
Zimmermann JB, Jackson A. 2014. Closed-loop control ofspinal cord stimulation to restore hand function afterparalysis. Front Neurosci 8: 87. doi:10.3389/fnins.2014.00087
Closed-Loop Neuromodulation
Advanced Online Article. Cite this article as Cold Spring Harb Perspect Med doi: 10.1101/cshperspect.a034314 17
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from
published online December 17, 2018Cold Spring Harb Perspect Med Stavros Zanos ResearchClosed-Loop Neuromodulation in Physiological and Translational
Subject Collection Bioelectronic Medicine
DiseaseMedicine in Treatment of Chronic Inflammatory Neural Control of Inflammation: Bioelectronic
Centa, et al.Michael Eberhardson, Laura Tarnawski, Monica
Disease Diagnosis and Treatmenton the Inflammatory Reflex to New Approaches in Bioelectronic Medicine: From Preclinical Studies
J. TraceyValentin A. Pavlov, Sangeeta S. Chavan and Kevin
Therapeutic ImplicationsPathways Using Ultrasound and Its Current Noninvasive Neuromodulation of Peripheral Nerve
Christopher Puleo and Victoria Cotero
SystemVagus Nerve Stimulation and the Cardiovascular
Lance B. BeckerMichael J. Capilupi, Samantha M. Kerath and
Enteric Neuromodulation for the Gut and BeyondYogi A. Patel and Pankaj J. Pasricha Treatment of Inflammation-Mediated Diseases
Harnessing the Inflammatory Reflex for the
ChernoffYaakov A. Levine, Michael Faltys and David
SystemOptogenetic Control of the Peripheral Nervous
Rui B. Chang and Biomarkers of DiseaseRelated to Changes in Physiological Parameters Recording and Decoding of Vagal Neural Signals
Theodoros P. Zanos
and Translational ResearchClosed-Loop Neuromodulation in Physiological
Stavros Zanos State and Future DirectionsBioelectronic Neural Bypass Approach: Current Restoring Movement in Paralysis with a
Chad E. Bouton
Assessment: An OverviewElectrical Impedance Methods in Neuromuscular
Seward B. Rutkove and Benjamin Sanchez
Ethical Concerns−−Bioelectronic Medicine
HaridatSamuel Packer, Nicholas Mercado and Anita
Solutions Precision-Guided by LightOptogenetic Medicine: Synthetic Therapeutic
Haifeng Ye and Martin Fussenegger
Use of Bioelectronics in the Gastrointestinal TractLarry Miller, Aydin Farajidavar and Anil Vegesna
NanoparticleTechnobiology's Enabler: The Magnetoelectric
Sakhrat KhizroevGut Interactions
−Vagus Nerve Stimulation at the Interface of Brain
Bruno Bonaz, Valérie Sinniger and Sonia Pellissier
http://perspectivesinmedicine.cshlp.org/cgi/collection/ For additional articles in this collection, see
Copyright © 2018 Cold Spring Harbor Laboratory Press; all rights reserved
Press on December 3, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from