Clinimetric Properties of Neuro-Motor Assessments
13
A systematic review of the clinimetric properties of neuromotor assessments for preterm infants during the first year of life Alicia J Spittle* MSc BPhysio, Victorian Infant Brain Studies; Lex W Doyle MD FRACP, Department of Obstetrics and Gynecology, University of Melbourne; Roslyn N Boyd PhD MSc (Physiotherapy) BAppSc BSc Pgrad (Biomechanics), Victorian Infant Brain Studies, Murdoch Childrens Research Institute, Melbourne, Australia. *Correspondence to first author at Victorian Infant Brain Studies, Murdoch Childrens Research Institute, 2nd Floor, Royal Children’s Hospital, Flemington Road, Parkville, Melbourne, Australia 3052. E-mail: [email protected] DOI: 10.1111/j.1469-8749.2008.02025.x Published online 8th January 2008 This systematic review evaluates assessments used to discriminate, predict, or evaluate the motor development of preterm infants during the first year of life. Eighteen assessments were identified; nine met the inclusion criteria. The Alberta Infant Motor Scale (AIMS), Bayley Scale of Infant and Toddler Development – Version III, Peabody Developmental Motor Scales – Version 2, Test of Infant Motor Performance (TIMP), and Toddler and Infant Motor Examination have good discriminative validity when examined in large populations. The AIMS, Prechtl’s Assessment of General Movements (GMs), Neuro Sensory Motor Development Assessment (NSMDA), and TIMP were designed for preterm infants and are able to detect more subtle changes in movement quality. The best predictive assessment tools are age dependent: GMs, the Movement Assessment of Infants, and TIMP are strongest in early infancy (age 4mo or less) and the AIMS and NSMDA are better at older ages (8–12mo). The TIMP is the only tool that has demonstrated a difference between groups in response to intervention in two randomized controlled trials. The AIMS, TIMP, and GMs demonstrated the highest levels of overall reliability (interrater and intrarater intraclass correlation coefficient or κ >0.85). Selection of motor assessment tools during the first year of life for infants born preterm will depend on the intended purpose of their use for discrimination, prediction, and/or evaluation. With survival rates of preterm and low-birthweight infants improving, there is an increase in the number of these infants with motor impairments later in life, ranging from develop- mental coordination disorder to cerebral palsy (CP). 1 In 2006, the American Academy of Pediatrics published guide- lines for the follow-up of preterm infants and recommended that all children with a very low birthweight (birthweight <1500g) should have a structured, age-appropriate neuro- motor examination at least twice during the first year of life. 2 Infant neuromotor examinations are performed for a vari- ety of purposes, including discriminating between infants who have motor dysfunction and those who are developing typically (discriminative tool), predicting which infants will have future motor problems from current performance (pre- dictive tool), and evaluating changes over time (evaluative tool). 3 There is a growing body of evidence that the first year of an infant’s life is a critical period of brain development. 4 The process of neuronal differentiation, which includes the forma- tion of dendrites and axons, and the production of neuro- transmitters and synapses, is particularly active in the few months before and after term. 5 Myelination begins during the second trimester and is most rapid in the first year of life, and the process continues up to 30 years of age. 4 It is, therefore, important that infants with motor dysfunction are identified early so that appropriate interventions can be implemented. Early neuromotor assessments can be challenging because motor development in the first year of life is rapid and exten- sive and is influenced by biological, environmental, and social factors. 6 Repeated assessments may reveal widely different 254 Developmental Medicine & Child Neurology 2008, 50: 254–266 Review See end of paper for list of abbreviations.
-
Upload
amiteshmpth -
Category
Documents
-
view
42 -
download
0
Transcript of Clinimetric Properties of Neuro-Motor Assessments

A systematic reviewof the clinimetricproperties ofneuromotorassessments forpreterm infants duringthe first year of life
Alicia J Spittle* MSc BPhysio, Victorian Infant Brain Studies;Lex W Doyle MD FRACP, Department of Obstetrics andGynecology, University of Melbourne;Roslyn N Boyd PhD MSc (Physiotherapy) BAppSc BSc Pgrad(Biomechanics), Victorian Infant Brain Studies, MurdochChildrens Research Institute, Melbourne, Australia.
*Correspondence to first author at Victorian Infant BrainStudies, Murdoch Childrens Research Institute, 2nd Floor,Royal Children’s Hospital, Flemington Road, Parkville,Melbourne, Australia 3052. E-mail: [email protected]
DOI: 10.1111/j.1469-8749.2008.02025.xPublished online 8th January 2008
This systematic review evaluates assessments used todiscriminate, predict, or evaluate the motor development ofpreterm infants during the first year of life. Eighteenassessments were identified; nine met the inclusion criteria.The Alberta Infant Motor Scale (AIMS), Bayley Scale ofInfant and Toddler Development – Version III, PeabodyDevelopmental Motor Scales – Version 2, Test of Infant MotorPerformance (TIMP), and Toddler and Infant MotorExamination have good discriminative validity whenexamined in large populations. The AIMS, Prechtl’sAssessment of General Movements (GMs), Neuro SensoryMotor Development Assessment (NSMDA), and TIMP weredesigned for preterm infants and are able to detect moresubtle changes in movement quality. The best predictiveassessment tools are age dependent: GMs, the MovementAssessment of Infants, and TIMP are strongest in earlyinfancy (age 4mo or less) and the AIMS and NSMDA arebetter at older ages (8–12mo). The TIMP is the only tool thathas demonstrated a difference between groups in response tointervention in two randomized controlled trials. The AIMS,TIMP, and GMs demonstrated the highest levels of overallreliability (interrater and intrarater intraclass correlationcoefficient or κ>0.85). Selection of motor assessment toolsduring the first year of life for infants born preterm willdepend on the intended purpose of their use fordiscrimination, prediction, and/or evaluation.
With survival rates of preterm and low-birthweight infantsimproving, there is an increase in the number of these infantswith motor impairments later in life, ranging from develop-mental coordination disorder to cerebral palsy (CP).1 In2006, the American Academy of Pediatrics published guide-lines for the follow-up of preterm infants and recommendedthat all children with a very low birthweight (birthweight<1500g) should have a structured, age-appropriate neuro-motor examination at least twice during the first year of life.2
Infant neuromotor examinations are performed for a vari-ety of purposes, including discriminating between infantswho have motor dysfunction and those who are developingtypically (discriminative tool), predicting which infants willhave future motor problems from current performance (pre-dictive tool), and evaluating changes over time (evaluativetool).3 There is a growing body of evidence that the first year ofan infant’s life is a critical period of brain development.4 Theprocess of neuronal differentiation, which includes the forma-tion of dendrites and axons, and the production of neuro-transmitters and synapses, is particularly active in the fewmonths before and after term.5 Myelination begins during thesecond trimester and is most rapid in the first year of life, andthe process continues up to 30 years of age.4 It is, therefore,important that infants with motor dysfunction are identifiedearly so that appropriate interventions can be implemented.
Early neuromotor assessments can be challenging becausemotor development in the first year of life is rapid and exten-sive and is influenced by biological, environmental, and socialfactors.6 Repeated assessments may reveal widely different
254 Developmental Medicine & Child Neurology 2008, 50: 254–266
Review
See end of paper for list of abbreviations.

Review 255
scores that represent random variation in performance acrosstesting sessions, rather than real change in performance.7
Furthermore, preterm infants have been shown to have dif-ferent motor trajectories from those of infants born at term,
Table II: Excluded infant motor assessments
Reason excluded Assessment tool
Neonatal developmental assessment Dubowitz Neurological Assessment of the Preterm and Full-term Newborn Infant40
Neonatal Intensive Care Unit Network Neurobehavioral Scale41
Infant developmental assessment Revised Gesell Developmental Schedules42
Griffith General Cognitive Index,43,Denver II44
Pediatric Evaluation of Disability Inventory45
Battelle Developmental Inventory46
Neurological assessment Infant Neurological International Battery47
Manual not published Structured Observation of Motor Performance48
Table I: Characteristics of infant motor assessments
Assessment Primary Other Age Type Normative Domains Components testedtool (y) purpose purposes range of test sample tested
AIMS Discriminative Predictive, 0–18mo Norm 2202 infants from Gross motor Weight bearing, posture, (1994) evaluative Alberta, Canada and antigravity movement
BSITD-III Discriminative Predictive, 1–42mo Norm 1700 infants from Gross motor, Gross motor and fine motor tasks(2005) evaluative USA fine motor
GMs Discriminative, Evaluative Preterm Criterion NA Gross motor Spontaneous movement(2004) predictive birth to 4mo and neurological integrity
MAI Discriminative Predictive, 0–12mo Criterion NA Gross motor, Muscle tone, reflexes, automatic(1980) evaluative fine motor reactions, and volitionalmovement
NSMDA Discriminative, Evaluative 1mo–6y Criterion NA Gross motor, Gross motor, fine motor, (1989) predictive fine motor neurological, primitive reflexes,
postural reactions, and motorresponses to sensory input
PDMS-2 Discriminative, 0–5y Norm 2003 infants from Gross motor, Reflexes, stationary, locomotion,(2000) predictive, USA and Canada fine motor object manipulation, grasping,
evaluative and visual motor integration
PFMAI Discriminative Evaluative 2–12mo Criterion NA Gross motor, Posture and fine motor(2000) fine motor control and function
TIMP Discriminative, Predictive 32wks’ PMA Norm 990 infants at risk of Gross motor Observation of movement and(2005) evaluative to 4mo poor neurological elicited items to assess postural
outcome from USA control and function
TIME Discriminative, 4–42mo Norm 731 typically Gross motor, Mobility, stability, motor(1994) evaluative developing and fine motor organization, andsocial/emotional 144 motor-delayedabilities, functional performance,
children from USA and atypical movement
AIMS, Alberta Infant Motor Scale;15 BSITD-III, Bayley Scales of Infant and Toddler Development – Version III;37 GMs, General MovementsAssessment;23 MAI, Movement Assessment of Infants;38 NSDMA, Neuro Sensory Motor Development Assessment;24 PDMS-2, PeabodyDevelopmental Motor Scale – Version 2;25 PFMAI, Posture and Fine Motor Assessment of Infants;26 TIMP, Test of Infant Motor Performance;39
TIME, Toddler and Infant Motor Examination;28 PMA, post-menstrual age; NA, not applicable.

which may result in the motor development of preterm infantsincorrectly being labeled as ‘abnormal’.8 These variations inmotor development over the first year can be for a variety ofreasons, including behaviours learned during long periodsin neonatal intensive care and alterations to brain develop-ment caused by exposure to the ex utero environment dur-ing critical periods of brain development. This results ininfants who have less flexed postures and are more extendedthan infants born at term.1 A standardized assessment toolappropriate for preterm infants that has a consistent set of
procedures for administering and scoring an assessmentshould, therefore, be used to ensure that all individuals areassessed under similar conditions. Longitudinal assessments,rather than a single assessment, are more predictive becausethey give information on developmental progression includ-ing monitoring peaks, plateaux, and, in some cases, regres-sion of infants.9,10 For this reason, it is important to ensurethat assessment tools can be used at more than one timepoint in the infant’s development.
The major types of standardized test are norm-referenced
256 Developmental Medicine & Child Neurology 2008, 50: 254–266
Table III: Clinical utility of included infant assessment tools
Assessment Time to administer Test procedure Manual/equipmenttool (min)
AIMS 10–30 Observation of infant in prone, Comprehensive manual and score sheets (US $80)supine, sitting, and standing No special equipment
BSITD-III 20–60 Therapist administers items in Comprehensive manual/kit (US $300)standardized procedure Test kit provides most equipment
GMs 10–30 Infants’ spontaneous movements Comprehensive manual with DVD (US $80)with no stimulation are filmed and Special equipment (video)scoring completed from videotape
MAI 30–60 Therapist observes and Manualadministers items No special equipment
NSMDA 10–30 Therapist observes and Basic manual (US $20)administers items Specific toys required but easily accessible
PDMS-2 30–60 Therapist administers items in Comprehensive manual/test kit (US $945)standardized procedure Test kit provides most equipment
PFMAI 25–30 Therapist administers elicited Manual (US $63)items in standardized procedure No special equipment
TIMP 20–40 Therapist observes infant and Comprehensive manual/test (US $60)then administers elicited items Test provides equipment
in standardized procedure
TIME 15–55 Therapist observes infant and Comprehensive manual/test kit (US $417)parent/caregiver is used to Test kit provides most equipment
encourage movement
AIMS, Alberta Infant Motor Scale;15 BSITD-III, Bayley Scales of Infant and Toddler Development – Version III;37 GMs, General MovementsAssessment;23 MAI, Movement Assessment of Infants;38 NSDMA, Neuro Sensory Motor Development Assessment;24 PDMS-2, PeabodyDevelopmental Motor Scale – Version 2;25 PFMAI, Posture and Fine Motor Assessment of Infants;26 TIMP, Test of Infant Motor Performance;39
TIME, Toddler and Infant Motor Examination.28

and criterion-referenced measures.11 Norm-referenced testsmeasure the performance of a person in relation to a specificpopulation. Raw scores from these tests are meaningless bythemselves and need to be compared with a population.When using norm-referenced assessments it is important toconsider the characteristics of the reference population, asmotor development may vary across different social and eth-nic populations.12 Criterion-referenced tests have criteria ora minimum competence that must be reached to score anitem or pass the test. The criterion test contrasts the child’s
performance with the test content rather than a population.Some tests are referenced both by norm and by criterion.
Infant motor examinations vary with the age of the childand the theoretical construct of the assessment tool.13 Someassessment tools involve observation of the infant’s move-ment repertoire with minimal or no handling, whereas othersinclude neurological examination (assessment of reflexes,muscle tone, postural reactions). Traditionally, motor assess-ments are based on the neuromaturational framework, whichassumes that the rate and sequence of motor development
Review 257
Table III: continued
Training Scoring Interpretation of scores
Not required 4 subscales – prone (21 items), supine (9 items), sitting (12 items), Raw scoresand standing (16 items). Score given to all observed items within Centile ranks
window and all items below the window Age equivalentGrowth scores
Required unless Motor scale – gross (72 items) and fine motor (66 items) subscales. Raw scorespsychologist Binary score for each item with reverse and discontinue rules Composite scores(2d course) Centile ranks
Age equivalentGrowth scores
Required (4–5d Movements classified as normal or abnormal (poor repertoire, Individual developmental training with cramped synchronized or chaotic) from preterm up to 6wks. trajectory GMs Trust) During fidgety period from 9 to 20wks’ movement classified Optimality score
as present, abnormal, or absent
Not required Scores development as normal, minimal problems, or specific Raw scoresproblems. Risk profiles for 4 and 8mo Risk scores
Not required Criteria given for items in 6 subscales: gross motor, fine motor, Raw scoresneurological, postural control, primitive movement patterns, Age equivalents
and sensory motor. Items scored as abnormal, suspicious, Functional scoresnormal for age
Not required Criteria given for items in 6 subscales: reflexes (8 items), Raw scoresstationary (30 items), locomotion (89 items), object Age equivalents
manipulation (24 items), grasping (26 items), Centile ranksvisual–motor integration (72 items) Standard scores for subtests
Not required PFMAI-I (0–6mo): 18 posture and 21 fine motor items, Raw scores PFMAI-II (6–12mo): 13 posture and 17 fine motor items Classification of infants’ motor
development as typical, at-risk,or delayed
Instructional DVD 42 items: 13 dichotomous observed items and Raw scoresavailable for self- 29 elicited items on 4–7-level rating scale Age equivalent scores education Centile ranks
Growth scores
Not required Subtests include mobility, motor organization, stability, Raw scoresfunctional performance, and social/emotional abilities. Scaled scores
Scoring differs for subtests Age equivalent scoresCentile ranks
Growth scores

are invariant and that the acquisition of motor skills reflectsthe hierarchical order of the central nervous system.14 Theenvironment is considered to have little impact on the per-formance of motor tasks in this framework.15 More recently,assessment tools have been developed that use alternativetheories of motor development such as the dynamic systemstheory, in which the development of motor skills is consid-ered to emerge through the interaction of multiple subsys-tems and is dependent on the context of the task.14 Assessmentsthat incorporate dynamic systems theory measure functionalcapacity and consider the environmental influences to sup-port the infant’s best performance. The theoretical frame-work should be considered when choosing an assessmentbecause it will influence the conclusions that can be madefrom the results.
There have been several reviews of newborn examinationsand preschool assessments; however, to our knowledge therehave been no recent systematic reviews of the clinimetricproperties of infant motor assessment tools.16,17 The aim ofthis review was to systematically identify and evaluate stan-dardized assessments that are used to discriminate, predict,or evaluate the motor development of preterm infants withinthe first year of life. For the purpose of this review, motor dys-function or delay will be referred to as ‘atypical’ developmentrather than ‘abnormal’ development because the latter termis ambiguous and does not always equate to abnormal motorfunction at a later age.8
MethodSEARCH STRATEGY
A comprehensive search was undertaken of computerizeddatabases including Medline Advanced (1966 to February2007), CINAHL (1982 to February 2007), PsycINFO (1966 toFebruary 2007), and EMBASE (1988 to February 2007). Thesearch strategy included the MeSH terms and text words for(‘premature infant’ OR ‘low-birthweight infant’) AND (‘out-come assessment’ OR ‘psychomotor performance’ OR ‘psy-chomotor disorders’ OR ‘cerebral palsy’ OR ‘developmentalcoordination disorder’ OR ‘movement disorders’ OR ‘motorskill disorders’). After this search, additional searches wereperformed using the names of each identified assessmenttool and their authors .
INCLUSION CRITERIA
Assessment tools were included if they met all of the followingcriteria: (1) discriminative, predictive, or evaluative of motordevelopment up to 12 months of age, corrected for prematu-rity; (2) appropriate for use with preterm infants (less than 37week’s gestational age); (3) standardized assessment proce-dure; and (4) criterion-referenced or norm-referenced test.
EXCLUSION CRITERIA
Assessment tools were excluded if they met any of the followingcriteria: (1) not published in English; (2) did not primarily assessmotor development (examination tools and developmentalassessments for newborn infants were excluded from thisreview, because motor development is only one componentof these assessments and other comprehensive reviews havebeen completed); and (3) primarily intended for screening.
DATA EXTRACTION
The titles and abstracts were screened by the first author.
Two authors (AS, RB) then reviewed one key paper for eachmeasure, selected on the basis that adequate detail was pro-vided for the determination of inclusion. Assessments wereincluded after agreement by both raters, and conflicting view-points were discussed until consensus was reached.
A modified version of the Outcome Measures Rating Form18
was used to collect information on the characteristics, clinicalutility, and psychometric properties of the included assess-ment tools. Characteristics of the assessment tools that weredocumented included the primary purpose of the tool, whetherit was discriminative, predictive, or evaluative, and age rangefor use, standardization samples, and domains tested.17,19
Psychometric properties included information on thevalidity and reliability of the assessment tools. Validity is theextent to which an assessment is measuring what it is intend-ed to measure.20 There are several different aspects to validi-ty, including content, construct, criterion and discriminativevalidity, and responsiveness.3,20,21 Content validity refers tothe extent to which measurement covers all the importantaspects or domains it is supposed to measure and is usuallydependent on a panel of experts and literature reviews.11
Construct validity is considered when there are no criteriaagainst which to evaluate the measure; instead the measureis compared with current theories and models of the con-struct. Criterion validity examines the agreement betweenthe assessment tool and a ‘gold standard’ tool used to evalu-ate the same construct. Criterion validity is usually dividedinto concurrent validity (correlation between the measure-ment tool and an alternative, equivalent measurement usedat the same time) and predictive validity (accuracy of a mea-surement tool to predict future outcome, such as CP),depending on whether the criteria refer to current or futureassessment. Evaluative validity or responsiveness refers tothe ability of an evaluative measure to detect minimal clini-cally important change over time.19 Sensitivity refers to theability for a test to detect someone with a condition (e.g.motor delay) when it is present. Specificity refers to the abili-ty of a test to correctly identify those infants without a condi-tion (e.g. normal motor development).19
Reliability describes the extent to which a test is depend-able, stable, and consistent when repeated under identicalconditions.21 Test–retest reliability refers to the relative stabilityof the assessment over time. Intrarater reliability is a compo-nent of test–retest reliability because it assesses the degree towhich an assessment yields similar results when the same raterscores the examination at different times in the absence ofgrowth or interventions. Interrater reliability assesses thedegree to which an assessment yields similar results for thesame individual at the same time with more than one rater.Internal consistency is defined as the extent to which the itemsof a test work together to measure a specific variable.20
Appropriate statistics for measuring inter- and intrarater relia-bility are intraclass correlation coefficient (ICC) or κ, not per-centage of agreement between raters or Pearson’scorrelation.21 Studies in which only the percentage of agree-ment was reported were excluded. Measures of 0.80 or abovewere considered excellent, 0.6 to 0.79 as adequate, and lessthan 0.60 as poor for reported ICC and κ statistics.18
ResultsEighteen motor assessment tools were identified by the searchstrategy, of which nine met all the predefined inclusion criteria
258 Developmental Medicine & Child Neurology 2008, 50: 254–266

on further examination. The nine included studies are theAlberta Infant Motor Scale (AIMS),15 Bayley Scale of Infant and
Toddler Development – Version III (BSITD-III),22 Prechtl’sAssessment of General Movements (GMs),23 Movement
Review 259
Table IV: Evidence of content, construct, and concurrent validity
Assessment tool Content Construct Concurrent
AIMS Literature review15 Multidimensional scaling, item Typically developing infants (n=103)Expert panel response theory and Guttman scaling15 0–13mo: BSID-II r=0.97
Mailout to 291 members of Scores increase with age49 0–13mo: PDMS r=0.99Canadian Physiotherapy Rasch analysis demonstrated items At-risk infants (n=68)
Association Pilot study ordered by increasing difficulty50 0–13mo: BSID-II r=0.93to test feasibility Preterm infants have lower scores 0–13mo: PDMS r=0.9515
than term infants12 Preterm infants (n=41)Discriminates between normal, suspect, 6mo: BSID-II r=0.78
and abnormal development (n=60)51 12mo: BSID-II r=0.9052
BSITD-III Literature review22 Factor analysis22 Typically developing infants (n=102)Expert panel Scores increase with age 1–42mo: BSID-II r=0.6022
Pilot, national try-out, and Children with cerebral palsy and high Typically developing infants (n=81)standardization studies risk of motor problems have lower 2–42mo: PDMS-2 Total Motor r=0.55
mean scores than controls
GMs Experts in field23 Theory supported by ultrasound studies23 Term infants with HIE (n=58)Discriminates between infants with 0–4mo: neurological exam
cerebral lesions and controls (n=22)53 %agree=78–8355
Discriminates between normal and Preterm infants (n=66)abnormal movements in term and 0–4mo: neurological exam
preterm infants (n=130)54 %agree=8056
MAI Literature review57 Discriminates between normal and Preterm and term infants (n=246)Risk scores based abnormal development in preterm 4mo: BSID r=0.6359
on at risk infants57 infants (n=35)38
Does not discriminate between normal and atypical development in healthy
term infants (n=50)58
NSMDA Literature review24 Factor analysis 60 Low-birthweight infants (n=148)Developed by experts in field Consistency of results over time24 24mo: No significant difference
Discriminates between normal and between NSDMA and paediatrician’s abnormal development (n=148)60 classification χ2=0.0860
Preterm infants with IUGR score lower than normal-birthweight preterm infants
(n=198)61
PDMS-2 Literature review25 Factor analysis25 Typically developing infants (n=30)Hierarchical sequence Sensitive to age-related change 1–11mo: PDMS-1 Gross Motor r=0.84,
Infants with disabilities score lower than Fine Motor r=0.9025
infants with no motor problems (n=65)
PFMAI Based upon literature26 Rasch analysis26 Typically developing infants (n=32)Criterion-referenced cut-off Sensitive to age-related change 2–6mo: PDMS Gross Motor r=0.83,
scores based on Discriminates between term and Fine Motor r=0.6726
term infants (n=185) preterm infants
TIMP Expert panel39 Rasch analysis39 Term and preterm infants (n=90)Literature review Sensitive to age-related change63 3mo: AIMS r=0.6464
Elicited items occurred during Infants with medical risk factors caregiver interactions62 score lower than peers
Pilot studies and revision of content Discriminates between infants with low and high risk of motor problems63
BSID, Bayley Scales of Infant Development – Version I;65 BSID-II, Bayley Scales of Infant Development – Version II;66 %agree, percentage agreement;HIE, hypoxic–ischemic encephalopathy; r, Pearson’s correlation coefficient; Sens, sensitivity; Spec, specificity; IUGR, intrauterine growthretardation; AIMS, Alberta Infant Motor Scale;15 BSITD-III, Bayley Scales of Infant and Toddler Development – Version III;37 GMs, GeneralMovements Assessment;23 MAI, Movement Assessment of Infants;38 NSDMA, Neuro Sensory Motor Development Assessment;24 PDMS-2,Peabody Developmental Motor Scale – Version 2;25 PFMAI, Posture and Fine Motor Assessment of Infants;26 TIMP, Test of Infant MotorPerformance;39 TIME, Toddler and Infant Motor Examination.28
260 Developmental Medicine & Child Neurology 2008, 50: 254–266
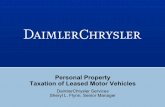
Table V: Evidence of predictive validity
Assessment Outcome assessment Sample Age at Age at initial Sensitivity Specificity Correlationtool characteristics outcome assessment (95% CI) (95% CI) (Pearson’s r)
AIMS Paediatrician classification Preterm and 18mo 4mo 77.3b 81.7b –of normal/suspicious term infants (10th centile)a
(n=142) vs abnormal (n=164) 8mo 86.4b 93.0b
development (n=22)67 (5th centile)a
BSID-II PDI52 Preterm infants 12mo 6mo – – 0.56 (BSID-II(n=41) PDI)
BSITD-III – – – – – –
GMs Cerebral palsy (n=19) Preterm infants 12–36mo 26–62wks PMA 100 (NA) 59.1 (38.5–79.6) –or mental retardationc (n=29)
(n=2)10
Cerebral palsy or Preterm and 24mo 46–60wks PCA 0.95 (89.49–1.00) 0.96 (90.96–100) –DQ<85)(n=60)54 term infants
(n=130)Cerebral palsy or Term infants 24mo 38–42wks PCA 0.94b 0.59b –DQ<85(n=18)55 (n=58) 43–47wks PCA 0.94b 0.86b –
48–56wks PCA 0.94b 0.83b –Cerebral palsy or Preterm infants 24mo 28–37wks 90.6b 57.6 b –DQ<85(n=31)56 (n=65) 38–42wks 100 (NA) 64.5b –
43–65wks 96.2–100b 74.2–98.8b –Cerebral palsy or IUGR and term 24mo Term 83.33 (62.24–1.00) 80.00 (68.9–91.09) –DQ<85(n=11)68 control (n=62) 49–51wks PCA 1.00d (NA) 1.00d (NA)
54–56wks PCA 1.00d (NA) 93.0d (84.9–1.00) –
MAI Cerebral palsy Preterm and 3–8y 4mo (≥8 total 73.5 (58.7–88.4) 62.7 (53.9–71.4) –(n=34)69 term infants risk score)a
(n=152)Cerebral palsy or Preterm and 18mo 4mo (≥10 total 83.3 (68.4–98.4) 78.2 (90.6–99.8) 0.67 (BSID
DQ <70 (n=27)32 term infants risk score)a PDI)(n=160) 8mo (≥10 total 96.0 (88.8–100) 64.5 (55.4–73.7) 0.68 (BSID
risk score)a PDI)Paediatrician Preterm and 18mo 4mo (>9 total 72.7b 93.0b –
classification normal/ term infants risk score)a
suspicious (n=142) (n=164) 8mo (>9 total 95.5b 80.3b –abnormal development risk score)a
(n=22)67
BSID PDI59 Preterm and 12–24mo 4mo – – 0.36–0.37term infants (BSID PDI)
(n=246)BSID MDI70 Term infant at 24mo 4mo (>9 total 0.63b 0.53b –
at social risk risk score)a
(n=134)
aCut-off score for normal versus atypical motor development; bvalue cannot be calculated from published data; cUK usage: learning disability;dabnormal and absent fidgety movements were combined. DQ, Developmental Quotient; PDI, Psycho Motor Index; MDI, Mental DevelopmentIndex; BOTMP, Bruniniks–Oseretsky Test of Motor Proficiency; PDMS GMQ, Peabody Developmental Motor Scales Gross Motor Quotient;PMA, post-menstrual age; CA, corrected age; –, no study identified; NA, not applicable; AIMS, Alberta Infant Motor Scale;15 BSITD-III, BayleyScales of Infant and Toddler Development – Version III;37 GMs, General Movements Assessment;23 MAI, Movement Assessment of Infants;38
NSDMA, Neuro Sensory Motor Development Assessment;24 PDMS-2, Peabody Developmental Motor Scale – Version 2;25 PFMAI, Posture andFine Motor Assessment of Infants;26 TIMP, Test of Infant Motor Performance;39 TIME, Toddler and Infant Motor Examination.28
Table IV: continued
Assessment tool Content Construct Concurrent
TIME Literature review28 Factor analysis28 Typically developing (n=731) andExpert panels Sensitive to age-related change delayed infants (n=153)
2 pilot and try-out studies Rasch analysis 4m–3.5y: physician/therapistDiscriminates between children with classification of development (%)
and without motor delays Mobility Scale Sens=94, Spec=86;Stability Scale Sens=91, Spec=90;Atypical Scale Sens=97, Spec=99

Assessment of Infants (MAI), Neuro Sensory MotorDevelopment Assessment (NSMDA),24 Peabody Develop-mental Motor Scales – Version 2 (PDMS-2),25 Posture and FineMotor Assessment of Infants (PFMAI),26 Test of Infant MotorPerformance (TIMP)27 and Toddler and Infant MotorExamination (TIME).28 The characteristics of all nine includedassessments are summarized in Table I. Two neonatal assess-ments and seven infant assessments were excluded becausethey did not primarily measure motor development or had nopublished manual. The reasons for exclusion are listed inTable II.
CHARACTERISTICS OF INCLUDED STUDIES
All the assessment tools included discriminate the motordevelopment of infants as being normal or atypical, with theAIMS, BSITD-III, PDMS-2, TIMP, and TIME comparing devel-opment with a norm-referenced group. The standardizationsamples for the norm-referenced tools consisted of infantsborn in the USA and/or Canada. The age ranges of the testswere variable; no assessment tool was able to assess apreterm infant from birth to 12 months after term. The TIMPand GMs are the only tools appropriate for use before term,
but they can only be used up to approximately 4 months afterterm. Many of the other assessment tools are appropriate foruse from 1 to 12 months of age, but their validity variesdepending on the age of the infant at assessment.
CLINICAL UTILITY
Clinical utility is summarized in Table III. The time to admin-ister assessments varied both between assessments and with-in assessments depending on the age of the infant, with mostassessments being longer as the infant grew older, with theexception of GMs. The shortest assessments were the AIMSand GMs; the BSITD-III, PDMS-2, and TIME were more com-plex and time-consuming. The AIMS and GMs assessmentsinvolve minimal handling in comparison with other assess-ments. The TIME involves interaction and handling by theprimary caregiver, which may lead to a more accurate perfor-mance of the child’s abilities. Most assessment tools can beused by a variety of health professionals; however, it isimportant for these professionals to have an understandingof preterm motor development and handling of infants, and,when appropriate, of test statistics. Some assessmentsrequire specific training, such as GMs and the BSITD-III,
Review 261
Table V: continued
Assessment Outcome assessment Sample Age at Age at initial Sensitivity Specificity Correlationtool characteristics outcome assessment (95% CI) (95% CI) (Pearson’s r)
NSMDA Paediatrician Low-birthweight 24mo 1mo (25% below 68.8b 72.6b –classification of infants (n=148) average)a
development60 4mo (25% below 80.0b 56.9b –average)a
8mo (25% below 82.4b 83.7b – average)a
12mo (25% below 58.8b 93.3b –average)a
PDMS-2 Paediatrician Preterm and 18mo 4mo (6th 36.1b 93.8b –classification of term infants centile)a
normal/suspicious (n=164) 8mo (6th 91.7b 52.3b
(n=142) vs abnormal centile)a
development (n=22)67
PFMAI – – – – – –
TIMP AIMS scores below Preterm and 6mo 32wk PMA– 62.5 (43.1–81.9) 77.4 (67.0–87.8) 0.37–0.675th centile (n=19 at 6mo, term infants 4mo CA (z score
14 at 9mo, and 12 at 12mo)71 (n=96)71 –0.5SD)a (AIMS centile)9mo 91.7 (76.0–100) 75.7 (65.7–85.8) 0.20–0.56
(AIMS centile)12mo 45–92 (b) 68–78 (b) 0.32–0.55
(AIMScentile)
Motor delay on BOTMP Preterm and 5.75y 32wks PMA– 50.0 (15.6–85.7) 100 (b) 0.36 (BOTMP(n=8)72 term infants 4mo CA (z score score)
(n=35)72 –1.6SD)a
Gross motor delay Preterm and 4–5y 1mo (z score 33 (19–47) 94 (87–100) 0.43 (PDMS(PDMS DQ>70) term infants –0.5SD)a GMQ)
(n=12)73 (n=61) 2mo (z score 50 (35–65) 86 (76–96) 0.42 (PDMS–0.5SD)a GMQ)
3mo (z score 72 (59–83) 91 (83–99) 0.65 (PDMS–0.5SD)a GMQ)
TIME – – – – – – –

which require both time and expense.
VALIDITY
The primary purpose of the assessment tool needs to be con-sidered when examining validity. Evidence of content, con-struct and concurrent validity is summarized in Table IV. Allassessment tools had adequate content validity and con-struct validity. However, the the BSITD-III reports thatinfants born at less than 37 weeks’ gestational age do notscore significantly lower than term infants on the grossmotor scale, which may limit its use in detecting minimalmotor problems with preterm infants. The concurrent validi-ty of the AIMS, BSITD-III, GMs, MAI, NSMDA, PDMS-2,PFMAI, TIMP, and TIME has been reported in relation to
another motor assessment or paediatrician classification ofnormal or atypical development. The predictive validity ofthe assessment tools is summarized in Table V. The predictivevalidity is dependent on the age of assessment: GMs have thegreatest combination of sensitivity and specificity in the firstmonths of life, and the AIMS and NSDMA in the later months.
RESPONSIVENESS
All tools report that they are appropriate for assessing changeover time or in response to intervention. However, there havebeen few validation studies. TIMP has been used in two ran-domized controlled trials of intervention and has demonstrat-ed a significant difference between groups.29,30 The AIMS andGMs have also been used as outcome assessments in trials of
262 Developmental Medicine & Child Neurology 2008, 50: 254–266
Table VI: Reliability of assessment tools
Assessment Test–retest Intrarater Interrater Internal consistency (Cronbach’s α)tool
AIMS 0–18mo (n=210) 0–18mo (n=195) 0–18mo (n=253) 0–18mo (n=unclear)ICC=0.9915 ICC=0.9915 ICC=0.99715 r2 = 0.9949
3–18mo (n=45) 3–18mo (n=41)ICC=0.98–0.9952 ICC=0.97–0.9952
0–12mo (n=14)ICC=0.98–9974
BSITD-III 2–4m (n=50) FM – – 1–12mo norm. pop. (n=1700) FMr=0.67, GM r=0.77 r=0.77–0.89, GM r=0.86–949–13m (n=50) FM 1–12mo atypical (n=688) FM
r=0.86, GM r=0.8622 r=0.90–0.92, GM r=0.93–0.96
GMs NA 3–26wks (n=20) Term (n=30) κ=0.8475 NAκ=1.0023 0–20wks (n=19) κ=0.9276
0–20wks (n=27) κ=0.8477
0–20wks (n=16) κ=0.9178
MAI 4mo (n=53) r=0.7679 – 4mo (n=53) r=0.7279 –
NSMDA – – 1–24mo (n=NR) r=0.8024 –
PDMS-2 2–11mo (n=20) FMQ – 3–36mo (n=60) FMQ 0–11mo FMQ =0.96, GMQ = 0.97,r=0.73, GMQ r=0.84, r=0.98, GMQ=0.97, TMQ= 0.9825
TMQ r=0.8925 TMQ=0.9625
4–5y (n=6) TMC ICC=0.91673
PFMAI – – 2–6mo (n=13) posture 0–6mo (n=59) posture scale=0.97,=0.97, FM=0.99 FM α=0.9926
6–12mo (n=18) posture 6–12mo (n=126) posture=0.95,=0.98, FM=0.9626 FM α=0.9626
TIMP 34wk PCA–4mo (n=108) Age not specified Age not specified –r=0.8980 (n=21) ICC=0.98–9930 (n=21) ICC=0.9530
TIME 4–41mo (n=33) 4–41mo (n=33) 2–42mo (n=31) 0–6mo (n=NR) α=0.79–9328
r=0.96–0.9928 r=0.96–0.9928 r=0.89–9928 7–12mo (n=NR) α=0.88–9728
8–35mo (n=10)r=0.98–1.0081
PMA, post-menstrual age; NA, not applicable; ICC, intraclass correlation coefficient; FM, fine motor; GM, gross motor; TM, total motor; Q,quotient; – , no study identified; NR, not reported; AIMS, Alberta Infant Motor Scale;15 BSITD-III, Bayley Scales of Infant and ToddlerDevelopment – Version III;37 GMs, General Movements Assessment;23 MAI, Movement Assessment of Infants;38 NSDMA, Neuro Sensory MotorDevelopment Assessment;24 PDMS-2, Peabody Developmental Motor Scale – Version 2;25 PFMAI, Posture and Fine Motor Assessment ofInfants;26 TIMP, Test of Infant Motor Performance;39 TIME, Toddler and Infant Motor Examination.28

intervention; however, no difference was reported betweengroups.23,31 It is unclear from these studies whether the inter-vention was not effective or whether the tool was not sensitiveenough to detect change.
RELIABILITY
Studies of the reliability of the assessment tools are summa-rized in Table VI. Studies of the BSITD-III, MAI, NSMDA,PDMS-2, and TIME reported correlations only (Pearson’s r),which does not take into account systematic differencesbetween assessors. The test–retest reliability of the AIMS isreported to be excellent with the use of appropriate statisti-cal methods. Intrarater reliability for the AIMS, GMs, andTIMP is excellent, as is the interrater reliability of the AIMS,GMs, MAI, and TIMP. Internal consistency has been studiedwith the AIMS, BSITD-III, PDMS-2, and PFMAI. Rasch analysishas been used to examine consistency of items for the TIMP.
DiscussionThe nine assessment tools identified in this systematicreview are all appropriate for measuring motor developmentof preterm infants, although each tool has its advantages anddisadvantages. The most important step in identifying thebest tool is for the clinician or researcher to identify the pur-pose of the assessment and then choose a test that has beenvalidated as a discriminative, predictive, or evaluative tool.Many assessments report that they are appropriate to use formore than one purpose; however, they do not have the valid-ity studies to support their claims.
The clinical utility of assessment tools should be taken intoaccount with the validity and reliability of the tool. Some toolssuch as GMs and the BSITD-III require standardized trainingand may be costly, although this may improve the reliabilityand validity of the assessments. This may be particularlyimportant in research when one intervention is being com-pared with another. GMs have the best predictive validity forCP and are considered to be a quick, inexpensive, and non-intrusive assessment; however, the cost of initial trainingneeds to be considered because the trainer may have to traveloverseas to attend a course. Some clinicians may require aneasily accessible tool that requires little training. The AIMS hasthe advantage of being easily administered in the clinical set-ting, which may make the instrument more feasible for thera-pists to use in follow-up clinics because of the minimalhandling and time needed to conduct the assessment, whilehaving strong correlation with the BSID-II and PDMS.
Norm-referenced tools are useful for comparing aninfant’s motor development with that of a large sample.Traditionally, these tools have examined the ability of aninfant to achieve a task and compare the child’s achievementwith a large sample representative of a population. All theassessments in this review take into account the way in whichthe infant performs the task to varying degrees, and the tasksare both qualitative and quantitative in nature. However,some tools, such as the BSITD-III, are more quantitative andmay not be sensitive enough to detect the subtle changes inquality of movement that are seen with preterm infants.These subtle changes in movement quality may lead toenhanced balance and coordination at later ages.
Preterm infants have been shown to have different patternsof motor development from those of term infants, but thelong-term implications of altered patterns of development are
not fully understood. This is demonstrated in the study by vanHaastert and colleagues, in which preterm infants (gestationalage <32wks) had significantly lower scores at all ages on theAIMS.12 Although these preterm infants do not have typicalmotor development, they have variation in motor develop-ment that may not necessarily be abnormal.8 For this reason,criterion-referenced tools designed specifically for preterminfants to discriminate between typical and atypical develop-ment or tools that have normative data for infants at risk ofdevelopmental problems may be more appropriate, depend-ing on the purpose of assessment. GMs, the NSDMA, MAI, andPFMAI are all criterion-referenced tests which seek to discrimi-nate between normal and abnormal motor development. TheNSMDA has the advantage of discriminating between normalmotor function and minimal, mild, moderate, and severemotor dysfunction. The PDMS-2, TIMP, and TIME have a largerthan normal proportion of infants at risk of developmentalproblems in their normative samples.
Although discriminative assessments are designed to clas-sify current motor performance, knowledge of their predic-tive value and stability over time is useful in determiningwhich infants require early intervention and informing care-givers of assessment results. Both the AIMS and MAI haveshown that up to 30% of healthy term infants perform out-side the cut-off for normal development at one point in time,despite having a normal outcome. Longitudinal assessmentsare recommended to improve the validity of assessments,because no assessment correctly identifies all children ashaving normal or atypical motor development with a singleassessment. Multiple assessments are also recommendedbecause infants with transient neuromotor abnormalitiesduring the first year are at greater risk of developmentalcoordination disorders at school age.32
Variation in development over the first year of life is inher-ent in normal development, but it can make prediction diffi-cult.33 Many assessment tools have improved predictivevalue as the child gets older, because children may be freefrom neurological signs of dysfunction at an early age butwhen the complexity of neurological function increases withage, deficits may become apparent.34 However, it may not beappropriate to wait, because intervention is thought to bemost beneficial when begun as early as possible.6 The plastic-ity of the infant’s brain, particularly in the first years of life,can lead to changes in brain function and may explain whywe can never predict outcome with 100% accuracy. The pre-diction of later problems early in life tends to be most effec-tive for severe disabilities such as CP. More subtledevelopmental problems can be difficult to predict early inlife because environmental, social, and biological interac-tions may have more of an influence on long-term outcomethan for infants with more severe disabilities.35 For example,a preterm infant who has been in hospital for many monthsmay have delayed motor development as a result of lack ofexperience to move in the hospital environment rather thanas a result of a neurological deficit.
The concurrent and predictive validities for some assess-ments were not measured with a ‘criterion standard tool’.Many studies used physicians’ judgments of developmentaldelay to establish validity, despite the greater accuracy ofstandardized assessment tools.36 However, it is not clearwhich motor assessment tool should be considered the ‘cri-terion standard’.
Review 263

It is important for outcome measurements to be sensitiveto measure change; however, there is no consensus on howthis should be assessed.21 Individual changes in the rate ofmotor development cannot necessarily indicate the success ofintervention because change may be due to the natural historyand variability of the rate of development of motor skills, and,therefore, large randomized controlled trials are needed inthe research of interventions.7 One of the most important con-siderations when assessing the effects of interventions iswhether the sample is large enough to allow a clinically impor-tant effect size to be detected. From a clinical viewpoint, indi-viduals and organizations will need to decide what theyconsider to be acceptable levels of change when assessing aninfant’s response to an intervention, and they should beencouraged to use multiple longitudinal assessments.
Research on infant assessment tools has focused on discrim-inative and predictive validity, with limited evidence on theability of the measurement tool to evaluate change. Futureresearch should focus on validating assessment tools that doc-ument change so that the efficacy of intervention programmesin the first year of life can be evaluated. Many studies havelooked only at the prediction of CP or of abnormal motordevelopment up to 2 years of age, with very few studies lookingat the long-term correlation with standardized motor assess-ments. Although long-term follow-up studies can be timely andcostly, further studies are needed for preterm infants that cor-relate early motor assessments with later motor outcome atschool age to improve our knowledge of what is a significantvariation in motor development for a preterm infant.
ConclusionPreterm infants develop differently from infants born atterm. However, this does not mean that all preterm infantswill have motor problems but rather that assessments appro-priate for preterm infants are needed. There is no assess-ment tool that can take into account all the multiple variablesthat influence motor development, such as social, environ-ment, and health factors. Norm-referenced tools can be use-ful to compare the infant’s development with other infants ofthe same age. The AIMS demonstrated the best psychometricproperties and clinical utility of these tools.
However, because preterm infants have different grossmotor developmental trajectories on the AIMS from those ofterm infants in the first 18 months of life, it is useful to also havea criterion tool designed specifically for predicting abnormalmotor development, such as the NSMDA or TIMP.12 GMs havethe best combination of sensitivity and specificity for predict-ing CP in the early months, whereas the AIMS and NSMDA arethe best predictors of atypical motor development in the latermonths. The TIMP is the only tool to demonstrate adequateevaluative validity, and along with the AIMS has demonstratedthe best reliability. The TIMP and GMs are the only tools appro-priate for use before term.
In clinical practice, we would recommend using morethan one assessment tool to meet the needs of an assess-ment. For example, in the period before term and in earlyinfancy the use of both GMs and the TIMP, and for the periodfrom 4 to 12 months’ corrected age the use of the AIMS andNSDMA, will ensure that one has appropriate predicative,discriminative, and evaluative assessments. Longitudinalmotor assessments are recommended, to improve the pre-dictive and discriminative validity.
Accepted for publication 30th August 2007.
AcknowledgementsWe acknowledge support from the National Health Medical Council(Australia) Public Health Postgraduate Scholarship for AS, an NHMRCPost Doctoral Hospital Training Fellowship for RB, and an NHMRCProject grant (ID 284512).
References1. Bracewell M, Marlow N. Patterns of motor disability in very preterm
children. Ment Retard Dev Disabil Res Rev 2002; 8: 241–48.2. Wang CJ, McGlynn EA, Brook RH, et al. Quality-of-care indicators
for the neurodevelopmental follow-up of very low birth weightchildren: results of an expert panel process. Pediatrics 2006;117: 2080–92.
3. Kirshner B, Guyatt G. A methodological framework for assessinghealth indices. J Chronic Dis 1985; 38: 27–36.
4. Vaccarino FM, Ment LR. Injury and repair in the developing brain.Arch Dis Child Fetal Neonatal Ed 2004; 89: F190–92.
5. Hadders-Algra M. The neuromotor examination of the preschoolchild and its prognostic significance. Ment Retard Dev DisabilRes Rev 2005; 11: 180–88.
6. Johnson S, Marlow N. Developmental screen or developmentaltesting? Early Hum Dev 2006; 82: 173–83.
7. Darrah J, Redfern L, Maguire T, Beaulne AP, Watt J. Intra-individualstability of rate of gross motor development in full-term infants.Early Hum Dev 1998; 52: 169–79.
8. Rosenbaum P. Variation and ‘abnormality’: recognizing thedifferences. J Pediatr 2006; 149: 593–94.
9. Barbosa VM, Campbell SK, Sheftel D, Singh J, Beligere N.Longitudinal performance of infants with cerebral palsy on theTest of Infant Motor Performance and on the Alberta Infant MotorScale. Phys Occup Ther Pediatr 2003; 23: 7–29.
10. Ferrari F, Cioni G, Prechtl HF. Qualitative changes of generalmovements in preterm infants with brain lesions. Early HumDev 1990; 23: 193–231.
11. Levine ME, Carey WB, Crocker AC, Gross RT.Developmental–Behavioral Pediatrics. 3rd edn. Philadelphia:W B Saunders, 1999.
12. van Haastert IC, de Vries LS, Helders PJ, Jongmans MJ. Earlygross motor development of preterm infants according to theAlberta Infant Motor Scale. J Pediatr 2006; 149: 617–22.
13. Long TM, Tieman B. Review of two recently publishedmeasurement tools: the AIMS and the T.I.M.E. Pediat Phys Ther1998; 10: 62–66.
14. Case-Smith J. Analysis of current motor development theory andrecently published infant motor assessments. Inf YoungChildren 1996 9: 29–41.
15. Piper MC, Darrah J. Motor Assessment of the Developing Infant.Philadelphia: W B Saunders, 1994.
16. Majnemer A, Mazer B. Neurologic evaluation of the newborninfant: definition and psychometric properties. Dev Med ChildNeurol 1998; 40: 708–715.
17. Tieman BL, Palisano RJ, Sutlive AC. () Assessment of motordevelopment and function in preschool children. Ment RetardDev Disabil Res Rev 2005; 11: 189–96.
18. Law M. Outcome Measures Rating Form.www.canchild.ca/Portals/0/outcomes/pdf/measrate.pdf(accessed 19th October 2007).
19. Guyatt G, Walter S, Norman G. Measuring change over time:assessing the usefulness of evaluative instruments. J Chronic Dis1987; 40: 171–78.
20. Waters E, Maher E. Assessing quality of life. In: Elliott E, Moyer V,editors. Evidence-Based Pediatrics and Child Health. 2nd edn.London: BMJ Books, 2004: 99–110.
21. McDowell I, Newell C. Measuring Health: A Guide to RatingScales and Questionnaires. 2nd edn. New York: OUP; 1996.
22. Bayley N. Bayley Scales of Infant and Toddler Development. 3rdedn. San Antonio: Harcourt Assessment, 2005.
23. Einspieler C, Prechtl HF, Bos AF, Ferrari F, Cioni G. Prechtl’sMethod on the Qualitative Assessment of General Movementsin Preterm, Term and Young Infants. Clinics in DevelopmentalMedicine No. 167. London: Mac Keith Press, 2004.
24. Burns YR, Ensbey RM, Norrie MA. The Neuro-Sensory MotorDevelopment Assessment part 1: development andadministration of the test. Aust J Physiother 1989; 35: 141–57.
264 Developmental Medicine & Child Neurology 2008, 50: 254–266

25. Folio MR, Fewell RR. Peabody Developmental Scales. 2nd edn.Austin: Pro-ed, 2000.
26. Case-Smith J, Bigsby R. Posture and Fine Motor Assessment ofInfants. San Antonio, TX: Therapy Skill Builders, 2000.
27. Campbell SK. The Test of Infant Motor Performance: Test User’sManual Version 1.4. Chicago: Infant Motor Performance Scales,LLC, 2001.
28. Miller LJ, Roid GH. The TIME Toddler and Infant MotorEvaluation: A Standardized Assessment. Tucson, AZ: TherapySkill Builders, 1994.
29. Girolami GL, Campbell SK. Efficacy of a neuro-developmentaltreatment program to improve motor control in infants bornprematurely. Pediat Phys Ther 1994; 6: 175–84.
30. Lekskulchai R, Cole J. Effect of a developmental program onmotor performance in infants born preterm. Aust J Physiother2001; 47: 169–76.
31. Cameron EC, Maehle V, Reid J. The effects of an early physicaltherapy intervention for very preterm, very low birth weightinfants: a randomized controlled clinical trial. Pediat Phys Ther2005; 17: 107–19.
32. Swanson MW, Bennett FC, Shy KK, Whitfield MF. Identificationof neurodevelopmental abnormality at four and eight months bythe movement assessment of infants. Dev Med Child Neurol1992; 34: 321–37.
33. Touwen BC. How normal is variable, or how variable is normal?Early Hum Dev 1993; 34: 1–12.
34. Hadders-Algra M. Evaluation of motor function in young infantsby means of assessment of general movements: a review. PediatPhys Ther 2001; 13: 27–36.
35. Salt A, Redshaw M. Neurodevelopmental follow-up afterpreterm birth: follow up after two years. Early Hum Dev 2006;82: 185–97.
36. De Kleine MJK, Nijhuis-Van Der Sanden MWG, Den Ouden AL. Ispaediatric assessment of motor development of very pretermand low-birthweight children appropriate? Acta Paediatr 2006;95: 1202–08.
37. Bayley N. Bayley Scales of Infant and Toddler Development. 3rdedn. San Antonio: Harcourt Assessment, 2005.
38. Chandler LS, Andrews MS, Swanson MW, Larson AH. MovementAssessment of Infants: A Manual. Washington: Rolling Bay;1980.
39. Campbell SK. The Test of Infant Motor Performance. Test User’sManual Version 2.0. Chicago: Infant Motor Performance Scales,LLC, 2005.
40. Dubowitz L, Dubowitz V, Mercuri E. The NeurologicalAssessment of the Preterm & Full-term Newborn Infant. Clinicsin Developmental Medicine No. 148. 2nd edn. London: MacKeith Press, 1999.
41. Lester BM, Tronick EZ. History and description of the NeonatalIntensive Care Unit Network Neurobehavioral Scale. Pediatrics2004; 113: 634–40.
42. Knobloch H, Stevens F, Malone AF. Manual of DevelopmentalDiagnosis: the Adminstration and Interpretation of the RevisedGesell and Amartuda Developmental and NeurologicExamination. Houston, TX: Gesell Developmental Materials,1987.
43. Griffiths R. The Abilities of Young Children: A ComprehensiveSystem of Mental Measurement for the First Eight Years.London: Child Development Research Center, 1970.
44. Frankenburg WK, Dodds J, Archer P. Denver II. Denver: DenverDevelopmental Materials, 1990.
45. Berg M, Jahnsen R, Froslie KF, Hussain A. Reliability of the PEDI.Phys Occup Ther Pediatr 2005; 24: 61–77.
46. Newborg J, Stock JR, Wnek L. Battelle DevelopmentalInventory. Allen, TX: DLM Teaching Resources, 1984.
47. DeGangi G. Critique of the Infanib: the Infant NeurologicalInternational Battery. Phys Occup Ther Pediatr 1995;14: 109–20.
48. Persson K, Stromberg B. Structured observation of motorperformance (SOMP-I) applied to preterm and full term infantswho needed neonatal intensive care. A cross-sectional analysisof progress and quality of motor performance at ages 0–10months. Early Hum Dev 1995; 43: 205–24.
49. Piper MC, Pinnell LE, Darrah J, Maguire T, Byrne PJ.Construction and validation of the Alberta Infant Motor Scale(AIMS). Can J Publ Health 1992; 83: S46–50.
50. Liao PM, Campbell SK. Examination of the item structure of theAlberta Infant Motor Scale. Pediat Phys Ther 2004 16: 31–8.
51. Bartlett DJ, Fanning JEK. Use of the Alberta Infant Motor Scale tocharacterize the motor development of infants born preterm ateight months corrected age. Phys Occup Ther Pediatr 2003;23: 31–45.
52. Jeng S, Yau KT, Chen L, Hsiao S. Alberta Infant Motor Scale:reliability and validity when used on preterm infants in Taiwan.Phys Ther 2000; 80: 168–78.
53. Guzzetta A, Mercuri E, Rapisardi G, et al. General movementsdetect early signs of hemiplegia in term infants with neonatalcerebral infarction. Neuropediatrics 2003; 34: 61–6.
54. Prechtl HF, Einspieler C, Cioni G, Bos AF, Ferrari F, SontheimerD. An early marker for neurological deficits after perinatal brainlesions. Lancet 1997; 349: 1361–63.
55. Cioni G, Prechtl HF, Ferrari F, Paolicelli PB, Einspieler C, RoversiMF. Which better predicts later outcome in full-term infants:quality of general movements or neurological examination?Early Hum Dev 1997; 50: 71–85.
56. Cioni G, Ferrari F, Einspieler C, Paolicelli PB, Barbani MT, PrechtlHF. Comparison between observation of spontaneousmovements and neurologic examination in preterm infants. J Pediatr 1997; 130: 704–11.
57. Chandler L. Screening for movement dysfunction in infancy.Phys Occup Ther Pediatr 1986; 6: 171–90.
58. Swanson MW. Neuromotor assessment of low-birth weightinfants with normal developmental outcome. Dev Med ChildNeurol 1989; 31: 27–28.
59. Harris SR, Swanson MW, Andrews MS, et al. Predictive validity ofthe ‘Movement Assessment of Infants’. J Dev Behav Pediatr1984; 5: 336–342.
60. Burns YR, Ensbey RM, Norrie MA. The Neuro Sensory MotorDevelopmental Assessment Part II: Predictive and concurrentvalidity. Aust J Physiother 1989; 35: 151–57.
61. Connors JM, O’Callaghan MJ, Burns YR, Gray PH, Tudehope DI,Mohay H, Rogers YM. The influence of growth on developmentoutcome in extremely low birthweight infants at 2 years of age.J Paediatr Child Health 1999; 35: 37–41.
62. Murney ME, Campbell SK. The ecological relevance of the Test ofInfant Motor Performance elicited scale items. Phys Ther 1998;78: 479–89.
63. Campbell SK, Kolobe TH, Osten ET, Lenke M, Girolami GL.Construct validity of the test of infant motor performance. PhysTher 1995; 75: 585–96.
64. Campbell SK, Kolobe THA. Concurrent validity of the Test ofInfant Motor Performance with the Alberta Infant Motor Scale.Pediat Phys Ther 2000; 12: 2–9.
65. Bayley N. Bayley Scales of Infant Development. New York: ThePsychological Corporation, 1969.
66. Bayley N. The Bayley Scales of Infant Development. 2nd edn.New York: The Psychological Corporation, 1993.
67. Darrah J, Piper MC, Watt J. Assessment of gross motor skills of at-risk infants: predictive validity of the Alberta Infant Motor Scale.Dev Med Child Neurol 1998; 40: 495–91.
68. Zuk L, Harel S, Leitner Y, Fattal-Valevski A. Neonatal generalmovements: an early predictor for neurodevelopmentaloutcome in infants with intrauterine growth retardation. J ChildNeurol 2004; 19: 14–18.
69. Harris SR. Early detection of cerebral palsy: sensitivity andspecificity of two motor assessment tools. J Perinatol 19877: 11–15.
70. Rose-Jacobs R, Cabral H, Beeghly M, Brown ER, Frank DA. TheMovement Assessment of Infants (MAI) as a predictor of two-year neurodevelopmental outcome for infants born at term whoare at social risk. Pediat Phys Ther 2004; 16: 212–21.
71. Campbell SK, Kolobe TH, Wright BD, Linacre JM. Validity of theTest of Infant Motor Performance for prediction of 6-, 9- and 12-month scores on the Alberta Infant Motor Scale. Dev Med ChildNeurol 2002; 44: 263–72.
72. Flegel J, Kolobe TH. Predictive validity of the test of infant motorperformance as measured by the Bruininks–Oseretsky test ofmotor proficiency at school age. Phys Ther 2002; 82: 762–71.
73. Kolobe TH, Bulanda M, Susman L. Predicting motor outcome atpreschool age for infants tested at 7, 30, 60, and 90 days afterterm age using the Test of Infant Motor Performance. Phys Ther2004; 82: 1144–56.
Review 265

266 Developmental Medicine & Child Neurology 2008, 50: 254–266
74. Blanchard Y, Neilan E, Busanich J, Garavuso L, Klimas D.Interrater reliability of early intervention providers scoring theAlberta Infant Motor Scale. Pediat Phys Ther 2004; 16: 13–18.
75. van Kranen-Mastenbroek V, van Oostenbrugge R, Palmans L, etal. Inter- and intra-observer agreement in the assessment of thequality of spontaneous movements in the newborn. Brain Dev1992; 14: 289–93.
76. Bos AF, van Loon AJ, Hadders-Algra M, Martijn A, Okken A,Prechtl HF. Spontaneous motility in preterm, small-for-gestational age infants. II. Qualitative aspects. Early Hum Dev1997; 50: 131–47.
77. Bos AF, Martijn A, Okken A, Prechtl HF. Quality of generalmovements in preterm infants with transient periventricularechodensities. Acta Paediatr 1998; 87: 328–35.
78. Cioni G, Bos AF, Einspieler C, et al. Early neurological signs inpreterm infants with unilateral intraparenchymal echodensity.Neuropediatrics 2000; 31: 240–51.
79. Harris SR, Haley SM, Tada WL, Swanson MW. Reliability ofobservational measures of the Movement Assessment of Infants.Phys Ther 1984; 64: 471–77.
80. Campbell SK. Test–retest reliability of the Test of Infant MotorPerformance. Pediat Phys Ther 1999; 11: 60–66.
81. Rahlin M, Rheault W, Cech D. Evaluation of the primary subtestsof toddler and infant motor evaluation: implications for clinicalpractice in pediatric physical therapy. Pediat Phys Ther 2003;15: 176–83.
List of abbreviations
AIMS Alberta Infant Motor ScaleBSITD-III Bayley Scale of Infant and Toddler Development –
Version IIIGMs Prechtl’s Assessment of General MovementsMAI Movement Assessment of InfantsNSMDA Neuro Sensory Motor Development AssessmentPDMS-2 Peabody Developmental Motor Scales – Version 2PFMAI Posture and Fine Motor Assessment of InfantsTIME Toddler and Infant Motor ExaminationTIMP Test of Infant Motor Performance
Pediatric Developmental Specialist in NeuroMotor Rehabilitation
Glenrose Rehabilitation and Stollery Children’s Hospitals Department of Pediatrics, University of Alberta
Edmonton, Alberta, Canada The Section of Pediatric Neurosciences at the University of Alberta invites applications for the academic position in Pediatric Neuromotor Rehabilitation. The successful applicant would join a well-established Developmental Pediatrics Program with comprehensive inpatient and outpatient services for children with complex disabilities. The Department of Pediatrics at the Stollery Children’s and Glenrose Rehabilitation Hospitals, service a complete range of pediatric subspecialties and is the tertiary and quaternary children’s hospital for Northern Alberta, with a population base of over 1.5 million people. Pediatric Neurosciences offers a full range of sub-specialties, and is a particular focus for growth within the Department. Pediatric Physiatrists and Developmental Pediatricians within the division of Neurodevelopmental Pediatrics have strong affiliations, and active clinical and research collaborations with the Department of Physical Medicine and Rehabilitation, Pediatric Neurology, Pediatric Surgery, and the Faculty of Rehabilitation. Substantial infrastructure is currently available to the successful candidate through already established programs within the hospitals and outreaching to the community and schools. Research support is also available through a number of government, foundation and institutional resources, unique to the province of Alberta. These include the Glenrose and Stollery Hospital Foundations, the Alberta Heritage Foundation for Medical Research, the Women and Children’s Health Research Institute, the Integrated Centre for Care Advancement through Research, the Alberta Centre for Child, Family and Community Research. Full-time funded positions are available through the Department of Pediatrics and Child Health, within our current, very competitive, alternate funding program (AFP). Successful candidates will have a clear interest in an academic career with experience in the area of childhood neuromotor and developmental disabilities. Academic responsibilities include resident and medical student education, contributing to the development of the Division of Neurodevelopmental Pediatrics and participating in research activities. Candidates with either a clinical research or basic research background are encouraged to apply. This position is open to Pediatric Physiatrists, Developmental Pediatricians or specialists in rehabilitation medicine with expertise in the care of children. Alberta is the fastest growing province in Canada, with the most rapidly expanding birth rate in the country. It is the only province that is debt free and financially secure. The Department of Pediatrics, the Glenrose Rehabilitation Hospital and the Stollery Children’s Hospital have been rapidly expanding in the last 5 years and continue to recruit to programs of excellence in a host of areas, with the Pediatric Neurosciences a priority. The city of Edmonton has an excellent school system, beautiful river valley and friendly people. Close to mountains and lakes, the city offers numerous outdoor activities and a vibrant arts and cultural scene. Interested applicants should forward their curriculum vitae, along with a cover letter and the names and contact information of 3 references to: Jerome Y. Yager MD
Professor and Head Section of Pediatric Neurosciences Department of Pediatrics University of Alberta Room 7317A Aberhart Centre One 11402 University Avenue NW Edmonton, Alberta, Canada, T6G 2J3 Email: [email protected]
Fax: (780) 407-8283