
Clinician’s Comments Dentures - ProSites, Inc.c1-preview.prosites.com/86920/wy/docs/Dental...
5
H ow valuable are com- fortable, attractive, functioning dentures? That question was posed last month in Part 1 of this article, and the answer was—invaluable. Last month, this patient’s pre-operative con- dition was outlined along with the treat- ment planning, evaluation, and tooth selection phases. The patient’s existing dentures—a 35-year-old maxillary denture and a 12-year-old mandibu- lar denture—are shown in Figs. 11a and 12a on page 104. Here, the case presentation resumes with the third appointment, which takes place af- ter base plates and wax rims are fabricated in the lab from the final im- pressions. The base plates and wax rims are used extensively for the clin- ical records. 100 October 2006 Dental Products Report Successful removables Clinician’s Comments DR. LORIN BERLAND A Fellow of the American Academy of Cosmetic Dentistry, Dr. Berland maintains a premier cosmetic and family practice in Dallas. Widely published in professional and general publications, he lectures international- ly. He created the first “dental spa” in 1996, developed the Lorin Library Smile Style Guide, produced a DVD CE course on a two-appointment full-mouth rehab, and is the founder of the www.denturewearers.co m Web site. (1) Floss helps locate the midline. (2) A caliper deter- mines vertical dimension at rest. (3) Old dentures result in overclosure and decreased vertical dimension. (4) The more natural vertical dimen- sion is determined by facial landmarks. 1 2 3 4 By Dr. Lorin F. Berland THIRD VISIT Dentures as full-mouth reconstruction PART 2: THE FINAL THREE VISITS Third visit: Clinical records The upper wax rim is inserted, and the resting up- per lip line and lip support are evaluated. The pos- terior occlusion of the maxillary rim should be close to parallel to the Camper’s line —the line connecting the tragus of the ear to the ala of the nose. The anterior horizontal occlusal plane is eval- uated and should be parallel to the line drawn be- tween the eyes. The ideal gum line is at the up- per lip line. This is scribed in the wax rim while the patient gives the biggest, broadest, and high- est smile. The midline can usually be determined by fol- lowing the natural location of the maxillary labi- al frenum. However, this frenum may not be at the facial midline. Although the incisive papilla and maxillary labial frenum are good intraoral in- dicators, I mark the midline by hanging dental floss down the midline of the patient’s face, between the eyes and the nose. I find it more helpful to vi- sualize once the two central incisors are set in wax (Fig. 1). It is best to make any modifications at chair- side. This is also a good time to check the align- ment as well as the width, length, shape, and col- or of the selected six maxillary anterior teeth. Correcting vertical dimension There are certain recurring relationships between fixed facial landmarks and the proportions of the lower half of the face. A caliper is used to deter- mine the vertical dimension at rest, from the fixed points of the external auditory meatus of the ear to the outer orbital rim of the eye (Fig. 2). The closed vertical dimension in maximum intercus- pation is then calculated by subtracting 3 mm for the freeway space. 1 While the patient has his old Before A great set of dentures can improve patient appearance and lifestyle. Here are some tips for ensuring the highest esthetics, function, and comfort. Continued on page 102 After
Transcript of Clinician’s Comments Dentures - ProSites, Inc.c1-preview.prosites.com/86920/wy/docs/Dental...

How valuable are com-fortable, attractive,functioning dentures?That question wasposed last month inPart 1 of this article,
and the answer was—invaluable. Lastmonth, this patient’s pre-operative con-dition was outlined along with the treat-ment planning, evaluation, and toothselection phases. The patient’s existingdentures—a 35-year-old maxillary denture and a 12-year-old mandibu-lar denture—are shown in Figs. 11a and 12a on page 104. Here, the casepresentation resumes with the third appointment, which takes place af-ter base plates and wax rims are fabricated in the lab from the final im-pressions. The base plates and wax rims are used extensively for the clin-ical records.
100 October 2006 Dental Products Report
Layout OK 1st edit sg 2nd edit rp 3rd edit Final edit Ad Production
Successful removablesClinician’s Comments
DR. LORIN BERLAND
A Fellow of the AmericanAcademy of CosmeticDentistry, Dr. Berlandmaintains a premier cosmetic and familypractice in Dallas.Widely published in professional and general publications, he lectures international-ly. He created the first “dental spa” in 1996, developed the Lorin Library Smile StyleGuide, produced a DVDCE course on a two-appointment full-mouth rehab, and isthe founder of thewww.denturewearers.com Web site.
(1) Floss helps locate themidline. (2) A caliper deter-mines vertical dimension at
rest. (3) Old dentures result inoverclosure and decreasedvertical dimension. (4) The
more natural vertical dimen-sion is determined by facial
landmarks.
1 2
3 4
By Dr. Lorin F. Berland
THIRD VISIT
Denturesas full-mouth reconstruction
PART 2: THE FINAL THREE VISITS
Third visit: Clinical recordsThe upper wax rim is inserted, and the resting up-per lip line and lip support are evaluated. The pos-terior occlusion of the maxillary rim should beclose to parallel to the Camper’s line—the lineconnecting the tragus of the ear to the ala of thenose. The anterior horizontal occlusal plane is eval-uated and should be parallel to the line drawn be-tween the eyes. The ideal gum line is at the up-per lip line. This is scribed in the wax rim whilethe patient gives the biggest, broadest, and high-est smile.
The midline can usually be determined by fol-lowing the natural location of the maxillary labi-al frenum. However, this frenum may not be atthe facial midline. Although the incisive papillaand maxillary labial frenum are good intraoral in-dicators, I mark the midline by hanging dental flossdown the midline of the patient’s face, betweenthe eyes and the nose. I find it more helpful to vi-sualize once the two central incisors are set in wax(Fig. 1).
It is best to make any modifications at chair-side. This is also a good time to check the align-ment as well as the width, length, shape, and col-or of the selected six maxillary anterior teeth.
Correcting vertical dimensionThere are certain recurring relationships betweenfixed facial landmarks and the proportions of thelower half of the face. A caliper is used to deter-mine the vertical dimension at rest, from the fixedpoints of the external auditory meatus of the earto the outer orbital rim of the eye (Fig. 2). Theclosed vertical dimension in maximum intercus-pation is then calculated by subtracting 3 mm forthe freeway space.1 While the patient has his old
Before
A great set ofdentures canimprove patientappearance andlifestyle. Here aresome tips forensuring thehighest esthetics,function, andcomfort.
Continued on page 102
After

dentures in his mouth, I asked him to closeinto maximum occlusal contact. Com-paring this to the previous measurement,there was a 7-mm loss of vertical dimen-sion (Figs. 3 & 4).
Gothic arch tracingAn excellent method of capturing a cen-tric-relation bite registration is through aGothic Arch Tracing device.2 First, thelower chest is measured to locate the cen-tral point. The lower plate is attached withcompound to the recording base. A trac-ing plate is then attached to the upperrecord base with wax. The plate is alignedalong the vertical plane and secured withcompound wax. The tracing plate is coat-ed with a black marker. When possible, Ilike to do the Gothic Arch Tracing withthe six front teeth set in wax for greateraccuracy (Fig. 5). This can help better vi-sualize the final result.
If necessary, this is a good time to re-set or choose different teeth. The ball bear-ing pin is adjusted to the approximateclosed vertical dimension. I let the patienttell me when it feels right (Fig. 6). Whenin doubt, I like to open it another 0.5 mm.Once the proper vertical dimension is cho-sen, both for esthetic proportions and forcomfort, the patient is instructed to movethe jaw in excursive movements, espe-cially lateral and protrusive movements.
Following all of the appropriate mandibu-lar movements, the ball bearing has markedan arrow-shaped figure into the upper plate.A plastic square with a circular cutout isplaced over the arrow tip and luted to theplate. The assembly is placed back in themouth (Fig. 7), and the ball bearing is nowset with in the plastic square. Genie rapid-setting (60 seconds) bite registration ma-terial (Sultan Healthcare, www.sultan-healthcare.com) is syringed into the as-sembly to capture centric relation. The biteis completely syringed to lock in the biterelationship between the upper and lowerjaw. Once set, the entire assembly is re-moved and the casts will then be mount-ed on a semi-adjustable articulator.
102 November 2006 Dental Products Report
practice webjr 1/2 h
miltexjr 1/2 h
See us at the XXX Meeting, Booth XXX.Use XXX on card or at www.dentalproducts.net
See us at the XXX Meeting, Booth XXX.Use XXX on card or at www.dentalproducts.net
Layout OK 1st edit 2nd edit 3rd edit Final edit Ad Production
6
7
8
5
(5) The Gothic Arch Tracingis done with the six frontteeth set in wax. (6) The
patient ultimately decides ifteeth are set properly.
Successful removablesClinician’s Comments
Continued from page 100
(7 & 8) Centric relation is captured bysyringeing the bite registration materialand locking in the bite relationshipbetween the upper and lower arches.

Posterior teethThe majority of complete denture patientsare older adults. Cuspal height should fol-low that natural progression of wear to alower or less steeply inclined cuspal plane.I generally use teeth with a 10° cuspal in-clination. Posterior teeth that are too steepcan place undo stress on the ridges as wellas the temporomandibular joint. This cancontribute to sore spots, as well as tem-poromandibular dysfunction.
Fourth visit: Wax try-inThe wax try-in is the critical point in thedenture process. We must evaluate thedenture in terms of fit, stability, phonet-ics, esthetics, and the occlusion (Fig. 8).We test for the consonant sound of “S”,“SH”, “T”, “N”, “L”, “CH”, “J”, “K”,“F”, and “V”. This is the time for every-one—the doctor, the dental team, andmost importantly, the patient—to evalu-ate everything from the tooth position,tooth shape and length, gumline, color,the way the denture feels against the lips,
cheeks and tongue as well as the “feel” ofthe occlusion. Having a family memberpresent always helps. I generally ask aman to bring his wife or daughter. For awoman, I suggest they bring a sister, adaughter, or a best friend. This is critical.A good-looking denture always fits bet-ter. Once the wax try-in is approved for thebest fit and bite, I take a new bite regis-tration (Fig. 9). With the bite registrationin place, I take wash impressions withlight-body material in the wax try-in-plates, maxillary arch first (Fig.10). I use
these additional records for a clinical re-base and remount. Remember—“denturescan’t be too tight, and the bite can’t be toogood.”
Before processing any removable pros-thesis, I always give the patient the optionof having a duplicate, or “identical twin,”
Dental Products Report November 2006 103
Glaxo smith klineStandard Page
ribbondJunior 1/6 h
Use XXX on card or at www.dentalproducts.netSee us at the XXX Meeting, Booth XXX.
Use XXX on card or at www.dentalproducts.net For sales visit, circle XXX on cardSee us at the XXX Meeting, Booth XXX.
Layout OK 1st edit 2nd edit 3rd edit Final edit Ad Production
10
(9) A new bite registration is taken afterthe wax try-in is approved. (10) Washimpressions with light-body materialare taken in the wax try-in plates.
9
FOURTH VISIT
Continued on page 104

made at a reduced fee. This helps preventunexpected emergencies that may result inno teeth. Also, this duplicate proves con-venient when the original is being relinedat the laboratory. Patients will never haveto go without a smile. Like most of my pa-tients, he appreciated this extra service.
Fifth visit: DeliveryAt the seating appointment, we comparethe old dentures (Figs. 11a & 12a) withthe new dentures (Figs. 11b & 12b). Thenew dentures are tried in for esthetics,speech, and comfort. The patient shouldbe aware that the delivery of the new den-ture is not the end, but only part of theprocess. Adjustments to the inside of thedenture and/or the teeth are to be expect-ed. Every adjustment has the potential toloosen the denture. It’s better to see the pa-tient more times for small adjustments,rather than fewer times for major adjust-ments. We can alleviate any potential sorespots through the use of pressure disclos-
104 November 2006 Dental Products Report
essential dentalStandard Page
Use XXX on card or at www.dentalproducts.net For sales visit, circle XXX on cardSee us at the XXX Meeting, Booth XXX.
Layout OK 1st edit 2nd edit 3rd edit Final edit Ad Production
Successful removablesClinician’s Comments
11b
12a
12b
(11a) The original maxillary denture.(11b) The new maxillary denture. (12a) The original mandibular denture.(12b) The new mandibular denture.
11a
FIFTH VISIT
“A well-made denture should have a bilaterallybalanced lingualized occlusion…[to] bettercentralize the forces over the ridge, improvechewing function and stabilize the dentures.”
Continued from page 103
ing paste and selective “buffing.”A well-made denture should have a bi-
laterally balanced lingualized occlusion.This type of occlusion will better cen-tralize the forces over the ridge, improvechewing function, and stabilize the den-tures. I evaluate the bite at first by usinghorseshoe-shaped articulating paper. Ini-tially, the patient bites into the paper withan open and closing motion of themandible. Adjustments are made untiluniform markings are seen on the lowerbuccal cusp tips, upper lingual cusp tips,and the central grooves of both upper andlower posterior denture teeth. Very heavyanterior contact will cause tipping and un-seating, especially of the upper denture.The lower denture should not interferewith the tongue and it movements.
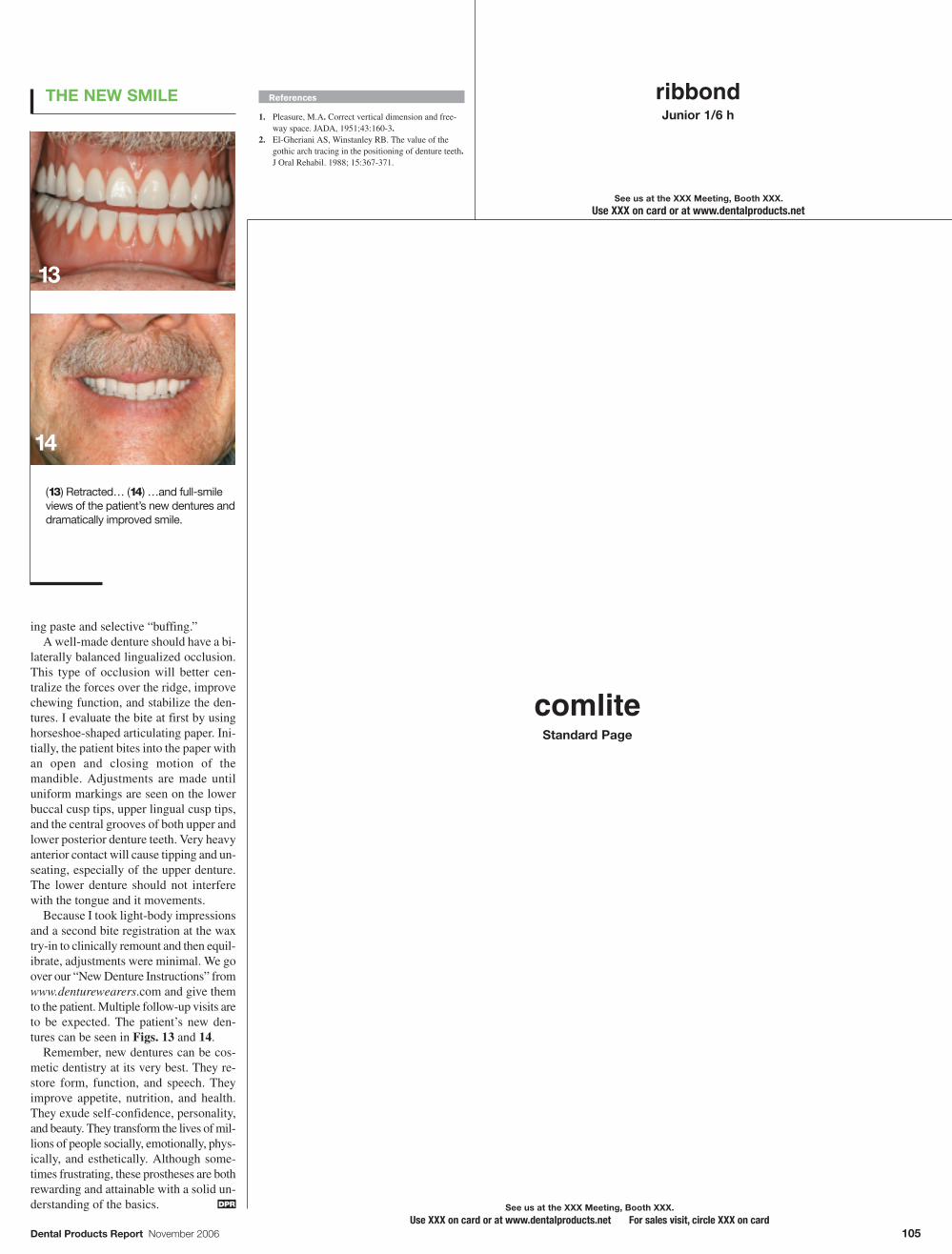
Because I took light-body impressionsand a second bite registration at the waxtry-in to clinically remount and then equil-ibrate, adjustments were minimal. We goover our “New Denture Instructions” fromwww.denturewearers.com and give themto the patient. Multiple follow-up visits areto be expected. The patient’s new den-tures can be seen in Figs. 13 and 14.
Remember, new dentures can be cos-metic dentistry at its very best. They re-store form, function, and speech. Theyimprove appetite, nutrition, and health.They exude self-confidence, personality,and beauty. They transform the lives of mil-lions of people socially, emotionally, phys-ically, and esthetically. Although some-times frustrating, these prostheses are bothrewarding and attainable with a solid un-derstanding of the basics.
References
1. Pleasure, M.A. Correct vertical dimension and free-way space. JADA, 1951;43:160-3.
2. El-Gheriani AS, Winstanley RB. The value of thegothic arch tracing in the positioning of denture teeth.J Oral Rehabil. 1988; 15:367-371.
DPR
Dental Products Report November 2006 105
comliteStandard Page
ribbondJunior 1/6 h
Use XXX on card or at www.dentalproducts.netSee us at the XXX Meeting, Booth XXX.
Use XXX on card or at www.dentalproducts.net For sales visit, circle XXX on cardSee us at the XXX Meeting, Booth XXX.
Layout OK 1st edit 2nd edit 3rd edit Final edit Ad Production
14
(13) Retracted… (14) …and full-smileviews of the patient’s new dentures anddramatically improved smile.
13
THE NEW SMILE













![DENT...Porcelain and cast restorations; prosthodontics (fixed partial dentures [bridges], removable partial dentures, and complete dentures); implants; etc. CLASS IV: ORTHODONTICS](https://static.fdocuments.in/doc/165x107/5ed5609cf98bb3308d2fa371/dent-porcelain-and-cast-restorations-prosthodontics-fixed-partial-dentures.jpg)

