Embrex Inovoject Systems - Zoetis | zoetisUS.com | Zoetis US

Expert Views from a Roundtable on Canine Allergic Disease
clinician’s forum™
Everything You Need to Know ButWere Too Busy to Ask About:
Itchy Dogs—Part 2Building a Clinical Toolboxfor Treating Allergic Patients
PARTICIPANTS
Michael J. Day, BSc, BVMS (Hons), PhD, DSc,DECVP, FASM, FRCPath, FRCVSProfessor of Veterinary PathologySchool of Veterinary SciencesUniversity of BristolBristol, United Kingdom
Craig Griffin, DVM, DACVDFounder and Co-ownerAnimal Dermatology ClinicsSan Diego, California
Rosanna Marsella, DVM, DACVDProfessor, Department of DermatologyCollege of Veterinary MedicineUniversity of FloridaGainesville, Florida
Tim Nuttall, BSc, BVSc, CertVD, PhD, CBiol, MSB, MRCVS Senior Lecturer in Veterinary DermatologyUniversity of Liverpool Liverpool, United Kingdom
Sonja Zabel, DVM, MS, DACVDAssistant Professor of DermatologyCollege of Veterinary MedicineUniversity of GeorgiaAthens, Georgia
This document reflects the discussion of the participantsat a live roundtable moderated by Dr. Kathy Gloyd of theGloyd Group, Inc., Wilmington, Delaware.
Building on the discussion from Part 1 of thisDermatology Roundtable (Itchy Dogs – Part 1Diagnosis & Communication, February 2013),our experts discuss treatment of allergic condi-tions in dogs and give advice on how to createa dermatology toolbox for your clinic. This col-lection of tools is essential to have in your clin-ic’s pharmacy for the treatment of a variety ofpruritic conditions in dogs.
UNDERSTANDING THEUNDERLYING DISEASEPROCESS IS FUNDAMENTALTO DEVELOPING A TREATMENT PLANKnowledge of the underlying disease processesis fundamental for clinicians to effectively diag-nose, treat, and manage allergic patients.Stopping the itch is a key first step in allowingskin to heal and restoring quality of life for thedog and its owner. Equally important is limit-ing exposure to allergens, addressing barrierfunction, and treating secondary infections.
Dr. Marsella: Scientific research outlined ina recent article (Marsella R, JAVMA 241 [2],
clinician’s forum™ • 1
Sponsored by
an educational
grant from
Zoetis
KEY POINTS FROM PART ONE• Knowledge about the
underlying disease process isessential context for clinicianstreating allergic dogs.
• Stopping the itch is a key firststep to allow the skin to healand to restore quality of life forthe dog and the owner.
• Equally important is identifyingthe underlying cause of theitch, regardless of whetherit is parasitic, infectious,immunologic, or as is oftenthe case in chronically itchydogs, a combination of these.
• Long-term management isbased on controlling flares bylimiting exposure to allergens,addressing barrier function, andcontrolling secondaryinfections.
• Open communication, includingempathizing with ownerfrustration, clearly settingexpectations, and outliningtreatment goals, creates apartnership with the pet ownerthat can lead to improvedcompliance with your treatmentrecommendations––therebyenhancing client loyalty andaiding in patient retention.

The pruritus is what is driving petowners to the clinic in the firstplace. Many owners will measureyour treatment success solely onthe dog’s level of pruritus.
—Dr. Zabel
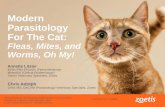
2012) has provided new insights into theimmunologic processes associated with aller-gic disease. We are now focused on neuroim-munology, the interaction between the nerv-ous system and the immune system, and therole it plays in allergies. In particular, it is therole of cytokines such as IL-31, IL-4, IL-5, IL-9, and IL-12. These cytokines are small pro-tein molecules that can act as signals at variouspoints in the cycle of itch, resulting in itch andinflammation (Figure 1). Understanding thevarious aspects of this cycle of itch, includinghow environmental allergens cross the skin toinitiate the immune response and howcytokines stimulate neuronal itch and inflam-mation, can identify places where varioustherapeutic modalities might be helpful indeveloping a treatment regimen tailored to theneeds of an individual patient. Taken together,these therapeutic options contribute to themultimodal toolbox we will discuss later.
FIRST LINE TREATMENT:STOPPING ITCH IS A KEYELEMENT OF YOUR INITIALPLANDr. Zabel: I think the pruritus is what isdriving pet owners to the clinic in the firstplace. Many owners will measure your treat-ment success solely on the dog’s level of pru-ritus. As clinicians, what we see is improve-ment in the lesions on the skin, but often ourowners don’t see that, only reduction of theitch.
Dr. Marsella: Owners definitely notice thattheir dog scratches all night long. Nobody getsany sleep, everyone is sleep deprived, and inthe end it is a bad day for everyone all around.
Dr. Nuttall: Of course—because it’s thescratching that results from itch that keepsthem awake at night! They don’t see the allergic
2 • clinician’s forum™
conjunctivitis that is so prevalent, but so minor,compared to the skin disease.
Dr. Griffin: What the owners can’t get past isthe self-trauma their dogs are inducing and therealization that this means their pet must besuffering. Stopping that really has an impact onthe owners and the pet.
Dr. Marsella: The self-trauma is potentiallycausing additional damage to the skin barri-er, which may increase the risk for coloniza-tion and infection with bacteria. So if thepruritus is not treated and the cycle contin-ues, a dog will get overcolonized—when thetrauma induces additional damage to theskin and you have a patient with a clinicalinfection. So while the owner sees the annoy-ance and suffering from pruritus, we have toconsider the end result of the itch and theimportance of the resulting inflammation.
Prof. Day: There are all kinds of specificreceptors and molecules that are involved inthe itch/scratch cycle. The triggers of pruri-tus can be multiple; for example, toxins fromstaphylococcal bacteria can nonspecificallyenhance the immune response and perpetu-ate T-cell activity. Therefore secondary bac-terial or yeast infections can further disturban abnormal immune system. So using anantipruritic that will stop the itch, regardlessof the cause, should be a cornerstone of treat-ment in general veterinary practice.
Dr. Marsella: Owners are typically looking forsomething fast-acting and highly effective tostop the itch—even if this is not the first timethe dog is presenting with allergic signs.Treating pruritus can also be important inchronic cases or dogs that present with a flare-up. I explain to my clients that itching is addi-tive and that we need to do cytology to see if
Owners are typicallylooking for somethingfast-acting and highlyeffective to stop theitch—even if this isnot the first time thedog is presentingwith allergic signs.
—Dr. Marsella

there is a bacterial or yeast component, which istypical of a first visit.
Dr. Nuttall: There is also the client’s perspec-tive of success; if you don’t manage the pruri-tus, you may either lose the client or managingthe secondary infection may become more dif-ficult if the dog continues to self-traumatize.Stopping the itch is a priority.
Dr. Griffin: Pruritus and skin inflammation arecharacteristic of all canine allergic dermatitispatients. Pruritus results from the stimulationof itch receptors by a variety of pruritic media-tors. So if you can eliminate the pruritus, youmake owners feel like you are successfully treat-ing their dog; but, in fact, you may not be con-trolling the underlying allergy and inflamma-tion. The result is an allergic mechanism that isstill occurring and allowing continued damageto the skin, which ultimately may lead to apoint where your treatment for pruritus is nolonger as effective. So the disease process andpruritus are very much related, but at the sametime they are also very separate.
DEVELOPING YOUR INITIALTREATMENT PLANDr. Griffin: Medicine is an art and a science.The science is in the consistent application of adiagnostic workup in each patient. It is impor-tant to have the discipline to keep working untilyou identify the underlying cause while effec-tively treating the clinical signs—but don’t justtreat the patient symptomatically. The art isreading the patient and the owner to under-stand their needs and develop an instinct onwhat to treat first. One approach is to initially“treat the treatable.” Start by ruling out diag-noses that can be readily identified and treated:flea allergy, parasitic disease, and bacterialinfection. Treat those and then recheck andreassess: have I cracked it yet? If not, move on
One thing that is characteristic ofallergic patients is they are itchy.Allergy creates inflammation andstimulation of itch receptors by avariety of pruritic mediators. So ifyou can eliminate the pruritus,you make owners feel like you aresuccessfully treating their dog.
—Dr. Griffin
Clinical Insight #1 Across the board, expertsagree that pruritus shouldbe addressed in everyallergic patient.
clinician’s forum™ • 3
to the more difficult conditions to identify ordiagnose—do a food trial or intradermal aller-gen testing. And as you move down that diag-nostic tree, keep tweaking the treatment proto-cols until you finally crack the code.
Dr. Marsella: One of the most important firststeps is stopping the itch! Continual scratchingin response to itch can further damage skin.Itch relief provides an opportunity for skin toheal. Scratching also frustrates owners anddiminishes the quality of life of the dog and itsfamily.
Dr. Zabel: On-going communication with thepet owner is another aspect to successful treat-ment of allergic disease. Long-term manage-ment of allergic patients requires that you cre-ate an environment in which the pet ownerscan become your partners in identifying thetherapeutic combination that will help manageflare-ups in their allergic dog. You need to setappropriate expectations: let pet owners knowit could require long-term management toeffectively control their dog’s allergies. Helpowners understand that allergy in dogs can becontrolled and managed, but not cured.
Dr. Griffin: Stopping the itch, while an essen-tial aspect of initial treatment regimens andlong-term protocols, does not solve the realproblem. Owners need to understand thatwhile controlling the itch is important, youmust continue until the underlying cause isidentified. If you stop short of communicatingthat to owners, the condition will likely recurand the owner can become more frustrated—with the dog and with you! In another exampleof good communication, I find in my practicethat when owners understand how rechecks fitinto the overall plan for reassessment and treat-ment, they are more likely to be compliant. Ifowners do not understand the importance of

4 • clinician’s forum™
each case, so will the selection of tools for eachtreatment protocol.
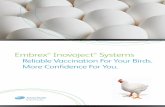
Dr. Griffin: I think each of us has a uniquemultimodal toolbox, like the one presented inTable 1, from which we are able to individualizeour treatment protocols.
Prof. Day: I think a “multimodal toolkit” is areally important concept. Realistically, no onething is the Holy Grail for treatment of everyallergic patient; each tool in our kit has a spe-cific action when treating allergic disease. It isthe ability to choose various elements from thekit for each patient and varying the combina-
rechecking and reassessing in the long-termmanagement of allergies, they may considerleaving your practice and finding another vet-erinarian. In many cases, this can be preventedwith open communication; as Dr. Zabel says,partner with the pet owner for successful long-term management.
ESSENTIAL ELEMENTS OFA MULTIMODAL TOOLBOX:INDIVIDUALIZINGTREATMENT PROTOCOLSAllergic dermatitis can be difficult to manageand can require a multimodal approach. Just asthe underlying cause of the pruritus varies in
Brain
Spinal Cord
DorsalRoot Ganglion
AllergensIncluding staphand malassezia
Allergen Presentation
Langerhans cell
Th Cell
Sensory Nerve
Blood Vessel
Mast Cell
Neutrophil Monocyte
Th2 Cell
Th1 Cell
Dendritic Cell
Cyto
kine
se.
g. a
aTSL
P
Cytokines
e.g. IL-31
Cyto
kine
se.
g. IL
-1, T
NF-α
Cytokinese.g. IFN-γ
Eosinophil
Pruritus, Pain
NeuronalItchStimulation
InflammatoryProcess
Scratching
Gc
Gc
Gc
GcGc
Gc
Gc
Gc
Fa
Fa
Fa
Fa
Gc
Gc
Gc
Gc
Gc
Ah
Ah
Cs
Cs
Cs
Cs
Cs
Cs
Ai
Ai
Glucocorticoids
Cyclosporine
Allergen-specific immunotherapy
Fatty acids
AntihistamineAh
Fa
Cs
Ai
Gc
Figure 1. Process underlying canine atopic dermatitis, including the sites where some common therapeutic interventions have some activity.From Marsella R, Sousa CA, Gonzales AJ, Fadok VA. Current understanding of the pathophysiologic mechanisms of canine atopic dermatitis. JAVMA 241:194-207, 2012. Used with permission.
Choosing various elements from the kit and varying thecombination of the “tools” we use to individually tailor a plan for each patient are the key totreatment success.
—Prof. Day
Clinical Insight #2 Veterinarians need todevelop a multimodaltoolkit that includesproducts to address itch aswell as inflammation,improve barrier function,treat underlying infections,and exert parasiticideactivity.

No two individual patients willrespond in exactly the same wayto a given treatment protocol forallergic and atopic conditions.
—Dr. Nuttall
clinician’s forum™ • 5
tion of the “tools” we use from it to individual-ly tailor a plan for each patient that is the key tosuccess.
Dr. Nuttall: No two individual patients willrespond in exactly the same way to a giventreatment protocol for allergic and atopic con-ditions. There is a great variety in response totreatment, where some dogs do brilliantly onimmunotherapy, others have no response, andstill others may partially respond but requiresupplemental antiinflammatory therapy. Thegenetics of the disease are very complicated,and that may partially explain this difference.Depending on which papers you read, there aremultiple genes involved and different areas ofmultiple chromosomes are associated with thedisease. The fascinating feature is that these arenot consistent and it is very much breed relat-ed, with a possible geographic component aswell. So a West Highland white terrier in Japanhas a different genetic background from one inthe U.S. or Europe.
Dr. Zabel: I would have to agree with your per-spective on the impact of geography. In myhands, cyclosporine* definitely worked for memuch better in Colorado than it does in Georgianow, where we see more flea-allergy dogs. It isthe fine-tuning that becomes the “art” of der-matology—there is no one recipe to treat everyallergic dog. This may be easier for dermatologyspecialists because that is what we do all day—and we tend to spend more time in each visitand follow-up. Veterinarians in general practicedo not always have this opportunity.
Dr. Nuttall: We have to look at our patientsand their varying levels of pathology and selecttreatments based on different modalities totreat the entire disease, including allergy, pruri-
Treatment of itch
Treatment Category Example
Antihistamine diphenhydramine
Systemic corticosteroids (oral orinjectable)
methylprednisolone, combinationantihistamine/prednisolone
Topical corticosteroids hydrocortisone
Treatment ofsecondary
infections and flare factors
Antibiotics for staphylococcalpyoderma and other secondaryinfections
Cephalosporins cefpodoxime, cefovecin, cephalexin
Potentiated sulfonamides sulfamethoxazole/trimethoprim, sulfadimethoxine/ormetoprim
Potentiated penicillins amoxicillin/clavulanic acid
Lincosamides clindamycin, lincomycin
Fluoroquinolones marbofloxacin, enrofloxacin
Antifungals for Malasseziacolonization
ketoconazole, itraconazole
Flea control any rapid-killing adulticide such asspinosad, fipronil, imidacloprid,selamectin; environmental therapy
Treatment of atopic
dermatitis
Allergen specific immunotherapy(injectable or sublingual)
Antiinflammatory drugs, nonsteroidal
cyclosporine or topical tacrolimus
Oral fatty acid supplements omega-3 fatty acids
Nonspecific therapies
Shampoos antiseptic, such as chlorhexidine,or properties to improve the skinbarrier with such agents as fattyacids or phytosphingosine
Moisturizing rinses containing phytosphingosine toimprove the skin barrier orpramoxine to help control itch
Hypoallergenic diet a diet containing both novel proteinand novel carbohydrate
tus, inflammation, and the flare factors. Thenselecting the modality may be a matter of aclient’s financial resources, client expectations,how quickly the owner wants a resolution, how
*In many resources cyclosporine may be alternatively referred to asciclosporin.
Table 1: Multimodal toolbox for treating allergic patients*
*Some of the products in this table are not labeled for use in animals in certain geographic areas and should be usedaccording to local regulations.

6 • clinician’s forum™
acids that was presented at the WorldCongress of Veterinary Dermatology. It wascontrolled, to overcome the concept of justclinical impression, and I think we showedsome efficacy. I believe topical fatty acids willnot be sufficient to work as the only therapy,but as an adjunctive therapy I think they havea place for sure, as there is preliminary evi-dence showing such therapy can actuallyrestore the skin barrier.
Dr. Nuttall: We like to look at all the optionswe have available for treatment, and bathing ismy favorite. But some owners cannot or willnot be compliant. So we look at fatty-acid sup-plementation. There is also the possibility ofspot-on fatty acids.
QUALITY OF LIFE INALLERGIC PETS ANDOWNERS: THE ROLE OFCORTICOSTEROIDSQuality of life is an issue that affects both theallergic pet and its owner. In Part 1 of this serieswe discussed an owner’s treatment objectivesand using them to create a common achievablegoal and to define what success looks like.
Dr. Nuttall: When managing an acute flare, Itypically do it with corticosteroids. However,because of long-term systemic effects and qual-ity of life issues, we try to manage flares orchronic cases using multimodal therapy thatmay include shampoos and other antipruritics.
Prof. Day: Corticosteroids should be used judi-ciously and at the lowest effective dose.Otherwise we can end up with the disastercases. Corticosteroids are the most commonlyused drug in veterinary practice, and yet theseare not licensed veterinary products. It is ironicthat we all talk about the broad spectrum of
As clinicians, what we see are the lesions on the skin, but oftenour owners don’t see that––onlyreduction of the itch! Treating theitch provides results that canultimately improve quality of lifefor the patient’s family.
—Dr. Zabel
risk-averse the client may be, and how capablehe or she is in giving an injection or pilling thedog. We really need to assess a client’s needsand abilities when individualizing a treatmentplan. Of course, we will always have pet ownerswho prefer monotherapy because it is simple.However, we really must consider everything inour toolbox and use tools in a multimodal reg-imen.
Dr. Marsella: I would say a lot of the atopicpatients that I see have multiple allergies: thatcan be hard to recognize. There are a multi-tude of allergens, some of which may or maynot be responsive to single treatments likecyclosporine. For instance, a lot of thepatients we see have a concurrent flea allergyand as much as we try to control the fleas,they may still have the occasional exposure.The cyclosporine is not going to be 100%effective in a case like this. In theorycyclosporine should also help with contactallergy but probably not as much as it doesfor atopic dermatitis.
Dr. Nuttall: Additionally there are dogs withunderlying parasitic infections that are notalways identified—a good example is scabies.We always scrape a case with nonresponsivepruritus multiple times. We also treat proac-tively if we suspect scabies but get negativescrapings. In my practice, I use one of the spot-on products registered for dogs every twoweeks for at least three applications, and wetreat the environment. I have never found a dogthat I know has scabies that has not respondedto one of those treatment regimens. But I willnot know if I missed one; you cannot prove anegative.
Dr. Marsella: Additionally, there is topicaltherapy to help address barrier function. Wehave actually done a study on spot-on fatty
Clinical Insight #3 Quality of life issues areimportant for dogs withchronic skin conditions.Corticosteroids can be used effectivelyshort-term to manageflares, but PU/PD can be a problem. And for a lot of owners this is notacceptable.

effects and how corticosteroids interfere withthe pruritus pathway, but we have absolutely noevidence base for such statements. There arevery few studies that have ever addressed thebasic pharmacokinetics of glucocorticoids indogs and cats, and even fewer that have shownprecisely what effects these drugs have on thenormal or diseased immune system in smallanimals.
Dr. Zabel: There are ways to judiciously usesteroids to minimize safety concerns. There arelots of patients for whom use of steroids is war-ranted but only when used correctly.
Dr. Griffin: There is a significant level of steroid-phobia in general practice today. I think it is acombination of what veterinarians were taughtin university as well as the fact that steroids dohave tremendous risk. But we don’t really knowthe risk, as there are no good, controlled studiesthat I am aware of. This makes it difficult toaccurately judge the actual risk of using corticos-teroids using an evidence-based approach.
Dr. Nuttall: I agree there is a generation of vetsand owners who are now steroid-phobic. It canpresent a real barrier in cases I think wouldbenefit from appropriate use of steroids. Thekey is close monitoring of the case and com-munication with the owners because sideeffects vary and what is acceptable for one dogmay not be acceptable for another. We willmonitor patients on long-term steroids by tak-ing a urine sample every 3 to 6 months and per-forming a culture, but we rarely have a positive.It can be difficult to predict how a patient—oran owner for that matter—will react to treat-ment with steroids. For a lot of my clients, anypolyuria or polydipsia is unacceptable. I canremember a chocolate Labrador I treated thatdid very poorly on a low dose of steroids. Butthen I can also remember small dogs that have
I think it is very important torecognize that although steroidsare very effective drugs, there are also limitations in terms of the extent of use and long-termefficacy.
—Dr. Marsella
been on 10 mg for years without a problem. Ithink a small population of dogs is very sensi-tive even to low doses of corticosteroids, butmore typically dogs are fine if steroids are usedjudiciously. I also see dogs that are being main-tained on very low doses, less than 0.5 mg/kgevery other day, and wonder how that can havean effect. But we can test that by taking them offtherapy: as soon as you remove a dog from anefficacious treatment regimen, the owner willtell you!
Dr. Marsella: I think it is very important torecognize that although steroids are a veryeffective drug, there are also limitations interms of the extent of use and long-term effica-cy. Overall I think clients tend to be more edu-cated and are looking for individualizedoptions: they are ready to explore alternativesthat they can feel better about rather than acookbook recipe.
MAXIMIZING TREATMENTSUCCESS WITH GOODCOMMUNICATIONDr. Griffin: We talked about the impact ofgood communication between the veterinari-an and the pet owner and how key it can be totreatment outcome. I always try to remember:if I talk about 15 things during the office visit,the owner might remember 2. So I alwaysemphasize the most important things in ourpersonal discussion, follow up with writtenmaterial that can be reviewed at home—andmake sure my hospital staff demonstratesprocedures such as how to pill a dog or thecorrect way to apply topical medications ifadditional reinforcement is needed.
Dr. Zabel: A treatment regimen can be suc-cessful only if the owner is able to execute itproperly! Create an environment of partner-
clinician’s forum™ • 7

ship and collaboration where you and theowner can work together to get the dog better.It is important to empathize with the owner onthe difficulty of managing a chronic dermatol-ogy patient. Reinforce good behavior; let themknow when they are doing a good job. Ask ifthere are specific limitations, such as an arthrit-ic condition, that can impact their ability to becompliant with the treatment recommenda-tions that have been made. Don’t seem judg-mental or dismissive, either.
Dr. Nuttall: It is a combination of assessingwhat the owner can handle and what is bestfor the patient. You really need to get the clienton board with long-term management withthe expectation that you will not solve theproblem with one visit, it just can’t be done; ittakes both time and patience. Many clients arejust looking for monotherapy. You may haveto work within those confines or patientlywork over time to convince them otherwiseand change their expectation.
NEW TREATMENT OPTIONS:LOOKING FORWARD TO THEFUTURENeuroimmunology, the interface between theimmune system and neuronal itch stimulation,is on the forefront of the development of futuretherapies for allergy. This area of research isstate-of-the art in human medicine and has thepotential to deliver a nonsteroidal treatment foritch or an antipruritic that blocks itch sensationregardless of what the underlying conditionmight be. New research findings have thepotential to provide us with the ultimate addi-tion to our toolbox!
Dr. Griffin: There is a whole new science now,that of neuro-endocrine-immuno-dermatol-ogy. A group of scientists is researching theinteractions between neurology, endocrinolo-
gy, immunology, and dermatitis and all four areinvolved in pruritus.
Dr. Marsella: Neuroimmunology, and the con-nection between the nervous system and theimmune system, plays a tremendous role inallergies and in immune responses in general.
Prof. Day: Allergic disease is a result of animmune system that is out of balance or dysreg-ulated. Allergic disease does not happen with-out cytokines; and the single most importantconcept is the balance between the variouscytokines and which specific cytokines domi-nate in the disease process. Cytokines are inter-cellular communication modules. Classicallyallergic disease is going to have more Th2-relat-ed cytokines, IL-4, -5, -9, and -13. When you getchronic secondary infections, there may be aswitch to Th1-related cytokines such as interfer-on gamma (IFN-γ) and the family of Th17-related cytokines. Moreover, underlying all ofthat is a deficiency in the cytokines that helpcontrol Th1- and Th2-related pathology; in par-ticular IL-10 from regulatory T cells (Treg).
Dr. Nuttall: It is an enormously complex anddynamic environment.
Dr. Marsella: It is a dynamic process. But stat-ed simply: cytokines are molecules that theimmune system uses to communicate witheach other and they affect immune responsesand proliferation.
Prof. Day: I believe that the new molecularand genetic studies will change our current wayof thinking and that in future allergic patientswill benefit from a more targeted therapeuticapproach that addresses the underlying mecha-nisms of allergy. The gold standard for treatingallergic diseases should ultimately target the T-cell imbalance in these diseases.
Allergic disease is the result of an immune system that is out of balance. Newtreatment options address this dysregulation.
—Prof. Day
8 • clinician’s forum™
AIF 1212055A
GLOSSARYNeuroimmunology:A branch of immunology that deals especially with the interrelationships of thenervous system, immuneresponses, and autoimmunedisorders
Cytokines: Small protein molecules that actbiochemically as intercellularcommunication molecules.Cytokines such as IL-31 havea role in the biochemicalstimulation of itch
Neuronal itchstimulation: Biochemicalprocess by which mediatorssuch as cytokines, proteases,or neuropeptides act onnerves to send a signal to thebrain, resulting in scratchingand other pruritic behaviors
Itch: A sensation that occurswhen irritation of the skincauses a desire to scratch*
Pruritus: A broader conceptthat involves perception atthe level of the CNS/brainfollowing stimulation of theneuronal network in the skin*
*“Pruritus” and “itch” are frequently usedinterchangeably byveterinarians in generalpractice when scratching or other pruritic behaviors(rubbing, licking, etc) areobserved in patients.