Clinical utility of the dexamethasone suppression test assessed by plasma and salivary cortisol...
8
Ps_vchiutry Research, 18, 143-150 Elsevier Clinical Utility of the Assessed by Plasma Determinations 143 Dexamethasone Suppression Test and Salivary Cortisol Nigel Cook, Brian Harris, Richard Walker, Rhoswen Hailwood, Emyr Jones, Sandra Johns, and Diana Riad-Fahmy Received JU(V 18. 1985; revised version received October 28, 1985; accepted January 9, 1986. Abstract. Concentrations of cortisol in saliva and plasma were compared in matched samples during a standard 1 mg dexamethasone suppression test. The study involved 185 routine psychiatric admissions, all of whom were classified according to DSM-III criteria. In a group of I22 matched samples of saliva and plasma, there was a Pearson correlation coefficient of 0.867 and a Spearman rank correlation coefficient of 0.869. Medication with anticholinergic side effects had little effect on the correlation and was not associated with major difficulties in salivary sampling due to “dry mouth.” In a group of 178 diagnoses where both saliva and plasma were obtained, results were almost identical. Although nonsuppression was found in all psychiatric conditions, there was a very significant association with major depressive episode with melancholia. Key Words. Dexamethasone suppression test, saliva, anticholinergic medication. The usefulness of the dexarnethasone suppression test (DST) has remained con- troversial since it was described as a possible marker for melancholia by Carroll et al. (1976a, 19766). Many groups of workers have attempted to replicate the original findings of Carroll et al. with varying degrees of success. Some reports support the original observations (Holden, 1983) while others have found a high percentage of nonsuppression in other psychiatric conditions and in normal volunteers. Further- more, the test appears to be influenced by many factors, including the stress of hospital admission (Berger et al., 1984) weight changes (Fichter and Pirke, 1985), and current medication, in addition to the various exclusion criteria outlined by Carroll et al. (1981). The system used for classification of patients may also influence the performance of the DST (Calloway et al,, 1984). Nigel Cook, B.Sc., M.L.S.O., is at the Tenovus Institute; Brian Harris, B.Sc., M.B., B.S., M.R.C.Psych., is Consultant Psychiatrist and Honorary Clinical Lecturer, Department of Psychological Medicine; Richard Walker, Ph.D., is Senior Biochemist, Tenovus Institute: and Rhoswen Hailwood, M.B., B.Ch., and Emyr Jones, M.B., B.Ch., M.R.C.Psych., are Registrars in Psychiatry, Department of Psychological Medicine, University of Wales College of Medicine, Cardiff. Sandra Johns. M.B., B.Ch., M.R.C.Psych., is Consultant Psychiatrist, Cefn Coed Hospital, Swansea. Diana Riad-Rahmy. Ph.D., is Top Grade Biochemist, Tenovus Institute, University of Wales College of Medicine, Cardiff. (Reprint requests to Dr. B. Harris, Department of Psychological Medicine, University of Wales College of Medicine, Heath Park, Cardiff, CF4 4XN, Wales, U.K.) 0165-1781~86:‘$03.50 @ 1986 Elsevier Science Publishers B.V.
-
Upload
nigel-cook -
Category
Documents
-
view
213 -
download
1
Transcript of Clinical utility of the dexamethasone suppression test assessed by plasma and salivary cortisol...

Ps_vchiutry Research, 18, 143-150 Elsevier
Clinical Utility of the Assessed by Plasma Determinations
143
Dexamethasone Suppression Test and Salivary Cortisol
Nigel Cook, Brian Harris, Richard Walker, Rhoswen Hailwood, Emyr Jones, Sandra Johns, and Diana Riad-Fahmy
Received JU(V 18. 1985; revised version received October 28, 1985; accepted January 9, 1986.
Abstract. Concentrations of cortisol in saliva and plasma were compared in matched samples during a standard 1 mg dexamethasone suppression test. The study involved 185 routine psychiatric admissions, all of whom were classified according to DSM-III criteria. In a group of I22 matched samples of saliva and plasma, there was a Pearson correlation coefficient of 0.867 and a Spearman rank correlation coefficient of 0.869. Medication with anticholinergic side effects had little effect on the correlation and was not associated with major difficulties in salivary sampling due to “dry mouth.” In a group of 178 diagnoses where both saliva and plasma were obtained, results were almost identical. Although nonsuppression was found in all psychiatric conditions, there was a very significant association with major depressive episode with melancholia.
Key Words. Dexamethasone suppression test, saliva, anticholinergic medication.
The usefulness of the dexarnethasone suppression test (DST) has remained con- troversial since it was described as a possible marker for melancholia by Carroll et al. (1976a, 19766). Many groups of workers have attempted to replicate the original findings of Carroll et al. with varying degrees of success. Some reports support the original observations (Holden, 1983) while others have found a high percentage of nonsuppression in other psychiatric conditions and in normal volunteers. Further- more, the test appears to be influenced by many factors, including the stress of hospital admission (Berger et al., 1984) weight changes (Fichter and Pirke, 1985), and current medication, in addition to the various exclusion criteria outlined by Carroll et al. (1981). The system used for classification of patients may also influence the performance of the DST (Calloway et al,, 1984).
Nigel Cook, B.Sc., M.L.S.O., is at the Tenovus Institute; Brian Harris, B.Sc., M.B., B.S., M.R.C.Psych., is Consultant Psychiatrist and Honorary Clinical Lecturer, Department of Psychological Medicine; Richard Walker, Ph.D., is Senior Biochemist, Tenovus Institute: and Rhoswen Hailwood, M.B., B.Ch., and Emyr Jones, M.B., B.Ch., M.R.C.Psych., are Registrars in Psychiatry, Department of Psychological Medicine, University of Wales College of Medicine, Cardiff. Sandra Johns. M.B., B.Ch., M.R.C.Psych., is Consultant Psychiatrist, Cefn Coed Hospital, Swansea. Diana Riad-Rahmy. Ph.D., is Top Grade Biochemist, Tenovus Institute, University of Wales College of Medicine, Cardiff. (Reprint requests to Dr. B. Harris, Department of Psychological Medicine, University of Wales College of Medicine, Heath Park, Cardiff, CF4 4XN, Wales, U.K.)
0165-1781~86:‘$03.50 @ 1986 Elsevier Science Publishers B.V.

144
In view of these findings, a recent workshop convened by the National Institute of
Mental Health concluded that although the DST may be a useful tool, its application in routine practice is limited (Hirschfeld et al., 1983). Furthermore, the Health and Public Policy Committee (1984) of the American College of Physicians recently concluded that the DST could not be recommended as a screening procedure for endogenous depression and, pending further investigation, should be considered a diagnostic test of unproven value. Despite these opinions, it is probable that the DST will continue to be used in research programs, and possibly in routine clinical practice as an aid to the diagnosis, prognosis, and management of endogenous depression (melancholia).
Although most workers rely on measurement of plasma cortisol concentrations for assessing the response to the DST, the introduction of radioimmunoassays having the sensitivity required for measurement of low concentrations of cortisol in saliva suggests the application of this noninvasive sampling procedure (Poland and Rubin, 1982). Early studies have shown that (1) changing cortisol concentrations in plasma are quickly and accurately reflected in saliva; (2) salivary cortisol concentrations are independent of changes in salivary flow rate; (3) salivary cortisol values reflect the more biologically active plasma “free” cortisol and may therefore have greater clinical significance than plasma “total” cortisol values in assessing the response to the DST, particularly in patients taking oral contraceptives or receiving estrogen therapy; and (4) salivary cortisol values provide a reliable indication of adrenocortical activity in patients with defects of the hypothalamic-pituitary-adrenal (HPA) axis (Riad-Fahmy et al., 1982). In the context of clinical psychiatry, however, it might be supposed that a number of problems would limit the usefulness of this technique, such as lack of cooperation in disturbed patients or the inability to produce saliva due to administra- tion of drugs with anticholinergic side effects (e.g., tricyclic antidepressants). Previous studies using saliva have been small, and carried out in a research situation (e.g., Ansseau et al., 1984). A large-scale clinical study is therefore necessary to validate the salivary DST. The work reported here has this as its main objective and is a comparison of the data derived from plasma and salivary cortisol determinations in assessing the response to the DST on a larger scale, with a critical evaluation of the test in routine clinical practice.
Methods
Patients. Over the course of 14 months (October 1. 1983-November 30, 1984), 187 routine psychiatric admissions were involved in the study. The age range of patients was from 17 to 90 years, with a sex ratio of females to males of 2: 1. Admission was usually for acute episodes of mental illness, but a group of patients with dementia were admitted to relieve relatives. Since the study was designed to investigate the usefulness of data derived from salivary sampling, patients remained on medication at the time of the test. This approach allowed evaluation of missed- sample rates due to problems of “dry mouth” in patients receiving anticholinergic drugs.
Patients were receiving a range of commonly prescribed psychotropic medications, including drugs reported to affect the DST such as carbamazepine and phenytoin (7 patients) and benzodiazepines (6 patients > 25 mg diazepam daily). They were allowed to settle in the ward for 4 days before the DST was carried out. On any one of the following 3 days, the test was administered. with I mg of dexamethasone being given orally at 2300h followed by saliva and plasma sampling at 1600h the next day. Saliva was always collected first, since a potentially

145
painful venipuncture may cause stress-induced changes in plasma and hence in salivary cortisol concentrations and produce a discrepancy in test results. Saliva was collected in plain 5 ml tubes; although patients were encouraged to produce as much saliva as possible, 0.5 ml is sufficient for the test. Blood (10 ml) was obtained by venipuncture and placed in standard lithium heparin tubes for centrifugation. The supernatant plasma was stored in a plain glass tube, as was the saliva specimen, and deep frozen. Samples were sent to the laboratory, and results were not made available to either psychiatrists or laboratory staff until after classification of the patients.
Classification of Patients. Patients were classified according to DSM-III (American Psychiatric Association, 1980) criteria in a team meeting involving three senior psychiatrists and junior trainees. Only four episodes of illness in three patients were subsequently reclassified.
It is, of course, possible for a patient to receive more than one diagnostic label, but such patients were not omitted from the study since a realistic, routine clinical situation was an essential requirement.
Radioimmunoassays. Plasma and salivary cortisol concentrations were determined by direct radioimmunoassay (RIA) techniques using a W-radioligand and an anticortisol serum coupled to a magnetizable-cellulose, solid-phase support. The antiserum, raised in rabbits against a cortisol-3-OCMO/ BSA conjugate by standard procedures, was coupled to the activated solid- phase support according to Seth and Brown (1978). The preparation of the homologous ‘*51-iodohistamine derivative, used as the label, was as described by Riad-Fahmy et al. (1975).
The standards used for constructing the dose-response curves were prepared using pools of cortisol free plasma and saliva, obtained from healthy volunteers in whom adrenal activity had been suppressed by prior administration of dexamethasone (2 mg).
The dose-response-curve standards for measurement of cortisol in plasma and saliva covered the range O-l 380 nmole/ 1 and O-4 1 nmole/l, respectively.
Based on precision profiles obtained from multiple sample analysis. both assays had acceptable lower limits of sensitivity (plasma 14 nmole/l; saliva 0.5 nmole/l).
The interassay coefficient of variation at the cutoff point of 137 nmole/l in plasma was 4.9%, and at 4.8 nmoleil in saliva was 5.6%.
Results
The comparisons of plasma and salivary cortisol levels were carried out at an earlier point in the study than the assessment of performance of the DST. For this reason, the patient numbers involved differ, and the results are presented in two parts.
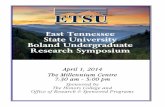
Comparison of Plasma and Saliva Cortisol Levels. A total of 160 patients were involved in the comparison of plasma and saliva cortisol levels. Twenty-one of these patients were excluded because either plasma or saliva samples were not available. A further 17 patients were repeat admissions and were also excluded from the comparison. Therefore, a total of 122 matched samples of plasma and saliva were considered. Fig. 1 illustrates the scatterplot obtained when saliva levels of cortisol were plotted against plasma levels. There is a clear positive association, with a correlation coefficient of 0.869 @ < 0.00 1) or a Spearman rank correlation coefficient of 0.867 (p < 0.001). The data were fitted by a straight line through the origin, according to which each unit of saliva cortisol corresponded to 28.66 units of plasma cortisol. This model gave a constant residual variance when log saliva cortisol was plotted against log plasma cortisol and the left-censored zero values (n ~44, plasma 14; saliva 0.5) representing the lower limits of detection were omitted.

146
Fig. 1. Correlation of plasma “total” and salivary cortisol determinations in 78 patients receiving and not receiving anticholinergic treatment
30,0-
240.
3 \ 5 : 18.0~
60 .
. I + Anthdiirgtc redcation
o - - Antichchnergic medicate
n= 70 r: 0869 m= O,OLl c= 0098
I , 0 200 400 600 800
Plasma cortisol (nmol/ L)
Twenty-six patients were identified who were receiving drugs such as tricyclic and quadricyclic antidepressants, phenothiazines, and butyrophenones. These were compared with 32 “anticholinergic free” patients. The two groups did not differ significantly in the slopes obtained when the log saliva cortisol concentration was plotted against log plasma cortisol. A further group of patients were identified who were receiving only tricylic or quadricyclic antidepressant medications (i.e., potently
anticholinergic) in doses of amitriptyline 2 75 mg/ day and mianserin > 30 mg/ day. In 10 of these patients, plasma and saliva cortisol levels were measurable, and these 10 were compared with 32 “anticholinergic free” patients. No significant differences emerged. In this smaller “anticholinergic” group, one saliva unit corresponded to 28.7 plasma units (95% confidence limits 17.1 to 48.2), and one plasma unit corresponded to 0.0348 saliva units (95yc confidence limits 0.0207 to 0.0585). In the “anticholinergic free” group, one saliva unit corresponded to 29.7 plasma units (95% confidence limits of 24.6 to 35.9) and one plasma unit corresponded to 0.0337 saliva units (95%

147
confidence limits 0.0279 to 0.0406). Thus, the “rate of exchange” for the smaller “anticholinergic” group is estimated to be 96.6% of that of the “anticholinergic free”
group. Bearing in mind the size of this smaller “anticholinergic” group, we concluded that anticholinergic drugs do not distort the relationship of saliva to plasma. This finding indicates that salivary cortisol concentrations reliably reflect those of plasma cortisol values in patients receiving medications with anticholinergic side effects; any reduction of flow rate that might possibly occur following such medication would therefore appear to have little if any effect on the plasma/saliva relationship (Fig. 1).
The data showed no evidence of bimodality as was the case with the data of Carroll et al. (1981) and therefore gave no clear indication of an escape value. We had no reason to reject the escape value of 137 nmole/l (5 pg/dl) specified by Carroll et al. (1981) and chose the corresponding salivary cortisol escape value of 4.8 nmole/l (I 74 ng/dl) according to the “rate of exchange” provided by the log-log regression model fitted.
DST Results. The performance of the DST is based on a larger group of admissions (n q 187). From this group, 15 patients refused to provide a saliva sample because they considered it to be “dirty or disgusting.” One patient, who was receiving high doses of clomipramine (200 mg/ day), was unable to provide a sufficient quantity of saliva for
analysis, giving a missed-sample rate for saliva of 8.6%. A further nine patients refused to supply a blood sample (4.8%). A total of 162 patients provided matched plasma and saliva samples. However, 16 of these patients had two psychiatric diagnoses. The performance of the DST was therefore assessed on a total of 178 diagnoses with matched plasma and saliva samples.
The six patients receiving benzodiazepines equivalent to > 25 mg diazepam/day were all suppressors. However, three of the seven patients receiving anti-epileptic medication (phenytoin) were nonsuppressors, and one of these was also melancholic.
DST responses in each diagnostic category are shown in Table 1. There were 10 discrepant results, of which only one was in the depression category. Discrepant results were those in which a patient was classified as a suppressor as judged by the plasma cortisol value but as a nonsuppressor as judged by the salivary cortisol value or vice versa. Discrepant results occurred when the patients’cortisol values were close to the escape value, e.g., the one discrepant result in the diagnostic category of “schizophreniform psychosis” had a plasma cortisol value of 130 nmole/l and a salivary cortisol value of 5.1 nmole/l. However, plasma and salivary cortisol determinations were found to perform equally well. Of 178 diagnoses, there were 42 nonsuppression results in plasma and 40 in saliva. Nonsuppression was found in most diagnostic categories. However, x2 tests show that nonsuppression is significantly associated with the DSM-/II diagnosis of “major depressive episode with melancholia” (p < 0.001, Table 1) in comparison to other episodes of depression.
There were a total of 74 diagnoses of depression, with the highest incidence of nonsuppression occurring in the DSM-II/diagnosis of”major depressive episode with melancholia” (58%). There were 41 diagnoses of “major depressive episode, unspecified, ” i.e., where melancholic features were present but were insufficient to justify the label “melancholia.” Of this group, only three were nonsuppressors (7%).

148
Table 1. Responses to the DST in plasma and saliva in various diagnostic subgroups
Plasma Saliva Discrepant DSM-III diagnoses n NS S % NS NS S % NS results
Major depressive episode with
melancholia 19 11 8 58 11 8 58 0
Major depressive episode unspecified
(probably melancholic) 41 3 38 7 3 38 7 0
Major depressive episode without
melancholia 9090090 0
Dysthymic disorder 1 0 1 0 0 1 0 0
Adjustment disorder with depressed
mood 2 1 1 50 0 2 0 1
Atypical depression 2 1 1 50 1 1 50 0
Primary degenerative dementia 11 3 8 27 3 8 27 0
Multi-infarct dementia 4 1 3 25 1 3 25 0
Paranoid schizophrenia 25 5 20 20 5 20 20 2
Schizophreniform psychosis 8 2 6 25 3 5 60 1
Manic episode 9 2 7 22 2 7 22 0
Substance abuse1 18 6 12 33 6 12 33 2
Personality disorders1 10 3 7 30 3 7 30 2
Neurotic disorders1 19 4 15 21 2 17 10 2
Total 178 42 136 40 138 10
Nonsuppression: Plasma cortisol. 137 nmole/l 15 rg/dll; salivary cortisol, 4.8 nmole/l (174 ng/dl~. DST = dexamethasone suppression test. NS = Nonsuppression. S = Suppression.
1. Various small subgroups of DSM-I// categories have been combined to form larger groupings.
Discussion
Several groups of workers have attempted to assess the role of salivary cortisol in the DST, with widely differing results. This is probably due both to variation and deficiencies in methodology. Some have developed their own “in-house” RIAs, while others have relied on modifications of commercially available kits. The sensitivity and specificity of modified kits may vary to a large extent. Levels of salivary cortisol are l-10% of those in plasma. Hence, any plasma cortisol assay must be completely re-optimized to maximize sensitivity and to take account of the change in hormone matrix.
Time spent in developing well-validated salivary assays is offset by the ease of sampling, particularly when multiple samples are required or in an outpatient setting. Furthermore, competitive protein binding (CPB) does not have the sensitivity or specificity of the RIA. Progesterone is known to cross-react with transcortin and may therefore interfere with the CPB assay; this problem is of particular relevance if the samples are from a woman of reproductive age in the luteal phase of the menstrual cycle.
The results presented demonstrate that plasma and salivary cortisol determinations

149
are equally valid in assessing the response to dexamethasone, provided that available immunoassays have the sensitivity and precision required for determining the low concentrations of this steroid in saliva. This contrasts markedly with the results of some workers who, using saliva, have only identified about 50% of the cases labeled as nonsuppressors with plasma (Wahby et al., 1984). However, in this preliminary communication, patient numbers were small and details of methodology sparse.
In matched plasma and saliva samples collected over several hours in a healthy volunteer after dexamethasone suppression and synacthen stimulation, the correla; tion was 0.95 (unpublished data). The lower correlation of 0.87 between plasma and salivary cortisol values from 78 patients is probably due to the varying levels of circulating transcortin between patients. There is no evidence that samples collected at any time other than 4 p.m. would fail to give an equally good correlation (Riad-Fahmy et al., 1982).
Neither disturbed mental state nor anticholinergic medication proved to be serious obstacles to saliva collection. Although reduced salivary flow rate and “dry mouth” are associated with anticholinergic medication, there was no problem in obtaining saliva samples. In addition, salivary cortisol continued to reflect plasma cortisol accurately. This is of importance since anticholinergic blockade not only reduces flow rate but, theoretically at least, alters the composition of saliva, and prevents parasympathetic nerve fibers from producing the normal profuse, watery, serous saliva from the parotid and submaxillary glands (Borgeat et al., 1984).
One of the main objectives of this study was to assess the DST in a routine clinical situation where more than one diagnosis was possible. There was no alternative, therefore, but to include such patients, and the results should be interpreted with this factor in mind. The rate of nonsuppression in the patients labeled as “major depressive episode with melancholia” (58%) is very similar to the result obtained by Carroll et al. (198 l), and our findings therefore support theirs, in that nonsuppression appears to be a useful marker of “melancholia” in the context of depression. Our results are of particular interest since they were obtained using saliva in a routine clinical setting where patients remained on medication and where exclusion criteria were ignored.
In our view, the salivary DST would be particularly useful in an outpatient setting,
where the patient may collect the saliva sample without contact with clinical workers; and also in a research setting where multiple samples are required, obviating the necessity of invasive techniques, such as intravenous cannulation.
References
American Psychiatric Association. DSM-III: Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. APA, Washington, DC (1980).
Ansseau, M., Sulon, J., Doumont, A., Cerfontaine, J.L., Legros, J.J., Sodoyez, J.C., and Demey-Ponsart, E. Use of saliva cortisol in the dexamethasone suppression test. Psychiatr) Research, 13,203 (1984).
Berger, M., Pirke, K.M., Doerr, P., Krieg, J.C., and von Zerssen, D. The limited utility of the dexamethasone suppression test for the diagnostic process in psychiatry. British Journal of Psychiatry, 145, 372 (1984).
Borgeat. F., Chagnon, G.. and Legault, Y. Comparison of the salivary changes associated with a relaxing and with a stressful procedure. Psychoph.vsiologv, 21, 690 (1984).

150
Calloway, S.P., Dolan, R.J., Fonagy, P., Desouza, V.F.A., and Wakeling, A. Endocrine changes and clinical profiles in depression: 1. The dexamethasone suppression test. Psychological Medicine, 14, 149 (1984).
Carroll, B.J., Curtis, G.C., and Mendels, J. Neuroendocrine regulation in depression: I. Limbic system-adrenocortical dysfunction. Archives of General Psychiatry, 33, 1039 (1976a).
Carroll, B.J., Curtis, G.C., and Mendels, J. Neuroendocrine regulation in depression: II. Discrimination of depressed from non-depressed patients. Archives of General Psychiatry, 33, 1051 (19766).
Carroll, B.J., Feinberg, M., Greden, J.F., Tarika, J., Albala, A.A., Haskett, R.F., James, N.Mc.I., Kronfol, Z., Lohr, N., Steiner, M., de Vigne, J.P., and Young, E. A specific laboratory test for the diagnosis of melancholia. Archives of General Psychiatry, 38, 15 (198 1).
Fichter, M.M., and Pirke, K.M. DST, endocrines and loss of weight. British Journal of Psychiatry, 147,94 (1985).
Health and Public Policy Committee, American College of Physicians. The dexamethasone suppression test for the detection, diagnosis and management of depression. Annals of Internal Medicine, 100, 307 (1984).
Hirschfeld, R.M.A., Koslow, S.H., and Kupfer, D.J. The clinical utility of the dexa- methasone suppression test in psychiatry: Summary of a National Institute of Mental Health workshop. Journal of the American Medical Association, 250,2172 (1983).
Holden, H.L. Depression and the Newcastle Scale: Their relationship to the dexamethasone suppression test. Brifish Journal of Psychiatry, 142, 505 (1983).
Poland, R.E., and Rubin, R.T. Saliva cortisol levels following dexamethasone administra- tion in endogenously depressed patients. Life Sciences, 30, 177 (1982).
Riad-Fahmy, D., Read, G.F., and Hillier, S.G. Radioimmunoassay for cortisol: Comparison of 3H, ‘5Se and r25I-labelled ligands. Journal of Endocrinology, 65,45P (1975).
Riad-Fahmy, D., Read, G.F., Walker, R.F., and Griffiths, K. Steroids in saliva for assessing endocrine function. Endocrine Reviews, 3, 367 (1982).
Seth, J., and Brown, L.M. A simple radioimmunoassay for plasma cortisol. Clinica Chimica Acta, 86, 109 (1978).
Wahby, V., Giller, E., and Mason, J. Use of saliva in the DST. Abstracts, XVth International Congress of the I. S. P. N. E., p. 14 ( 1984).