
Clinical Uses of HPV Testing
32
Clinical Uses of Human Papillomavirus (HPV) DNA Clinical Uses of Human Papillomavirus (HPV) DNA Testing Testing Kevin Holcomb, MD Division of Gynecologic Oncology New York Presbyterian Hospital Associate Clinical Professor Weill Medical College of Cornell University
-
Upload
macroglobulin35 -
Category
Health & Medicine
-
view
3.802 -
download
0
Transcript of Clinical Uses of HPV Testing
Clinical Uses of Human Papillomavirus (HPV) DNA Clinical Uses of Human Papillomavirus (HPV) DNA TestingTesting
Kevin Holcomb, MDDivision of Gynecologic OncologyNew York Presbyterian Hospital
Associate Clinical ProfessorWeill Medical College of Cornell University
Clinical Uses of HPV DNA TestingClinical Uses of HPV DNA Testing
• Management of women with abnormal cytologyManagement of women with abnormal cytology– Triage of women with ASC-US cytologyTriage of women with ASC-US cytology– Triage of postmenopausal women with LSIL cytologyTriage of postmenopausal women with LSIL cytology– Triage of adolescents with LGSIL cytologyTriage of adolescents with LGSIL cytology– Post-colposcopy follow-upPost-colposcopy follow-up– Post-treatment follow-up of CIN II and IIIPost-treatment follow-up of CIN II and III
• Adjunct to cytology for primary screeningAdjunct to cytology for primary screening
HPV Testing – Essential FactsHPV Testing – Essential Facts
• HPV is the major etiologic agent of cervical cancerHPV is the major etiologic agent of cervical cancer11
• HPV detection is associated with a 12X increased HPV detection is associated with a 12X increased risk of high-grade CIN risk of high-grade CIN 22
• Essentially all women with high-grade CIN have Essentially all women with high-grade CIN have detectable HPV DNA detectable HPV DNA 11
• Persistent infection with high-risk HPV is Persistent infection with high-risk HPV is necessary for development and maintenance of necessary for development and maintenance of CIN3 CIN3 3 3
1 Walboomers JMM, et al. J Pathol. 1999;189:12-19.2 Liaw K-l et al. J Natl Cancer Inst. 1999;91:954-960.3 Nobbenhuis MAE, et al. Lancet. 1999;354:20-25.
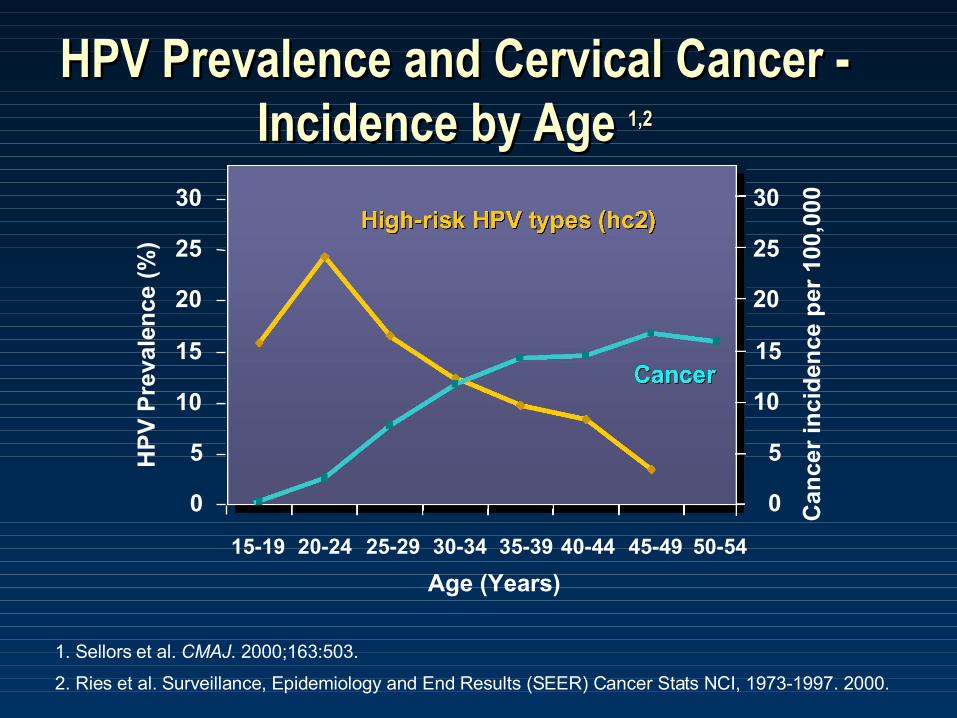
HPV Prevalence and Cervical Cancer - HPV Prevalence and Cervical Cancer - Incidence by Age Incidence by Age 1,21,2
1. Sellors et al. CMAJ. 2000;163:503.
2. Ries et al. Surveillance, Epidemiology and End Results (SEER) Cancer Stats NCI, 1973-1997. 2000.
Age (Years)
HP
V P
reva
len
ce (
%)
40-4415-19 20-24 25-29 30-34 35-39 45-49 50-54
0
5
10
15
20
25
30
0
5
10
15
20
25
30
Can
cer
inci
den
ce p
er 1
00,0
00
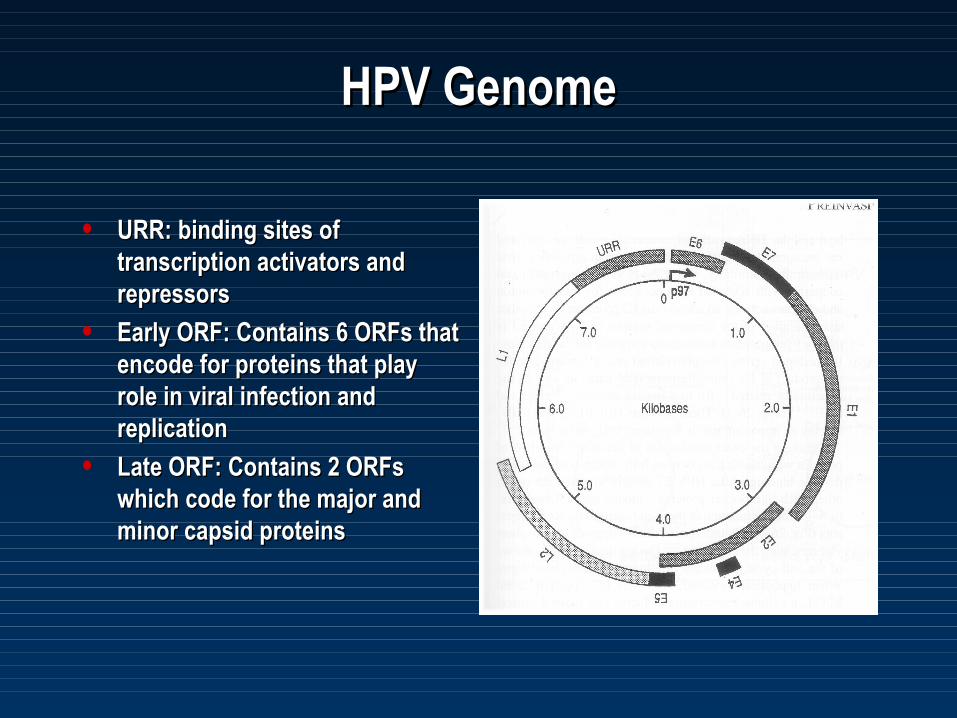
HPV GenomeHPV Genome
• URR: binding sites of URR: binding sites of transcription activators and transcription activators and repressorsrepressors
• Early ORF: Contains 6 ORFs that Early ORF: Contains 6 ORFs that encode for proteins that play encode for proteins that play role in viral infection and role in viral infection and replicationreplication
• Late ORF: Contains 2 ORFs Late ORF: Contains 2 ORFs which code for the major and which code for the major and minor capsid proteinsminor capsid proteins

HPV E7 ProteinHPV E7 Protein
• The major transforming and The major transforming and immortalizing activity of immortalizing activity of HPVHPV
• Cooperates with activated Cooperates with activated rasras oncogene oncogene
• Contains binding site for Contains binding site for Rb Rb gene product and gene product and RbRb-like -like pocket proteinspocket proteins
• E7 binding to E7 binding to RbRb blocks the blocks the tumor suppressor gene tumor suppressor gene function of function of RbRb
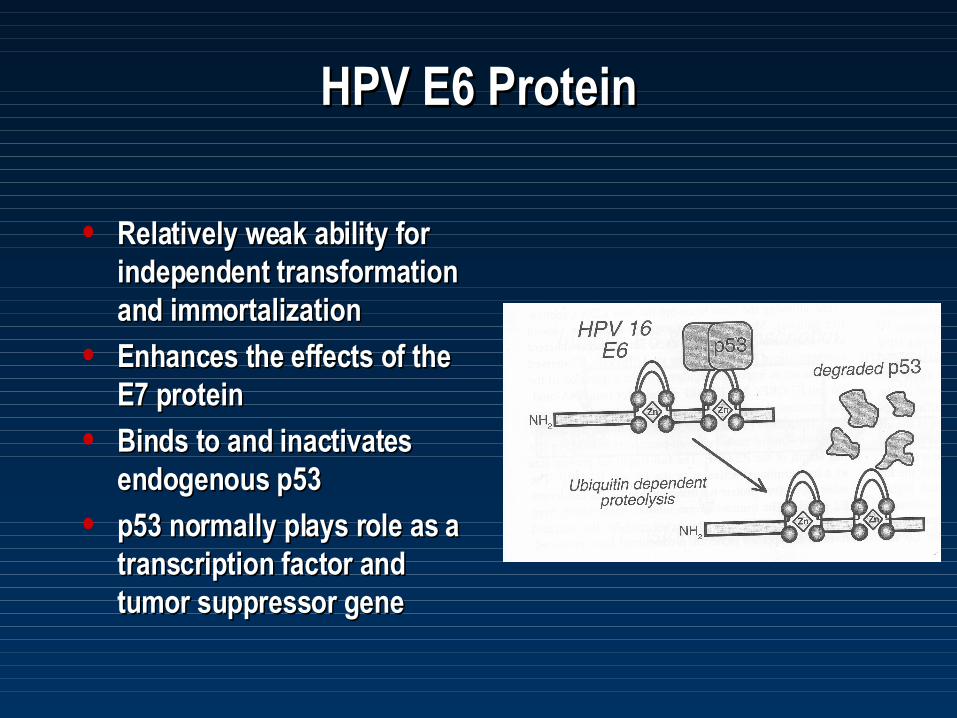
HPV E6 ProteinHPV E6 Protein
• Relatively weak ability for Relatively weak ability for independent transformation independent transformation and immortalizationand immortalization
• Enhances the effects of the Enhances the effects of the E7 proteinE7 protein
• Binds to and inactivates Binds to and inactivates endogenous p53endogenous p53
• p53 normally plays role as a p53 normally plays role as a transcription factor and transcription factor and tumor suppressor genetumor suppressor gene
Anogenital HPV TypesAnogenital HPV Types
• ““Low-risk” types: 6,11,40,42,43,44,53,54,61,72,73,81Low-risk” types: 6,11,40,42,43,44,53,54,61,72,73,81
• ““High-risk” types: 16,18,31,33,35,39,45,51,52,56,58,59,68,82High-risk” types: 16,18,31,33,35,39,45,51,52,56,58,59,68,82
• Possible “high-risk” types: 26, 66,73Possible “high-risk” types: 26, 66,73
Methods for Detecting HPV DNAMethods for Detecting HPV DNA
• Solution hybridization methodsSolution hybridization methods
• Polymerase chain reaction (PCR)Polymerase chain reaction (PCR)
• In-situ hybridization methods (ISH)In-situ hybridization methods (ISH)
HPV Risk TypesHPV Risk Types
• Hybrid CaptureHybrid Capture®®2 (hc2) HPV DNA Test uses two 2 (hc2) HPV DNA Test uses two RNA Probe cocktails to differentiate between RNA Probe cocktails to differentiate between carcinogenic and low-risk HPV types:carcinogenic and low-risk HPV types:Low-risk
6, 11, 42, 43, 44
High/Intermediate-risk
16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68
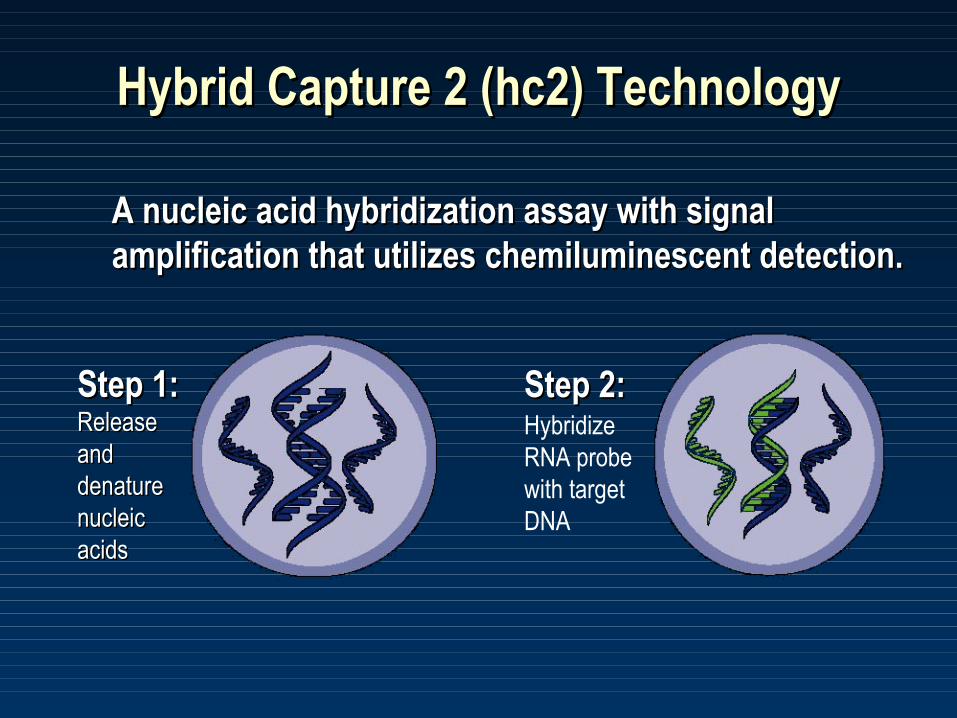
Hybrid Capture 2 (hc2) TechnologyHybrid Capture 2 (hc2) Technology
A nucleic acid hybridization assay with signal A nucleic acid hybridization assay with signal amplification that utilizes chemiluminescent detection.amplification that utilizes chemiluminescent detection.
Step 1: Step 1: Release Release and and denature denature nucleic nucleic acidsacids
Step 2:Step 2: Hybridize RNA probe with target DNA
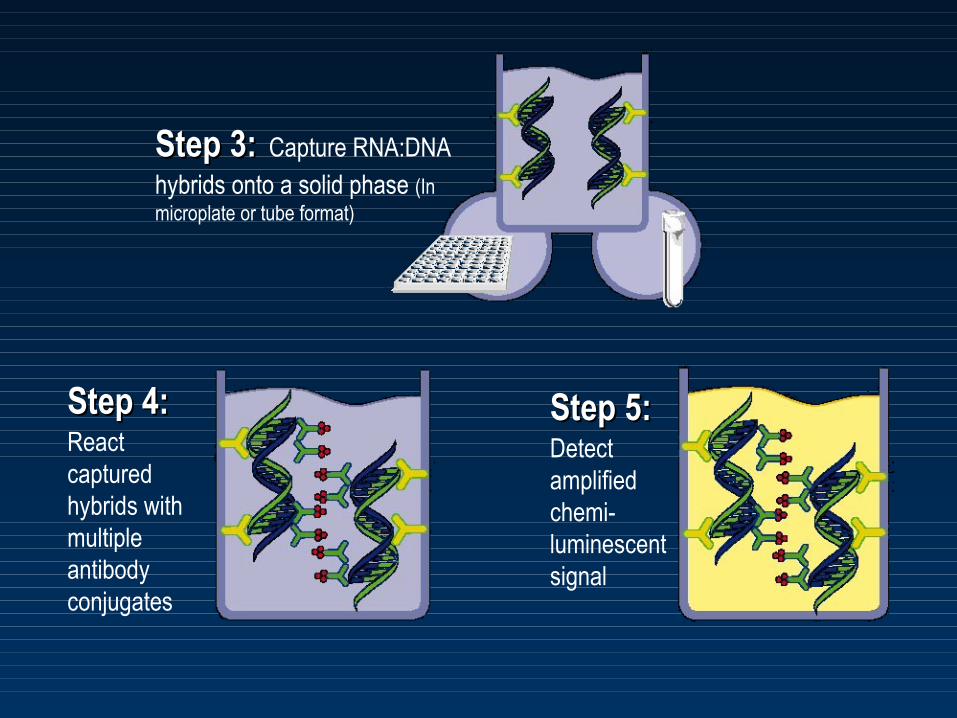
Step 3:Step 3: Capture RNA:DNA hybrids onto a solid phase (In microplate or tube format)
Step 4:Step 4: React captured hybrids with multiple antibody conjugates
Step 5:Step 5: Detect amplified chemi-luminescent signal
Polymerase Chain Reaction (PCR)Polymerase Chain Reaction (PCR)
• Extremely sensitive (lower limit several copies of target DNA)Extremely sensitive (lower limit several copies of target DNA)
• Typically uses consensus primers that amplify L1 gene of Typically uses consensus primers that amplify L1 gene of HPVHPV
• Can perform genomic sequencing of amplified materialCan perform genomic sequencing of amplified material
• Can determine the specific types of HPV present Can determine the specific types of HPV present
• Not approved by FDA for clinical useNot approved by FDA for clinical use
In-Situ Hybridization Methods (ISH)In-Situ Hybridization Methods (ISH)
• Labeled HPV DNA or RNA probes are hybridized with tissue Labeled HPV DNA or RNA probes are hybridized with tissue or cellsor cells
• Maintains the morphology of the tissue being testedMaintains the morphology of the tissue being tested
• Mainly used by pathology labs to identify HPV related lesionsMainly used by pathology labs to identify HPV related lesions
• Not FDA approved for clinical useNot FDA approved for clinical use
HPV DNA Testing in Women with HPV DNA Testing in Women with Abnormal CytologyAbnormal Cytology
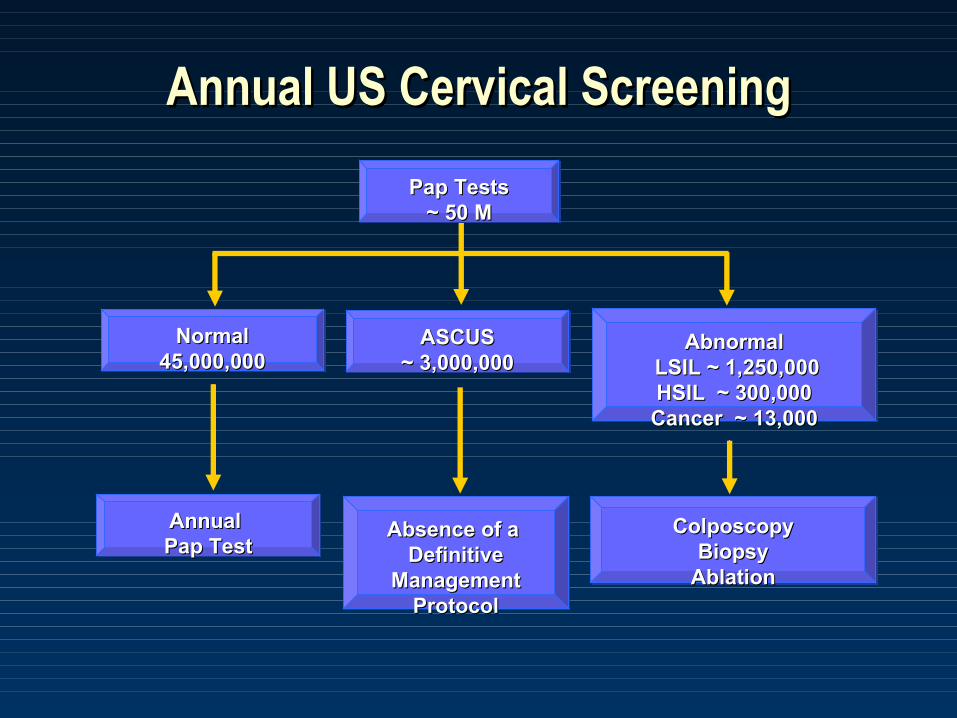
Annual US Cervical ScreeningAnnual US Cervical Screening
Pap TestsPap Tests~ 50 M~ 50 M
ASCUSASCUS~ 3,000,000~ 3,000,000
NormalNormal45,000,00045,000,000
AbnormalAbnormal LSIL ~ 1,250,000LSIL ~ 1,250,000HSIL ~ 300,000HSIL ~ 300,000Cancer ~ 13,000Cancer ~ 13,000
Absence of a Absence of a Definitive Definitive
ManagementManagementProtocolProtocol
Annual Annual Pap TestPap Test
ColposcopyColposcopyBiopsyBiopsy
AblationAblation
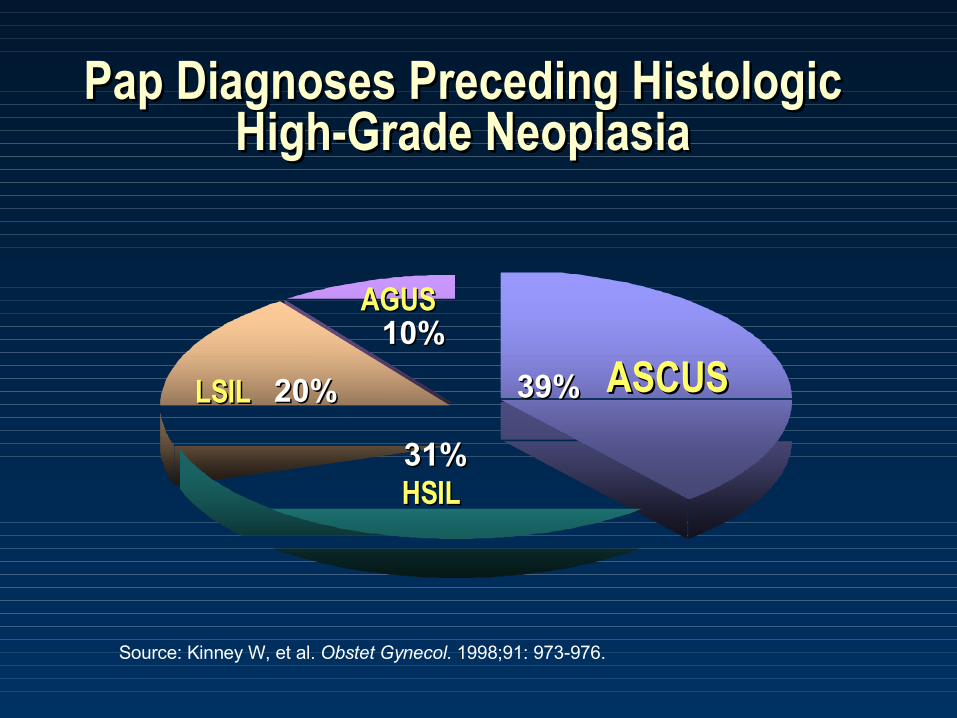
Pap Diagnoses Preceding Histologic Pap Diagnoses Preceding Histologic High-Grade NeoplasiaHigh-Grade Neoplasia
AGUSAGUS
LSILLSIL
HSILHSIL
ASCUSASCUS
Source: Kinney W, et al. Obstet Gynecol. 1998;91: 973-976.
20%20%
10%10%
31%31%
39%39%
ASCUS / LSIL Triage Study (ALTS)ASCUS / LSIL Triage Study (ALTS)
• Randomized clinical trial sponsored by National Randomized clinical trial sponsored by National Cancer InstituteCancer Institute 1 1
• University of Alabama, BirminghamUniversity of Alabama, Birmingham
• University of Oklahoma, Oklahoma CityUniversity of Oklahoma, Oklahoma City
• Magee-Woman’s Hospital, PittsburghMagee-Woman’s Hospital, Pittsburgh
• University of Washington, SeattleUniversity of Washington, Seattle
• Designed to determine the optimal patient Designed to determine the optimal patient management plan for ASCUS / LSIL cytologymanagement plan for ASCUS / LSIL cytology
• Began in 1996 – completed in 2002Began in 1996 – completed in 2002
1. Solomon D, et al. J Natl Cancer Inst. 2001;93:293-299.
ALTS Study DesignALTS Study Design
• Enrolled 3488 women with community-based Enrolled 3488 women with community-based ASCUS and 1572 with LSIL results, randomized ASCUS and 1572 with LSIL results, randomized to three management arms: to three management arms: 11
• Immediate colposcopyImmediate colposcopy• HPV triageHPV triage• Repeat cytologyRepeat cytology
• Clinical follow-up every 6 months for 2-year Clinical follow-up every 6 months for 2-year periodperiod
• LSIL arm discontinued due to limited utility of LSIL arm discontinued due to limited utility of positive test resultpositive test result
1. Solomon D, et al. J Natl Cancer Inst. 2001;93:293-299.
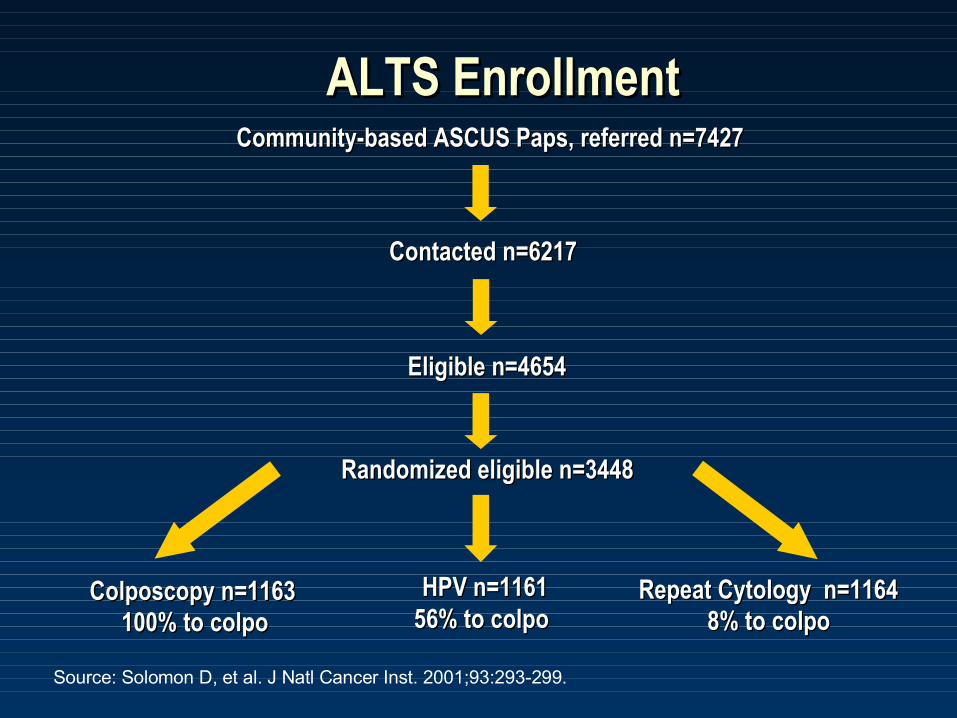
ALTS EnrollmentALTS EnrollmentCommunity-based ASCUS Paps, referred n=7427Community-based ASCUS Paps, referred n=7427
Contacted n=6217Contacted n=6217
Eligible n=4654Eligible n=4654
Randomized eligible n=3448Randomized eligible n=3448
Colposcopy n=1163Colposcopy n=1163 HPV n=1161HPV n=1161 Repeat Cytology n=1164Repeat Cytology n=1164 100% to colpo100% to colpo 56% to colpo56% to colpo 8% to colpo8% to colpo
Source: Solomon D, et al. J Natl Cancer Inst. 2001;93:293-299.
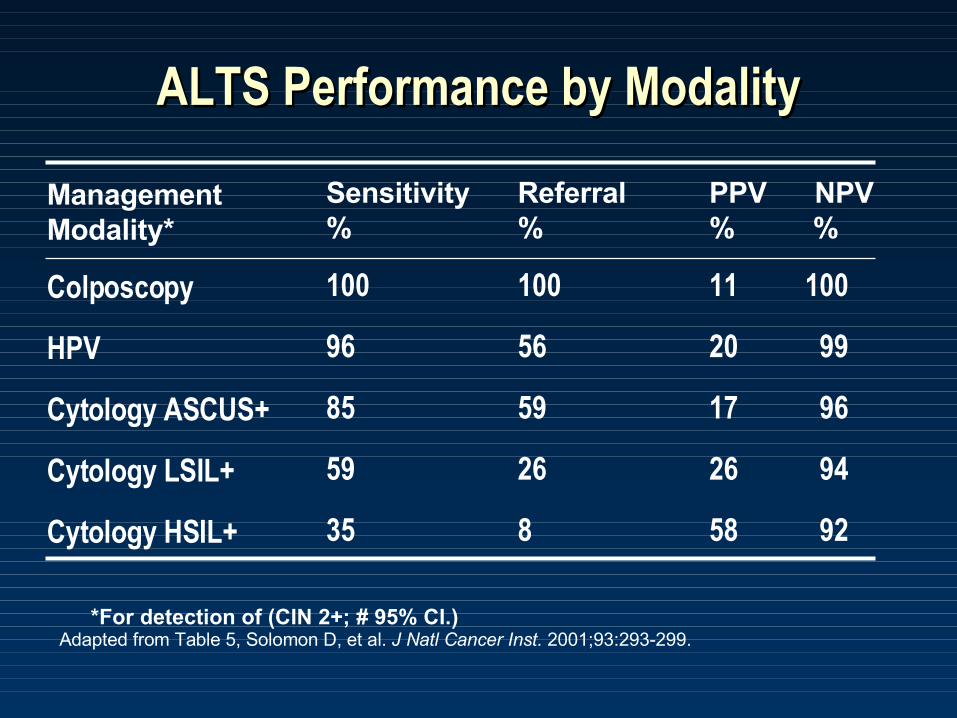
ALTS Performance by ModalityALTS Performance by Modality
ManagementModality*
Colposcopy
HPV
Cytology ASCUS+
Cytology LSIL+
Cytology HSIL+
Sensitivity Referral PPV NPV% % % %
100 100 11 100
96 56 20 99
85 59 17 96 59 26 26 94
35 8 58 92
*For detection of (CIN 2+; # 95% CI.)Adapted from Table 5, Solomon D, et al. J Natl Cancer Inst. 2001;93:293-299.
Summary of ALTS ResultsSummary of ALTS Results
• HPV testing detected 96% CIN 2/3+ with 56% HPV testing detected 96% CIN 2/3+ with 56% colposcopy referralcolposcopy referral
• Pap ASCUS+ detected 85% CIN 2/3+ with 59% Pap ASCUS+ detected 85% CIN 2/3+ with 59% colposcopy referralcolposcopy referral
• Pap HSIL+ or LSIL+ thresholds were specific but Pap HSIL+ or LSIL+ thresholds were specific but less sensitiveless sensitive
• Compared to colposcopy for all women HPV triage Compared to colposcopy for all women HPV triage by hc2 reduced unnecessary biopsies by 50% by hc2 reduced unnecessary biopsies by 50%
Source: Solomon D, et al. J Natl Cancer Inst. 2001;93:293-299.
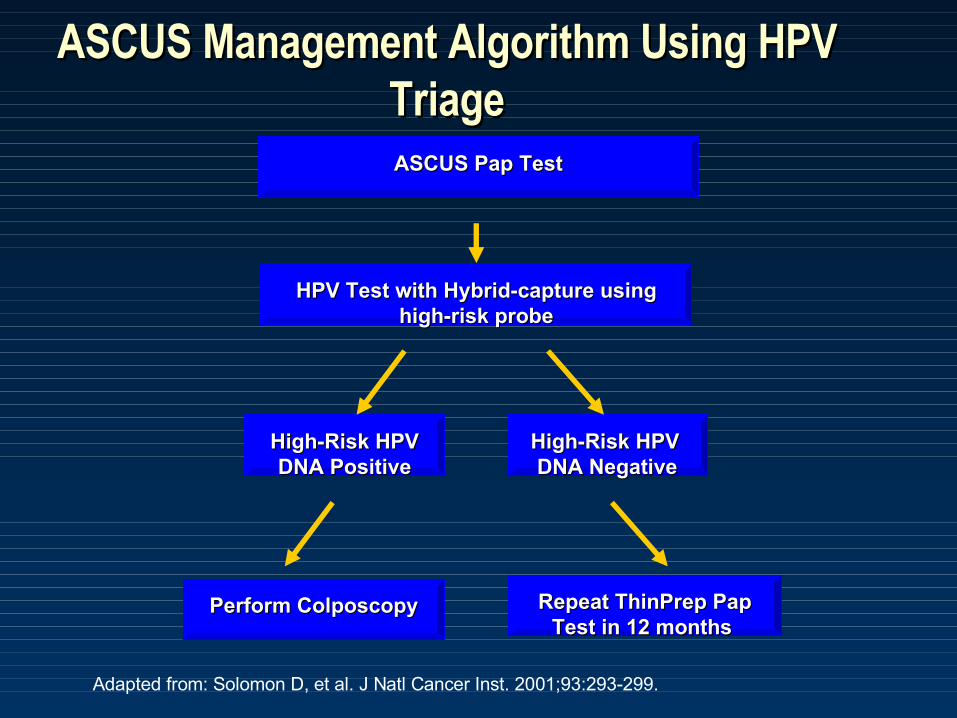
ASCUS Management Algorithm Using HPV ASCUS Management Algorithm Using HPV TriageTriageASCUS Pap TestASCUS Pap Test
Perform ColposcopyPerform Colposcopy Repeat ThinPrep Pap Repeat ThinPrep Pap Test in 12 months Test in 12 months
High-Risk HPV High-Risk HPV DNA PositiveDNA Positive
High-Risk HPV High-Risk HPV DNA NegativeDNA Negative
HPV Test with Hybrid-capture using HPV Test with Hybrid-capture using high-risk probehigh-risk probe
Adapted from: Solomon D, et al. J Natl Cancer Inst. 2001;93:293-299.
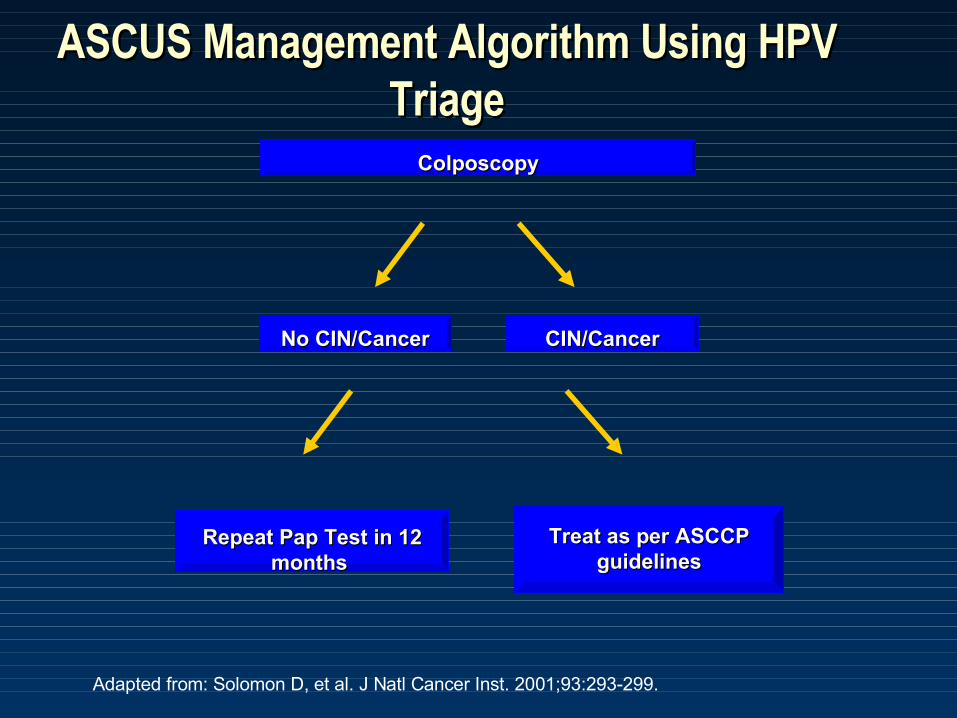
ASCUS Management Algorithm Using HPV ASCUS Management Algorithm Using HPV TriageTriage
ColposcopyColposcopy
Treat as per ASCCP Treat as per ASCCP guidelinesguidelines
Repeat Pap Test in 12 Repeat Pap Test in 12 months months
No CIN/CancerNo CIN/Cancer CIN/CancerCIN/Cancer
Adapted from: Solomon D, et al. J Natl Cancer Inst. 2001;93:293-299.
Triage of Postmenopausal Women with Triage of Postmenopausal Women with LGSIL CytologyLGSIL Cytology
• The prevalence of CIN 2,3 decreases with increasing ageThe prevalence of CIN 2,3 decreases with increasing age
• A cytological diagnosis of LGSIL is a less accurate predictor A cytological diagnosis of LGSIL is a less accurate predictor of HPV infection in postmenopausal womenof HPV infection in postmenopausal women
• ASCCP Consensus Guidelines ASCCP Consensus Guidelines – HPV DNA testing 12 months after a LGSIL Pap is an option for HPV DNA testing 12 months after a LGSIL Pap is an option for
selected postmenopausal womenselected postmenopausal women– Alternatively, reflex HPV testing of residual fluid medium from Alternatively, reflex HPV testing of residual fluid medium from
Thinprep could be performedThinprep could be performed– Should be reserved for postmenopausal women with history of Should be reserved for postmenopausal women with history of
adequate screening and no hx of CIN 2,3adequate screening and no hx of CIN 2,3

Triage of Adolescents with LGSIL CytologyTriage of Adolescents with LGSIL Cytology
• Cytologic abnormalities secondary to transient HPV Cytologic abnormalities secondary to transient HPV infections are quite commoninfections are quite common
• Clinically significant CIN III is rare and invasive disease Clinically significant CIN III is rare and invasive disease almost non-existentalmost non-existent
• 2001 ASCCP guidelines consider HPV testing at 12 months an 2001 ASCCP guidelines consider HPV testing at 12 months an option for initial management of LGSIL in adolescentsoption for initial management of LGSIL in adolescents
• Colposcopy reserved for HPV positive casesColposcopy reserved for HPV positive cases
• Other alternative to immediate colposcopyOther alternative to immediate colposcopy– repeat cytology at 6 and 12 months and colpo for ASC-US+repeat cytology at 6 and 12 months and colpo for ASC-US+
HPV DNA Testing in Post-Colposcopy HPV DNA Testing in Post-Colposcopy Follow-UpFollow-Up
• High-risk HPV testing at 12 months considered acceptable High-risk HPV testing at 12 months considered acceptable post-colposcopy follow-up forpost-colposcopy follow-up for– LGSIL with normal colposcopyLGSIL with normal colposcopy– Histologically confirmed CIN I if referral Pap Histologically confirmed CIN I if referral Pap < < LGSILLGSIL– ASC-H (after review of Pap, colpo directed biopsies)ASC-H (after review of Pap, colpo directed biopsies)– ASC-US with positive HPV screenASC-US with positive HPV screen
• Women HPV positive after 12 months should be referred back Women HPV positive after 12 months should be referred back to colposcopyto colposcopy
HPV DNA Testing in Post-Treatment Follow-HPV DNA Testing in Post-Treatment Follow-UpUp
• Risk of invasive cervical cancer following treatment for CIN is Risk of invasive cervical cancer following treatment for CIN is 5.8/1000 after 8 years of follow-up5.8/1000 after 8 years of follow-up11
• Limited data comparing post-treatment surveillance Limited data comparing post-treatment surveillance strategiesstrategies
• Several small studies show most women without Several small studies show most women without persistent/recurrent CIN become at least transiently HPV persistent/recurrent CIN become at least transiently HPV negativenegative
• HPV testing has a high negative predictive value for HPV testing has a high negative predictive value for persistent diseasepersistent disease
• Test should be performed no sooner than 6 months after Test should be performed no sooner than 6 months after treatment of CIN 2,3treatment of CIN 2,3
1. Soutter WP, et al. Lancet 1997
HPV DNA As An Adjunct To Cytology HPV DNA As An Adjunct To Cytology for Primary Screeningfor Primary Screening
HPV DNA Testing in Primary ScreeningHPV DNA Testing in Primary Screening
• HPV DNA testing may be added to cytology for screening of HPV DNA testing may be added to cytology for screening of women 30 years of age or olderwomen 30 years of age or older
• Combination screening should be discontinued at the same Combination screening should be discontinued at the same time and under the same circumstances as cytological time and under the same circumstances as cytological screeningscreening
• Not indicated for screeningNot indicated for screening– women < 30 years of agewomen < 30 years of age– immunosuppressed womenimmunosuppressed women– women s/p total hysterectomy for disease other than cervical cancer women s/p total hysterectomy for disease other than cervical cancer
or CISor CIS
HPV DNA Testing in Primary ScreeningHPV DNA Testing in Primary Screening
• Pap negative/HPV negative: do not rescreen before 3 yearsPap negative/HPV negative: do not rescreen before 3 years
• Pap negative/HPV positive: repeat double screen in 6-12 Pap negative/HPV positive: repeat double screen in 6-12 months. No colposcopy as initial managementmonths. No colposcopy as initial management
• Pap abnormal/HPV positive or negative: manage as per Pap abnormal/HPV positive or negative: manage as per ASCCP guidelines for management of abnormal Pap smearASCCP guidelines for management of abnormal Pap smear
ConclusionsConclusions
• HPV is the main etiologic agent of invasive cervical cancerHPV is the main etiologic agent of invasive cervical cancer
• The E7 and E6 HPV gene products play an integral role in The E7 and E6 HPV gene products play an integral role in carcinogenesis by inhibition of host tumor suppressor genescarcinogenesis by inhibition of host tumor suppressor genes
• HPV testing is clinically useful in HPV testing is clinically useful in – the triage of patients with equivocal pap smear resultsthe triage of patients with equivocal pap smear results– triage of postmenopausal women and adolescents with LGSIL Pap triage of postmenopausal women and adolescents with LGSIL Pap
smearssmears– post treatment surveillance for CIN II/IIIpost treatment surveillance for CIN II/III– primary screening of women > 30 years of ageprimary screening of women > 30 years of age– screening for prophylactic vaccine eligibility?screening for prophylactic vaccine eligibility?


















