
Accelerating Clinical Transformation Using Community Collaboration Tools
Upload
medsphereCategory
view
2.689download
2description
Clinical Transformation, Part II
March 2009 Community Call
Presenters
• Edmund Billings, MD - CMO
• Jeff Parker, RN, BsBA - Clinical Informatics Manager
• Janine Powell - Sr. Director of Client Services
• Debbie Daspit - Director of Product Management
• George Lilly - CCD/CCR Developer
• Adam Waterbury - GT.M Product Manager
• Ben Mehling - Director of Ecosystem Operations
Agenda
• Clinical Transformation– A Blueprint
– In Practice
• Transformation Working Group Update– Status Update
– Framework for Planning
– Discussion
• Open Project Updates– OpenVista/GT.M Integration
– CCD-CCR Project
• Medsphere.org: Tip of the Month
Clinical Transformation, a Blueprint5 Million Lives Project Example: The Central Line Bundle
Edmund Billings, MD

5
http://www.ihi.org/IHI/Programs/Campaign/
Central Line
6

Central Line: Subclavian
7
Preventing Catheter-Related Bloodstream Infections
• Central venous catheters (CVCs) are being used increasingly in the inpatient and outpatient setting to provide long-term venous access.
• CVCs disrupt the integrity of the skin, making infection with bacteria and/or fungi possible.
• Infection may spread to the bloodstream and hemodynamic changes and organ dysfunction (severe sepsis) may ensue, possibly leading to death.
• Approximately 90% of the catheter-related bloodstream infections (CR-BSIs) occur with CVCs.
8

Preventing Catheter-Related Bloodstream Infections
• 48% of intensive care unit (ICU) patients have central venous catheters, accounting for about 15,000,000 central-venous-catheter-days per year in ICUs.
• Approximately 5.3 central line infections occur per 1,000 catheter days in ICUs.
• The attributable mortality for such central line infections is approximately 18%.
• Thus, probably about 14,000 deaths occur annually due to central line infections. Some estimates put this figure as high as 28,000 deaths per year.
• In addition, nosocomial bloodstream infections prolong hospitalization by a mean of 7 days. Estimates of attributable cost per bloodstream infection are estimated to be between $3,700 and $29,000.
9
References
1. Mermel LA. Prevention of intravascular catheter-related infections. Ann Intern Med. 2000;132(5):391-402.
2. Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1994;271:1598-1601.
3. Saint S. Chapter 16. Prevention of intravascular catheter-related infection. Making health care safer: a critical analysis of patient safety practices. AHRQ evidence report, number 43, July 20, 2001. Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014-2020.
4. Soufir L, Timsit JF, Mahe C, Carlet J, Regnier B, Chevret S. Attributable morbidity and mortality of catheter-related septicemia in critically ill patients: a matched, risk-adjusted, cohort study. Infect Control Hosp Epidemiol. 1999;20(6):396-401.
10

Care Bundles
• Care bundles, in general, are groupings of best practices with respect to a when applied together result in substantially greater improvement. The science supporting each bundle component is sufficiently established to be considered the standard of care.
• Evidence-based interventions result in better outcomes than when implemented individually.
11
Central Line Bundle
12
Central Line Bundle
The central line bundle has five key components:
1. Hand hygiene
2. Maximal barrier precautions
3. Chlorhexidine skin antisepsis
4. Optimal catheter site selection, with subclavian vein as the preferred site for non-tunneled catheters
5. Daily review of line necessity, with prompt removal of unnecessary lines
• Compliance with the central line bundle can be measured by simple assessment of the completion of each item.
• The approach has been most successful when all elements are executed together, an “all or none” strategy.
13
Central Line Bundle
14

Central Line Bundle Results
Berenholtz SM, Pronovost PJ, Lipset PA, et al. Eliminating catheter-related bloodstream
infection in the intensive care unit. Critical Care Medicine. 2004;32:2014-2020.
15
Model for Improvement
The model has two parts:
1. Three fundamental questions that guide improvement teams to
1. Set clear aims,
2. Establish measures that will tell if changes are leading to improvement
3. identify changes that are likely to lead to improvement.
2. The Plan-Do-Study-Act (PDSA) cycle to conduct small-scale tests of change in real work settings — by planning a test, trying it, observing the results, and acting on what is learned. This is the scientific method, used for action-oriented learning.
16
Model for Improvement
• Implementation: After testing a change on a small scale, learning from each test, and refining the change through several PDSA cycles, the team can implement the change on a broader scale — for example, test medication reconciliation on admissions first.
• Spread: After successful implementation of a change or package of changes for a pilot population or an entire unit, the team can spread the changes to other parts of the organization or to other organizations.
Model for Improvement on www.IHI.org
17

Get Started
1. Select the team and the venue. It is often best to start in one ICU. Many hospitals will have only one ICU, making the choice easier.
2. Assess where you stand presently. What precautions are taken presently when placing lines? Is there a process in place? If so, work with staff to begin preparing for changes.
3. Contact the infectious diseases/infection control department. Learn about your catheter-related bloodstream infection rate and how frequently the hospital reports it to regulatory agencies.
4. Organize an educational program. Teaching the core principles to the ICU staff will open many people’s minds to the process of change.
5. Introduce the central line bundle to the staff.
18
Metrics
Rate
Total no. of CR-BSI cases
No. of catheter days
Compliance
# with ALL 5 elements of central line bundle
# with CVCs on the day of the sample
Track and Scoreboard Overtime
Rate & Compliance
19
x 1000 = CR-BSI per 1000 catheter days
= reliability of compliance

Track Overtime: Rate & Compliance
20
Automation Helps Knockdown Barriers
1. Fear of change
– “It works and its proven”
– It’s the reason to use the system
2. Communication breakdown
– “Its built in”
– The system supports compliance
3. Physician and staff “partial buy-in”
– “I thought I was doing better than that”
– Measuring performance is compelling
21
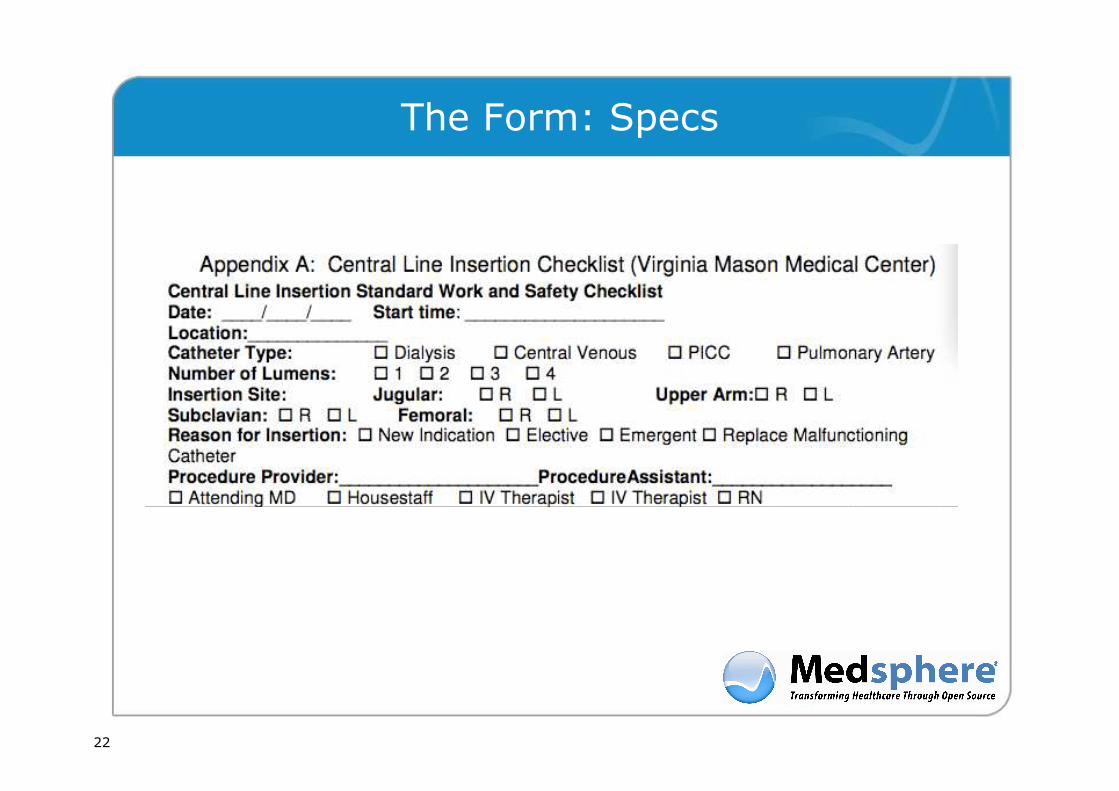
The Form: Specs
22

The Form: Prep
23

The Form: During
24

The Form: After
25

Ongoing Daily Review
• Daily review for necessity and prompt removal of unnecessary lines:
• The ICU patient with a central line will be reviewed daily, with a notation on the daily goals sheet or medical record indicating the continued need for the central line.
• Routine replacement should be avoided, and all lines should be removed as early as possible.
26

Clinical Transformation, in Practice
Jeff Parker, Midland Memorial Hospital
Outcomes
• Central line days in ICCU averaged over the past year = 178 month.
• We have scored 100% on bundle compliant forms.
• We use maximum barrier kits.
Quality Improvement: Order Sets
• Using the in place order sets, the physician with a mere click or two can order all the necessary orders for central line placement – including X-rays for placement, flushes, with an order that staff can start using when placement is confirmed. In the old days, we would have to call the physician as most did not write the orders out in the detail we have with the electronic record.
Quality Improvement: Chart Availability
• Radiology immediately can view the order and can check the patients record for a signed consent, what the H&P shows, and the patients overall medical condition prior to them ever actually seeing the patient.
• The physician can view the X-ray immediately from any location within the hospital, from his home or office.

Quality Improvement: Efficiency
• Often, the chest X-ray is done within minutes of inserting the central line, allowing the use of the central line to be started much more quickly than was previously possible –which could be a crucial five minutes if it’s a unit patient.

Quality Improvement: Measuring and Compliance
• The electronic record has made it possible to easily audit charts and monitor for central line compliance.

Transformation Working Group
Janine Powell & Debbie Daspit

Community Collaboration
• Organized Collaboration - Just getting started..– Work as a Group
– Divide and Conquer option
• Collaboration Dependences – Values
– Interpretation
– Understanding
– Workflow
– Distribution of information
• Framework as a collaboration path to design and document and distribute strategies and content – Core Measure Reporting
– “Never Event” Prevention
– Performance Improvement
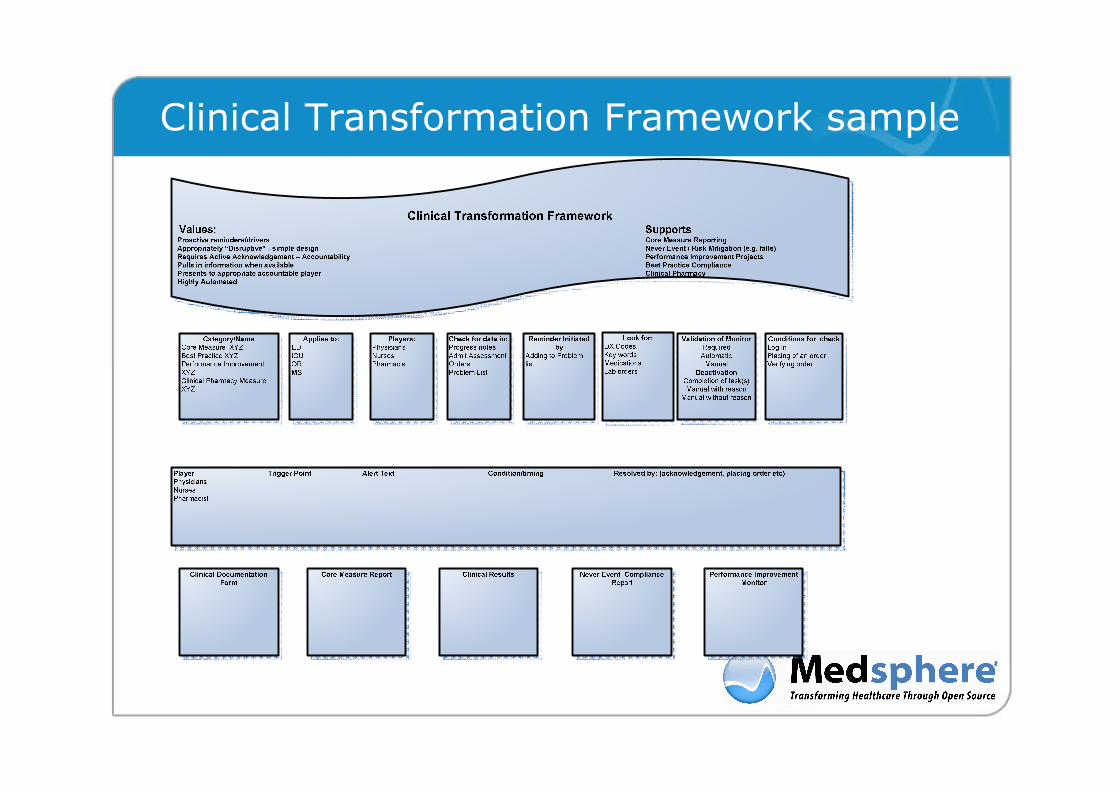
Clinical Transformation Framework sample
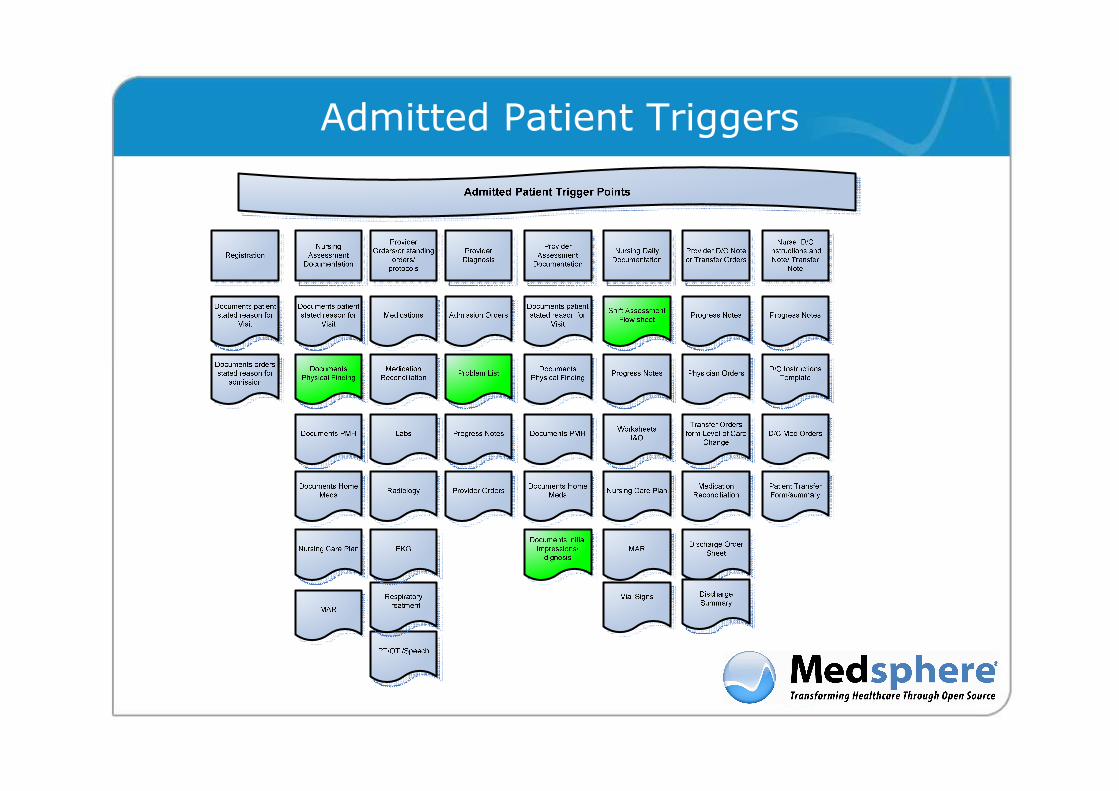
Admitted Patient Triggers
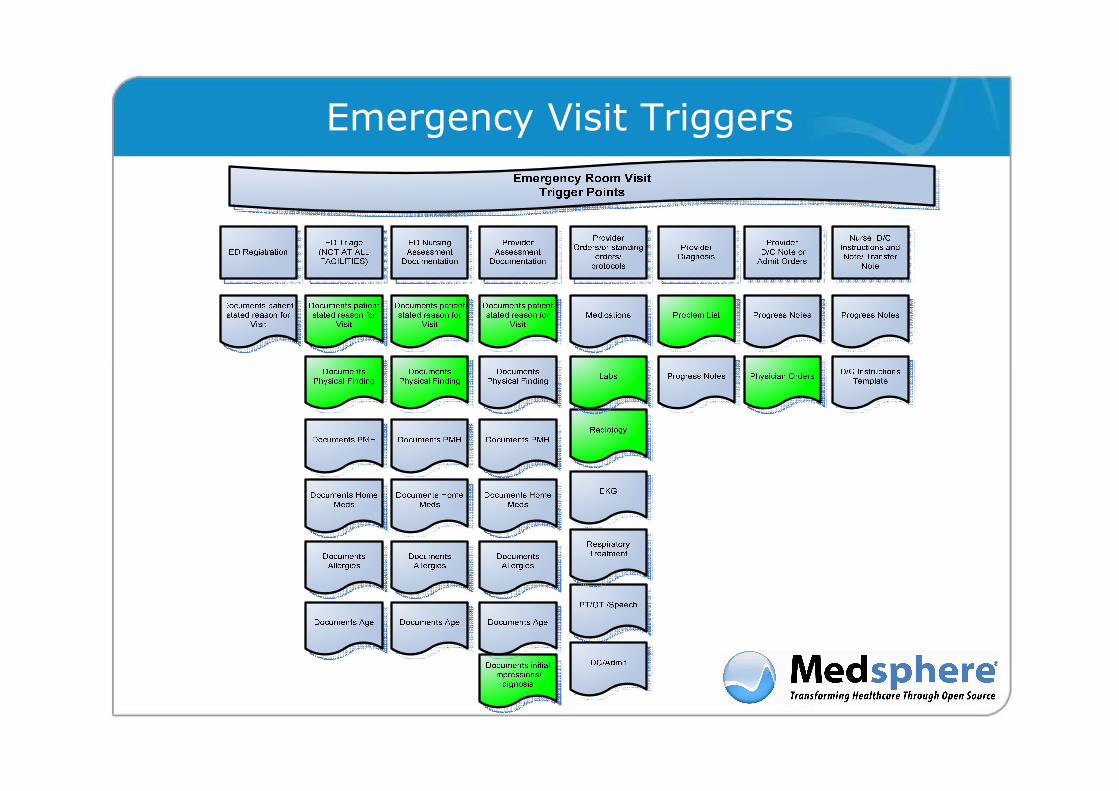
Emergency Visit Triggers

Orders/Standing Orders Triggers

Design and Documentation Example

Open Development Projects
George Lilly & Fay Struble
Adam Waterbury

OpenVista/GT.M Integration Project
Adam Waterbury
Get Involved
� Code is available on Launchpad
� Not production ready; for developers only
� Bugs are in Launchpad
� You can help!
� File a bug
� Comment on a bug with suggestions
� Create a branch and fix a bug yourself
� Not sure how to get started?
� Post on Medsphere.org with your interests; we'll find something for you!

Opensource CCR and CCD supportfor VistA based systems
Project Update
March 26, 2009by
George [email protected]
* This project has been funded in part with Federal funds from the National Institutes of Health, under Contract No. H HSN268200425212C, “Re-engineering the Clinical Research Enterprise".

CollaboratorsOrganizations
WorldVista
HP
KRM
Medsphere
Robert Morris University
Sequence Managers
University of Minnesota
Individuals
� George Lilly
� Christopher Anderson
� Nancy Anthracite
� Lee Castonguay
� Duane DeCorteau
� Emory Fry
� Sam Habiel
� Jose Lacal
� John McCormack
� Ben Mehling
� Dennis Menor
� Ken Miller
� Kevin Peterson
� Mike Schendel
� Fay Strubel
� Thomas Sullivan
� Chris Uyehara
� David Whitten
� Greg Woodhouse
� JohnLeo Zimmer

Topics
� Definition
� Purpose
� Snapshot
� Highlight
� Contributors

Definition: The Continuity of Care Record (CCR) is a machine readable and human readable ASTM XML standard data set of a person's clinical status

The CCR dataset has many intended purposes including the exchange of medical records, synchronization with clinical repositories, and the transformation into clinical messages
Exchange of medical records:� Between two EHR systems (VistA<->VistA and VistA<->O ther) �
� With a Personal Health Record (PHR) – like Google He alth or MS HealthVault
Synchronization with clinical repositories:� For clinical decision support � For research and clinical trials – as with the Elect ronic
Primary Care Research Network (ePCRN) �
Transformation into clinical messages� XSLT transformation into a Continuity of Care Docum ent (CCD) �
� For use the the National Health Information Network (NHIN) �� For CCHIT Certification� For HIPAA Claims Attachments
� Transformation into XML Web Service messages for eP rescribing

CCR/CCD PROJECT SNAPSHOT 3/26/2009
Payers
Advance Directives
Support
Functional Status
Problems
Alerts/Allergies
Lab Results
Medications
Family History
Medical Equipment
Immunizations
Procedures
Encounters
Plan of Care
Recent Change
Vital Signs
Social History
Actors
Export
TestingPlanned In ProductionIn DevelopmentLegend
Import (Accessioning)�Alerts/Allergies
Medication Advisories(ePrescribing)�
OpenVistA WorldVistAEHR FOIA VistA RPMS
GTM GTM
GTM
Cache
GTM
Cache
Fileman CCR Elements
MUMPS Temporary Globals
CCRTemplate
CCRProcessor
File WebService
XPath Library
Template File
Template Import
Parameters
Lab Date Limits
Meds Date Limits
Vitals Date Limits
PicklistProcessing
BatchProccessing
XML RPC Variables RPC
Checksums
CCD Transformation
ePrescription XMLSupport
FilemanMenu
Options
Fileman Parameters
ePCRNConnection
Codes

Recently, we demonstrated the transformation of our CCRs into level 2 CCDs thanks to an XSLT transformation contributed by Ken Miller

Medsphere.org Tip of the Month
Ben Mehling

Start a new Blog Post

Create a Personal Blog

Setup your Blog
Write a new post

Medsphere.org Blogs



















