
Clinical Study Validation and Test-Retest Reliability...
12
Clinical Study Validation and Test-Retest Reliability of New Thermographic Technique Called Thermovision Technique of Dry Needling for Gluteus Minimus Trigger Points in Sciatica Subjects and TrPs-Negative Healthy Volunteers Elhbieta Skorupska, 1 MichaB Rychlik, 2 and WBodzimierz Samborski 1 1 Department of Rheumatology and Rehabilitation, Poznan University of Medical Sciences, Fredry 10, 61-701 Poznan, Poland 2 Department of Virtual Engineering, Poznan University of Technology, Plac Marii Skłodowskiej-Curie 5, 60-965 Poznan, Poland Correspondence should be addressed to El˙ zbieta Skorupska; [email protected] Received 19 December 2014; Revised 9 May 2015; Accepted 26 May 2015 Academic Editor: Matteo Paci Copyright © 2015 El˙ zbieta Skorupska et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. e aim of this study was to assess the validity and test-retest reliability of ermovision Technique of Dry Needling (TTDN) for the gluteus minimus muscle. TTDN is a new thermography approach used to support trigger points (TrPs) diagnostic criteria by presence of short-term vasomotor reactions occurring in the area where TrPs refer pain. Method. irty chronic sciatica patients (n = 15 TrP-positive and n = 15 TrPs-negative) and 15 healthy volunteers were evaluated by TTDN three times during two consecutive days based on TrPs of the gluteus minimus muscle confirmed additionally by referred pain presence. TTDN employs average temperature (T avr ), maximum temperature (T max ), low/high isothermal-area, and autonomic referred pain phenomenon (AURP) that reflects vasodilatation/vasoconstriction. Validity and test-retest reliability were assessed concurrently. Results. Two components of TTDN validity and reliability, T avr and AURP, had almost perfect agreement according to (e.g., thigh: 0.880 and 0.938; calf: 0.902 and 0.956, resp.). e sensitivity for T avr , T max , AURP, and high isothermal-area was 100% for everyone, but specificity of 100% was for T avr and AURP only. Conclusion. TTDN is a valid and reliable method for T avr and AURP measurement to support TrPs diagnostic criteria for the gluteus minimus muscle when digitally evoked referred pain pattern is present. 1. Introduction e main problem of the pain research filed is the difficulty with an objective quantification of pain. Most authorities agree that a fair amount of pain is leſt undertreated, especially in the chronic form [1]. It has been estimated that in around 30% of patients consulting for pain in primary care the coexistence of myofascial pain syndrome (MPS) caused by trigger points (TrPs) was confirmed [2]. Unfortunately, this MPS is drug-resistant and very oſten diagnostically overlooked. Nevertheless, a grown interest in MPS has been lastly observed and the main controversy around pain studies, namely, an objective confirmation of TrPs presence, is again the main research theme. Two new methods, sonoelastogra- phy and magnetic resonance elastography, have been recently introduced allowing noninvasive imaging of TrPs [3, 4]. Both are not cheap or easily accessible; thus, TrP confirmation is still based on palpatory diagnostic criteria defined by Travell and Simons [5, 6]. Interestingly, for years MPS has been defined as nocicep- tive pain, but today the importance of sympathetic nervous system (SNS) activity for MPS pain propagation is indicated more and more frequently [7–9]. Vasomotor responses and hyperalgesia observed in the area of TrPs related referred pain can be also attributed to possible sympathetic mechanism [10–14]. is supports the last point of Simons’ integrated Hindawi Publishing Corporation BioMed Research International Volume 2015, Article ID 546497, 11 pages http://dx.doi.org/10.1155/2015/546497
Transcript of Clinical Study Validation and Test-Retest Reliability...

Clinical StudyValidation and Test-Retest Reliability ofNew Thermographic Technique Called Thermovision Techniqueof Dry Needling for Gluteus Minimus Trigger Points in SciaticaSubjects and TrPs-Negative Healthy Volunteers
Elhbieta Skorupska1 MichaB Rychlik2 and WBodzimierz Samborski1
1Department of Rheumatology and Rehabilitation Poznan University of Medical Sciences Fredry 10 61-701 Poznan Poland2Department of Virtual Engineering Poznan University of Technology Plac Marii Skłodowskiej-Curie 5 60-965 Poznan Poland
Correspondence should be addressed to Elzbieta Skorupska skorupskaumpedupl
Received 19 December 2014 Revised 9 May 2015 Accepted 26 May 2015
Academic Editor Matteo Paci
Copyright copy 2015 Elzbieta Skorupska et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
The aim of this study was to assess the validity and test-retest reliability of Thermovision Technique of Dry Needling (TTDN) forthe gluteus minimus muscle TTDN is a new thermography approach used to support trigger points (TrPs) diagnostic criteria bypresence of short-term vasomotor reactions occurring in the area where TrPs refer painMethodThirty chronic sciatica patients (n= 15 TrP-positive and n = 15 TrPs-negative) and 15 healthy volunteers were evaluated by TTDN three times during two consecutivedays based on TrPs of the gluteus minimus muscle confirmed additionally by referred pain presence TTDN employs averagetemperature (Tavr) maximum temperature (Tmax) lowhigh isothermal-area and autonomic referred pain phenomenon (AURP)that reflects vasodilatationvasoconstriction Validity and test-retest reliability were assessed concurrentlyResults Two componentsof TTDN validity and reliability Tavr and AURP had almost perfect agreement according to 120581 (eg thigh 0880 and 0938 calf0902 and 0956 resp) The sensitivity for Tavr Tmax AURP and high isothermal-area was 100 for everyone but specificity of100 was for Tavr and AURP only Conclusion TTDN is a valid and reliable method for Tavr and AURP measurement to supportTrPs diagnostic criteria for the gluteus minimus muscle when digitally evoked referred pain pattern is present
1 Introduction
The main problem of the pain research filed is the difficultywith an objective quantification of pain Most authoritiesagree that a fair amount of pain is left undertreated especiallyin the chronic form [1] It has been estimated that inaround 30 of patients consulting for pain in primary carethe coexistence of myofascial pain syndrome (MPS) causedby trigger points (TrPs) was confirmed [2] Unfortunatelythis MPS is drug-resistant and very often diagnosticallyoverlooked Nevertheless a grown interest in MPS has beenlastly observed and themain controversy aroundpain studiesnamely an objective confirmation of TrPs presence is again
the main research theme Two new methods sonoelastogra-phy andmagnetic resonance elastography have been recentlyintroduced allowing noninvasive imaging of TrPs [3 4] Bothare not cheap or easily accessible thus TrP confirmation isstill based on palpatory diagnostic criteria defined by Travelland Simons [5 6]
Interestingly for years MPS has been defined as nocicep-tive pain but today the importance of sympathetic nervoussystem (SNS) activity for MPS pain propagation is indicatedmore and more frequently [7ndash9] Vasomotor responses andhyperalgesia observed in the area of TrPs related referred paincan be also attributed to possible sympathetic mechanism[10ndash14] This supports the last point of Simonsrsquo integrated
Hindawi Publishing CorporationBioMed Research InternationalVolume 2015 Article ID 546497 11 pageshttpdxdoiorg1011552015546497
2 BioMed Research International
hypothesis concerning TrPs etiology which states that auto-nomic modulation has a potential influence on the increaseof ACh release which can aggravate symptoms caused byTrPs [15] It is commonly accepted that infrared thermovision(IRT) camera can objectively support the diagnosis of painpatients especially when SNS activity is involved [16] HighIRT reliability for muscle examination [17 18] and significantcorrelation between pressure pain threshold and temperaturedifferences inMPS have been recently proved [19] Moreovera new idea for pain medicine studies is a stress loading IRTtest for example by coldwarm stress exercise pharmaco-logical stress vibration and visual stimulation Enhancedsensitivity and specificity for the diagnosis of SNS relateddiseases for example CRPS by cold stress thermographyhas been recommended Unfortunately it causes pain in thepatient and no standardized guidelines for the stress load-ing test have been established [20ndash22] Additionally someauthors claim that IRTwith its temperaturemeasurement andvisual thermogram analysis is not sufficient as a diagnostictool in medicine as it needs to provide thermogram analysismore objectively [16] Interestingly the new awardedmethodcalled Thermovision Technique of Dry Needling (TTDN)allows measuring changes of isothermal-area size (everythermogram can be divided into subareas of 07∘C each) [23]Additionally for TrPs-positive subjects TTDN can measureintensive short-term vasomotor response related to noxiousstimulation of TrPs alone If everyTrP can provoke vasomotorresponse TTDN can objectively support Travell and SimonsrsquoTrPs diagnostic criteria
For the purposes of the study trigger points of thegluteusminimusmuscle were considered because of themostintensive and longest referred pain pattern which spreadsalmost in the whole lower limb [5 6]Thus thismuscle seemsto be the best choice for TTDN validation conducted for thefirst time According to the literature trigger points withinthe gluteusminimusmuscle can be observed among radicularsciatica patients as secondary symptoms due to disc lesion orcan provoke sciatic-like pain pseudoradicular pain [26 27]Objective distinction of radicular and nonradicular sciaticpain is not possible Based on the literature a patient whopresents for example the lack of positive Lasegue test resultaccompanied by the lack of neurological signs of sciatic nerveirritation should be diagnosed as pseudosciatica or sciatic-like pain However Rolke posited that pseudoradicular andradicular low back pain should be considered to be diseasecontinuum rather than different entities [28]
The coexistence of gluteus minimus TrPs in around30 of subacute and chronic radicular sciatica patientswas proved [10 11] as well as the presence of active TrPsamong sciatica-like cases [12 13] Based on some previousstudies it can be hypothesized that the presence of short-termvasomotor changes in the area where TrPs provoke pain mayenable objective trigger points confirmation Whether thecommonly used palpatory criteria are reliable is controversialThus it is very important to find an objective and easy tool forTrPs confirmation
The main aim of this study was to validate Thermovi-sion Technique of Dry Needling (TTDN) and examine itstest-retest reliability for the gluteus minimus muscle The
additional aim was to analyze the average value of TTDNcomponents in the light of clinical division
2 Material and Method
The study was conducted in accordance with the DeclarationofHelsinki approved by the EthicsCommittee of PoznanUni-versity of Medical Sciences (number 77214) It was prospec-tively registered at the AustralianNewZealandClinical TrialsRegistry (ACTRN12614001168640) All subjects gave writteninformed consent to participate in the study before datacollection A detailed description of all examinations andtreatment procedures including dry needling (DN) aswell asof risks involved in the studywas provided to the participantsParticipants had the right to refuse the DN treatment andwithdraw from the study at any time without penalty
21 Subjects Thirty Caucasian chronic sciatica subjectswhere half of themwere TrPs-positive and half TrPs-negativeand fifteen Caucasian healthy volunteers were recruited tothe study from Poznan GP doctors the University PainClinic by press announcement and University staff The ageranged from 35 to 58 years (average 466 plusmn 87 y) Sciat-ica subjects were diagnosed by an experienced neurologisttowards radicular origin of sciatica on the basis of bedsideexamination extensive neurological screening examinationaccompanied by a positive straight leg test and magneticresonance imaging results
Clinical Criteria for Gluteus Minimus Muscle TrPs Confirma-tion According to Travell and Simons the taut band (oneof the essential criteria) is unlikely to be palpated because itlies deeper than both the gluteus maximus and the gluteusmediusmusclesHowever TrPs spot tenderness can be clearlylocalized Additionally the referred pain pattern is morelikely to be observed when needle encounters TrPs ratherthan when sustained pressure on the tender spot is applied[5 6]
The diagnosis of TrPs within the gluteus minimus musclein the present study was based on Travell and Simonsrsquoclinical criteria [5 6] However due to the lack of the tautband of the gluteus minimus muscle the presence of theconfirmatory sign (referred pain pattern) was added to thefull range of possible essential criteria for strong evidenceActive trigger points within gluteusminimus were confirmedif spot tenderness pain recognition and limited range ofmovement were confirmed and the full referred pain patternfelt in the thigh and calf was present (evoked by snappingpalpation)
Key Inclusion Criteria Key inclusion criteria for sciaticapatients were as follows age between 30 and 60 (inclusive)both lower limbs present pain durationgt3monthsgt3 on the1ndash10-point VAS scale of leg pain with this being the dominantpain problem and pain felt minimum to the calf and theresults of the straight leg test between 30 and 60 degrees
Key inclusion criteria for healthy volunteers were generalgood health condition age between 30 and 60 (inclusive)
BioMed Research International 3
both lower limbs present and lack of latent trigger pointswithin the gluteus minimus muscle
Key Exclusion Criteria Subjects were excluded owing tocomplex regional pain syndrome cauda equina syndromeprevious back surgery spinal tumors scoliosis pregnancycoagulant treatment disseminated intravascular coagulationdiabetes epilepsy infection inflammatory rheumatologicdiseases stroke or oncological history
22 Methods All patients recruited to the study were consec-utively examined using TTDN (detailed description below)Also side-to-side IRT comparison of the lower limbs wasperformed
The IRT camera operator was not aware of the results ofgluteus minimus TrPs examination and the physician whoperformed dry needling was not aware of the IRT resultsduring the procedure TTDN was performed three timesduring two consecutive days On the first day TTDN wasperformed once and on the second two sessions with one-hour break were performed for the same marked pointsA thermovision touchless camera (NEC-AVIO TVS-200EX)with a 8ndash14 120583m wave band temperature resolution betterthan 0080∘C and sensitivity of 80mK and working in realtime was applied The camera was equipped with a high-speed (60Hz) uncooled FPA 320 times 240 (119867 times 119881) pixelsVOx (vanadium oxide) microbolometer For thermal imagesanalysis the specialist program ldquoThermography Studio 2007Professionalrdquo was used Every day before the procedure everyparticipant was reexamined towards active gluteus minimusTrPs Then the localization of the two most active TrPswas marked For non-TrPs sciatica subjects and healthyvolunteers two nontender points were marked The dryneedling specialist had no knowledge of whether the markedpoints were TrPs or non-TrPs
221 General Protocol for TTDN TTDN result is thought tobe positive if significant 119879sk (maximum and average temper-ature) changes accompanied by significant isothermal-areachanges in the area of pain are confirmed Isothermal-areais defined as an area of the patientrsquos body with the sametemperature at the samemoment of timeThe TTDNmethodwas partially described in the authorsrsquo previous studies [1011]
(a) Statement Thermographic images were recorded by anexpert following a standard protocol recommended by theAcademy of Neuromuscular Thermography The expert alsoevaluated the images [24] Patients were instructed to avoidphysiotherapy and manual therapy 24 hours prior to thetest and to avoid using nasal decongestants analgesicsanti-inflammatory drugs or any substances affecting thesympathetic functionThey were also instructed not to drinkcoffee or alcohol and to refrain from smoking 2 hours beforethe recording
To obtain the stability of the patientrsquos body temperatureand to ensure the adjustment of the recording camerarsquostemperature to the interior conditions the evaluation began30 minutes after the patient had entered the examination
room Thermal isolation of the evaluated area from otherthermal factors that might have influenced the evaluationincluding other parts of the patientrsquos and doctorrsquos bodies wasensured Moreover when performing thermovision imagingthe general rules of camera usage were followed
(b) Patient Preparation Consider the following
(1) Drawing pain on the pain diagramSide-to-side comparison of the painful area by IRTwas as follows
(a) Comparison of 119879sk differences in the painful legversus the opposite side
(b) When a 119879sk decrease of more than 05∘C in thepainful area compared to nonpainful leg wasobserved then the feature of neuropathic painwas considered possible
(2) Positioning the patient according to dry needlingrules for the examined muscle In this positionthermovision images of the patient were recordedFor adequate representation of dimensions a cali-bration standard was applied The next step involvedrecording the ldquobaserdquo image The image was recordedto establish the initial level of the patientrsquos temperatureparameters
(3) When the above-mentioned conditions weremet dryneedling under IRT control was performed
(c) Dry Needling (DN) Session under IRT Control Dryneedling of every point lasted for 5 minutes During thewhole procedure the subarea of referred pain reported bythe patient was recorded After the needling of both markedpoints was completed further thermovision imaging wasperformed The IRT observation lasted for six consecutiveminutes after DN At the end of the procedure the patientswere asked to answer the question ldquoWas the pain evoked byneedling similar to your daily painrdquo
(d) Thermogram Analysis
Skin Temperature Changes The analysis of thermogramsassumed skin temperature changes maximum temperature(119879max) minimum temperature (119879min) and average tempera-ture (119879avr) in the observed area after the dry needling sessionand during 6 minutes after DN
Analysis of the Impact of Vasomotor Reactions Presence onthe Referred Pain The expected vasomotor changes in thearea of TrPs related referred pain were named autonomicreferred pain (AuRP) if present (Table 1) Post-DN andpostobservation analysis assumed the calculation (in cm2) ofskin isothermal-area changes with the reference point being119879max at rest for AURP-vasodilatation and 119879min at rest for AURP-vasoconstriction from the thermogram at rest Additionallythe size of high 119879sk isothermal-area (15∘C below 119879max at rest)and low 119879sk isothermal-area (15∘C above 119879min at rest) was
4 BioMed Research International
Table 1 Isothermal-area analysis related to TTDN
Initial state After DN After observation
119879min at restIf isothermal-area decreases below 119879min at restmdashthe confirmation of AuRP (vasoconstriction)
Low Tsk isothermal-area (15∘C above 119879min at rest)
119879max at restHigh Tsk isothermal-area (15∘C below 119879max at rest)
If isothermal-area increases above 119879max at restmdashthe confirmation of AuRP (vasodilatation)
Table 2 Definitions of validity elements [24 25]
Validity elements Definition EquationSensitivity Proportion of the positive values that the test correctly identifies 119886 (119886 + 119888) times 100Specificity Proportion of the negative values that the test correctly identifies 119886 (119887 + 119889) times 100Positive predictive value (PPV) Proportion of the patients with positive test results who are correctly diagnosed 119886 (119886 + 119887) times 100Negative predictive value (PNV) Proportion of the patients with negative test results who are correctly diagnosed 119889 (119888 + 119889) times 100
calculated The size of each isothermal-area was recalculatedfrom cm2 to the percentage value
TTDN for Gluteus Minimus Trigger PointsmdashAdditional Infor-mationThe area to be observed by IRTwas chosen accordingto the gluteus minimus referred pain pattern The examinedpatients were positioned on the side on the uninvolvedextremity with the hip and knee flexed The muscle wasneedled with flat palpation perpendicular to the musclealong the counter of the iliac crest Strong depression ofthe subcutaneous tissue was applied in order to reduce thedistance of the skin from the muscle Depth of penetrationdepended on the amount of adipose tissue [25] Therapeuticneedling was performed with 030mm diameter 60mm longsterile acupuncture needles SE L (Serin Corp ShizuokaJapan) Each needle was packed separately
23 Statistical Analysis
TTDN Results Dependent on Clinical Division The chronicsciatica subjects and healthy volunteers were compared withtrigger points coexistence being the differentiating criterionFor the strong evidence of data presented the significancelevel was set based on exact tests not on the default asymp-totic method Exact two-way Mann-Whitney 119880 tests wereperformed in order to ensure that data were representativeof the whole population of possible data values Tests wereapplied to compare the differences for maximum minimumand average skin temperatures and the percentage size ofisothermal-area for the state after dry needling and secondlyfor the postobservation state Values figures and tables inthe text were expressed as plusmn standard error of the mean (SE)Significance level was set at 119901 lt 005 IBM SPSS Statisticsversion 2010158401015840 was used
Validity and Reliability of TTDN A validity analysis wasperformed to confirm the validity of TTDN towards sensitiv-ity and specificity of the obtained results (skin temperaturechanges and percentage size of vasomotor responses) Thecomponents of validity that were used in this study includesensitivity and specificity as well as positive and negative
predictive values Tables 2 and 3 provide definitions andexplanations for the components of validity [30 31]
Reliability of the TTDN Method Test-retest was used tocheck the reliability of TTDN according to the Guidelinesfor Evaluating and Expressing the Uncertainty of NISTMeasurement Results TTDN was performed using the sameexperimental tools the same observer the same measur-ing instrument used under the same conditions the samelocation and repetition over a short period of time on thesame patient Intraclass correlation coefficients (ICC) for test-retest reliability (intraobserved variability) were calculatedto illustrate the differences between repeated measures [29]Intraclass correlation coefficients above 090 were consideredexcellent values form 075 to 090 were considered good andbelow 075 considered poor to moderate [32]
To overcome the problem of tests agreement the 120581coefficient was usedThe guidelines by Landis and Koch wereused to interpret the obtained 120581 values and are presented inTable 4 [33]
3 Results
31 TTDN Results Dependent on Clinical Division Amongthe sciatica group only two patients (both TrPs-positivesubjects) felt pain going to the foot as a daily complaintDuringTTDN dry needling related pain sensation consistentwith gluteus minimus referred pain was confirmed for TrPs-positive exclusively Among TrPs-positive sciatica subjectsDN related pain sensation on the thigh during TTDN wasconfirmed for every subject in all three sessionsDN reactivityfor the calf for the three sessions was 100 80 and 733respectively Two TrPs-positive subjects complained of thedaily pain of the foot but during the procedure they did notreport needle sensation going to the foot
Skin Temperature Changes Related to TTDN TTDN con-firmed 119879sk and isothermal-area changes for every subjectThe exact two-way Mann-Whitney 119880 tests confirmed signif-icant increase of 119879max(thighcalf foot) and 119879avr(thighcalf) for TrPs-positive sciatic group as compared to TrPs-negative sciatic
BioMed Research International 5
Table 3 Validity elements [24 25]
Test performed
Results detected by the test True picture TotalPatient has the condition Patient is clear
Positive test A (true positive) B (false positive) A + B (total positive tests)Negative test C (false negative) D (true negative) C + D (total negative tests)Total Total subjects diagnosed with the condition Total subjects without the condition 119873 (total number tested)
Table 4 Landis and Koch guidelines for 120581 interpretation [29]
120581 value Strength of agreementlt000 Poor agreement000ndash020 Slight agreement021ndash040 Fair agreement041ndash060 Moderate agreement061ndash080 Substantial agreement081ndash100 Almost perfect agreement100 Perfect agreement
patients and heathy volunteers (all 119901 lt 005) (Tables 5and 6) The sciatic group presented contrary 119879sk changesdependent on TrPs and DN related referred pain presenceFor TrPs-negative 119879sk decrease contrary to 119879sk increase ofTrPs-positive was observed
Isothermal-Area Changes Related to TTDN None of TrPs-positive subjects presented vasoconstriction or any signifi-cant changes of the low 119879sk isothermal-area and 119879sk decreaseSignificant 119879sk and isothermal-area changes for every TrPs-positive sciatica subject were confirmed
The exact two-way Mann-Whitney 119880 tests confirmed asignificant increase of the observed isothermal-area (calcu-lated together AURP and high119879sk isothermal-area) for TrPs-positive sciatica subjects compared to TrPs-negative sciaticapatients and healthy volunteers (all 119901 lt 005) for both post-DN and postobservation phases (every 119901 lt 005) Afterdividing the isothermal-area into high 119879sk isothermal-areaand AURP (shown in Figure 1) the results were as follows
The exact two-way Mann-Whitney 119880 tests confirmed asignificant increase of the high 119879sk isothermal-area (thighand calf) for TrPs-positive compared toTrPs-negative sciaticasubjects (119901 lt 005) but not to healthy volunteers (Table 7)The significant increase of AURP (vasodilatation) for TrPs-positive compared to TrPs-negative and healthy volunteerswas confirmed (The exact two-way Mann-Whitney 119880 testsevery 119901 lt 005) The average value of the percentage increaseof AURP was shown in Table 8
32 Validity and Reliability of TTDN There were consid-erable differences detected in the results of TTDN when itwas performed on the non-TrPs sciatic group TrP-positivesciatic group and non-TrPs healthy volunteers The agree-ment between TTDN and TrPs diagnosis was almost perfect(according to 120581) for changes of119879avr and isothermal-area above119879max at rest of the thigh and calf (Tables 9 and 10) In terms
of validity components TTDN was useful for identifyingthe positive values of 119879max changes and isothermal-area(below 119879max at rest) or full AURP (namely below and above119879max at rest calculated together) changes but was not useful foridentifying the negative values (specificity) Although 119879maxand isothermal-area below 119879max at rest or full AURP have highsensitivity the low specificity does not allow recommendingtheir diagnostic value
4 Discussion
The results of skin temperature (both 119879avr and 119879max) andisothermal-area significantly differ for TrPs-positive sciaticasubjects compared to non-TrPs sciatica subjects and healthyvolunteers (119901 lt 005 Tables 5ndash8) which is consistent withthe previous study involving sciatica subjects only [10 11]However the main purpose of the present study was tocheck the validity and reliability of TTDN This new IRTmethod was assumed to allow observing vasomotor andtemperature reactions related to TrPs andwas validated for itsability to distinguish active TrPs from non-TrPs of the gluteusminimus muscle and non-TrPs of healthy volunteers It wasfound that TTDN identifies active gluteus minimus TrPs forevery positive subjectThemost discriminatory indicators forTrPs presence were 119879avr increase and the presence of high119879sk increase above 119879max (isothermal-area defined as AURPTables 9 and 10) in the area where dry needling intensifiedpain The results showed that TTDN validly measured 119879avrchanges and the presence of AURP (grey picture in Figure 1)for active TrPs of the gluteus minimus muscle The ICCresults confirmedmoderate reliability forAURPpresence andpoor to moderate for 119879avr increase However these two typesof thermogram analysis showed almost prefect agreementaccording to 120581 (Tables 9 and 10) which is recommended as amore suitablemeasure of agreement amongnonexchangeableobservers in comparison with ICC It seems that AURP andsignificant 119879avr increase can objectively support Travell andSimonsrsquo clinical criteria for active TrPs within the gluteusminimus muscle when referred pain is evoked by snappingpalpation [5 6] However similar tendency for AURP and119879avr for some of the healthy volunteers was observed (AURPnot exceeding 25 with insignificant 119879avr of +014
∘C) (Tables6 and 8) and small changes can be explained by 119879sk differ-ences in time due to the physiological variability of blood flow[34]
IRT reliability was checked for the muscle examinationand was found more reliable compared to the present studybut they examined the thermograms of the subjects at rest [1718] The quantitative measurement of the percentage value of
6 BioMed Research International
Table 5 Mean value of maximum temperature changes
119879max Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus012 plusmn 016 121 plusmn 018 lowastlowastlowast 09 plusmn 014
Calf minus047 plusmn 015 066 plusmn 019 lowastlowastlowast minus005 plusmn 013
Foot minus024 plusmn 014 01 plusmn 011 mdash minus005 plusmn 015
After observThigh 012 plusmn 018 129 plusmn 018 lowastlowastlowast 025 plusmn 013
Calf minus047 plusmn 015 065 plusmn 017 lowastlowastlowast minus018 plusmn 013
Foot minus029 plusmn 016 minus02 plusmn 008 mdash minus023 plusmn 014
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 6 Mean value of average temperature changes
119879avr Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus051 plusmn 011 099 plusmn 012 lowastlowastlowast 007 plusmn 012
Calf minus07 plusmn 011 045 plusmn 011 lowastlowastlowast minus025 plusmn 010
Foot minus056 plusmn 010 minus03 plusmn 07 lowastlowastlowast minus045 plusmn 011
After observThigh minus038 plusmn 014 113 plusmn 013 lowastlowastlowast 015 plusmn 012
Calf minus066 plusmn 012 044 plusmn 014 lowastlowastlowast minus025 plusmn 011
Foot minus053 plusmn 014 minus007 plusmn 008 lowastlowastlowast minus045 plusmn 010
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
isothermal-area changes is presented for the first time andallowed observing the changes of a specific subarea of definedtemperature very precisely However it should be underlinedthat it was possible because dry needling provoked intensive119879sk changes (Figure 1) which again is unusual compared toacupuncture studieswhere postneedling stimulationwas lim-ited to the site of needling [35 36] TTDN allowed observingdynamic thermogram changes due to the stimulation by dryneedling and the fact that DN is a treatment technique forTrPs release [37]The difference between the first and the lastsession could have resulted from the therapeutic DN effectapart from the skin blood flow variability
Moreover it should be underlined that the strong inclu-sion and exclusion criteria for TrPs confirmation did notallow claiming that TTDN is a new objective method forevery gluteus minimus TrP confirmation It has been claimedthat digitally evoked referred pain pattern from the gluteusminimus muscle is rare and for the diagnostic purposes thepresence of a tender point and needle encouraged referredpain were postulated as diagnostic criteria for that muscle
The diagnostic criteria established for the gluteus min-imus muscle in the present study were as severe as possiblebecause it has been lastly postulated that the methodologicalquality of the majority of studies conducted for the purposeof establishing trigger point reproducibility is generally poor[38] Tough et al [39] indicated that only 15 of authorsused the combination of a tender spot in a taut band ofa skeletal muscle patientsrsquo pain recognition predicted painreferral pattern and local twitch response Thanks to TrPsdiagnostic criteria used in the present study the diagnosisof TrPs presence cannot be questioned and additionally the
consistency condition regarding the referred pain presenceminimum to the calf ensures the group homogeneity Ofcourse the choice of the gluteus minimus muscle for the firstuse of TTDN can be questioned However an advantage ofthis choice is the size of the referred pain pattern which isone of the most extensive froms all of the TrPs referred painpatterns Thus it was predicted that the observed vasomotorreactions if present should be probably the widest and easilydetectable by IRT
TTDN Results in the Light of the Previous Studies The use ofthermography is not a new way for TrPs evaluation Most ofthe authors tried to correlate the localization of TrPs with hotspots on the thermogram [16] Brioschi et al [40] analyzedmost of the available studies on the subject and concludedthat IRT findings represent an objective means of document-ing TrPs if the thermogram is analyzed by an experiencedphysician skilled in clinical thermology together with clinicalevaluation of the patient However in one of the oldeststudies Swerdlow andDieter [41] evaluated the sensitivity andspecificity of medical thermography for the documentationof TrPs and they concluded that the localizations of TrPsand hot spots were not associated Moreover some otherauthors stated that skin temperature measurement in TrPsarea cannot be used to detect myofascial tender spots [42]Additionally in the latest review regarding IRT application toTrPs it has been stated that there are few studies evaluatingthe accuracy and reliability of infrared thermography for thediagnosis and assessment of TrPs In the few studies presentthere is no agreement on skin temperature patterns in thepresence of TrPs [43]
BioMed Research International 7
448
419
390
362
333
304
275
246
217451
423
394
365
336
307
279
250
221
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
446
412
378
344
310
276
242
208
175446
412
378
344
310
276
242
208
175
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
450
418
387
355
324
293
261
230
199
450
418
387
355
324
293
261
230
199
450
416
382
349
315
282
248
214
181450
416
382
349
315
282
248
214
181
Case 1 Case 2a b c a b c
Ia
Ib
IIa
IIb
IIIa
IIIb
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
Figure 1 TTDN related thermograms presenting temperature reaction measured on skin surface of TrPs and non-TrPs sciatica patients andhealthy volunteers In rows I two cases of TrPs-negative sciatica II two cases of TrPs-positive sciatica and III two cases of healthy volunteerswere shown In rows Ia IIa and IIIa full thermogramwas presented In rows Ib IIb and IIIb the picture of the isothermal-area above119879max at restcalled AURP was shown (visualization of the vasodilation) In columns (a) Before TTDN (initial state) (b) state immediately after DN and(c) state immediately after observation were presented
IRT was also used for TrPs related referred pain areaexamination Although Brioschi et al [44] evaluated 304chronic myofascial pain patients using IRT before and afterDN or anesthetic infiltration they found that referred areaswere thermally asymmetric andKimura et al [8] confirmed asignificant decrease in 119879sk over time after glutamate injection(nociceptive stimulation) in latent TrPs (119901 lt 005) theusefulness of IRT for postnoxious stimulation of latent TrPsreferred pain observation was contradicted by Zhang et al[9] On the other hand one of the oldest studies on thesubject presents results similar to the present study Kruse Jrand Christiansen [45] observed referred pain pattern by IRTwhen palpation pressure over TrPs lasted around 1 minuteInitially they observed a small 119879sk increase followed by asignificant decrease in the area of the observed referredpain The DN stimulation is a much more severe type ofTrPs stimulation compared to pressure and the time ofstimulation in the present study was ten times longer Itcan be hypothesized that a stronger noxious stimulationcould provoke much more intensive 119879sk increase and maybeKruse Jr and Christiansen [45] observed the same vasomotorreactions but of a weak and short form Additionally another
difference between the studies is the localization of visiblethermal response They reported visible 119879sk changes onthe thermogram more extensive than that of the reportedreferred pain during TrPs compression contrary to thepresent study where AURP localization is limited precisely tothe area where DN provoked pain during TTDN (Figure 1)The thermogram analysis before isothermal-area calculationwas based on the indirect thermogram analysis where theexaminer had to distinguish subtle color differences Theisothermal-area calculation together with the thermogram ofAURP (gray picture Figure 1) is a nonquestionable proof ofsignificant vasomotor changes and can be easily interpretedby everyone
Interestingly the analysis of 119879avr changes in the wholegroup of subjects in the present study (Table 6) clearlyindicated 119879avr decrease for non-TrPs healthy volunteersand needle insensitive foot of TrPs-positive sciatica subjectscontrary to 119879avr increase of DN reactive subarea of TrPs-positive subjects Moreover when the thermograms of non-TrPs sciatica subjects were observed some of them presenteddiscreet vasoconstriction feature (Figure 1) and 119879sk decrease(Tables 5 and 6) These results allow putting the question of
8 BioMed Research International
Table 7 Mean value of isothermal-area below 119879max at rest changes
Isothermal-area below 119879max at rest [] Sciatica patients Healthy volunteersTTDN Phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus276 plusmn 46 76 plusmn 78 lowast minus28 plusmn 52
Calf minus265 plusmn 52 34 plusmn 57 lowast minus85 plusmn 45
Foot minus139 plusmn 513 minus39 plusmn 29 mdash minus97 plusmn 45
After observThigh minus2507 plusmn 45 102 plusmn 784 lowast minus142 plusmn 56
Calf minus248 plusmn 57 minus06 plusmn 53 lowast minus1042 plusmn 55
Foot minus152 plusmn 52 minus42 plusmn 27 mdash minus1015 plusmn 42
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 8 Mean value of isothermal-area above 119879max at rest (AURP) changes
Isothermal-area above 119879max at rest [] Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampnon-DN
After DN Thigh 0 plusmn 00 212 plusmn 265 lowastlowastlowast 114 plusmn 08
Calf 0 plusmn 00 482 plusmn 107 lowastlowastlowast 003 plusmn 002
After observ Thigh 0 plusmn 00 264 plusmn 333 lowastlowastlowast 125 plusmn 08
Calf 0 plusmn 00 663 plusmn 14 lowastlowastlowast 004 plusmn 003
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 9 Validity and reliability of TTDN components for 119879sk changes
119879sk [∘C] TTDN phases Area Sensitivity [] Specificity [] Average [∘C] Min [∘C] Max [∘C] PPV [] ICC 120581
MaximumAfter DN Thigh 100 313 119 minus02 26 577 0622 0702
Calf 100 842 066 minus08 21 667 0422 0786
After observ Thigh 100 167 129 minus01 27 545 0670 0556Calf 100 500 065 minus07 195 857 0440 0680
AverageAfter DN Thigh 100 100 099 004 195 100 0400 0880
Calf 100 100 045 minus04 13 100 0511 0902
After observ Thigh 100 846 111 009 22 750 0333 0786Calf 100 944 044 minus06 15 857 0422 0845
Table 10 Validity and reliability of TTDN components for isothermal-area changes
Isothermal-area TTDN phases Area Sensitivity [] Specificity [] Mean [] Min [] Max [] PPV [] ICC 120581
AURP (above 119879max at rest)After DN Thigh 100 100 212 06 418 100 0689 0938
Calf 100 100 48 minus35 131 100 0778 0956
After observ Thigh 100 100 264 06 522 100 0644 0929Calf 100 100 66 minus44 177 100 0778 0956
Below 119879max at rest
After DN Thigh 100 00 758 minus527 678 500 0778 0656Calf 100 200 337 minus407 474 778 0556 0707
After observ Thigh 100 00 102 minus597 618 500 0778 0656Calf 100 750 minus059 minus419 407 875 0511 0827
Below + above 119879max at rest
After DN Thigh 100 222 288 minus293 869 682 0578 0696Calf 100 370 819 minus136 628 778 0578 0782
After observ Thigh 100 00 1987 minus55 453 483 0733 0643Calf 100 782 605 minus127 576 794 0644 0847
BioMed Research International 9
whether the authors of the previous study who confirmedTrPs-related vasoconstriction really stimulated TrPs On theother hand maybe the type of TrPs (latent TrPs) or regionof IRT observation (upper extremity) or type of noxiousstimulation (glutamate injection) can explain contrary results[8 9] Further studies considering both active and latent TrPsdifferent regions of the body and so forth are required
The New IdeamdashIsothermal-Area Calculation The standardusage of IRT in medicine is based on mean temperature andstandard deviation within the fixed region of interest (ROi)as well as the visualized interpretation of the thermogramwhere each temperature value (or a group of similar values)is attributed to a specified color The color variation is theonly indirect analysis and this type of interpretation is limitedto the physician trained in thermology Additionally theuse of spot temperature measurements or observation ofselected values of 119879max or 119879avr may not produce the expectedoutcomes and the results obtained this way may differ a lotfrom the real situation In summary the comparison of 119879avrof ROi is performed without considering the size of ROiThus an error resulting from the statistical interpretation ispossible These facts can explain the controversies aroundthe merit of IRT measurement in medicine However it hasbeen postulated that considering the number of pixels inthe observed ROi that is the qualitative evaluation of forexample its size and shape together with 119879avr can lead to anobjective interpretation of the results [16]
TTDN is the method which allows assessing the thermo-gram in this recommended wayThemeasurement of the sizeof isothermal-areas in the present study guarantees the pre-cise results of the occurring process of thermal phenomenaappearing on the human skin In addition TTDN analysisaccounts for 100 of the information recorded on a singlethermogram
The next innovativeness of TTDN apart from calculatingthe size of ROi is the possibility of showing vasomotorreactions in TrPs referred pain area The results are easyto interpret and not limited by a physician experience Themeasurement of the size of isothermal-areas in the presentstudy guarantees the precise results of the occurring processof thermal phenomena appearing on the human skin Inaddition the validity of TTDN confirmed the most discrimi-natory indicators for TrPs presence119879avr and isothermal-areacalculation
5 Summary and Limitations of the Study
We are unaware of any other published studies regardingthe validity and reliability of TrPs noxious stimulation byDN under IRT control to support the diagnosis of TrPsThe results of the present study were subject to the rigorand diagnostic protocol of the standards thermographicprocedure Moreover side-to-side 119879sk comparison of thepatient at rest performed before the main procedure allowedexcluding pain states related to sympathetic nervous systemactivity
TTDN seems to be a promising tool for objective TrPsconfirmation However this is the first study of this type
and the validation of TTDN on other muscles with TrPs andsome studies presenting a group with active and latent TrPsof the same muscle are required After a series of studies thatwould give the same results TTDN could be claimed as a newobjectivemethod for TrPs confirmation where DN is possibleto perform
The limitations of this study are the strong inclusion andexclusion criteria for the confirmation of gluteus minimusmuscle TrPs This muscle should be checked by TTDN whenTrPs confirmation is based on tender point presence whichprovoked typical referred pain when needle encounteredTrPs
Moreover Travell and Simons claimed that autonomicphenomena (including vasomotor reaction) within TrPsreferred pain area are limited to severe active TrPs onlyIn the present study TrPs-positive sciatic patients can beassumed to probably have severe active TrPs due to thechronicity and length of the referred pain pattern evokedby snapping palpation However the severity of active TrPsstill remains only a theoretical consideration because thereare no criteria for distinguishing the severity of active TrPs[26] Additionally other TrPs for example within the uppertrapezius muscle should be examined by TTDN to answerthe question if every TrPs present AURP is accompanied by119879avr increase
Finally the present study is limited by the lack of inter-rater reliability of TTDN
6 Conclusion
TTDN is valid and reliable for 119879avr and AURP measurementto support TrPs diagnostic criteria for the gluteus minimusmuscle when a digitally evoked referred pain pattern ispresented In the light of clinical division TTDN results indi-cate skin temperature increase for TrPs-positive contrary todecrease for TrPs-negative chronic sciatica patients and smallchanges (both increasedecrease) for healthy volunteers
Conflict of Interests
The authors declare no conflict of interests especially regard-ing patent application
Authorsrsquo Contribution
All authors listed have contributed substantially to the paperElzbieta Skorupska contributed conception and design ofthe work acquisition of data interpretation of data anddrafting the paper Michał Rychlik contributed Conceptionand design of the work acquisition of data analysis of dataand drafting the paper Włodzimierz Samborski contributedcorrection and final approval of the resubmitted version
Acknowledgments
The authors gratefully acknowledge the critical reading andcorrection of this paper by Malgorzata Mankowska Thiswork was partially supported by the Polish National ScienceCentre Grant no N N404 268339 and Poznan University ofMedical Sciences
10 BioMed Research International
References
[1] R SWeiner PainManagement A Practical Guide for CliniciansCRC Press LLC 6th edition 2002
[2] S A Skootsky B Jaeger and R K Oye ldquoPrevalence ofmyofascial pain in general internal medicine practicerdquoWesternJournal of Medicine vol 151 no 2 pp 157ndash160 1989
[3] Q Chen S Bensamoun J R Basford J M Thompsonand K-N An ldquoIdentification and quantification of myofascialtaut bands with magnetic resonance elastographyrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1658ndash1661 2007
[4] S Sikdar J P Shah T Gebreab et al ldquoNovel applications ofultrasound technology to visualize and characterize myofascialtrigger points and surrounding soft tissuerdquo Archives of PhysicalMedicine and Rehabilitation vol 90 no 11 pp 1829ndash1838 2009
[5] J G Travell andD G SimonsMyofascial Pain andDysfunctionThe Trigger PointManual vol 1WilliamsampWilkins BaltimoreMd USA 2nd edition 1999
[6] J G Travell andD G SimonsMyofascial Pain andDysfunctionTheTrigger PointManual vol 2 LippincottWilliamsampWilkinsBaltimore Md USA 1993
[7] H-Y Ge C Fernandez-de-las-Penas and L Arendt-NielsenldquoSympathetic facilitation of hyperalgesia evoked from myofas-cial tender and trigger points in patients with unilateral shoul-der painrdquoClinical Neurophysiology vol 117 no 7 pp 1545ndash15502006
[8] Y Kimura H-Y Ge Y Zhang M Kimura H Sumikura andL Arendt-Nielsen ldquoEvaluation of sympathetic vasoconstrictorresponse following nociceptive stimulation of latent myofascialtrigger points in humansrdquo Acta Physiologica vol 196 no 4 pp411ndash417 2009
[9] Y Zhang H-Y Ge S-W Yue Y Kimura and L Arendt-Nielsen ldquoAttenuated Skin blood flow response to nociceptivestimulation of latent myofascial trigger pointrdquo Archives ofPhysical Medicine and Rehabilitation vol 90 no 2 pp 325ndash3322009
[10] E Skorupska M Rychlik W Pawelec and W Samborski ldquoDryneedling related short-term vasodilation in chronic sciaticaunder infrared thermovisionrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 214374 10 pages2015
[11] E SkorupskaM Rychlik andW Samborski ldquoIntensive vasodi-latation in the sciatic pain area after dry needlingrdquo BMCComplementary and Alternative Medicine vol 15 article 722015
[12] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoTrigger point-related sympathetic nerve activity inchronic sciatic leg pain a case studyrdquo Acupuncture in Medicinevol 32 no 5 pp 418ndash422 2014
[13] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoIntensive short-term vasodilation effect in the painarea of sciatica patientsmdashcase studyrdquo BMC Research Notes vol7 no 1 article 620 2014
[14] G Affaitati A Fabrizio A Savini et al ldquoA randomizedcontrolled study comparing a lidocaine patch a placebo patchand anesthetic injection for treatment of trigger points inpatients with myofascial pain syndrome evaluation of pain andsomatic pain thresholdsrdquoClinicalTherapeutics vol 31 no 4 pp705ndash720 2009
[15] D G Simons ldquoReview of enigmatic MTrPs as a common causeof enigmatic musculoskeletal pain and dysfunctionrdquo Journal
of Electromyography and Kinesiology vol 14 no 1 pp 95ndash1072004
[16] F S Nahm ldquoInfrared thermography in pain medicinerdquo KoreanJournal of Pain vol 26 no 3 pp 219ndash222 2013
[17] A C S Costa A V D Filho A C Packer and D Rodrigues-Bigaton ldquoIntra and inter-rater reliability of infrared image anal-ysis of masticatory and upper trapezius muscles in women withand without temporomandibular disorderrdquo Brazilian Journal ofPhysical Therapy vol 17 no 1 pp 24ndash31 2013
[18] M McCoy I Campbell P Stone C Fedorchuk S Wijayawar-dana and K Easley ldquoIntra-examiner and inter-examiner repro-ducibility of paraspinal thermographyrdquo PLoS ONE vol 6 no 2Article ID e16535 2011
[19] D S Haddad M L Brioschi and E S Arita ldquoThermographicand clinical correlation of myofascial trigger points in themasticatory musclesrdquo Dentomaxillofacial Radiology vol 41 no8 pp 621ndash629 2012
[20] S J Gulevich T D Conwell J Lane et al ldquoStress infraredtelethermography is useful in the diagnosis of complex regionalpain syndrome type I (formerly reflex sympathetic dystrophy)rdquoClinical Journal of Pain vol 13 no 1 pp 50ndash59 1997
[21] G Wasner J Schattschneider and R Baron ldquoSkin temperatureside differencesmdasha diagnostic tool for CRPSrdquo Pain vol 98 no1-2 pp 19ndash26 2002
[22] E J Park K R Han Y J Chae W H Jeong and C KimldquoEffectiveness of cold stress thermography in the diagnosis ofcomplex of regional pain syndrome type 1rdquoThe Korean Journalof Pain vol 19 pp 159ndash163 2006
[23] E Skorupska M Rychlik and W Pawelec ldquoSkeletal striatedmuscle examination instrument amp new method of myofascialpain diagnosis based on the use of the instrumentrdquo Patentapplication No P-403467 Silver Medal 14ndash16 November 2013Brussels Innova the International Exhibition of InnovationEntrepreneurship and New Technologies Bronze Medal at theConcours Lepine International Paris 3004-11052014 FranceGoldMedal at the Euroinvent EuropeanExhibition ofCreativityand Innovation 22-24052014 Iasi Romania Gold Medal withDistinction at the 29th Invention and New Product ExpositionINPEX 18ndash20062014 Pittsburgh Pa USA
[24] R G Schwartz R Elliott G S Goldberg et al ldquoThe AmericanAcademy of Thermology Guidelines for neuromusculoskeletalthermographyrdquoThermology International vol 16 pp 5ndash9 2006
[25] J Dommerholt and C Fernandez-de-las-Penas Trigger PointDry Needling An Evidence and Clinical-Based ApproachChurchill Livingstone Elsevier 2013
[26] C Z Hong Braddom Physical Medicine and Rehabilitationin Muscle Pain Syndrome Elsevier New York NY USA 4thedition 2011
[27] S Mense D G Simons and I J Russell Muscle PainUnderstanding Its Nature Diagnosis and Treatment LippincottWilliams ampWilkins 2001
[28] R Rolke ldquoPseudoradicular and radicular low-back painmdashadisease continuum Rather than different entities Reply to theletters by Leffler and Hansson and by Van Boxem et alrdquo Painvol 135 pp 311ndash316 2008
[29] J M Bland and D G Altman ldquoStatistical methods for assessingagreement between two methods of clinical measurementrdquoTheLancet vol 1 no 8476 pp 307ndash310 1986
[30] D G Altman ldquoSome common problems in medical researchrdquoin Practical Statistics for Medical Research Chapman amp HallCRC Press London UK 1997
BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
hypothesis concerning TrPs etiology which states that auto-nomic modulation has a potential influence on the increaseof ACh release which can aggravate symptoms caused byTrPs [15] It is commonly accepted that infrared thermovision(IRT) camera can objectively support the diagnosis of painpatients especially when SNS activity is involved [16] HighIRT reliability for muscle examination [17 18] and significantcorrelation between pressure pain threshold and temperaturedifferences inMPS have been recently proved [19] Moreovera new idea for pain medicine studies is a stress loading IRTtest for example by coldwarm stress exercise pharmaco-logical stress vibration and visual stimulation Enhancedsensitivity and specificity for the diagnosis of SNS relateddiseases for example CRPS by cold stress thermographyhas been recommended Unfortunately it causes pain in thepatient and no standardized guidelines for the stress load-ing test have been established [20ndash22] Additionally someauthors claim that IRTwith its temperaturemeasurement andvisual thermogram analysis is not sufficient as a diagnostictool in medicine as it needs to provide thermogram analysismore objectively [16] Interestingly the new awardedmethodcalled Thermovision Technique of Dry Needling (TTDN)allows measuring changes of isothermal-area size (everythermogram can be divided into subareas of 07∘C each) [23]Additionally for TrPs-positive subjects TTDN can measureintensive short-term vasomotor response related to noxiousstimulation of TrPs alone If everyTrP can provoke vasomotorresponse TTDN can objectively support Travell and SimonsrsquoTrPs diagnostic criteria
For the purposes of the study trigger points of thegluteusminimusmuscle were considered because of themostintensive and longest referred pain pattern which spreadsalmost in the whole lower limb [5 6]Thus thismuscle seemsto be the best choice for TTDN validation conducted for thefirst time According to the literature trigger points withinthe gluteusminimusmuscle can be observed among radicularsciatica patients as secondary symptoms due to disc lesion orcan provoke sciatic-like pain pseudoradicular pain [26 27]Objective distinction of radicular and nonradicular sciaticpain is not possible Based on the literature a patient whopresents for example the lack of positive Lasegue test resultaccompanied by the lack of neurological signs of sciatic nerveirritation should be diagnosed as pseudosciatica or sciatic-like pain However Rolke posited that pseudoradicular andradicular low back pain should be considered to be diseasecontinuum rather than different entities [28]
The coexistence of gluteus minimus TrPs in around30 of subacute and chronic radicular sciatica patientswas proved [10 11] as well as the presence of active TrPsamong sciatica-like cases [12 13] Based on some previousstudies it can be hypothesized that the presence of short-termvasomotor changes in the area where TrPs provoke pain mayenable objective trigger points confirmation Whether thecommonly used palpatory criteria are reliable is controversialThus it is very important to find an objective and easy tool forTrPs confirmation
The main aim of this study was to validate Thermovi-sion Technique of Dry Needling (TTDN) and examine itstest-retest reliability for the gluteus minimus muscle The
additional aim was to analyze the average value of TTDNcomponents in the light of clinical division
2 Material and Method
The study was conducted in accordance with the DeclarationofHelsinki approved by the EthicsCommittee of PoznanUni-versity of Medical Sciences (number 77214) It was prospec-tively registered at the AustralianNewZealandClinical TrialsRegistry (ACTRN12614001168640) All subjects gave writteninformed consent to participate in the study before datacollection A detailed description of all examinations andtreatment procedures including dry needling (DN) aswell asof risks involved in the studywas provided to the participantsParticipants had the right to refuse the DN treatment andwithdraw from the study at any time without penalty
21 Subjects Thirty Caucasian chronic sciatica subjectswhere half of themwere TrPs-positive and half TrPs-negativeand fifteen Caucasian healthy volunteers were recruited tothe study from Poznan GP doctors the University PainClinic by press announcement and University staff The ageranged from 35 to 58 years (average 466 plusmn 87 y) Sciat-ica subjects were diagnosed by an experienced neurologisttowards radicular origin of sciatica on the basis of bedsideexamination extensive neurological screening examinationaccompanied by a positive straight leg test and magneticresonance imaging results
Clinical Criteria for Gluteus Minimus Muscle TrPs Confirma-tion According to Travell and Simons the taut band (oneof the essential criteria) is unlikely to be palpated because itlies deeper than both the gluteus maximus and the gluteusmediusmusclesHowever TrPs spot tenderness can be clearlylocalized Additionally the referred pain pattern is morelikely to be observed when needle encounters TrPs ratherthan when sustained pressure on the tender spot is applied[5 6]
The diagnosis of TrPs within the gluteus minimus musclein the present study was based on Travell and Simonsrsquoclinical criteria [5 6] However due to the lack of the tautband of the gluteus minimus muscle the presence of theconfirmatory sign (referred pain pattern) was added to thefull range of possible essential criteria for strong evidenceActive trigger points within gluteusminimus were confirmedif spot tenderness pain recognition and limited range ofmovement were confirmed and the full referred pain patternfelt in the thigh and calf was present (evoked by snappingpalpation)
Key Inclusion Criteria Key inclusion criteria for sciaticapatients were as follows age between 30 and 60 (inclusive)both lower limbs present pain durationgt3monthsgt3 on the1ndash10-point VAS scale of leg pain with this being the dominantpain problem and pain felt minimum to the calf and theresults of the straight leg test between 30 and 60 degrees
Key inclusion criteria for healthy volunteers were generalgood health condition age between 30 and 60 (inclusive)
BioMed Research International 3
both lower limbs present and lack of latent trigger pointswithin the gluteus minimus muscle
Key Exclusion Criteria Subjects were excluded owing tocomplex regional pain syndrome cauda equina syndromeprevious back surgery spinal tumors scoliosis pregnancycoagulant treatment disseminated intravascular coagulationdiabetes epilepsy infection inflammatory rheumatologicdiseases stroke or oncological history
22 Methods All patients recruited to the study were consec-utively examined using TTDN (detailed description below)Also side-to-side IRT comparison of the lower limbs wasperformed
The IRT camera operator was not aware of the results ofgluteus minimus TrPs examination and the physician whoperformed dry needling was not aware of the IRT resultsduring the procedure TTDN was performed three timesduring two consecutive days On the first day TTDN wasperformed once and on the second two sessions with one-hour break were performed for the same marked pointsA thermovision touchless camera (NEC-AVIO TVS-200EX)with a 8ndash14 120583m wave band temperature resolution betterthan 0080∘C and sensitivity of 80mK and working in realtime was applied The camera was equipped with a high-speed (60Hz) uncooled FPA 320 times 240 (119867 times 119881) pixelsVOx (vanadium oxide) microbolometer For thermal imagesanalysis the specialist program ldquoThermography Studio 2007Professionalrdquo was used Every day before the procedure everyparticipant was reexamined towards active gluteus minimusTrPs Then the localization of the two most active TrPswas marked For non-TrPs sciatica subjects and healthyvolunteers two nontender points were marked The dryneedling specialist had no knowledge of whether the markedpoints were TrPs or non-TrPs
221 General Protocol for TTDN TTDN result is thought tobe positive if significant 119879sk (maximum and average temper-ature) changes accompanied by significant isothermal-areachanges in the area of pain are confirmed Isothermal-areais defined as an area of the patientrsquos body with the sametemperature at the samemoment of timeThe TTDNmethodwas partially described in the authorsrsquo previous studies [1011]
(a) Statement Thermographic images were recorded by anexpert following a standard protocol recommended by theAcademy of Neuromuscular Thermography The expert alsoevaluated the images [24] Patients were instructed to avoidphysiotherapy and manual therapy 24 hours prior to thetest and to avoid using nasal decongestants analgesicsanti-inflammatory drugs or any substances affecting thesympathetic functionThey were also instructed not to drinkcoffee or alcohol and to refrain from smoking 2 hours beforethe recording
To obtain the stability of the patientrsquos body temperatureand to ensure the adjustment of the recording camerarsquostemperature to the interior conditions the evaluation began30 minutes after the patient had entered the examination
room Thermal isolation of the evaluated area from otherthermal factors that might have influenced the evaluationincluding other parts of the patientrsquos and doctorrsquos bodies wasensured Moreover when performing thermovision imagingthe general rules of camera usage were followed
(b) Patient Preparation Consider the following
(1) Drawing pain on the pain diagramSide-to-side comparison of the painful area by IRTwas as follows
(a) Comparison of 119879sk differences in the painful legversus the opposite side
(b) When a 119879sk decrease of more than 05∘C in thepainful area compared to nonpainful leg wasobserved then the feature of neuropathic painwas considered possible
(2) Positioning the patient according to dry needlingrules for the examined muscle In this positionthermovision images of the patient were recordedFor adequate representation of dimensions a cali-bration standard was applied The next step involvedrecording the ldquobaserdquo image The image was recordedto establish the initial level of the patientrsquos temperatureparameters
(3) When the above-mentioned conditions weremet dryneedling under IRT control was performed
(c) Dry Needling (DN) Session under IRT Control Dryneedling of every point lasted for 5 minutes During thewhole procedure the subarea of referred pain reported bythe patient was recorded After the needling of both markedpoints was completed further thermovision imaging wasperformed The IRT observation lasted for six consecutiveminutes after DN At the end of the procedure the patientswere asked to answer the question ldquoWas the pain evoked byneedling similar to your daily painrdquo
(d) Thermogram Analysis
Skin Temperature Changes The analysis of thermogramsassumed skin temperature changes maximum temperature(119879max) minimum temperature (119879min) and average tempera-ture (119879avr) in the observed area after the dry needling sessionand during 6 minutes after DN
Analysis of the Impact of Vasomotor Reactions Presence onthe Referred Pain The expected vasomotor changes in thearea of TrPs related referred pain were named autonomicreferred pain (AuRP) if present (Table 1) Post-DN andpostobservation analysis assumed the calculation (in cm2) ofskin isothermal-area changes with the reference point being119879max at rest for AURP-vasodilatation and 119879min at rest for AURP-vasoconstriction from the thermogram at rest Additionallythe size of high 119879sk isothermal-area (15∘C below 119879max at rest)and low 119879sk isothermal-area (15∘C above 119879min at rest) was
4 BioMed Research International
Table 1 Isothermal-area analysis related to TTDN
Initial state After DN After observation
119879min at restIf isothermal-area decreases below 119879min at restmdashthe confirmation of AuRP (vasoconstriction)
Low Tsk isothermal-area (15∘C above 119879min at rest)
119879max at restHigh Tsk isothermal-area (15∘C below 119879max at rest)
If isothermal-area increases above 119879max at restmdashthe confirmation of AuRP (vasodilatation)
Table 2 Definitions of validity elements [24 25]
Validity elements Definition EquationSensitivity Proportion of the positive values that the test correctly identifies 119886 (119886 + 119888) times 100Specificity Proportion of the negative values that the test correctly identifies 119886 (119887 + 119889) times 100Positive predictive value (PPV) Proportion of the patients with positive test results who are correctly diagnosed 119886 (119886 + 119887) times 100Negative predictive value (PNV) Proportion of the patients with negative test results who are correctly diagnosed 119889 (119888 + 119889) times 100
calculated The size of each isothermal-area was recalculatedfrom cm2 to the percentage value
TTDN for Gluteus Minimus Trigger PointsmdashAdditional Infor-mationThe area to be observed by IRTwas chosen accordingto the gluteus minimus referred pain pattern The examinedpatients were positioned on the side on the uninvolvedextremity with the hip and knee flexed The muscle wasneedled with flat palpation perpendicular to the musclealong the counter of the iliac crest Strong depression ofthe subcutaneous tissue was applied in order to reduce thedistance of the skin from the muscle Depth of penetrationdepended on the amount of adipose tissue [25] Therapeuticneedling was performed with 030mm diameter 60mm longsterile acupuncture needles SE L (Serin Corp ShizuokaJapan) Each needle was packed separately
23 Statistical Analysis
TTDN Results Dependent on Clinical Division The chronicsciatica subjects and healthy volunteers were compared withtrigger points coexistence being the differentiating criterionFor the strong evidence of data presented the significancelevel was set based on exact tests not on the default asymp-totic method Exact two-way Mann-Whitney 119880 tests wereperformed in order to ensure that data were representativeof the whole population of possible data values Tests wereapplied to compare the differences for maximum minimumand average skin temperatures and the percentage size ofisothermal-area for the state after dry needling and secondlyfor the postobservation state Values figures and tables inthe text were expressed as plusmn standard error of the mean (SE)Significance level was set at 119901 lt 005 IBM SPSS Statisticsversion 2010158401015840 was used
Validity and Reliability of TTDN A validity analysis wasperformed to confirm the validity of TTDN towards sensitiv-ity and specificity of the obtained results (skin temperaturechanges and percentage size of vasomotor responses) Thecomponents of validity that were used in this study includesensitivity and specificity as well as positive and negative
predictive values Tables 2 and 3 provide definitions andexplanations for the components of validity [30 31]
Reliability of the TTDN Method Test-retest was used tocheck the reliability of TTDN according to the Guidelinesfor Evaluating and Expressing the Uncertainty of NISTMeasurement Results TTDN was performed using the sameexperimental tools the same observer the same measur-ing instrument used under the same conditions the samelocation and repetition over a short period of time on thesame patient Intraclass correlation coefficients (ICC) for test-retest reliability (intraobserved variability) were calculatedto illustrate the differences between repeated measures [29]Intraclass correlation coefficients above 090 were consideredexcellent values form 075 to 090 were considered good andbelow 075 considered poor to moderate [32]
To overcome the problem of tests agreement the 120581coefficient was usedThe guidelines by Landis and Koch wereused to interpret the obtained 120581 values and are presented inTable 4 [33]
3 Results
31 TTDN Results Dependent on Clinical Division Amongthe sciatica group only two patients (both TrPs-positivesubjects) felt pain going to the foot as a daily complaintDuringTTDN dry needling related pain sensation consistentwith gluteus minimus referred pain was confirmed for TrPs-positive exclusively Among TrPs-positive sciatica subjectsDN related pain sensation on the thigh during TTDN wasconfirmed for every subject in all three sessionsDN reactivityfor the calf for the three sessions was 100 80 and 733respectively Two TrPs-positive subjects complained of thedaily pain of the foot but during the procedure they did notreport needle sensation going to the foot
Skin Temperature Changes Related to TTDN TTDN con-firmed 119879sk and isothermal-area changes for every subjectThe exact two-way Mann-Whitney 119880 tests confirmed signif-icant increase of 119879max(thighcalf foot) and 119879avr(thighcalf) for TrPs-positive sciatic group as compared to TrPs-negative sciatic
BioMed Research International 5
Table 3 Validity elements [24 25]
Test performed
Results detected by the test True picture TotalPatient has the condition Patient is clear
Positive test A (true positive) B (false positive) A + B (total positive tests)Negative test C (false negative) D (true negative) C + D (total negative tests)Total Total subjects diagnosed with the condition Total subjects without the condition 119873 (total number tested)
Table 4 Landis and Koch guidelines for 120581 interpretation [29]
120581 value Strength of agreementlt000 Poor agreement000ndash020 Slight agreement021ndash040 Fair agreement041ndash060 Moderate agreement061ndash080 Substantial agreement081ndash100 Almost perfect agreement100 Perfect agreement
patients and heathy volunteers (all 119901 lt 005) (Tables 5and 6) The sciatic group presented contrary 119879sk changesdependent on TrPs and DN related referred pain presenceFor TrPs-negative 119879sk decrease contrary to 119879sk increase ofTrPs-positive was observed
Isothermal-Area Changes Related to TTDN None of TrPs-positive subjects presented vasoconstriction or any signifi-cant changes of the low 119879sk isothermal-area and 119879sk decreaseSignificant 119879sk and isothermal-area changes for every TrPs-positive sciatica subject were confirmed
The exact two-way Mann-Whitney 119880 tests confirmed asignificant increase of the observed isothermal-area (calcu-lated together AURP and high119879sk isothermal-area) for TrPs-positive sciatica subjects compared to TrPs-negative sciaticapatients and healthy volunteers (all 119901 lt 005) for both post-DN and postobservation phases (every 119901 lt 005) Afterdividing the isothermal-area into high 119879sk isothermal-areaand AURP (shown in Figure 1) the results were as follows
The exact two-way Mann-Whitney 119880 tests confirmed asignificant increase of the high 119879sk isothermal-area (thighand calf) for TrPs-positive compared toTrPs-negative sciaticasubjects (119901 lt 005) but not to healthy volunteers (Table 7)The significant increase of AURP (vasodilatation) for TrPs-positive compared to TrPs-negative and healthy volunteerswas confirmed (The exact two-way Mann-Whitney 119880 testsevery 119901 lt 005) The average value of the percentage increaseof AURP was shown in Table 8
32 Validity and Reliability of TTDN There were consid-erable differences detected in the results of TTDN when itwas performed on the non-TrPs sciatic group TrP-positivesciatic group and non-TrPs healthy volunteers The agree-ment between TTDN and TrPs diagnosis was almost perfect(according to 120581) for changes of119879avr and isothermal-area above119879max at rest of the thigh and calf (Tables 9 and 10) In terms
of validity components TTDN was useful for identifyingthe positive values of 119879max changes and isothermal-area(below 119879max at rest) or full AURP (namely below and above119879max at rest calculated together) changes but was not useful foridentifying the negative values (specificity) Although 119879maxand isothermal-area below 119879max at rest or full AURP have highsensitivity the low specificity does not allow recommendingtheir diagnostic value
4 Discussion
The results of skin temperature (both 119879avr and 119879max) andisothermal-area significantly differ for TrPs-positive sciaticasubjects compared to non-TrPs sciatica subjects and healthyvolunteers (119901 lt 005 Tables 5ndash8) which is consistent withthe previous study involving sciatica subjects only [10 11]However the main purpose of the present study was tocheck the validity and reliability of TTDN This new IRTmethod was assumed to allow observing vasomotor andtemperature reactions related to TrPs andwas validated for itsability to distinguish active TrPs from non-TrPs of the gluteusminimus muscle and non-TrPs of healthy volunteers It wasfound that TTDN identifies active gluteus minimus TrPs forevery positive subjectThemost discriminatory indicators forTrPs presence were 119879avr increase and the presence of high119879sk increase above 119879max (isothermal-area defined as AURPTables 9 and 10) in the area where dry needling intensifiedpain The results showed that TTDN validly measured 119879avrchanges and the presence of AURP (grey picture in Figure 1)for active TrPs of the gluteus minimus muscle The ICCresults confirmedmoderate reliability forAURPpresence andpoor to moderate for 119879avr increase However these two typesof thermogram analysis showed almost prefect agreementaccording to 120581 (Tables 9 and 10) which is recommended as amore suitablemeasure of agreement amongnonexchangeableobservers in comparison with ICC It seems that AURP andsignificant 119879avr increase can objectively support Travell andSimonsrsquo clinical criteria for active TrPs within the gluteusminimus muscle when referred pain is evoked by snappingpalpation [5 6] However similar tendency for AURP and119879avr for some of the healthy volunteers was observed (AURPnot exceeding 25 with insignificant 119879avr of +014
∘C) (Tables6 and 8) and small changes can be explained by 119879sk differ-ences in time due to the physiological variability of blood flow[34]
IRT reliability was checked for the muscle examinationand was found more reliable compared to the present studybut they examined the thermograms of the subjects at rest [1718] The quantitative measurement of the percentage value of
6 BioMed Research International
Table 5 Mean value of maximum temperature changes
119879max Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus012 plusmn 016 121 plusmn 018 lowastlowastlowast 09 plusmn 014
Calf minus047 plusmn 015 066 plusmn 019 lowastlowastlowast minus005 plusmn 013
Foot minus024 plusmn 014 01 plusmn 011 mdash minus005 plusmn 015
After observThigh 012 plusmn 018 129 plusmn 018 lowastlowastlowast 025 plusmn 013
Calf minus047 plusmn 015 065 plusmn 017 lowastlowastlowast minus018 plusmn 013
Foot minus029 plusmn 016 minus02 plusmn 008 mdash minus023 plusmn 014
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 6 Mean value of average temperature changes
119879avr Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus051 plusmn 011 099 plusmn 012 lowastlowastlowast 007 plusmn 012
Calf minus07 plusmn 011 045 plusmn 011 lowastlowastlowast minus025 plusmn 010
Foot minus056 plusmn 010 minus03 plusmn 07 lowastlowastlowast minus045 plusmn 011
After observThigh minus038 plusmn 014 113 plusmn 013 lowastlowastlowast 015 plusmn 012
Calf minus066 plusmn 012 044 plusmn 014 lowastlowastlowast minus025 plusmn 011
Foot minus053 plusmn 014 minus007 plusmn 008 lowastlowastlowast minus045 plusmn 010
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
isothermal-area changes is presented for the first time andallowed observing the changes of a specific subarea of definedtemperature very precisely However it should be underlinedthat it was possible because dry needling provoked intensive119879sk changes (Figure 1) which again is unusual compared toacupuncture studieswhere postneedling stimulationwas lim-ited to the site of needling [35 36] TTDN allowed observingdynamic thermogram changes due to the stimulation by dryneedling and the fact that DN is a treatment technique forTrPs release [37]The difference between the first and the lastsession could have resulted from the therapeutic DN effectapart from the skin blood flow variability
Moreover it should be underlined that the strong inclu-sion and exclusion criteria for TrPs confirmation did notallow claiming that TTDN is a new objective method forevery gluteus minimus TrP confirmation It has been claimedthat digitally evoked referred pain pattern from the gluteusminimus muscle is rare and for the diagnostic purposes thepresence of a tender point and needle encouraged referredpain were postulated as diagnostic criteria for that muscle
The diagnostic criteria established for the gluteus min-imus muscle in the present study were as severe as possiblebecause it has been lastly postulated that the methodologicalquality of the majority of studies conducted for the purposeof establishing trigger point reproducibility is generally poor[38] Tough et al [39] indicated that only 15 of authorsused the combination of a tender spot in a taut band ofa skeletal muscle patientsrsquo pain recognition predicted painreferral pattern and local twitch response Thanks to TrPsdiagnostic criteria used in the present study the diagnosisof TrPs presence cannot be questioned and additionally the
consistency condition regarding the referred pain presenceminimum to the calf ensures the group homogeneity Ofcourse the choice of the gluteus minimus muscle for the firstuse of TTDN can be questioned However an advantage ofthis choice is the size of the referred pain pattern which isone of the most extensive froms all of the TrPs referred painpatterns Thus it was predicted that the observed vasomotorreactions if present should be probably the widest and easilydetectable by IRT
TTDN Results in the Light of the Previous Studies The use ofthermography is not a new way for TrPs evaluation Most ofthe authors tried to correlate the localization of TrPs with hotspots on the thermogram [16] Brioschi et al [40] analyzedmost of the available studies on the subject and concludedthat IRT findings represent an objective means of document-ing TrPs if the thermogram is analyzed by an experiencedphysician skilled in clinical thermology together with clinicalevaluation of the patient However in one of the oldeststudies Swerdlow andDieter [41] evaluated the sensitivity andspecificity of medical thermography for the documentationof TrPs and they concluded that the localizations of TrPsand hot spots were not associated Moreover some otherauthors stated that skin temperature measurement in TrPsarea cannot be used to detect myofascial tender spots [42]Additionally in the latest review regarding IRT application toTrPs it has been stated that there are few studies evaluatingthe accuracy and reliability of infrared thermography for thediagnosis and assessment of TrPs In the few studies presentthere is no agreement on skin temperature patterns in thepresence of TrPs [43]
BioMed Research International 7
448
419
390
362
333
304
275
246
217451
423
394
365
336
307
279
250
221
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
446
412
378
344
310
276
242
208
175446
412
378
344
310
276
242
208
175
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
450
418
387
355
324
293
261
230
199
450
418
387
355
324
293
261
230
199
450
416
382
349
315
282
248
214
181450
416
382
349
315
282
248
214
181
Case 1 Case 2a b c a b c
Ia
Ib
IIa
IIb
IIIa
IIIb
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
Figure 1 TTDN related thermograms presenting temperature reaction measured on skin surface of TrPs and non-TrPs sciatica patients andhealthy volunteers In rows I two cases of TrPs-negative sciatica II two cases of TrPs-positive sciatica and III two cases of healthy volunteerswere shown In rows Ia IIa and IIIa full thermogramwas presented In rows Ib IIb and IIIb the picture of the isothermal-area above119879max at restcalled AURP was shown (visualization of the vasodilation) In columns (a) Before TTDN (initial state) (b) state immediately after DN and(c) state immediately after observation were presented
IRT was also used for TrPs related referred pain areaexamination Although Brioschi et al [44] evaluated 304chronic myofascial pain patients using IRT before and afterDN or anesthetic infiltration they found that referred areaswere thermally asymmetric andKimura et al [8] confirmed asignificant decrease in 119879sk over time after glutamate injection(nociceptive stimulation) in latent TrPs (119901 lt 005) theusefulness of IRT for postnoxious stimulation of latent TrPsreferred pain observation was contradicted by Zhang et al[9] On the other hand one of the oldest studies on thesubject presents results similar to the present study Kruse Jrand Christiansen [45] observed referred pain pattern by IRTwhen palpation pressure over TrPs lasted around 1 minuteInitially they observed a small 119879sk increase followed by asignificant decrease in the area of the observed referredpain The DN stimulation is a much more severe type ofTrPs stimulation compared to pressure and the time ofstimulation in the present study was ten times longer Itcan be hypothesized that a stronger noxious stimulationcould provoke much more intensive 119879sk increase and maybeKruse Jr and Christiansen [45] observed the same vasomotorreactions but of a weak and short form Additionally another
difference between the studies is the localization of visiblethermal response They reported visible 119879sk changes onthe thermogram more extensive than that of the reportedreferred pain during TrPs compression contrary to thepresent study where AURP localization is limited precisely tothe area where DN provoked pain during TTDN (Figure 1)The thermogram analysis before isothermal-area calculationwas based on the indirect thermogram analysis where theexaminer had to distinguish subtle color differences Theisothermal-area calculation together with the thermogram ofAURP (gray picture Figure 1) is a nonquestionable proof ofsignificant vasomotor changes and can be easily interpretedby everyone
Interestingly the analysis of 119879avr changes in the wholegroup of subjects in the present study (Table 6) clearlyindicated 119879avr decrease for non-TrPs healthy volunteersand needle insensitive foot of TrPs-positive sciatica subjectscontrary to 119879avr increase of DN reactive subarea of TrPs-positive subjects Moreover when the thermograms of non-TrPs sciatica subjects were observed some of them presenteddiscreet vasoconstriction feature (Figure 1) and 119879sk decrease(Tables 5 and 6) These results allow putting the question of
8 BioMed Research International
Table 7 Mean value of isothermal-area below 119879max at rest changes
Isothermal-area below 119879max at rest [] Sciatica patients Healthy volunteersTTDN Phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus276 plusmn 46 76 plusmn 78 lowast minus28 plusmn 52
Calf minus265 plusmn 52 34 plusmn 57 lowast minus85 plusmn 45
Foot minus139 plusmn 513 minus39 plusmn 29 mdash minus97 plusmn 45
After observThigh minus2507 plusmn 45 102 plusmn 784 lowast minus142 plusmn 56
Calf minus248 plusmn 57 minus06 plusmn 53 lowast minus1042 plusmn 55
Foot minus152 plusmn 52 minus42 plusmn 27 mdash minus1015 plusmn 42
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 8 Mean value of isothermal-area above 119879max at rest (AURP) changes
Isothermal-area above 119879max at rest [] Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampnon-DN
After DN Thigh 0 plusmn 00 212 plusmn 265 lowastlowastlowast 114 plusmn 08
Calf 0 plusmn 00 482 plusmn 107 lowastlowastlowast 003 plusmn 002
After observ Thigh 0 plusmn 00 264 plusmn 333 lowastlowastlowast 125 plusmn 08
Calf 0 plusmn 00 663 plusmn 14 lowastlowastlowast 004 plusmn 003
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 9 Validity and reliability of TTDN components for 119879sk changes
119879sk [∘C] TTDN phases Area Sensitivity [] Specificity [] Average [∘C] Min [∘C] Max [∘C] PPV [] ICC 120581
MaximumAfter DN Thigh 100 313 119 minus02 26 577 0622 0702
Calf 100 842 066 minus08 21 667 0422 0786
After observ Thigh 100 167 129 minus01 27 545 0670 0556Calf 100 500 065 minus07 195 857 0440 0680
AverageAfter DN Thigh 100 100 099 004 195 100 0400 0880
Calf 100 100 045 minus04 13 100 0511 0902
After observ Thigh 100 846 111 009 22 750 0333 0786Calf 100 944 044 minus06 15 857 0422 0845
Table 10 Validity and reliability of TTDN components for isothermal-area changes
Isothermal-area TTDN phases Area Sensitivity [] Specificity [] Mean [] Min [] Max [] PPV [] ICC 120581
AURP (above 119879max at rest)After DN Thigh 100 100 212 06 418 100 0689 0938
Calf 100 100 48 minus35 131 100 0778 0956
After observ Thigh 100 100 264 06 522 100 0644 0929Calf 100 100 66 minus44 177 100 0778 0956
Below 119879max at rest
After DN Thigh 100 00 758 minus527 678 500 0778 0656Calf 100 200 337 minus407 474 778 0556 0707
After observ Thigh 100 00 102 minus597 618 500 0778 0656Calf 100 750 minus059 minus419 407 875 0511 0827
Below + above 119879max at rest
After DN Thigh 100 222 288 minus293 869 682 0578 0696Calf 100 370 819 minus136 628 778 0578 0782
After observ Thigh 100 00 1987 minus55 453 483 0733 0643Calf 100 782 605 minus127 576 794 0644 0847
BioMed Research International 9
whether the authors of the previous study who confirmedTrPs-related vasoconstriction really stimulated TrPs On theother hand maybe the type of TrPs (latent TrPs) or regionof IRT observation (upper extremity) or type of noxiousstimulation (glutamate injection) can explain contrary results[8 9] Further studies considering both active and latent TrPsdifferent regions of the body and so forth are required
The New IdeamdashIsothermal-Area Calculation The standardusage of IRT in medicine is based on mean temperature andstandard deviation within the fixed region of interest (ROi)as well as the visualized interpretation of the thermogramwhere each temperature value (or a group of similar values)is attributed to a specified color The color variation is theonly indirect analysis and this type of interpretation is limitedto the physician trained in thermology Additionally theuse of spot temperature measurements or observation ofselected values of 119879max or 119879avr may not produce the expectedoutcomes and the results obtained this way may differ a lotfrom the real situation In summary the comparison of 119879avrof ROi is performed without considering the size of ROiThus an error resulting from the statistical interpretation ispossible These facts can explain the controversies aroundthe merit of IRT measurement in medicine However it hasbeen postulated that considering the number of pixels inthe observed ROi that is the qualitative evaluation of forexample its size and shape together with 119879avr can lead to anobjective interpretation of the results [16]
TTDN is the method which allows assessing the thermo-gram in this recommended wayThemeasurement of the sizeof isothermal-areas in the present study guarantees the pre-cise results of the occurring process of thermal phenomenaappearing on the human skin In addition TTDN analysisaccounts for 100 of the information recorded on a singlethermogram
The next innovativeness of TTDN apart from calculatingthe size of ROi is the possibility of showing vasomotorreactions in TrPs referred pain area The results are easyto interpret and not limited by a physician experience Themeasurement of the size of isothermal-areas in the presentstudy guarantees the precise results of the occurring processof thermal phenomena appearing on the human skin Inaddition the validity of TTDN confirmed the most discrimi-natory indicators for TrPs presence119879avr and isothermal-areacalculation
5 Summary and Limitations of the Study
We are unaware of any other published studies regardingthe validity and reliability of TrPs noxious stimulation byDN under IRT control to support the diagnosis of TrPsThe results of the present study were subject to the rigorand diagnostic protocol of the standards thermographicprocedure Moreover side-to-side 119879sk comparison of thepatient at rest performed before the main procedure allowedexcluding pain states related to sympathetic nervous systemactivity
TTDN seems to be a promising tool for objective TrPsconfirmation However this is the first study of this type
and the validation of TTDN on other muscles with TrPs andsome studies presenting a group with active and latent TrPsof the same muscle are required After a series of studies thatwould give the same results TTDN could be claimed as a newobjectivemethod for TrPs confirmation where DN is possibleto perform
The limitations of this study are the strong inclusion andexclusion criteria for the confirmation of gluteus minimusmuscle TrPs This muscle should be checked by TTDN whenTrPs confirmation is based on tender point presence whichprovoked typical referred pain when needle encounteredTrPs
Moreover Travell and Simons claimed that autonomicphenomena (including vasomotor reaction) within TrPsreferred pain area are limited to severe active TrPs onlyIn the present study TrPs-positive sciatic patients can beassumed to probably have severe active TrPs due to thechronicity and length of the referred pain pattern evokedby snapping palpation However the severity of active TrPsstill remains only a theoretical consideration because thereare no criteria for distinguishing the severity of active TrPs[26] Additionally other TrPs for example within the uppertrapezius muscle should be examined by TTDN to answerthe question if every TrPs present AURP is accompanied by119879avr increase
Finally the present study is limited by the lack of inter-rater reliability of TTDN
6 Conclusion
TTDN is valid and reliable for 119879avr and AURP measurementto support TrPs diagnostic criteria for the gluteus minimusmuscle when a digitally evoked referred pain pattern ispresented In the light of clinical division TTDN results indi-cate skin temperature increase for TrPs-positive contrary todecrease for TrPs-negative chronic sciatica patients and smallchanges (both increasedecrease) for healthy volunteers
Conflict of Interests
The authors declare no conflict of interests especially regard-ing patent application
Authorsrsquo Contribution
All authors listed have contributed substantially to the paperElzbieta Skorupska contributed conception and design ofthe work acquisition of data interpretation of data anddrafting the paper Michał Rychlik contributed Conceptionand design of the work acquisition of data analysis of dataand drafting the paper Włodzimierz Samborski contributedcorrection and final approval of the resubmitted version
Acknowledgments
The authors gratefully acknowledge the critical reading andcorrection of this paper by Malgorzata Mankowska Thiswork was partially supported by the Polish National ScienceCentre Grant no N N404 268339 and Poznan University ofMedical Sciences
10 BioMed Research International
References
[1] R SWeiner PainManagement A Practical Guide for CliniciansCRC Press LLC 6th edition 2002
[2] S A Skootsky B Jaeger and R K Oye ldquoPrevalence ofmyofascial pain in general internal medicine practicerdquoWesternJournal of Medicine vol 151 no 2 pp 157ndash160 1989
[3] Q Chen S Bensamoun J R Basford J M Thompsonand K-N An ldquoIdentification and quantification of myofascialtaut bands with magnetic resonance elastographyrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1658ndash1661 2007
[4] S Sikdar J P Shah T Gebreab et al ldquoNovel applications ofultrasound technology to visualize and characterize myofascialtrigger points and surrounding soft tissuerdquo Archives of PhysicalMedicine and Rehabilitation vol 90 no 11 pp 1829ndash1838 2009
[5] J G Travell andD G SimonsMyofascial Pain andDysfunctionThe Trigger PointManual vol 1WilliamsampWilkins BaltimoreMd USA 2nd edition 1999
[6] J G Travell andD G SimonsMyofascial Pain andDysfunctionTheTrigger PointManual vol 2 LippincottWilliamsampWilkinsBaltimore Md USA 1993
[7] H-Y Ge C Fernandez-de-las-Penas and L Arendt-NielsenldquoSympathetic facilitation of hyperalgesia evoked from myofas-cial tender and trigger points in patients with unilateral shoul-der painrdquoClinical Neurophysiology vol 117 no 7 pp 1545ndash15502006
[8] Y Kimura H-Y Ge Y Zhang M Kimura H Sumikura andL Arendt-Nielsen ldquoEvaluation of sympathetic vasoconstrictorresponse following nociceptive stimulation of latent myofascialtrigger points in humansrdquo Acta Physiologica vol 196 no 4 pp411ndash417 2009
[9] Y Zhang H-Y Ge S-W Yue Y Kimura and L Arendt-Nielsen ldquoAttenuated Skin blood flow response to nociceptivestimulation of latent myofascial trigger pointrdquo Archives ofPhysical Medicine and Rehabilitation vol 90 no 2 pp 325ndash3322009
[10] E Skorupska M Rychlik W Pawelec and W Samborski ldquoDryneedling related short-term vasodilation in chronic sciaticaunder infrared thermovisionrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 214374 10 pages2015
[11] E SkorupskaM Rychlik andW Samborski ldquoIntensive vasodi-latation in the sciatic pain area after dry needlingrdquo BMCComplementary and Alternative Medicine vol 15 article 722015
[12] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoTrigger point-related sympathetic nerve activity inchronic sciatic leg pain a case studyrdquo Acupuncture in Medicinevol 32 no 5 pp 418ndash422 2014
[13] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoIntensive short-term vasodilation effect in the painarea of sciatica patientsmdashcase studyrdquo BMC Research Notes vol7 no 1 article 620 2014
[14] G Affaitati A Fabrizio A Savini et al ldquoA randomizedcontrolled study comparing a lidocaine patch a placebo patchand anesthetic injection for treatment of trigger points inpatients with myofascial pain syndrome evaluation of pain andsomatic pain thresholdsrdquoClinicalTherapeutics vol 31 no 4 pp705ndash720 2009
[15] D G Simons ldquoReview of enigmatic MTrPs as a common causeof enigmatic musculoskeletal pain and dysfunctionrdquo Journal
of Electromyography and Kinesiology vol 14 no 1 pp 95ndash1072004
[16] F S Nahm ldquoInfrared thermography in pain medicinerdquo KoreanJournal of Pain vol 26 no 3 pp 219ndash222 2013
[17] A C S Costa A V D Filho A C Packer and D Rodrigues-Bigaton ldquoIntra and inter-rater reliability of infrared image anal-ysis of masticatory and upper trapezius muscles in women withand without temporomandibular disorderrdquo Brazilian Journal ofPhysical Therapy vol 17 no 1 pp 24ndash31 2013
[18] M McCoy I Campbell P Stone C Fedorchuk S Wijayawar-dana and K Easley ldquoIntra-examiner and inter-examiner repro-ducibility of paraspinal thermographyrdquo PLoS ONE vol 6 no 2Article ID e16535 2011
[19] D S Haddad M L Brioschi and E S Arita ldquoThermographicand clinical correlation of myofascial trigger points in themasticatory musclesrdquo Dentomaxillofacial Radiology vol 41 no8 pp 621ndash629 2012
[20] S J Gulevich T D Conwell J Lane et al ldquoStress infraredtelethermography is useful in the diagnosis of complex regionalpain syndrome type I (formerly reflex sympathetic dystrophy)rdquoClinical Journal of Pain vol 13 no 1 pp 50ndash59 1997
[21] G Wasner J Schattschneider and R Baron ldquoSkin temperatureside differencesmdasha diagnostic tool for CRPSrdquo Pain vol 98 no1-2 pp 19ndash26 2002
[22] E J Park K R Han Y J Chae W H Jeong and C KimldquoEffectiveness of cold stress thermography in the diagnosis ofcomplex of regional pain syndrome type 1rdquoThe Korean Journalof Pain vol 19 pp 159ndash163 2006
[23] E Skorupska M Rychlik and W Pawelec ldquoSkeletal striatedmuscle examination instrument amp new method of myofascialpain diagnosis based on the use of the instrumentrdquo Patentapplication No P-403467 Silver Medal 14ndash16 November 2013Brussels Innova the International Exhibition of InnovationEntrepreneurship and New Technologies Bronze Medal at theConcours Lepine International Paris 3004-11052014 FranceGoldMedal at the Euroinvent EuropeanExhibition ofCreativityand Innovation 22-24052014 Iasi Romania Gold Medal withDistinction at the 29th Invention and New Product ExpositionINPEX 18ndash20062014 Pittsburgh Pa USA
[24] R G Schwartz R Elliott G S Goldberg et al ldquoThe AmericanAcademy of Thermology Guidelines for neuromusculoskeletalthermographyrdquoThermology International vol 16 pp 5ndash9 2006
[25] J Dommerholt and C Fernandez-de-las-Penas Trigger PointDry Needling An Evidence and Clinical-Based ApproachChurchill Livingstone Elsevier 2013
[26] C Z Hong Braddom Physical Medicine and Rehabilitationin Muscle Pain Syndrome Elsevier New York NY USA 4thedition 2011
[27] S Mense D G Simons and I J Russell Muscle PainUnderstanding Its Nature Diagnosis and Treatment LippincottWilliams ampWilkins 2001
[28] R Rolke ldquoPseudoradicular and radicular low-back painmdashadisease continuum Rather than different entities Reply to theletters by Leffler and Hansson and by Van Boxem et alrdquo Painvol 135 pp 311ndash316 2008
[29] J M Bland and D G Altman ldquoStatistical methods for assessingagreement between two methods of clinical measurementrdquoTheLancet vol 1 no 8476 pp 307ndash310 1986
[30] D G Altman ldquoSome common problems in medical researchrdquoin Practical Statistics for Medical Research Chapman amp HallCRC Press London UK 1997
BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
both lower limbs present and lack of latent trigger pointswithin the gluteus minimus muscle
Key Exclusion Criteria Subjects were excluded owing tocomplex regional pain syndrome cauda equina syndromeprevious back surgery spinal tumors scoliosis pregnancycoagulant treatment disseminated intravascular coagulationdiabetes epilepsy infection inflammatory rheumatologicdiseases stroke or oncological history
22 Methods All patients recruited to the study were consec-utively examined using TTDN (detailed description below)Also side-to-side IRT comparison of the lower limbs wasperformed
The IRT camera operator was not aware of the results ofgluteus minimus TrPs examination and the physician whoperformed dry needling was not aware of the IRT resultsduring the procedure TTDN was performed three timesduring two consecutive days On the first day TTDN wasperformed once and on the second two sessions with one-hour break were performed for the same marked pointsA thermovision touchless camera (NEC-AVIO TVS-200EX)with a 8ndash14 120583m wave band temperature resolution betterthan 0080∘C and sensitivity of 80mK and working in realtime was applied The camera was equipped with a high-speed (60Hz) uncooled FPA 320 times 240 (119867 times 119881) pixelsVOx (vanadium oxide) microbolometer For thermal imagesanalysis the specialist program ldquoThermography Studio 2007Professionalrdquo was used Every day before the procedure everyparticipant was reexamined towards active gluteus minimusTrPs Then the localization of the two most active TrPswas marked For non-TrPs sciatica subjects and healthyvolunteers two nontender points were marked The dryneedling specialist had no knowledge of whether the markedpoints were TrPs or non-TrPs
221 General Protocol for TTDN TTDN result is thought tobe positive if significant 119879sk (maximum and average temper-ature) changes accompanied by significant isothermal-areachanges in the area of pain are confirmed Isothermal-areais defined as an area of the patientrsquos body with the sametemperature at the samemoment of timeThe TTDNmethodwas partially described in the authorsrsquo previous studies [1011]
(a) Statement Thermographic images were recorded by anexpert following a standard protocol recommended by theAcademy of Neuromuscular Thermography The expert alsoevaluated the images [24] Patients were instructed to avoidphysiotherapy and manual therapy 24 hours prior to thetest and to avoid using nasal decongestants analgesicsanti-inflammatory drugs or any substances affecting thesympathetic functionThey were also instructed not to drinkcoffee or alcohol and to refrain from smoking 2 hours beforethe recording
To obtain the stability of the patientrsquos body temperatureand to ensure the adjustment of the recording camerarsquostemperature to the interior conditions the evaluation began30 minutes after the patient had entered the examination
room Thermal isolation of the evaluated area from otherthermal factors that might have influenced the evaluationincluding other parts of the patientrsquos and doctorrsquos bodies wasensured Moreover when performing thermovision imagingthe general rules of camera usage were followed
(b) Patient Preparation Consider the following
(1) Drawing pain on the pain diagramSide-to-side comparison of the painful area by IRTwas as follows
(a) Comparison of 119879sk differences in the painful legversus the opposite side
(b) When a 119879sk decrease of more than 05∘C in thepainful area compared to nonpainful leg wasobserved then the feature of neuropathic painwas considered possible
(2) Positioning the patient according to dry needlingrules for the examined muscle In this positionthermovision images of the patient were recordedFor adequate representation of dimensions a cali-bration standard was applied The next step involvedrecording the ldquobaserdquo image The image was recordedto establish the initial level of the patientrsquos temperatureparameters
(3) When the above-mentioned conditions weremet dryneedling under IRT control was performed
(c) Dry Needling (DN) Session under IRT Control Dryneedling of every point lasted for 5 minutes During thewhole procedure the subarea of referred pain reported bythe patient was recorded After the needling of both markedpoints was completed further thermovision imaging wasperformed The IRT observation lasted for six consecutiveminutes after DN At the end of the procedure the patientswere asked to answer the question ldquoWas the pain evoked byneedling similar to your daily painrdquo
(d) Thermogram Analysis
Skin Temperature Changes The analysis of thermogramsassumed skin temperature changes maximum temperature(119879max) minimum temperature (119879min) and average tempera-ture (119879avr) in the observed area after the dry needling sessionand during 6 minutes after DN
Analysis of the Impact of Vasomotor Reactions Presence onthe Referred Pain The expected vasomotor changes in thearea of TrPs related referred pain were named autonomicreferred pain (AuRP) if present (Table 1) Post-DN andpostobservation analysis assumed the calculation (in cm2) ofskin isothermal-area changes with the reference point being119879max at rest for AURP-vasodilatation and 119879min at rest for AURP-vasoconstriction from the thermogram at rest Additionallythe size of high 119879sk isothermal-area (15∘C below 119879max at rest)and low 119879sk isothermal-area (15∘C above 119879min at rest) was
4 BioMed Research International
Table 1 Isothermal-area analysis related to TTDN
Initial state After DN After observation
119879min at restIf isothermal-area decreases below 119879min at restmdashthe confirmation of AuRP (vasoconstriction)
Low Tsk isothermal-area (15∘C above 119879min at rest)
119879max at restHigh Tsk isothermal-area (15∘C below 119879max at rest)
If isothermal-area increases above 119879max at restmdashthe confirmation of AuRP (vasodilatation)
Table 2 Definitions of validity elements [24 25]
Validity elements Definition EquationSensitivity Proportion of the positive values that the test correctly identifies 119886 (119886 + 119888) times 100Specificity Proportion of the negative values that the test correctly identifies 119886 (119887 + 119889) times 100Positive predictive value (PPV) Proportion of the patients with positive test results who are correctly diagnosed 119886 (119886 + 119887) times 100Negative predictive value (PNV) Proportion of the patients with negative test results who are correctly diagnosed 119889 (119888 + 119889) times 100
calculated The size of each isothermal-area was recalculatedfrom cm2 to the percentage value
TTDN for Gluteus Minimus Trigger PointsmdashAdditional Infor-mationThe area to be observed by IRTwas chosen accordingto the gluteus minimus referred pain pattern The examinedpatients were positioned on the side on the uninvolvedextremity with the hip and knee flexed The muscle wasneedled with flat palpation perpendicular to the musclealong the counter of the iliac crest Strong depression ofthe subcutaneous tissue was applied in order to reduce thedistance of the skin from the muscle Depth of penetrationdepended on the amount of adipose tissue [25] Therapeuticneedling was performed with 030mm diameter 60mm longsterile acupuncture needles SE L (Serin Corp ShizuokaJapan) Each needle was packed separately
23 Statistical Analysis
TTDN Results Dependent on Clinical Division The chronicsciatica subjects and healthy volunteers were compared withtrigger points coexistence being the differentiating criterionFor the strong evidence of data presented the significancelevel was set based on exact tests not on the default asymp-totic method Exact two-way Mann-Whitney 119880 tests wereperformed in order to ensure that data were representativeof the whole population of possible data values Tests wereapplied to compare the differences for maximum minimumand average skin temperatures and the percentage size ofisothermal-area for the state after dry needling and secondlyfor the postobservation state Values figures and tables inthe text were expressed as plusmn standard error of the mean (SE)Significance level was set at 119901 lt 005 IBM SPSS Statisticsversion 2010158401015840 was used
Validity and Reliability of TTDN A validity analysis wasperformed to confirm the validity of TTDN towards sensitiv-ity and specificity of the obtained results (skin temperaturechanges and percentage size of vasomotor responses) Thecomponents of validity that were used in this study includesensitivity and specificity as well as positive and negative
predictive values Tables 2 and 3 provide definitions andexplanations for the components of validity [30 31]
Reliability of the TTDN Method Test-retest was used tocheck the reliability of TTDN according to the Guidelinesfor Evaluating and Expressing the Uncertainty of NISTMeasurement Results TTDN was performed using the sameexperimental tools the same observer the same measur-ing instrument used under the same conditions the samelocation and repetition over a short period of time on thesame patient Intraclass correlation coefficients (ICC) for test-retest reliability (intraobserved variability) were calculatedto illustrate the differences between repeated measures [29]Intraclass correlation coefficients above 090 were consideredexcellent values form 075 to 090 were considered good andbelow 075 considered poor to moderate [32]
To overcome the problem of tests agreement the 120581coefficient was usedThe guidelines by Landis and Koch wereused to interpret the obtained 120581 values and are presented inTable 4 [33]
3 Results
31 TTDN Results Dependent on Clinical Division Amongthe sciatica group only two patients (both TrPs-positivesubjects) felt pain going to the foot as a daily complaintDuringTTDN dry needling related pain sensation consistentwith gluteus minimus referred pain was confirmed for TrPs-positive exclusively Among TrPs-positive sciatica subjectsDN related pain sensation on the thigh during TTDN wasconfirmed for every subject in all three sessionsDN reactivityfor the calf for the three sessions was 100 80 and 733respectively Two TrPs-positive subjects complained of thedaily pain of the foot but during the procedure they did notreport needle sensation going to the foot
Skin Temperature Changes Related to TTDN TTDN con-firmed 119879sk and isothermal-area changes for every subjectThe exact two-way Mann-Whitney 119880 tests confirmed signif-icant increase of 119879max(thighcalf foot) and 119879avr(thighcalf) for TrPs-positive sciatic group as compared to TrPs-negative sciatic
BioMed Research International 5
Table 3 Validity elements [24 25]
Test performed
Results detected by the test True picture TotalPatient has the condition Patient is clear
Positive test A (true positive) B (false positive) A + B (total positive tests)Negative test C (false negative) D (true negative) C + D (total negative tests)Total Total subjects diagnosed with the condition Total subjects without the condition 119873 (total number tested)
Table 4 Landis and Koch guidelines for 120581 interpretation [29]
120581 value Strength of agreementlt000 Poor agreement000ndash020 Slight agreement021ndash040 Fair agreement041ndash060 Moderate agreement061ndash080 Substantial agreement081ndash100 Almost perfect agreement100 Perfect agreement
patients and heathy volunteers (all 119901 lt 005) (Tables 5and 6) The sciatic group presented contrary 119879sk changesdependent on TrPs and DN related referred pain presenceFor TrPs-negative 119879sk decrease contrary to 119879sk increase ofTrPs-positive was observed
Isothermal-Area Changes Related to TTDN None of TrPs-positive subjects presented vasoconstriction or any signifi-cant changes of the low 119879sk isothermal-area and 119879sk decreaseSignificant 119879sk and isothermal-area changes for every TrPs-positive sciatica subject were confirmed
The exact two-way Mann-Whitney 119880 tests confirmed asignificant increase of the observed isothermal-area (calcu-lated together AURP and high119879sk isothermal-area) for TrPs-positive sciatica subjects compared to TrPs-negative sciaticapatients and healthy volunteers (all 119901 lt 005) for both post-DN and postobservation phases (every 119901 lt 005) Afterdividing the isothermal-area into high 119879sk isothermal-areaand AURP (shown in Figure 1) the results were as follows
The exact two-way Mann-Whitney 119880 tests confirmed asignificant increase of the high 119879sk isothermal-area (thighand calf) for TrPs-positive compared toTrPs-negative sciaticasubjects (119901 lt 005) but not to healthy volunteers (Table 7)The significant increase of AURP (vasodilatation) for TrPs-positive compared to TrPs-negative and healthy volunteerswas confirmed (The exact two-way Mann-Whitney 119880 testsevery 119901 lt 005) The average value of the percentage increaseof AURP was shown in Table 8
32 Validity and Reliability of TTDN There were consid-erable differences detected in the results of TTDN when itwas performed on the non-TrPs sciatic group TrP-positivesciatic group and non-TrPs healthy volunteers The agree-ment between TTDN and TrPs diagnosis was almost perfect(according to 120581) for changes of119879avr and isothermal-area above119879max at rest of the thigh and calf (Tables 9 and 10) In terms
of validity components TTDN was useful for identifyingthe positive values of 119879max changes and isothermal-area(below 119879max at rest) or full AURP (namely below and above119879max at rest calculated together) changes but was not useful foridentifying the negative values (specificity) Although 119879maxand isothermal-area below 119879max at rest or full AURP have highsensitivity the low specificity does not allow recommendingtheir diagnostic value
4 Discussion
The results of skin temperature (both 119879avr and 119879max) andisothermal-area significantly differ for TrPs-positive sciaticasubjects compared to non-TrPs sciatica subjects and healthyvolunteers (119901 lt 005 Tables 5ndash8) which is consistent withthe previous study involving sciatica subjects only [10 11]However the main purpose of the present study was tocheck the validity and reliability of TTDN This new IRTmethod was assumed to allow observing vasomotor andtemperature reactions related to TrPs andwas validated for itsability to distinguish active TrPs from non-TrPs of the gluteusminimus muscle and non-TrPs of healthy volunteers It wasfound that TTDN identifies active gluteus minimus TrPs forevery positive subjectThemost discriminatory indicators forTrPs presence were 119879avr increase and the presence of high119879sk increase above 119879max (isothermal-area defined as AURPTables 9 and 10) in the area where dry needling intensifiedpain The results showed that TTDN validly measured 119879avrchanges and the presence of AURP (grey picture in Figure 1)for active TrPs of the gluteus minimus muscle The ICCresults confirmedmoderate reliability forAURPpresence andpoor to moderate for 119879avr increase However these two typesof thermogram analysis showed almost prefect agreementaccording to 120581 (Tables 9 and 10) which is recommended as amore suitablemeasure of agreement amongnonexchangeableobservers in comparison with ICC It seems that AURP andsignificant 119879avr increase can objectively support Travell andSimonsrsquo clinical criteria for active TrPs within the gluteusminimus muscle when referred pain is evoked by snappingpalpation [5 6] However similar tendency for AURP and119879avr for some of the healthy volunteers was observed (AURPnot exceeding 25 with insignificant 119879avr of +014
∘C) (Tables6 and 8) and small changes can be explained by 119879sk differ-ences in time due to the physiological variability of blood flow[34]
IRT reliability was checked for the muscle examinationand was found more reliable compared to the present studybut they examined the thermograms of the subjects at rest [1718] The quantitative measurement of the percentage value of
6 BioMed Research International
Table 5 Mean value of maximum temperature changes
119879max Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus012 plusmn 016 121 plusmn 018 lowastlowastlowast 09 plusmn 014
Calf minus047 plusmn 015 066 plusmn 019 lowastlowastlowast minus005 plusmn 013
Foot minus024 plusmn 014 01 plusmn 011 mdash minus005 plusmn 015
After observThigh 012 plusmn 018 129 plusmn 018 lowastlowastlowast 025 plusmn 013
Calf minus047 plusmn 015 065 plusmn 017 lowastlowastlowast minus018 plusmn 013
Foot minus029 plusmn 016 minus02 plusmn 008 mdash minus023 plusmn 014
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 6 Mean value of average temperature changes
119879avr Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus051 plusmn 011 099 plusmn 012 lowastlowastlowast 007 plusmn 012
Calf minus07 plusmn 011 045 plusmn 011 lowastlowastlowast minus025 plusmn 010
Foot minus056 plusmn 010 minus03 plusmn 07 lowastlowastlowast minus045 plusmn 011
After observThigh minus038 plusmn 014 113 plusmn 013 lowastlowastlowast 015 plusmn 012
Calf minus066 plusmn 012 044 plusmn 014 lowastlowastlowast minus025 plusmn 011
Foot minus053 plusmn 014 minus007 plusmn 008 lowastlowastlowast minus045 plusmn 010
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
isothermal-area changes is presented for the first time andallowed observing the changes of a specific subarea of definedtemperature very precisely However it should be underlinedthat it was possible because dry needling provoked intensive119879sk changes (Figure 1) which again is unusual compared toacupuncture studieswhere postneedling stimulationwas lim-ited to the site of needling [35 36] TTDN allowed observingdynamic thermogram changes due to the stimulation by dryneedling and the fact that DN is a treatment technique forTrPs release [37]The difference between the first and the lastsession could have resulted from the therapeutic DN effectapart from the skin blood flow variability
Moreover it should be underlined that the strong inclu-sion and exclusion criteria for TrPs confirmation did notallow claiming that TTDN is a new objective method forevery gluteus minimus TrP confirmation It has been claimedthat digitally evoked referred pain pattern from the gluteusminimus muscle is rare and for the diagnostic purposes thepresence of a tender point and needle encouraged referredpain were postulated as diagnostic criteria for that muscle
The diagnostic criteria established for the gluteus min-imus muscle in the present study were as severe as possiblebecause it has been lastly postulated that the methodologicalquality of the majority of studies conducted for the purposeof establishing trigger point reproducibility is generally poor[38] Tough et al [39] indicated that only 15 of authorsused the combination of a tender spot in a taut band ofa skeletal muscle patientsrsquo pain recognition predicted painreferral pattern and local twitch response Thanks to TrPsdiagnostic criteria used in the present study the diagnosisof TrPs presence cannot be questioned and additionally the
consistency condition regarding the referred pain presenceminimum to the calf ensures the group homogeneity Ofcourse the choice of the gluteus minimus muscle for the firstuse of TTDN can be questioned However an advantage ofthis choice is the size of the referred pain pattern which isone of the most extensive froms all of the TrPs referred painpatterns Thus it was predicted that the observed vasomotorreactions if present should be probably the widest and easilydetectable by IRT
TTDN Results in the Light of the Previous Studies The use ofthermography is not a new way for TrPs evaluation Most ofthe authors tried to correlate the localization of TrPs with hotspots on the thermogram [16] Brioschi et al [40] analyzedmost of the available studies on the subject and concludedthat IRT findings represent an objective means of document-ing TrPs if the thermogram is analyzed by an experiencedphysician skilled in clinical thermology together with clinicalevaluation of the patient However in one of the oldeststudies Swerdlow andDieter [41] evaluated the sensitivity andspecificity of medical thermography for the documentationof TrPs and they concluded that the localizations of TrPsand hot spots were not associated Moreover some otherauthors stated that skin temperature measurement in TrPsarea cannot be used to detect myofascial tender spots [42]Additionally in the latest review regarding IRT application toTrPs it has been stated that there are few studies evaluatingthe accuracy and reliability of infrared thermography for thediagnosis and assessment of TrPs In the few studies presentthere is no agreement on skin temperature patterns in thepresence of TrPs [43]
BioMed Research International 7
448
419
390
362
333
304
275
246
217451
423
394
365
336
307
279
250
221
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
446
412
378
344
310
276
242
208
175446
412
378
344
310
276
242
208
175
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
450
418
387
355
324
293
261
230
199
450
418
387
355
324
293
261
230
199
450
416
382
349
315
282
248
214
181450
416
382
349
315
282
248
214
181
Case 1 Case 2a b c a b c
Ia
Ib
IIa
IIb
IIIa
IIIb
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
Figure 1 TTDN related thermograms presenting temperature reaction measured on skin surface of TrPs and non-TrPs sciatica patients andhealthy volunteers In rows I two cases of TrPs-negative sciatica II two cases of TrPs-positive sciatica and III two cases of healthy volunteerswere shown In rows Ia IIa and IIIa full thermogramwas presented In rows Ib IIb and IIIb the picture of the isothermal-area above119879max at restcalled AURP was shown (visualization of the vasodilation) In columns (a) Before TTDN (initial state) (b) state immediately after DN and(c) state immediately after observation were presented
IRT was also used for TrPs related referred pain areaexamination Although Brioschi et al [44] evaluated 304chronic myofascial pain patients using IRT before and afterDN or anesthetic infiltration they found that referred areaswere thermally asymmetric andKimura et al [8] confirmed asignificant decrease in 119879sk over time after glutamate injection(nociceptive stimulation) in latent TrPs (119901 lt 005) theusefulness of IRT for postnoxious stimulation of latent TrPsreferred pain observation was contradicted by Zhang et al[9] On the other hand one of the oldest studies on thesubject presents results similar to the present study Kruse Jrand Christiansen [45] observed referred pain pattern by IRTwhen palpation pressure over TrPs lasted around 1 minuteInitially they observed a small 119879sk increase followed by asignificant decrease in the area of the observed referredpain The DN stimulation is a much more severe type ofTrPs stimulation compared to pressure and the time ofstimulation in the present study was ten times longer Itcan be hypothesized that a stronger noxious stimulationcould provoke much more intensive 119879sk increase and maybeKruse Jr and Christiansen [45] observed the same vasomotorreactions but of a weak and short form Additionally another
difference between the studies is the localization of visiblethermal response They reported visible 119879sk changes onthe thermogram more extensive than that of the reportedreferred pain during TrPs compression contrary to thepresent study where AURP localization is limited precisely tothe area where DN provoked pain during TTDN (Figure 1)The thermogram analysis before isothermal-area calculationwas based on the indirect thermogram analysis where theexaminer had to distinguish subtle color differences Theisothermal-area calculation together with the thermogram ofAURP (gray picture Figure 1) is a nonquestionable proof ofsignificant vasomotor changes and can be easily interpretedby everyone
Interestingly the analysis of 119879avr changes in the wholegroup of subjects in the present study (Table 6) clearlyindicated 119879avr decrease for non-TrPs healthy volunteersand needle insensitive foot of TrPs-positive sciatica subjectscontrary to 119879avr increase of DN reactive subarea of TrPs-positive subjects Moreover when the thermograms of non-TrPs sciatica subjects were observed some of them presenteddiscreet vasoconstriction feature (Figure 1) and 119879sk decrease(Tables 5 and 6) These results allow putting the question of
8 BioMed Research International
Table 7 Mean value of isothermal-area below 119879max at rest changes
Isothermal-area below 119879max at rest [] Sciatica patients Healthy volunteersTTDN Phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus276 plusmn 46 76 plusmn 78 lowast minus28 plusmn 52
Calf minus265 plusmn 52 34 plusmn 57 lowast minus85 plusmn 45
Foot minus139 plusmn 513 minus39 plusmn 29 mdash minus97 plusmn 45
After observThigh minus2507 plusmn 45 102 plusmn 784 lowast minus142 plusmn 56
Calf minus248 plusmn 57 minus06 plusmn 53 lowast minus1042 plusmn 55
Foot minus152 plusmn 52 minus42 plusmn 27 mdash minus1015 plusmn 42
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 8 Mean value of isothermal-area above 119879max at rest (AURP) changes
Isothermal-area above 119879max at rest [] Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampnon-DN
After DN Thigh 0 plusmn 00 212 plusmn 265 lowastlowastlowast 114 plusmn 08
Calf 0 plusmn 00 482 plusmn 107 lowastlowastlowast 003 plusmn 002
After observ Thigh 0 plusmn 00 264 plusmn 333 lowastlowastlowast 125 plusmn 08
Calf 0 plusmn 00 663 plusmn 14 lowastlowastlowast 004 plusmn 003
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 9 Validity and reliability of TTDN components for 119879sk changes
119879sk [∘C] TTDN phases Area Sensitivity [] Specificity [] Average [∘C] Min [∘C] Max [∘C] PPV [] ICC 120581
MaximumAfter DN Thigh 100 313 119 minus02 26 577 0622 0702
Calf 100 842 066 minus08 21 667 0422 0786
After observ Thigh 100 167 129 minus01 27 545 0670 0556Calf 100 500 065 minus07 195 857 0440 0680
AverageAfter DN Thigh 100 100 099 004 195 100 0400 0880
Calf 100 100 045 minus04 13 100 0511 0902
After observ Thigh 100 846 111 009 22 750 0333 0786Calf 100 944 044 minus06 15 857 0422 0845
Table 10 Validity and reliability of TTDN components for isothermal-area changes
Isothermal-area TTDN phases Area Sensitivity [] Specificity [] Mean [] Min [] Max [] PPV [] ICC 120581
AURP (above 119879max at rest)After DN Thigh 100 100 212 06 418 100 0689 0938
Calf 100 100 48 minus35 131 100 0778 0956
After observ Thigh 100 100 264 06 522 100 0644 0929Calf 100 100 66 minus44 177 100 0778 0956
Below 119879max at rest
After DN Thigh 100 00 758 minus527 678 500 0778 0656Calf 100 200 337 minus407 474 778 0556 0707
After observ Thigh 100 00 102 minus597 618 500 0778 0656Calf 100 750 minus059 minus419 407 875 0511 0827
Below + above 119879max at rest
After DN Thigh 100 222 288 minus293 869 682 0578 0696Calf 100 370 819 minus136 628 778 0578 0782
After observ Thigh 100 00 1987 minus55 453 483 0733 0643Calf 100 782 605 minus127 576 794 0644 0847
BioMed Research International 9
whether the authors of the previous study who confirmedTrPs-related vasoconstriction really stimulated TrPs On theother hand maybe the type of TrPs (latent TrPs) or regionof IRT observation (upper extremity) or type of noxiousstimulation (glutamate injection) can explain contrary results[8 9] Further studies considering both active and latent TrPsdifferent regions of the body and so forth are required
The New IdeamdashIsothermal-Area Calculation The standardusage of IRT in medicine is based on mean temperature andstandard deviation within the fixed region of interest (ROi)as well as the visualized interpretation of the thermogramwhere each temperature value (or a group of similar values)is attributed to a specified color The color variation is theonly indirect analysis and this type of interpretation is limitedto the physician trained in thermology Additionally theuse of spot temperature measurements or observation ofselected values of 119879max or 119879avr may not produce the expectedoutcomes and the results obtained this way may differ a lotfrom the real situation In summary the comparison of 119879avrof ROi is performed without considering the size of ROiThus an error resulting from the statistical interpretation ispossible These facts can explain the controversies aroundthe merit of IRT measurement in medicine However it hasbeen postulated that considering the number of pixels inthe observed ROi that is the qualitative evaluation of forexample its size and shape together with 119879avr can lead to anobjective interpretation of the results [16]
TTDN is the method which allows assessing the thermo-gram in this recommended wayThemeasurement of the sizeof isothermal-areas in the present study guarantees the pre-cise results of the occurring process of thermal phenomenaappearing on the human skin In addition TTDN analysisaccounts for 100 of the information recorded on a singlethermogram
The next innovativeness of TTDN apart from calculatingthe size of ROi is the possibility of showing vasomotorreactions in TrPs referred pain area The results are easyto interpret and not limited by a physician experience Themeasurement of the size of isothermal-areas in the presentstudy guarantees the precise results of the occurring processof thermal phenomena appearing on the human skin Inaddition the validity of TTDN confirmed the most discrimi-natory indicators for TrPs presence119879avr and isothermal-areacalculation
5 Summary and Limitations of the Study
We are unaware of any other published studies regardingthe validity and reliability of TrPs noxious stimulation byDN under IRT control to support the diagnosis of TrPsThe results of the present study were subject to the rigorand diagnostic protocol of the standards thermographicprocedure Moreover side-to-side 119879sk comparison of thepatient at rest performed before the main procedure allowedexcluding pain states related to sympathetic nervous systemactivity
TTDN seems to be a promising tool for objective TrPsconfirmation However this is the first study of this type
and the validation of TTDN on other muscles with TrPs andsome studies presenting a group with active and latent TrPsof the same muscle are required After a series of studies thatwould give the same results TTDN could be claimed as a newobjectivemethod for TrPs confirmation where DN is possibleto perform
The limitations of this study are the strong inclusion andexclusion criteria for the confirmation of gluteus minimusmuscle TrPs This muscle should be checked by TTDN whenTrPs confirmation is based on tender point presence whichprovoked typical referred pain when needle encounteredTrPs
Moreover Travell and Simons claimed that autonomicphenomena (including vasomotor reaction) within TrPsreferred pain area are limited to severe active TrPs onlyIn the present study TrPs-positive sciatic patients can beassumed to probably have severe active TrPs due to thechronicity and length of the referred pain pattern evokedby snapping palpation However the severity of active TrPsstill remains only a theoretical consideration because thereare no criteria for distinguishing the severity of active TrPs[26] Additionally other TrPs for example within the uppertrapezius muscle should be examined by TTDN to answerthe question if every TrPs present AURP is accompanied by119879avr increase
Finally the present study is limited by the lack of inter-rater reliability of TTDN
6 Conclusion
TTDN is valid and reliable for 119879avr and AURP measurementto support TrPs diagnostic criteria for the gluteus minimusmuscle when a digitally evoked referred pain pattern ispresented In the light of clinical division TTDN results indi-cate skin temperature increase for TrPs-positive contrary todecrease for TrPs-negative chronic sciatica patients and smallchanges (both increasedecrease) for healthy volunteers
Conflict of Interests
The authors declare no conflict of interests especially regard-ing patent application
Authorsrsquo Contribution
All authors listed have contributed substantially to the paperElzbieta Skorupska contributed conception and design ofthe work acquisition of data interpretation of data anddrafting the paper Michał Rychlik contributed Conceptionand design of the work acquisition of data analysis of dataand drafting the paper Włodzimierz Samborski contributedcorrection and final approval of the resubmitted version
Acknowledgments
The authors gratefully acknowledge the critical reading andcorrection of this paper by Malgorzata Mankowska Thiswork was partially supported by the Polish National ScienceCentre Grant no N N404 268339 and Poznan University ofMedical Sciences
10 BioMed Research International
References
[1] R SWeiner PainManagement A Practical Guide for CliniciansCRC Press LLC 6th edition 2002
[2] S A Skootsky B Jaeger and R K Oye ldquoPrevalence ofmyofascial pain in general internal medicine practicerdquoWesternJournal of Medicine vol 151 no 2 pp 157ndash160 1989
[3] Q Chen S Bensamoun J R Basford J M Thompsonand K-N An ldquoIdentification and quantification of myofascialtaut bands with magnetic resonance elastographyrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1658ndash1661 2007
[4] S Sikdar J P Shah T Gebreab et al ldquoNovel applications ofultrasound technology to visualize and characterize myofascialtrigger points and surrounding soft tissuerdquo Archives of PhysicalMedicine and Rehabilitation vol 90 no 11 pp 1829ndash1838 2009
[5] J G Travell andD G SimonsMyofascial Pain andDysfunctionThe Trigger PointManual vol 1WilliamsampWilkins BaltimoreMd USA 2nd edition 1999
[6] J G Travell andD G SimonsMyofascial Pain andDysfunctionTheTrigger PointManual vol 2 LippincottWilliamsampWilkinsBaltimore Md USA 1993
[7] H-Y Ge C Fernandez-de-las-Penas and L Arendt-NielsenldquoSympathetic facilitation of hyperalgesia evoked from myofas-cial tender and trigger points in patients with unilateral shoul-der painrdquoClinical Neurophysiology vol 117 no 7 pp 1545ndash15502006
[8] Y Kimura H-Y Ge Y Zhang M Kimura H Sumikura andL Arendt-Nielsen ldquoEvaluation of sympathetic vasoconstrictorresponse following nociceptive stimulation of latent myofascialtrigger points in humansrdquo Acta Physiologica vol 196 no 4 pp411ndash417 2009
[9] Y Zhang H-Y Ge S-W Yue Y Kimura and L Arendt-Nielsen ldquoAttenuated Skin blood flow response to nociceptivestimulation of latent myofascial trigger pointrdquo Archives ofPhysical Medicine and Rehabilitation vol 90 no 2 pp 325ndash3322009
[10] E Skorupska M Rychlik W Pawelec and W Samborski ldquoDryneedling related short-term vasodilation in chronic sciaticaunder infrared thermovisionrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 214374 10 pages2015
[11] E SkorupskaM Rychlik andW Samborski ldquoIntensive vasodi-latation in the sciatic pain area after dry needlingrdquo BMCComplementary and Alternative Medicine vol 15 article 722015
[12] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoTrigger point-related sympathetic nerve activity inchronic sciatic leg pain a case studyrdquo Acupuncture in Medicinevol 32 no 5 pp 418ndash422 2014
[13] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoIntensive short-term vasodilation effect in the painarea of sciatica patientsmdashcase studyrdquo BMC Research Notes vol7 no 1 article 620 2014
[14] G Affaitati A Fabrizio A Savini et al ldquoA randomizedcontrolled study comparing a lidocaine patch a placebo patchand anesthetic injection for treatment of trigger points inpatients with myofascial pain syndrome evaluation of pain andsomatic pain thresholdsrdquoClinicalTherapeutics vol 31 no 4 pp705ndash720 2009
[15] D G Simons ldquoReview of enigmatic MTrPs as a common causeof enigmatic musculoskeletal pain and dysfunctionrdquo Journal
of Electromyography and Kinesiology vol 14 no 1 pp 95ndash1072004
[16] F S Nahm ldquoInfrared thermography in pain medicinerdquo KoreanJournal of Pain vol 26 no 3 pp 219ndash222 2013
[17] A C S Costa A V D Filho A C Packer and D Rodrigues-Bigaton ldquoIntra and inter-rater reliability of infrared image anal-ysis of masticatory and upper trapezius muscles in women withand without temporomandibular disorderrdquo Brazilian Journal ofPhysical Therapy vol 17 no 1 pp 24ndash31 2013
[18] M McCoy I Campbell P Stone C Fedorchuk S Wijayawar-dana and K Easley ldquoIntra-examiner and inter-examiner repro-ducibility of paraspinal thermographyrdquo PLoS ONE vol 6 no 2Article ID e16535 2011
[19] D S Haddad M L Brioschi and E S Arita ldquoThermographicand clinical correlation of myofascial trigger points in themasticatory musclesrdquo Dentomaxillofacial Radiology vol 41 no8 pp 621ndash629 2012
[20] S J Gulevich T D Conwell J Lane et al ldquoStress infraredtelethermography is useful in the diagnosis of complex regionalpain syndrome type I (formerly reflex sympathetic dystrophy)rdquoClinical Journal of Pain vol 13 no 1 pp 50ndash59 1997
[21] G Wasner J Schattschneider and R Baron ldquoSkin temperatureside differencesmdasha diagnostic tool for CRPSrdquo Pain vol 98 no1-2 pp 19ndash26 2002
[22] E J Park K R Han Y J Chae W H Jeong and C KimldquoEffectiveness of cold stress thermography in the diagnosis ofcomplex of regional pain syndrome type 1rdquoThe Korean Journalof Pain vol 19 pp 159ndash163 2006
[23] E Skorupska M Rychlik and W Pawelec ldquoSkeletal striatedmuscle examination instrument amp new method of myofascialpain diagnosis based on the use of the instrumentrdquo Patentapplication No P-403467 Silver Medal 14ndash16 November 2013Brussels Innova the International Exhibition of InnovationEntrepreneurship and New Technologies Bronze Medal at theConcours Lepine International Paris 3004-11052014 FranceGoldMedal at the Euroinvent EuropeanExhibition ofCreativityand Innovation 22-24052014 Iasi Romania Gold Medal withDistinction at the 29th Invention and New Product ExpositionINPEX 18ndash20062014 Pittsburgh Pa USA
[24] R G Schwartz R Elliott G S Goldberg et al ldquoThe AmericanAcademy of Thermology Guidelines for neuromusculoskeletalthermographyrdquoThermology International vol 16 pp 5ndash9 2006
[25] J Dommerholt and C Fernandez-de-las-Penas Trigger PointDry Needling An Evidence and Clinical-Based ApproachChurchill Livingstone Elsevier 2013
[26] C Z Hong Braddom Physical Medicine and Rehabilitationin Muscle Pain Syndrome Elsevier New York NY USA 4thedition 2011
[27] S Mense D G Simons and I J Russell Muscle PainUnderstanding Its Nature Diagnosis and Treatment LippincottWilliams ampWilkins 2001
[28] R Rolke ldquoPseudoradicular and radicular low-back painmdashadisease continuum Rather than different entities Reply to theletters by Leffler and Hansson and by Van Boxem et alrdquo Painvol 135 pp 311ndash316 2008
[29] J M Bland and D G Altman ldquoStatistical methods for assessingagreement between two methods of clinical measurementrdquoTheLancet vol 1 no 8476 pp 307ndash310 1986
[30] D G Altman ldquoSome common problems in medical researchrdquoin Practical Statistics for Medical Research Chapman amp HallCRC Press London UK 1997
BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
Table 1 Isothermal-area analysis related to TTDN
Initial state After DN After observation
119879min at restIf isothermal-area decreases below 119879min at restmdashthe confirmation of AuRP (vasoconstriction)
Low Tsk isothermal-area (15∘C above 119879min at rest)
119879max at restHigh Tsk isothermal-area (15∘C below 119879max at rest)
If isothermal-area increases above 119879max at restmdashthe confirmation of AuRP (vasodilatation)
Table 2 Definitions of validity elements [24 25]
Validity elements Definition EquationSensitivity Proportion of the positive values that the test correctly identifies 119886 (119886 + 119888) times 100Specificity Proportion of the negative values that the test correctly identifies 119886 (119887 + 119889) times 100Positive predictive value (PPV) Proportion of the patients with positive test results who are correctly diagnosed 119886 (119886 + 119887) times 100Negative predictive value (PNV) Proportion of the patients with negative test results who are correctly diagnosed 119889 (119888 + 119889) times 100
calculated The size of each isothermal-area was recalculatedfrom cm2 to the percentage value
TTDN for Gluteus Minimus Trigger PointsmdashAdditional Infor-mationThe area to be observed by IRTwas chosen accordingto the gluteus minimus referred pain pattern The examinedpatients were positioned on the side on the uninvolvedextremity with the hip and knee flexed The muscle wasneedled with flat palpation perpendicular to the musclealong the counter of the iliac crest Strong depression ofthe subcutaneous tissue was applied in order to reduce thedistance of the skin from the muscle Depth of penetrationdepended on the amount of adipose tissue [25] Therapeuticneedling was performed with 030mm diameter 60mm longsterile acupuncture needles SE L (Serin Corp ShizuokaJapan) Each needle was packed separately
23 Statistical Analysis
TTDN Results Dependent on Clinical Division The chronicsciatica subjects and healthy volunteers were compared withtrigger points coexistence being the differentiating criterionFor the strong evidence of data presented the significancelevel was set based on exact tests not on the default asymp-totic method Exact two-way Mann-Whitney 119880 tests wereperformed in order to ensure that data were representativeof the whole population of possible data values Tests wereapplied to compare the differences for maximum minimumand average skin temperatures and the percentage size ofisothermal-area for the state after dry needling and secondlyfor the postobservation state Values figures and tables inthe text were expressed as plusmn standard error of the mean (SE)Significance level was set at 119901 lt 005 IBM SPSS Statisticsversion 2010158401015840 was used
Validity and Reliability of TTDN A validity analysis wasperformed to confirm the validity of TTDN towards sensitiv-ity and specificity of the obtained results (skin temperaturechanges and percentage size of vasomotor responses) Thecomponents of validity that were used in this study includesensitivity and specificity as well as positive and negative
predictive values Tables 2 and 3 provide definitions andexplanations for the components of validity [30 31]
Reliability of the TTDN Method Test-retest was used tocheck the reliability of TTDN according to the Guidelinesfor Evaluating and Expressing the Uncertainty of NISTMeasurement Results TTDN was performed using the sameexperimental tools the same observer the same measur-ing instrument used under the same conditions the samelocation and repetition over a short period of time on thesame patient Intraclass correlation coefficients (ICC) for test-retest reliability (intraobserved variability) were calculatedto illustrate the differences between repeated measures [29]Intraclass correlation coefficients above 090 were consideredexcellent values form 075 to 090 were considered good andbelow 075 considered poor to moderate [32]
To overcome the problem of tests agreement the 120581coefficient was usedThe guidelines by Landis and Koch wereused to interpret the obtained 120581 values and are presented inTable 4 [33]
3 Results
31 TTDN Results Dependent on Clinical Division Amongthe sciatica group only two patients (both TrPs-positivesubjects) felt pain going to the foot as a daily complaintDuringTTDN dry needling related pain sensation consistentwith gluteus minimus referred pain was confirmed for TrPs-positive exclusively Among TrPs-positive sciatica subjectsDN related pain sensation on the thigh during TTDN wasconfirmed for every subject in all three sessionsDN reactivityfor the calf for the three sessions was 100 80 and 733respectively Two TrPs-positive subjects complained of thedaily pain of the foot but during the procedure they did notreport needle sensation going to the foot
Skin Temperature Changes Related to TTDN TTDN con-firmed 119879sk and isothermal-area changes for every subjectThe exact two-way Mann-Whitney 119880 tests confirmed signif-icant increase of 119879max(thighcalf foot) and 119879avr(thighcalf) for TrPs-positive sciatic group as compared to TrPs-negative sciatic
BioMed Research International 5
Table 3 Validity elements [24 25]
Test performed
Results detected by the test True picture TotalPatient has the condition Patient is clear
Positive test A (true positive) B (false positive) A + B (total positive tests)Negative test C (false negative) D (true negative) C + D (total negative tests)Total Total subjects diagnosed with the condition Total subjects without the condition 119873 (total number tested)
Table 4 Landis and Koch guidelines for 120581 interpretation [29]
120581 value Strength of agreementlt000 Poor agreement000ndash020 Slight agreement021ndash040 Fair agreement041ndash060 Moderate agreement061ndash080 Substantial agreement081ndash100 Almost perfect agreement100 Perfect agreement
patients and heathy volunteers (all 119901 lt 005) (Tables 5and 6) The sciatic group presented contrary 119879sk changesdependent on TrPs and DN related referred pain presenceFor TrPs-negative 119879sk decrease contrary to 119879sk increase ofTrPs-positive was observed
Isothermal-Area Changes Related to TTDN None of TrPs-positive subjects presented vasoconstriction or any signifi-cant changes of the low 119879sk isothermal-area and 119879sk decreaseSignificant 119879sk and isothermal-area changes for every TrPs-positive sciatica subject were confirmed
The exact two-way Mann-Whitney 119880 tests confirmed asignificant increase of the observed isothermal-area (calcu-lated together AURP and high119879sk isothermal-area) for TrPs-positive sciatica subjects compared to TrPs-negative sciaticapatients and healthy volunteers (all 119901 lt 005) for both post-DN and postobservation phases (every 119901 lt 005) Afterdividing the isothermal-area into high 119879sk isothermal-areaand AURP (shown in Figure 1) the results were as follows
The exact two-way Mann-Whitney 119880 tests confirmed asignificant increase of the high 119879sk isothermal-area (thighand calf) for TrPs-positive compared toTrPs-negative sciaticasubjects (119901 lt 005) but not to healthy volunteers (Table 7)The significant increase of AURP (vasodilatation) for TrPs-positive compared to TrPs-negative and healthy volunteerswas confirmed (The exact two-way Mann-Whitney 119880 testsevery 119901 lt 005) The average value of the percentage increaseof AURP was shown in Table 8
32 Validity and Reliability of TTDN There were consid-erable differences detected in the results of TTDN when itwas performed on the non-TrPs sciatic group TrP-positivesciatic group and non-TrPs healthy volunteers The agree-ment between TTDN and TrPs diagnosis was almost perfect(according to 120581) for changes of119879avr and isothermal-area above119879max at rest of the thigh and calf (Tables 9 and 10) In terms
of validity components TTDN was useful for identifyingthe positive values of 119879max changes and isothermal-area(below 119879max at rest) or full AURP (namely below and above119879max at rest calculated together) changes but was not useful foridentifying the negative values (specificity) Although 119879maxand isothermal-area below 119879max at rest or full AURP have highsensitivity the low specificity does not allow recommendingtheir diagnostic value
4 Discussion
The results of skin temperature (both 119879avr and 119879max) andisothermal-area significantly differ for TrPs-positive sciaticasubjects compared to non-TrPs sciatica subjects and healthyvolunteers (119901 lt 005 Tables 5ndash8) which is consistent withthe previous study involving sciatica subjects only [10 11]However the main purpose of the present study was tocheck the validity and reliability of TTDN This new IRTmethod was assumed to allow observing vasomotor andtemperature reactions related to TrPs andwas validated for itsability to distinguish active TrPs from non-TrPs of the gluteusminimus muscle and non-TrPs of healthy volunteers It wasfound that TTDN identifies active gluteus minimus TrPs forevery positive subjectThemost discriminatory indicators forTrPs presence were 119879avr increase and the presence of high119879sk increase above 119879max (isothermal-area defined as AURPTables 9 and 10) in the area where dry needling intensifiedpain The results showed that TTDN validly measured 119879avrchanges and the presence of AURP (grey picture in Figure 1)for active TrPs of the gluteus minimus muscle The ICCresults confirmedmoderate reliability forAURPpresence andpoor to moderate for 119879avr increase However these two typesof thermogram analysis showed almost prefect agreementaccording to 120581 (Tables 9 and 10) which is recommended as amore suitablemeasure of agreement amongnonexchangeableobservers in comparison with ICC It seems that AURP andsignificant 119879avr increase can objectively support Travell andSimonsrsquo clinical criteria for active TrPs within the gluteusminimus muscle when referred pain is evoked by snappingpalpation [5 6] However similar tendency for AURP and119879avr for some of the healthy volunteers was observed (AURPnot exceeding 25 with insignificant 119879avr of +014
∘C) (Tables6 and 8) and small changes can be explained by 119879sk differ-ences in time due to the physiological variability of blood flow[34]
IRT reliability was checked for the muscle examinationand was found more reliable compared to the present studybut they examined the thermograms of the subjects at rest [1718] The quantitative measurement of the percentage value of
6 BioMed Research International
Table 5 Mean value of maximum temperature changes
119879max Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus012 plusmn 016 121 plusmn 018 lowastlowastlowast 09 plusmn 014
Calf minus047 plusmn 015 066 plusmn 019 lowastlowastlowast minus005 plusmn 013
Foot minus024 plusmn 014 01 plusmn 011 mdash minus005 plusmn 015
After observThigh 012 plusmn 018 129 plusmn 018 lowastlowastlowast 025 plusmn 013
Calf minus047 plusmn 015 065 plusmn 017 lowastlowastlowast minus018 plusmn 013
Foot minus029 plusmn 016 minus02 plusmn 008 mdash minus023 plusmn 014
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 6 Mean value of average temperature changes
119879avr Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus051 plusmn 011 099 plusmn 012 lowastlowastlowast 007 plusmn 012
Calf minus07 plusmn 011 045 plusmn 011 lowastlowastlowast minus025 plusmn 010
Foot minus056 plusmn 010 minus03 plusmn 07 lowastlowastlowast minus045 plusmn 011
After observThigh minus038 plusmn 014 113 plusmn 013 lowastlowastlowast 015 plusmn 012
Calf minus066 plusmn 012 044 plusmn 014 lowastlowastlowast minus025 plusmn 011
Foot minus053 plusmn 014 minus007 plusmn 008 lowastlowastlowast minus045 plusmn 010
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
isothermal-area changes is presented for the first time andallowed observing the changes of a specific subarea of definedtemperature very precisely However it should be underlinedthat it was possible because dry needling provoked intensive119879sk changes (Figure 1) which again is unusual compared toacupuncture studieswhere postneedling stimulationwas lim-ited to the site of needling [35 36] TTDN allowed observingdynamic thermogram changes due to the stimulation by dryneedling and the fact that DN is a treatment technique forTrPs release [37]The difference between the first and the lastsession could have resulted from the therapeutic DN effectapart from the skin blood flow variability
Moreover it should be underlined that the strong inclu-sion and exclusion criteria for TrPs confirmation did notallow claiming that TTDN is a new objective method forevery gluteus minimus TrP confirmation It has been claimedthat digitally evoked referred pain pattern from the gluteusminimus muscle is rare and for the diagnostic purposes thepresence of a tender point and needle encouraged referredpain were postulated as diagnostic criteria for that muscle
The diagnostic criteria established for the gluteus min-imus muscle in the present study were as severe as possiblebecause it has been lastly postulated that the methodologicalquality of the majority of studies conducted for the purposeof establishing trigger point reproducibility is generally poor[38] Tough et al [39] indicated that only 15 of authorsused the combination of a tender spot in a taut band ofa skeletal muscle patientsrsquo pain recognition predicted painreferral pattern and local twitch response Thanks to TrPsdiagnostic criteria used in the present study the diagnosisof TrPs presence cannot be questioned and additionally the
consistency condition regarding the referred pain presenceminimum to the calf ensures the group homogeneity Ofcourse the choice of the gluteus minimus muscle for the firstuse of TTDN can be questioned However an advantage ofthis choice is the size of the referred pain pattern which isone of the most extensive froms all of the TrPs referred painpatterns Thus it was predicted that the observed vasomotorreactions if present should be probably the widest and easilydetectable by IRT
TTDN Results in the Light of the Previous Studies The use ofthermography is not a new way for TrPs evaluation Most ofthe authors tried to correlate the localization of TrPs with hotspots on the thermogram [16] Brioschi et al [40] analyzedmost of the available studies on the subject and concludedthat IRT findings represent an objective means of document-ing TrPs if the thermogram is analyzed by an experiencedphysician skilled in clinical thermology together with clinicalevaluation of the patient However in one of the oldeststudies Swerdlow andDieter [41] evaluated the sensitivity andspecificity of medical thermography for the documentationof TrPs and they concluded that the localizations of TrPsand hot spots were not associated Moreover some otherauthors stated that skin temperature measurement in TrPsarea cannot be used to detect myofascial tender spots [42]Additionally in the latest review regarding IRT application toTrPs it has been stated that there are few studies evaluatingthe accuracy and reliability of infrared thermography for thediagnosis and assessment of TrPs In the few studies presentthere is no agreement on skin temperature patterns in thepresence of TrPs [43]
BioMed Research International 7
448
419
390
362
333
304
275
246
217451
423
394
365
336
307
279
250
221
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
446
412
378
344
310
276
242
208
175446
412
378
344
310
276
242
208
175
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
450
418
387
355
324
293
261
230
199
450
418
387
355
324
293
261
230
199
450
416
382
349
315
282
248
214
181450
416
382
349
315
282
248
214
181
Case 1 Case 2a b c a b c
Ia
Ib
IIa
IIb
IIIa
IIIb
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
Figure 1 TTDN related thermograms presenting temperature reaction measured on skin surface of TrPs and non-TrPs sciatica patients andhealthy volunteers In rows I two cases of TrPs-negative sciatica II two cases of TrPs-positive sciatica and III two cases of healthy volunteerswere shown In rows Ia IIa and IIIa full thermogramwas presented In rows Ib IIb and IIIb the picture of the isothermal-area above119879max at restcalled AURP was shown (visualization of the vasodilation) In columns (a) Before TTDN (initial state) (b) state immediately after DN and(c) state immediately after observation were presented
IRT was also used for TrPs related referred pain areaexamination Although Brioschi et al [44] evaluated 304chronic myofascial pain patients using IRT before and afterDN or anesthetic infiltration they found that referred areaswere thermally asymmetric andKimura et al [8] confirmed asignificant decrease in 119879sk over time after glutamate injection(nociceptive stimulation) in latent TrPs (119901 lt 005) theusefulness of IRT for postnoxious stimulation of latent TrPsreferred pain observation was contradicted by Zhang et al[9] On the other hand one of the oldest studies on thesubject presents results similar to the present study Kruse Jrand Christiansen [45] observed referred pain pattern by IRTwhen palpation pressure over TrPs lasted around 1 minuteInitially they observed a small 119879sk increase followed by asignificant decrease in the area of the observed referredpain The DN stimulation is a much more severe type ofTrPs stimulation compared to pressure and the time ofstimulation in the present study was ten times longer Itcan be hypothesized that a stronger noxious stimulationcould provoke much more intensive 119879sk increase and maybeKruse Jr and Christiansen [45] observed the same vasomotorreactions but of a weak and short form Additionally another
difference between the studies is the localization of visiblethermal response They reported visible 119879sk changes onthe thermogram more extensive than that of the reportedreferred pain during TrPs compression contrary to thepresent study where AURP localization is limited precisely tothe area where DN provoked pain during TTDN (Figure 1)The thermogram analysis before isothermal-area calculationwas based on the indirect thermogram analysis where theexaminer had to distinguish subtle color differences Theisothermal-area calculation together with the thermogram ofAURP (gray picture Figure 1) is a nonquestionable proof ofsignificant vasomotor changes and can be easily interpretedby everyone
Interestingly the analysis of 119879avr changes in the wholegroup of subjects in the present study (Table 6) clearlyindicated 119879avr decrease for non-TrPs healthy volunteersand needle insensitive foot of TrPs-positive sciatica subjectscontrary to 119879avr increase of DN reactive subarea of TrPs-positive subjects Moreover when the thermograms of non-TrPs sciatica subjects were observed some of them presenteddiscreet vasoconstriction feature (Figure 1) and 119879sk decrease(Tables 5 and 6) These results allow putting the question of
8 BioMed Research International
Table 7 Mean value of isothermal-area below 119879max at rest changes
Isothermal-area below 119879max at rest [] Sciatica patients Healthy volunteersTTDN Phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus276 plusmn 46 76 plusmn 78 lowast minus28 plusmn 52
Calf minus265 plusmn 52 34 plusmn 57 lowast minus85 plusmn 45
Foot minus139 plusmn 513 minus39 plusmn 29 mdash minus97 plusmn 45
After observThigh minus2507 plusmn 45 102 plusmn 784 lowast minus142 plusmn 56
Calf minus248 plusmn 57 minus06 plusmn 53 lowast minus1042 plusmn 55
Foot minus152 plusmn 52 minus42 plusmn 27 mdash minus1015 plusmn 42
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 8 Mean value of isothermal-area above 119879max at rest (AURP) changes
Isothermal-area above 119879max at rest [] Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampnon-DN
After DN Thigh 0 plusmn 00 212 plusmn 265 lowastlowastlowast 114 plusmn 08
Calf 0 plusmn 00 482 plusmn 107 lowastlowastlowast 003 plusmn 002
After observ Thigh 0 plusmn 00 264 plusmn 333 lowastlowastlowast 125 plusmn 08
Calf 0 plusmn 00 663 plusmn 14 lowastlowastlowast 004 plusmn 003
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 9 Validity and reliability of TTDN components for 119879sk changes
119879sk [∘C] TTDN phases Area Sensitivity [] Specificity [] Average [∘C] Min [∘C] Max [∘C] PPV [] ICC 120581
MaximumAfter DN Thigh 100 313 119 minus02 26 577 0622 0702
Calf 100 842 066 minus08 21 667 0422 0786
After observ Thigh 100 167 129 minus01 27 545 0670 0556Calf 100 500 065 minus07 195 857 0440 0680
AverageAfter DN Thigh 100 100 099 004 195 100 0400 0880
Calf 100 100 045 minus04 13 100 0511 0902
After observ Thigh 100 846 111 009 22 750 0333 0786Calf 100 944 044 minus06 15 857 0422 0845
Table 10 Validity and reliability of TTDN components for isothermal-area changes
Isothermal-area TTDN phases Area Sensitivity [] Specificity [] Mean [] Min [] Max [] PPV [] ICC 120581
AURP (above 119879max at rest)After DN Thigh 100 100 212 06 418 100 0689 0938
Calf 100 100 48 minus35 131 100 0778 0956
After observ Thigh 100 100 264 06 522 100 0644 0929Calf 100 100 66 minus44 177 100 0778 0956
Below 119879max at rest
After DN Thigh 100 00 758 minus527 678 500 0778 0656Calf 100 200 337 minus407 474 778 0556 0707
After observ Thigh 100 00 102 minus597 618 500 0778 0656Calf 100 750 minus059 minus419 407 875 0511 0827
Below + above 119879max at rest
After DN Thigh 100 222 288 minus293 869 682 0578 0696Calf 100 370 819 minus136 628 778 0578 0782
After observ Thigh 100 00 1987 minus55 453 483 0733 0643Calf 100 782 605 minus127 576 794 0644 0847
BioMed Research International 9
whether the authors of the previous study who confirmedTrPs-related vasoconstriction really stimulated TrPs On theother hand maybe the type of TrPs (latent TrPs) or regionof IRT observation (upper extremity) or type of noxiousstimulation (glutamate injection) can explain contrary results[8 9] Further studies considering both active and latent TrPsdifferent regions of the body and so forth are required
The New IdeamdashIsothermal-Area Calculation The standardusage of IRT in medicine is based on mean temperature andstandard deviation within the fixed region of interest (ROi)as well as the visualized interpretation of the thermogramwhere each temperature value (or a group of similar values)is attributed to a specified color The color variation is theonly indirect analysis and this type of interpretation is limitedto the physician trained in thermology Additionally theuse of spot temperature measurements or observation ofselected values of 119879max or 119879avr may not produce the expectedoutcomes and the results obtained this way may differ a lotfrom the real situation In summary the comparison of 119879avrof ROi is performed without considering the size of ROiThus an error resulting from the statistical interpretation ispossible These facts can explain the controversies aroundthe merit of IRT measurement in medicine However it hasbeen postulated that considering the number of pixels inthe observed ROi that is the qualitative evaluation of forexample its size and shape together with 119879avr can lead to anobjective interpretation of the results [16]
TTDN is the method which allows assessing the thermo-gram in this recommended wayThemeasurement of the sizeof isothermal-areas in the present study guarantees the pre-cise results of the occurring process of thermal phenomenaappearing on the human skin In addition TTDN analysisaccounts for 100 of the information recorded on a singlethermogram
The next innovativeness of TTDN apart from calculatingthe size of ROi is the possibility of showing vasomotorreactions in TrPs referred pain area The results are easyto interpret and not limited by a physician experience Themeasurement of the size of isothermal-areas in the presentstudy guarantees the precise results of the occurring processof thermal phenomena appearing on the human skin Inaddition the validity of TTDN confirmed the most discrimi-natory indicators for TrPs presence119879avr and isothermal-areacalculation
5 Summary and Limitations of the Study
We are unaware of any other published studies regardingthe validity and reliability of TrPs noxious stimulation byDN under IRT control to support the diagnosis of TrPsThe results of the present study were subject to the rigorand diagnostic protocol of the standards thermographicprocedure Moreover side-to-side 119879sk comparison of thepatient at rest performed before the main procedure allowedexcluding pain states related to sympathetic nervous systemactivity
TTDN seems to be a promising tool for objective TrPsconfirmation However this is the first study of this type
and the validation of TTDN on other muscles with TrPs andsome studies presenting a group with active and latent TrPsof the same muscle are required After a series of studies thatwould give the same results TTDN could be claimed as a newobjectivemethod for TrPs confirmation where DN is possibleto perform
The limitations of this study are the strong inclusion andexclusion criteria for the confirmation of gluteus minimusmuscle TrPs This muscle should be checked by TTDN whenTrPs confirmation is based on tender point presence whichprovoked typical referred pain when needle encounteredTrPs
Moreover Travell and Simons claimed that autonomicphenomena (including vasomotor reaction) within TrPsreferred pain area are limited to severe active TrPs onlyIn the present study TrPs-positive sciatic patients can beassumed to probably have severe active TrPs due to thechronicity and length of the referred pain pattern evokedby snapping palpation However the severity of active TrPsstill remains only a theoretical consideration because thereare no criteria for distinguishing the severity of active TrPs[26] Additionally other TrPs for example within the uppertrapezius muscle should be examined by TTDN to answerthe question if every TrPs present AURP is accompanied by119879avr increase
Finally the present study is limited by the lack of inter-rater reliability of TTDN
6 Conclusion
TTDN is valid and reliable for 119879avr and AURP measurementto support TrPs diagnostic criteria for the gluteus minimusmuscle when a digitally evoked referred pain pattern ispresented In the light of clinical division TTDN results indi-cate skin temperature increase for TrPs-positive contrary todecrease for TrPs-negative chronic sciatica patients and smallchanges (both increasedecrease) for healthy volunteers
Conflict of Interests
The authors declare no conflict of interests especially regard-ing patent application
Authorsrsquo Contribution
All authors listed have contributed substantially to the paperElzbieta Skorupska contributed conception and design ofthe work acquisition of data interpretation of data anddrafting the paper Michał Rychlik contributed Conceptionand design of the work acquisition of data analysis of dataand drafting the paper Włodzimierz Samborski contributedcorrection and final approval of the resubmitted version
Acknowledgments
The authors gratefully acknowledge the critical reading andcorrection of this paper by Malgorzata Mankowska Thiswork was partially supported by the Polish National ScienceCentre Grant no N N404 268339 and Poznan University ofMedical Sciences
10 BioMed Research International
References
[1] R SWeiner PainManagement A Practical Guide for CliniciansCRC Press LLC 6th edition 2002
[2] S A Skootsky B Jaeger and R K Oye ldquoPrevalence ofmyofascial pain in general internal medicine practicerdquoWesternJournal of Medicine vol 151 no 2 pp 157ndash160 1989
[3] Q Chen S Bensamoun J R Basford J M Thompsonand K-N An ldquoIdentification and quantification of myofascialtaut bands with magnetic resonance elastographyrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1658ndash1661 2007
[4] S Sikdar J P Shah T Gebreab et al ldquoNovel applications ofultrasound technology to visualize and characterize myofascialtrigger points and surrounding soft tissuerdquo Archives of PhysicalMedicine and Rehabilitation vol 90 no 11 pp 1829ndash1838 2009
[5] J G Travell andD G SimonsMyofascial Pain andDysfunctionThe Trigger PointManual vol 1WilliamsampWilkins BaltimoreMd USA 2nd edition 1999
[6] J G Travell andD G SimonsMyofascial Pain andDysfunctionTheTrigger PointManual vol 2 LippincottWilliamsampWilkinsBaltimore Md USA 1993
[7] H-Y Ge C Fernandez-de-las-Penas and L Arendt-NielsenldquoSympathetic facilitation of hyperalgesia evoked from myofas-cial tender and trigger points in patients with unilateral shoul-der painrdquoClinical Neurophysiology vol 117 no 7 pp 1545ndash15502006
[8] Y Kimura H-Y Ge Y Zhang M Kimura H Sumikura andL Arendt-Nielsen ldquoEvaluation of sympathetic vasoconstrictorresponse following nociceptive stimulation of latent myofascialtrigger points in humansrdquo Acta Physiologica vol 196 no 4 pp411ndash417 2009
[9] Y Zhang H-Y Ge S-W Yue Y Kimura and L Arendt-Nielsen ldquoAttenuated Skin blood flow response to nociceptivestimulation of latent myofascial trigger pointrdquo Archives ofPhysical Medicine and Rehabilitation vol 90 no 2 pp 325ndash3322009
[10] E Skorupska M Rychlik W Pawelec and W Samborski ldquoDryneedling related short-term vasodilation in chronic sciaticaunder infrared thermovisionrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 214374 10 pages2015
[11] E SkorupskaM Rychlik andW Samborski ldquoIntensive vasodi-latation in the sciatic pain area after dry needlingrdquo BMCComplementary and Alternative Medicine vol 15 article 722015
[12] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoTrigger point-related sympathetic nerve activity inchronic sciatic leg pain a case studyrdquo Acupuncture in Medicinevol 32 no 5 pp 418ndash422 2014
[13] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoIntensive short-term vasodilation effect in the painarea of sciatica patientsmdashcase studyrdquo BMC Research Notes vol7 no 1 article 620 2014
[14] G Affaitati A Fabrizio A Savini et al ldquoA randomizedcontrolled study comparing a lidocaine patch a placebo patchand anesthetic injection for treatment of trigger points inpatients with myofascial pain syndrome evaluation of pain andsomatic pain thresholdsrdquoClinicalTherapeutics vol 31 no 4 pp705ndash720 2009
[15] D G Simons ldquoReview of enigmatic MTrPs as a common causeof enigmatic musculoskeletal pain and dysfunctionrdquo Journal
of Electromyography and Kinesiology vol 14 no 1 pp 95ndash1072004
[16] F S Nahm ldquoInfrared thermography in pain medicinerdquo KoreanJournal of Pain vol 26 no 3 pp 219ndash222 2013
[17] A C S Costa A V D Filho A C Packer and D Rodrigues-Bigaton ldquoIntra and inter-rater reliability of infrared image anal-ysis of masticatory and upper trapezius muscles in women withand without temporomandibular disorderrdquo Brazilian Journal ofPhysical Therapy vol 17 no 1 pp 24ndash31 2013
[18] M McCoy I Campbell P Stone C Fedorchuk S Wijayawar-dana and K Easley ldquoIntra-examiner and inter-examiner repro-ducibility of paraspinal thermographyrdquo PLoS ONE vol 6 no 2Article ID e16535 2011
[19] D S Haddad M L Brioschi and E S Arita ldquoThermographicand clinical correlation of myofascial trigger points in themasticatory musclesrdquo Dentomaxillofacial Radiology vol 41 no8 pp 621ndash629 2012
[20] S J Gulevich T D Conwell J Lane et al ldquoStress infraredtelethermography is useful in the diagnosis of complex regionalpain syndrome type I (formerly reflex sympathetic dystrophy)rdquoClinical Journal of Pain vol 13 no 1 pp 50ndash59 1997
[21] G Wasner J Schattschneider and R Baron ldquoSkin temperatureside differencesmdasha diagnostic tool for CRPSrdquo Pain vol 98 no1-2 pp 19ndash26 2002
[22] E J Park K R Han Y J Chae W H Jeong and C KimldquoEffectiveness of cold stress thermography in the diagnosis ofcomplex of regional pain syndrome type 1rdquoThe Korean Journalof Pain vol 19 pp 159ndash163 2006
[23] E Skorupska M Rychlik and W Pawelec ldquoSkeletal striatedmuscle examination instrument amp new method of myofascialpain diagnosis based on the use of the instrumentrdquo Patentapplication No P-403467 Silver Medal 14ndash16 November 2013Brussels Innova the International Exhibition of InnovationEntrepreneurship and New Technologies Bronze Medal at theConcours Lepine International Paris 3004-11052014 FranceGoldMedal at the Euroinvent EuropeanExhibition ofCreativityand Innovation 22-24052014 Iasi Romania Gold Medal withDistinction at the 29th Invention and New Product ExpositionINPEX 18ndash20062014 Pittsburgh Pa USA
[24] R G Schwartz R Elliott G S Goldberg et al ldquoThe AmericanAcademy of Thermology Guidelines for neuromusculoskeletalthermographyrdquoThermology International vol 16 pp 5ndash9 2006
[25] J Dommerholt and C Fernandez-de-las-Penas Trigger PointDry Needling An Evidence and Clinical-Based ApproachChurchill Livingstone Elsevier 2013
[26] C Z Hong Braddom Physical Medicine and Rehabilitationin Muscle Pain Syndrome Elsevier New York NY USA 4thedition 2011
[27] S Mense D G Simons and I J Russell Muscle PainUnderstanding Its Nature Diagnosis and Treatment LippincottWilliams ampWilkins 2001
[28] R Rolke ldquoPseudoradicular and radicular low-back painmdashadisease continuum Rather than different entities Reply to theletters by Leffler and Hansson and by Van Boxem et alrdquo Painvol 135 pp 311ndash316 2008
[29] J M Bland and D G Altman ldquoStatistical methods for assessingagreement between two methods of clinical measurementrdquoTheLancet vol 1 no 8476 pp 307ndash310 1986
[30] D G Altman ldquoSome common problems in medical researchrdquoin Practical Statistics for Medical Research Chapman amp HallCRC Press London UK 1997
BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
Table 3 Validity elements [24 25]
Test performed
Results detected by the test True picture TotalPatient has the condition Patient is clear
Positive test A (true positive) B (false positive) A + B (total positive tests)Negative test C (false negative) D (true negative) C + D (total negative tests)Total Total subjects diagnosed with the condition Total subjects without the condition 119873 (total number tested)
Table 4 Landis and Koch guidelines for 120581 interpretation [29]
120581 value Strength of agreementlt000 Poor agreement000ndash020 Slight agreement021ndash040 Fair agreement041ndash060 Moderate agreement061ndash080 Substantial agreement081ndash100 Almost perfect agreement100 Perfect agreement
patients and heathy volunteers (all 119901 lt 005) (Tables 5and 6) The sciatic group presented contrary 119879sk changesdependent on TrPs and DN related referred pain presenceFor TrPs-negative 119879sk decrease contrary to 119879sk increase ofTrPs-positive was observed
Isothermal-Area Changes Related to TTDN None of TrPs-positive subjects presented vasoconstriction or any signifi-cant changes of the low 119879sk isothermal-area and 119879sk decreaseSignificant 119879sk and isothermal-area changes for every TrPs-positive sciatica subject were confirmed
The exact two-way Mann-Whitney 119880 tests confirmed asignificant increase of the observed isothermal-area (calcu-lated together AURP and high119879sk isothermal-area) for TrPs-positive sciatica subjects compared to TrPs-negative sciaticapatients and healthy volunteers (all 119901 lt 005) for both post-DN and postobservation phases (every 119901 lt 005) Afterdividing the isothermal-area into high 119879sk isothermal-areaand AURP (shown in Figure 1) the results were as follows
The exact two-way Mann-Whitney 119880 tests confirmed asignificant increase of the high 119879sk isothermal-area (thighand calf) for TrPs-positive compared toTrPs-negative sciaticasubjects (119901 lt 005) but not to healthy volunteers (Table 7)The significant increase of AURP (vasodilatation) for TrPs-positive compared to TrPs-negative and healthy volunteerswas confirmed (The exact two-way Mann-Whitney 119880 testsevery 119901 lt 005) The average value of the percentage increaseof AURP was shown in Table 8
32 Validity and Reliability of TTDN There were consid-erable differences detected in the results of TTDN when itwas performed on the non-TrPs sciatic group TrP-positivesciatic group and non-TrPs healthy volunteers The agree-ment between TTDN and TrPs diagnosis was almost perfect(according to 120581) for changes of119879avr and isothermal-area above119879max at rest of the thigh and calf (Tables 9 and 10) In terms
of validity components TTDN was useful for identifyingthe positive values of 119879max changes and isothermal-area(below 119879max at rest) or full AURP (namely below and above119879max at rest calculated together) changes but was not useful foridentifying the negative values (specificity) Although 119879maxand isothermal-area below 119879max at rest or full AURP have highsensitivity the low specificity does not allow recommendingtheir diagnostic value
4 Discussion
The results of skin temperature (both 119879avr and 119879max) andisothermal-area significantly differ for TrPs-positive sciaticasubjects compared to non-TrPs sciatica subjects and healthyvolunteers (119901 lt 005 Tables 5ndash8) which is consistent withthe previous study involving sciatica subjects only [10 11]However the main purpose of the present study was tocheck the validity and reliability of TTDN This new IRTmethod was assumed to allow observing vasomotor andtemperature reactions related to TrPs andwas validated for itsability to distinguish active TrPs from non-TrPs of the gluteusminimus muscle and non-TrPs of healthy volunteers It wasfound that TTDN identifies active gluteus minimus TrPs forevery positive subjectThemost discriminatory indicators forTrPs presence were 119879avr increase and the presence of high119879sk increase above 119879max (isothermal-area defined as AURPTables 9 and 10) in the area where dry needling intensifiedpain The results showed that TTDN validly measured 119879avrchanges and the presence of AURP (grey picture in Figure 1)for active TrPs of the gluteus minimus muscle The ICCresults confirmedmoderate reliability forAURPpresence andpoor to moderate for 119879avr increase However these two typesof thermogram analysis showed almost prefect agreementaccording to 120581 (Tables 9 and 10) which is recommended as amore suitablemeasure of agreement amongnonexchangeableobservers in comparison with ICC It seems that AURP andsignificant 119879avr increase can objectively support Travell andSimonsrsquo clinical criteria for active TrPs within the gluteusminimus muscle when referred pain is evoked by snappingpalpation [5 6] However similar tendency for AURP and119879avr for some of the healthy volunteers was observed (AURPnot exceeding 25 with insignificant 119879avr of +014
∘C) (Tables6 and 8) and small changes can be explained by 119879sk differ-ences in time due to the physiological variability of blood flow[34]
IRT reliability was checked for the muscle examinationand was found more reliable compared to the present studybut they examined the thermograms of the subjects at rest [1718] The quantitative measurement of the percentage value of
6 BioMed Research International
Table 5 Mean value of maximum temperature changes
119879max Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus012 plusmn 016 121 plusmn 018 lowastlowastlowast 09 plusmn 014
Calf minus047 plusmn 015 066 plusmn 019 lowastlowastlowast minus005 plusmn 013
Foot minus024 plusmn 014 01 plusmn 011 mdash minus005 plusmn 015
After observThigh 012 plusmn 018 129 plusmn 018 lowastlowastlowast 025 plusmn 013
Calf minus047 plusmn 015 065 plusmn 017 lowastlowastlowast minus018 plusmn 013
Foot minus029 plusmn 016 minus02 plusmn 008 mdash minus023 plusmn 014
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 6 Mean value of average temperature changes
119879avr Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus051 plusmn 011 099 plusmn 012 lowastlowastlowast 007 plusmn 012
Calf minus07 plusmn 011 045 plusmn 011 lowastlowastlowast minus025 plusmn 010
Foot minus056 plusmn 010 minus03 plusmn 07 lowastlowastlowast minus045 plusmn 011
After observThigh minus038 plusmn 014 113 plusmn 013 lowastlowastlowast 015 plusmn 012
Calf minus066 plusmn 012 044 plusmn 014 lowastlowastlowast minus025 plusmn 011
Foot minus053 plusmn 014 minus007 plusmn 008 lowastlowastlowast minus045 plusmn 010
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
isothermal-area changes is presented for the first time andallowed observing the changes of a specific subarea of definedtemperature very precisely However it should be underlinedthat it was possible because dry needling provoked intensive119879sk changes (Figure 1) which again is unusual compared toacupuncture studieswhere postneedling stimulationwas lim-ited to the site of needling [35 36] TTDN allowed observingdynamic thermogram changes due to the stimulation by dryneedling and the fact that DN is a treatment technique forTrPs release [37]The difference between the first and the lastsession could have resulted from the therapeutic DN effectapart from the skin blood flow variability
Moreover it should be underlined that the strong inclu-sion and exclusion criteria for TrPs confirmation did notallow claiming that TTDN is a new objective method forevery gluteus minimus TrP confirmation It has been claimedthat digitally evoked referred pain pattern from the gluteusminimus muscle is rare and for the diagnostic purposes thepresence of a tender point and needle encouraged referredpain were postulated as diagnostic criteria for that muscle
The diagnostic criteria established for the gluteus min-imus muscle in the present study were as severe as possiblebecause it has been lastly postulated that the methodologicalquality of the majority of studies conducted for the purposeof establishing trigger point reproducibility is generally poor[38] Tough et al [39] indicated that only 15 of authorsused the combination of a tender spot in a taut band ofa skeletal muscle patientsrsquo pain recognition predicted painreferral pattern and local twitch response Thanks to TrPsdiagnostic criteria used in the present study the diagnosisof TrPs presence cannot be questioned and additionally the
consistency condition regarding the referred pain presenceminimum to the calf ensures the group homogeneity Ofcourse the choice of the gluteus minimus muscle for the firstuse of TTDN can be questioned However an advantage ofthis choice is the size of the referred pain pattern which isone of the most extensive froms all of the TrPs referred painpatterns Thus it was predicted that the observed vasomotorreactions if present should be probably the widest and easilydetectable by IRT
TTDN Results in the Light of the Previous Studies The use ofthermography is not a new way for TrPs evaluation Most ofthe authors tried to correlate the localization of TrPs with hotspots on the thermogram [16] Brioschi et al [40] analyzedmost of the available studies on the subject and concludedthat IRT findings represent an objective means of document-ing TrPs if the thermogram is analyzed by an experiencedphysician skilled in clinical thermology together with clinicalevaluation of the patient However in one of the oldeststudies Swerdlow andDieter [41] evaluated the sensitivity andspecificity of medical thermography for the documentationof TrPs and they concluded that the localizations of TrPsand hot spots were not associated Moreover some otherauthors stated that skin temperature measurement in TrPsarea cannot be used to detect myofascial tender spots [42]Additionally in the latest review regarding IRT application toTrPs it has been stated that there are few studies evaluatingthe accuracy and reliability of infrared thermography for thediagnosis and assessment of TrPs In the few studies presentthere is no agreement on skin temperature patterns in thepresence of TrPs [43]
BioMed Research International 7
448
419
390
362
333
304
275
246
217451
423
394
365
336
307
279
250
221
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
446
412
378
344
310
276
242
208
175446
412
378
344
310
276
242
208
175
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
450
418
387
355
324
293
261
230
199
450
418
387
355
324
293
261
230
199
450
416
382
349
315
282
248
214
181450
416
382
349
315
282
248
214
181
Case 1 Case 2a b c a b c
Ia
Ib
IIa
IIb
IIIa
IIIb
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
Figure 1 TTDN related thermograms presenting temperature reaction measured on skin surface of TrPs and non-TrPs sciatica patients andhealthy volunteers In rows I two cases of TrPs-negative sciatica II two cases of TrPs-positive sciatica and III two cases of healthy volunteerswere shown In rows Ia IIa and IIIa full thermogramwas presented In rows Ib IIb and IIIb the picture of the isothermal-area above119879max at restcalled AURP was shown (visualization of the vasodilation) In columns (a) Before TTDN (initial state) (b) state immediately after DN and(c) state immediately after observation were presented
IRT was also used for TrPs related referred pain areaexamination Although Brioschi et al [44] evaluated 304chronic myofascial pain patients using IRT before and afterDN or anesthetic infiltration they found that referred areaswere thermally asymmetric andKimura et al [8] confirmed asignificant decrease in 119879sk over time after glutamate injection(nociceptive stimulation) in latent TrPs (119901 lt 005) theusefulness of IRT for postnoxious stimulation of latent TrPsreferred pain observation was contradicted by Zhang et al[9] On the other hand one of the oldest studies on thesubject presents results similar to the present study Kruse Jrand Christiansen [45] observed referred pain pattern by IRTwhen palpation pressure over TrPs lasted around 1 minuteInitially they observed a small 119879sk increase followed by asignificant decrease in the area of the observed referredpain The DN stimulation is a much more severe type ofTrPs stimulation compared to pressure and the time ofstimulation in the present study was ten times longer Itcan be hypothesized that a stronger noxious stimulationcould provoke much more intensive 119879sk increase and maybeKruse Jr and Christiansen [45] observed the same vasomotorreactions but of a weak and short form Additionally another
difference between the studies is the localization of visiblethermal response They reported visible 119879sk changes onthe thermogram more extensive than that of the reportedreferred pain during TrPs compression contrary to thepresent study where AURP localization is limited precisely tothe area where DN provoked pain during TTDN (Figure 1)The thermogram analysis before isothermal-area calculationwas based on the indirect thermogram analysis where theexaminer had to distinguish subtle color differences Theisothermal-area calculation together with the thermogram ofAURP (gray picture Figure 1) is a nonquestionable proof ofsignificant vasomotor changes and can be easily interpretedby everyone
Interestingly the analysis of 119879avr changes in the wholegroup of subjects in the present study (Table 6) clearlyindicated 119879avr decrease for non-TrPs healthy volunteersand needle insensitive foot of TrPs-positive sciatica subjectscontrary to 119879avr increase of DN reactive subarea of TrPs-positive subjects Moreover when the thermograms of non-TrPs sciatica subjects were observed some of them presenteddiscreet vasoconstriction feature (Figure 1) and 119879sk decrease(Tables 5 and 6) These results allow putting the question of
8 BioMed Research International
Table 7 Mean value of isothermal-area below 119879max at rest changes
Isothermal-area below 119879max at rest [] Sciatica patients Healthy volunteersTTDN Phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus276 plusmn 46 76 plusmn 78 lowast minus28 plusmn 52
Calf minus265 plusmn 52 34 plusmn 57 lowast minus85 plusmn 45
Foot minus139 plusmn 513 minus39 plusmn 29 mdash minus97 plusmn 45
After observThigh minus2507 plusmn 45 102 plusmn 784 lowast minus142 plusmn 56
Calf minus248 plusmn 57 minus06 plusmn 53 lowast minus1042 plusmn 55
Foot minus152 plusmn 52 minus42 plusmn 27 mdash minus1015 plusmn 42
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 8 Mean value of isothermal-area above 119879max at rest (AURP) changes
Isothermal-area above 119879max at rest [] Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampnon-DN
After DN Thigh 0 plusmn 00 212 plusmn 265 lowastlowastlowast 114 plusmn 08
Calf 0 plusmn 00 482 plusmn 107 lowastlowastlowast 003 plusmn 002
After observ Thigh 0 plusmn 00 264 plusmn 333 lowastlowastlowast 125 plusmn 08
Calf 0 plusmn 00 663 plusmn 14 lowastlowastlowast 004 plusmn 003
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 9 Validity and reliability of TTDN components for 119879sk changes
119879sk [∘C] TTDN phases Area Sensitivity [] Specificity [] Average [∘C] Min [∘C] Max [∘C] PPV [] ICC 120581
MaximumAfter DN Thigh 100 313 119 minus02 26 577 0622 0702
Calf 100 842 066 minus08 21 667 0422 0786
After observ Thigh 100 167 129 minus01 27 545 0670 0556Calf 100 500 065 minus07 195 857 0440 0680
AverageAfter DN Thigh 100 100 099 004 195 100 0400 0880
Calf 100 100 045 minus04 13 100 0511 0902
After observ Thigh 100 846 111 009 22 750 0333 0786Calf 100 944 044 minus06 15 857 0422 0845
Table 10 Validity and reliability of TTDN components for isothermal-area changes
Isothermal-area TTDN phases Area Sensitivity [] Specificity [] Mean [] Min [] Max [] PPV [] ICC 120581
AURP (above 119879max at rest)After DN Thigh 100 100 212 06 418 100 0689 0938
Calf 100 100 48 minus35 131 100 0778 0956
After observ Thigh 100 100 264 06 522 100 0644 0929Calf 100 100 66 minus44 177 100 0778 0956
Below 119879max at rest
After DN Thigh 100 00 758 minus527 678 500 0778 0656Calf 100 200 337 minus407 474 778 0556 0707
After observ Thigh 100 00 102 minus597 618 500 0778 0656Calf 100 750 minus059 minus419 407 875 0511 0827
Below + above 119879max at rest
After DN Thigh 100 222 288 minus293 869 682 0578 0696Calf 100 370 819 minus136 628 778 0578 0782
After observ Thigh 100 00 1987 minus55 453 483 0733 0643Calf 100 782 605 minus127 576 794 0644 0847
BioMed Research International 9
whether the authors of the previous study who confirmedTrPs-related vasoconstriction really stimulated TrPs On theother hand maybe the type of TrPs (latent TrPs) or regionof IRT observation (upper extremity) or type of noxiousstimulation (glutamate injection) can explain contrary results[8 9] Further studies considering both active and latent TrPsdifferent regions of the body and so forth are required
The New IdeamdashIsothermal-Area Calculation The standardusage of IRT in medicine is based on mean temperature andstandard deviation within the fixed region of interest (ROi)as well as the visualized interpretation of the thermogramwhere each temperature value (or a group of similar values)is attributed to a specified color The color variation is theonly indirect analysis and this type of interpretation is limitedto the physician trained in thermology Additionally theuse of spot temperature measurements or observation ofselected values of 119879max or 119879avr may not produce the expectedoutcomes and the results obtained this way may differ a lotfrom the real situation In summary the comparison of 119879avrof ROi is performed without considering the size of ROiThus an error resulting from the statistical interpretation ispossible These facts can explain the controversies aroundthe merit of IRT measurement in medicine However it hasbeen postulated that considering the number of pixels inthe observed ROi that is the qualitative evaluation of forexample its size and shape together with 119879avr can lead to anobjective interpretation of the results [16]
TTDN is the method which allows assessing the thermo-gram in this recommended wayThemeasurement of the sizeof isothermal-areas in the present study guarantees the pre-cise results of the occurring process of thermal phenomenaappearing on the human skin In addition TTDN analysisaccounts for 100 of the information recorded on a singlethermogram
The next innovativeness of TTDN apart from calculatingthe size of ROi is the possibility of showing vasomotorreactions in TrPs referred pain area The results are easyto interpret and not limited by a physician experience Themeasurement of the size of isothermal-areas in the presentstudy guarantees the precise results of the occurring processof thermal phenomena appearing on the human skin Inaddition the validity of TTDN confirmed the most discrimi-natory indicators for TrPs presence119879avr and isothermal-areacalculation
5 Summary and Limitations of the Study
We are unaware of any other published studies regardingthe validity and reliability of TrPs noxious stimulation byDN under IRT control to support the diagnosis of TrPsThe results of the present study were subject to the rigorand diagnostic protocol of the standards thermographicprocedure Moreover side-to-side 119879sk comparison of thepatient at rest performed before the main procedure allowedexcluding pain states related to sympathetic nervous systemactivity
TTDN seems to be a promising tool for objective TrPsconfirmation However this is the first study of this type
and the validation of TTDN on other muscles with TrPs andsome studies presenting a group with active and latent TrPsof the same muscle are required After a series of studies thatwould give the same results TTDN could be claimed as a newobjectivemethod for TrPs confirmation where DN is possibleto perform
The limitations of this study are the strong inclusion andexclusion criteria for the confirmation of gluteus minimusmuscle TrPs This muscle should be checked by TTDN whenTrPs confirmation is based on tender point presence whichprovoked typical referred pain when needle encounteredTrPs
Moreover Travell and Simons claimed that autonomicphenomena (including vasomotor reaction) within TrPsreferred pain area are limited to severe active TrPs onlyIn the present study TrPs-positive sciatic patients can beassumed to probably have severe active TrPs due to thechronicity and length of the referred pain pattern evokedby snapping palpation However the severity of active TrPsstill remains only a theoretical consideration because thereare no criteria for distinguishing the severity of active TrPs[26] Additionally other TrPs for example within the uppertrapezius muscle should be examined by TTDN to answerthe question if every TrPs present AURP is accompanied by119879avr increase
Finally the present study is limited by the lack of inter-rater reliability of TTDN
6 Conclusion
TTDN is valid and reliable for 119879avr and AURP measurementto support TrPs diagnostic criteria for the gluteus minimusmuscle when a digitally evoked referred pain pattern ispresented In the light of clinical division TTDN results indi-cate skin temperature increase for TrPs-positive contrary todecrease for TrPs-negative chronic sciatica patients and smallchanges (both increasedecrease) for healthy volunteers
Conflict of Interests
The authors declare no conflict of interests especially regard-ing patent application
Authorsrsquo Contribution
All authors listed have contributed substantially to the paperElzbieta Skorupska contributed conception and design ofthe work acquisition of data interpretation of data anddrafting the paper Michał Rychlik contributed Conceptionand design of the work acquisition of data analysis of dataand drafting the paper Włodzimierz Samborski contributedcorrection and final approval of the resubmitted version
Acknowledgments
The authors gratefully acknowledge the critical reading andcorrection of this paper by Malgorzata Mankowska Thiswork was partially supported by the Polish National ScienceCentre Grant no N N404 268339 and Poznan University ofMedical Sciences
10 BioMed Research International
References
[1] R SWeiner PainManagement A Practical Guide for CliniciansCRC Press LLC 6th edition 2002
[2] S A Skootsky B Jaeger and R K Oye ldquoPrevalence ofmyofascial pain in general internal medicine practicerdquoWesternJournal of Medicine vol 151 no 2 pp 157ndash160 1989
[3] Q Chen S Bensamoun J R Basford J M Thompsonand K-N An ldquoIdentification and quantification of myofascialtaut bands with magnetic resonance elastographyrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1658ndash1661 2007
[4] S Sikdar J P Shah T Gebreab et al ldquoNovel applications ofultrasound technology to visualize and characterize myofascialtrigger points and surrounding soft tissuerdquo Archives of PhysicalMedicine and Rehabilitation vol 90 no 11 pp 1829ndash1838 2009
[5] J G Travell andD G SimonsMyofascial Pain andDysfunctionThe Trigger PointManual vol 1WilliamsampWilkins BaltimoreMd USA 2nd edition 1999
[6] J G Travell andD G SimonsMyofascial Pain andDysfunctionTheTrigger PointManual vol 2 LippincottWilliamsampWilkinsBaltimore Md USA 1993
[7] H-Y Ge C Fernandez-de-las-Penas and L Arendt-NielsenldquoSympathetic facilitation of hyperalgesia evoked from myofas-cial tender and trigger points in patients with unilateral shoul-der painrdquoClinical Neurophysiology vol 117 no 7 pp 1545ndash15502006
[8] Y Kimura H-Y Ge Y Zhang M Kimura H Sumikura andL Arendt-Nielsen ldquoEvaluation of sympathetic vasoconstrictorresponse following nociceptive stimulation of latent myofascialtrigger points in humansrdquo Acta Physiologica vol 196 no 4 pp411ndash417 2009
[9] Y Zhang H-Y Ge S-W Yue Y Kimura and L Arendt-Nielsen ldquoAttenuated Skin blood flow response to nociceptivestimulation of latent myofascial trigger pointrdquo Archives ofPhysical Medicine and Rehabilitation vol 90 no 2 pp 325ndash3322009
[10] E Skorupska M Rychlik W Pawelec and W Samborski ldquoDryneedling related short-term vasodilation in chronic sciaticaunder infrared thermovisionrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 214374 10 pages2015
[11] E SkorupskaM Rychlik andW Samborski ldquoIntensive vasodi-latation in the sciatic pain area after dry needlingrdquo BMCComplementary and Alternative Medicine vol 15 article 722015
[12] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoTrigger point-related sympathetic nerve activity inchronic sciatic leg pain a case studyrdquo Acupuncture in Medicinevol 32 no 5 pp 418ndash422 2014
[13] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoIntensive short-term vasodilation effect in the painarea of sciatica patientsmdashcase studyrdquo BMC Research Notes vol7 no 1 article 620 2014
[14] G Affaitati A Fabrizio A Savini et al ldquoA randomizedcontrolled study comparing a lidocaine patch a placebo patchand anesthetic injection for treatment of trigger points inpatients with myofascial pain syndrome evaluation of pain andsomatic pain thresholdsrdquoClinicalTherapeutics vol 31 no 4 pp705ndash720 2009
[15] D G Simons ldquoReview of enigmatic MTrPs as a common causeof enigmatic musculoskeletal pain and dysfunctionrdquo Journal
of Electromyography and Kinesiology vol 14 no 1 pp 95ndash1072004
[16] F S Nahm ldquoInfrared thermography in pain medicinerdquo KoreanJournal of Pain vol 26 no 3 pp 219ndash222 2013
[17] A C S Costa A V D Filho A C Packer and D Rodrigues-Bigaton ldquoIntra and inter-rater reliability of infrared image anal-ysis of masticatory and upper trapezius muscles in women withand without temporomandibular disorderrdquo Brazilian Journal ofPhysical Therapy vol 17 no 1 pp 24ndash31 2013
[18] M McCoy I Campbell P Stone C Fedorchuk S Wijayawar-dana and K Easley ldquoIntra-examiner and inter-examiner repro-ducibility of paraspinal thermographyrdquo PLoS ONE vol 6 no 2Article ID e16535 2011
[19] D S Haddad M L Brioschi and E S Arita ldquoThermographicand clinical correlation of myofascial trigger points in themasticatory musclesrdquo Dentomaxillofacial Radiology vol 41 no8 pp 621ndash629 2012
[20] S J Gulevich T D Conwell J Lane et al ldquoStress infraredtelethermography is useful in the diagnosis of complex regionalpain syndrome type I (formerly reflex sympathetic dystrophy)rdquoClinical Journal of Pain vol 13 no 1 pp 50ndash59 1997
[21] G Wasner J Schattschneider and R Baron ldquoSkin temperatureside differencesmdasha diagnostic tool for CRPSrdquo Pain vol 98 no1-2 pp 19ndash26 2002
[22] E J Park K R Han Y J Chae W H Jeong and C KimldquoEffectiveness of cold stress thermography in the diagnosis ofcomplex of regional pain syndrome type 1rdquoThe Korean Journalof Pain vol 19 pp 159ndash163 2006
[23] E Skorupska M Rychlik and W Pawelec ldquoSkeletal striatedmuscle examination instrument amp new method of myofascialpain diagnosis based on the use of the instrumentrdquo Patentapplication No P-403467 Silver Medal 14ndash16 November 2013Brussels Innova the International Exhibition of InnovationEntrepreneurship and New Technologies Bronze Medal at theConcours Lepine International Paris 3004-11052014 FranceGoldMedal at the Euroinvent EuropeanExhibition ofCreativityand Innovation 22-24052014 Iasi Romania Gold Medal withDistinction at the 29th Invention and New Product ExpositionINPEX 18ndash20062014 Pittsburgh Pa USA
[24] R G Schwartz R Elliott G S Goldberg et al ldquoThe AmericanAcademy of Thermology Guidelines for neuromusculoskeletalthermographyrdquoThermology International vol 16 pp 5ndash9 2006
[25] J Dommerholt and C Fernandez-de-las-Penas Trigger PointDry Needling An Evidence and Clinical-Based ApproachChurchill Livingstone Elsevier 2013
[26] C Z Hong Braddom Physical Medicine and Rehabilitationin Muscle Pain Syndrome Elsevier New York NY USA 4thedition 2011
[27] S Mense D G Simons and I J Russell Muscle PainUnderstanding Its Nature Diagnosis and Treatment LippincottWilliams ampWilkins 2001
[28] R Rolke ldquoPseudoradicular and radicular low-back painmdashadisease continuum Rather than different entities Reply to theletters by Leffler and Hansson and by Van Boxem et alrdquo Painvol 135 pp 311ndash316 2008
[29] J M Bland and D G Altman ldquoStatistical methods for assessingagreement between two methods of clinical measurementrdquoTheLancet vol 1 no 8476 pp 307ndash310 1986
[30] D G Altman ldquoSome common problems in medical researchrdquoin Practical Statistics for Medical Research Chapman amp HallCRC Press London UK 1997
BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
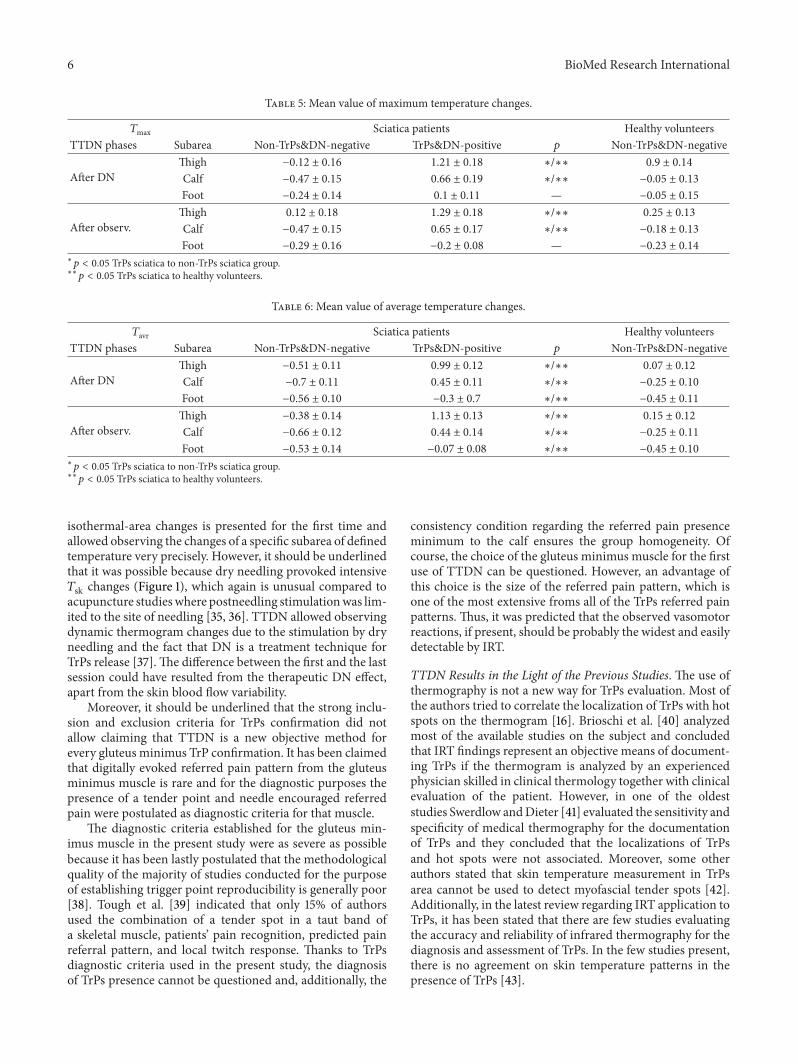
6 BioMed Research International
Table 5 Mean value of maximum temperature changes
119879max Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus012 plusmn 016 121 plusmn 018 lowastlowastlowast 09 plusmn 014
Calf minus047 plusmn 015 066 plusmn 019 lowastlowastlowast minus005 plusmn 013
Foot minus024 plusmn 014 01 plusmn 011 mdash minus005 plusmn 015
After observThigh 012 plusmn 018 129 plusmn 018 lowastlowastlowast 025 plusmn 013
Calf minus047 plusmn 015 065 plusmn 017 lowastlowastlowast minus018 plusmn 013
Foot minus029 plusmn 016 minus02 plusmn 008 mdash minus023 plusmn 014
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 6 Mean value of average temperature changes
119879avr Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus051 plusmn 011 099 plusmn 012 lowastlowastlowast 007 plusmn 012
Calf minus07 plusmn 011 045 plusmn 011 lowastlowastlowast minus025 plusmn 010
Foot minus056 plusmn 010 minus03 plusmn 07 lowastlowastlowast minus045 plusmn 011
After observThigh minus038 plusmn 014 113 plusmn 013 lowastlowastlowast 015 plusmn 012
Calf minus066 plusmn 012 044 plusmn 014 lowastlowastlowast minus025 plusmn 011
Foot minus053 plusmn 014 minus007 plusmn 008 lowastlowastlowast minus045 plusmn 010
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
isothermal-area changes is presented for the first time andallowed observing the changes of a specific subarea of definedtemperature very precisely However it should be underlinedthat it was possible because dry needling provoked intensive119879sk changes (Figure 1) which again is unusual compared toacupuncture studieswhere postneedling stimulationwas lim-ited to the site of needling [35 36] TTDN allowed observingdynamic thermogram changes due to the stimulation by dryneedling and the fact that DN is a treatment technique forTrPs release [37]The difference between the first and the lastsession could have resulted from the therapeutic DN effectapart from the skin blood flow variability
Moreover it should be underlined that the strong inclu-sion and exclusion criteria for TrPs confirmation did notallow claiming that TTDN is a new objective method forevery gluteus minimus TrP confirmation It has been claimedthat digitally evoked referred pain pattern from the gluteusminimus muscle is rare and for the diagnostic purposes thepresence of a tender point and needle encouraged referredpain were postulated as diagnostic criteria for that muscle
The diagnostic criteria established for the gluteus min-imus muscle in the present study were as severe as possiblebecause it has been lastly postulated that the methodologicalquality of the majority of studies conducted for the purposeof establishing trigger point reproducibility is generally poor[38] Tough et al [39] indicated that only 15 of authorsused the combination of a tender spot in a taut band ofa skeletal muscle patientsrsquo pain recognition predicted painreferral pattern and local twitch response Thanks to TrPsdiagnostic criteria used in the present study the diagnosisof TrPs presence cannot be questioned and additionally the
consistency condition regarding the referred pain presenceminimum to the calf ensures the group homogeneity Ofcourse the choice of the gluteus minimus muscle for the firstuse of TTDN can be questioned However an advantage ofthis choice is the size of the referred pain pattern which isone of the most extensive froms all of the TrPs referred painpatterns Thus it was predicted that the observed vasomotorreactions if present should be probably the widest and easilydetectable by IRT
TTDN Results in the Light of the Previous Studies The use ofthermography is not a new way for TrPs evaluation Most ofthe authors tried to correlate the localization of TrPs with hotspots on the thermogram [16] Brioschi et al [40] analyzedmost of the available studies on the subject and concludedthat IRT findings represent an objective means of document-ing TrPs if the thermogram is analyzed by an experiencedphysician skilled in clinical thermology together with clinicalevaluation of the patient However in one of the oldeststudies Swerdlow andDieter [41] evaluated the sensitivity andspecificity of medical thermography for the documentationof TrPs and they concluded that the localizations of TrPsand hot spots were not associated Moreover some otherauthors stated that skin temperature measurement in TrPsarea cannot be used to detect myofascial tender spots [42]Additionally in the latest review regarding IRT application toTrPs it has been stated that there are few studies evaluatingthe accuracy and reliability of infrared thermography for thediagnosis and assessment of TrPs In the few studies presentthere is no agreement on skin temperature patterns in thepresence of TrPs [43]
BioMed Research International 7
448
419
390
362
333
304
275
246
217451
423
394
365
336
307
279
250
221
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
446
412
378
344
310
276
242
208
175446
412
378
344
310
276
242
208
175
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
450
418
387
355
324
293
261
230
199
450
418
387
355
324
293
261
230
199
450
416
382
349
315
282
248
214
181450
416
382
349
315
282
248
214
181
Case 1 Case 2a b c a b c
Ia
Ib
IIa
IIb
IIIa
IIIb
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
Figure 1 TTDN related thermograms presenting temperature reaction measured on skin surface of TrPs and non-TrPs sciatica patients andhealthy volunteers In rows I two cases of TrPs-negative sciatica II two cases of TrPs-positive sciatica and III two cases of healthy volunteerswere shown In rows Ia IIa and IIIa full thermogramwas presented In rows Ib IIb and IIIb the picture of the isothermal-area above119879max at restcalled AURP was shown (visualization of the vasodilation) In columns (a) Before TTDN (initial state) (b) state immediately after DN and(c) state immediately after observation were presented
IRT was also used for TrPs related referred pain areaexamination Although Brioschi et al [44] evaluated 304chronic myofascial pain patients using IRT before and afterDN or anesthetic infiltration they found that referred areaswere thermally asymmetric andKimura et al [8] confirmed asignificant decrease in 119879sk over time after glutamate injection(nociceptive stimulation) in latent TrPs (119901 lt 005) theusefulness of IRT for postnoxious stimulation of latent TrPsreferred pain observation was contradicted by Zhang et al[9] On the other hand one of the oldest studies on thesubject presents results similar to the present study Kruse Jrand Christiansen [45] observed referred pain pattern by IRTwhen palpation pressure over TrPs lasted around 1 minuteInitially they observed a small 119879sk increase followed by asignificant decrease in the area of the observed referredpain The DN stimulation is a much more severe type ofTrPs stimulation compared to pressure and the time ofstimulation in the present study was ten times longer Itcan be hypothesized that a stronger noxious stimulationcould provoke much more intensive 119879sk increase and maybeKruse Jr and Christiansen [45] observed the same vasomotorreactions but of a weak and short form Additionally another
difference between the studies is the localization of visiblethermal response They reported visible 119879sk changes onthe thermogram more extensive than that of the reportedreferred pain during TrPs compression contrary to thepresent study where AURP localization is limited precisely tothe area where DN provoked pain during TTDN (Figure 1)The thermogram analysis before isothermal-area calculationwas based on the indirect thermogram analysis where theexaminer had to distinguish subtle color differences Theisothermal-area calculation together with the thermogram ofAURP (gray picture Figure 1) is a nonquestionable proof ofsignificant vasomotor changes and can be easily interpretedby everyone
Interestingly the analysis of 119879avr changes in the wholegroup of subjects in the present study (Table 6) clearlyindicated 119879avr decrease for non-TrPs healthy volunteersand needle insensitive foot of TrPs-positive sciatica subjectscontrary to 119879avr increase of DN reactive subarea of TrPs-positive subjects Moreover when the thermograms of non-TrPs sciatica subjects were observed some of them presenteddiscreet vasoconstriction feature (Figure 1) and 119879sk decrease(Tables 5 and 6) These results allow putting the question of
8 BioMed Research International
Table 7 Mean value of isothermal-area below 119879max at rest changes
Isothermal-area below 119879max at rest [] Sciatica patients Healthy volunteersTTDN Phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus276 plusmn 46 76 plusmn 78 lowast minus28 plusmn 52
Calf minus265 plusmn 52 34 plusmn 57 lowast minus85 plusmn 45
Foot minus139 plusmn 513 minus39 plusmn 29 mdash minus97 plusmn 45
After observThigh minus2507 plusmn 45 102 plusmn 784 lowast minus142 plusmn 56
Calf minus248 plusmn 57 minus06 plusmn 53 lowast minus1042 plusmn 55
Foot minus152 plusmn 52 minus42 plusmn 27 mdash minus1015 plusmn 42
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 8 Mean value of isothermal-area above 119879max at rest (AURP) changes
Isothermal-area above 119879max at rest [] Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampnon-DN
After DN Thigh 0 plusmn 00 212 plusmn 265 lowastlowastlowast 114 plusmn 08
Calf 0 plusmn 00 482 plusmn 107 lowastlowastlowast 003 plusmn 002
After observ Thigh 0 plusmn 00 264 plusmn 333 lowastlowastlowast 125 plusmn 08
Calf 0 plusmn 00 663 plusmn 14 lowastlowastlowast 004 plusmn 003
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 9 Validity and reliability of TTDN components for 119879sk changes
119879sk [∘C] TTDN phases Area Sensitivity [] Specificity [] Average [∘C] Min [∘C] Max [∘C] PPV [] ICC 120581
MaximumAfter DN Thigh 100 313 119 minus02 26 577 0622 0702
Calf 100 842 066 minus08 21 667 0422 0786
After observ Thigh 100 167 129 minus01 27 545 0670 0556Calf 100 500 065 minus07 195 857 0440 0680
AverageAfter DN Thigh 100 100 099 004 195 100 0400 0880
Calf 100 100 045 minus04 13 100 0511 0902
After observ Thigh 100 846 111 009 22 750 0333 0786Calf 100 944 044 minus06 15 857 0422 0845
Table 10 Validity and reliability of TTDN components for isothermal-area changes
Isothermal-area TTDN phases Area Sensitivity [] Specificity [] Mean [] Min [] Max [] PPV [] ICC 120581
AURP (above 119879max at rest)After DN Thigh 100 100 212 06 418 100 0689 0938
Calf 100 100 48 minus35 131 100 0778 0956
After observ Thigh 100 100 264 06 522 100 0644 0929Calf 100 100 66 minus44 177 100 0778 0956
Below 119879max at rest
After DN Thigh 100 00 758 minus527 678 500 0778 0656Calf 100 200 337 minus407 474 778 0556 0707
After observ Thigh 100 00 102 minus597 618 500 0778 0656Calf 100 750 minus059 minus419 407 875 0511 0827
Below + above 119879max at rest
After DN Thigh 100 222 288 minus293 869 682 0578 0696Calf 100 370 819 minus136 628 778 0578 0782
After observ Thigh 100 00 1987 minus55 453 483 0733 0643Calf 100 782 605 minus127 576 794 0644 0847
BioMed Research International 9
whether the authors of the previous study who confirmedTrPs-related vasoconstriction really stimulated TrPs On theother hand maybe the type of TrPs (latent TrPs) or regionof IRT observation (upper extremity) or type of noxiousstimulation (glutamate injection) can explain contrary results[8 9] Further studies considering both active and latent TrPsdifferent regions of the body and so forth are required
The New IdeamdashIsothermal-Area Calculation The standardusage of IRT in medicine is based on mean temperature andstandard deviation within the fixed region of interest (ROi)as well as the visualized interpretation of the thermogramwhere each temperature value (or a group of similar values)is attributed to a specified color The color variation is theonly indirect analysis and this type of interpretation is limitedto the physician trained in thermology Additionally theuse of spot temperature measurements or observation ofselected values of 119879max or 119879avr may not produce the expectedoutcomes and the results obtained this way may differ a lotfrom the real situation In summary the comparison of 119879avrof ROi is performed without considering the size of ROiThus an error resulting from the statistical interpretation ispossible These facts can explain the controversies aroundthe merit of IRT measurement in medicine However it hasbeen postulated that considering the number of pixels inthe observed ROi that is the qualitative evaluation of forexample its size and shape together with 119879avr can lead to anobjective interpretation of the results [16]
TTDN is the method which allows assessing the thermo-gram in this recommended wayThemeasurement of the sizeof isothermal-areas in the present study guarantees the pre-cise results of the occurring process of thermal phenomenaappearing on the human skin In addition TTDN analysisaccounts for 100 of the information recorded on a singlethermogram
The next innovativeness of TTDN apart from calculatingthe size of ROi is the possibility of showing vasomotorreactions in TrPs referred pain area The results are easyto interpret and not limited by a physician experience Themeasurement of the size of isothermal-areas in the presentstudy guarantees the precise results of the occurring processof thermal phenomena appearing on the human skin Inaddition the validity of TTDN confirmed the most discrimi-natory indicators for TrPs presence119879avr and isothermal-areacalculation
5 Summary and Limitations of the Study
We are unaware of any other published studies regardingthe validity and reliability of TrPs noxious stimulation byDN under IRT control to support the diagnosis of TrPsThe results of the present study were subject to the rigorand diagnostic protocol of the standards thermographicprocedure Moreover side-to-side 119879sk comparison of thepatient at rest performed before the main procedure allowedexcluding pain states related to sympathetic nervous systemactivity
TTDN seems to be a promising tool for objective TrPsconfirmation However this is the first study of this type
and the validation of TTDN on other muscles with TrPs andsome studies presenting a group with active and latent TrPsof the same muscle are required After a series of studies thatwould give the same results TTDN could be claimed as a newobjectivemethod for TrPs confirmation where DN is possibleto perform
The limitations of this study are the strong inclusion andexclusion criteria for the confirmation of gluteus minimusmuscle TrPs This muscle should be checked by TTDN whenTrPs confirmation is based on tender point presence whichprovoked typical referred pain when needle encounteredTrPs
Moreover Travell and Simons claimed that autonomicphenomena (including vasomotor reaction) within TrPsreferred pain area are limited to severe active TrPs onlyIn the present study TrPs-positive sciatic patients can beassumed to probably have severe active TrPs due to thechronicity and length of the referred pain pattern evokedby snapping palpation However the severity of active TrPsstill remains only a theoretical consideration because thereare no criteria for distinguishing the severity of active TrPs[26] Additionally other TrPs for example within the uppertrapezius muscle should be examined by TTDN to answerthe question if every TrPs present AURP is accompanied by119879avr increase
Finally the present study is limited by the lack of inter-rater reliability of TTDN
6 Conclusion
TTDN is valid and reliable for 119879avr and AURP measurementto support TrPs diagnostic criteria for the gluteus minimusmuscle when a digitally evoked referred pain pattern ispresented In the light of clinical division TTDN results indi-cate skin temperature increase for TrPs-positive contrary todecrease for TrPs-negative chronic sciatica patients and smallchanges (both increasedecrease) for healthy volunteers
Conflict of Interests
The authors declare no conflict of interests especially regard-ing patent application
Authorsrsquo Contribution
All authors listed have contributed substantially to the paperElzbieta Skorupska contributed conception and design ofthe work acquisition of data interpretation of data anddrafting the paper Michał Rychlik contributed Conceptionand design of the work acquisition of data analysis of dataand drafting the paper Włodzimierz Samborski contributedcorrection and final approval of the resubmitted version
Acknowledgments
The authors gratefully acknowledge the critical reading andcorrection of this paper by Malgorzata Mankowska Thiswork was partially supported by the Polish National ScienceCentre Grant no N N404 268339 and Poznan University ofMedical Sciences
10 BioMed Research International
References
[1] R SWeiner PainManagement A Practical Guide for CliniciansCRC Press LLC 6th edition 2002
[2] S A Skootsky B Jaeger and R K Oye ldquoPrevalence ofmyofascial pain in general internal medicine practicerdquoWesternJournal of Medicine vol 151 no 2 pp 157ndash160 1989
[3] Q Chen S Bensamoun J R Basford J M Thompsonand K-N An ldquoIdentification and quantification of myofascialtaut bands with magnetic resonance elastographyrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1658ndash1661 2007
[4] S Sikdar J P Shah T Gebreab et al ldquoNovel applications ofultrasound technology to visualize and characterize myofascialtrigger points and surrounding soft tissuerdquo Archives of PhysicalMedicine and Rehabilitation vol 90 no 11 pp 1829ndash1838 2009
[5] J G Travell andD G SimonsMyofascial Pain andDysfunctionThe Trigger PointManual vol 1WilliamsampWilkins BaltimoreMd USA 2nd edition 1999
[6] J G Travell andD G SimonsMyofascial Pain andDysfunctionTheTrigger PointManual vol 2 LippincottWilliamsampWilkinsBaltimore Md USA 1993
[7] H-Y Ge C Fernandez-de-las-Penas and L Arendt-NielsenldquoSympathetic facilitation of hyperalgesia evoked from myofas-cial tender and trigger points in patients with unilateral shoul-der painrdquoClinical Neurophysiology vol 117 no 7 pp 1545ndash15502006
[8] Y Kimura H-Y Ge Y Zhang M Kimura H Sumikura andL Arendt-Nielsen ldquoEvaluation of sympathetic vasoconstrictorresponse following nociceptive stimulation of latent myofascialtrigger points in humansrdquo Acta Physiologica vol 196 no 4 pp411ndash417 2009
[9] Y Zhang H-Y Ge S-W Yue Y Kimura and L Arendt-Nielsen ldquoAttenuated Skin blood flow response to nociceptivestimulation of latent myofascial trigger pointrdquo Archives ofPhysical Medicine and Rehabilitation vol 90 no 2 pp 325ndash3322009
[10] E Skorupska M Rychlik W Pawelec and W Samborski ldquoDryneedling related short-term vasodilation in chronic sciaticaunder infrared thermovisionrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 214374 10 pages2015
[11] E SkorupskaM Rychlik andW Samborski ldquoIntensive vasodi-latation in the sciatic pain area after dry needlingrdquo BMCComplementary and Alternative Medicine vol 15 article 722015
[12] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoTrigger point-related sympathetic nerve activity inchronic sciatic leg pain a case studyrdquo Acupuncture in Medicinevol 32 no 5 pp 418ndash422 2014
[13] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoIntensive short-term vasodilation effect in the painarea of sciatica patientsmdashcase studyrdquo BMC Research Notes vol7 no 1 article 620 2014
[14] G Affaitati A Fabrizio A Savini et al ldquoA randomizedcontrolled study comparing a lidocaine patch a placebo patchand anesthetic injection for treatment of trigger points inpatients with myofascial pain syndrome evaluation of pain andsomatic pain thresholdsrdquoClinicalTherapeutics vol 31 no 4 pp705ndash720 2009
[15] D G Simons ldquoReview of enigmatic MTrPs as a common causeof enigmatic musculoskeletal pain and dysfunctionrdquo Journal
of Electromyography and Kinesiology vol 14 no 1 pp 95ndash1072004
[16] F S Nahm ldquoInfrared thermography in pain medicinerdquo KoreanJournal of Pain vol 26 no 3 pp 219ndash222 2013
[17] A C S Costa A V D Filho A C Packer and D Rodrigues-Bigaton ldquoIntra and inter-rater reliability of infrared image anal-ysis of masticatory and upper trapezius muscles in women withand without temporomandibular disorderrdquo Brazilian Journal ofPhysical Therapy vol 17 no 1 pp 24ndash31 2013
[18] M McCoy I Campbell P Stone C Fedorchuk S Wijayawar-dana and K Easley ldquoIntra-examiner and inter-examiner repro-ducibility of paraspinal thermographyrdquo PLoS ONE vol 6 no 2Article ID e16535 2011
[19] D S Haddad M L Brioschi and E S Arita ldquoThermographicand clinical correlation of myofascial trigger points in themasticatory musclesrdquo Dentomaxillofacial Radiology vol 41 no8 pp 621ndash629 2012
[20] S J Gulevich T D Conwell J Lane et al ldquoStress infraredtelethermography is useful in the diagnosis of complex regionalpain syndrome type I (formerly reflex sympathetic dystrophy)rdquoClinical Journal of Pain vol 13 no 1 pp 50ndash59 1997
[21] G Wasner J Schattschneider and R Baron ldquoSkin temperatureside differencesmdasha diagnostic tool for CRPSrdquo Pain vol 98 no1-2 pp 19ndash26 2002
[22] E J Park K R Han Y J Chae W H Jeong and C KimldquoEffectiveness of cold stress thermography in the diagnosis ofcomplex of regional pain syndrome type 1rdquoThe Korean Journalof Pain vol 19 pp 159ndash163 2006
[23] E Skorupska M Rychlik and W Pawelec ldquoSkeletal striatedmuscle examination instrument amp new method of myofascialpain diagnosis based on the use of the instrumentrdquo Patentapplication No P-403467 Silver Medal 14ndash16 November 2013Brussels Innova the International Exhibition of InnovationEntrepreneurship and New Technologies Bronze Medal at theConcours Lepine International Paris 3004-11052014 FranceGoldMedal at the Euroinvent EuropeanExhibition ofCreativityand Innovation 22-24052014 Iasi Romania Gold Medal withDistinction at the 29th Invention and New Product ExpositionINPEX 18ndash20062014 Pittsburgh Pa USA
[24] R G Schwartz R Elliott G S Goldberg et al ldquoThe AmericanAcademy of Thermology Guidelines for neuromusculoskeletalthermographyrdquoThermology International vol 16 pp 5ndash9 2006
[25] J Dommerholt and C Fernandez-de-las-Penas Trigger PointDry Needling An Evidence and Clinical-Based ApproachChurchill Livingstone Elsevier 2013
[26] C Z Hong Braddom Physical Medicine and Rehabilitationin Muscle Pain Syndrome Elsevier New York NY USA 4thedition 2011
[27] S Mense D G Simons and I J Russell Muscle PainUnderstanding Its Nature Diagnosis and Treatment LippincottWilliams ampWilkins 2001
[28] R Rolke ldquoPseudoradicular and radicular low-back painmdashadisease continuum Rather than different entities Reply to theletters by Leffler and Hansson and by Van Boxem et alrdquo Painvol 135 pp 311ndash316 2008
[29] J M Bland and D G Altman ldquoStatistical methods for assessingagreement between two methods of clinical measurementrdquoTheLancet vol 1 no 8476 pp 307ndash310 1986
[30] D G Altman ldquoSome common problems in medical researchrdquoin Practical Statistics for Medical Research Chapman amp HallCRC Press London UK 1997
BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 7
448
419
390
362
333
304
275
246
217451
423
394
365
336
307
279
250
221
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
446
412
378
344
310
276
242
208
175446
412
378
344
310
276
242
208
175
451
422
393
365
336
307
278
249
221
451
422
393
365
336
307
278
249
221
450
418
387
355
324
293
261
230
199
450
418
387
355
324
293
261
230
199
450
416
382
349
315
282
248
214
181450
416
382
349
315
282
248
214
181
Case 1 Case 2a b c a b c
Ia
Ib
IIa
IIb
IIIa
IIIb
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
(∘C)
Figure 1 TTDN related thermograms presenting temperature reaction measured on skin surface of TrPs and non-TrPs sciatica patients andhealthy volunteers In rows I two cases of TrPs-negative sciatica II two cases of TrPs-positive sciatica and III two cases of healthy volunteerswere shown In rows Ia IIa and IIIa full thermogramwas presented In rows Ib IIb and IIIb the picture of the isothermal-area above119879max at restcalled AURP was shown (visualization of the vasodilation) In columns (a) Before TTDN (initial state) (b) state immediately after DN and(c) state immediately after observation were presented
IRT was also used for TrPs related referred pain areaexamination Although Brioschi et al [44] evaluated 304chronic myofascial pain patients using IRT before and afterDN or anesthetic infiltration they found that referred areaswere thermally asymmetric andKimura et al [8] confirmed asignificant decrease in 119879sk over time after glutamate injection(nociceptive stimulation) in latent TrPs (119901 lt 005) theusefulness of IRT for postnoxious stimulation of latent TrPsreferred pain observation was contradicted by Zhang et al[9] On the other hand one of the oldest studies on thesubject presents results similar to the present study Kruse Jrand Christiansen [45] observed referred pain pattern by IRTwhen palpation pressure over TrPs lasted around 1 minuteInitially they observed a small 119879sk increase followed by asignificant decrease in the area of the observed referredpain The DN stimulation is a much more severe type ofTrPs stimulation compared to pressure and the time ofstimulation in the present study was ten times longer Itcan be hypothesized that a stronger noxious stimulationcould provoke much more intensive 119879sk increase and maybeKruse Jr and Christiansen [45] observed the same vasomotorreactions but of a weak and short form Additionally another
difference between the studies is the localization of visiblethermal response They reported visible 119879sk changes onthe thermogram more extensive than that of the reportedreferred pain during TrPs compression contrary to thepresent study where AURP localization is limited precisely tothe area where DN provoked pain during TTDN (Figure 1)The thermogram analysis before isothermal-area calculationwas based on the indirect thermogram analysis where theexaminer had to distinguish subtle color differences Theisothermal-area calculation together with the thermogram ofAURP (gray picture Figure 1) is a nonquestionable proof ofsignificant vasomotor changes and can be easily interpretedby everyone
Interestingly the analysis of 119879avr changes in the wholegroup of subjects in the present study (Table 6) clearlyindicated 119879avr decrease for non-TrPs healthy volunteersand needle insensitive foot of TrPs-positive sciatica subjectscontrary to 119879avr increase of DN reactive subarea of TrPs-positive subjects Moreover when the thermograms of non-TrPs sciatica subjects were observed some of them presenteddiscreet vasoconstriction feature (Figure 1) and 119879sk decrease(Tables 5 and 6) These results allow putting the question of
8 BioMed Research International
Table 7 Mean value of isothermal-area below 119879max at rest changes
Isothermal-area below 119879max at rest [] Sciatica patients Healthy volunteersTTDN Phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus276 plusmn 46 76 plusmn 78 lowast minus28 plusmn 52
Calf minus265 plusmn 52 34 plusmn 57 lowast minus85 plusmn 45
Foot minus139 plusmn 513 minus39 plusmn 29 mdash minus97 plusmn 45
After observThigh minus2507 plusmn 45 102 plusmn 784 lowast minus142 plusmn 56
Calf minus248 plusmn 57 minus06 plusmn 53 lowast minus1042 plusmn 55
Foot minus152 plusmn 52 minus42 plusmn 27 mdash minus1015 plusmn 42
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 8 Mean value of isothermal-area above 119879max at rest (AURP) changes
Isothermal-area above 119879max at rest [] Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampnon-DN
After DN Thigh 0 plusmn 00 212 plusmn 265 lowastlowastlowast 114 plusmn 08
Calf 0 plusmn 00 482 plusmn 107 lowastlowastlowast 003 plusmn 002
After observ Thigh 0 plusmn 00 264 plusmn 333 lowastlowastlowast 125 plusmn 08
Calf 0 plusmn 00 663 plusmn 14 lowastlowastlowast 004 plusmn 003
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 9 Validity and reliability of TTDN components for 119879sk changes
119879sk [∘C] TTDN phases Area Sensitivity [] Specificity [] Average [∘C] Min [∘C] Max [∘C] PPV [] ICC 120581
MaximumAfter DN Thigh 100 313 119 minus02 26 577 0622 0702
Calf 100 842 066 minus08 21 667 0422 0786
After observ Thigh 100 167 129 minus01 27 545 0670 0556Calf 100 500 065 minus07 195 857 0440 0680
AverageAfter DN Thigh 100 100 099 004 195 100 0400 0880
Calf 100 100 045 minus04 13 100 0511 0902
After observ Thigh 100 846 111 009 22 750 0333 0786Calf 100 944 044 minus06 15 857 0422 0845
Table 10 Validity and reliability of TTDN components for isothermal-area changes
Isothermal-area TTDN phases Area Sensitivity [] Specificity [] Mean [] Min [] Max [] PPV [] ICC 120581
AURP (above 119879max at rest)After DN Thigh 100 100 212 06 418 100 0689 0938
Calf 100 100 48 minus35 131 100 0778 0956
After observ Thigh 100 100 264 06 522 100 0644 0929Calf 100 100 66 minus44 177 100 0778 0956
Below 119879max at rest
After DN Thigh 100 00 758 minus527 678 500 0778 0656Calf 100 200 337 minus407 474 778 0556 0707
After observ Thigh 100 00 102 minus597 618 500 0778 0656Calf 100 750 minus059 minus419 407 875 0511 0827
Below + above 119879max at rest
After DN Thigh 100 222 288 minus293 869 682 0578 0696Calf 100 370 819 minus136 628 778 0578 0782
After observ Thigh 100 00 1987 minus55 453 483 0733 0643Calf 100 782 605 minus127 576 794 0644 0847
BioMed Research International 9
whether the authors of the previous study who confirmedTrPs-related vasoconstriction really stimulated TrPs On theother hand maybe the type of TrPs (latent TrPs) or regionof IRT observation (upper extremity) or type of noxiousstimulation (glutamate injection) can explain contrary results[8 9] Further studies considering both active and latent TrPsdifferent regions of the body and so forth are required
The New IdeamdashIsothermal-Area Calculation The standardusage of IRT in medicine is based on mean temperature andstandard deviation within the fixed region of interest (ROi)as well as the visualized interpretation of the thermogramwhere each temperature value (or a group of similar values)is attributed to a specified color The color variation is theonly indirect analysis and this type of interpretation is limitedto the physician trained in thermology Additionally theuse of spot temperature measurements or observation ofselected values of 119879max or 119879avr may not produce the expectedoutcomes and the results obtained this way may differ a lotfrom the real situation In summary the comparison of 119879avrof ROi is performed without considering the size of ROiThus an error resulting from the statistical interpretation ispossible These facts can explain the controversies aroundthe merit of IRT measurement in medicine However it hasbeen postulated that considering the number of pixels inthe observed ROi that is the qualitative evaluation of forexample its size and shape together with 119879avr can lead to anobjective interpretation of the results [16]
TTDN is the method which allows assessing the thermo-gram in this recommended wayThemeasurement of the sizeof isothermal-areas in the present study guarantees the pre-cise results of the occurring process of thermal phenomenaappearing on the human skin In addition TTDN analysisaccounts for 100 of the information recorded on a singlethermogram
The next innovativeness of TTDN apart from calculatingthe size of ROi is the possibility of showing vasomotorreactions in TrPs referred pain area The results are easyto interpret and not limited by a physician experience Themeasurement of the size of isothermal-areas in the presentstudy guarantees the precise results of the occurring processof thermal phenomena appearing on the human skin Inaddition the validity of TTDN confirmed the most discrimi-natory indicators for TrPs presence119879avr and isothermal-areacalculation
5 Summary and Limitations of the Study
We are unaware of any other published studies regardingthe validity and reliability of TrPs noxious stimulation byDN under IRT control to support the diagnosis of TrPsThe results of the present study were subject to the rigorand diagnostic protocol of the standards thermographicprocedure Moreover side-to-side 119879sk comparison of thepatient at rest performed before the main procedure allowedexcluding pain states related to sympathetic nervous systemactivity
TTDN seems to be a promising tool for objective TrPsconfirmation However this is the first study of this type
and the validation of TTDN on other muscles with TrPs andsome studies presenting a group with active and latent TrPsof the same muscle are required After a series of studies thatwould give the same results TTDN could be claimed as a newobjectivemethod for TrPs confirmation where DN is possibleto perform
The limitations of this study are the strong inclusion andexclusion criteria for the confirmation of gluteus minimusmuscle TrPs This muscle should be checked by TTDN whenTrPs confirmation is based on tender point presence whichprovoked typical referred pain when needle encounteredTrPs
Moreover Travell and Simons claimed that autonomicphenomena (including vasomotor reaction) within TrPsreferred pain area are limited to severe active TrPs onlyIn the present study TrPs-positive sciatic patients can beassumed to probably have severe active TrPs due to thechronicity and length of the referred pain pattern evokedby snapping palpation However the severity of active TrPsstill remains only a theoretical consideration because thereare no criteria for distinguishing the severity of active TrPs[26] Additionally other TrPs for example within the uppertrapezius muscle should be examined by TTDN to answerthe question if every TrPs present AURP is accompanied by119879avr increase
Finally the present study is limited by the lack of inter-rater reliability of TTDN
6 Conclusion
TTDN is valid and reliable for 119879avr and AURP measurementto support TrPs diagnostic criteria for the gluteus minimusmuscle when a digitally evoked referred pain pattern ispresented In the light of clinical division TTDN results indi-cate skin temperature increase for TrPs-positive contrary todecrease for TrPs-negative chronic sciatica patients and smallchanges (both increasedecrease) for healthy volunteers
Conflict of Interests
The authors declare no conflict of interests especially regard-ing patent application
Authorsrsquo Contribution
All authors listed have contributed substantially to the paperElzbieta Skorupska contributed conception and design ofthe work acquisition of data interpretation of data anddrafting the paper Michał Rychlik contributed Conceptionand design of the work acquisition of data analysis of dataand drafting the paper Włodzimierz Samborski contributedcorrection and final approval of the resubmitted version
Acknowledgments
The authors gratefully acknowledge the critical reading andcorrection of this paper by Malgorzata Mankowska Thiswork was partially supported by the Polish National ScienceCentre Grant no N N404 268339 and Poznan University ofMedical Sciences
10 BioMed Research International
References
[1] R SWeiner PainManagement A Practical Guide for CliniciansCRC Press LLC 6th edition 2002
[2] S A Skootsky B Jaeger and R K Oye ldquoPrevalence ofmyofascial pain in general internal medicine practicerdquoWesternJournal of Medicine vol 151 no 2 pp 157ndash160 1989
[3] Q Chen S Bensamoun J R Basford J M Thompsonand K-N An ldquoIdentification and quantification of myofascialtaut bands with magnetic resonance elastographyrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1658ndash1661 2007
[4] S Sikdar J P Shah T Gebreab et al ldquoNovel applications ofultrasound technology to visualize and characterize myofascialtrigger points and surrounding soft tissuerdquo Archives of PhysicalMedicine and Rehabilitation vol 90 no 11 pp 1829ndash1838 2009
[5] J G Travell andD G SimonsMyofascial Pain andDysfunctionThe Trigger PointManual vol 1WilliamsampWilkins BaltimoreMd USA 2nd edition 1999
[6] J G Travell andD G SimonsMyofascial Pain andDysfunctionTheTrigger PointManual vol 2 LippincottWilliamsampWilkinsBaltimore Md USA 1993
[7] H-Y Ge C Fernandez-de-las-Penas and L Arendt-NielsenldquoSympathetic facilitation of hyperalgesia evoked from myofas-cial tender and trigger points in patients with unilateral shoul-der painrdquoClinical Neurophysiology vol 117 no 7 pp 1545ndash15502006
[8] Y Kimura H-Y Ge Y Zhang M Kimura H Sumikura andL Arendt-Nielsen ldquoEvaluation of sympathetic vasoconstrictorresponse following nociceptive stimulation of latent myofascialtrigger points in humansrdquo Acta Physiologica vol 196 no 4 pp411ndash417 2009
[9] Y Zhang H-Y Ge S-W Yue Y Kimura and L Arendt-Nielsen ldquoAttenuated Skin blood flow response to nociceptivestimulation of latent myofascial trigger pointrdquo Archives ofPhysical Medicine and Rehabilitation vol 90 no 2 pp 325ndash3322009
[10] E Skorupska M Rychlik W Pawelec and W Samborski ldquoDryneedling related short-term vasodilation in chronic sciaticaunder infrared thermovisionrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 214374 10 pages2015
[11] E SkorupskaM Rychlik andW Samborski ldquoIntensive vasodi-latation in the sciatic pain area after dry needlingrdquo BMCComplementary and Alternative Medicine vol 15 article 722015
[12] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoTrigger point-related sympathetic nerve activity inchronic sciatic leg pain a case studyrdquo Acupuncture in Medicinevol 32 no 5 pp 418ndash422 2014
[13] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoIntensive short-term vasodilation effect in the painarea of sciatica patientsmdashcase studyrdquo BMC Research Notes vol7 no 1 article 620 2014
[14] G Affaitati A Fabrizio A Savini et al ldquoA randomizedcontrolled study comparing a lidocaine patch a placebo patchand anesthetic injection for treatment of trigger points inpatients with myofascial pain syndrome evaluation of pain andsomatic pain thresholdsrdquoClinicalTherapeutics vol 31 no 4 pp705ndash720 2009
[15] D G Simons ldquoReview of enigmatic MTrPs as a common causeof enigmatic musculoskeletal pain and dysfunctionrdquo Journal
of Electromyography and Kinesiology vol 14 no 1 pp 95ndash1072004
[16] F S Nahm ldquoInfrared thermography in pain medicinerdquo KoreanJournal of Pain vol 26 no 3 pp 219ndash222 2013
[17] A C S Costa A V D Filho A C Packer and D Rodrigues-Bigaton ldquoIntra and inter-rater reliability of infrared image anal-ysis of masticatory and upper trapezius muscles in women withand without temporomandibular disorderrdquo Brazilian Journal ofPhysical Therapy vol 17 no 1 pp 24ndash31 2013
[18] M McCoy I Campbell P Stone C Fedorchuk S Wijayawar-dana and K Easley ldquoIntra-examiner and inter-examiner repro-ducibility of paraspinal thermographyrdquo PLoS ONE vol 6 no 2Article ID e16535 2011
[19] D S Haddad M L Brioschi and E S Arita ldquoThermographicand clinical correlation of myofascial trigger points in themasticatory musclesrdquo Dentomaxillofacial Radiology vol 41 no8 pp 621ndash629 2012
[20] S J Gulevich T D Conwell J Lane et al ldquoStress infraredtelethermography is useful in the diagnosis of complex regionalpain syndrome type I (formerly reflex sympathetic dystrophy)rdquoClinical Journal of Pain vol 13 no 1 pp 50ndash59 1997
[21] G Wasner J Schattschneider and R Baron ldquoSkin temperatureside differencesmdasha diagnostic tool for CRPSrdquo Pain vol 98 no1-2 pp 19ndash26 2002
[22] E J Park K R Han Y J Chae W H Jeong and C KimldquoEffectiveness of cold stress thermography in the diagnosis ofcomplex of regional pain syndrome type 1rdquoThe Korean Journalof Pain vol 19 pp 159ndash163 2006
[23] E Skorupska M Rychlik and W Pawelec ldquoSkeletal striatedmuscle examination instrument amp new method of myofascialpain diagnosis based on the use of the instrumentrdquo Patentapplication No P-403467 Silver Medal 14ndash16 November 2013Brussels Innova the International Exhibition of InnovationEntrepreneurship and New Technologies Bronze Medal at theConcours Lepine International Paris 3004-11052014 FranceGoldMedal at the Euroinvent EuropeanExhibition ofCreativityand Innovation 22-24052014 Iasi Romania Gold Medal withDistinction at the 29th Invention and New Product ExpositionINPEX 18ndash20062014 Pittsburgh Pa USA
[24] R G Schwartz R Elliott G S Goldberg et al ldquoThe AmericanAcademy of Thermology Guidelines for neuromusculoskeletalthermographyrdquoThermology International vol 16 pp 5ndash9 2006
[25] J Dommerholt and C Fernandez-de-las-Penas Trigger PointDry Needling An Evidence and Clinical-Based ApproachChurchill Livingstone Elsevier 2013
[26] C Z Hong Braddom Physical Medicine and Rehabilitationin Muscle Pain Syndrome Elsevier New York NY USA 4thedition 2011
[27] S Mense D G Simons and I J Russell Muscle PainUnderstanding Its Nature Diagnosis and Treatment LippincottWilliams ampWilkins 2001
[28] R Rolke ldquoPseudoradicular and radicular low-back painmdashadisease continuum Rather than different entities Reply to theletters by Leffler and Hansson and by Van Boxem et alrdquo Painvol 135 pp 311ndash316 2008
[29] J M Bland and D G Altman ldquoStatistical methods for assessingagreement between two methods of clinical measurementrdquoTheLancet vol 1 no 8476 pp 307ndash310 1986
[30] D G Altman ldquoSome common problems in medical researchrdquoin Practical Statistics for Medical Research Chapman amp HallCRC Press London UK 1997
BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
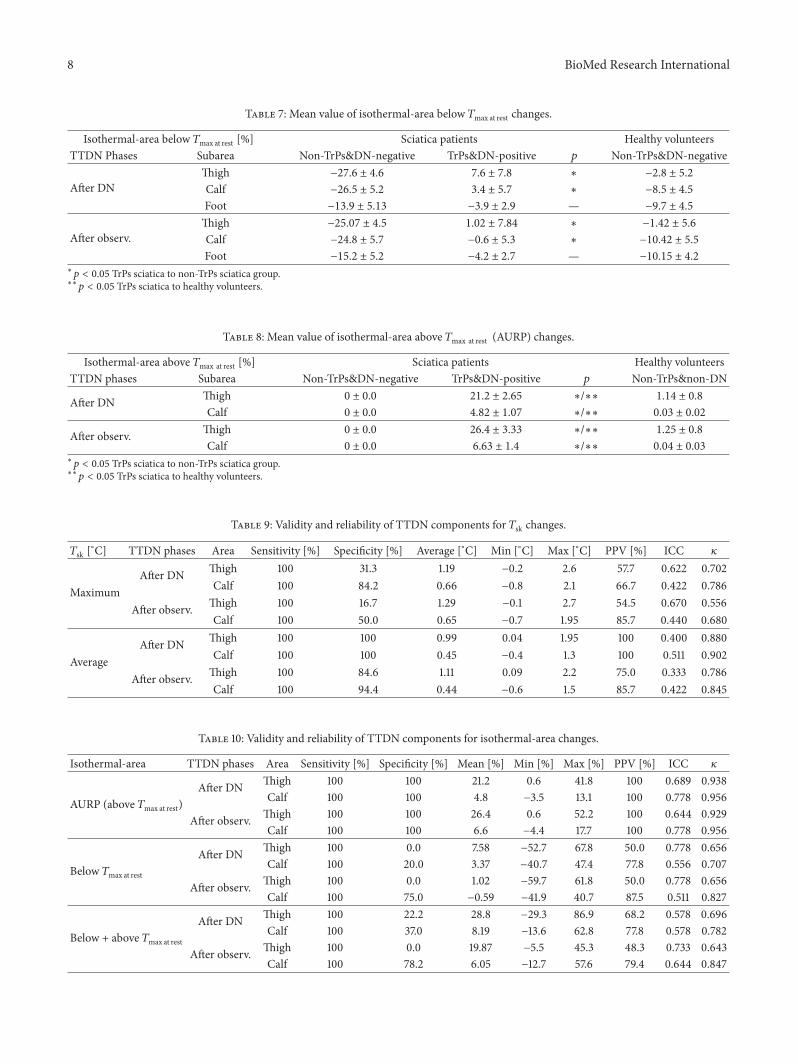
8 BioMed Research International
Table 7 Mean value of isothermal-area below 119879max at rest changes
Isothermal-area below 119879max at rest [] Sciatica patients Healthy volunteersTTDN Phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampDN-negative
After DNThigh minus276 plusmn 46 76 plusmn 78 lowast minus28 plusmn 52
Calf minus265 plusmn 52 34 plusmn 57 lowast minus85 plusmn 45
Foot minus139 plusmn 513 minus39 plusmn 29 mdash minus97 plusmn 45
After observThigh minus2507 plusmn 45 102 plusmn 784 lowast minus142 plusmn 56
Calf minus248 plusmn 57 minus06 plusmn 53 lowast minus1042 plusmn 55
Foot minus152 plusmn 52 minus42 plusmn 27 mdash minus1015 plusmn 42
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 8 Mean value of isothermal-area above 119879max at rest (AURP) changes
Isothermal-area above 119879max at rest [] Sciatica patients Healthy volunteersTTDN phases Subarea Non-TrPsampDN-negative TrPsampDN-positive 119901 Non-TrPsampnon-DN
After DN Thigh 0 plusmn 00 212 plusmn 265 lowastlowastlowast 114 plusmn 08
Calf 0 plusmn 00 482 plusmn 107 lowastlowastlowast 003 plusmn 002
After observ Thigh 0 plusmn 00 264 plusmn 333 lowastlowastlowast 125 plusmn 08
Calf 0 plusmn 00 663 plusmn 14 lowastlowastlowast 004 plusmn 003
lowast
119901 lt 005 TrPs sciatica to non-TrPs sciatica grouplowastlowast
119901 lt 005 TrPs sciatica to healthy volunteers
Table 9 Validity and reliability of TTDN components for 119879sk changes
119879sk [∘C] TTDN phases Area Sensitivity [] Specificity [] Average [∘C] Min [∘C] Max [∘C] PPV [] ICC 120581
MaximumAfter DN Thigh 100 313 119 minus02 26 577 0622 0702
Calf 100 842 066 minus08 21 667 0422 0786
After observ Thigh 100 167 129 minus01 27 545 0670 0556Calf 100 500 065 minus07 195 857 0440 0680
AverageAfter DN Thigh 100 100 099 004 195 100 0400 0880
Calf 100 100 045 minus04 13 100 0511 0902
After observ Thigh 100 846 111 009 22 750 0333 0786Calf 100 944 044 minus06 15 857 0422 0845
Table 10 Validity and reliability of TTDN components for isothermal-area changes
Isothermal-area TTDN phases Area Sensitivity [] Specificity [] Mean [] Min [] Max [] PPV [] ICC 120581
AURP (above 119879max at rest)After DN Thigh 100 100 212 06 418 100 0689 0938
Calf 100 100 48 minus35 131 100 0778 0956
After observ Thigh 100 100 264 06 522 100 0644 0929Calf 100 100 66 minus44 177 100 0778 0956
Below 119879max at rest
After DN Thigh 100 00 758 minus527 678 500 0778 0656Calf 100 200 337 minus407 474 778 0556 0707
After observ Thigh 100 00 102 minus597 618 500 0778 0656Calf 100 750 minus059 minus419 407 875 0511 0827
Below + above 119879max at rest
After DN Thigh 100 222 288 minus293 869 682 0578 0696Calf 100 370 819 minus136 628 778 0578 0782
After observ Thigh 100 00 1987 minus55 453 483 0733 0643Calf 100 782 605 minus127 576 794 0644 0847
BioMed Research International 9
whether the authors of the previous study who confirmedTrPs-related vasoconstriction really stimulated TrPs On theother hand maybe the type of TrPs (latent TrPs) or regionof IRT observation (upper extremity) or type of noxiousstimulation (glutamate injection) can explain contrary results[8 9] Further studies considering both active and latent TrPsdifferent regions of the body and so forth are required
The New IdeamdashIsothermal-Area Calculation The standardusage of IRT in medicine is based on mean temperature andstandard deviation within the fixed region of interest (ROi)as well as the visualized interpretation of the thermogramwhere each temperature value (or a group of similar values)is attributed to a specified color The color variation is theonly indirect analysis and this type of interpretation is limitedto the physician trained in thermology Additionally theuse of spot temperature measurements or observation ofselected values of 119879max or 119879avr may not produce the expectedoutcomes and the results obtained this way may differ a lotfrom the real situation In summary the comparison of 119879avrof ROi is performed without considering the size of ROiThus an error resulting from the statistical interpretation ispossible These facts can explain the controversies aroundthe merit of IRT measurement in medicine However it hasbeen postulated that considering the number of pixels inthe observed ROi that is the qualitative evaluation of forexample its size and shape together with 119879avr can lead to anobjective interpretation of the results [16]
TTDN is the method which allows assessing the thermo-gram in this recommended wayThemeasurement of the sizeof isothermal-areas in the present study guarantees the pre-cise results of the occurring process of thermal phenomenaappearing on the human skin In addition TTDN analysisaccounts for 100 of the information recorded on a singlethermogram
The next innovativeness of TTDN apart from calculatingthe size of ROi is the possibility of showing vasomotorreactions in TrPs referred pain area The results are easyto interpret and not limited by a physician experience Themeasurement of the size of isothermal-areas in the presentstudy guarantees the precise results of the occurring processof thermal phenomena appearing on the human skin Inaddition the validity of TTDN confirmed the most discrimi-natory indicators for TrPs presence119879avr and isothermal-areacalculation
5 Summary and Limitations of the Study
We are unaware of any other published studies regardingthe validity and reliability of TrPs noxious stimulation byDN under IRT control to support the diagnosis of TrPsThe results of the present study were subject to the rigorand diagnostic protocol of the standards thermographicprocedure Moreover side-to-side 119879sk comparison of thepatient at rest performed before the main procedure allowedexcluding pain states related to sympathetic nervous systemactivity
TTDN seems to be a promising tool for objective TrPsconfirmation However this is the first study of this type
and the validation of TTDN on other muscles with TrPs andsome studies presenting a group with active and latent TrPsof the same muscle are required After a series of studies thatwould give the same results TTDN could be claimed as a newobjectivemethod for TrPs confirmation where DN is possibleto perform
The limitations of this study are the strong inclusion andexclusion criteria for the confirmation of gluteus minimusmuscle TrPs This muscle should be checked by TTDN whenTrPs confirmation is based on tender point presence whichprovoked typical referred pain when needle encounteredTrPs
Moreover Travell and Simons claimed that autonomicphenomena (including vasomotor reaction) within TrPsreferred pain area are limited to severe active TrPs onlyIn the present study TrPs-positive sciatic patients can beassumed to probably have severe active TrPs due to thechronicity and length of the referred pain pattern evokedby snapping palpation However the severity of active TrPsstill remains only a theoretical consideration because thereare no criteria for distinguishing the severity of active TrPs[26] Additionally other TrPs for example within the uppertrapezius muscle should be examined by TTDN to answerthe question if every TrPs present AURP is accompanied by119879avr increase
Finally the present study is limited by the lack of inter-rater reliability of TTDN
6 Conclusion
TTDN is valid and reliable for 119879avr and AURP measurementto support TrPs diagnostic criteria for the gluteus minimusmuscle when a digitally evoked referred pain pattern ispresented In the light of clinical division TTDN results indi-cate skin temperature increase for TrPs-positive contrary todecrease for TrPs-negative chronic sciatica patients and smallchanges (both increasedecrease) for healthy volunteers
Conflict of Interests
The authors declare no conflict of interests especially regard-ing patent application
Authorsrsquo Contribution
All authors listed have contributed substantially to the paperElzbieta Skorupska contributed conception and design ofthe work acquisition of data interpretation of data anddrafting the paper Michał Rychlik contributed Conceptionand design of the work acquisition of data analysis of dataand drafting the paper Włodzimierz Samborski contributedcorrection and final approval of the resubmitted version
Acknowledgments
The authors gratefully acknowledge the critical reading andcorrection of this paper by Malgorzata Mankowska Thiswork was partially supported by the Polish National ScienceCentre Grant no N N404 268339 and Poznan University ofMedical Sciences
10 BioMed Research International
References
[1] R SWeiner PainManagement A Practical Guide for CliniciansCRC Press LLC 6th edition 2002
[2] S A Skootsky B Jaeger and R K Oye ldquoPrevalence ofmyofascial pain in general internal medicine practicerdquoWesternJournal of Medicine vol 151 no 2 pp 157ndash160 1989
[3] Q Chen S Bensamoun J R Basford J M Thompsonand K-N An ldquoIdentification and quantification of myofascialtaut bands with magnetic resonance elastographyrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1658ndash1661 2007
[4] S Sikdar J P Shah T Gebreab et al ldquoNovel applications ofultrasound technology to visualize and characterize myofascialtrigger points and surrounding soft tissuerdquo Archives of PhysicalMedicine and Rehabilitation vol 90 no 11 pp 1829ndash1838 2009
[5] J G Travell andD G SimonsMyofascial Pain andDysfunctionThe Trigger PointManual vol 1WilliamsampWilkins BaltimoreMd USA 2nd edition 1999
[6] J G Travell andD G SimonsMyofascial Pain andDysfunctionTheTrigger PointManual vol 2 LippincottWilliamsampWilkinsBaltimore Md USA 1993
[7] H-Y Ge C Fernandez-de-las-Penas and L Arendt-NielsenldquoSympathetic facilitation of hyperalgesia evoked from myofas-cial tender and trigger points in patients with unilateral shoul-der painrdquoClinical Neurophysiology vol 117 no 7 pp 1545ndash15502006
[8] Y Kimura H-Y Ge Y Zhang M Kimura H Sumikura andL Arendt-Nielsen ldquoEvaluation of sympathetic vasoconstrictorresponse following nociceptive stimulation of latent myofascialtrigger points in humansrdquo Acta Physiologica vol 196 no 4 pp411ndash417 2009
[9] Y Zhang H-Y Ge S-W Yue Y Kimura and L Arendt-Nielsen ldquoAttenuated Skin blood flow response to nociceptivestimulation of latent myofascial trigger pointrdquo Archives ofPhysical Medicine and Rehabilitation vol 90 no 2 pp 325ndash3322009
[10] E Skorupska M Rychlik W Pawelec and W Samborski ldquoDryneedling related short-term vasodilation in chronic sciaticaunder infrared thermovisionrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 214374 10 pages2015
[11] E SkorupskaM Rychlik andW Samborski ldquoIntensive vasodi-latation in the sciatic pain area after dry needlingrdquo BMCComplementary and Alternative Medicine vol 15 article 722015
[12] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoTrigger point-related sympathetic nerve activity inchronic sciatic leg pain a case studyrdquo Acupuncture in Medicinevol 32 no 5 pp 418ndash422 2014
[13] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoIntensive short-term vasodilation effect in the painarea of sciatica patientsmdashcase studyrdquo BMC Research Notes vol7 no 1 article 620 2014
[14] G Affaitati A Fabrizio A Savini et al ldquoA randomizedcontrolled study comparing a lidocaine patch a placebo patchand anesthetic injection for treatment of trigger points inpatients with myofascial pain syndrome evaluation of pain andsomatic pain thresholdsrdquoClinicalTherapeutics vol 31 no 4 pp705ndash720 2009
[15] D G Simons ldquoReview of enigmatic MTrPs as a common causeof enigmatic musculoskeletal pain and dysfunctionrdquo Journal
of Electromyography and Kinesiology vol 14 no 1 pp 95ndash1072004
[16] F S Nahm ldquoInfrared thermography in pain medicinerdquo KoreanJournal of Pain vol 26 no 3 pp 219ndash222 2013
[17] A C S Costa A V D Filho A C Packer and D Rodrigues-Bigaton ldquoIntra and inter-rater reliability of infrared image anal-ysis of masticatory and upper trapezius muscles in women withand without temporomandibular disorderrdquo Brazilian Journal ofPhysical Therapy vol 17 no 1 pp 24ndash31 2013
[18] M McCoy I Campbell P Stone C Fedorchuk S Wijayawar-dana and K Easley ldquoIntra-examiner and inter-examiner repro-ducibility of paraspinal thermographyrdquo PLoS ONE vol 6 no 2Article ID e16535 2011
[19] D S Haddad M L Brioschi and E S Arita ldquoThermographicand clinical correlation of myofascial trigger points in themasticatory musclesrdquo Dentomaxillofacial Radiology vol 41 no8 pp 621ndash629 2012
[20] S J Gulevich T D Conwell J Lane et al ldquoStress infraredtelethermography is useful in the diagnosis of complex regionalpain syndrome type I (formerly reflex sympathetic dystrophy)rdquoClinical Journal of Pain vol 13 no 1 pp 50ndash59 1997
[21] G Wasner J Schattschneider and R Baron ldquoSkin temperatureside differencesmdasha diagnostic tool for CRPSrdquo Pain vol 98 no1-2 pp 19ndash26 2002
[22] E J Park K R Han Y J Chae W H Jeong and C KimldquoEffectiveness of cold stress thermography in the diagnosis ofcomplex of regional pain syndrome type 1rdquoThe Korean Journalof Pain vol 19 pp 159ndash163 2006
[23] E Skorupska M Rychlik and W Pawelec ldquoSkeletal striatedmuscle examination instrument amp new method of myofascialpain diagnosis based on the use of the instrumentrdquo Patentapplication No P-403467 Silver Medal 14ndash16 November 2013Brussels Innova the International Exhibition of InnovationEntrepreneurship and New Technologies Bronze Medal at theConcours Lepine International Paris 3004-11052014 FranceGoldMedal at the Euroinvent EuropeanExhibition ofCreativityand Innovation 22-24052014 Iasi Romania Gold Medal withDistinction at the 29th Invention and New Product ExpositionINPEX 18ndash20062014 Pittsburgh Pa USA
[24] R G Schwartz R Elliott G S Goldberg et al ldquoThe AmericanAcademy of Thermology Guidelines for neuromusculoskeletalthermographyrdquoThermology International vol 16 pp 5ndash9 2006
[25] J Dommerholt and C Fernandez-de-las-Penas Trigger PointDry Needling An Evidence and Clinical-Based ApproachChurchill Livingstone Elsevier 2013
[26] C Z Hong Braddom Physical Medicine and Rehabilitationin Muscle Pain Syndrome Elsevier New York NY USA 4thedition 2011
[27] S Mense D G Simons and I J Russell Muscle PainUnderstanding Its Nature Diagnosis and Treatment LippincottWilliams ampWilkins 2001
[28] R Rolke ldquoPseudoradicular and radicular low-back painmdashadisease continuum Rather than different entities Reply to theletters by Leffler and Hansson and by Van Boxem et alrdquo Painvol 135 pp 311ndash316 2008
[29] J M Bland and D G Altman ldquoStatistical methods for assessingagreement between two methods of clinical measurementrdquoTheLancet vol 1 no 8476 pp 307ndash310 1986
[30] D G Altman ldquoSome common problems in medical researchrdquoin Practical Statistics for Medical Research Chapman amp HallCRC Press London UK 1997
BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 9
whether the authors of the previous study who confirmedTrPs-related vasoconstriction really stimulated TrPs On theother hand maybe the type of TrPs (latent TrPs) or regionof IRT observation (upper extremity) or type of noxiousstimulation (glutamate injection) can explain contrary results[8 9] Further studies considering both active and latent TrPsdifferent regions of the body and so forth are required
The New IdeamdashIsothermal-Area Calculation The standardusage of IRT in medicine is based on mean temperature andstandard deviation within the fixed region of interest (ROi)as well as the visualized interpretation of the thermogramwhere each temperature value (or a group of similar values)is attributed to a specified color The color variation is theonly indirect analysis and this type of interpretation is limitedto the physician trained in thermology Additionally theuse of spot temperature measurements or observation ofselected values of 119879max or 119879avr may not produce the expectedoutcomes and the results obtained this way may differ a lotfrom the real situation In summary the comparison of 119879avrof ROi is performed without considering the size of ROiThus an error resulting from the statistical interpretation ispossible These facts can explain the controversies aroundthe merit of IRT measurement in medicine However it hasbeen postulated that considering the number of pixels inthe observed ROi that is the qualitative evaluation of forexample its size and shape together with 119879avr can lead to anobjective interpretation of the results [16]
TTDN is the method which allows assessing the thermo-gram in this recommended wayThemeasurement of the sizeof isothermal-areas in the present study guarantees the pre-cise results of the occurring process of thermal phenomenaappearing on the human skin In addition TTDN analysisaccounts for 100 of the information recorded on a singlethermogram
The next innovativeness of TTDN apart from calculatingthe size of ROi is the possibility of showing vasomotorreactions in TrPs referred pain area The results are easyto interpret and not limited by a physician experience Themeasurement of the size of isothermal-areas in the presentstudy guarantees the precise results of the occurring processof thermal phenomena appearing on the human skin Inaddition the validity of TTDN confirmed the most discrimi-natory indicators for TrPs presence119879avr and isothermal-areacalculation
5 Summary and Limitations of the Study
We are unaware of any other published studies regardingthe validity and reliability of TrPs noxious stimulation byDN under IRT control to support the diagnosis of TrPsThe results of the present study were subject to the rigorand diagnostic protocol of the standards thermographicprocedure Moreover side-to-side 119879sk comparison of thepatient at rest performed before the main procedure allowedexcluding pain states related to sympathetic nervous systemactivity
TTDN seems to be a promising tool for objective TrPsconfirmation However this is the first study of this type
and the validation of TTDN on other muscles with TrPs andsome studies presenting a group with active and latent TrPsof the same muscle are required After a series of studies thatwould give the same results TTDN could be claimed as a newobjectivemethod for TrPs confirmation where DN is possibleto perform
The limitations of this study are the strong inclusion andexclusion criteria for the confirmation of gluteus minimusmuscle TrPs This muscle should be checked by TTDN whenTrPs confirmation is based on tender point presence whichprovoked typical referred pain when needle encounteredTrPs
Moreover Travell and Simons claimed that autonomicphenomena (including vasomotor reaction) within TrPsreferred pain area are limited to severe active TrPs onlyIn the present study TrPs-positive sciatic patients can beassumed to probably have severe active TrPs due to thechronicity and length of the referred pain pattern evokedby snapping palpation However the severity of active TrPsstill remains only a theoretical consideration because thereare no criteria for distinguishing the severity of active TrPs[26] Additionally other TrPs for example within the uppertrapezius muscle should be examined by TTDN to answerthe question if every TrPs present AURP is accompanied by119879avr increase
Finally the present study is limited by the lack of inter-rater reliability of TTDN
6 Conclusion
TTDN is valid and reliable for 119879avr and AURP measurementto support TrPs diagnostic criteria for the gluteus minimusmuscle when a digitally evoked referred pain pattern ispresented In the light of clinical division TTDN results indi-cate skin temperature increase for TrPs-positive contrary todecrease for TrPs-negative chronic sciatica patients and smallchanges (both increasedecrease) for healthy volunteers
Conflict of Interests
The authors declare no conflict of interests especially regard-ing patent application
Authorsrsquo Contribution
All authors listed have contributed substantially to the paperElzbieta Skorupska contributed conception and design ofthe work acquisition of data interpretation of data anddrafting the paper Michał Rychlik contributed Conceptionand design of the work acquisition of data analysis of dataand drafting the paper Włodzimierz Samborski contributedcorrection and final approval of the resubmitted version
Acknowledgments
The authors gratefully acknowledge the critical reading andcorrection of this paper by Malgorzata Mankowska Thiswork was partially supported by the Polish National ScienceCentre Grant no N N404 268339 and Poznan University ofMedical Sciences
10 BioMed Research International
References
[1] R SWeiner PainManagement A Practical Guide for CliniciansCRC Press LLC 6th edition 2002
[2] S A Skootsky B Jaeger and R K Oye ldquoPrevalence ofmyofascial pain in general internal medicine practicerdquoWesternJournal of Medicine vol 151 no 2 pp 157ndash160 1989
[3] Q Chen S Bensamoun J R Basford J M Thompsonand K-N An ldquoIdentification and quantification of myofascialtaut bands with magnetic resonance elastographyrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1658ndash1661 2007
[4] S Sikdar J P Shah T Gebreab et al ldquoNovel applications ofultrasound technology to visualize and characterize myofascialtrigger points and surrounding soft tissuerdquo Archives of PhysicalMedicine and Rehabilitation vol 90 no 11 pp 1829ndash1838 2009
[5] J G Travell andD G SimonsMyofascial Pain andDysfunctionThe Trigger PointManual vol 1WilliamsampWilkins BaltimoreMd USA 2nd edition 1999
[6] J G Travell andD G SimonsMyofascial Pain andDysfunctionTheTrigger PointManual vol 2 LippincottWilliamsampWilkinsBaltimore Md USA 1993
[7] H-Y Ge C Fernandez-de-las-Penas and L Arendt-NielsenldquoSympathetic facilitation of hyperalgesia evoked from myofas-cial tender and trigger points in patients with unilateral shoul-der painrdquoClinical Neurophysiology vol 117 no 7 pp 1545ndash15502006
[8] Y Kimura H-Y Ge Y Zhang M Kimura H Sumikura andL Arendt-Nielsen ldquoEvaluation of sympathetic vasoconstrictorresponse following nociceptive stimulation of latent myofascialtrigger points in humansrdquo Acta Physiologica vol 196 no 4 pp411ndash417 2009
[9] Y Zhang H-Y Ge S-W Yue Y Kimura and L Arendt-Nielsen ldquoAttenuated Skin blood flow response to nociceptivestimulation of latent myofascial trigger pointrdquo Archives ofPhysical Medicine and Rehabilitation vol 90 no 2 pp 325ndash3322009
[10] E Skorupska M Rychlik W Pawelec and W Samborski ldquoDryneedling related short-term vasodilation in chronic sciaticaunder infrared thermovisionrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 214374 10 pages2015
[11] E SkorupskaM Rychlik andW Samborski ldquoIntensive vasodi-latation in the sciatic pain area after dry needlingrdquo BMCComplementary and Alternative Medicine vol 15 article 722015
[12] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoTrigger point-related sympathetic nerve activity inchronic sciatic leg pain a case studyrdquo Acupuncture in Medicinevol 32 no 5 pp 418ndash422 2014
[13] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoIntensive short-term vasodilation effect in the painarea of sciatica patientsmdashcase studyrdquo BMC Research Notes vol7 no 1 article 620 2014
[14] G Affaitati A Fabrizio A Savini et al ldquoA randomizedcontrolled study comparing a lidocaine patch a placebo patchand anesthetic injection for treatment of trigger points inpatients with myofascial pain syndrome evaluation of pain andsomatic pain thresholdsrdquoClinicalTherapeutics vol 31 no 4 pp705ndash720 2009
[15] D G Simons ldquoReview of enigmatic MTrPs as a common causeof enigmatic musculoskeletal pain and dysfunctionrdquo Journal
of Electromyography and Kinesiology vol 14 no 1 pp 95ndash1072004
[16] F S Nahm ldquoInfrared thermography in pain medicinerdquo KoreanJournal of Pain vol 26 no 3 pp 219ndash222 2013
[17] A C S Costa A V D Filho A C Packer and D Rodrigues-Bigaton ldquoIntra and inter-rater reliability of infrared image anal-ysis of masticatory and upper trapezius muscles in women withand without temporomandibular disorderrdquo Brazilian Journal ofPhysical Therapy vol 17 no 1 pp 24ndash31 2013
[18] M McCoy I Campbell P Stone C Fedorchuk S Wijayawar-dana and K Easley ldquoIntra-examiner and inter-examiner repro-ducibility of paraspinal thermographyrdquo PLoS ONE vol 6 no 2Article ID e16535 2011
[19] D S Haddad M L Brioschi and E S Arita ldquoThermographicand clinical correlation of myofascial trigger points in themasticatory musclesrdquo Dentomaxillofacial Radiology vol 41 no8 pp 621ndash629 2012
[20] S J Gulevich T D Conwell J Lane et al ldquoStress infraredtelethermography is useful in the diagnosis of complex regionalpain syndrome type I (formerly reflex sympathetic dystrophy)rdquoClinical Journal of Pain vol 13 no 1 pp 50ndash59 1997
[21] G Wasner J Schattschneider and R Baron ldquoSkin temperatureside differencesmdasha diagnostic tool for CRPSrdquo Pain vol 98 no1-2 pp 19ndash26 2002
[22] E J Park K R Han Y J Chae W H Jeong and C KimldquoEffectiveness of cold stress thermography in the diagnosis ofcomplex of regional pain syndrome type 1rdquoThe Korean Journalof Pain vol 19 pp 159ndash163 2006
[23] E Skorupska M Rychlik and W Pawelec ldquoSkeletal striatedmuscle examination instrument amp new method of myofascialpain diagnosis based on the use of the instrumentrdquo Patentapplication No P-403467 Silver Medal 14ndash16 November 2013Brussels Innova the International Exhibition of InnovationEntrepreneurship and New Technologies Bronze Medal at theConcours Lepine International Paris 3004-11052014 FranceGoldMedal at the Euroinvent EuropeanExhibition ofCreativityand Innovation 22-24052014 Iasi Romania Gold Medal withDistinction at the 29th Invention and New Product ExpositionINPEX 18ndash20062014 Pittsburgh Pa USA
[24] R G Schwartz R Elliott G S Goldberg et al ldquoThe AmericanAcademy of Thermology Guidelines for neuromusculoskeletalthermographyrdquoThermology International vol 16 pp 5ndash9 2006
[25] J Dommerholt and C Fernandez-de-las-Penas Trigger PointDry Needling An Evidence and Clinical-Based ApproachChurchill Livingstone Elsevier 2013
[26] C Z Hong Braddom Physical Medicine and Rehabilitationin Muscle Pain Syndrome Elsevier New York NY USA 4thedition 2011
[27] S Mense D G Simons and I J Russell Muscle PainUnderstanding Its Nature Diagnosis and Treatment LippincottWilliams ampWilkins 2001
[28] R Rolke ldquoPseudoradicular and radicular low-back painmdashadisease continuum Rather than different entities Reply to theletters by Leffler and Hansson and by Van Boxem et alrdquo Painvol 135 pp 311ndash316 2008
[29] J M Bland and D G Altman ldquoStatistical methods for assessingagreement between two methods of clinical measurementrdquoTheLancet vol 1 no 8476 pp 307ndash310 1986
[30] D G Altman ldquoSome common problems in medical researchrdquoin Practical Statistics for Medical Research Chapman amp HallCRC Press London UK 1997
BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
10 BioMed Research International
References
[1] R SWeiner PainManagement A Practical Guide for CliniciansCRC Press LLC 6th edition 2002
[2] S A Skootsky B Jaeger and R K Oye ldquoPrevalence ofmyofascial pain in general internal medicine practicerdquoWesternJournal of Medicine vol 151 no 2 pp 157ndash160 1989
[3] Q Chen S Bensamoun J R Basford J M Thompsonand K-N An ldquoIdentification and quantification of myofascialtaut bands with magnetic resonance elastographyrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1658ndash1661 2007
[4] S Sikdar J P Shah T Gebreab et al ldquoNovel applications ofultrasound technology to visualize and characterize myofascialtrigger points and surrounding soft tissuerdquo Archives of PhysicalMedicine and Rehabilitation vol 90 no 11 pp 1829ndash1838 2009
[5] J G Travell andD G SimonsMyofascial Pain andDysfunctionThe Trigger PointManual vol 1WilliamsampWilkins BaltimoreMd USA 2nd edition 1999
[6] J G Travell andD G SimonsMyofascial Pain andDysfunctionTheTrigger PointManual vol 2 LippincottWilliamsampWilkinsBaltimore Md USA 1993
[7] H-Y Ge C Fernandez-de-las-Penas and L Arendt-NielsenldquoSympathetic facilitation of hyperalgesia evoked from myofas-cial tender and trigger points in patients with unilateral shoul-der painrdquoClinical Neurophysiology vol 117 no 7 pp 1545ndash15502006
[8] Y Kimura H-Y Ge Y Zhang M Kimura H Sumikura andL Arendt-Nielsen ldquoEvaluation of sympathetic vasoconstrictorresponse following nociceptive stimulation of latent myofascialtrigger points in humansrdquo Acta Physiologica vol 196 no 4 pp411ndash417 2009
[9] Y Zhang H-Y Ge S-W Yue Y Kimura and L Arendt-Nielsen ldquoAttenuated Skin blood flow response to nociceptivestimulation of latent myofascial trigger pointrdquo Archives ofPhysical Medicine and Rehabilitation vol 90 no 2 pp 325ndash3322009
[10] E Skorupska M Rychlik W Pawelec and W Samborski ldquoDryneedling related short-term vasodilation in chronic sciaticaunder infrared thermovisionrdquo Evidence-Based Complementaryand Alternative Medicine vol 2015 Article ID 214374 10 pages2015
[11] E SkorupskaM Rychlik andW Samborski ldquoIntensive vasodi-latation in the sciatic pain area after dry needlingrdquo BMCComplementary and Alternative Medicine vol 15 article 722015
[12] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoTrigger point-related sympathetic nerve activity inchronic sciatic leg pain a case studyrdquo Acupuncture in Medicinevol 32 no 5 pp 418ndash422 2014
[13] E Skorupska M Rychlik W Pawelec A Bednarek and WSamborski ldquoIntensive short-term vasodilation effect in the painarea of sciatica patientsmdashcase studyrdquo BMC Research Notes vol7 no 1 article 620 2014
[14] G Affaitati A Fabrizio A Savini et al ldquoA randomizedcontrolled study comparing a lidocaine patch a placebo patchand anesthetic injection for treatment of trigger points inpatients with myofascial pain syndrome evaluation of pain andsomatic pain thresholdsrdquoClinicalTherapeutics vol 31 no 4 pp705ndash720 2009
[15] D G Simons ldquoReview of enigmatic MTrPs as a common causeof enigmatic musculoskeletal pain and dysfunctionrdquo Journal
of Electromyography and Kinesiology vol 14 no 1 pp 95ndash1072004
[16] F S Nahm ldquoInfrared thermography in pain medicinerdquo KoreanJournal of Pain vol 26 no 3 pp 219ndash222 2013
[17] A C S Costa A V D Filho A C Packer and D Rodrigues-Bigaton ldquoIntra and inter-rater reliability of infrared image anal-ysis of masticatory and upper trapezius muscles in women withand without temporomandibular disorderrdquo Brazilian Journal ofPhysical Therapy vol 17 no 1 pp 24ndash31 2013
[18] M McCoy I Campbell P Stone C Fedorchuk S Wijayawar-dana and K Easley ldquoIntra-examiner and inter-examiner repro-ducibility of paraspinal thermographyrdquo PLoS ONE vol 6 no 2Article ID e16535 2011
[19] D S Haddad M L Brioschi and E S Arita ldquoThermographicand clinical correlation of myofascial trigger points in themasticatory musclesrdquo Dentomaxillofacial Radiology vol 41 no8 pp 621ndash629 2012
[20] S J Gulevich T D Conwell J Lane et al ldquoStress infraredtelethermography is useful in the diagnosis of complex regionalpain syndrome type I (formerly reflex sympathetic dystrophy)rdquoClinical Journal of Pain vol 13 no 1 pp 50ndash59 1997
[21] G Wasner J Schattschneider and R Baron ldquoSkin temperatureside differencesmdasha diagnostic tool for CRPSrdquo Pain vol 98 no1-2 pp 19ndash26 2002
[22] E J Park K R Han Y J Chae W H Jeong and C KimldquoEffectiveness of cold stress thermography in the diagnosis ofcomplex of regional pain syndrome type 1rdquoThe Korean Journalof Pain vol 19 pp 159ndash163 2006
[23] E Skorupska M Rychlik and W Pawelec ldquoSkeletal striatedmuscle examination instrument amp new method of myofascialpain diagnosis based on the use of the instrumentrdquo Patentapplication No P-403467 Silver Medal 14ndash16 November 2013Brussels Innova the International Exhibition of InnovationEntrepreneurship and New Technologies Bronze Medal at theConcours Lepine International Paris 3004-11052014 FranceGoldMedal at the Euroinvent EuropeanExhibition ofCreativityand Innovation 22-24052014 Iasi Romania Gold Medal withDistinction at the 29th Invention and New Product ExpositionINPEX 18ndash20062014 Pittsburgh Pa USA
[24] R G Schwartz R Elliott G S Goldberg et al ldquoThe AmericanAcademy of Thermology Guidelines for neuromusculoskeletalthermographyrdquoThermology International vol 16 pp 5ndash9 2006
[25] J Dommerholt and C Fernandez-de-las-Penas Trigger PointDry Needling An Evidence and Clinical-Based ApproachChurchill Livingstone Elsevier 2013
[26] C Z Hong Braddom Physical Medicine and Rehabilitationin Muscle Pain Syndrome Elsevier New York NY USA 4thedition 2011
[27] S Mense D G Simons and I J Russell Muscle PainUnderstanding Its Nature Diagnosis and Treatment LippincottWilliams ampWilkins 2001
[28] R Rolke ldquoPseudoradicular and radicular low-back painmdashadisease continuum Rather than different entities Reply to theletters by Leffler and Hansson and by Van Boxem et alrdquo Painvol 135 pp 311ndash316 2008
[29] J M Bland and D G Altman ldquoStatistical methods for assessingagreement between two methods of clinical measurementrdquoTheLancet vol 1 no 8476 pp 307ndash310 1986
[30] D G Altman ldquoSome common problems in medical researchrdquoin Practical Statistics for Medical Research Chapman amp HallCRC Press London UK 1997
BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 11
[31] D Coggon Probability Statistics in Clinical Practice BMJPublishing Group London UK 1995
[32] L Portney and C Watkins Foundations of Clinical ResearchApplications to Practice Prentice-Hall Upper Saddle River NJUSA 2nd edition 2000
[33] J Carletta ldquoAssessing agreement on classification tasks thekappa statisticrdquo Computational Linguistics vol 22 no 2 pp249ndash254 1996
[34] N Zaproudina V Varmavuo O Airaksinen and M NarhildquoReproducibility of infrared thermography measurements inhealthy individualsrdquo Physiological Measurement vol 29 no 4pp 515ndash524 2008
[35] M Sandberg T Lundeberg L G Lindberg and B GerdleldquoEffects of acupuncture on skin and muscle blood flow inhealthy subjectsrdquo European Journal of Applied Physiology vol90 no 1-2 pp 114ndash119 2003
[36] H Shinbara M Okubo K Kimura K Mizunuma andE Sumiya ldquoParticipation of calcitonin gene related peptidereleased via axon reflex in the local increase in muscle bloodflow following manual acupuncturerdquo Acupuncture in Medicinevol 31 no 1 pp 81ndash87 2013
[37] J Dommerholt ldquoDry needlingmdashperipheral and central consid-erationsrdquo Journal of Manual and Manipulative Therapy vol 19no 4 pp 223ndash237 2011
[38] C Myburgh A H Larsen and J Hartvigsen ldquoA systematiccritical review of manual palpation for identifying myofascialtrigger points evidence and clinical significancerdquo Archives ofPhysical Medicine and Rehabilitation vol 89 no 6 pp 1169ndash1176 2008
[39] E A Tough A R White S Richards and J CampbellldquoVariability of criteria used to diagnose myofascial trigger pointpain syndrome-evidence from a review of the literaturerdquo TheClinical Journal of Pain vol 23 no 3 pp 278ndash286 2007
[40] M L Brioschi L T Yeng E M H Pastor D Colman and FMR Moraes Silva ldquoDocumentation of myofascial pain syndromewith infrared imaginrdquo Revista Acta Fisiatrica vol 14 no 1 pp41ndash48 2007
[41] B Swerdlow and J N I Dieter ldquoAn evaluation of the sensitivityand specificity of medical thermography for the documentationof myofascial trigger pointsrdquo Pain vol 48 no 2 pp 205ndash2131992
[42] M Radhakrishna and R Burnham ldquoInfrared skin temperaturemeasurement cannot be used to detectmyofascial tender spotsrdquoArchives of Physical Medicine and Rehabilitation vol 82 no 7pp 902ndash905 2001
[43] A V Dibai-Filho and R R Guirro ldquoEvaluation of myofascialtrigger points using infrared thermography a critical reviewof the literaturerdquo Journal of Manipulative and PhysiologicalTherapeutics vol 38 no 1 pp 86ndash92 2015
[44] M L Brioschi D Colman and A Kosikov ldquoTerapia de pontos-gatilhos guiada por termografia infravermelhardquo Revista daSociedade Brasileira Para Estudo da Dor vol 5 no 3 p 9 2004
[45] R A Kruse Jr and J A Christiansen ldquoThermographic imagingof myofascial trigger points a follow-up studyrdquo Archives ofPhysical Medicine and Rehabilitation vol 73 no 9 pp 819ndash8231992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom


















