
CLINICAL SITE INFORMATION FORM - University of...
21
·t I: Inti ormatio CLINICAL SITE INFORMATION FORM Irmation For tile Academic PrOflTllm Initial Date 03-13-06 Revision Date 1-30-07 Angie Norman, PT rson Angie [email protected] Name of Clinical Center Valley Medical Center 400 South 43rd Street Renton State I WA I Zip 98058 (425) 228-3450 Ext. (425) 251-5165 Ext. (425) 656-4028 -mail Clinical Center Web www.Valleymed.org Director of Physical Melinda Glass, Director of Rehabilitation Services Director of Physical Therapy E-mail Melinda [email protected] al Angie Norman, PT Person CCCE / Contact Person Phone (425) 251-5165 ail Angie [email protected] Angie Norman, PT (List name and credentials) Other Credentialed Cis (List name and credentials) Indicate which of the following are X Proof of student health clearance the X Current (2 years) Washington State Criminal background check o Child clearance o Drug screening X First Aid and CPR o HIP AA education o OSHA education X Other: Please list Bloodborne Pathogen Training TB test Proof of immunization ID badge with first and last name and school 4
-
Upload
nguyenhuong -
Category
Documents
-
view
215 -
download
0
Transcript of CLINICAL SITE INFORMATION FORM - University of...

·t I: Intiormatio
CLINICAL SITE INFORMATION FORM
Irmation For tile Academic PrOflTllmInitial Date 03-13-06
11 About the Clinical Site - PrimaryRevision Date 1-30-07
Person Completing CSIF
Angie Norman, PT
E-mai I address of person
Angie [email protected] CSIF Name of Clinical Center
Valley Medical Center
Street Address
400 South 43rd Street
City
RentonState I WAI Zip
98058
Facility Phone
(425) 228-3450Ext.
PT Department Phone
(425) 251-5165Ext.
PT Department Fax
(425) 656-4028
PT Department E-mail Clinical Center Web
www.Valleymed.orgAddress Director of Physical
Melinda Glass, Director of Rehabilitation ServicesTherapy Director of Physical Therapy E-mail
Melinda [email protected]
Center Coordinator of Clinical
Angie Norman, PTEducation (CCCE) / Contact Person CCCE / Contact Person Phone
(425) 251-5165
CCCE / Contact Person E-mail
Angie [email protected]
APT A Credentialed Clinical
Angie Norman, PTInstructors (CI) (List name and credentials)
Other Credentialed Cis(List name and credentials)Indicate which of the following are
XProof of student health clearance
required by your facility prior to the
XCurrent (2 years) Washington State Criminal background checkclinical education experience:
o Child clearance
o Drug screeningX
First Aid and CPR
o HIPAA educationo OSHA educationXOther: Please list Bloodborne Pathogen Training
TB testProof of immunizationID badge with first and last name and school
4
Valley Medical Center will require a Student Program Checklist to besigned by the ACCE and returned to Valley Medical Center prior toinitiation of the internship. The Checklist attests that the educationalprogram has the above information on file. It will be provided byValley Medical Center to the ACCE in a timely manner. ValleyMedical Center will not require copies of individual certifications.
5
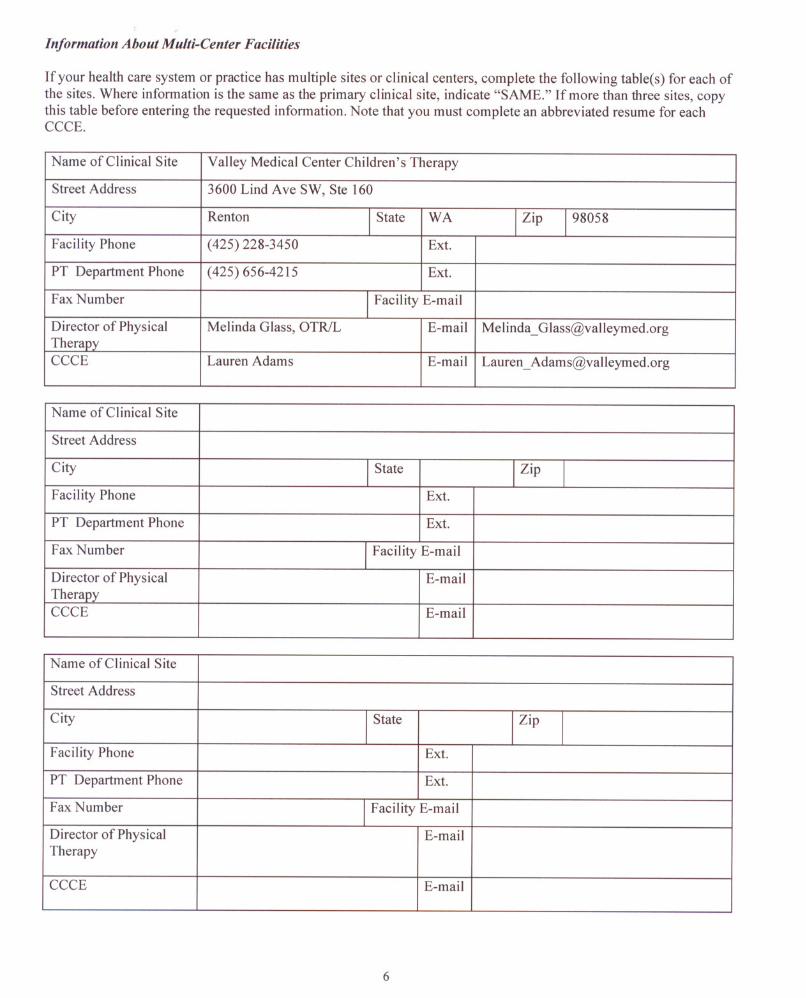
Information About Multi-Center Facilities
If your health care system or practice has multiple sites or clinical centers, complete the following table(s) for each ofthe sites. Where information is the same as the primary clinical site, indicate "SAME." Ifmore than three sites, copythis table before entering the requested information. Note that you must complete an abbreviated resume for eachCCCE.
Name of Clinical Site Valley Medical Center Children's Therapy
Street Address
3600 Lind Ave SW, Ste 160
City
RentonI State
WAI Zip198058
Facility Phone
(425) 228-3450Ext.
PT Department Phone
(425) 656-4215Ext.
Fax NumberI Facility E-mail
Director of Physical
Melinda Glass, OTRILE-mailMelinda_ [email protected] CCCE
Lauren AdamsE-mailLauren [email protected]
Name of Clinical Site
Street AddressCityI StateI ZipI
Facility Phone
Ext.
PT Department Phone
Ext.
Fax NumberI Facility E-mail
Director of Physical
E-mailTherapy CCCE
Name of Clinical Site
Street AddressCityI StateI ZipI
Facility Phone
Ext.
PT Department Phone
Ext.
Fax NumberI Facility E-mail
Director of Physical
E-mailTherapy
CCCE
6
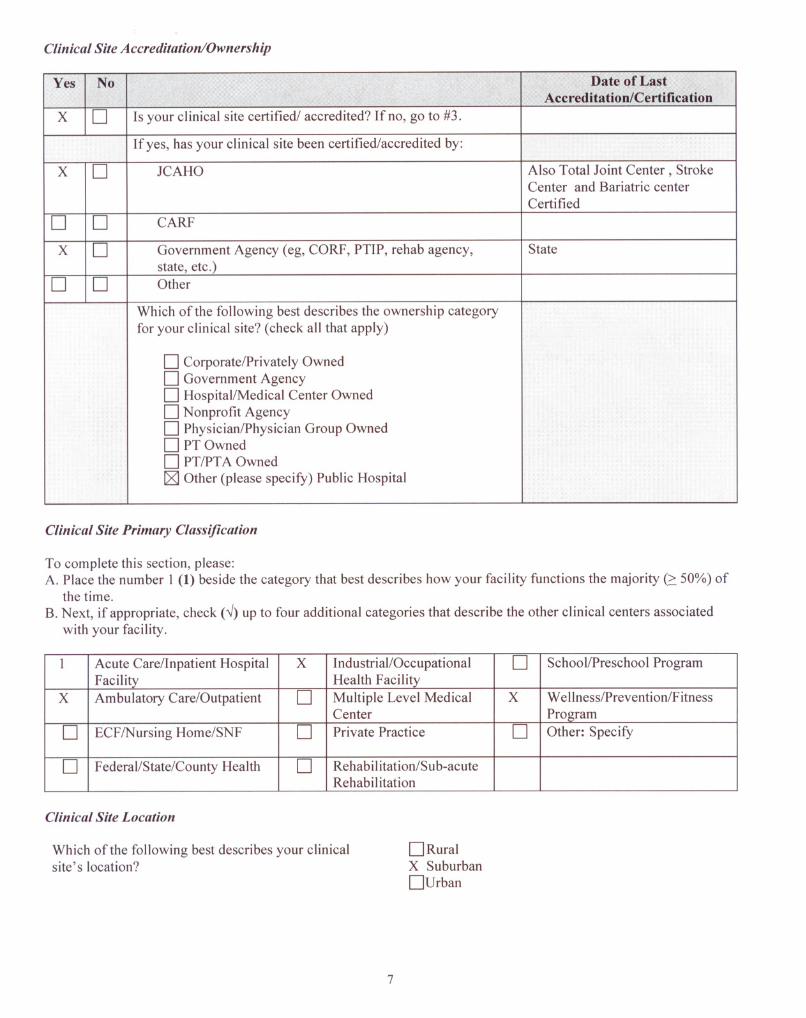
Clinical Site Accreditation/Ownership
Yes No Date of LastAccred itatio n/Certifica tio nX
DIs your clinical site certified/ accredited? If no, go to #3.
If yes, has your clinical site been certified/accredited by:X
D JCAHO Also Total Joint Center, StrokeCenter and Bariatric centerCertifiedD
D CARF
X
D Government Agency (eg, CORP, PTIP, rehab agency,State
state, etc.) DD Other
Which of the following best describes the ownership categoryfor your clinical site? (check all that apply)
D Corporate/Privately OwnedD Government AgencyD Hospital/Medical Center OwnedDNonprofit AgencyD Physician/Physician Group OwnedD PT OwnedD PT/PTA OwnedI:8J Other (please specify) Public Hospital
Clinical Site Primary Classification
To complete this section, please:A. Place the number 1 (1) beside the category that best describes how your facility functions the majority (:::50%) of
the time.B. Next, if appropriate, check (.J) up to four additional categories that describe the other clinical centers associated
with your facility.
I Acute Care/Inpatient HospitalXIndustrial/Occupational DSchool/Preschool ProgramFacility
Health FacilityX
Ambulatory Care/Outpatient DMultiple Level Medical XWe Ilness/Prevention/F itnessCenter
Program
DECF/Nursing Home/SNF DPrivate Practice DOther: Specify
DFederal/State/County Health DRehabi Iitation/S ub-acute
Rehabilitation
Clinical Site Location
Which of the following best describes your clinicalsite's location?
7
DRuralX Suburban
Durban

Information About the Clinical Teaching Faculty
ABBREVIATED RESUME FOR CENTER COORDINATORS OF CLINICAL EDUCATIONPlease uvdate as each new CCCE assumes this vasil·
NAME: Angie Norman Length of time as the CCCE: 3 years
DA TE: (mm/dd/yy) 06/1 1/08
Length of time as a CI: 13 years
PRESENT POSITION: PT III
Mark (X) all thatLength ofValley Medical Center
apply:time inXPT
clinicalDPTA
practice: 14D Other, specify
Y2 years
LICENSURE: (State/Numbers)
APT A Credentialed CIOther CI CredentialingWA, PTOO06459
Yes XNo D YesDNo X
Eligible for Licensure:
Yes XNoD
I Certified Clinical Specialist:YesDNoxD
Area of Clinical Specialization: Other credentials:
SUMMARY OF COLLEGE AND UNIVERSITY EDUCATION (Start with most current):
INSTITUTION
PERIOD OFMAJORDEGREESTUDY FROM
TO
Eastern Washington University
19921994Physical TherapyBS
University of Washington
19851990Zoology BS
SUMMARY OF PRIMARY EMPLOYMENT (For current and previous four positions since graduation fromcollege; start with most current):
EMPLOYER POSITIONPERIOD OFEMPLOYMENTFROM
TO
Valley Medical Center
PT III2003Present
Canterbury House (SNF)
PT20012003
Highline Community Hospital Specialty Center (acute care,
PT19972001TCU, acute rehab and sub acute brain injury rehabilitation) Providence St. Peter Hospital (acute care, inpatient rehab,
PT19941997home health)
8
CONTINUING PROFESSIONAL PREPARATION RELATED DIRECTLY TO CLINICAL TEACHINGRESPONSIBILITIES (for example, academic for credit courses [dates and titles], continuing education [courses andinstructors], research, clinical practice/expertise, etc. in the last three (3) years):
Course Provider/LocationDate
Contact CCCE directly for this list if desired
9

CLINICAL INSTRUCTOR INFORMATION
Provide the following infonnation on all PTs or PT As employed at your clinical site who are CIs. For clinical sites with multiple locations, use one formfor each location and identify the location here.
Name followed by credentials
PT/PT A ProgramYear ofHighestNo. ofNo. of YearsList Certifications L= Licensed, Number
(eg, Joe Therapist, OPT, OCS
from Which CIGraduationEarnedYears ofof ClinicalKEY: E= EligibleJane Assistant, PT A, BS)
GraduatedPhysicalClinicalTeachingA = APT A credentialed. CIAPTAT= Temporary
Therapy
Practice B = Other CI credentialingMember
Degree
C = Cert. clinical specialistYes/N 0L/EITState of
List others
NumberLicensure
Barbara Areggar, PT
Washington]99]MSPT17]5Outpatient Ortho LWA
University
Inpatient SupervisorPTOOOO5552Julie Fulton, PT
University of200]MPT76 Lymphedema YesLWA
Puget Sound
Outpatient NeuroPTOOOO8576Melissa Reed
University of]978PT3027Lymphedema LWA
Washington
Hand TherapyPTOOOO2262Robert Sancilio
D'Youville]995MSPT13]2Outpatient OrthoYesLWA
College
Back RehabPTOOOO
6721Susan GillCheepmanPT]989]9]0Outpatient OrthoYesLWA
University
PTOOOO
5609Angie Norman
EasternPT19941413Inpatient Acute CareYesLWA
Washington
PTOOOO
University
6459
Vicky Lerner
DukePT199414]2Vestibular RehabYesLWAWIC fitting
PTOOOOOutpatient Neuro 7254
Marianne WickUniversity ofPT1976]915Outpatient Neuro LWA
Washington
PTOOOO
2039John KincaidUniversity ofPT]992]6? Occupational HealthYesLWA
Washington
ServicesPTOOOO
5783
10

Jon Takagi University ofMSPT200082 Inpatient Acute Care LWAWashington
PTOOOO8384Tera Martin
University ofMSPT200264 Outpatient Ortho LWAWashington
PTOOOO7079Mai Haynes
WesternMSPT200087 Inpatient Acute Care LWAUniversity of
PTOOOOHealth Sciences
8260
Mathew HunkovicUniversity ofPT199414<1Oupatient Ortho LWA
Maryland -
OCS certifiedPT
Eastern Shore
LevellIl NAIOMT
Darlene Bumgarner
Green RiverPTA19891917Inpatient Acute Care N/A
Community CollegeClaude McCrimmonGreen RiverPTA1997119 Outpatient N/A
Community CollegeTanya Baldwin
Green RiverPTA1998104 Outpatient N/A
Community CollegeTamara PetersGreen RiverPTA199710lh5 Outpatient N/A
Community CollegeTanya Van Winkle
Green RiverPTA20061 1/2< 1Inpatient Acute CareNoN/A
Community College
11

Clinical Instructors
What criteria do you use to select clinical instructors? (Mark (X) all that apply):
X APT A Clinical Instructor CredentialingDNo criteriaX
Career ladder opportunity DOther (not APT A) clinical instructor credentialingX
Certification/training course XTherapist initiative/volunteerX
Clinical competence XYears of experience: Number: > 1
DDelegated in job description DOther (please specify):
XDemonstrated strength in clinical
teaching
How are clinical instructors trained? (Mark (X) all that apply)
X 1:1 individual training (CCCE:CI)DContinuing education by consortia
Academic for-credit coursework
DNo training
X
APT A Clinical Instructor Education andDOther (not APTA) clinical instructor credentialingCredentialing Program - voluntary
programX
Clinical center inservices XProfessional continuing education (eg, chapter,CEU course)D
Continuing education by academicDOther (please specify):program
Information About the Physical Therapy Service
Number of Inpatient Beds
For clinical sites with inpatient care, please provide the number of beds available in each of the subcategories listed, --- -- ----r -- --- ----. - -- ---- ------ ------/
Acute care 328Psychiatric center 0
Intensive care
16Rehabilitation center 0
Step down
4-6Other specialty centers: Specify 0
Subacute/transitional care unit
0
Extended care
0Total Number of Beds 348
Number of Patients/Clients
.INPATIENT OUTPATIENT
10-12
Individual PT Individual PT(depends upon area of
8-10
Student PT - at end of internship Student PTservice and individual
I 0-14
Individual PTA Individual PTAtherapist's schedule. Will10-12
Student PTA - at end of internship Student PTAfloat up to inpatient pm.)PT/PTA Team
PT/PTA Team
100-120Total patient/client visits per day Total patient/client visits per day
E . h ber of oatient/cl· d
12

Patient/Client Lifespan and Continuum of Care
Indicate the frequency of time typically spent with patients/clients in each of the categories using the key below:1=(0%) 2=(1-25%) 3=(26-50%) 4=(51-75%) 5=(76-100%)
Rating Patient Lifespan RatingContinuum of Care
1
0-12 years (this population covered by3Critical care, ICU, acuteChildren's Therapy and NICU staff 2
13-21 years SNF /ECF /sub-acute
422-65 years Rehabilitation
5Over 65 years 3Am bulatory /outpatient
Home health/hosoiceWellness/fitness/industry
Patient/Client Diagnoses1. Indicate the frequency of time typically spent with patients/clients in the primary diagnostic groups (bolded) using
the key below:1=(0%) 2=(1-25%) 3=(26-50%) 4=(51-75%) 5=(76-100%)
2. Check (--1) those patient/client diagnostic sub-categories available to the student.
(1-5) Musculoskeletal
4
Acute injury 3Muscle disease/dysfunction2
Amputation 3Musculoskeletal degenerative disease3
Arthritis 4Orthopedic surgery2
Bone disease/dysfunction 0Other: (SpecifY)2
Connective tissue disease/dysfunction(1-5)
Neuro-muscular
2
Brain injury 2Peripheral nerve iniury4
Cerebral vascular accident 2Spinal cord iniury2
Chronic pain 3Vestibular disorderI
Congen italldevelopmental Other: (Specify)2
Neuromuscular degenerative disease(1-5)
Cardiovascular-pulmonary
4
Cardiac dysfunction/disease 4Peripheral vascular dysfunction/disease1
Fitness 0Other: (Specify)3
Lymphedema4
Pulmonary dysfunction/disease(1-5)
Integumentary
IBurns 0Other: (Specify)
2Open wounds
IScar formation
(1-5)
Other (May cross a number of diagnostic groups)
4
Cognitive impairment 2Organ transolant - as a comorbidity only4
General medical conditions 2Well ness/Prevention4
General surgery 0Other: (Soecifv)3
Oncologic conditions
13
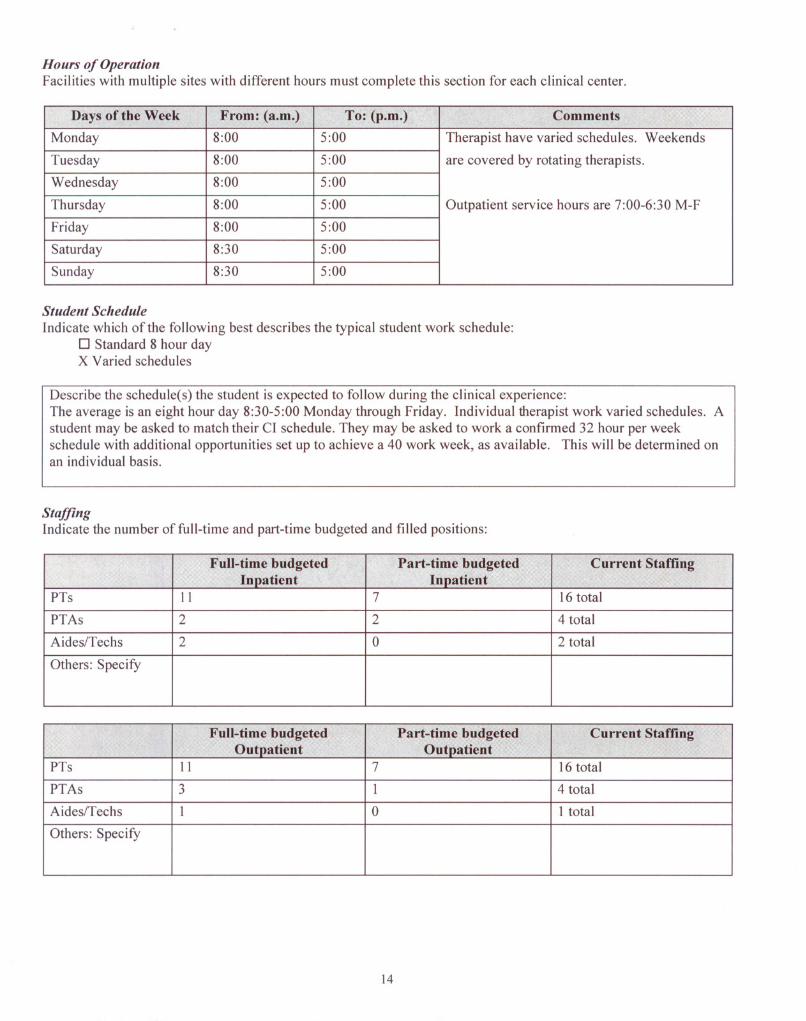
Hours of OperatiollFacilities with multiple sites with different hours must complete this section for each clinical center.
Days of the Week From: (a.m.)To: (p.m.) Comments
Monday
8:005:00Therapist have varied schedules. Weekends
Tuesday
8:005:00are covered by rotating therapists.
Wednesday
8:005:00
Thursday
8:005:00Outpatient service hours are 7:00-6:30 M-F
Friday
8:005:00
Saturday
8:305:00
Sunday
8:305:00
Studellt Schedule
Indicate which of the following best describes the typical student work schedule:o Standard 8 hour dayX Varied schedules
Describe the schedule(s) the student is expected to follow during the clinical experience:The average is an eight hour day 8:30-5:00 Monday through Friday. Individual therapist work varied schedules. Astudent may be asked to match their CI schedule. They may be asked to work a confirmed 32 hour per week
schedule with additional opportunities set up to achieve a 40 work week, as available. This will be determined onan individual basis.
StaffillgIndicate the number of full-time and part-time budgeted and filled positions:
Full-time budgetedPart-time budgetedCurrent StaffingInpatient
InpatientPTs
II 716 total
PTAs
2 24 total
Aides/Techs
2 02 total
Others: Specify
Full-time budgetedPart-time budgetedCurrent StaffingOutpatient
OutpatientPTs
II 716 total
PTAs
3 14 total
Aides/Techs
1 0I total
Others: Specify
14

Information About the Clinical Education Experience
Special Programs/Activities/Learning Opportunities
Please mark (X) all special programs/activities/learning opportunities available to students.
0 Administration XIndustrial/ergonomic PT 0Qual ityAssurance/CQ I/TQ MX
Aquatic therapy XInservice training/lectures 0Radiology0 Athletic venue coverage XNeonatal (very limited) access 0Research experience0Back school 0Nursing home/ECF/SNF 0Screening/prevention0Biomechanics lab 0Orthotic/Prosthetic fabrication XSports physical therapy
0Cardiac rehabilitation 0Pain management program XSurgery (observation)
0 Com munityIre-entry XPediatric-general: at Children's XTeam meetings/roundsactivities
Therapy only (outpatient)X
Critical care/intensive care0Classroom consultation XVestibular rehab
0 Departmental administration0Developmental program XWomen's Health/OB-GYN
0 Early intervention 0Cognitive impairment XWork
Hardening/conditioning0 Employee intervention XMusculoskeletal XWound care
0 Employee wellness programXNeurological XOther (specify below)Lymphedema/hand clinicX
Group programs/classes XPrevention/wellness
0Home health program 0Pulmonary rehabilitation
Specialty Clinics
Please mark (X) all specialty clinics available as student learning experiences.
0 Arthritis 0Orthopedic clinic 0Screening clinics0Balance 0Pain clinic 0Developmental0 Feeding clinic 0Prosthetic/orthotic clinic 0Scoliosis
X
Hand clinic XSeating/mobility clinic (limited)0Preparticipation sports0 Hemophilia clinic 0Sports medicine clinic 0Wellness
0 Industry 0Women's health 0Other (specify below)
0Neurology clinic
15

Health and Educational Providers at the Clinical Site
Please mark (X) all health care and educational providers at your clinical site students typically observe and/or withwhom they interact.
X Administrators 0Massage therapists XSpeech/languagepathologists0 Alternative therapies: XNurses XSocial workers
List: 0 Athletic trainers XOccupational therapists 0Special education teachers
0Audiologists XPhysicians (list specialties) XStudents from other
disciplinesXDietitians XPhysician assistants XStudents from other physical
therapv education programsX
Enterostomal /wound XPodiatrists 0Therapeutic recreationspecial ists
therapists
0 Exercise physiologistsXProsthetists /orthotists 0Vocational rehabilitationcounselorsX
Fitness professionals XPsychologists 0Others (specify below)
0Health information XRespiratory therapists
technologists
Affiliated PT and PT A Educational ProgramsList all PT and PTA education programs with which you currently affiliate.
Program Name City and StatePTPTA
University of Washington
Seattle, WAX0University of Puget Sound
Tacoma, WAX0Eastern Washington University
Cheney, WAX0Green River Community College
Auburn, WA0X
University of Montana
MOX
University of the Pacific
CAX0Western University of Health Sciences
CAX
Texas Women's University
TXX0University of Idaho
IDX00
00
00
00
00
00
00
00
0
16
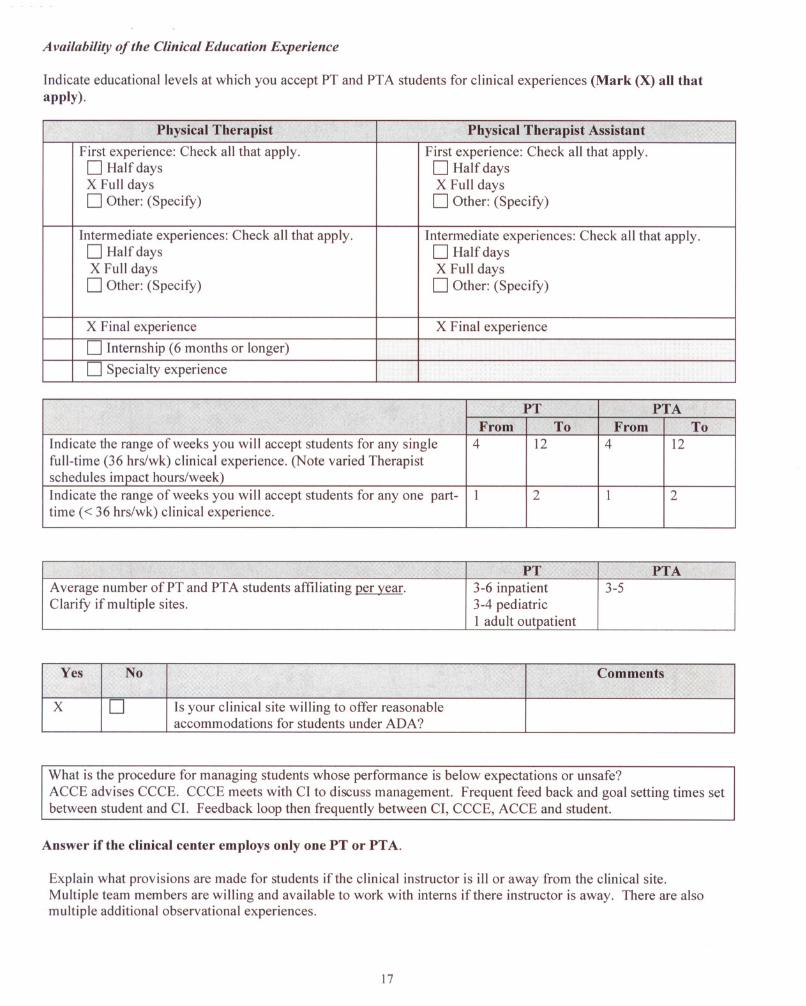
A vailability of the Clinical Education Experience
Indicate educational levels at which you accept PT and PTA students for clinical experiences (Mark (X) all thatapply).
Physical Therapist Physical Therapist Assistant
First experience: Check all that apply.
First experience: Check all that apply.D Halfdays
D Half daysX Full days
X Full daysD Other: (Specify)
D Other: (Specify)
Intermediate experiences: Check all that apply.
Intermediate experiences: Check all that apply.D Half days
D Half daysX Full days
X Full daysD Other: (Specify)
D Other: (Specify)
X Final experience
X Final experience
D Internship (6 months or longer) D Specialty experience
PTPTAFrom
ToFromTo
Indicate the range of weeks you will accept students for any single
412412
full-time (36 hrslwk) clinical experience. (Note varied Therapist schedules impact hours/week)Indicate the range of weeks you will accept students for anyone part-
12 12
time « 36 hrs/wk) clinical experience.
PTPTA
A verage number of PT and PT A students affiliating per year.3-6 inpatient3-5
Clarify if multiple sites.3-4 pediatric
I adult outpatient
Yes No Comments
X
DIs your clinical site willing to offer reasonableaccommodations for students under ADA?
What is the procedure for managing students whose performance is below expectations or unsafe?ACCE advises CCCE. CCCE meets with CI to discuss management. Frequent feed back and goal setting times setbetween student and CI. Feedback loop then frequently between CI, CCCE, ACCE and student.
Answer if the clinical center employs only one PT or PT A.
Explain what provisions are made for students if the clinical instructor is ill or away from the clinical site.Multiple team members are willing and available to work with interns if there instructor is away. There are alsomultiple additional observational experiences.
17

Clinical Site's Learning Objectives and Assessment
Yes No
XDI. Does your clinical site provide written clinical education objectives to students?
Ifno, go to # 3.2. Do these objectives accommodate:
XD •The student's objectives?
XD •Students prepared at different levels within the academic curriculum?
XD •The academic program's objectives for specific learning experiences?
XD •Students with disabilities? (on an as needed basis)
XD3. Are all professional staff members who provide physical therapy services acquainted with the
clinical site's learning objectives?
When do the CCCE and/or CI typically discuss the clinical site's learning objectives with students? (Mark (X) allthat apply)
X Beginning of the clinical experience XAt mid-clinical experience
DDaily XAt end of clinical experience
X
Weekly XOther PRN
Indicate which of the following methods are typically utilized to inform students about their clinical performance?(Mark (X) all that apply)
X Written and oral mid-evaluation XOngoing feedback throughout the clinical
X
Written and oral summative final evaluationXAs per student request in addition to formaland ongoing written & oral feedbackX
Student self-assessment throughout the clinicalXWeekly written goals and feedback, prn only
OPTIONAL: Please feel free to use the space provided below to share additional information about your clinicalsite (eg, strengths, special learning opportunities, clinical supervision, organizational structure, clinicalphilosophies of treatment, pacing expectations ofstudents [early, final]).
Surgery observation available (for total hip or knee only)Participation in community events available throughout the year. (bike helmet fittings, backpackawareness, Senior Fair, Career Fair, Bring Your Kids to Work Day, etc ... )Exposure to Team RoundsAquatic Therapy
18

1<

Part II. Information for Students
Use the check (~) boxes provided for Yes/No responses. For all other responses or to provide additional detail,please use the Comment box.
Arranging the Experience
Yes No Comments
X
DI. Do students need to contact the clinical site for specific workRecommended two weekshours related to the clinical experience?
prior to internshipX
D2. Do students receive the same official holidays as staff?
DX3. Does your clinical site require a student interview?
4. Indicate the time the student should report to the clinical site on
To be determined on anthe first day of the experience.
individual basisX
D5. Is a Mantoux TB test (PPO) required?a)one step (1/ check)
b)two step__ X__ c..J check)
If yes, within what time frame?XD6.Is a Rubella Titer Test or immunization required?
X
7.Are any other health tests/immunizations required prior to the Measles, Mumps,clinical experience?
Td, Tetanus, Oiptheria,If yes, please specify:
Hep B8.
How is this information communicated to the clinic? Provide Student Program Checklistfax number if required.
provided by VMC needs to besigned by ACCE. Individualcertifications not required.9.
How current are student physical exam records required to currentbe?
DX10. Are any other health tests or immunizations required on-site?
If yes, please specify:X
II. Is the student required to provide proof of OSHA training?Bloodborne pathogens
DX12. Is the student required to provide proof of HIPAA training?Provided on site
DX13. Is the student required to provide proof of any other training
prior to orientation at your facility?If yes, please list.X
D14. Is the student required to attest to an understanding of thebenefits and risks of Hepatitis-B immunization?X
D15. Is the student required to have proof of health insurance?
X
D16. Is emergency health care available for students?
X
D a) Is the student responsible for emergency health care costs?
X
D17. Is other non-emergency medical care available to students?
X
D18. Is the student required to be CPR certified?(Please note if a specific course is required).
20

Yes No Comments
D
X a) Can the student receive CPR certification while on-site?
DX19. Is the student required to be certified in First Aid?
D
X a) Can the student receive First Aid certification on-site?
X
D20. Is a criminal background check required (eg, Criminal Washington State - withinOffender Record Information)?
past two years prior toIf yes, please indicate which background check is required and
internshiptime frame. D
X21.Is a child abuse clearance required?
X
22.Is the student responsible for the cost or required clearances?
DX23. Is the student required to submit to a drug test?
If yes, please describe parameters.D
X24. Is medical testing available on-site for students? Only in instances of workrelated exposure25. Other requirements: (On-site orientation, sign an ethics
On site orientation with
statement, sign a confidentiality statement.)
Human Resources will occur
the first day of the internshipand will include privacystatements, etc ...
Housing
Yes No Comments
DX26. Is housing provided for male students? (If no, go to #32)
DX27. Is housing provided for female students? (If no, go to #32)
28. What is the average cost of housing?29. Description of the type of housing provided:
30. How far is the housing from the facility?
31. Person to contact to obtain/confirm housing:Name:Address:City:
State:
I Zip:Phone:
E-mail:
Yes
No Comments
21

32.If housing is not provided for either gender:
DX a) Is there a contact person for information on housing in
the area of the clinic?Please list contact person and phone #.D
X b) Is there a list available concerning housing in the area ofPlease reference Valley Medicalthe clinic? If yes, please attach to the end ofthis form.
Center Website for links
Transportation
Yes No Comments
X
D33. Will a student need a car to complete the clinical experience?Or public transportationX
D34. Is parking available at the clinical center? limited
a)
What is the cost for parking? free
X
D35. Is public transportation available?
36. How close is the nearest transportation (in miles) to your site?a) Train station?
5 miles
b)
Subway station? miles
c)
Bus station? ] block
d)Airport? miles
37. Briefly describe the area, population density, and any safetyissues regarding where the clinical center is located. No unusual safety issues
38. Please enclose a map of your facility, specifically the location
Map and parking directionsof the department and parking. Travel directions can be
will be mailed prior to eachobtained from several travel directories on the internet.
internship. Please reference(eg, Delorme, Microsoft, Yahoo, Mapquest).
Valley Medical Center websiteto access this information priorto internship confirmation.
Meals
Yes No Comments
X
39. Are meals available for students on-site? (If no, go to #40)Cafeteria available
Breakfast (if yes, indicate
$ 3-6approximate cost) Lunch (if yes, indicate
$ 5-7approximate cost) Dinner (if yes, indicate
$ 5-7approximate cost) X
D40. Are facilities available for the storage and preparation of food?Microwave and refrigerator
22

Stipend/Sell olars Itip
Yes No Comments
DX41. Is a stipend/salary provided for students? If no, go to #43.
a) How much is the stipend/salary? ($ / week)DX42. Is this stipend/salary in lieu of meals or housing?
43. What is the minimum length of time the student needs to be onthe clinical experience to be eligible for a stipend/salary?
Special Information
Yes No Comments
X
D44. Is there a facility/student dress code? Ifno, go to # 45. Lab jacket -loaners availableIf yes, please describe or attach.
Casual professional. Scruba)
Specify dress code for men: pants okay. No scrub tops.No skirts or shorts. Closed toeb)
Specify dress code for women: and heel on all shoes.
D
X45. Do you require a case study or inservice from all students Determined on an individual
(part-time and full-time)?
basis.
DX46. Do you require any additional written or verbal work from theWill support educational
student (eg, article critiques, journal review, patient/clientinstitution requirements.
education handout/brochure)?Additional assignments may
be given prn to facilitateprogression of internship.X47. Does your site have a written policy for missed days due toBased on circumstances and
illness, emergency situations, other? If yes, please summarize.educational institution policy.
X
D48. Will the student have access to the Internet at the clinical site?Very limited
Otlter Student Information
Yes No
X
D49. Do you provide the student with an on-site orientation to your clinical site?
(mark X
a) Please indicate the typical orientation content by marking an X by all items that are included.below) X
Documentation/billing XReview of goals/objectives of clinical experience
DFacility-wide or volunteer orientationXStudent expectations
XLearning style inventory XSupplemental readings
X
Patient information/assignments XTour of facility/department
X
Policies and procedures (specificallyXOther (specify below - eg, bloodborne pathogens,outlined plan for emergency responses)
hazardous materials, etc.) HIP AA, Healthstream (safetyX
Quality assurance and quality issues)
X
Reimbursement issues
X
Required assignments (eg, case study,diary/log, inservice)
23
In appreciation ...
Many thanks for your time and cooperation in completing the CSIF and continuing to serve the physical therapyprofession as clinical mentors and role models. Your contributions to learners' professional growth and developmentensure that patients/clients today and tomorrow receive high-quality patient/client care services.
24














