Clinical Review The mechanisms of action of vacuum assisted … · 2016-01-08 · healing defined...
12
Clinical Review The mechanisms of action of vacuum assisted closure: More to learn Dennis P. Orgill, MD, PhD,a Emest K. Manders, MD,b Bauer E. Sumpio, MD,CRaphael C. Lee, MD, PhD,d Christopher E. Attinger, MD,e Geoffrey C. Gurtner, MD,r and H. Paul Ehrlich, PhD,g Boston, MA, Pittsburg, PA, New Haven, CT, Chicago,IL, Washington, DC, Stanford, CA, and Hershey,PA Division of Plastic and &constructive Surgery, Brigham and Women's HosPital, a Boston, MA; Division of Plastic and &constructive Surgery, University of Pittsburg School of Medicine, bPittsburg, PA; Department of Surgery, Vale University School of Medicine, c New Haven, CT; Department of Surgery, University of Chicago Hospitals, d Chicago, IL; Limb Center, Georgetown University Medical Center, e Washington, DC; Department of Surgery, Stanford University Medical Center/ Stanford, CA; Division of Plastic Surgery, Department of Surgery, Penn State University Milton S. Hershey Medical Center,gHershey, PA THERE liAS BEEN RAPID ADOPTION OF VACUUM-ASSISTED CLOSURE (VAC) TECHNOLOGY to treat many acute and chronic wounds despite a rudimentary under- standing of the biologic mechanisms of action and few weIl-controIled, prospective, randomized c1ini- cal trials of its use. An expert panel carried out a selected review of published literature regarding the mechanisms of action of the VAC device in the context of published c1inical studies. The current literature suggests primary mecha- nisms of action of the VAC device may inc1ude the foIlowing: (I) drawing the wound edges together; (2) stabilization of the wound environment; (3) decrease in wound edema and rem oval of wound exudate; and (4) microdeformations of the wound surface. Secondary effects inc1ude increased angiogenesis, granulation tissue formation, and, in some cases, a decrease in bacterial bioburden. Supported by a grant from Kinetic Concepts, Inc. (KCI). This document reflects the opinion of the authors and was not influ- enced by KCI. Dr Orgill reports having received consulting fees and a research contract from Kinetic Concepts, Inc. (KCI) for studies per- formed at Brigham and Woman's Hospital; he is an expert witness for KCI and Wake Forest University. Dr Sumpio, Dr Attinger, and Dr Lee disclosed consulting fees from KCI, San Antonio, TX. Accepted for publication February 2, 2009. Reprint requests: Dennis P. Orgill, MD, PhD, Division of Plastic and Reconstructive Surgery, Brigham and Women's Hospital, 75 Francis Street, Boston, MA 02115. E-mail: [email protected]. Surgery 2009;146:40-51. 0039-6060/$ - see front matter @ 2009 Mosby, Inc. AlI rights reserved. doi: 10.1016/j.surg.2009.02.002 40 SURGERY INTRODUCTION The c1inical evidence for the efficacy of the VAC device is mostly in retrospective case series. A few randomized control studies have shown efficacy in diabetic foot infections, pressure ulcerations, and skin grafts. Additional research into the mecha- nism of action wiIl provide a better understanding of how to best use current devices and help make improvements in future device designo With our aging population and increases in obesity and diabetes, problem wounds are becom- ing an increasing burden to our healthcare system. In addition, c1inicians are faced with an array of problem wounds from military and domestic trauma as weIl as from complex surgical procedures. Better, cost-effective methods of c10sing difficult wounds efficiently wiIl reduce the pain and ampu- tation rates associated with wounds. Despite the theoretical promise of topicaIly applied growth factors, there is currently only a limited c1inical role with only 1 commercial product available for c1inical use in the United States.1 Other methods, such as bioengineered skin substitutes, have been successful in certain defined areas of wound heal- ing, but most advanced wound care products in use today are based on the principIe of moist wound healing defined by Winter and Scales in the 1960s.2,3 WOUND HEALING PHYSIOLOGY Acute wounds progress through a complex series of biochemical and ceIlular events described as the phases of wound healing: hemostasis, in- flammation, proliferation, and remodeling. Suc- cessful wound healing is contingent on the orchestration of a myriad of biochemical signal pathways from a wide range of ceIl types during the 82
Transcript of Clinical Review The mechanisms of action of vacuum assisted … · 2016-01-08 · healing defined...

Clinical Review
The mechanisms of action of vacuumassisted closure: More to learnDennis P. Orgill, MD, PhD,a Emest K. Manders, MD,b Bauer E. Sumpio, MD,CRaphael C. Lee, MD,PhD,d Christopher E. Attinger, MD,e Geoffrey C. Gurtner, MD,r and H. Paul Ehrlich, PhD,g Boston,MA, Pittsburg, PA, New Haven, CT, Chicago,IL, Washington, DC, Stanford, CA, and Hershey,PA
Division of Plastic and &constructive Surgery, Brigham and Women's HosPital, a Boston, MA; Division ofPlastic and &constructive Surgery, University of Pittsburg Schoolof Medicine, bPittsburg, PA; Department ofSurgery, Vale University School of Medicine, c New Haven, CT; Department of Surgery, University of ChicagoHospitals, d Chicago, IL; Limb Center, Georgetown University Medical Center, e Washington, DC; Departmentof Surgery, Stanford University Medical Center/ Stanford, CA; Division of Plastic Surgery, Department ofSurgery, Penn State University Milton S. Hershey Medical Center,gHershey, PA
THERE liAS BEEN RAPID ADOPTION OF VACUUM-ASSISTED
CLOSURE (VAC) TECHNOLOGYto treat many acuteand chronic wounds despite a rudimentary under-standing of the biologic mechanisms of action andfew weIl-controIled, prospective, randomized c1ini-cal trials of its use.
An expert panel carried out a selected review
of published literature regarding the mechanismsof action of the VAC device in the context of
published c1inical studies.The current literature suggests primary mecha-
nisms of action of the VAC device may inc1ude thefoIlowing: (I) drawing the wound edges together;(2) stabilization of the wound environment;(3) decrease in wound edema and rem oval ofwound exudate; and (4) microdeformations of the
wound surface. Secondary effects inc1ude increasedangiogenesis, granulation tissue formation, and, insome cases, a decrease in bacterial bioburden.
Supported by a grant from Kinetic Concepts, Inc. (KCI). Thisdocument reflects the opinion of the authors and was not influ-enced by KCI.
Dr Orgill reports having received consulting fees and a researchcontract from Kinetic Concepts, Inc. (KCI) for studies per-formed at Brigham and Woman's Hospital; he is an expertwitness for KCI and Wake Forest University. Dr Sumpio,Dr Attinger, and Dr Lee disclosed consulting fees from KCI,San Antonio, TX.
Accepted for publication February 2, 2009.
Reprint requests: Dennis P. Orgill, MD, PhD, Division of Plasticand Reconstructive Surgery, Brigham and Women's Hospital, 75Francis Street, Boston, MA 02115. E-mail: [email protected].
Surgery 2009;146:40-51.0039-6060/$ - see front matter
@ 2009 Mosby, Inc. AlI rights reserved.
doi: 10.1016/j.surg.2009.02.002
40 SURGERY
INTRODUCTION
The c1inical evidence for the efficacy of the VACdevice is mostly in retrospective case series. A fewrandomized control studies have shown efficacy indiabetic foot infections, pressure ulcerations, andskin grafts. Additional research into the mecha-
nism of action wiIl provide a better understandingof how to best use current devices and help makeimprovements in future device designo
With our aging population and increases inobesity and diabetes, problem wounds are becom-ing an increasing burden to our healthcare system.In addition, c1inicians are faced with an array ofproblem wounds from military and domestictrauma as weIl as from complex surgical procedures.Better, cost-effective methods of c10sing difficultwounds efficiently wiIl reduce the pain and ampu-tation rates associated with wounds. Despite thetheoretical promise of topicaIly applied growthfactors, there is currently only a limited c1inicalrole with only 1 commercial product available forc1inical use in the United States.1 Other methods,
such as bioengineered skin substitutes, have beensuccessful in certain defined areas of wound heal-
ing, but most advanced wound care products inuse today are based on the principIe of moist woundhealing defined by Winter and Scales in the 1960s.2,3
WOUND HEALING PHYSIOLOGY
Acute wounds progress through a complexseries of biochemical and ceIlular events describedas the phases of wound healing: hemostasis, in-flammation, proliferation, and remodeling. Suc-cessful wound healing is contingent on theorchestration of a myriad of biochemical signalpathways from a wide range of ceIl types during the
82---

SurgeryVolume146, Number 1
Table. Health technology assessment summary
Healthtechnologyassessment Conclusions
Orgillet al 41
Ontario Health Technology AdvisoryCommittee, 200414
Comments
VAC therapy may be useful forhealing various types of woundsbut effectiveness could not be
empirically quantified
AHRQ/BlueCross/BlueShield,200415
- Small sample size and patientpopulations
- Poor study design- Outcome measures could not be
compared- Small number of studies
- Inadequate randomization inmost studies
- Study groups not comparable
Body of evidence insufficient tosupport conclusions abouteffectiveness
Weak evidence of effectiveness
VAC may have advantages over otherforms of wound dressings studiedbut toa few reports to say
Limited evidence for effectivenessand adverse events
Cochrane Review, VI{, 200316Centre for Clinical Excellence,
Australia, 200317
NHS Quality ImprovementScotland,200318
Cochrane Review, VI{, 200119
- 3 articles met inclusion criteria
- No LeveI I or 11were identified
- Saline gauze is not standard treat-ment of wounds in Scotland
- Need for more RCTs
- Small sample sizes- Methodologicallimitations
Weak evidence that TNP is superiorto gauze dressings
VAG,Vacuum-assisted closure; AHRQ, Agency for Healthcare Research and Quality; RGT, randomized clinical lrial; TNP, topical negative pressure.
4 phases. Chronic wounds, in contrast, do notmake an orderly progression through the phasesand are unable to complete the sequence. The lackof wound progression can be due to a number offactors, including increased protease production,infection, nutritional state, vascular disease, andradiation. Common to chronic wounds is a de-
creased proliferative response in the healing cas-cade. There are a variety of pharmacologic,ceIlular, biochemical, and mechanical methodsthat alter the normal wound healing sequence.4-6Correcting defects in the normal healing phasesor devising methods to accelerate wound healingwould be of great benefit. For an active prolifera-tive process to occur in wound healing, the funda-mental drivers of mitogenesis should beconsidered, which include growth factors, extracel-lular matrices, and mechanical forces.
VAC DEVICE
Argen ta and Morykwas7and Morykwas et al8 firstdescribed the beneficial use of the vacuum assisted
closure (VAC) device for wound healing in 1997 (Ki-netic Concepts, Inc., San Antonio, TX). The deviceconsists of a vacuum pump, a canis ter with a con-necting tube, an open-pore foam, and a semiocclu-sive dressing. Although suction devices havecommonly been used to drain surgical sites and in-vestigators such as Fleischmann et al9 have de-scribed a vacuum-sealing technique, the VACdevice has gained increased popularity among users
over the past decade. A number of other deviceshave or wiIl be marketed based on the concept ofwound suction, which is sometimes referred to asnegative pressurewound therapy.Although these de-vices share some of the same design characteristicsof the VAC device, we restricted our review to theVAC device and the most common interface mate-
rial, the open-pore polyurethane ether foam, be-cause of a lack of peer-reviewed articles aboutother devices. The polyvinyl alcohol foam is a white,nonadherent foam that is used by some cliniciansover viscera and to reduce pain with dressingchanges; there are no LeveI I or 11 studies usingthis type offoam.
Since the original reports,7,8 more than 500peer-reviewed papers in the medical literaturehave been published describing the effect of VACin a number of wound types. Most of the reportshave been case series and retrospective reviews,with a few prospective, randomized studies pub-lished in the areas of diabetic foot infection,IO,11pressure sores,12 and skin grafts.13 Several system-atic reviews ofVAC technology have also been pub-lished (Table).14-19 Although a number ofindependent reports suggest compelling evidence,the smaIl number of prospective, randomized stud-ies makes it difficult for public health policymakersto assess clinical efficacy.20 The foIlowing is a se-lected review of the current literature and descrip-tion of current knowledge regarding themechanism of action of the VAC device.
83

42 Orgillet ai
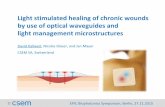
Fig 1. Proposed mechanisms of action of the VAC de-vice. The device covers the wound and keeps the woundsurface moist and insulated. For deformable wounds, thedevice can be used to pull the edges together (macrode-formation). It removes extracellular fluid and wound ex-udate and causes microdeformation at the foam-wound
interface. Secondary effects include changes in bloodflow, wound biochemistry, systemic inflammatory re-sponse, and bacterial load.
MECHANISM OF ACTION OF VAC DEVICE
Primary effects. There are 4 primary mecha-nisms of action of the VAC device described in theliterature: (1) contraction of the wound (macro-deformation); (2) stabilization of the wound envi-ronment; (3) removal of extraceIlular fluid; and(4) microdeformation at the foam-wound inter-face (Fig 1).
Contractionof wound (macrorkfvrmation):Skin andsoft tissues have a natural tension in their normal
state. When an incision is made through the skin,it naturaIly pulls apart. For example, in patientswith midline abdominal wounds that are left open,there is shrinkage of the abdominal wall that isreferred to as loss of domain. Maintaining approxi-mation of tissues during wound healing allowsfor earlier closure by delayed primary or secondaryintention. Studies of traumatic abdominal injurieshave shown that use of a modified VAC device can
allow for subsequent wound closure and may cir-cumvent the need for skin grafts over viscera.21The open-pore polyurethane foam that is usedwith the VAC device efficiently transmits pressureand evacuates exudates. When exposed to suctionat 125 mm Hg, the foam volume decreases byabout 80%.22 The shrinkage is in 3 dimensions,and the amount of shrinkage of the wound willmostly be determined by the deformability of thesurrounding tissues.
~.\, ,
; },. t
/ i
Surgeryluiy 2009
The effect of the macroscopic deformation oftissues as a result ofVAC placement will depend onthe type of tissue treated. For example, placementof the VAC device into an incisional wound in anobese abdomen with a large amount of deformableskin and soft tissue wiIl result in near approxima-tion of the wound edges. In contrast, use of thedevice on scalp wounds causes minimal contrac-tion of the wound edges, with the foam shrinkageoccurring mostly perpendicular to the woundsurface.
For deformable wounds, cutting the foam in astrategic fashion will facilitate wound closure byaIlowing the wound edges to come together morequickly. Depending on the structural characteris-tics of the foam, the foam exerts mechanicalforces on the tissue exposed to the VAC device.23For example, in a circumferential extremitywound, there is a theoretical possibility for circum-ferential shrinkage of the foam to cause a com-pressive force on the underlying tissues (Fig 2).Kairinos et al24 recently confirmed this hypothesisin humans treated with VAC therapy for 48 hours.In this same study, they showed that tissue pres-sures were increased when measured about 1 cm
from the wound with the VAC in place. Thesepressures increased as suction levels were in-creased; over time, there was some normalizationof these pressures.24 Quantitative modeling ofthis phenomenon will be important to predictchanges in wound volume as a function of the an-atomic location of the wound and the patient ageand body habitus.
Stabiiization of wound environment The VAC de-vice uses a semiocclusive polyurethane drape thathas limited permeability to gases and water vaporand impermeability to proteins and microorgan-isms. The dressing is typically changed every 2-3days, which eliminates the discomfort of the dailydressing changes typically associated with tradi-tional gauze-based dressings. Gauze dressings canallow evaporation of fluids and concentration ofproteins at the wound surface and eventuallyproduce a scab that delays healing. In contrast,moist wound-healing modalities, such as alginates,promote angiogenesis and the breakdown of ne-crotic tissues while decreasing pain.2,3 The VACdevice appears to evacuate fluid with its accompa-nying electrolytes and proteins, thereby keepingthe osmotic and oncotic gradients at the woundsurface theoretically stable. Objective studies, how-ever, are needed for confirmation. Clinicians usingthe VAC device have noted that part of the woundwill desiccate if a small hole develops in the overly-ing drape.25
84

SurgeryVolume146, Number 1
Orgill et al 43
A Macrodeformation
BloocIVessel Deformation
---.
:---!.
J'~'
Without Suction With Suction
B Microdeformation
5trut
NormalWoundTissue
P = 125 mmHg
Stiffer Tissue(Scar)
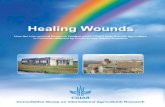
Fig 2. Wound defonnation. (A) Macrodefonnation: The foam contracts when vacuum is applied and can cause tensionon wound edges to bring the wound edges together, which might potentially cause a compressive force on circumfer-ential wounds. (B) Microdefonnation: The VAC device causes rapid fonnation of granulation tissue that mirrors thefoam surface. Stiffer tissue will deform less with the same foam pore size and suction.
The physical properties of the polyurethaneether foam very like1y contribute to the efficacyof the VAC device by allowing efficient pressuredistribution and removal of exudates. The cur-
rently available polyurethane ether foam (blackfoam) has a mean pore size of 423 J.L,a mean porevolume (when uncompressed) of 97%, a bulkmodulus of e1asticity of 3.06 kPa (23 mm Hg)when 50% compressed, and a Poisson's ratio ofO.O(K. Kieswetter, KCI, San Antonio, TX, personalcommunication, December 2007). Based on clini-cal experience, one suction device is adequate formost large wounds. However, more than 1 suctionpump may be necessary in patients with very largewounds involving a large extremity or trunk area.
More clinical information about the flow and
pressure distribution characteristics of the foamin large and highly exudative wounds would helpclinicians determine the optimal number of suc-tion ports to apply.
The thermal conductivity of the VAC device willbe an aggregate of the conductivity of the overlyingsemiocclusive drape and the polyurethane foam(Fig 3). Because the compressed foam is likely tobe saturated with liquid during application, thethermaI conductivity will be on the order of wateror 0.014 (calorie per second [cal/s] meter degreesCe1sius [m CO]) and will be roughly comparable totissue at a similar thickness. Additional heat trans-fer is minimized because of the reduction of
85

44 Orgillet ai
Wound Environment
SemipermeableMembrane ,~ ThermalInsulation
-.~1
, I
BiomaterlalInteractlon
Fig 3. Wound environment. The VAC device keeps thewound moist and wann compared with dry dressingsthat allow the wound to dry out and fonn a scab. TheVAC device also acts as an insulating layer.
evaporation of water from the wound surface. Arandomized study by Kloth et al26 showed that nor-mothermic wound therapy speeds wound healingin chronic, full-thickness pressure sores. Morework with actual temperature measurements andwater content of the wound and foam would be
helpful in better understanding this mechanismof action.
The uniform apposition of a skin graft orartificial dermal matrix to the underlying woundis critical for optimal take. Randomized studies ofskin graft take comparing VAC devices to conven-tional bolster dressings have shown better, morereliable take in the skin grafts and dermal matriceswhen they are bolstered with a VAC device.27Jeschke et al27 compared 11 patients treated witha combination of artificial dermis (Integra; IntegraLifeSciences, Plainsboro, NJ), fibrin glue, and VACtherapy with 6 patients that received Integra cov-ered with a compression dressing. The researchersfound a significant increase in the Integra take anda decreased time to apply the autograft in the studygroup.27 Moisidis et al13 designed a prospective,randomized study in which skin-grafted woundswere divided into 2 areas-I treated with VACand the other treated with a standard bois ter dress-
ing. They were able to show improved graft take inthe areas treated with the VAC device. Two weeks
after grafting, the VAC-treated areas appeared tobe of better quality than the bolster group.
Decrease in edema and removai of wound exudate: Anobvious consequence of VAC therapy is the abilityto evacuate wound exudates. Clinicians are well
aware that edema impedes healing and recom-mend eIevation and compression of extremities todecrease edema and facilitate healing. Swelling
Surgeryluiy 2009
Fluid RemovalPore
~I~
Without Suction With Suction
Fig 4. Fluid remova!. The foam distributes the vacuumevenly throughout the wound and allows for transportof extracellular fluid to the wound surface.
from edema may actually cause compression ofcells within the extracellular matrix, thereby de-creasing their intrinsic tension, resulting in adecreased proliferative response (Fig 4). Applica-tion of a distributed suction allows direct evacua-
tion of fluid from the extracellular space andappears to decrease edema (Fig 4). In compart-ment syndrome of the extremities, there is massiveswelling that necessitates release of fascial compart-ments to maintain perfusion and prevent celldeath. By removing extracellular fluid, the VAC de-vice may hasten resolution of compartment syn-drome after fascial release and allow for earlier
closure of the fasciotomy wounds. In addition,there may be an increase in blood flow when theedema fluid concentrated around small blood ves-
seis is evacuated, but more research is needed.
Yang et al28 retrospectiveIy compared lower ex-tremity fasciotomies and demonstrated that thewounds could be closed in an average of 6.7 dayswith the VAC device versus 16.1 days without thedevice. Weiland29 used VAC devices in combina-
tion with hyperbaric oxygen therapy in 3 complexlower extremity crush injuries and suggested thatboth modalities may be synergistic in decreasingedema. DeFranzo et al30 showed decreases in the
extremity circumference and ::5500 ml/24 h re-moval of fluid from lower extremity wounds withexposed bone. The fluid flow past cells in thewound may also exert important shear stressesthat could modulate cell function.
At a basic leveI, tissue is composed of both fluidand solid phases. Within the extracellular matrix,the fluid phase is the interstitial electrolyte solu-tion, whereas the solid phase is the collagenousextracellular matrix. Mechanically deforming thisbiphasic material results in 2 phenomena, (1) astrain field is established in the solid matrix uponwhich the cells are anchored, and (2) a flow of
I
i86

SurgeryVolume146, Number 1
fluid is created within the interstices of the ma-
trix.31 Thus, cells are subjected to mechanicalstretch mediated by their attachments to the ma-trix and shear stress due to fluid flow. It is well es-
tablished that fluid shear stresses can regulatecellular proliferation and biosynthetic responsesin cell cultures.32 In addition, the movement of
ions in solution past matrix glycoproteins estab-lishes electric fields (ie, streaming potentials)that can also stimulate cellular responses.33,34 InVAC therapy, tissue deformation occurs by movinginterstitial fluid and deformation of the solid
phase, which is a process similar to what happenswhen one squeezes a wet sponge. Mechanicalloading directly drives the flow of interstitial fluidand mechanical deformation of structural macro-
molecules such as collagen.Murphey et al35 measured interstitial pressure
adjacent to the VAC device in an animal modeland found a gradient of pressures out to nearly1 mm from the wound surface when suction was
applied. Theoretically, cells embedded in the tis-sue are also deformed or, at the least, subjectedto forces that tend to deform the cell membrane,
Furthermore, deformation of tissue leads to
changes in ionic concentrations of the interstitialfluid as well as generation of interstitial electricalcurrents.31 To date, studies on shear stress have pri-marily concentrated on endothelial, bone, and in-testinal epithelial cells, and the results may not bedirectly translatable to wounds.36-39 In addition,there are notable toxic materiaIs within the wound,
including bacteria, inflammatory cytokines, andmatrix metalloproteinases (MMPs). A preliminarystudy from Stechmiller et al40 showed a significantdecrease in TNF-alpha from VAC wound fluid ex-tracted from pressure sores during the course ofI week.
Argenta and Morykwas 7 and Morykwas et aIS rec-ognized the importance of fluid removal as a sig-nificant benefit of the VAC device. Fluid removalis critical in burns to modulate the 3 zones of
injury originally described by Jackson.41 Jacksondescribed a zone of stasis that is a potentially re-versible area of the burn, which can be made worse
by hypoperfusion and edema. In experimental par-tial-thickness porcine burns, Morykwas et al42 sawsignificant decreases in burn depth when thewounds were treated with the VAC device. Accord-
ing to Jackson's description, the zone of stasis ex-ists for only the first 24 hours after injury; thiszone then becomes incorporated into either thezone of hyperemia (tissue should recover) or coag-ulation (irreversible tissue loss) .41The effect of theVAC device was to decrease the accumulation of
Orgillet ai 45
edema fluid, thereby limiting the depth of cellulardeath. The observed decrease in burn depth hasclinical importance because superficial 2nd-degreeburns have the capacity to heal, whereas deep2nd-degree burns are best treated with the more
invasive method of excision and graftin§.42 In 7patients with bilateral burns, Kamolz et al4 studiedperfusion and the amount of fluid removed. Inthis small study, their impression was that theVAC device increased perfusion to the hand, andthey removed a clinically relevant volume of extra-cellular fluid ($500 ml).
Intraabdominal hypertension can lead to intra-abdominal compartment syndrome. Release of theabdomen can be a lifesaving event but leaves thepatient with a very large, open wound with poten-tial complications of infection, hernia, and fistula.The VAC device provides a method to keep thewound moist, draw the wound together to mini-mize loss of domain, and evacuate excess abdom-inal fluidoThe bowel is covered with a plastic drapeto avoid direct contact of the polyurethane foamwith the bowel. Many centers perform VACchanges on open abdomens every 2-3 days in theoperating room with successive closure of theabdominal wound. Using this approach, skin graft-ing directly over bowel can be avoided in manycases.21
Microdeformation at the foam-wound interface:Woltr4 recognized the fundamental role of me-chanical force in regulating tissue growth, repair,and remodeling more than a century ago. Tissueadaptation to changing physical stresses is a basicrequirement for growth and survival of living sys-tems.32 Application of mechanical loading of tis-sues results in deformation. The magnitude ofthe biomechanical responses described above is de-pendent on the stiffness of the tissue to which theVACis applied and the dynamics ofthe mechanicalloading. If there is a rapid pressure change, thenthe flow of interstitial fluid will be more rapid. Ifthe pressure change is applied slowly,then intersti-tial flows will be more gradual and matrix stress ap-plied to cells will be much less. Thus, it is likely thatthe biologic response to VAC loading will dependon the frequency of vacuum application. There islimited published work done on phasic VAC ther-apy. Morykwas et aIs applied 125-mm Hg suctionto porcine wounds using a 5 minute on/2 minuteoff cycle and noted increased blood flow in thearea and an increase in hyperproliferative tissue.Wackenfors et al45applied 125 mm Hg of pressurewith the VAC device on porcine wounds intermit-tently with increasing periods of time between the"on" vacuum and "off" vacuum. They observed
87

46 Orgill et ai
that peak blood flow in the tissues decreased dur-ing the "on" periods and increased 40-50% abovebaseline when the vacuum was turned off.45 The
optimal waveform for the VAC device has yet tobe determined for specific wound types.
For biphasic materiaIs, mechanical deformationimposed on the surface defuses through the ma-trix at a rate that depends on tissue hydraulicpermeability, matrix stiffness, and deformationkinetics.34 Thus, both shear and deformation
forces acting on cells are dependent on the rateat which the fluid flows through the matrix. Theprecise mechanisms by which the frequency of im-posed stress influences cellular response are notwell described.
Microdeformations induce cellular proliferationand angiogenesis in vivO.22Skin expands as a resultof stretch in growth, morbid obesity, aging, andpregnancy. We commonly take advantage of this ef-fect in tissue expansion that shows a well-definedproliferative and angiogenic response.46 Ilizarov's. .
k b I h . 4748 h dplOneenng wor on one engt enmg , s owethat introducing gradual traction on bone leads toosteogenesis and that skin, muscle, and nervecould lengthen in tandem. A controlled distrac-tion rate of 0.25-0.7 mm per day in experimental
animal models showed increased cellular rrolifera-tion. In soft tissue, Pietramaggiori et al4 showedboth a vascular and proliferative response whenrat ears were placed under tension.
Often, in clinical practice, a number of woundsthat have minimal exudate into the VAC canis ter
have a dramatic proliferative response to VACtherapy. Huang et al50 and Huang and Ingber51 il-lustrated that nonmalignant cells require tensionto divide and prolifera te. Mechanical stresses cause
physiologic changes in cell function through amechanism referred to as mechanotransduction.52
According to the basic cell model proposed byHuang et ai50 and Huang and Ingber,51 much ofthe mechanotransduction cell signaling occursthrough the cytoskeleton. Integrins are also knownto be important in mechanotransduction and cantransmit surface signals to intracellular signalingmechanisms to alter gene transcription. To date,most mechanotransduction experiments havebeen conducted on vascular cells, osteocytes, andenterocytes.37
The currently known responses of vascular cellsto mechanical stimuli include inhibition of apo-ptosis, upregulation of cell signaling molecules(such as extracellular signal-regulated kinase path-way, Jun N-terminal kinase, stress-activated protein
~inase, an~ p38), ~hang.es i~ ~ene expression, andmcreases m prohferatlOn: 3,.4 McNulty et al53
SurgeryJuly 2009
showed greater cell death and less cell migrationand proliferation of fibroblasts with gauze undersuction than with VAC or static controls.Nishimura et al54 observed differences in human
dermal fibroblast response under differentfrequencies of stretch. Jacobs et ai 55 showed in-creased collagen organization and maturationand increased expression of vascular endothelialgrowth factor and fibroblast growth factor-2 in arat wound model using VAC compared to controI.
Saxena et al23 reported a mathematical modelof a wound treated with the VAC device. The
open-pore polyurethane sponge was modeled asa rigid device with a uniform pore structure in a2-dimensional modeI. Linear elastic propertiesfor the underlying tissue were assumed. The modelshowed that the wound would be compressedwhere it was in contact with the foam and, undertension, in the void between the foam struts. The
result was an undulating surface where the woundcontacted the foam. Increasing the vacuum or thepore size resulted in increased wound deforma-tion. Increasing the stiffness of the wound, a com-mon phenomenon during the healing process,decreased the deformation of the wound. When
the model was compared to histologic cross sec-tions ofwounds treated with the VAC device, there
was a remarkable similarity in the deformation pat-tem. The authors hypothesized that lengtheningthe wound surface on a microscale (microdefor-mation) resulted in stretching the cells within thewound.23 The model predicted that the VAC de-vice induced average tissue strains in the range of5-20%, depending on the stiffness of the woundand foam characteristics. These strains are
consistent with the range shown to promote cellu-lar proliferation in vitro.
The optimal physicochemical properties of theinterface materiaIs have not yet been elucidated,but a properly designed interface material may becritical to device performance. The current poly-urethane foam appears to have been discoveredempirically. A previous study by Scherer et al22shows that the foam by itself causes a vascularresponse of the wound. Application of suction tothe foam induces microdeformations of the wound
bed and induces both cellular proliferation androbust angiogenesis. The concept of microdefor-mation will be an important future area ofinvestigation.
Secondary effects. Speedswound healing.Josephet al12 randomized patients with pressure sore(s)to use of a VAC device or normal saline dressings;they found a decrease in wound volume of patientstreated with the VAC device at 6 weeks (78% vs
88.-.

SurgeryVolume146, Number 1
30%). Eginton et al56 designed a cross-over, ran-domized trial in diabetic foot wounds and showed
a decrease in wound volume of 59% vs 9%. Largerstudies in different wounds types are needed tobetter understand this effect.
Increasesin bloodflow around wounds: Because ofone or more of the primary mechanisms describedabove, there is an eventual increase in blood flowin the wound due to the VAC treatment. When a
c1inician changes a VAC device a few days afterapplication, increased granulation tissue with nu-merous smaIl blood vessels is observed on histo-logic sections.23 To study potential increasedperfusion to the tissues, most investigators haveused the noninvasive laser Doppler device. Al-though useful, laser Doppler does not determineblood flow directly, and so results from studies us-ing the device need to be interpreted with caution.Laser Doppler measures red ceIl velocity and con-verts it to blood flow by a derived formula. A de-crease in vessel diameter can cause increases influid velocity even though the overaIl flow is de-creased. Timmers et al57showed that laser Dopplerreadings increased when a VAC device was placedon normal human skin. Morykwas et al8 showedsimilar results on open porcine wounds using animplantable Doppler probe. Wackenfors et al45measured blood flow around a porcine groinwound treated with VAC and found an area ofhypoperfusion within about 1.5 cm from thewound edge.
Ichioka et al58designed an experimental modelthat quantitatively visualized the wound bed micro-circulation under subatmospheric application.They determined that a gauge pressure of -125 mmHg significantly increased blood flow in the woundbed immediately after pressure application and for1 minute after pressure release. In contrast, applica-tion of -500 mm Hg caused a decrease in bloodflow, reaching statistical significance after 5 minutes.Recently, Kairinos et al59measured tissue perfusionin healthy human subjects with a radiotracertechnique and showed a decrease in perfusion thatcorrelated to increased values of suction. Further
studies using thermal diffusion technology, corro-sion casting, fluorescent particles, or radioactivetracer methods may be more useful in providinga more thorough understanding of the angiogenicresponse to the VAC device and the appropriatetype and application of negative pressure to whichthe wound is exposed.
Changes in bacterialburden: Morykwas et al8 firstdescribed a decrease in bacterial load using theVAC device in experimental pigs. The mechanismbehind the observation is not c1ear, and there
Orgillet al 47
may be several factors that influence the total bac-terial burden of the wound, such as direct removalof bacteria and alterations in blood flow. Clinicalresults from other centers have yielded mixed re-sults. Moues et al60 studied 54 patients in a pro-spective, randomized trial in which one half ofthe patients were assigned to VAC therapy andthe other half was assigned to dressing changeswith normal (0.9%) NaCl. The researchers foundthat patients with wounds culturing nonfermenta-tive, gram-negative bacilli had decreased bacterialloads over time, whereas patients with wounds cul-turing Staphylococcusaureus had increased bacteriallevels over time.60
Alterations of the polyurethane foam may be animportant mechanism to better treat bacterial
colonization. One method involves coatin~ thepolyurethane foam with silver. Gerry et aI 1 re-ported on 2 patients with complex venous stasis ul-cers that were unresponsive to conventional VACtherapy but that responded weIl to the use of asilver-impregnated foam with the VAC device. In-stiIlation of solutions into the foam and wound
via the vacuum pump, a technique popularizedby Moch et al,62 may provide another method tohelp keep bacterial levels low in wounds. The is-sues of biofilms and defensins wiIl be important fu-ture areas of research.
Changes in wound biochemistry and systemic re-sponse: The expression of genes by ceIls in thewound and the regulation of gene expression arelikely to be important factors in explaining themechanisms of action of VAC therapy. Greeneet al63 studied the MMP profiles in 3 debilitatedpatients undergoing VAC therapy. In 1 area ofeach wound, the foam was not placed in contactwith the wound bed. Wound biopsy samples com-paring areas of foam contact with non-foam con-tact showed dramatic differences in angiogenicresponse and decreases in the MMP-9jNGAL(neutrophil gelatinase-associated lipocalin) andMMP-2. Shi et al64 performed a consecutive,1 week study of chronic wounds and showed adecrease in MMP-l and MMP-13 that was deter-mined by real time-polymerase chain reaction ofwound biopsy samples. The researchers64 hypothe-sized that the decreased MMP activity decreasedthe breakdown of the wound connective tissue ma-
trix, thereby blocking the inhibitory effects ofMMPs on wound healing. The biologic responsein the wound likely has some systemic effect.Norbury and Kieswetter65 showed a decrease in cir-culating monocytes and interluekin-6 36 hoursafter injury in porcine wounds treated with theVAC device.
89

48 Orgillet ai
lmproves wound bed preparation:Surgeons recog-nize that a nicely granulating wound is likely to befavorable for skin grafting. Lack of granulationtissue is commonly seen in radiation or vascularwounds. Morykwas et al8 showed a greater than60% increase in granulation tissue formationwith application of VAC to porcine wounds incomparison to wounds treated with moist gauze.Further porcine studies showed that a 125-mmHg vacuum resulted in faster formation of granula-tion tissue than either 25 mm Hg or 500 mm Hg.66Armstrong and Lavery, in conjunction with theDiabetic Foot Study Consortium,10 performed aprospective, randomized controlled study of 162diabetic foot amputation sites; their study'sprimary endpoint demonstrated a greater rate ofclosure of the VACgroup compared to the controlgroup using standard wound care at 112 days (56%vs 39%).
Blume et al67studied diabetic foot wounds in 2
groups of patients; they noted that granulation tis-sue covered the wound more quickly in the groupof patients treated with the VAC device, resultingin faster wound closure, than the group of patientsreceiving standard treatment. Vuerstaek et al68carried out a prospective, randomized trial oflower extremity ulcerations, mostly venous in na-ture, and compared the effect of VAC therapywith standard compression therapy. When thewounds had filled with granulation tissue, the re-searchers applied 4-mm punch full-thickness skingrafts to the wounds. Wounds healed faster inthe VAC group (29 vs 45 days), and the time towound bed preparation was also shorter (7 vs 17days) .
DISCUSSION
The VACdevice most commonly is used with anopen-pore polyurethane ether foam that appearsto be an important component and contributes toseveral of the device's mechanisms of action byproviding an efficient removal of exudate, evenlydistributing pressure within the wound, and in-ducing angiogenesis. The compressibility of thefoam allows for the VAC device to exert tension
on many types of wounds, drawing the edges to-gether. In skin grafts, the foam provides a uniformdistribution of the vacuum, which results in a morereliable take of skin grafts. Effective fluid removalis important for swollen or edematous wounds,such as burns or the wounds used to relieve a com-
partment syndrome. Furthermore, microdeforma-tions of the wound surface seem to induce amechanotransduction mechanism that alters
Surgeryjuiy 2009
genomic expression to promote increased vasculargrowth and alter wound biochemistry. Additionalresearch in biomaterial properties of the foam, sur-face coatings, optimal pore structure, and mechan-ical properties will be important to identify theoptimal interface material.
Clinical research with wound healing devices ischallenging due to the heterogeneity of thewounds treated by clinicians, the variability ofresponse, the lack of agreement on the best end-point metrics, and the difficulty of blinding thetreatment arms. Most studies of the VACdevice are
case reports or retrospective clinical studies, oftenwithout optimal controls. Carefully designed clin-ical trials based on our recent understanding ofwound healing should add to our understandingof the mechanisms of action. The advances in
molecular biology, including gene chips, proteo-mics, zymography, and advanced methods to studycell biology, provide powerful tools for both basicscientists and clinicians to elucidate mechanismsof action.
The mechanotransduction and alterations in
extracellular fluid may be 2 of the unique mech-anisms of action of the VAC device. The time
course of the biologic response to microdeforma-tion in conjunction with the study of the optimalwaveform should be very important for the designof new therapies. Understanding the response ofcell deformation, cell wall tension, and cell shape,as well as fluid flow past cells may also add newknowledge to the mechanism of action.
Although the VAC device has caused a majorshift in wound care practice, the therapy is notbeneficial for the treatment of alI wounds. In
addition, the use of the VAC device is expensiveand should not be used in wounds that derive no
clinically important benefit. Some patients find thedevice cumbersome to wear as an outpatient andare happy to switch to a less complex modality.
Although most fgatients have reduced pain usingthe VACdevice, 9 some patients have reported sig-nificant pain. Caution should be used with patientsthat are anticoagulated or with bleeding that hasnot completely stopped before application. In-creased levels of bacteria in certain wounds cancause increased odor or delay healing. A better un-derstanding of the mechanisms of bacterial growthwhen the device is used and the effect of biofilms
would be helpful. The introduction of a silver-im-pregnated VACdevice61 and VAC devices irrigatedwith antibiotic solutions 70may provide more effec-tive methods to treat an increased bacterial load,but there are little published data to support theiruse.
90..

SurgeryVolume146, Number 1
Since being introduced just more than 10 yearsago, the VACdevice has had a major impact on theclinical care of complex wounds throughout theworld. Like with any new technology, clinicians arestilllearning the optimal methods of application. Asmore is discovered about the mechanism of action,clinicians willlearn the most appropriate use ofVACtherapy in specific wound types and better devicesmay be designed in the future for the increasingnumber of complex wounds seen each year.
We would like to thank Lauren Bayer, PA-C, andKimberly Ross for their help with the manuscript, andjason Orgill and Britlyn Orgill for the figures.
REFERENCES
1. Smiell JM, Wieman TJ, Steed OL, Perry BH, Sampson AR,Schwab BH. Efficacy and safety of becaplermin (recombi-nant human platelet-derived growth factor-BB) in patientswith nonhealing, lower extremity diabetic ulcers: a com-bined analysis of four randomized studies. Wound RepairRegen 1999;7:335-46.
2. Winter GO. Effect of air exposure and occlusion on exper-imental human skin wounds. Nature 1963;200:378-9.
3. Winter GO, Scales JT. Effect of air drying and dressings onthe surface of a wound. Nature 1963;197:91-2.
4. Burke JF, Yannas IV, Quinby WC Jr, Bondoc CC, Jung WK.Successful use of a physiologically acceptable artificial skinin the treatment of extensive bum injury. Ann Surg 1981;194:413-28.
5. Parenteau N. Skin: the first tissue-engineered products. SciAm 1999;280:83-4.
6. O'Connor NE, Mulliken JB, Banks-Schlegel S, Kehinde O,Green H. Grafting of burns with cultured epithelium pre-pared from autologous epidermal cells. Lancet 1981;1:75-8.
7. Argenta LC, Morykwas MJ. Vacuum-assisted cIosure: a newmethod for wound control and treatment: cIinical experi-ence. Ann Plast Surg 1997;38:563-76.
8. Morykwas MJ, Argenta LC, Shelton-Brown EI, McGuirt W.Vacuum-assisted cIosure: a new method for wound controland treatment: animal studies and basic foundation. Ann
Plast Surg 1997;38:553-62.9. Fleischmann W, Strecker W, Bombelli M, Kinzl L. Vacuum
sealing as treatment of soft tissue damage in open fractures[in German]. Unfallchirurg 1993;96:488-92.
10. Armstrong OG, Lavery LA. Oiabetic Foot Study Consortium.Negative pressure wound therapy after partial diabetic footamputation: a multicentre, randomised controlled trial.Lancet 2005;366:1704-10.
11. Armstrong OG, Lavery LA, Boulton AJ. Negative pressurewound therapy via vacuum-assisted cIosure following partialfoot amputation: what is the role of wound chronicity? IntWoundJ 2007;4:79-86.
12. Joseph E, Hamori CA, Bergman S, Roaf E, Swann NF, Anas-tasi GW.A prospective, randomized trial of vacuum-assistedcIosure versus standard therapy of chronic nonhealingwounds. Wounds 2000;12:60-7.
13. Moisidis E, Heath T, Boorer C, Ho K, Oeva AR. A prospec-tive, blinded, randomized, controlled cIinical trial oftopicalnegative pressure use in skin grafting. Plast Reconstr Surg2004;14:917-22.
Orgill el al 49
14. Ontario Ministry of Health and Long-Term Care. Vacuumassisted cIosure therapy for wound care. Toronto: OntarioMinistry of Health and Long-Term Care; 2004.
15. Samson O, Lefevere F, Aronson N. Wound-healing technol-ogies: low-Ievellaser and vacuum-assisted cIosure. Summary,Evidence Report/Technology Assessment No. 111. Publica-tion No. 05-EOO5-1.Rockville (MO): Agency for HealthcareResearch and Quality (AHRQ); 2004.
16. Evans O, Land L. Topical negative pressure for treatingchronic wounds (Cochrane Review). In: The CochraneLibrary, Issue 4, 2003. Chichester, UK: John Wiley & Sons,Ltd.
17. Pham C, Middleton P, Maddem G. Vacuum-assisted cIosure
for the management of wounds: an accelerated systematicreview. North Adelaide (Australia): Australian Safety and Ef-ficacy Register of New Interventional Procedures-Surgical(ASERNIP-S), Royal Australasian College of Surgeons; 2003.
18. Vacuum Assisted Closure for Wound Healing. NHS QualityImprovement Scotland. November 2003. Available onlineat http://www.nhshealthquality.org/nhsqis/1129.htmI.Ac-cessed February 27, 2009.
19. Evans O, Land L. Topical negative pressure for treatingchronic wounds: a systematic review. Br J Plast Surg 2001;54:238-42.
20. Ubbink OT, Westerbos SJ, Nelson EA, Vermeulen H. A sys-tematic review of topical negative pressure therapy for acuteand chronic wounds. Br J Surg 2008;95:685-92.
21. Kaplan M, Banwell P, Orgill O, lvatury R, Oemetriades O,Moore FA, et aI. Guidelines for the management of theopen abdomen. Wounds 2005;Oct:SI-24.
22. Scherer S, Pietramaggiori G, MathewsJ, Prsa MJ, Huang S,Orgill OP. The mechanism of action of the vacuum assistedcIosure device. Plast Reconstr Surg 2008;122:786-97.
23. Saxena V, Hwang CW, Huang S, Eichbaum Q, Ingber O, Or-giII OP. Vacuum-assisted cIosure: microdeformations ofwounds and cell proliferation. Plast Reconstr Surg 2004;114:1086-98.
24. Kairinos N, Solomons M, Hudson OA. Negative-pressurewound therapy I: the paradox of negative-pressure woundtherapy. Plast Reconstr Surg 2009;123:589-98; discussion599-600.
25. Morykwas MJ, SimpsonJ, Punger K, Argenta A, Kremers L,Argenta J. Vacuum-assisted cIosure: state of basic researchand physiologic foundation. Plast Reconstr Surg 2006;(Suppl. 121):126.
26. KIoth LC, BermanJE, Nett M, Papanek PE, Oumit-Minkel S.A randomized controlled cIinical trial to evaluate the effects
of noncontact normothermic wound therapy on chronicfull-thickness pressure ulcers. Adv Skin Wound Care 2002;15:270-6.
27. Jeschke MG, Rose C, Angele P, Füchtmeier B, Nerlich MN,Bolder U. Oevelopment of new reconstructive techniques:use of Integra in combination with fibrin glue and nega-tive-pressure therapy for reconstruction of acute andchronic wounds. Plast Reconstr Surg 2004;113:525-30.
28. Yang ML, Chang OS, Webb LX. Vacuum-assisted cIosure forfasciotomy wounds following compartment syndrome of theleg. J Surg Orthop Adv 2006;15:19-23.
29. Weiland OE. Fasciotomy cIosure using simultaneous vac-uum-assisted cIosure and hyperbaric oxygen. Am Surg2007;73:261-6.
30. OeFranzo AJ, Argenta LC, Marks MW, Molnar JA, Oavid LR,Webb LX, et aI. The use of vacuum-assisted cIosure therapy
for the treatment of lower-extremity wounds with exposed
bone. Plast Reconstr Surg 2001;108:1184-91.
l
91

50 Orgillet ai
31. Lee RC. Gowrishankar TR. Basch RM. Patel PK, Golan DE.Cell shape-dependent rectification of surface receptortransport in a sinusoidal electric field. Biophysical j 1993;64:44-57.
32. McLeod Kj. Lee RC, Ehrlich HP. Frequency dependence ofelectrical field modulation of fibroblast protein synthesis.Science 1987;236:1465-9.
33. Folkmanj, Moscon A. Role of cell shape in growth control.Nature 1978;273:345-9.
34. Lee RC. Frank EH, Grodzinsky Aj, Reliance DK. Oscillatorycompressional behavior of articular cartilage and its associ-ated electromechanical properties. j Biomech Eng 1981;103:280.
35. Murphey GC, Macias BR, Hargens AR. Depth of penetra-tion of negative pressure wound therapy into underlying tis-sues. Wound Repair Regen 2009;17:113-7.
36. Kadohama T, Nishimura K, Hoshino Y,Sasajima T, SumpioBE. Effects of different types of fluid shear stress on endo-thelial cell proliferation and survival. j Cell Physiol 2007;212:244-51.
37. Zhangj, Li W. Sanders MA, et aI. Regulation of the intesti-nal epithelial response to cyclic strain by extracellular ma-trix proteins. FASEBj 2003;17:926-8.
38. Gilbert jA, Weinhold PS, Banes Aj, Link GW, jones GL.Strain profiles for circular cell culture plates containingflexible surfaces employed to mechanically deform cells invitro. j Biomech 1994;27:1169-77.
39. Buckley~, Banes Aj, Levin LG, Sumpio BE, Sato M,jordanR. et aI. Osteoblasts increase their rate of division and alignin response to cyclic, mechanical tension in vitro. BoneMiner 1988;4:225-36.
40. Stechmiller jK, Kilpadi DV, Childress B. Schultz GS. Effectof v.A.C.~ therapy on the expression of TNF-a, IL-l,MMP-2, MMP-3 and TIMP-I in wound fluid of adults withpressure ulcers. Wound Repair Regen 2006;14:371-4.
41. jackson DM. The diagnosis of the depth of buming. Br jSurg 1953;40:588-96.
42. Morykwas Mj. David LR, Schneider AM, Whang C,jenningsDA, Canty C, et aI. Use of subatmospheric pressure to pre-vent progression of partial-thickness bums in a swinemodel. j Bum Care Rehabil 1999;20:15-21.
43. Kamolz LP, Andei H, Haslik W, Winter W, Meissl G, Frey M.Use of subatmospheric pressure therapy to prevent bumwound progression in human: first experiences. Bums2004;30:253-8.
44. WolffJ. The law of bone remodeling. Maquet p. Furlong R,translators. Berlin: Springer-Verlag; 1986.
45. Wackenfors A, Sjogren j, Gustafsson R, AIgostsson L, In-gemansson R. Malmsjõ M. Effects of vacuum-assisted clo-sure therapy on inguinal wound edge microvascular bloodflow. Wound Repair Regen 2004;12:600-6.
46. Takei T, Mills I, Katsuyuki A. Sumpio BE. Molecular basis fortissue expansion: clinical implications for the surgeon. PlastReconstr Surg 1998;101:247.
47. llizarov GA. The tension-stress effect on the genesis andgrowth of tissues: part I. The influence of stability of fixa-tion and soft-tissue preservation. Clin Orthop Relat Res1989;238:249-81.
48. llizarov GA. The tension-stress effect on the genesis andgrowth of tissues: part 11. The influence of the rate andfrequency of distraction. Clin Orthop Relat Res 239;263-85.
49. Pietramaggiori G, Liu p. Scherer SS. et aI. Tensile forcesstimulate vascular remodeling and epidermal cell prolifera-tion. Ann Surg 2007;246:896-902.
Surgeryluly 2009
50. Huang S, Chen CS, Ingber DE. Control of cyclin DI, p27(Kipl), and cell cycle progression in human capillary endo-thelial cells by cell shape and cytoskeletal tension. Moi BiolCell 1998;9:3179-93.
51. Huang S, Ingber DE. Shape-dependent control of cell growth,differenriation, and apoptosis: switching between attractors incell regulatory networks. Exp Cell Res 2000;261:91-103.
52. Garcia-Cardena G. Comande r j, Anderson KR, BlackmanBR, Gimbrone MA. Biomechanical activation ofvascular en-
dothelium as a determinant of its functional phenotype.Proc Natl Acad Sci USA 2001;98:4478-85.
53. McNulty AK, Schmidt M, Feeley T, Kieswetter K. Effects ofnegative pressure wound therapy on fibroblast viability, che-motactic signaling, and proliferation in a provisional wound(fibrin) matrix. Wound Rep Regen 2007;15:838-46.
54. Nishimura K, Blume P, Ohgi S. Sumpio B. Effect of differ-ent frequencies of tensile strain on human dermal fibro-blast proliferation and survival. Wound Rep Regen 2007;15:646-56.
55. jacobs S. Simhaee DA. Marsano A, Fomovsky GM, Niedt G.WujK. Efficacy and mechanisms ofvacuum-assisted closure(VAC) therapy in promoting wound healing: a rodentmodel. j Plast Reconstr Aesthet Surg 2008 jul 8 [Epubahead of print].
56. Eginton MT, Brown KR, Seabrook GR, Towne jB, CambriaRA. A prospective randomized evaluation of negative-pres-sure wound dressings for diabetic foot wounds. Ann VascSurg 2003;17:645-9.
57. Timmers MS, Le Cessie S, Banwell P, jukema GN. The ef-fects of varying degrees of pressure delivered by negative-pressure wound therapy on skin perfusion. Ann Plast Surg2005;55:665-71.
58. Ichioka S, Watanabe H, Sekiva N, Shibata M, Nakatsuka T. A
technique to visualize wound bed microcirculation and the
acute effect of negative pressure. Wound Repair Regen2008; 16:460-5.
59. Kairinos N, Voogd AM. Botha PH, Kotze T, Kahn D, HudsonDA, et aI. Negative-pressure wound therapy 11: negative-pressure wound therapy and increased perfusion. just an il-lusion? Plast Reconstr Surg 2009;123:601-12.
60. Moues CM, van den Bemd Gj, Meerding "'], Hovius SE. Aneconomic evaluation of the use of TNP on full-thicknesswounds. j Wound Care 2005;14:224-7.
61. Gerry R, Kwei S. Bayer L, Breuing KH. Silver-impregnatedvacuum-assisted closure in the treatment of recalcitrant ve-
nous stasis ulcers. Ann Plast Surg 2007;59:58-62.62. Moch D, Fleischmann W, Westhauser A. Instillation vacuum
sealing-report ofinitial experiences [in German]. Langen-becks Arch Chir Suppl Kongressbd 1998;115:1197-9.
63. Greene AK, Puder M, Roy R, Arsenault D, Kwei S. MosesMA, et aI. Microdeformational wound therapy: effects onangiogenesis and matrix metalloproteinases in chronicwounds of 3 debilitated patients. Ann Plast Surg 2006;56:418-22.
64. Shi B, Chen SZ. Zhang P, Li jQ. Effects of vacuum-assistedclosure (VAC)on the expressions of,MMP-l 2,13 in humangranulation wound [in Chinese]. Zhonghua Zheng XingWai Ke Za Zhi 2003;19:279-81.
65. Norbury K, Kieswetter K. Vacuum-assisted closure therapyattenuates the inflammatory response in a porcine acutewound healing model. Wounds 2007;19:97-106.
66. Morykwas ~, Faler Bj, Pearce Dj, Argenta LC. Effects ofvarying levels of subatmospheric pressure on the rate ofgranulation tissue formation in experimental wounds inswine. Ann Plast Surg 2001;47:547-51.
92
-.

SurgeryVolume146, Number 1
67. B\ume PA,WaltersJ, Payne W, AyalaJ, LantisJ. Comparisonof negaúve pressure wound therapy using vacuum-assistedclosure with advanced moist wound therapy in the treat-ment of diabeúc foot ulcers. Diabetes Care 2008;31:631-6.
68. Vuerstaek JD, Vainas T, Thissen CA, van der KleyJ, Nele-mans P, Neumann MHA, et aI. State-of-the-art treatmentof chronic leg ulcers: a randomized controlled trial com-paring vacuum-assisted closure (V.A.C.) with modem
Orgill et al 51
wound dressings. J Vasc Surg 2006;44:1029-37; discussion1038.
69. Ozturk E, Ozguc H, Yilmazlar T. The use ofvacuum assistedclosure therapy in the management ofFoumier's gangrene.ArnJ Surg 2009;197:660-5.
70. Jerome D. Advances in negaúve pressure wound therapy:the VAC insúll. J Wound Ostomy Conúnence Nurs 2007;34:191-4.
Reprintedwith permission from Surgery 2009; 146(1):40-51. Orgill DP,Manders EK, Sumpio BE, et aI.The mechanisms ofaction ofvacuumassisted closure: more to leam. Copyright 2009 (Ç)EIsevier, Inc.
93