Clinical Review of Current Treatment Strategies for Colorectal Cancer John L. Marshall, MD Chief,...
57
Clinical Review of Current Treatment Strategies for Colorectal Cancer John L. Marshall, MD John L. Marshall, MD Chief, Division Hematology and Oncology Chief, Division Hematology and Oncology Director, Developmental Therapeutics and GI Oncology Director, Developmental Therapeutics and GI Oncology Lombardi Cancer Center Lombardi Cancer Center Georgetown University Georgetown University Washington, DC Washington, DC Oncology Journal Club
-
Upload
frank-green -
Category
Documents
-
view
216 -
download
1
Transcript of Clinical Review of Current Treatment Strategies for Colorectal Cancer John L. Marshall, MD Chief,...

Clinical Review of Current Treatment Strategies for Colorectal Cancer
John L. Marshall, MDJohn L. Marshall, MDChief, Division Hematology and OncologyChief, Division Hematology and Oncology
Director, Developmental Therapeutics and GI OncologyDirector, Developmental Therapeutics and GI Oncology
Lombardi Cancer CenterLombardi Cancer Center
Georgetown UniversityGeorgetown University
Washington, DCWashington, DC
Oncology Journal Club

Management of mCRC: An Evolving Treatment Algorithm
Diagnosis of mCRC
Resectable Unresectable
Adjuvant therapy
Surgery
Neo-adjuvant/Pre-operative
therapy
First-line
Second-line
Third-line
Borderline/PotentiallyResectable
Fourth-line
Treatment continuum

Advances in the Treatment of Colorectal Cancer
1980 1985 1990 1995 2000 2005
Therapeutic concepts
Palliative chemotherapy
Adjuvant chemotherapy
Neoadjuvant chemotherapy
Capecitabine
Oxaliplatin
Cetuximab
Bevacizumab
Irinotecan
5-FU
PanitumumabTargeted Therapies {

News from ASCO 2008
• EGFR/KRAS: Colon Cancer is split in two
– Trials close to re-tool
• MSI-H: Colon Cancer is split again?
– 5-FU harmful in adjuvant setting
• VEGF/EGFR: Dual inhibition may be bad
– PACCE
– CAIRO-2

Management of mCRC: An Evolving Treatment Algorithm
Diagnosis of mCRC
Resectable Unresectable
Adjuvant therapy
Surgery
Neo-adjuvant/Pre-operative
therapy
First-line
Second-line
Third-line
Borderline/PotentiallyResectable
Fourth-line
Treatment continuum

NCCN Guidelines: Advanced mCRC
NCCN Clinical Practice Guidelines in Oncology. Colon Cancer. v2.2007.
Good Tolerance to Intensive Therapy
Poor Tolerance to Intensive Therapy
First-line Second-line Third- or Fourth-line
FOLFOX + BEV or
CapeOx + BEV
FOLFIRI + BEV
5-FU/LV + BEV
Cape ± BEV or5-FU + LV ± BEV
FOLFIRI orIrinotecan
FOLFIRI + cetuximab orCetuximab + irinotecan
FOLFOX or CapeOx
Cetuximab or panitumumab or cetuximab + irinotecan
Improvement in functional status
No improvement in functional status
Cetuximab or panitumumab
or cetuximab + irinotecan
Cetuximab or panitumumab
or cetuximab + irinotecan
Cetuximab or panitumumab
or cetuximab + irinotecan
Clinical trial or best supportive care
FOLFOX or CapeOx
FOLFOX or CapeOx
Irinotecan or FOLFIRI
Irinotecan
Best supportive care
Therapy after first progression as above

Camptosar: 180 mg/mCamptosar: 180 mg/m22 D 1 q 2wk D 1 q 2wkLV: 400 mg/mLV: 400 mg/m22 over 2hr D 1 q 2 wk over 2hr D 1 q 2 wk5-FU: 400 mg/m5-FU: 400 mg/m22 (bolus) D1 q 2 wk (bolus) D1 q 2 wk5-FU: 2,400 mg/m5-FU: 2,400 mg/m22 (46 hr infusion) (46 hr infusion)D 1 q 2 wkD 1 q 2 wk
Arm A – Camptosar + infusional
Camptosar:Camptosar: 125 mg/m 125 mg/m22
5-FU:5-FU:500 mg/m500 mg/m22
LV:LV: 20 mg/m 20 mg/m22 D 1, 8, q 3 wksD 1, 8, q 3 wks
Arm B – D1, D8 bolus
Camptosar: Camptosar: 250250 mg/mmg/m22 d1 q 3 wks d1 q 3 wksCapecitabine: 1,000 mg/mCapecitabine: 1,000 mg/m22 bid d1-14 q 3 wks bid d1-14 q 3 wks
Arm C - Campcape
RANDOMIZATION
Met
asta
tic D
isea
se
+ Celecoxib or Placebo
400 mg bid
+ Celecoxib or Placebo
400 mg bid
N = 900N = 900
BICC-C Trial
+ Bevacizumab
+ Bevacizumab

Period 1: Progression Free Survival Data thru March 1, 2006 (ITT)
RegimenMedian PFS
(Months)HR
(95% CI) P Value
FOLFIRI 7.6 -- --
mIFL 5.8 1.55(1.2, 2.0)
0.0009
CapeIRI 5.5 1.47(1.1, 1.9)
0.0049
00.10.20.30.40.50.60.70.80.9
1
0 5 10 15 20 25 30Months
Pro
port
ion
of P
FS
FOLFIRI
mIFL
CapeIRI

Period 2: Overall Survival Data Thru March 1, 2006 (ITT)
Regimen Median OS (Months) 1 Year HR
(95% CI) P Value
FOLFIRI+ BEV Not Reached 87% -- --
mIFL + BEV 18.7 61% 2.5(1.3,5.0)
0.01
00.10.20.30.40.50.60.70.80.9
1
0 5 10 15 20 25 30
Pro
port
ion
of P
atie
nts
Who
Sur
vive
d
Survival Time (months)
mIFL + bevacizumab
FOLFIRI + bevacizumab

Phase III Trial of XELOX vs. FOLFOX4 + Bevacizumab or Placebo in First-line mCRC
Study Design and Drugs
Protocol amended to 2x2 placebo-controlled design after bevacizumab Phase III data1 became available (N=1,401)
1Hurwitz H., et al. Proc ASCO 2003;22 (Abstract 3646)
XELOX + placebo N=350
FOLFOX4 + placebo N=351
XELOX + bevacizumab N=350
FOLFOX4 + bevacizumab N=350
XELOX N=317
FOLFOX4 N=317
Recruitment June 2003–May 2004 Recruitment Feb 2004–Feb 2005
Initial 2-arm open-label study (N=634)
OX = oxaliplatin; LV = leucovorin; BV = bevacizumab; PL = placebo; 5-FU = 5-fluorouracil
XELOX + bevacizumab/placebo: 21-day cycle
D1 D2 D15
Rest
Oral capecitabine 1,000 mg/m2 BID
BV or PL 7.5mg/kg IV 30–90 min
OX 130mg/m2
IV 2 h
D21
D1
FOLFOX4 + bevacizumab/placebo: 14-day cycleOX 85mg/m2
IV 2 hBV or PL5mg/kg IV 30–90 min
5-FU 600mg/m2 IV 22 h
5-FU 600mg/m2 IV 22 h
D2 D3
LV 200mg/m2 IV 2 h
LV 200mg/m2 IV 2 h
5-FU
400m
g/m
2
IV b
olu
s
5-FU
400m
g/m
2
IV b
olu
s
Cassidy et al. ESMO 2006. Oral PresentationCassidy et al. ESMO 2006. Oral Presentation

Roche Medical Affairs. All rights reserved.Roche Medical Affairs. All rights reserved.
Phase III Trial of XELOX vs. FOLFOX4 + Bevacizumab or Placebo in First-line mCRC
PFS XELOX Non-inferiority
FOLFOX/FOLFOX + placebo/FOLFOX + bevacizumab N = 1,017; 826 events XELOX/XELOX + placebo/XELOX + bevacizumab N = 1,017; 813 events
Primary Objective Achieved Based on ITTPrimary Objective Achieved Based on ITT
Cassidy et al. ESMO 2006. Oral PresentationCassidy et al. ESMO 2006. Oral Presentation

Roche Medical Affairs. All rights reservedRoche Medical Affairs. All rights reserved ..
FOLFOX + placebo/XELOX + placeboN = 701; 547 events FOLFOX + bevacizumab/XELOX+bevacizumabN = 699; 513 events
HR = 0.83 [97.5% CI 0.72–0.95] (ITT)P = 0.0023
Primary Objective Achieved XELOX Subgroup FOLFOX SubgroupHR = 0.77 [97.5% CI 0.63–0.94] (ITT)
P = 0.0026
XELOX + placeboN = 350; 270 events XELOX + bevacizumabN = 350; 258 events
HR = 0.89 [97.5% CI 0.73–1.08] (ITT)P = 0.1871
FOLFOX + placeboN = 351; 277 events FOLFOX + bevacizumabN = 349; 255 events
Phase III Trial of XELOX vs. FOLFOX4 + Bevacizumab or Placebo in First-line mCRC
PFS Superiority of Bevacizumab + CT
Cassidy et al. ESMO 2006. Oral PresentationCassidy et al. ESMO 2006. Oral Presentation

ASCO 2007, Abstract 4013
Final Results of OPTIMOX-2 - A Large Randomized Phase II Study of Maintenance
Therapy or Chemotherapy-free Intervals (CFI) After FOLFOX in Patients with Metastatic Colorectal Cancer (Mrc):
A GERCOR Study
Maindrault-Goebel F, et al.

OPTIMOX Studies
OPTIMOX-1: Maintenance therapy
(N = 620)
FOLFOX 4 until progression
FOLFOX 7 FOLFOX 7
sLV5FU2
OPTIMOX-2: Chemotherapy-free interval
(N = 202)
mFOLFOX 7 mFOLFOX 7
sLV5FU2
mFOLFOX 7 mFOLFOX 7
Chemotherapy-free interval
Tournigand et al. J Clin Oncol. 2006;24:394.Maindrault-Goebel et al. ASCO 2007. Abstract 4013.

Progression-free Survival
0 10 20 30 40 50 60 70 80 90 1000.0
0.2
0.4
0.6
0.8
1.0
OPTIMOX1 median 36 weeks
OPTIMOX2 median 29 weeks
Weeks
Pro
babi
lity
P = 0.08

Overall Survival
0 10 20 30 40 500.0
0.2
0.4
0.6
0.8
1.0
OPTIMOX1 median 26 months
OPTIMOX2 median 19 months
P = 0.0549
Months
Pro
babi
lity

Intermittent Oxaliplatin (Oxali) Administrationand Time-to-Treatment-Failure (TTF) in
Metastatic Colorectal Cancer (mCRC): Final Results of the Phase III CONcePT Trial
Grothey A., et al.
ASCO 2008, Abstract 4010

CONcePT Trial Design
Grothey A, et al. ASCO 2008. Abstract 4010.
*Treat to failure. †8 cycles with oxaliplatin, 8 cycles without oxaliplatin, 8 cycles with oxaliplatin.
Patients with mCRC
(N = 140)
Continuous Oxaliplatin*mFOLFOX7 + bevacizumab +placebo
(N = 34)
Continuous Oxaliplatin*mFOLFOX7 + bevacizumab +Ca2+/Mg2+
(N = 35)
Intermittent Oxaliplatin†
mFOLFOX7 + bevacizumab + placebo
(N = 36)
Intermittent Oxaliplatin†
mFOLFOX7 + bevacizumab + Ca2+/Mg2+
(N = 35)

CONcePT: Kaplan-Meier Estimate of TTFP
ropo
rtio
n of
Pat
ient
s
0.00.10.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17Months
N at riskCO: 68 63 58 46 36 28 20 11 6 4 4 4 2 2 1 1 0
IO: 71 65 61 56 52 43 32 28 21 18 12 12 10 7 4 1 1
TTF(mos)
95% CI
COIO
4.25.6
3.7–5.54.7–7.0
Unstratified(IO relative to CO), P = .002*
Stratified by CaMg(IO relative to CO), P = .003*
* Log rank test
Continuous Oxaliplatin (CO)
Intermittent Oxaliplatin (IO)
Censored data
Grothey A, et al. ASCO 2008. Abstract 4010.

CONcePT: Kaplan-Meier Estimate of PFS
Grothey A, et al. ASCO 2008. Abstract 4010.
0.00.10.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Pro
port
ion
of P
atie
nts
1.0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17Months
N at riskCO: 68 64 46 39 29 24 13 7 3 3 3 1 0 0 0 0 0
IO: 71 64 55 51 43 38 27 24 18 15 10 9 8 3 2 1 1
Unstratified (IO relative to CO), P = .044*
Stratified by CaMg (IO relative to CO), P = .030*
* Log rank test
CO
PFS(mos)
95% CI
IO7.312.0
6.9–NE8.2–NE
Continuous Oxaliplatin (CO)
Intermittent Oxaliplatin (IO)
Censored data

ASCO 2007, Abstract 4000
Randomized Phase III Study of Irinotecan and 5-FU/FA With or Without Cetuximab in the First-
line Treatment of Patients with Metastatic Colorectal Cancer (mCRC): The CRYSTAL Trial
Van Cutsem E, et al.

Irinotecan and 5-FU/FA ± CetuximabThe CRYSTAL Trial
Van Cutsem E, et al. ASCO 2007. Abstract 4000.
Stratification factors:
• Regions
• ECOG PS
Populations
• Randomized patients: N = 1,217
• Safety population: N = 1,202
• ITT population: N = 1,198
Study DesignStudy Design
Cetuximab + FOLFIRICetuximab IV 400 mg/m2 on day 1,
then 250 mg/m2 weekly+ irinotecan (180 mg/m2)
+ 5-FU (400 mg/m2 bolus + 2400 mg/m2 as 46-hr continuous infusion)
+ FA every 2 weeks
FOLFIRIIrinotecan (180 mg/m2)
+ 5-FU (400 mg/m2 bolus + 2400 mg/m2 as 46-hr
continuous infusion)+ FA every 2 weeks
RR
EGFR-expressingMetastatic CRC

CRYSTAL TrialProgression Free Survival
Van Cutsem E, et al. ASCO 2007. Abstract 4000.

What is the Role of the Epidermal Growth Factor Receptor (EGFR) in Cancer?
Proliferation MetastasisAngiogenesisApoptosis Resistance
Shc
PI3-K
RafMEKK-1
MEKMKK-7
JNKERK
Ras
mTOR
Grb2
AKT
Sos-1
Cell Membrane
EGFR
Signaling Proteins
Cell Response to
Signaling

A. Friedman and N. Perrimon, Cell 128, January 26, 2007
Pathway vs. Network SignalingPathway vs. Network Signaling
Network “Chaotic”Pathway “Newtonian”

ASCO 2008, Abstract 2
KRAS Status and Efficacy in the First-line Treatment of Patients with Metastatic
Colorectal Cancer (mCRC) Treated with FOLFIRI With or Without Cetuximab: The
CRYSTAL Experience
Van Cutsem E, et al.

CRYSTAL PFS in Patients with KRAS Wild-type
Van Cutsem E, et al. ASCO 2008. Abstract 2. Reproduced with permission.
0.0
0.2
0.4
0.6
0.8
1.0
0 4 8 12
Months
PF
S E
stim
ate
18
Cetuximab + FOLFIRI
FOLFIRI
KRAS wild-type (N = 348) HR = 0.68: P = .017
2 6 10 14
Median PFS Cetuximab + FOLIFIRI: 9.9 months
Median PFS FOLIFIRI: 8.7 months
0.1
0.3
0.5
0.7
0.9
16
1-year PFS rate: 43%
1-year PFS rate: 25%

Relating KRAS Status to EfficacyProgression Free Survival
Cetuximab + FOLFIRI HR = 0.63; P = 0.007 mPFS wild-type (N = 172): 9.9 monthsmPFS mutant (N = 105): 7.6 months
FOLFIRI HR = 0.97; P = 0.87 mPFS wild-type (N = 176): 8.7 months
mPFS mutant (N = 87): 8.1 months
0.5
1.0
0.4
0.3
0.2
0.1
0.0
0.6
0.7
0.8
0.9
80 2 4 6 10 16
PF
S E
stim
ate
Months
Cetuximab +FOLFIRI wild-type
Cetuximab +FOLFIRI mutant
12 14
0.5
1.0
0.4
0.3
0.2
0.1
0.0
0.6
0.7
0.8
0.9
Months
FOLFIRI wild-type
FOLFIRI mutant
80 2 4 6 10 1612 14

ASCO 2008, Abstract 4000
KRAS Status and Efficacy of First-line Treatment of Patients with Metastatic Colorectal Cancer
(mCRC) with FOLFOX With or Without Cetuximab: The OPUS Experience
Bokemeyer C. et al.

1Bokemeyer C. et al, ASCO 2008. Abstract 4000.
Res
pons
e ra
te (
%)
59
37
0
10
20
30
40
50
60
70
CRYSTAL(N = 540)
OPUS1
(N = 233)
43
61
FOLFIRI FOLFOXCetuximab + FOLFIRI
Cetuximab + FOLF0X
CRYSTAL - KRAS wild-type: HR = 0.68
P = 0.017
32% risk reductionfor progression
OPUS - KRAS wild-type: HR = 0.57
P = 0.016
43% risk reductionfor progression
0.00.10.20.30.40.50.60.70.80.91.0
0 2 4 6 8 10 12 14 16 18
Months
PF
S e
stim
ate
0.00.10.20.30.40.50.60.70.80.91.0
0 2 4 6 8 10 12
Months
PF
S e
stim
ate
Cetuximab + CT in KRAS Wild-Type: Data Consistency

ECCO 2007, Abstract 0007
Amado RG, et al.
Analysis of KRAS Mutations in Patients with Metastatic Colorectal Cancer Receiving
Panitumumab Monotherapy

KRAS as a Biomarker for Panitumumab Response in mCRC
Amado RG, et al. ECCO 2007. Abstract 0007.
• Pts with mutant KRAS receiving panitumumab had 0% RR and SD similar to BSC alone (12% vs 8%)
• PFS log HR significantly different depending on K-ras status (P < .0001)• Percentage decrease in target lesion greater in patients with wild-type KRAS receiving
panitumumab
Patients With Mutant KRAS
Meanin Wks
Stratified log rank test: P < .0001
115/124 (93)
Patients With Wild-type KRAS
1.0
0.9
Pro
po
rtio
n W
ith P
FS 0.8
0.70.60.50.4
0.3
0.20.1
00 2 4 6 8 10
Events/N (%)Medianin Wks
Pmab + BSCBSC alone
114/119 (96)
12.37.3
19.09.3
HR: 0.45 (95% CI: 0.34-0.59)
12 14 16 18 20 22 24 26 28 30 32 3436 38 4042 44 46 48 50 52
Weeks
Pro
po
rtio
n W
ith P
FS
1.0
0.90.8
0.70.60.50.4
0.30.20.1
00 2 4 6 8 10 12 14 16 18 20 22 24 26 2830 32 3436 38 4042 44 46 48 50
Weeks
Pmab + BSCBSC alone Mean
in Wks
76/84 (90)
Events/N (%)Medianin Wks
95/100 (95)
7.47.3
9.910.2
HR: 0.99 (95% CI: 0.73-1.36)
52

Q: Is More Always Better?

Correlation Between Survival and Percentage of Patients Receiving Three Drugs in
Phase III Trials
.Grothey A, et al. J Clin Oncol. 2005;23:9441-9442.
12
13
14
15
16
17
18
19
20
21
22
0 10 20 30 40 50 60 70 80
Patients with three drugs (%)
Me
dia
n O
S (
mo
nth
s)
3 Drugs: 5-FU/LV, irinotecan, oxaliplatin

FOLFOXIRI vs. FOLFIRI
JCO 2007

Open-label, Phase II-III Trial of Irinotecan or Oxaliplatin-based CTX + Bevacizumab ±
Panitumumab in First-line mCRC: PACCE Trial
aThe choice of either Ox/CTX or Irino/CTX was at the oncologist’s discretion
• Discontinued 3/2007 due to significantly inferior PFS
in planned interim analysis
• OS significantly inferior in unplanned analysis
• ECOG score• Prior adjuvant TX• Disease site• Oxaliplatin doses/
Irinotecan regimen• Number of
metastatic organs
Oxaliplatin-based CTXa
Irinotecan-based CTXa
Oxaliplatin/CTX +Bevacizumab + Panitumumab
N = 407
Oxaliplatin/CTX +Bevacizumab
N = 405
Irinotecan/CTX +Bevacizumab +Panitumumab
N = 68
Irinotecan/CTX +Bevacizumab
N = 67
Phase III
Phase II
RANDOMIZATION
Hecht et al. World Congress on GI Cancer, 2007

ECCO 2007, Abstract 3000
Tol J, et al.
Randomised Phase III Study of Capecitabine, Oxaliplatin and Bevacizumab (CAPOXB) With or Without Cetuximab in Advanced Colorectal
Cancer (ACC), The CAIRO-2 Study of the Dutch Colorectal Cancer Group (DCCG)
an Interim Safety Analysis

Dutch Colorectal Cancer Group (DCCG)
Arm A Arm B
Randomization
CapecitabineOxaliplatin
Bevacizumab
CapecitabineOxaliplatin
BevacizumabCetuximab
CAIRO-2 Study Design

Adverse Event, %
Arm A:
Capecitabine, Oxaliplatin, Bevacizumab
(N = 197)
Arm B:
Capecitabine, Oxaliplatin, Bevacizumab, Cetuximab
(N= 192)
Gastrointestinal, grade 3/4
Diarrhea 20 23
Nausea 9 6
Vomiting 8 6
Cardiovascular, grade 3/4
Hypertension 7 4
Thromboembolic event 9 9
Grade 3/4 neurotoxicity 8 6
Grade 3/4 allergic reaction
3 7
Grade 3/4 bleeding 2 1
Tol J, et al. ECCO 2007. Abstract 3000.
CAIRO-2Interim Safety Analysis

Progression-free Survival
Dutch Colorectal Cancer Group (DCCG)
Arm A (without cetuximab) 10.7 months (9.7-12.5) Arm B (with cetuximab) 9.6 months (8.5-10.7)
HR: 1.21
P = 0.018
0 6 12 18 24 30
Months from randomization
0.0
0.2
0.4
0.6
0.8
1.0
Pro
gre
ssio
n f
ree
surv
ival
pro
bab
ility
Arm A (without cetuximab)
Arm B (with cetuximab)

Wildtype
N = 305 (61%)
Mutation
N = 196 (39%)P value
Arm A 152 (50%) 103 (53%)
Arm B 153 (50%) 93 (47%)
Median PFS (months)
Arm A 10.7 12.5 0.92
Arm B 10.5 8.6 0.47
P value 0.10 0.043
KRAS Genotyping (N = 501)
Dutch Colorectal Cancer Group (DCCG)

CALGB/Intergroup Front-line Trial
FOLFOX or
FOLFIRI
Bevacizumab
Cetuximab
Bevacizumab/Cetuximab

Adjuvant Oxaliplatin Mosaic Trial (3-year Data)
FOLFOX-4 (1,100 pts)
LV5FU2 (1,100 pts)
T3, T4 N0 = 40% (87% vs 84%)
Tx, N1, N2 = 60% (72% vs 65%)
77.8%
72.9%
P < 0.01
RANDOMIZATION
DFS Endpoint

Overall Survival: ITT
Data cut-off: January 2007
Overall survival (months)
FOLFOX4
LV5FU2
Pro
babi
lity
1.0
0.8
0.6
0.4
0.2
0
0.9
0.7
0.5
0.3
0.1
0 6 12 18 24 6030 36 42 48 54 66 9672 78 84 90
Events
FOLFOX4 243/1123 (21.6%)
LV5FU2 279/1123 (24.8%)
HR [95% CI]: 0.85 [0.72–1.01]
2.6%
P = 0.057

Overall SurvivalStage II and III
Data cut-off: January 2007
FOLFOX4 stage II
LV5FU2 stage II
FOLFOX4 stage III
LV5FU2 stage III
Overall survival (months)
Pro
babi
lity
1.0
0.8
0.6
0.4
0.2
0
0.9
0.7
0.5
0.3
0.1
0 6 12 18 24 6030 36 42 48 54 66 9672 78 84 90
HR [95% CI]
Stage II 1.00 [0.71–1.42]
Stage III 0.80 [0.66–0.98]
0.1%
4.4%
P = 0.996
P = 0.029

ASCO 2008 Abstract LBA4005
Wolmark N, et al.
A Phase III Trial Comparing FULV to FULV + Oxaliplatin in Stage II or III Carcinoma of
The Colon: Survival Results of NSABP Protocol C-07

Survival Results of NSABP C-07
Wolmark N, et al. ASCO 2008. Abstract LBA4005.
FULV5-FU 500 m2 IV bolus weekly x 6; LV 500 mg/m2 IV weekly x 6, each
8-week cycle x 3 (N = 1,209)
FLOX FULV + oxaliplatin 85 mg/m2 IV on Weeks 1, 3, and 5 of each 8-week
cycle x 3(N = 1,200)
Patients with stage II or III carcinoma of the colon
stratified by number of positive lymph nodes
N = 2,409
Primary endpoint: DFS

C-07: Disease-Free Survival
Wolmark N, et al. ASCO 2008. Abstract LBA4005.
0
20
40
60
80
100
0 2 4 6
3-years 5-years
1 3 5 7
10
30
50
70
90
P = .002 HR: 0.81 [0.70-0.93]FLOX 76.1% 69.4%
FULV 71.5% 64.2%
∆ 4.6% 5.2%
FLOX (N = 1,200)
FULV (N = 1,209)
Years
Pro
port
ion
of P
atie
nts
(%)

C-07: Overall Survival
Wolmark N, et al. ASCO 2008. Abstract LBA4005.
0
20
40
60
80
100
0 2 4 6
D(n) 3y 5y
1 3 5 7
10
30
50
70
90
FLOX 259 80.3% 77.7%
FULV 301 78.3% 73.5%
∆ 42 2.0% 4.2%
P = .06
HR: 0.85 [0.72-1.01]
FLOX (N = 1,200)
FULV (N = 1,209)
Years
Pro
port
ion
of P
atie
nts
(%)

C-07: Overall Survival Hazard Ratios
Wolmark N, et al. ASCO 2008. Abstract LBA4005.
FLOX Better FULV Better
0.5 0.75 1 1.25 1.5 1.75
Overall
< 65 yr
≥ 65 yr
Stage II
Stage III

Confirmation of Deficient Mismatch Repair (Dmmr) as a Predictive Marker for Lack of Benefit from 5-FU Based Chemotherapy in
Stage II and III Colon Cancer (CC): A Pooled Molecular Reanalysis of Randomized
Chemotherapy Trials
ASCO 2008 Abstract 4008
Sargent D. J., et al.

MSI-H and Adjuvant 5-FUSargent, ASCO 2008

MSI-H and Adjuvant 5FUSargent, ASCO 2008

Accrual goal: 3,125
E5202: Stage II Colon Cancer
mFOLFOX6 vs.
mFOLFOX6 +bevacizumab qow
Tumor block risk assessed based on biology
(18q/MSI)
High risk (MSS and 18q LOH)
Low risk (MSI + or no
loss 18q) Observation
Surgery

Where We Are Today
AdjuvantAdjuvant
5-FU/LV
FOLFOX
Capecitabine
First-lineFirst-line
5-FU/LV
CPT-11
Oxaliplatin
Capecitabine
Bevacizumab
Second-lineSecond-line
5-FU/LV
Oxaliplatin
CPT-11
Capecitabine
Bevacizumab
Cetuximab
Third-lineThird-line
Cetuximab/CPT-11
Panitumumab

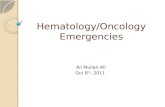
Colon Cancer is More than One Disease
KRAS Wild Type KRAS mutant
MSI-High MSS
+ EGFR Agents – EGFR Agents
? No 5-FU
50-60% 40-50%
15-20% 80-85%

Clinical Review of Current Treatment Strategies for Colorectal Cancer
Closing CommentsClosing Comments
Oncology Journal Club