Clinical research: the potential of practice development
10
Click here to load reader
-
Upload
mary-fitzgerald -
Category
Documents
-
view
215 -
download
1
Transcript of Clinical research: the potential of practice development

150 PRACTICE DEVELOPMENT IN HEALTH CARE4(3): 150–159 (2005) DOI: 10.1002/pdh.10
Copyright © 2005 John Wiley & Sons, Ltd. 4(3): 150–159 (2005)
150
Introduction
Through an inductive process of analysing thework of practice developers reported in the liter-ature and interviews with nurses with practicedevelopment roles, Garbett and McCormack,(2002: 87) define practice development (PD) as:
‘a continuous process of improvement
designed to promote increased effectiveness in
patient-centred care. It is brought about by
enabling health care teams to develop their
knowledge and skills and in doing so, transform
the culture and context of care. It is enabled and
supported by facilitators who are committed to
systematic, rigorous and continuous processes
of change that will free practitioners to act in
new ways that better reflect the perspectives of
both service users and service providers.’
Practice development has been thelaunching pad of nursing initiatives such as‘New nursing’ described by Salvage (1990),
and those associated with the NursingDevelopment Units in the UK and Australia(Pearson, 1983, 1997; Wright, 1991;Greenwood, 1999; FitzGerald and Solman2003). Furthermore, PD has much in commonwith the work of the Magnet Hospitals in theUSA (Aiken et al., 2000). Both have anemphasis on person-centred care and profes-sional team building. It is this latter link thathas caught the attention of funding bodies inthe current climate of acute staff shortages.This is mainly because PD, like the work of theMagnet Hospitals, is seen to improve satisfac-tion with and commitment to professionalhealth service, thereby having the potential toincrease retention rates. It is also beingendorsed by university staff as a positive pursuitthat engages academics with practice providingopportunities for research, consultancy andclinical roles for academics.
This paper is based on preliminary workdone by a team of practice developers in onearea health service in New South Wales,
Clinical research: The potential of practice development
Mary FitzGerald—Professor of Nursing, James Cook University, Queensland, AustraliaDeborah Armitage—Clinical Nurse Consultant, Northern Sydney Central Coast Health,NSW, Australia
Abstract: Research and development are strategic initiatives that, when built into modern practice set-tings, help to create a culture in which people have the potential to promote best practice. It is argued thatthe potential of practice development (PD) as a means of researching contemporary clinical practice islargely underestimated by mainstream scientists. PD, as part of a research design, is discussed in detail fromthe perspectives of research in the critical paradigm, participatory world views and action research.Fundamental components of PD such as facilitation, team building, practice projects and ethical comport-ment within a structure of a research design or proposal are discussed and examples from current studies aregiven. Copyright © 2005 John Wiley & Sons, Ltd.
Key words: practice development, action research, critical social theory
RESEARCH AND REVIEW?
PDHC 4.3 crc 30/9/05 2:46 pm Page 150

Copyright © 2005 John Wiley & Sons, Ltd. 4(3): 150–159 (2005)
Clinical research: The potential of practice development 151151
Australia. The practice development teamchose to create research teams, write formalproposals and pursue competitive researchfunding. In doing this we have attempted topersuade the scientific community that this isa bone fide research endeavour. The researchdesign included the elements of PD describedby Garbett and McCormack (2001) andaction research typically incorporating thecollection of qualitative and quantitative data(Hart and Bond, 1995; Winter and Munn-Giddings, 2001). Furthermore it is plannedthat discrete PD projects in the area healthservice will be linked in order to strengthenthe power of statistical results in the evalua-tion of PD as a strategy.
Background
In the 1980s practice development (PD) wasadopted widely in Oxfordshire, UK, as a practi-cal means of supporting patient-focused profes-sional practice. Pearson researched during thistime as did Binnie and Titchen and FitzGeraldusing action research designs to frame develop-ments (Pearson, 1983, 1988, 1992; FitzGerald,1986; Binnie and Titchen, 1999). With theexception of the work in the Burford and Oxforddevelopment units, results of PD were used tomaintain local support and inform further devel-opment on site. They did not lead to researchfunding nor were the results deemed to be gener-alizable. The majority of the work remained inthe practical local domain and was aligned toquality improvement rather than traditionalresearch.
The tide turned when the King’s Fund sup-ported PD through nursing development units.Most of these units employed researchers toevaluate developments. However, the evalua-tion of change inherent in practice develop-ment is small scale and does not generateknowledge that is generally accepted as con-tributing to disciplinary knowledge; a hallmarkof research that Unsworth (2000) points out ismissing from PD. This is a perceived weaknessthat should be addressed by practice developerswho want to compete for research funding.
However it should also be acknowledged thatusing ‘before and after’ studies in a traditionalway to measure the effectiveness of an inter-vention detracts from the primary means ofknowledge generation in action research andpractice development which is critical reflec-tion on and in action.
Researchers from the Royal College ofNursing Institute have developed the earlywork done in Oxfordshire doing much to refinethe techniques employed by developers and toanalyse successful PD (Titchen, 1998; Ward etal., 1998; McCormack et al., 1999;McCormack and Wright, 1999; Garbett andMcCormack, 2001, 2002; McCormack, 2001,2003). They continue to consult widely andadvise on practice development initiatives.Despite progress, Kitson and Currie (1996)reported on a survey of nurses in four districthealth authorities in the UK (141 responses).They found that PD was still predominantlysmall scale, unfunded, with little or no researchsupervision and that there were few reports onmeasurable outcomes.
PD is a systematic process resultingin the generation of knowledge andunderstanding … derived from botha critique of the processes of PD asenacted and measures ofpatient/client benefit as a result ofchange implemented in PD.
Clarke and Procter (1999) discussed prac-tice development and research and describedthe ambiguities inherent in traditional viewsof practice and research. They conclude thatexcluding PD from research may result in afailure to pursue practical questions throughresearch. They wrote, ‘the issues which aretruly problematic in patient care will fail to beaddressed because they are messy, invisible andnot researchable’ (1999: 981). We would arguethat, typically, PD is perceived by traditionalscientists as reliant on small-scale ‘before-and-after’ studies to evaluate progress rather than
PDHC 4.3 crc 30/9/05 2:46 pm Page 151

as a systematic process of knowledge genera-tion through action. Findings from internalchange processes are informative and entirelyconsistent with action research methodologybut to date they are not recognized as usefulbeyond the local situation. However we wouldargue from experience that experimental stud-ies are not suited to solving the types of com-plex problems found in contemporary healthservice environments. Setting up trials wherethe aim is to control what is normally uncon-trollable is counter-productive in a healthservice fraught with moral, social, physical,economic and cultural problems.
Bearing in mind the central significance toPD of person-centred care (Garbett andMcCormack, 2001, 2002; Gerrish, 2001), out-comes that gauge improvements for patientsshould be paramount even though they arenotoriously difficult to capture. One strategyfor PD to maintain momentum and achievegreater sophistication in terms of knowledgegeneration and disciplinary influence is forfacilitators to pay increased attention to it as aresearch methodology. That is, to reinforcethat PD is a systematic process resulting in thegeneration of knowledge and understanding.This knowledge is derived from both a critiqueof the processes of PD as enacted and measuresof patient/client benefit as a result of changeimplemented in PD.
Methodology
PD research is classically situated in the criticalparadigm in as much as it is openly political anddesigned to result in change (Denzin andLincoln, 1994). Garbett and McCormack iden-tify the critical social science (CSS) perspectiveas the philosophical base for PD, making it acongruent partner with action research (Carrand Kemmis, 1986; Binnie and Titchen, 1999;Kennedy, 2001; Dewing and Traynor, 2005).Action researchers, like practice developers,emphasize ‘the value of insights derived frompractical involvement in a situation, rather thanthe contribution of supposedly “objective” meth-ods applied by outsiders’ (Winter and Munn-
Giddings, 2001: 7). Action research is a socialscience methodology wherein knowledge is gen-erated from the data that emerge from change inpractice. It is defined by Winter and Munn-Giddings (2001: 8) as:
‘the study of a social situation carried out by
those involved in that situation in order to
improve both their practice and the quality of
their understanding.’
The participative nature of action researchhas been developed by a range of actionresearchers and promoted as a ‘participatoryworld view’ by Reason and Bradbury (2001).Park (2001: 81), in a contemporary discussion ofthe forms of knowledge that are inherent in par-ticipatory action-oriented research, first estab-lishes three activities in action research, namely:
‘inquiring into the nature of the problem to
solve by understanding its causes and mean-
ings; getting together by organizing themselves
as community units; and mobilizing themselves
for action by raising their awareness of what
should be done on moral and political grounds.’
These activities, Park (2001: 82–7) goeson to argue, require ‘representational knowl-edge’ (functional and interpretive subtypes)that draws on conventional empirical andinterpretive research; ‘relational knowledge’ a‘knowing that resides in the act of relating andshows itself in words, expressions, actions andother forms of doing relationship’; and ‘reflec-tive knowledge’ that is critical reflection byactors in order to bring about change.
The first phase of the PD research project isusually the establishment of a team of develop-ers/co-researchers and a critique of the statusquo. The critique (stimulated by questions suchas, What is happening here? What are we want-ing/trying to achieve? Who are the key players?Who benefits from the current situation? Whois disadvantaged?) is fundamental to both theenlightenment and consequent empowermentand emancipation of the team. Establishingcommon values and revealing dominant influ-
152 FitzGerald and Armitage
Copyright © 2005 John Wiley & Sons, Ltd. 4(3): 150–159 (2005)
152
PDHC 4.3 crc 30/9/05 2:46 pm Page 152

ences that impact on the team is a part of thestudy that should not be hurried. There is atemptation to hasten this phase in order to geton with the ‘real research’ and thus unwittinglyundermine the importance of the growth of theteam as co-researchers and practice developers.This phase of PD FitzGerald and Solman (2003)warn is something that may be missed by teamswho retrospectively claim PD status for a seriesof clinical projects. It is also the important firstphase in action research cycles (Carr andKemmis, 1986; Hart and Bond, 1995; Winterand Munn-Giddings, 2001).
Research design
By the ‘design’ of a study we mean the overallplan or strategy to complete the study andanswer the research question. It should be possi-ble to assess the likelihood of any researchstudy’s success by the congruence between thequestion asked and the methods employed tocollect and analyse data (Brink and Wood 2001:101). There is immediately a problem with PDin that it is rare that one question is asked orone problem stated at the proposal stage. Indeedthe complexity of the social situation meansthere will be more than one problem and that
the problems to be addressed are identified asthe team develops. This is an issue that is inte-gral to the very nature of action research andhas been addressed by action researchers innumerous forums (Binnie and Titchen, 1999;Winter and Munn-Giddings, 2001).
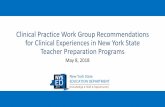
Within a PD project we have chosen toidentify an overarching study of team buildingand professional practice with several smallerpractice projects embedded in the study (seeFigure 1). It is possible to ask a broad question atthe beginning of the research bearing in mindthat specific sub-problems or questions will bedeveloped by the team as the research progress-es and that each new research question or prob-lem will constitute a discrete but integral part ofthe project. In a recent study the research ques-tion posed in the first proposal was:
● What processes will a group of nurses use inorder to review their practice and imple-ment change?
● Is it possible to achieve significantimprovements in standards of patient careand nurses’ satisfaction with their profes-sional practice through the process of prac-tice development?
Copyright © 2005 John Wiley & Sons, Ltd. 4(3): 150–159 (2005)
Clinical research: The potential of practice development 153153
CPD Project
Pre-test evaluation
Post-test evaluation
Critical so
cial theo
ry
Team b
uild
ing
Pro
fession
al practice
Ap
pro
ximately o
ne year
Knowledge-generatingaction research cycles
FIGURE 1: Practice development research design.
PDHC 4.3 crc 30/9/05 2:46 pm Page 153

Under the cover of CSS, actionresearchers may adopt reasonably flexiblemethods to conduct cycles of data collection,critique, planning, action, data collection andcritique, etc. (Carr and Kemmis, 1986; Hartand Bond, 1995; Winter and Munn-Giddings,2001). Knowledge is generated during the cri-tique or critical reflection phases of the cycles.
Figure 1 illustrates the study design withthe process of professional team building as thesuperstructure for the PD, discrete cyclicalclinical projects addressing clinical issues ofimportance to the team, and with due regardfor best available evidence to inform change.There is potential for other PD teams to collectthe same data, either in the teambuilding orthe smaller project work, and thereforeincrease the significance of statistical resultsand conclusions that can relate cause andeffect. However, in line with the principles ofparticipation and empowerment, this practiceis not mandated and only likely to work wherethere is an area health service-wide strategy forPD that is being evaluated (FitzGerald andSolman, 2003; Conway and FitzGerald, 2004).Examples of smaller projects within PD aregiven in the next section.
As research teams gain confidence throughthe experience of researching and sharing theirresults with other clinicians it is anticipatedthat the projects will gain in research sophisti-cation and become more influential. Influencewill depend on the transferability of the knowl-edge generated as judged by receivers of infor-mation and credibility of the action researchprocess. Hart and Bond (1995) suggest knowl-edge generated in action research may be usedto initiate another project or as a guide foradaptation in another area. Combining thedata from a number of projects, particularly inregard to consumer satisfaction and profession-al development of staff in PD areas, has thepotential to produce significant results that mayestablish the efficacy of PD as a professionalteam building process in conventional researchterms. However, it is a shame to concentratepurely on traditional evaluation rather than thedevelopment of disciplinary knowledge.
Action research has critics who liken itmore to a change process than theory building.However proponents (Winter and Munn-Giddings, 2001: 19) emphasize the generationof theory from the process of change:
‘The main purpose of action researchers … is
not only to improve their understanding of a sit-
uation with which they are already intensively
involved, but also to engage in an attempt to
change things … and to describe what is
learned from the change process as it occurs.’
This practical engagement means thatresearchers embrace the reality of a complexworld and the variables that confound so manyconventional clinical researchers. Such har-mony enables the action researcher and prac-tice developer to circumvent the tensiondescribed by Clarke and Procter (1999)between practice and research. Winter andMunn-Giddings (2001) argue that rather thandescribing a static situation, as researchers inthe interpretive and positivist paradigms,action researchers become involved and learnat the same time as changing a situation. Thispoint does not make the approach better but itdoes render it attractive to clinicians who aredaily confronted with issues that have a dualimperative to change and research. In the PDresearch proposals we aim to generate under-standing from change and also to evaluate thechange simultaneously.
Concrete examples
Examples from the work of four PD teams mayhelp to describe the components of the projects.Some of these developments may be described inthe initial proposal for funding. However, otherswould have evolved as a result of the teamworkand could not be predicted at the proposal stageof the project. How this evolving design is pre-sented to the ethics committee for approval isdealt with later.
Fundamental to action research and PD, isthe team’s ability to examine the current rou-tines, culture and knowledge that impact on
154 FitzGerald and Armitage
Copyright © 2005 John Wiley & Sons, Ltd. 4(3): 150–159 (2005)
154
PDHC 4.3 crc 30/9/05 2:46 pm Page 154

clinical practice. This reflection forms the firstphase of the PD project enabling discussion onvalues that should underpin patient care andleading to the formulation of each unit’s phi-losophy or values statement. Being idealistic(how practice ought to be) rather thandescriptive (how practice is), the philosophystatements allow for critique of the status quoand the identification of a number of issuesthat could potentially be addressed throughsmall action research cycles (FitzGerald et al.,2003). It was at this point that research fund-ing and ethics approval was sought.
Congruent with the participatory nature ofPD and action research, members of the PDteams were named in the proposals as co-researchers. While an overarching researchquestion was posed, it was clearly indicated inthe proposal that there would be continuousand inter-related research cycles within theproject and that specific issues would be pro-gressively identified and addressed at a laterstage. The method of data collection and analy-sis for each research cycle was determined bythe nature of the issue under investigation.
An example of one of the issues initiallychosen by a PD team centred on the need toimprove end-of-life care for people withdementia. Less than positive outcomes forthese patients were initially thought to be aresult of a lack of timely and appropriate med-ication prescribing. Following a period ofrecording and critiquing of incidents it was evi-dent that the timely prescribing and adminis-tration of medications was reliant on a numberof inter-related and interdependent factors.These included the need for patient advocacy,nurses’ confidence in their own clinical deci-sion making, communication skills, and nurses’and general practitioners’ knowledge. Theendpoint of this cascade was the need forimproved education and professional network-ing with specialized services.
To facilitate improvement the teamfocused firstly on addressing those issues thatwere within its province. Literature searcheswere conducted to gather evidence of contem-porary best practice in the management of
common end-of-life symptoms. This informa-tion formed the basis of education sessions runby and for the nurses and was collated as aresource manual for all staff. Improvements inknowledge were evaluated through pre- andpost-education surveys of staff, the results ofwhich were positive.
Contact was also made with the local pal-liative care service to ensure that the PD teamwas advocating clinical practice consistentwith that of the specialist service. This re-establishment of what had previously been astrong professional network allowed for clarifi-cation of roles and responsibilities in relationto the care of end-stage dementia patients andprovided an opportunity for a collaborativeapproach to problem solving that was botharea health service wide and contextual.
On critical reflection the increase in con-fidence in the nurses’ own clinical decisionmaking and their ability to act as patient advo-cate, subsequent to improved knowledge,empowered the PD team to engage in a multi-disciplinary review of end-of-life care.Meetings were held with the local generalpractitioners who worked as visiting medicalofficers (VMOs) in the unit. These meetingsprovided an avenue for addressing issues ofpatient care for both nurses and VMOs, manyof which were a consequence of the absence of24-hour on-site medical cover. Such open dis-cussion fostered an atmosphere of professionalrespect and collaboration and resulted in smallyet significant changes to processes that hadimpeded quality care provision. Improvementsin end-of-life care were evident almost imme-diately and long-term evaluation will monitorthe sustainability of these improvements.
This project was rewarded for its excel-lence at the area-wide quality awards. Theteam was commended for its sensitive atten-tion to this emotional issue and congratulatedfor the multidisciplinary involvement. Prizemoney from this award will be used to furtherthe PD efforts.
Another project, led by enrolled nurses,aimed at addressing concerns that long-termpatients often became withdrawn and suffered
Copyright © 2005 John Wiley & Sons, Ltd. 4(3): 150–159 (2005)
Clinical research: The potential of practice development 155155
PDHC 4.3 crc 30/9/05 2:46 pm Page 155

156 FitzGerald and Armitage
Copyright © 2005 John Wiley & Sons, Ltd. 4(3): 150–159 (2005)
156
a decrease in social skills as a result of theirextended admission period. Reflecting on cur-rent routines it was identified that many ofthese patients were returned to their roomearly each afternoon, remaining there until thefollowing morning. In addition many wereconfined to single rooms by the nature of theirillness or accommodated in shared wards withpatients who were unable to communicate.
Recognizing that meals were a social expe-rience, the enrolled nurses sought to restruc-ture the ward environment and routine prac-tices. Collaboration between patient care assis-tants and kitchen staff enabled the patientlounge to be rearranged each afternoon to cre-ate a dining room. Meal delivery routines weremodified and patients were assisted to come tothe dining room for the evening meal.
Before and after surveys of patients’ andnurses’ recorded observations showed anincrease in social interaction between thepatients, with some remaining in conversationfor up to two hours after the evening meal. Inaddition the dining room project increased thefrequency with which patients mobilized,potentially decreasing pressure ulcer develop-ment and deconditioning. The positive com-ments by the patients and improvements intheir demeanour indicated an improved quali-ty of life.
Evidence has shown that family carershave a major role to play in the planning ofcare for patients with dementia and can offerhealth professionals useful information andstrategies to manage the idiosyncrasies of indi-viduals. For some family carers, the admissionof the care recipient to hospital is also seen asa loss of control and a forced relinquishing oftheir carer role and expertise. One PD teamnominated improved involvement of familycarers of patients with dementia as a priority inimproving care. Inherent in addressing thisissue was the need to improve communicationbetween families and staff. To facilitate this thepractice of inviting family members to attend aformal interview and information exchangesession within the first few days of a patient’sadmission was adopted. This interview is con-
ducted by a senior registered nurse and thesocial worker and includes discussion onpatients’ and carers’ goals of care, patient inter-ests and families’ requests for continuing toprovide care. This has resulted in some familymembers choosing to assist staff with the prac-tical aspects of patient care, which promotes asense of self-efficacy at a time of potentialdespondency. Information obtained at the fam-ily interview guides all decisions for treatmentand care, ensuring a degree of autonomy forone of our most disenfranchised patient groups.
Evaluation of this cycle has been undertak-en by a survey on three levels – family carers,nursing and allied health staff, and visitingmedical officers (VMOs). Many family mem-bers have reported that, despite their relativeexperiencing numerous admissions to otherfacilities, this was the first time they had beengiven any chance for honest discussion aboutfuture care planning or prognosis or an oppor-tunity to assist in care provision. In additionfamilies consistently indicated this opportunityreassured them that their relative was beingtreated as a dignified individual. From thehealth professional perspective, all disciplineshave reported that the information obtainedduring the interview has improved the careplanning process, particularly for patients whodisplay challenging behaviours as a result oftheir disease. In addition the nursing staff andsocial workers report the interview and discus-sion aids the development of trust between staffand families, opening communication channelsfor the duration of the patient’s admission.
PD at its best involves radicalchange that endures and this is not achieved in a hurry. Too oftenPD loses momentum because toomuch is expected too quickly.
While PD remains a relatively new conceptfor some of the teams their progress in improv-ing the quality of patient care is transparent.Through the rigorous and systematic process ofPD teams have recognized the potential of cli-
PDHC 4.3 crc 30/9/05 2:46 pm Page 156

nicians to effect significant changes to currentpractices and processes in care provision. Thishas motivated ongoing endeavours to improve-ments in care that are increasingly becomingpart of an area-wide culture.
The potential for evidence to be generatedrises as the sophistication of the change cyclesdevelops. PD at its best involves radical changethat endures and this is not achieved in ahurry. Too often PD loses momentum becausetoo much is expected too quickly. The rigor ofthe process is dependent on realistic under-standing of progress and steady incrementalimplementation of plans with attendantreview, critique and modification.
Ethical comportment
PD projects are not routinely submitted to insti-tutional ethics committees (IEC). They aredeemed to be non-invasive and more alignedwith quality assurance than experimentation.However if they are proposed as research studiesthat involve the collection, analysis and inter-pretation of data and dissemination of resultsthat will influence practice they should be sub-jected to appraisal by an IEC. There is provisionin the Australian NH and MRC (2001) guide-lines for human research for this type of projectto be assessed with a degree of flexibility thataccommodates the intricacies of action research.In our proposal we emphasized the collaborativenature of the study and the co-operation of theteam as co-researchers rather than participantsor subjects.
The voluntary nature of involvement isimportant but should not be over-stated for thesake of gaining ethics committee approval.The early phase of the study is designed toallow the team to decide whether or not toembark on the development work.Contributions to data collection are entirelyvoluntary – whether that involves beingobserved, completing surveys or being inter-viewed. However, unlike other studies, it is notreasonable to withdraw from the study at anytime (i.e. when the team is engaged on anaction that is intended to improve standards of
care an individual nurse will create difficultyfor the team and patients by refusing to engagein the work without an explanation, or engag-ing with the team by discussing the problem).An example of this might be the introductionof a system for improving analgesic provisionfor patients receiving palliative care. Co-researchers are knowledgeable about theresearch – they have opportunities to attendPD meetings and written information is alwaysavailable in the form of minutes from meet-ings, communication books and handouts.Patients in a PD area are given informationabout the project and invited to ask questionsat any time, examples of these papers areappended to the proposal. As usual anyoneinvolved in the study is encouraged to expressany concerns about the study to the chair ofthe IEC or a senior member of staff.
Institutional ethics committees do have aremit to protect study participants from beinginvolved in futile research. Therefore the IECdoes have a responsibility to appraise themethodological quality of the study. Our IECnominates a supervisor for every project fromthe committee. As the PD study develops,information will be given to the IEC abouteach action research cycle planned and thedata collection instruments that will be used,together with descriptions of each instrument’sreliability and validity, bearing in mind, ofcourse, the purpose of the measurement.Recruitment of participants and informed con-sent remain constant, any deviation from theprotocol first proposed will be reported to theIEC and advice from the supervisor sought. Aswith other research studies progress reports aresubmitted regularly to the IEC.
Conclusion
Advocating for recognition of PD as bone fideresearch within an action research frameworkand within the critical paradigm has achievedmoderate success in the area health service todate with one PD team obtaining competitivefunding of $10,000 from the area health serviceand two teams receiving approval from the
Copyright © 2005 John Wiley & Sons, Ltd. 4(3): 150–159 (2005)
Clinical research: The potential of practice development 157157
PDHC 4.3 crc 30/9/05 2:46 pm Page 157

research ethics committee. Much has beenlearned locally from the action research cyclesand professional team building. As planned,knowledge to date is confined to unit level.Validity and reliability of information are judgedby the recipients of the knowledge rather thanclaimed by the researchers (Hart and Bond,1995; Winter and Munn-Giddings, 2001)
Following this early work there is now sub-stantial interest in PD and a number of otherareas are requesting support to initiate PD proj-ects. This is an obvious endorsement of thearea’s strategic plan for practice developmentin which research and leadership are integralcomponents (FitzGerald and Solman, 2003).
We argue that knowledge generated fromPD research should not be restricted to smallevaluations of incremental change. Rather it isa combination of the various sources ofenlightenment afforded by critical reflectionon experience during the process of changethrough PD initiatives and full use of opportu-nities for multi-site work and more conven-tional means of studying the effectiveness ofPD as an intervention. Formal research bodies(funding and ethics committees) need to beconstantly reminded that there are evolvingdefinitions of research by receiving proposalsfor review and applications for funding.
Acknowledgements
The support of Central Coast Health for thiswork is gratefully acknowedged.
References
Aiken L, Havens D, Sloane D (2000). The Magnet nurs-ing services recognition program: A comparison oftwo groups of Magnet groups. American Journal ofNursing 100: 26–36.
Binnie A, Titchen A (1999). Freedom to Practise: TheDevelopment of Patient-Centred Nursing. Oxford:Butterworth Heinemann.
Brink P, Wood M (2001). Basic Steps in PlanningNursing Research. From Question to Proposal (5thedn) Mississauga: Jones and Bartlett Publishers.
Carr W, Kemmis S (1986). Becoming Critical:Education, Knowledge and Action ResearchLondon: Falmer Press.
Clarke C, Procter S (1999). Practice development:Ambiguity in research and practice. Journal ofAdvanced Nursing 30(4): 975–82.
Conway J, FitzGerald M (2004). Processes, outcomes andevaluation: Challenges to practice development ingerontological nursing. International Journal ofOlder People Nursing 13(6b): 112–20.
Denzin N, Lincoln Y (1994). Handbook of QualitativeResearch. Thousand Oaks: Sage.
Dewing J, Traynor V (2005). Admiral nursing competen-cy project: Practice development and actionresearch. Journal of Clinical Nursing 14: 695–703.
FitzGerald M (1986). Lecturer Practitioner: ActionResearcher. Masters Thesis School of Nursing, TheUniversity of Wales, Cardiff.
FitzGerald M, Pearson A, Walsh K, Long L, Heinrich N(2003). Patterns of nursing: A review of nursing in alarge metropolitan hospital. Journal of ClinicalNursing 12(3): 326–32.
FitzGerald M, Solman A (2003). Clinical practice devel-opment in Central Coast Health. Collegian, 10(3):8–13.
Garbett R, McCormack B (2001). The experience ofpractice development: An exploratory telephoneinterview study. Journal of Clinical Nursing 10:94–102.
Garbett R, McCormack B (2002). A concept analysis ofpractice development. NT Research 7: 87–100.
Gerrish K (2001). A pluralistic evaluation ofnursing/practice development units. Journal ofClinical Nursing 10: 109–18.
Greenwood J (1999). Clinical development (nursing):The Western Sydney approach. Journal ofAdvanced Nursing 29: 674–9.
Hart E, Bond M (1995). Action Research for Health andSocial Care: A Guide to Practice. Buckingham:Open University Press.
Kennedy N (2001). Developing nursing practice:Introducing knee-length anti-embolic stockings. InR Winter, C Munn-Giddings (eds.) A Handbook forAction Research in Health and Social Care.London: Routledge.
Kitson A, Currie L (1996). Clinical practice develop-ment and research activities in four district healthauthorities. Journal of Clinical Nursing 5: 41–51.
McCormack B (2001). Negotiating Partnerships withOlder People: A Person-Centred Approach.Basingstoke: Ashgate.
McCormack B (2003). The characteristics, qualities andskills of practice developers. Journal of ClinicalNursing 12: 317–25.
McCormack B, Manley K, Titchen A (1999). Towardspractice development – a vision in reality or a reali-ty without vision? Journal of Nursing Management,
158 FitzGerald and Armitage
Copyright © 2005 John Wiley & Sons, Ltd. 4(3): 150–159 (2005)
158
PDHC 4.3 crc 30/9/05 2:46 pm Page 158

Copyright © 2005 John Wiley & Sons, Ltd. 4(3): 150–159 (2005)
Clinical research: The potential of practice development 159159
7: 255–64.McCormack B, Wright J (1999). Achieving dignified
care for older people through practice development:A systematic approach. NT Research 4: 340–52.
NHMRC (2002). Human Research Ethics Handbook.Canberra: Commonwealth of Australia.
Park P (2001). Knowledge and participatory research. InP Reason, H Bradbury (eds.) Handbook of ActionResearch Participative Inquiry and Practice.London: Sage Publications.
Pearson A (1983). The Clinical Nursing Unit. London:Heinemann.
Pearson A (1988). Primary Nursing: Nursing in theBurford and Oxford Development Units. London:Croome Helm.
Pearson A (1992). Nursing at Burford: A Story ofChange. London: Scutari Press.
Pearson A (1997). An evaluation of the King’s FundCentre Nursing Development Unit Network1989–91. Journal of Clinical Nursing 6: 25–33.
Reason P, Bradbury H (eds.) (2001). Handbook of ActionResearch Participative Inquiry and Practice.
London: Sage Publications.Salvage J (1990). The theory and practice of the ‘new’
nursing, Nursing Times 86: 42–5.Titchen A (1998). A conceptual framework for facilitat-
ing learning in clinical practice. Centre forProfessional Education Advancement.
Unsworth J (2000). Practice development: A conceptanalysis. Journal of Nursing Management 8: 317–26.
Ward M, Titchen A, Morrell C, McCormack B, Kitson A(1998). Using a supervisory framework to supportand evaluate a multiproject practice developmentprogramme. Journal of Clinical Nursing 7: 29–36.
Winter R, Munn-Giddings C (2001). A Handbook forAction Research in Health and Social Care.London: Routledge.
Wright S (1991). Nursing development units: Ten yearsat Tameside. Nursing the Elderly 3: 10–11.
Address correspondence to: Mary Fitzgerald, James CookUniversity, PO Box 6811, Cairns 4870, Australia.E-mail: [email protected]
PDHC 4.3 crc 30/9/05 2:46 pm Page 159


















