
Clinical Research AACR-FDA-NCI Cancer Biomarkers ...AACR-FDA-NCI Cancer Biomarkers Collaborative...
21
Special Report AACR-FDA-NCI Cancer Biomarkers Collaborative Consensus Report: Advancing the Use of Biomarkers in Cancer Drug Development Samir N. Khleif 1 , James H. Doroshow 1 , and William N. Hait 2 ; for the AACR-FDA-NCI Cancer Biomarkers Collaborative Abstract Recent discoveries in cancer biology have greatly increased our understanding of cancer at the mo- lecular and cellular level, but translating this knowledge into safe and effective therapies for cancer patients has proved to be challenging. There is a growing imperative to modernize the drug develop- ment process by incorporating new techniques that can predict the safety and effectiveness of new drugs faster, with more certainty, and at lower cost. Biomarkers are central to accelerating the identification and adoption of new therapies, but currently, many barriers impede their use in drug development and clinical practice. In 2007, the AACR-FDA-NCI Cancer Biomarkers Collaborative stepped into the nation- al effort to bring together disparate stakeholders to clearly delineate these barriers, to develop recom- mendations for integrating biomarkers into the cancer drug development enterprise, and to set in motion the necessary action plans and collaborations to see the promise of biomarkers come to fru- ition, efficiently delivering quality cancer care to patients. Clin Cancer Res; 16(13); 3299–318. ©2010 AACR. Knowledge of cancer at the cellular and molecular levels has grown exponentially in the past two decades and has resulted in significant improvement in the character- ization of human tumors, which in turn has catalyzed a shift toward the development of targeted therapies. Advances in technology are increasingly leading to large- scale, high-throughput research and to the development and improvement of the tools capable of analyzing the whole genome, proteome, transcriptome, and metabo- lome (often referred to as the “-omics” approaches). This tremendous revolution in biomedical sciences and techno- logy produces massive amounts of data and has unprece- dented potential to fuel the pipeline of therapeutics in development. Unfortunately, the degree to which this knowledge is translated into safe and effective cancer ther- apies is not keeping pace, in large part because the current drug development process is increasingly costly, ineffi- cient, and unpredictable. Despite a major increase in investment by government and industry over the last two decades, the overall U.S. approval success rate for cancer therapeutics has remained low (1). The cost and time required to evaluate and devel- op drug candidates have increased dramatically; the clin- ical phase of development can cost hundreds of millions of dollars and take nearly a decade to complete (2). Fur- thermore, the failure rate of clinical trials has increased, with one half of oncology drugs entering phase III trials never making it to U.S. regulatory approval (2). Many drug candidates fail in early clinical development because outdated trial designs are used for their clinical testing and evaluation. Although advances in technology and genomic information have fueled the use of innovative tools, methods, standards, and approaches—including those using biomarkers—throughout the drug develop- ment process, the incorporation of cutting-edge science and evidence-based knowledge into regulatory decision making has lagged behind. The resulting uncertainty in the drug approval process can make it difficult to get targeted therapies approved and implemented into clinical practice. Thus, both the drug development and regulatory approval processes are often constrained by outdated assessment tools. The model for development of “blockbuster” drugs, that is, drugs given to an unselected population even though they may only be effective in a small percentage of the population, may not be sustainable. Traditional popula- tion-based models of clinical trials used for drug approval are designed to guard against bias of selection, which may form the antithesis of personalized medicine, and accord- ingly, these trials expose large numbers of patients to drugs from which they may not benefit. In oncology, where treatments are costly, life expectancy is limited, and the risk of drug toxicity is often high, there is a press- ing need to identify and treat those patients for whom a given drug is most likely to be beneficial. Authors' Affiliations: 1 National Cancer Institute and 2 Ortho Biotech Oncology R&D, Johnson and Johnson Family of Companies, Raritan, New Jersey Corresponding Author: William N. Hait, Ortho Biotech Oncology R&D, Johnson and Johnson Family of Companies, 920 Route 202, Raritan, NJ 08869-1424. Phone: 9089273516; Fax: 9089277716; E-mail: [email protected]. doi: 10.1158/1078-0432.CCR-10-0880 ©2010 American Association for Cancer Research. Clinical Cancer Research www.aacrjournals.org 3299 Research. on July 10, 2020. © 2010 American Association for Cancer clincancerres.aacrjournals.org Downloaded from Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
Transcript of Clinical Research AACR-FDA-NCI Cancer Biomarkers ...AACR-FDA-NCI Cancer Biomarkers Collaborative...
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
Special Report Clinical
CancerResearch
AACR-FDA-NCI Cancer Biomarkers Collaborative ConsensusReport: Advancing the Use of Biomarkers in CancerDrug Development
Samir N. Khleif1, James H. Doroshow1, and William N. Hait2; for the AACR-FDA-NCI Cancer Biomarkers Collaborative
Abstract
Authors' AOncologyNew Jersey
CorresponJohnson aNJ 08869WHait@ITS
doi: 10.115
©2010 Am
www.aacr
Do
Recent discoveries in cancer biology have greatly increased our understanding of cancer at the mo-lecular and cellular level, but translating this knowledge into safe and effective therapies for cancerpatients has proved to be challenging. There is a growing imperative to modernize the drug develop-ment process by incorporating new techniques that can predict the safety and effectiveness of new drugsfaster, with more certainty, and at lower cost. Biomarkers are central to accelerating the identificationand adoption of new therapies, but currently, many barriers impede their use in drug development andclinical practice. In 2007, the AACR-FDA-NCI Cancer Biomarkers Collaborative stepped into the nation-al effort to bring together disparate stakeholders to clearly delineate these barriers, to develop recom-mendations for integrating biomarkers into the cancer drug development enterprise, and to set inmotion the necessary action plans and collaborations to see the promise of biomarkers come to fru-ition, efficiently delivering quality cancer care to patients. Clin Cancer Res; 16(13); 3299–318. ©2010 AACR.
Knowledge of cancer at the cellular and molecular levelshas grown exponentially in the past two decades andhas resulted in significant improvement in the character-ization of human tumors, which in turn has catalyzeda shift toward the development of targeted therapies.Advances in technology are increasingly leading to large-scale, high-throughput research and to the developmentand improvement of the tools capable of analyzing thewhole genome, proteome, transcriptome, and metabo-lome (often referred to as the “-omics” approaches). Thistremendous revolution in biomedical sciences and techno-logy produces massive amounts of data and has unprece-dented potential to fuel the pipeline of therapeutics indevelopment. Unfortunately, the degree to which thisknowledge is translated into safe and effective cancer ther-apies is not keeping pace, in large part because the currentdrug development process is increasingly costly, ineffi-cient, and unpredictable.Despite a major increase in investment by government
and industry over the last two decades, the overall U.S.approval success rate for cancer therapeutics has remainedlow (1). The cost and time required to evaluate and devel-op drug candidates have increased dramatically; the clin-
ffiliations: 1National Cancer Institute and 2Ortho BiotechR&D, Johnson and Johnson Family of Companies, Raritan,
ding Author: William N. Hait, Ortho Biotech Oncology R&D,nd Johnson Family of Companies, 920 Route 202, Raritan,-1424. Phone: 9089273516; Fax: 9089277716; E-mail:.JNJ.COM.
8/1078-0432.CCR-10-0880
erican Association for Cancer Research.
journals.org
Researcon July clincancerres.aacrjournals.org wnloaded from
ical phase of development can cost hundreds of millionsof dollars and take nearly a decade to complete (2). Fur-thermore, the failure rate of clinical trials has increased,with one half of oncology drugs entering phase III trialsnever making it to U.S. regulatory approval (2). Manydrug candidates fail in early clinical development becauseoutdated trial designs are used for their clinical testingand evaluation. Although advances in technology andgenomic information have fueled the use of innovativetools, methods, standards, and approaches—includingthose using biomarkers—throughout the drug develop-ment process, the incorporation of cutting-edge scienceand evidence-based knowledge into regulatory decisionmaking has lagged behind. The resulting uncertainty inthe drug approval process can make it difficult to gettargeted therapies approved and implemented into clinicalpractice. Thus, both the drug development and regulatoryapproval processes are often constrained by outdatedassessment tools.The model for development of “blockbuster” drugs, that
is, drugs given to an unselected population even thoughthey may only be effective in a small percentage of thepopulation, may not be sustainable. Traditional popula-tion-based models of clinical trials used for drug approvalare designed to guard against bias of selection, which mayform the antithesis of personalized medicine, and accord-ingly, these trials expose large numbers of patients todrugs from which they may not benefit. In oncology,where treatments are costly, life expectancy is limited,and the risk of drug toxicity is often high, there is a press-ing need to identify and treat those patients for whom agiven drug is most likely to be beneficial.
3299
h. 10, 2020. © 2010 American Association for Cancer

Biomarker: A characteristic that is objectivelymeasured and evaluated as an indicator of normalbiological processes, pathogenic processes, or pharma-cologic responses to a therapeutic intervention (34).
Diagnostic Biomarkers• Early detection biomarkers• Disease classificationPredictive Biomarkers• Predict patients likely to respond to a specific agent• Predict patients likely to have an adverse event to aspecific agent
Metabolism Biomarkers• Dose definingOutcome Biomarkers• Forecast response• Forecast progression• Forecast recurrence
Analytic validation or assay validation: The processof assessing the assay and its performance characteris-tics and determining the optimal conditions that willgenerate a reliable, reproducible, and accurate bio-marker assay for the intended application (3).
Clinical qualification: The evidentiary process oflinking a biomarker (using data obtained by a bio-marker assay) with meaningful biological or clinicaloutcomes (3).
Known valid biomarker: A biomarker that is mea-sured in an analytic test system with well-establishedperformance characteristics and for which there is anestablished scientific framework or body of evidencethat elucidates the physiologic, toxicologic, pharmaco-logic, or clinical significance of the test results (35).
Khleif et al.
3300
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
Prospectively identifying populations of responders re-quires the development of predictive biomarkers, that is,biomarkers that predict the likelihood of response to aparticular pharmaceutical agent(s). Such biomarkers canalso be used to identify patient populations that are like-ly to have an adverse event. Development of a drug andcompanion diagnostic (i.e., an assay or test that detectsrelevant biomarkers) can aid in patient selection andtreatment decisions and forms the basis of what is re-ferred to as personalized medicine—using molecular di-agnosis of disease to prescribe the right treatment to theright patient. Biomarkers are also useful throughout thedrug development process (3), not only to better deter-mine drug efficacy with fewer patients by identifying crit-ical responder subpopulations but also to provide earlyinformation about unpromising candidates such that acompany can abandon its efforts sooner, saving valuabletime and resources.
Clin Cancer Res; 16(13) July 1, 2010
Researcon July clincancerres.aacrjournals.org Downloaded from
Like drug discovery and development, the discovery anddevelopment cycle for biomarkers can be defined as a setof linked processes in a pipeline: hypothesis generation,research study design, sample collection, data collection,data analysis, assay development, assay validation, clinicalqualification, regulatory approval, and clinical use. Overthe last several years, remarkable effort by the biomedicalresearch community has gone into discovering and devel-oping biomarkers for the diagnosis and treatment of can-cer. Although this research has paid off in a plethora ofnovel biomarkers (4–7), most of them are stalled in aresearch setting, unable to be exploited for widespreadclinical use. To date, it has been difficult for individual re-search laboratories to determine which biomarkers havethe greatest potential for use in a clinical setting and todevelop them, independently or concomitant with com-panion drug development, to standards that regulatoryagencies would find acceptable. The biomarker fieldneeds a clear path for taking biomarkers from the re-search discovery phase, through validation, qualification,and the global regulatory approval process, and then onto use in clinical practice. Achieving the goal of usingvalidated biomarkers to accelerate drug approvals willrequire a collaborative, multidisciplinary effort thatbrings together those in the basic, clinical, translational,and regulatory sciences.Recognizing the great promise of personalized medicine
but seeing that forward momentum was slow, in March2004 the Food and Drug Administration (FDA) unveiledtheCritical Path Initiative, a nationwide effort tomodernizethe scientific process through which potential therapeuticsor devices are transformed from discoveries into medicalproducts. The initiative was launched with the release of areport entitled “Innovation or Stagnation: Challenge andOpportunity on the Critical Path to NewMedical Products”(8), which detailed the scientific reasons for the recent de-crease in the number of innovative medical productssubmitted for FDA approval. The Critical Path Initiativeidentified biomarkers as one of the most important areasfor improving progress in therapeutic drug development.Numerous other organizations and agencies worldwide
have launched efforts to address the complexities of cancerdrug development, and many have also identified biomar-kers as a key component for accelerating progress alongthe critical path from the laboratory bench to the patientbedside. Yet despite this broad interest, considerable pub-lic and private research spending, and the drive towardpersonalized medicine, surprisingly few biomarkers havebeen successfully translated into fully validated diagnostictools. Indeed, less than two dozen cancer biomarkers havebeen approved by the FDA (9).
Accelerating Progress along the Critical Path:The AACR-FDA-NCI Cancer BiomarkersCollaborativeA major factor contributing to the lack of progress in the
biomarker field seems to be the diversity of stakeholders
Clinical Cancer Research
h. 10, 2020. © 2010 American Association for Cancer

Advancing Biomarker Use in Cancer Drug Development
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
involved at the different phases of the biomarker lifecycle.Each stakeholder may have a particular agenda that is notwell aligned, and is often in direct conflict, with others'agendas. In an effort to understand how disparate stake-holder motivations and perspectives contribute to thestagnation of biomarker development and clinical integra-tion, the American Association for Cancer Research(AACR), in partnership with the FDA, the National CancerInstitute (NCI), and the Pharmaceutical Research andManufacturers Association (PhRMA), convened a 2-dayworkshop to discuss the use of biomarkers in oncologicdrug development and therapy in November 2006. TheAACR-FDA-NCI Cancer Biomarkers Workshop3 catalyzedinteractions among stakeholders from academia, industry,government, and the patient advocacy community. Thisworkshop, alongwith insightful discussions with FDA lead-ership about how the AACR could help advance the CriticalPath Initiative, led to the establishment of the AACR-FDA-NCI Cancer Biomarkers Collaborative (CBC) in April 2007.The goal of the CBC is to accelerate the translation of can-
cer therapeutics into the clinic by shaping the processes forthe effective development of validated biomarkers and theiruse in clinical trials for maximum patient benefit. Para-mount to the success of the CBC is that it seeks input fromand develops consensus among distinguished experts andkey stakeholders—academia, pharmaceutical and diagnos-tics industries, government agencies, regulators, and patientadvocates—worldwide. The CBC currently consists of morethan 120 experts in all areas of cancer biomarker researchworking in four committees to address the priority areasof biospecimens, assay validation, bioinformatics, andinformation sharing (listed in no order of importance).The objectives of the four CBC committees, which
conducted their work over the course of the following18 months, were (a) to identify the barriers to developingbiomarkers for clinical use; (b) to define best practices andmake recommendations to hasten the integration of bio-markers into drug development and clinical practice; and(c) to develop action plans with short- and long-termsolutions to help move these vitally important areas for-ward. These action plans and related activities form thegroundwork for a comprehensive strategy to facilitate thedevelopment of the methodologies, infrastructure, andpolicies necessary for effective and efficient use of biomar-kers during cancer therapy. The processes addressed by theCBC's work are relevant to the development of most bio-markers. Nonetheless, the CBC discussed the importanceof other diagnostic techniques (e.g., imaging modalities)and other intended uses of biomarkers (e.g., forecastingresponse, progression, or recurrence) and noted the poten-tial for future expansion based on its initial work.The imperative to develop and apply quality standards,
quality criteria, and quality systems for biospecimens and
3 AACR-FDA-NCI Cancer Biomarkers Workshop, November 2006. Furtherinformation available from: http://www.aacr.org/home/scientists/working-groups-task-forces.aspx.
www.aacrjournals.org
Researcon July clincancerres.aacrjournals.org Downloaded from
biomarker assay validation, as well as to construct anenabling environment of infrastructure, regulations, andpolicies that foster efforts tomeet these goals, emerged fromthe CBC discussions. An enabling environment wouldinclude, among other things, a system for harmonizingterminology and standards, a supportive bioinformaticsplatform, incentives for following standards and sharingdata, and improved awareness among stakeholders.Specifically, the CBC committees identified eight critical
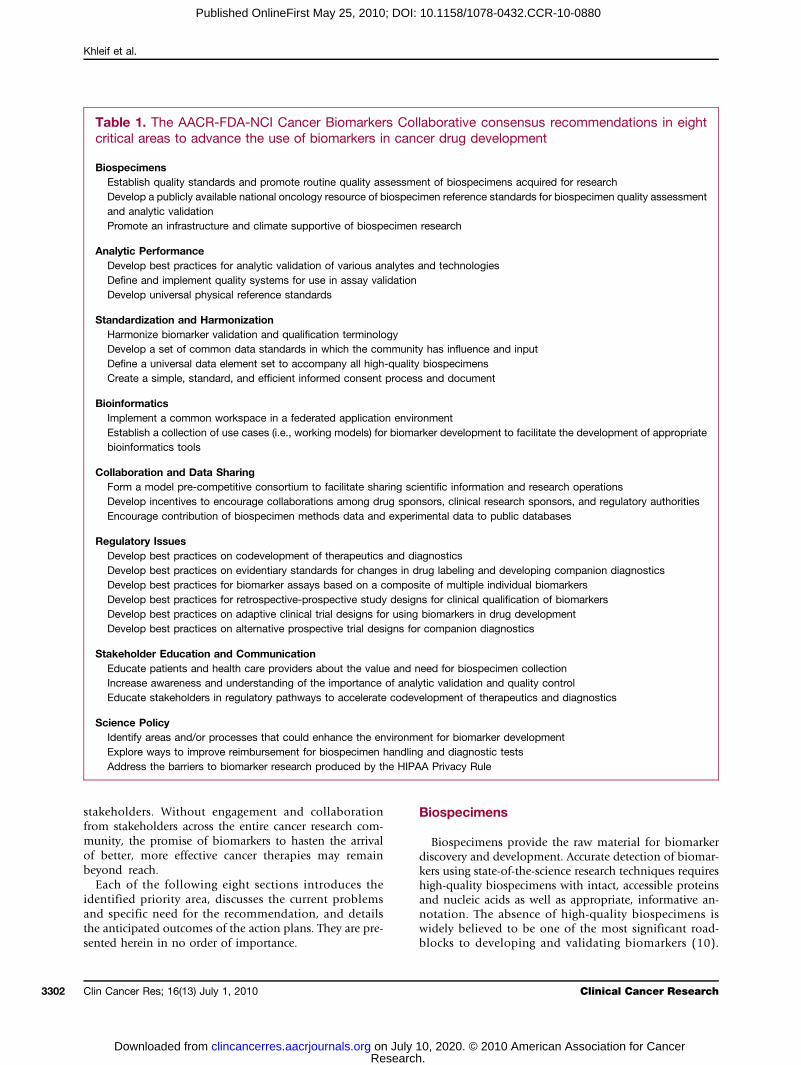
areas for efficient and effective biomarker developmentand came to consensus on 27 recommendations (Table 1)that span these areas and address the most pressing barriersto the advancement of biomarkers in the developmentof cancer therapeutics. For ease of discussion, the CBC'srecommendations are categorized into eight critical areasfor biomarker development: (a) biospecimens, (b) analyticperformance, (c) standardization and harmonization, (d)bioinformatics, (e) collaboration and data sharing, (f)stakeholder education and communication, (g) regulatoryissues, and (h) science policy. For each recommendation,a corresponding action plan toward overcoming thesebarriers was developed. The CBC recognizes that many ofthe recommendations need to be addressed contemporane-ously, with continual feedback and dissemination of prog-ress to the broader community, especially in light of therapidly evolving technologies and scientific advances thatpervade the biomarker field.Accomplishing the recommendations is no trivial un-
dertaking and cannot be implemented by a single sectoror a single group working in isolation. It will require theclose involvement and cooperation of governmentalagencies, legislative bodies, industry, academia, and ad-vocacy and nongovernmental not-for-profit organiza-tions. The CBC recognizes and applauds the hard workof the numerous agencies and organizations worldwidethat are already making strides toward surmounting bar-riers to biomarker development. The unique structure ofthe CBC, which boasts a deep interest and participationfrom the entire gamut of stakeholders engaged in thebiomarker pipeline, means its greatest contributions arethrough its roles as a convener and an educator—theCBC can act as a catalyst for the numerous efforts thatrequire coordination of multiple stakeholders, can buildconsensus and speak as a strong, collective voice to advo-cate for necessary process and policy changes, and canserve as a valuable resource for the cancer research com-munity. The CBC will continue to organize workshopsand working groups to advance the development ofwhite papers, best practice documents, and educationalmaterials to meet the specific challenges of individualrecommendations. Furthermore, the CBC, which hasprimarily focused on the United States, will broadenits purview by seeking out additional international part-ners to collaborate on the many areas requiring globalparticipation and harmonization. To make progress onthe recommendations herein will require a substantialinvestment of resources—intellectual, personnel, time,and fiscal—and a committed, collective action from
Clin Cancer Res; 16(13) July 1, 2010 3301
h. 10, 2020. © 2010 American Association for Cancer
Khleif et al.
3302
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
stakeholders. Without engagement and collaborationfrom stakeholders across the entire cancer research com-munity, the promise of biomarkers to hasten the arrivalof better, more effective cancer therapies may remainbeyond reach.Each of the following eight sections introduces the
identified priority area, discusses the current problemsand specific need for the recommendation, and detailsthe anticipated outcomes of the action plans. They are pre-sented herein in no order of importance.
Clin Cancer Res; 16(13) July 1, 2010
Researcon July clincancerres.aacrjournals.org Downloaded from
Biospecimens
Biospecimens provide the raw material for biomarkerdiscovery and development. Accurate detection of biomar-kers using state-of-the-science research techniques requireshigh-quality biospecimens with intact, accessible proteinsand nucleic acids as well as appropriate, informative an-notation. The absence of high-quality biospecimens iswidely believed to be one of the most significant road-blocks to developing and validating biomarkers (10).
Table 1. The AACR-FDA-NCI Cancer Biomarkers Collaborative consensus recommendations in eightcritical areas to advance the use of biomarkers in cancer drug development
BiospecimensEstablish quality standards and promote routine quality assessment of biospecimens acquired for researchDevelop a publicly available national oncology resource of biospecimen reference standards for biospecimen quality assessmentand analytic validationPromote an infrastructure and climate supportive of biospecimen research
Analytic PerformanceDevelop best practices for analytic validation of various analytes and technologiesDefine and implement quality systems for use in assay validationDevelop universal physical reference standards
Standardization and HarmonizationHarmonize biomarker validation and qualification terminologyDevelop a set of common data standards in which the community has influence and inputDefine a universal data element set to accompany all high-quality biospecimensCreate a simple, standard, and efficient informed consent process and document
BioinformaticsImplement a common workspace in a federated application environmentEstablish a collection of use cases (i.e., working models) for biomarker development to facilitate the development of appropriatebioinformatics tools
Collaboration and Data SharingForm a model pre-competitive consortium to facilitate sharing scientific information and research operationsDevelop incentives to encourage collaborations among drug sponsors, clinical research sponsors, and regulatory authoritiesEncourage contribution of biospecimen methods data and experimental data to public databases
Regulatory IssuesDevelop best practices on codevelopment of therapeutics and diagnosticsDevelop best practices on evidentiary standards for changes in drug labeling and developing companion diagnosticsDevelop best practices for biomarker assays based on a composite of multiple individual biomarkersDevelop best practices for retrospective-prospective study designs for clinical qualification of biomarkersDevelop best practices on adaptive clinical trial designs for using biomarkers in drug developmentDevelop best practices on alternative prospective trial designs for companion diagnostics
Stakeholder Education and CommunicationEducate patients and health care providers about the value and need for biospecimen collectionIncrease awareness and understanding of the importance of analytic validation and quality controlEducate stakeholders in regulatory pathways to accelerate codevelopment of therapeutics and diagnostics
Science PolicyIdentify areas and/or processes that could enhance the environment for biomarker developmentExplore ways to improve reimbursement for biospecimen handling and diagnostic testsAddress the barriers to biomarker research produced by the HIPAA Privacy Rule
Clinical Cancer Research
h. 10, 2020. © 2010 American Association for Cancer

Advancing Biomarker Use in Cancer Drug Development
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
The reasons leading to low-quality biospecimens are nu-merous and broad-ranging, but the use of low-quality spe-cimens often results in the same unfavorable outcome:variability in assays that causes erroneous conclusionsand failure to advance the translational process. Improv-ing the quality and consistency of biospecimen resourceswas identified by the CBC as a top priority for action. CBCrecommendations aim to improve universal biospecimencollections by addressing quality, reference standards, andthe field of biospecimen research.
Quality—Establish quality standards and promoteroutine quality assessment of biospecimens acquiredfor researchBiological samples used in clinical hypothesis testing
must be validated before use to ensure their adequacyfor the proposed analytic platform. The physical state ofbiospecimens is affected by many factors, including pre-acquisition (e.g., type of anesthesia given to the patient),acquisition (e.g., type of biopsy), and post-acquisition(e.g., how biospecimen is processed, stored, and preparedfor analysis) variables. Currently, there is little quality assur-ance or quality control on newly collected or archivedbiospecimens, and collections used for retrospective studiesmost frequently are composed of biospecimens of un-known and often poor quality. Although numerous guide-lines and recommendations for biospecimen collectionexist (11–14), there are no uniformly applied standardsfor biospecimen quality. Neither international consensusnor widespread implementation has been achieved. Theextent of this problem was highlighted when The CancerGenome Atlas (TCGA) project of the NCI surveyed speci-mens for its large-scale sequencing effort. Many large collec-tions of biospecimens previously assumed to be of highquality were found to be unacceptable for use in the TCGApilot project (15). Thus, from the initial stages of biomarkerdiscovery research, low-quality samples hinder progress. Toaddress the lack of high-quality biospecimens, consensusdocuments on evidence-basedbest practices for biospecimencollection, evaluation of biospecimen quality, and qualitycontrol are needed. Best practices are dependent, to some de-gree, on the biospecimen type, the molecular analysis to beperformed, and the goal or application of the research, andefforts in this area must aim to address the implausibility ofapplying a “one-size-fits-all” approach. Understanding thatlimited data exist on which to base best practices, efforts tobolster biospecimen research are also needed (see “Research”below). Changes in biospecimen collection methods andimplementation of quality testing to comply with best prac-tices will require a commitment of laboratory time andresources. Thus, universal uptake of best practices is not likelyto happenwithout added incentives or appropriate disincen-tives. The idea of an accreditation program for biospecimenrepositories should also be explored. Annotationof biospeci-mens with associated clinical data and the permitted use ofbiospecimens based on ethical, legal, and policy issues alsoaffect the quality of biospecimen resources and are discussedin the appropriate sections below.
www.aacrjournals.org
Researcon July clincancerres.aacrjournals.org Downloaded from
Reference standards—Develop a publicly availablenational oncology resource of biospecimen referencestandards for biospecimen quality assessment andanalytic validationA critical component of quality control is having access
to reference standards that enable methodologic standard-ization, increase the confidence with which quality controldata are interpreted, and provide material for proficiencytesting of personnel. No such reference standards exist forbiospecimens, and as a consequence, routine and reliablequality assessment is severely impeded. A reference repos-itory of carefully characterized biospecimens that wouldinclude blood for genomic DNA, tumor tissue, and adja-cent “normal” tissue of known molecular content andintegrity would be valuable for control and comparisonpurposes. Additionally, availability of carefully annotatedreference biospecimens appropriate for use in analyticvalidation would result in better, faster analytic validationof new biomarker assays. These specimens would need tobe representative of those that will be used in clinical test-ing and be available in sufficient numbers to allow mean-ingful statistical analysis. The NCI Office of Biorepositoriesand Biospecimen Research (OBBR) has invested consider-able time and effort toward this goal and is in the earlystages of developing a national, standardized humanbiospecimen resource called the cancer Human Biobank(caHUB). To facilitate the establishment of a publiclyavailable resource of biospecimen reference standards forquality assessment and assay validation, best practices forstorage and use of biospecimen reference standards shouldbe developed, as should best practices needed to facilitatesuch a resource, which agencies could utilize to improvenational infrastructures. Standardized measures of biospe-cimen quality plus the availability of reference biospeci-men standards would improve individual studies andfacilitate cross-repository studies and sample sharing byallaying the common concern that specimens from otherfacilities are of unknown quality and thus potentiallyunreliable.
Research—Promote an infrastructure and climatesupportive of biospecimen researchThe lack of evidence to define best practices for biospe-
cimen use is a barrier to establishing universal standardsfor use in biomarker research. Biospecimen science, where-in the biospecimen itself is the subject of research, is per-ceived to be undervalued by the scientific community.Moreover, most empirical methods used currently inbiomarker research do not incorporate data-driven bio-specimen practices. The generation of large collectionsof high-quality biospecimens necessary for biomarkerresearch and development may require significant changesto the current infrastructure and research climate. Initia-tives aimed at educating researchers, funding agencies,scientific journals, and other stakeholders on the meritsand necessity of biospecimen research are needed. A coor-dinated effort to alter the publication process to encourageresearchers to communicate optimized biospecimen
Clin Cancer Res; 16(13) July 1, 2010 3303
h. 10, 2020. © 2010 American Association for Cancer

Khleif et al.
3304
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
protocol details is also warranted. Wider access to back-ground biospecimen research should promote better sam-ple procurement practices and avoid duplication of effort.
Biospecimens of known high quality would enableresearchers to take full advantage of the newest, mostexacting analytic platforms. As discussed above, toachieve universal high quality for biospecimens requirescollective progress in quality measures and assessment,development of reference standards, and advancementof the scientific knowledge that drives best practices.The CBC will help to drive the field toward establishingrigorous standards for biospecimen procurement andstorage by working with the NCI OBBR and reachingout to other U.S. and international agencies and organi-zations to help develop consensus needed to establishbest practices in the aforementioned areas. The CBC willalso dedicate efforts toward initiating and supporting theneeded culture shift by encouraging compliance with bestpractices and building on the ongoing efforts of otherorganizations to coordinate and augment initiativesaimed at educating researchers, funding agencies, scien-tific journals, and other stakeholders on the merits andnecessity of biospecimen research. Progress will also re-quire standardization of quality measures, terminology,and annotation. Once high-quality biospecimens areroutinely collected, reaping their full potential to advancebiomarker development will be dependent on increasedcollection of and broader access to samples and will involveimprovement in the informed consent process and ineducating the public. Recommendations to address thesechallenges are discussed in the appropriate sections below.
Analytic Performance
Another major reason that cancer biomarkers are not bet-ter incorporated into the drug development process, andtherefore clinical practice, is the challenge of developing,using, and communicating proper information about bio-marker diagnostics. Without proper determination of ana-lytic performance and biological and/or clinical relevance,biomarkers cannot have the expected and desired impacton improving the quality of cancer care. The diversity of per-spective among groups and individuals in the field hascomplicated efforts to achieve well-founded and under-standable analytic validation methods. Indeed, the term“biomarker assay validation” remains one that is controver-sial and is defined differently depending on the stakeholderusing the term. Defining, optimizing, and standardizing theprocesses used to validate biomarker assays will improvebiomarker integration into clinical trials and encourageacceptance by regulatory agencies.
Assay validation methodologies—Develop bestpractices for analytic validation of various analytesand technologiesAnalytic validation is necessary to demonstrate that an as-
say is accurate and reliable and that it meets the experimen-
Clin Cancer Res; 16(13) July 1, 2010
Researcon July clincancerres.aacrjournals.org Downloaded from
tal objectives in a reproducible and comparable manner.There are significant differences in approaches and eviden-tiary standards required by regulatory agencies, accreditingorganizations, granting agencies, scientific journals, profes-sional organizations, and others. Only recently has a stan-dardized template for defining diagnostic accuracy, theSTARD initiative (16), been encouraged by biomedicaljournals. The paucity of specific guidelines for analytic va-lidity may lead to omissions or failures that are detrimentalto ensuring that an assay is accurate and reliable. Moreover,it is becoming increasingly clear that assay developmentshould account for the analytic variability in testing andfor the pre-analytic (e.g., biospecimen acquisition and han-dling) and post-analytic (e.g., reporting methods) factorsthat may affect the generation of reliable results and properuse of these results.Widely accepted standards andmethod-ologies for analytic validation of analytes and technologieswould benefit the cancer research community. Validatedbiomarker assays would provide the confidence with whichdata could be interpreted and would allow standardizationto facilitate the pooling of data across investigational sites.Additionally, physician understanding and clinical uptakeof new tests may be aided by standardized methods of an-alytic validation.
Quality systems—Define and implement qualitysystems for use in assay validationAnalytic validation of an assay does not ensure continual
high-performance results unless supported by an integratedsystem to implement andmaintain quality objectives. Stud-ies to validate biomarker assays that are carried out in re-search laboratories lacking defined quality systems maygenerate inconsistent results leading to a reduced level ofconfidence in the assay. Thus, a quality system should bein place and functioning effectively before attempting tovalidate the biomarker assay or initiating clinical servicesthat use the biomarker. A quality system approach willmake this aspect of the pipeline more efficient and reliable.Guidelines for quality system requirements are needed,along with appropriate incentives or disincentives and ed-ucational programs to encourage laboratories to adoptmodel quality system approaches. The application of qual-ity system principles to all levels of biomarker work, fromdiscovery to clinical qualification, should help streamlinethe process, providing assurance that data are reliable andminimizing the unexpected failures that result from poorquality approaches.
Physical standards—Develop universal physicalreference standardsOften, results from clinical trials using biomarker mea-
surements cannot be directly compared because there arefew universally available physical standards on which tobase such comparisons. Physical standards for analytesand matrices relevant to cancer biomarker measurementwould be a valuable resource during biomarker develop-ment and during clinical trials. Ideally, a universal standardwould be available for each individual biomarker; however,
Clinical Cancer Research
h. 10, 2020. © 2010 American Association for Cancer

Advancing Biomarker Use in Cancer Drug Development
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
time and cost constraints limit the number of standards thatcan be generated and will force prioritization of standards,their most useful form, and their biological and chemicalfeatures. In addition, the organizations responsible for de-veloping, characterizing, curating, and distributing the stan-dards will need to be identified. Achieving a resource ofphysical standards would expedite inter-study comparisonsby promoting cross-referencing of biomarker measure-ments within and between clinical trials.
The CBC recommendations on improving the process ofanalytic validation of biomarkers address major problemsin the quality and reproducibility of methods. To facilitatetheir implementation, the CBC will help develop consen-sus needed to establish best practices and provide educa-tional activities and resources to encourage laboratoriesto follow best practices for assay validation and adoptmodel quality system approaches. The CBC's consensusapproach is particularly valuable for prioritization becausethe needs among user groups and communities are quitevaried. Similar to the burdens of improving biospecimenquality, engaging stakeholders to comply with best prac-tices, incorporate quality systems into research activities,and contribute to and utilize universal physical standardswill require additional expenditures of personnel and fiscalresources. Widespread adoption and implementation ofnew practices may require considerable stakeholder educa-tion and outreach and/or appropriate incentives or disin-centives from regulatory and funding agencies.
Standardization and Harmonization
Every dimension of biomarker translation—from dis-covery to clinical practice—is riddled with the problemsof heterogeneity and an absence of universal standards.Each stakeholder may use a different language and meth-ods of operating, restricting the potential for collabora-tion, utilization of others' samples, and building onprevious work. The expansion of the global economy,the prevalence of diagnostic manufacturers with world-wide distribution, and the increased regulatory oversightat local, regional, and national levels have significantlyincreased the need for harmonization. Yet, currentlythere is no comprehensive effort to develop the necessarystandards. The CBC recommends action in four areas inneed of standardization and harmonization: terminolo-gy, data standards, biospecimen annotation, and in-formed consent.
Terminology—Harmonize biomarker validation andqualification terminologyConsiderable differences exist in the nomenclature and
definitions used at the various stages of biomarker discov-ery, development, and clinical use. Further complicatingmatters is the lack of consistency within each of thesestages, in which terminology varies depending on the sci-entific specialty or the specific analytic technique used formeasurement of the biomarker. Some nomenclature and
www.aacrjournals.org
Researcon July clincancerres.aacrjournals.org Downloaded from
definitions have been introduced by federal legislation[e.g., the Clinical Laboratory Improvement Amendments(CLIA) of 1988], whereas other terminologies have beenproposed by outside organizations (e.g., the InternationalFederation for Clinical Chemistry, the International Orga-nization for Standardization, and the International Unionof Pure and Applied Chemistry, among others) seeking toestablish appropriate standards. Unfortunately, few ofthese documents can be immediately and freely accessed,limiting their potential for widespread adoption. Interna-tional, national, and other organizations should continueto collaborate to develop harmonized terms and defini-tions. Existing databases should be improved and/or otherresources should be created that are user-friendly and pub-licly accessible. Harmonizing biomarker validation andqualification terminology will lay the foundation forcollaboration and will improve the interactions with regu-lators and the education of stakeholders.
Data standards—Develop a set of common datastandards in which the community hasinfluence and inputSemantic interoperability (i.e., the ability of two or
more systems or components to exchange informationand to use the information that has been exchanged)allows the exchange and use of information across plat-forms and between institutions and is a prerequisite to afunctional biomedical cyber-infrastructure and a collec-tion of common analysis tools. The field of informaticsand its applications in biology have benefited greatlyfrom the adoption of common data models for maturingtechnologies. Obtaining data is a costly endeavor; how-ever, establishing databases that provide interoperabilityaffords the ongoing opportunity for data mining and ret-rospective studies and, thus, enhances the value of thecollected data. Developing a set of common data stan-dards that address data elements, domain level data, me-tadata (i.e., data that describe the content of a document,image, or website; examples include the date created, im-age resolution, keywords, and security features), dataontologies (i.e., common vocabulary for researchers toaid in understanding the structure of information sharedamong people or software components), and modelswould support the development of interoperable bioin-formatics processes. Although the informatics frameworkto support cancer biomarker discovery is still evolving,existing community and network-based efforts such asthe Cancer Biomedical Informatics Grid (caBIG) andthe EDRN (Early Detection Research Network) Knowl-edge System at the NCI have already defined many ofthe key components required to address challenges asso-ciated with cyber-infrastructure, such as data heterogene-ity, data integration, data analysis, and data sharing.The NCI meta-thesaurus system provides a model forsemantic mappings between representations. The workof these programs should be used as starting points for
Clin Cancer Res; 16(13) July 1, 2010 3305
h. 10, 2020. © 2010 American Association for Cancer

Khleif et al.
3306
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
a larger-scale standardization initiative to develop a setof common data standards in which the community ofresearchers has influence and input. The developmentof standards will require the participation and acceptanceof the biomedical research and regulatory communities,particularly at the interface between communities wheredifferent vocabularies, ontologies, data elements, anddata collection instruments currently exist. As the fieldis continually and rapidly changing, the end productmust be flexible enough to address evolving technical,analytic, and protocol requirements. A process for review-ing and amending the standards must also be developed.
Biospecimen annotation—Define a universal dataelement set to accompany all high-qualitybiospecimensThe lack of universal standards for biospecimen annota-
tion that meet the diverse needs of the various stakeholdersoften compromises the biomarker validation and qualifica-tion process. Currently, there is no consensus on estab-lished standards for the type or amount of clinical datathat should be collected for biospecimens, nor is there acommon vocabulary or formatting standards (as discussedin “Terminology”). Minimal and comprehensive data setsmust be defined and a template document should be gen-erated and provided to institutions. Defining a universal da-ta element set that should accompany all high-qualitybiospecimens would facilitate the collection and recordingof data at individual sites and set a universal template onwhich investigators and repositories could build. As elec-tronicmedical records (EMR) are developed and implemen-ted universally, these biospecimen data should be linked tothe clinical information contained in EMRs. A furtherchallenge in biospecimen annotation involves the lack ofstandardized labels to facilitate biospecimen identificationand tracking. A system for a legible, durable, coded label foreach sample with certain minimum information must bedefined. Forward progress will have to contend with com-plex cyber-infrastructure requirements as well as tackleintricate ethical and legal concerns such as informed con-sent, patient privacy, and intellectual property. Ultimately,standardized annotation of biospecimenswill increase theirresearch value by facilitating data sharing for comparisonamong studies and for consolidation of data from differentstudies. Universal standards for biospecimen annotationwill help ensure the quality of biospecimens and acceleratethe integrated cyber-infrastructure that is fundamental tothe advancement of personalized medicine.
Informed consent—Create a simple, standard, andefficient informed consent process and documentAnother major challenge to widespread use of biospeci-
mens in cancer research is the lack of a common informedconsent document (ICD) for use in biospecimen collection.Current ICDs vary substantially, in part because there is noconsensus on the definitions and terms related to biospeci-men collection. There is also a lack of agreement among sta-
Clin Cancer Res; 16(13) July 1, 2010
Researcon July clincancerres.aacrjournals.org Downloaded from
keholders regarding the level of detail to be included toadequately address genomic research issues and to explaincoding, confidentiality, and the “honest-broker-system” ina way that a majority of research participants can under-stand (17). A related problem is the process by which in-formed consent is obtained. Whereas studies have shownthat patients generally are willing to provide biospecimensfor research (18), the timing of introduction of the ICD tothe patient is important. Typically, consent is sought imme-diately before surgery when patients are more focused ontheir pending medical care and may be less willing to con-front complex consent issues in the limited time available.Broad-based consent programs are being tested at variousinstitutions across the country to address the many chal-lenges associated with the informed consent process. Con-sensus is needed on the elements to be contained in acommon ICD, and a template ICD should be generatedand provided to institutions and institutional reviewboards, along with recommendations on how to imple-ment the common ICD. Essential to the success of acommon ICD is the standardization of biospecimen termi-nology (as recommended above) and addressing issues ofpatient privacy (see below) and intellectual property rights.Widespread adoption of a simple, standard, and efficientICD and process has the potential to increase the numberof biospecimens collected, clarify authorized research usebased on participant choices, lessen the variability in insti-tutional review board rulings, and facilitate sharing of bios-pecimens and associated data among the cancer researchcommunity—all of which would facilitate biomarker re-search and development.
The CBC determined that steps must be taken to solvethe lack of standardization and harmonization in the afore-mentioned areas. Again, the CBC will facilitate progress byhelping appropriate agencies and organizations to developconsensus needed to achieve harmonization, develop stan-dards, and create template documents for use by the cancerresearch community. The CBC will also play a key role ineducating stakeholders about the existence and use of thesestandards and documents and can assist the community inaligning its efforts with the Department of Health andHuman Services (HHS) and other agencies. Resolution ofthese differences will greatly facilitate progress in the criti-cal areas described throughout this report, in particular an-alytic performance, biospecimens, and bioinformatics.Reconciling differences to achieve successful, broad-basedharmonization will be challenging because it will requireboth intellectual contribution and compromise on the partof multiple stakeholders.
Bioinformatics
The biomarker discovery and development cycle is adata-intensive enterprise where informatics capabilitiesand cyber-infrastructure play critical roles in the collec-tion, organization, management, and analysis of verylarge volumes of heterogeneous, unstructured data from
Clinical Cancer Research
h. 10, 2020. © 2010 American Association for Cancer

Advancing Biomarker Use in Cancer Drug Development
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
constantly evolving experimental modalities. Informaticssolutions need to ensure a cyber-infrastructure that pro-vides interoperability and data access to a diverse range ofstakeholders while simultaneously exhibiting flexibilityand robustness tomeet the rapidly evolving needs and tech-nological advances in instrumentations and procedures.The CBC recommends addressing challenges surroundingbiomarker bioinformatics by developing a universal set ofdata standards (see “Standardization and Harmoniza-tion”), implementing a common workspace for data shar-ing, and establishing a collection of use cases to guideeffective strategies for bioinformatics designs.
Common workspace—Implement a common workspacein a federated application environmentStandard infrastructure at most institutions is inadequate
for storing, moving, mining, and manipulating—inreal time—the terabytes worth of complex data generatedby -omics research approaches. As discussed above in“Standardization and Harmonization,” interoperability ofdiverse cyber-infrastructure and informatics tools is essen-tial to facilitate the exchange of data across platforms andacross institutions, and efforts such as caBIG and EDRNhave invested considerable time and effort toward this goal.A publicly accessible common workspace (or set of work-spaces) in a federated application environment wouldleverage individual efforts within the cancer research com-munity. The application environment must encompass thefull spectrum of informatics needs for biomarker discovery,validation, and qualification, facilitating the flow of data,information, and knowledge across each component ofthe pipeline. Further development and increased use of ca-BIG and EDRN is encouraged. A federated informatics sys-tem on a grid, rather than centralization of data andservices, is preferable for several reasons: the data sourcesare often federated; a grid supports community-member–initiated provision and discovery of supporting informaticsservices; and a grid supports open access and commercialsoftware developers as well as both public and private dataproviders. To ensure broad participation from stakeholders,these efforts must seek to address issues related to intellec-tual property in designing the commonworkspace and pro-vide for education of researchers.
Use cases—Establish a collection of use cases(i.e., working models) for biomarker development tofacilitate the development of appropriatebioinformatics toolsIn addition to being data-intensive, the biomarker dis-
covery and development cycle is neither fixed nor linear.Biomarker development strategies and study designs are de-termined by the intended clinical application and the typesof samples available or to be collected. Such designs and theassociated workflows influence the use of bioinformaticstools in the biomarker development process. To take intoaccount the unique attributes of an individual biomarkerstudy and the limitations of existing infrastructure availablefor that study, bioinformatics tools are often developed
www.aacrjournals.org
Researcon July clincancerres.aacrjournals.org Downloaded from
both ad hoc and de novo, neither of which is efficient. More-over, informatics developers may not be fully conversant inthe unique constraints, limitations, or compromises duringthe data collection process and, thus, may not account forthese when building the tools. Similarly, the researcherusing the tools may not fully understand the assumptionsinherent in many analytic algorithms that could bias theanalysis. The process from candidate biomarker to knownvalid biomarker requires a bioinformatics platform thatcan support the needs of discovery, validation, and qualifi-cation. A collection of use cases will help address the dis-connect between the tool maker and the tool user. Thiseffort should include both academic and industry stake-holders in order to achieve a smooth transition along thediscovery-development pipeline.
The above CBC recommendations are designed to ad-vance the biomarker bioinformatics field by enhancingefficiency through standardizing and reducing duplica-tive efforts. Large-scale implementation of cyber-infra-structure to support biomarker research will requireinstitutional commitments to adopt new technologies,to train new scientists in its deployment and use, andto share information technology resources and dataavailable through them.
Collaboration and Data Sharing
Most stakeholders agree that working collaboratively andsharing data and resources would speed biomarker discov-ery and development; however, the need to establish viable,profitable business models is at times in direct conflict withsuch an approach. Discovering, validating, and qualifyingbiomarkers is costly, and companies are often unwillingto take the investment risk unless they can be assured of in-tellectual property protection as a means of maximizingtheir return on investment. Additionally, researchers inmany academic institutions need to independently publishtheir novel findings to be considered for promotion. Devel-oping protected environments to share data and resourcesand incentivizing collaboration are critical to acceleratingprogress in biomarker use.
Pre-competitive consortium—Form a modelpre-competitive consortium to facilitate sharingscientific information and research operationsTo obtain the broadest intellectual property protection
in the form of worldwide patents, information must re-main undisclosed to the public until the appropriate pat-ent applications have been filed. This nondisclosurerequirement conflicts with the need to publish and freelyshare information among individuals, institutions, public-private partnerships, and consortia in a timely manner toavoid duplication of effort and to build rapidly on thegrowing knowledge base. The semiconductor industryprovides precedence for a successful cooperative and col-laborative pre-competitive consortium that can facilitatescientific information sharing and research collaboration
Clin Cancer Res; 16(13) July 1, 2010 3307
h. 10, 2020. © 2010 American Association for Cancer

Khleif et al.
3308
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
(19). The structuring of such a precompetitive consortiumwould require standard agreements and establishedboundaries so that companies, sponsors, and developerscan share their data without fear of jeopardizing future in-tellectual property rights. Stakeholders would need toidentify scientific opportunities for sharing data, and astructure and business plan for a precompetitive consor-tiumwould need to be developed. Defining and expandingthe precompetitive space, where benefits of informationsharing outweigh the competitive risks, would facilitatethe biomarker development process and allay antitrustconcerns arising from industry consortia. Sharing failedbiomarker development experiences, for example, wouldprovide precompetitive advantages for all members.
Incentives—Develop incentives to encouragecollaborations among drug sponsors, clinical researchsponsors, and regulatory authoritiesSharing biomedical research and health care data is vital,
and many efforts have addressed the technical approachesto data sharing for willing parties. However, these effortsmust also be complemented by appropriate ethical, legal,and social frameworks. Some communities, notably thegenomics, structural biology, and clinical trials communi-ties, have established policies and practices to facilitate da-ta sharing, but few have focused on incentives for keystakeholders to encourage innovation and enhance colla-borations among drug sponsors, clinical research sponsors,and regulatory authorities. The necessary incentives willvary depending on the risk (real or perceived) of sharingdata. Well-designed incentives should have immediatebenefit, especially for those individuals who are judgedon recent performance. Potential economic, strategic, logis-tic, or legislative incentives and disincentives must be iden-tified and a priority list of opportunities for providing theseincentives should be generated along with recommenda-tions to appropriate organizations for implementation. In-creasing data sharing and collaboration will improve thespeed with which biomarkers can be validated and incor-porated in clinical research and clinical practice.
Public accessibility of biospecimen data—Encouragecontribution of biospecimen methods data andexperimental data to public databasesBroader accessibility to biospecimen research protocols
and data through public databases would prevent duplica-tion of efforts by minimizing the need for investigators toconduct optimization studies that have been completed byothers. Making biospecimen data collected with publicfunds publicly available could be accomplished by furtherdeveloping and encouraging the use of the BiospecimenResearch Database (BRD) established by the NCI Officeof Biorepositories and Biospecimen Research. BRD is asearchable, web-based curation tool designed to help in-vestigators maximize the quality and utility of biospeci-mens by analyzing existing data on how biospecimensare affected by pre-analytic handling variables such as ac-quisition, processing, storage, and distribution. The data-
Clin Cancer Res; 16(13) July 1, 2010
Researcon July clincancerres.aacrjournals.org Downloaded from
base is being populated with evidence curated frompublished studies, unpublished results, and ongoingBRD experimentation. Additionally, methods informationfrom industry submissions to the FDA will populate theBRD. Wider adoption of caBIG would also improve inter-operability and would promote accessibility of biospeci-men research data for laboratories worldwide.
The CBC itself is composed of members representingsectors facing the conflicts associated with data sharingand is thus positioned to educate and engage the cancerresearch community across all levels to define ways tocollaborate productively.
Regulatory Issues
In the area of biomarkers, as with any burgeoningfield, clarity, transparency, and direction from regulatoryagencies are essential to help industry, to avoid confu-sion, and to efficiently meet regulatory requirements forapproval or clearance of medical products. Althoughdraft guidances have been put forth in some relevantareas and interest has been expressed for guidances inother areas, many regulatory processes have not yet beendeveloped for this rapidly evolving field. This may beone factor contributing to the speed of integration of bio-markers into the drug development process. Regulatoryagencies such as FDA will need to continue to provideclear direction to the cancer research community thatprovides the stability in the regulatory process necessaryfor industry participation. The CBC believes it is importantfor regulatory agencies to continue to issue guidance docu-ments onmultiple aspects of the biomarker process, includ-ing codevelopment, labeling, composite biomarkers, andnovel trial designs.
Codevelopment guidance—Develop best practices oncodevelopment of therapeutics and diagnosticsCodevelopment of biomarker diagnostics and therapeu-
tics will involve complex interactions between investiga-tors with different skill sets as well as between differentregulatory work groups—for example, the FDA Centerfor Devices and Radiological Health (CDRH) and theCenter for Drug Evaluation and Research (CDER) or theCenter for Biologics Evaluation and Research (CBER)—applying different regulatory statutes. In addition to con-cerns over harmonizing the work done under differentregulatory systems (i.e., outside of the United States), therehave been concerns about how sponsors should interactwith the FDA when biomarker assays require clearance ver-sus approval, and what administrative and evidentiarystandards apply to new biomarker development, particular-ly those connected to drug use. The FDA issued draft guid-ance in 2005 (20), providing a starting point for discussionof the numerous issues involved in this complex area; how-ever, further clarification is needed. A best practices docu-ment on codevelopment that addresses the scientific,
Clinical Cancer Research
h. 10, 2020. © 2010 American Association for Cancer

Advancing Biomarker Use in Cancer Drug Development
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
regulatory, and administrative issues that are important forbringing new biomarkers to market is warranted.
Evidentiary standards—Develop best practices onevidentiary standards for changes in drug labelingand developing companion diagnosticsThe inclusion of pharmacogenomics information in
FDA-approved drug labels is increasing (21). When theFDA introduced a series of labeling changes to includenew pharmacogenomic information in drug labeling forat least three new biomarkers (e.g., CYP450 2D6/2C19,UGT1A1, and CYP450 2C9/VKORC1), it prompted the de-velopment of new FDA-cleared diagnostics for these bio-markers. It should be noted that although the FDA haschanged labels based on evidence, it does not require thatthe biomarker assays be approved or cleared. This nascentarea is in need of clarification from regulatory agencies withregard to the kinds of pharmacogenomic information thatare needed on both drug and diagnostic test labels and theevidentiary standards that should be applied when makingchanges to drug labels in the future. A best practices docu-ment based on case studies that discusses the evidentiarythresholds needed to inform a drug label change for addingnew biomarker information; whether evidentiary thresh-olds should vary with biomarker use as described in thedrug label; and possible approaches to assess the risk ofthe biomarker assay to determine its regulatory path (see“Regulatory Policy” below) could expedite progress in thisarea. Clarification of the similarities or differences betweenFDA-mandated data requirements and those used by payersand health care providers in setting standards for qualitycare is also needed to promote smooth integration of newbiomarkers into clinical practice.
Composite biomarkers—Develop best practices forbiomarker assays based on a composite of multipleindividual biomarkersA composite of numerous biomarkers, each individually
identified with respect to its significance to various endpoints, can be more predictive and accurate collectivelythan individual markers. However, biomarker assays devel-oped from amultiplicity ofmeasurements introduce specif-ic scientific questions related to analytic validation. Forexample, the statistical significance assigned to eachmarkerindividually should take into account the multiplicity interms of the large number of other markers that were alsoanalyzed. Even when the number of markers is small, whatconstitutes appropriate evaluation of a composite marker isunclear. Additionally, there is uncertainty with regard towhen it is appropriate to report only the composite markerresult versus all individual biomarker results in addition tothe composite results. Clarification on how regulatory deci-sions will be made for biomarker assays based on a com-posite of multiple individual markers should address thecurrent situation. Careful consideration of appropriatemethodologies and techniques for testing new signaturesand identification of areas of particular concern for properanalytic validation of composite biomarkers will help the
www.aacrjournals.org
Researcon July clincancerres.aacrjournals.org Downloaded from
cancer research community more rapidly identify and vali-date real and useful biomarkers.
Retrospective study designs for clinical qualification—Develop best practices for retrospective-prospectivestudy designs for clinical qualification of biomarkersFor new biomarkers to rapidly enter clinical practice, it
may not always be desirable or necessary to await the com-pletion of long-term prospective studies. In some cases, itmay be possible to provide interim credentialing of thebiomarker using archived samples from external samplebanks, recent randomized clinical trials, or both to identifybiomarkers for certain intended uses. It may then be pos-sible to build from an initial study to strengthen claimsand understanding of its clinical relevance by addingsamples from a well-studied cohort or by initiating a morerobust prospective study. At least two biomarker assays—the Oncotype Dx (22, 23) by Genomic Health and theMammaPrint (24, 25) by Agendia, both for breast cancerprognosis—have been brought to the market based ondata gathered in this manner. Using banked samples, clin-ical studies of both assays provided preliminary estimatesof clinical relevance, and both are the subject of ongoing,more extensive prospective trials to further establish per-formance. Retrospective studies can present limitations.For example, populations studied retrospectively may betoo narrow for broad application of results, or samplesidentified and studied may represent either conveniencesample collections or banks with collection bias. A guid-ance document on clinical qualification of biomarkersthat addresses the numerous issues that must be consid-ered when applying retrospective studies to regulatorydecision making will help the cancer community navigatethis area in the most expeditious manner. A best practicesdocument that describes several approaches to the use ofretrospective-prospective trial designs and archived speci-mens in the evaluation of predictive biomarkers andaddresses the tradeoffs of traditional comprehensive de-signs with the potential increase in speed of new studydesigns is warranted; one such document was recentlypublished (26). If designed and implemented properly,retrospective studies can be highly beneficial in enablingmore rapid and parsimonious development of biomarkersand more rapid clinical uptake.
Adaptive clinical trial designs—Develop best practiceson adaptive clinical trial designs for using biomarkersin drug developmentThe use of biomarkers for early forecasting with regard to
study parameters and study end points may create a need torevisit the traditional four-phase sequential models used inthe process of drug development. Adaptive clinical trial de-signs allow for changes to a study in progress based on in-terim results, with the goal of streamlining and enhancingthe study without losing scientific rigor. Whereas there is agrowing literature base on adaptive designs (27, 28), andthe FDA and other groups have growing experience withthe use of enrichment studies (see below), to date there
Clin Cancer Res; 16(13) July 1, 2010 3309
h. 10, 2020. © 2010 American Association for Cancer

Khleif et al.
3310
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
has been no consensus generated on which approachesmight work best or specifically enunciating good practicesfor this process. Best practices in the use of adaptive clinicaltrial designs as they apply to both drugs and diagnostic de-vices used in the codevelopment process should be defined.A best practices document should include a road map forintroduction of adaptive designs, including specific exam-ples for modeling application of the methodology, shouldidentify situations in which adaptive designs are of par-ticular value, and may move beyond the traditional drug-diagnostic codevelopment model to consider prognosticuse of biomarkers and novel designs for promoting theseuses. It is hoped that such designs will foster rapid develop-ment of new drug-diagnostic combinations.
Alternative prospective trials—Develop best practiceson alternative prospective trial designs forcompanion diagnosticsProspective trials for new drug-diagnostic combinations
can be performed in a variety of configurations. Random-ization in such prospective studies may be performed bybiomarker status, by treatment status, or by sequential ran-domization of both. The FDA has historically requestedclinical trial studies in which the drug and diagnostic inter-actions are well established; however, an increasingly re-quested and applied alternative design is one in whichan enriched patient population (e.g., only biomarker pos-itive) is studied with the therapeutic (27, 28). This ap-proach allows rapid accumulation of data to support theapproval of the therapeutic and device in parallel and al-lows the biomarker-drug combination product to move tomarket relatively quickly to benefit the identified subset ofthe population. However, this type of trial cannot assessdrug effectiveness in biomarker negative patients. It alsodoes not provide for evaluation of diagnostic sensitivityor specificity of the bioassay or the predictive value of anegative result. Among the requisites discussed at a recentNCI-FDA-Industry Workshop (29) for when an enrichedpatient study would be useful in establishing the safetyand efficacy are a well-established biomarker assay and aclear understanding of the biology of the biomarker andits relationship to the target(s) of interest. Although theseseem like reasonable requirements and the difficulties offull population (all-comers) studies are easy to recognize,the issue remains highly contentious. The lack of consensuswithin the cancer community underscores the need for bestpractices that will address the disconnection between thescientific and regulatory requirements for enriched designsand identify the circumstances that warrant enrichmentstudies to evaluate the clinical relevance of biomarkers.
The unique ability of the CBC to convene a compre-hensive group of stakeholders enables the CBC to helpdevelop consensus documents that will address some ofthe outstanding regulatory issues related to biomarkerdevelopment and speak to the concerns of the cancercommunity. Such information should assist regulatoryagencies in developing the necessary guidance docu-
Clin Cancer Res; 16(13) July 1, 2010
Researcon July clincancerres.aacrjournals.org Downloaded from
ments to provide stakeholders with much needed clarityand direction.
Stakeholder Education and Communication
As more information is generated, new standards are de-veloped, and new guidance documents are released, thereis a need to communicate this progress to various stake-holders and educate them about their potential rolesand about the importance of compliance with guidanceor adoption of new standards. To address this growingneed, the CBC plans to help coordinate the productionand dissemination of educational materials and other in-itiatives beginning with those areas deemed to be in themost immediate need of outreach: biospecimen collectionand use, the importance of analytic validation, and thespecifics of the regulatory process.
Biospecimen collection—Educate patients and healthcare providers about the value and need forbiospecimen collectionA significant factor undermining biospecimen collection
is the general lack of knowledge and awareness among pri-mary care physicians, patients, and families about the valueof biospecimen research in improving clinical practice andpublic health. In general, members of the public are morelikely to contribute biospecimens when they fully under-stand the benefits and are presented with the opportunityto do so (18). Without appropriate education, however,patients entering hospitals may view biospecimen collec-tion programs as being in competition with routine proce-dures that are part of health care, and may fear that theircare will be compromised if they consent to contributespecimens for research. Patients also may be sensitive toprivacy issues or have other concerns about the risks ofcontributing biospecimens to research. Educational initia-tives from patient advocacy groups and other communitiescould mitigate many of these concerns and increase the ac-ceptance of biospecimen collection. If health care providersare more aware of the relevance of biospecimen collection,they would be better able to participate in the education oftheir patients. Moreover, if patients and families better un-derstand the purpose of and need for biospecimen re-search, they may be more likely to choose to contribute.A successful public education effort must address issuesof public trust, alleviate individuals' concerns, and empha-size potential benefits. Education and increased awarenessof relevant stakeholders should increase the number ofbiospecimens contributed to research.
Analytic validation—Increase awareness andunderstanding of the importance of analyticvalidation and quality controlA number of professional organizations are addressing
issues of assay validation and analytic quality control,but considerable stakeholder education is still required toenable implementation of solutions for establishing goodlaboratory practice (GLP) and for reporting of the data by
Clinical Cancer Research
h. 10, 2020. © 2010 American Association for Cancer

Advancing Biomarker Use in Cancer Drug Development
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
cancer researchers. The cancer research community wouldbenefit from clear, specific information about analytic val-idation approaches—including the criteria of GLP that arerequisite for valid data and the measures for maintainingquality control assurance for the accuracy and reproducibil-ity of validated analytic methods—that have been devel-oped and recognized by academia, government, andindustry. Toward increasing awareness and understandingof the importance of analytic validation, educationalprogramming and other materials for all stakeholders re-garding drug and device regulations should be developed.Although it will require time for the complexities inherentin the basic principles of analytic validation to becomeproperly understood by the cancer research communityand for GLP to become more fully integrated into research,new educational forums on assay validation in cancer re-search will certainly facilitate robust credentialing of bio-markers for investigations, which will, in turn, lead tobetter cancer interventions.
Regulatory pathways—Educate stakeholders inregulatory pathways to accelerate codevelopment oftherapeutics and diagnosticsDrug, biologic, and device regulations are markedly dif-
ferent, in part because they are performed under differentlegislative mandates and because of cultural and adminis-trative differences among work units at the FDA. Drug sta-keholders tend to know less about device regulation andvice versa. If the field of codevelopment of therapeuticsand biomarkers is to move forward quickly, it is impera-tive that as much information as possible be shared withinterested stakeholders so that there is a clear and compre-hensive understanding of the regulatory processes for bothdrugs and devices. An enunciation of differences may helpoutside stakeholders better understand how to developnew products and may also assist the FDA and global reg-ulatory agencies in considering mechanisms for harmoniz-ing regulatory policies and finding mechanisms to ensurethat drug and diagnostic work is as consistent as possibleunder existing regulations and statutes. The FDA alreadyhas useful educational materials for explaining regulatorypolicy, including a yearly workshop and web-based andprinted materials; however, many stakeholders currentlyare not aware of them or do not use them consistently.Thus, additional efforts and alternative approaches mustbe taken to reach the intended audiences. This would re-quire a commitment of time and resources on the part ofthe regulatory agencies to create educational videos andother materials on the various regulatory pathways, andnumerous outside organizations and additional venuescould be utilized to provide the FDA and other regulatoryagencies with the greatest opportunities for knowledgesharing. These and other efforts to communicate the spe-cific regulatory requirements should help accelerate code-velopment of therapeutics and diagnostics.
Stakeholder education and communication are areas ofongoing need in the dynamic biomarker field, and are
www.aacrjournals.org
Researcon July clincancerres.aacrjournals.org Downloaded from
particular strengths of the AACR. The CBC will leverageAACR venues, including its numerous scholarly publica-tions, the CR advocacy magazine, its Annual Meeting andmany other international meetings, educational work-shops, and website resources to educate and engage thesestakeholders and the general public.
Science Policy
A final area for consideration for the advancement ofbiomarker use in drug development is science policy. It istypical for the discoveries and applications of a rapidly ad-vancing and evolving scientific discipline to outpace thenecessary policy development that protects public healthand safety. This is certainly the case for the role of biomar-kers in the drug development process. Given the potentialfor biomarkers to improve and accelerate the drug develop-ment process and the subsequent delivery of quality care topatients, it is vitally important to develop policies that alsocultivate innovation while safeguarding the public. TheCBC has identified several areas in which current policiesfall short of promoting biomarker development, includinglaboratory-developed tests, in vitro diagnostic multivariateindex assays, reimbursement, and the Privacy Rule of theHealth Insurance Portability and Accountability Act (HI-PAA). The CBC believes it is important that relevant federalagencies engage in a process to address these areas and takenecessary action through regulatory or statutory changes.
Regulatory policy—Identify areas and/or processes thatcould enhance the environment for biomarkerdevelopmentThere is a dichotomy between the approval pathways for
commercially marketed laboratory diagnostic tests at theFDA and at the Centers for Medicare and Medicaid Services(CMS) under CLIA. Before entering the marketplace, theFDA review process assures that new assays have been val-idated for both analytic and clinical performance and haveadequate instructions for use. Alternatively, when individ-ual laboratories develop assays for use at their own uniquesite, called laboratory-developed tests (LDT) or “home-brew” tests, the laboratories are subject to CMS regulatoryoversight under CLIA, which requires that, at the time of ascheduled inspection, assays developed during the reviewcycle are subject to ad hoc sampling to assure analytic va-lidity and quality control. Although there is nothing to pre-clude laboratories from establishing clinical relevance fornew LDTs, CLIA does not mandate this requirement and,for this reason, is perceived as a less burdensome pathwayfor rapid promulgation of new tests. Despite commonpractice, the FDA has viewed LDTs as medical devices sub-ject to FDA oversight, but has traditionally applied enforce-ment discretion and not actively regulated them. In 2004,however, the FDA formally recognized a subtype of LDTsthat involve integration of multiple signals into a compos-ite clinical result, categorized as in vitro diagnostic multi-variate index assays (IVDMIA). FDA published draftguidance that defined this niche set of LDTs and clarified
Clin Cancer Res; 16(13) July 1, 2010 3311
h. 10, 2020. © 2010 American Association for Cancer

Khleif et al.
3312
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
its authority to regulate them (30), thereby creating greatuncertainty in the industry. In 2008, in response to acharge from the U.S. Department of Health and HumanServices Secretary, the Secretary's Advisory Committee onGenetics, Health, and Society (SACGHS) evaluated federaloversight of genetic tests and recommended that the FDAconsider regulating all LDTs on a risk-defined basis to as-sure clinical relevance and public health safety (31). Giventhe considerable, ongoing debate surrounding this issue(32), independent input from a diverse group of stake-holders on the IVDMIA guidance, the SACGHS recom-mendations, and other relevant sources would add auseful voice and broad-based perspective to the ongoingdialogue in this complex and controversial area, withthe goal of helping regulators move forward the publichealth agenda in support of personalized medicine.
Reimbursement policy—Explore ways to improvereimbursement for biospecimen handling anddiagnostic testsDiscussed above were some of the many challenges in
biospecimen procurement, such as the need for high-quality samples, proper annotation, and patient educa-tion. Pathologists are central to the process, yet there islittle incentive for them to participate in biospecimenprocurement for research. An additional change to cur-rent policy that would increase the collection of high-quality biospecimens is the establishment of a billingcode and reimbursement rate for pathologists' handlingof biospecimens. There is a need for improvement ofthe reimbursement process for diagnostic tests as well,as billing codes are often not sufficiently specific for nov-el biomarker assays and the reimbursement rates forthese tests often do not reflect their value. By providingincentives for key stakeholders and setting precedent forother third-party payers' coverage and reimbursement de-cisions, adequate CMS reimbursement for biospecimenhandling and diagnostic tests would accelerate the wide-spread use of biomarker assays in clinical settings.
HIPAA—Address the barriers to biomarker researchproduced by the HIPAA Privacy RuleHospitals, health plans, and other U.S. organizations
that handle medical records and samples must complywith the Privacy Rule of the HIPAA of 1996. Implementedto protect the privacy of an individual's health informa-tion, HIPAA provisions also have unintentionally affectedthe performance of biomedical research, including cancerbiomarker studies. In many instances, access to existingbiospecimen collections and the acquisition of new bio-logical samples have been hampered by current interpre-tation of HIPAA law. Also, the informed consent process isinfluenced by these federal stipulations, as are the ways inwhich researchers are permitted to share data and thetypes of data that can be shared. It is important that a thor-ough evaluation of the impact of HIPAA provisions on bio-marker research be conducted. The Institute of Medicine(IOM) recently published a report “Beyond the HIPAA
Clin Cancer Res; 16(13) July 1, 2010
Researcon July clincancerres.aacrjournals.org Downloaded from
Privacy Rule: Enhancing Privacy, Improving Health throughResearch” (33), which identifies issues and problems withinterpretation of HIPAA regulations as they pertain to re-search. This new report could serve as a starting point fordiscussions on how to overcome the unintended restric-tions, including those that may be perceived, of the PrivacyRule.
The policy areas discussed in this section, as well as pos-sible legislative incentives (or disincentives) to encouragecollaborations (see “Collaboration and Data Sharing”),hold clear opportunities to initiate change that would ac-celerate biomarker research. The CBC is uniquely suited toserve as a resource for these agencies by assessing therange of stakeholder perspectives, collecting and synthe-sizing information, and ultimately, providing recommen-dations for effective policy changes with respect to areas inneed of further exploration and attention. In addition, theAACR government relations and science policy capacity,along with its network of patient advocacy groups, will al-low it to advocate for necessary legislative, regulatory, orother process and policy changes relevant to biomarkerdevelopment. The CBC intends to leverage the importantongoing efforts of other organizations engaged in similarinitiatives as well.
Summary
The AACR-FDA-NCI Cancer Biomarkers Collaborative isa stakeholder-driven effort to inform and accelerate the FDACritical Path Initiative and the work of the broader cancercommunity. CBC committees identified eight critical areasfor biomarker development—biospecimens, analytic per-formance, standardization and harmonization, bioinfor-matics, collaboration and data sharing, regulations,stakeholder education and communication, and sciencepolicy—and put forward 27 recommendations with corre-sponding action plans to address and overcome barriers ineach of these areas. CBC recommendations address theneed to develop and apply quality standards, criteria, andsystems for biospecimens and biomarker assay validation;to create a supportive bioinformatics platform and a systemfor harmonizing terminology and standards; to identify in-centives for following standards and sharing data; and toeducate and improve awareness among stakeholders andthe public.The CBC serves as a valuable resource for the FDA, NCI,
and other organizations, agencies, and individuals in the can-cer research community. Through its work, the CBC hasbrought to the forefront many key issues with regard to bio-marker development that need to be addressed. It has con-vened stakeholders from around the world to developconsensus on these important issues and continues to seekU.S. and international input. Furthermore, the CBC servesas a catalyst to initiate collaborative projects to implement so-lutions to improve biomarker validation and integration intoclinical trials and, ultimately, into clinical use. Collectively,these efforts should not only improve the treatment of cancer
Clinical Cancer Research
h. 10, 2020. © 2010 American Association for Cancer

Advancing Biomarker Use in Cancer Drug Development
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
but also lead to advances in the treatment of other diseases inwhich biomarkers increasingly play important roles.TheCBCwill rely on the ongoing, active participation of a
broad spectrum of stakeholders to continue its work to ac-celerate progress along the critical path in oncology drug de-velopment and will leverage and complement the ongoingefforts of numerous other groups. Successful integration ofbiomarker research and cancer drug development will re-quire that all sectors engage, collaborate, and comply withbest practices and guidance. Success also requires that edu-cational efforts result in changes in attitudes, such as stake-holder compliance with standards or patient involvement.Importantly, success requires overall collaboration—whether to build and contribute to national common re-sources or to share data, a willingness of all stakeholdersto engage is essential. While other groups have identifiedsimilar barriers to biomarker use, the CBC intends to takeaction and help lead the cancer community in the joint for-ward movement that is necessary to surmount the barriersby changing the current inefficient paradigms. The recom-mendations described within this report aim to acceleratethe speed with which biomarkers can be used to fulfill theirgreat promise to the personalized medicine revolution thatcancer patients so critically await.
AACR-FDA-NCI Cancer BiomarkersCollaborative
Chairpersons
William N. Hait, M.D., Ph.D.Ortho Biotech Oncology Research & DevelopmentJohnson and Johnson Family of CompaniesRaritan, NJ
Samir N. Khleif, M.D.4
National Cancer InstituteBethesda, MD
James H. Doroshow, M.D.National Cancer InstituteBethesda, MD
Assay Validation Committee
Steven I. Gutman, M.D., Lead Co-Chairperson4
Blue Cross and Blue Shield AssociationWashington, DC
Peter E. Barker, Ph.D., Co-ChairpersonNational Institute of Standards and TechnologyGaithersburg, MD
Nicholas C. Dracopoli, Ph.D., Co-Chairperson4
Centocor, Inc.Radnor, PA
Alberto Gutierrez, Ph.D., Co-ChairpersonFood and Drug AdministrationRockville, MD
www.aacrjournals.org
Research. on July 10clincancerres.aacrjournals.org Downloaded from
Steven J. Skates, Ph.D., Co-ChairpersonMassachusetts General HospitalBoston, MA
M.J. Finley Austin, Ph.D.Hoffman-La RocheNutley, NJ
Robert C. Bast, Jr., M.D.UT M.D. Anderson Cancer CenterHouston, TX
Robert L. Becker, Ph.D.Food and Drug AdministrationRockville, MD
Donald A. Berry, Ph.D.UT M.D. Anderson Cancer CenterHouston, TX
Linda A. Bradley, Ph.D.4
Women & Infants Hospital of Rhode IslandGray, ME
Peter F. Bross, M.D.Food and Drug AdministrationRockville, MD
Mark Chang, Ph.D.Millennium Pharmaceuticals, Inc.Cambridge, MA
Adam Michael Clark, Ph.D.4
Lance Armstrong Healthcare FoundationAustin, TX
Viswanath Devanarayan, Ph.D.Abbott LaboratoriesParsippany, NJ
Lynn G. Dressler, Dr.P.H.UNC-Chapel HillChapel Hill, NC
David B. Endres, Ph.D.USC-Keck School of MedicineLos Angeles, CA
Russel K. Enns, Ph.D.CepheidSunnyvale, CA
Fred J. FrulloBristol-Myers Squibb CompanyPrinceton, NJ
Courtney C. HarperFood and Drug AdministrationRockville, MD
Daniel F. Hayes, M.D.University of Michigan Cancer CenterAnn Arbor, MI
Clin Cancer Res; 16(13) July 1, 2010 3313
, 2020. © 2010 American Association for Cancer
Khleif et al.
C3314
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
M. Carolina Hinestrosa, M.A., M.P.H.5
National Breast Cancer CoalitionWashington, DC
Lois Hinman, Ph.D.Novartis Pharmaceuticals CorporationEast Hanover, NJ
Andrew Hruszkewycz, M.D., Ph.D.National Cancer InstituteBethesda, MD
Pearl S. Huang, Ph.D.Merck & Co.North Wales, PA
J. Milburn Jessup, M.D.National Cancer InstituteBethesda, MD
Malik E. Juweid, M.D.University of Iowa, College of MedicineIowa City, IA
Francis Kalush, Ph.D.Food and Drug AdministrationRockville, MD
Karen L. Kaul, M.D., Ph.D.4
NorthShore University HealthSystemEvanston, IL
Gary Kelloff, M.D.National Cancer InstituteRockville, MD
George G. Klee, M.D., Ph.D.Mayo Clinic and FoundationRochester, MN
Walter H. Koch, Ph.D.Roche Molecular SystemsPleasanton, CA
Steven Lemery, M.D.Food and Drug AdministrationSilver Spring, MD
Joan B. Levy, Ph.D.Multiple Myeloma Research FoundationNorwalk, CT
Elizabeth Mansfield, Ph.D.Food and Drug AdministrationRockville, MD
Karen M. MaureyNational Cancer InstituteRockville, MD
George B. Moseley III, MBA, JDHarvard School of Public HealthBoston, MA
lin Cancer Res; 16(13) July 1, 2010
Research. on July 10clincancerres.aacrjournals.org Downloaded from
Richard NaplesBecton, Dickinson and CompanyFranklin Lakes, NJ
James P. Omel, M.D.Central Nebraska Multiple Myeloma Support GroupGrand Island, NE
Michael S. Orr, Ph.D.Food and Drug AdministrationSilver Spring, MD
Gene A. Pennello, Ph.D.Food and Drug AdministrationRockville, MD
William J. PignatoGenentech, Inc.South San Francisco, CA
David F. Ransohoff, M.D.UNC-Chapel HillChapel Hill, NC
Laura H. Reid, Ph.D.4
Conatus Consulting, LLCRaleigh, NC
Henry Rodriguez, Ph.D., MBANational Cancer InstituteBethesda, MD
Richard L. Schilsky, M.D.University of ChicagoChicago, IL
Robert SchuerenGenentech, Inc.South San Francisco, CA
Richard M. Simon, D.Sc.National Cancer InstituteBethesda, MD
Patrick M. Sluss, Ph.D.Harvard Medical SchoolBoston, MA
John J. Sninsky, Ph.D.Celera DiagnosticsAlameda, CA
Sudhir Srivastava, Ph.D.National Cancer InstituteRockville, MD
Sheila E. Taube, Ph.D.4
ST-ConsultingBethesda, MD
Jeremy M.G. Taylor, Ph.D.University of MichiganAnn Arbor, MI
Clinical Cancer Research
, 2020. © 2010 American Association for Cancer

Advancing Biomarker Use in Cancer Drug Development
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
Laura J. van't Veer, Ph.D.4
The Netherlands Cancer InstituteAmsterdam, the Netherlands
Lakshmi Vishnuvajjala, Ph.D.Food and Drug AdministrationRockville, MD
Sue-Jane Wang, Ph.D.Food and Drug AdministrationSilver Spring, MD
Janet A. Warrington, Ph.D.Affymetrix, Inc.Santa Clara, CA
Michael S. Watson, Ph.D., FACMGAmerican College of Medical GeneticsBethesda, MD
Russell S. Weiner, Ph.D.Bristol-Myers Squibb CompanyLawrenceville, NJ
Judy Yost, M.A., M.T.Centers for Medicare and Medicaid ServicesBaltimore, MD
Bioinformatics Committee
Gunaretnam Rajagopal, Ph.D., Lead Co-Chairperson4
Cancer Institute of New JerseyNew Brunswick, NJ
Kenneth H. Buetow, Ph.D., Co-ChairpersonNational Cancer InstituteBethesda, MD
Weida Tong, Ph.D., Co-ChairpersonFDA National Center for Toxicological ResearchJefferson, AR
Greg Tucker-Kellogg, Ph.D., Co-ChairpersonLilly Singapore Centre for Drug DiscoverySingapore
J. Robert Beck, M.D.Fox Chase Cancer CenterPhiladelphia, PA
Barbara M. Bryant, Ph.D.4
Constellation PharmaceuticalsCambridge, MA
Daniel Crichton, M.S.NASA Jet Propulsion LaboratoryPasadena, CA
Paula KimTranslating Research Across Communities NetworkFallbrook, CA
Martin W. McIntosh, Ph.D.Fred Hutchinson Cancer Research CenterSeattle, WA
www.aacrjournals.org
Researcon July clincancerres.aacrjournals.org Downloaded from
Timothy O'Leary, M.D., Ph.D.U.S. Department of Veterans AffairsWashington, DC
Michael S. Orr, Ph.D.Food and Drug AdministrationSilver Spring, MD
Joel H. Saltz, M.D., Ph.D.Ohio State UniversityColumbus, OH
Weichung Joe Shih, Ph.D.Cancer Institute of New JerseyNew Brunswick, NJ
Nathan Siemers, Ph.D.Bristol-Myers Squibb CompanyPrinceton, NJ
John SpeakmanNational Cancer InstituteRockville, MD
Patty SpearsPatient AdvocateRaleigh, NC
Sudhir Srivastava, Ph.D.National Cancer InstituteRockville, MD
Blaze A. Stancampiano4
Booz Allen HamiltonWashington, DC
Zhen Zhang, Ph.D.Johns Hopkins UniversityBaltimore, MD
JoAnne Zujewski, M.D.National Cancer InstituteBethesda, MD
Biospecimens Committee
Carolyn Compton, M.D., Ph.D., Lead Co-ChairpersonNational Cancer InstituteBethesda, MD
Brian Holloway, Ph.D., Co-ChairpersonAstraZeneca PharmaceuticalsMacclesfield, United Kingdom
Scott D. Jewell, Ph.D., Co-ChairpersonOhio State UniversityColumbus, OH
Elizabeth Mansfield, Ph.D., Co-ChairpersonFood and Drug AdministrationRockville, MD
Kerry L. Blanchard, M.D., Ph.D.Eli Lilly & CompanyIndianapolis, IN
Clin Cancer Res; 16(13) July 1, 2010 3315
h. 10, 2020. © 2010 American Association for Cancer

Khleif et al.
C3316
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
L. Mark Cosentino, DPM, Ph.D.Science Applications InternationalCorporation-Frederick, Inc.Frederick, MD
Kerstin A. David, Ph.D.Indivumed GmbHHamburg, Germany
Maryellen de Mars, Ph.D.The Critical Path InstituteRockville, MD
Lynn G. Dressler, Dr.P.H.UNC-Chapel HillChapel Hill, NC
Ian M. Fore, Ph.D.National Cancer InstituteRockville, MD
Patricia GoldmanOvarian Cancer National AllianceWashington, DC
Elizabeth H. Hammond, M.D.University of Utah School of MedicineSalt Lake City, UT
Richard G. Hegele, M.D., FRCPC, Ph.D.4
University of TorontoToronto, Ontario
Hartmut H. Juhl, M.D., Ph.D.Indivumed GmbHHamburg, Germany
Irina A. Lubensky, M.D.National Cancer InstituteRockville, MD
Glenn A. Miller, Ph.D.Genzyme Analytical ServicesWestborough, MA
Brian P. Mullaney, M.D., Ph.D.Eli Lilly & CompanyIndianapolis, IN
Reena Philip, Ph.D.Food and Drug AdministrationRockville, MD
Stephen J. Qualman, M.D.5
Children's Hospital Research InstituteColumbus, OH
Elizabeth M. Rohlfs, Ph.D.Genzyme Analytical ServicesWestborough, MA
Mark E. Sobel, M.D., Ph.D.American Society for Investigative PathologyBethesda, MD
lin Cancer Res; 16(13) July 1, 2010
Researcon July clincancerres.aacrjournals.org Downloaded from
Howard M. Stern, M.D., Ph.D.Genentech, Inc.South San Francisco, CA
Elizabeth A. Thompson4
Susan G. Komen for the CureDallas, TX
Information Sharing Committee
George D. Demetri, M.D., Lead Co-ChairpersonDana-Farber Cancer InstituteBoston, MA
Kapil Dhingra, M.B.B.S., Co-Chairperson4
KAPital Consulting LLCSparta, NJ
Gary J. Kelloff, M.D., Co-ChairpersonNational Cancer InstituteRockville, MD
Richard Pazdur, M.D., Co-ChairpersonFood and Drug AdministrationSilver Spring, MD
Martin J. Adelman, M.S., J.D.George Washington UniversityWashington, DC
Jeffrey Alexander, Ph.D.Washington CORE LLCBethesda, MD
J. Carl Barrett, Ph.D.Novartis Institutes for BioMedical ResearchCambridge, MA
David D. Chang, M.D., Ph.D.Amgen, Inc.Thousand Oaks, CA
John M. Engel, Esq.Engel & Novitt, LLPWashington, DC
Cindy Geoghegan4
Patient and Partners LLCWilton, CT
David S. Grayzel, M.D.Infinity Pharmaceuticals, Inc.Cambridge, MA
Louise Barnett Grochow, M.D.AstraZeneca PharmaceuticalsWaltham, MA
Josephine Johnston, LLB, MBHLThe Hastings CenterGarrison, NY
Sara Kenkare-Mitra, Ph.D.Genentech, Inc.South San Francisco, CA
Clinical Cancer Research
h. 10, 2020. © 2010 American Association for Cancer

4 DrasioGuDBrGAwaAnBeatFrSiMMMCAwa5 D
Advancing Biomarker Use in Cancer Drug Development
w
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
David Pensak, Ph.D.V.i. Laboratories, Inc.Wilmington, DE
uring the planning and implementation of the CBC's work and prepa-tion of the manuscript, Dr. Khleif was Special Assistant to the Commis-ner at the U.S. Food and Drug Administration, Rockville, MD; Dr.tman was at the U.S. Food and Drug Administration, Rockville, MD;
r. Dracopoli was at Bristol-Myers Squibb Company, Princeton, NJ; Dr.adley was at the Centers for Disease Control and Prevention, Atlanta,; Dr. Clark was at the National Cancer Institute, Bethesda, MD; Dr. Kauls at Northwestern University, Evanston, IL; Dr. Reid was at Expressionalysis, Inc., Durham, NC; Dr. Taube was at the National Cancer Institute,thesda, MD; for some of this period, Dr. van't Veer was on sabbaticalUCSF Helen Diller Family Comprehensive Cancer Center, Sanancisco, CA; Dr. Rajagopal was at the Bioinformatics Institute ofngapore; Dr. Bryant was at Millennium Pharmaceuticals, Cambridge,A; Mr. Stancampiano was at AstraZeneca Pharmaceuticals, Waltham,A; Dr. Hegele was at the University of British Columbia, Vancouver, BC;s. Thompson was at the Pancreatic Cancer Action Network, El Segundo,; Dr. Dhingra was at Hoffmann-La Roche, Inc., Nutley, NJ;Ms. Geoghagens at the Susan G. Komen Breast Cancer Foundation, Wilton, CT.eceased.
ww.aacrjournals.org
Researcon July clincancerres.aacrjournals.org Downloaded from
Dominic G. Spinella, Ph.D.Pfizer, Inc.San Diego, CA
Gillian R. Woollett, M.A., D.PhilEngel & Novitt, LLPWashington, DC
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
The authors gratefully acknowledge the participants of the AACR-FDA-NCI Cancer Biomarkers Workshop and the members of the AACR-FDA-NCI Cancer Biomarkers Collaborative (CBC), in particular thecommittee chairpersons, for their insightful contributions to thisreport and the ongoing work of the CBC. Special thanks to Drs.Kimberly Sabelko, Pamela Bradley, and David Bernstein of theAACR for research, organizational support, and editorial assistance.
Received 04/06/2010; revised 05/03/2010; accepted 05/17/2010;published OnlineFirst 05/25/2010.
References
1. Reichert JM, Wenger JB. Development trends for new cancertherapeutics and vaccines. Drug Discov Today 2008;13:30–7.2. DiMasi JA, Grabowski HG. Economics of new oncology drug
development. J Clin Oncol 2007;25:209–16.3. Chau CH, Rixe O, McLeod H, Figg WD. Validation of analytic
methods for biomarkers used in drug development. Clin CancerRes 2008;14:5967–76.
4. Duffy MJ. Predictive markers in breast and other cancers: a review.Clin Chem 2005;51:494–503.
5. Duffy MJ, Crown J. A personalized approach to cancer treatment:how biomarkers can help. Clin Chem 2008;54:1770–9.
6. Gasparini G, Longo R, Torino F, Gattuso D, Morabito A, Toffoli G. Istailored therapy feasible in oncology? Crit Rev in Oncol Hematol2006;57:79–101.
7. Hayes DF. Prognostic and predictive factors revisited. Breast 2005;14:493–9.
8. U.S. Food and Drug Administration. Innovation or stagnation:challenge and opportunity on the critical path to new medicalproducts. March 2004 [cited April 5, 2010]. Available from:http://www.fda.gov/downloads/ScienceResearch/Special-Topics/CriticalPathInitiative/CriticalPathOpportunitiesReports/ucm113411.pdf.
9. Ludwig JA, Weinstein JN. Biomarkers in cancer staging, prognosisand treatment selection. Nat Rev Cancer 2005;5:845–56.
10. Moore HM, Compton CC, Lim MD, Vaught J, Christiansen KN,Alper J. 2009 Biospecimen research network symposium: advan-cing cancer research through biospecimen science. Cancer Res2009;69:6770–2.
11. National Cancer Institute. Office of Biorepositories and Bio-specimen Research. National Cancer Institute best practices forbiospecimen resources. June 2007 [cited March 26, 2010].Available from: http://biospecimens.cancer.gov/global/pdfs/NCI_Best_Practices_060507.pdf.
12. Caboux E, Plymoth A, Hainaut P, editors. Common minimumtechnical standards and protocols for biological resource centresdedicated to cancer research, IARC Working Group Report 2. Inter-national Agency for Research on Cancer; 2007 [cited March 26,2010], pp. 1–38. Available from: http://www.iarc.fr/en/publications/pdfs-online/wrk/wrk2/standardsBRC-1.pdf.
13. Organisation for Economic Co-Operation and Development. OECDbest practices guidelines for biological resource centres. Paris:OECD Publishing; 2007 [cited March 26, 2010]. Available from:http://www.oecd.org/dataoecd/7/13/38777417.pdf.
14. Pitt KE, Campbell LD, Skubitz APN, Somiari SB, Sexton KC,Pugh RS, editors. International Society for Biological and En-vironmental Repositories. 2008 Best practices for repositories:collection, storage, retrieval and distribution of biological mate-rials for research. Cell Preservation Technology 2008;6:3–58.
15. National Cancer Institute, Office of Biorepositories and Biospeci-men Research. Summary: National Cancer Institute BiospecimenBest Practices Forum; November 5, 2007 [cited February 25,2010]; Boston, MA. Available from: http://biospecimens.cancer.gov/practices/forum/boston2007/pdf/FINAL_11-05-07_NCI_BPs_Forum_Boston_Summary_Rev1-24-08_Ed.pdf.
16. Bossuyt PM, Reitsma JB, Bruns DE, et al. Towards complete andaccurate reporting of studies of diagnostic accuracy: the STARDinitiative. Standards for reporting of diagnostic accuracy. Clin Chem2003;49:1–6.
17. Haga SB, Beskow LM. Ethical, legal, and social implications ofbiobanks for genetics research. Adv Genet 2008;60:505–44.
18. Report of the Public Responsibility in Medicine and Research(PRIM&R) Human Tissue/Specimen Banking Working Group. March2007 [cited February 25, 2010]. Available from: http://www.primr.org/uploadedFiles/PRIMR_Site_Home/Public_Policy/Recently_Files_Comments/Tissue%20Banking%20White%20Paper%203-7-07%20final%20combined.pdf.
19. Irwin DA, Klenow PJ. Sematech: purpose and performance. ProcNatl Acad Sci U S A 1996;93:12739–42.
20. U.S. Food and Drug Administration. Drug-diagnostic codevel-opment concept paper—draft. April 2005 [cited April 5, 2010].Available from: http://www.fda.gov/downloads/Drugs/ScienceRe-search/ResearchAreas/Pharmacogenetics/UCM116689.pdf.
21. U.S. Food and Drug Administration. Table of valid genomic biomar-kers in the context of approved drug labels [updated March 152010; accessed April 5, 2010]. Available from: http://www.fda.gov/Drugs/ScienceResearch/ResearchAreas/Pharmacogenetics/ucm083378.htm.
22. Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence
Clin Cancer Res; 16(13) July 1, 2010 3317
h. 10, 2020. © 2010 American Association for Cancer

Khleif et al.
3318
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880
of tamoxifen-treated, node-negative breast cancer. N Engl J Med2004;351:2817–26.
23. Paik S, Shak S, Tang G, et al. Gene expression and benefit ofchemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol 2006;24:3726–34.
24. van de Vijver MJ, He YD, van't Veer LJ, et al. A gene-expressionsignature as a predictor of survival in breast cancer. N Engl J Med2002;347:1999–2009.
25. Buyse M, Loi S, van't Veer L, et al. Validation and clinical utility of a70-gene prognostic signature for women with node-negative breastcancer. J Natl Cancer Inst 2006;98:1183–92.
26. Simon R, Paik S, Hayes D. Use of archived specimens in evaluationof prognostic and predictive biomarkers. J Natl Cancer Inst 2009;101:1446–52.
27. Simon R. The use of genomics in clinical trial design. Clin Cancer Res2008;14:5984–93.
28. Mandrekar SJ, Sargent DJ. Clinical trial designs for predictivebiomarker validation: theoretical considerations and practicalchallenges. J Clin Oncol 2009;27:4027–34.
29. Taube SE, Clark GM, Dancey JE, McShane LM, Sigman CC,Gutman SI. A perspective on challenges and issues in biomarkerdevelopment and drug and biomarker codevelopment. J NatlCancer Inst 2009;101:1453–63.
30. U.S. Food and Drug Administration, Center for Devices andRadiological Health and Center for Biologics Evaluation andResearch. Draft guidance for industry, clinical laboratories, andFDA staff: in vitro diagnostic multivariate index assays. July 26,
Clin Cancer Res; 16(13) July 1, 2010
Researcon July clincancerres.aacrjournals.org Downloaded from
2007 [cited April 5, 2010]. Available from: http://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/ucm071455.pdf.
31. U.S. Department of Health and Human Services, Report of theSecretary's Advisory Committee on Genetics, Health, and Society.U.S. system of oversight of genetic testing: a response to the chargeof the Secretary of Health and Human Services. April 2008 [citedApril 5, 2010]. Available from: http://oba.od.nih.gov/oba/SACGHS/reports/SACGHS_oversight_report.pdf.
32. Genentech, Inc. Citizen petition: regulation of in vitro diagnostictests. Submitted December 5, 2008 [cited March 26, 2010]. Availablefrom: http://www.regulations.gov/search/Regs/contentStreamer?objectId=09000064807d4a7e&disposition=attachment&contentType=pdf.
33. Institute of Medicine of the National AcademiesCommittee on HealthResearch and the Privacy of Health Information. Beyond the HIPAAprivacy rule: enhancing privacy, improving health through research.Washington, DC: National Academies Press; 2009.
34. Biomarkers Definitions Working Group. Biomarkers and surrogateend points: preferred definitions and conceptual framework. ClinPharmacol Ther 2001;69:89–95.
35. U.S. Food andDrugAdministration,Center forDrug Evaluation andRe-search, Center for Biologics Evaluation and Research, and Center forDevices and Radiological Health. Guidance for industry: pharmacoge-nomic data submissions. March 2005 [citedMarch 26, 2010]. Availablefrom: http://www.fda.gov/downloads/RegulatoryInformation/Guidances/ucm126957.pdf.
Clinical Cancer Research
h. 10, 2020. © 2010 American Association for Cancer

2010;16:3299-3318. Published OnlineFirst May 25, 2010.Clin Cancer Res Samir N. Khleif, James H. Doroshow and William N. Hait DevelopmentReport: Advancing the Use of Biomarkers in Cancer Drug AACR-FDA-NCI Cancer Biomarkers Collaborative Consensus
Updated version
10.1158/1078-0432.CCR-10-0880doi:
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/16/13/3299.full#ref-list-1
This article cites 21 articles, 10 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/16/13/3299.full#related-urls
This article has been cited by 15 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/16/13/3299To request permission to re-use all or part of this article, use this link
Research. on July 10, 2020. © 2010 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 25, 2010; DOI: 10.1158/1078-0432.CCR-10-0880


















