Clinical Pearls Painful Tongue Swelling
4
918 CLINICAL PEARLS Ho, Bush • PAINFUL TONGUE SWELLING CLINICAL PRACTICE Clinical Pearls: Painful Tongue Swelling JAI HO, MD, SEAN P. BUSH, MD Figures 1 and 2. The patient’s tongue on physical ex- amination. Chief Complaint. Painful, swollen tongue. History of Present Illness. A 27-year-old man presents with a four-day history of progressive left- sided tongue swelling and pain. He additionally has difficulty handling oral secretions, and odyno- phagia. He denies trauma, fevers, chills, sore throat, dysphagia, or vomiting. He denies prior oral infections or recent illnesses. Past medical his- tory is unremarkable. He has no pror surgeries or medical conditions. He is not currently taking medications and has no known allergies. Social history is significant for social alcohol use and smoking. He denies intra- venous drug abuse. No HIV risk factors are iden- tified. Physical Examination. The patient positions himself in a tripod position while wiping off saliva that drools continuously from his mouth. He ap- pears awake and alert but is fatigued and dehy- drated. His voice is muffled and he appears to have difficulty breathing. Vital signs show a blood pres- sure of 141/79 mm Hg, pulse rate of 82 beats/min, respiratory rate of 32 breaths/min, and tempera- ture of 99.17F (oral). Head and neck examination is significant for a fluctuant and exquisitely tender mass on the left side of the tongue (Figs. 1 and 2). The tongue is not erythematous and no external lesions are present. There is no tongue elevation or brawny edema of the submandibular region. Dentition is poor but no dental infections are evi- dent. The oropharynx is otherwise clear with nor- mal-appearing tonsils. Cervical lymph nodes are From the Department of Emergency Medicine, Loma Linda University Medical Center, Loma Linda, CA (JH, SPB). Section editor: Lawrence B. Stack, MD, Vanderbilt University Medical Center, Nashville, TN. Photographic critique: Michael A. Morris, University of Arkan- sas for Medical Sciences, Little Rock, AR. Received November 4, 1999; revision received March 2, 2000; accepted March 4, 2000. Address for correspondence and reprints: Sean Bush, MD, De- partment of Emergency Medicine, Loma Linda University Medical Center, Room A108, 11234 Anderson Street, Loma Linda, CA 92354. Fax: 909-558-0121; e-mail: famensean@aol. com mildly enlarged and tender. The neck is supple and the remaining physical exam is unremarkable. Laboratory. The white blood cell count is 14,000/mL. No differential is obtained. The remain- der of the complete blood cell count is normal. The serum potassium is 2.9 mmol/L. The remainder of the basic metabolic panel is normal. Radiologic and additional tests are performed. (The diagnosis, clinical course, discussion, and clinical pearls appear on page 941.)
Transcript of Clinical Pearls Painful Tongue Swelling

918 CLINICAL PEARLS Ho, Bush • PAINFUL TONGUE SWELLING
CLINICAL PRACTICE
Clinical Pearls: Painful Tongue Swelling
JAI HO, MD, SEAN P. BUSH, MD
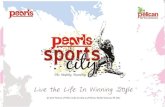
Figures 1 and 2. The patient’s tongue on physical ex-amination.
Chief Complaint. Painful, swollen tongue.
History of Present Illness. A 27-year-old manpresents with a four-day history of progressive left-sided tongue swelling and pain. He additionallyhas difficulty handling oral secretions, and odyno-phagia. He denies trauma, fevers, chills, sorethroat, dysphagia, or vomiting. He denies priororal infections or recent illnesses. Past medical his-tory is unremarkable. He has no pror surgeries ormedical conditions.
He is not currently taking medications and hasno known allergies. Social history is significant forsocial alcohol use and smoking. He denies intra-venous drug abuse. No HIV risk factors are iden-tified.
Physical Examination. The patient positionshimself in a tripod position while wiping off salivathat drools continuously from his mouth. He ap-pears awake and alert but is fatigued and dehy-drated. His voice is muffled and he appears to havedifficulty breathing. Vital signs show a blood pres-sure of 141/79 mm Hg, pulse rate of 82 beats/min,respiratory rate of 32 breaths/min, and tempera-ture of 99.17F (oral). Head and neck examinationis significant for a fluctuant and exquisitely tendermass on the left side of the tongue (Figs. 1 and 2).The tongue is not erythematous and no externallesions are present. There is no tongue elevationor brawny edema of the submandibular region.Dentition is poor but no dental infections are evi-dent. The oropharynx is otherwise clear with nor-mal-appearing tonsils. Cervical lymph nodes are
From the Department of Emergency Medicine, Loma LindaUniversity Medical Center, Loma Linda, CA (JH, SPB).Section editor: Lawrence B. Stack, MD, Vanderbilt UniversityMedical Center, Nashville, TN.Photographic critique: Michael A. Morris, University of Arkan-sas for Medical Sciences, Little Rock, AR.Received November 4, 1999; revision received March 2, 2000;accepted March 4, 2000.Address for correspondence and reprints: Sean Bush, MD, De-partment of Emergency Medicine, Loma Linda UniversityMedical Center, Room A108, 11234 Anderson Street, LomaLinda, CA 92354. Fax: 909-558-0121; e-mail: [email protected]
mildly enlarged and tender. The neck is supple andthe remaining physical exam is unremarkable.
Laboratory. The white blood cell count is14,000/mL. No differential is obtained. The remain-der of the complete blood cell count is normal. Theserum potassium is 2.9 mmol/L. The remainder ofthe basic metabolic panel is normal.
Radiologic and additional tests are performed.
(The diagnosis, clinical course, discussion, and clinical pearlsappear on page 941.)

ACADEMIC EMERGENCY MEDICINE • August 2000, Volume 7, Number 8 941
ing pathways: recent advances and implications for cardiovas-cular disease. Trends Cardiovasc Med. 1996; 6:109–15.118. Dinarello CA, Gelfand JA, Wolff SM. Anticytokine strat-egies in the treatment of the sytemic inflammatory responsesyndrome. JAMA. 1993; 269:1829–35.119. Fisher SCJ, Opal SM, Dhainaut JF, et al. Influence of ananti-tumor necrosis factor monoclonal antibody on cytokinelevels in patients with sepsis. Crit Care Med. 1993; 21:318–27.120. Beutler B, Milsark IW, Cerami AC. Passive immunizationagainst cachectin/tumor necrosis factor protects mice from le-thal effects of endotoxin. Science. 1985; 229:869–71.121. Chaudry IH, Ayala A, Ertel W, Stephan RN. Hemorrhageand resuscitation: immunological aspects. Am J Physiol. 1990;259 (Regul Integr Comp Physiol. 28):R663–R678.122. Fisher CJJ, Agosti JM, Opal SM, et al. Treatment of sep-tic shock with the tumor necrosis factor receptor: Fc fusionprotein. N Engl J Med. 1996; 334:1697–702.123. Steinshamn S, Bemelmans MH, vanTits LJ, Bergh K,Buurman WA, Waage A. TNF receptors in murine Candidaalbicans infection: evidence for an important role of TNF re-ceptor p55 in antifungal defense. J Immunol. 1996; 157:2155–9.124. Echtenacher B, Falk BW, Mannel DN, Krammer PH. Re-quirement of endogenous tumor necrosis factor/cachectin forrecovery from experimental peritonitis. J Immunol. 1990; 145:3762–6.125. Amiot F, Boussadia O, Cases S, et al. Mice heterozygousfor a deletion of the tumor necrosis factor-alpha and lympho-toxin-alpha genes: biological importance of a nonlinear re-sponse of tumor necrosis factor-alpha to gene dosage. Eur JImmunol. 1997; 27:1035–42.126. Reinhart K, Wiegand-Lohnert C, Grimminger F, et al. As-sessment of the safety and efficacy of the monoclonal anti-tu-mor necrosis factor antibody-fragment, MAK 195F, in patients
with sepsis and septic shock: a multicenter, randomized, pla-cebo-controlled, dose-ranging study. Crit Care Med. 1996; 24:733–42.127. Panacek EA, Marshall J, Barchuk W, Fischkoff S. Resultsof the MONARCS study of a murine monoclonal antibodyagainst TNF in patients with severe sepsis. Toronto, Canada:American Thoracic Society presentation, May 2000.128. Schwieterman WD. FDA perspective on anti-TNF treat-ments. Ann Rheum Dis. 1999; 58(suppl 1):I90–I91.129. Lovell DJ, Giannini EH, Reiff A, et al. Etanercept in chil-dren with polyarticular juvenile rheumatoid arthritis. Pediat-ric Rheumatology Collaborative Study Group. N Engl J Med.2000; 342:763–9.130. Mathias SD, Colwell HH, Miller DP, Moreland LW, BuattiM, Wanke L. Health-related quality of life and functionalstatus of patients with rheumatoid arthritis randomly assignedto receive etanercept or placebo. Clin Ther. 2000; 22:128–39.131. Khademi M, Wallstrom E, Andersson M, Piehl F, DiMarco R, Olsson T. Reduction of both pro- and anti-inflam-matory cytokines after 6 months of interferon beta-1a treat-ment of multiple sclerosis. J Neuroimmunol. 2000; 103:202–10.132. Liu J, Marino MW, Wong G, et al. TNF is a potent anti-inflammatory cytokine in autoimmune-mediated demyelina-tion. Nat Med. 1998; 4(1):78–83.133. Present DH. Review article: the efficacy of infliximab inCrohn’s disease—healing of fistulae. Aliment Pharmacol Ther.1999; 13(suppl 4):23–8.134. Present DH, Rutgeerts P, Targan S, et al. Infliximab forthe treatment of fistulas in patients with Crohn’s disease. NEngl J Med. 1999; 340:1398–405.135. Wordliczek J, Szczepanik AM, Banach M, et al. The effectof pentoxifiline on post-injury hyperalgesia in rats and post-operative pain in patients. Life Sci. 2000; 66:1155–64.
Clinical Pearls (cont. from p. 918)
Diagnosis. Tongue abscess.
Clinical Course. Computed tomography (CT)scan revealed the presence of a tongue abscess.Treatment consisted of nasotracheal intubationand hydration followed by surgical incision anddrainage in the operating room under general an-esthesia. Clindamycin was administered empiri-cally. The patient remained intubated for 24 hoursafter presentation. Tongue edema resolved rapidlyfollowing incision and drainage. The patient wasdischarged within two days of admission. Bloodcultures were subsequently negative. Pasteurellamultocida grew from abscess cultures. On follow-up, the patient denied having a cat or any regularexposure to cats. He resided with his mother anda family dog in a rural section of California. Hehad worked odd jobs, including some farm work,and was last seen in northern California living ina homemade shack working on a farm. Unfortu-nately, we were unable to determine his level ofexposure to his family dog or possibly to any straycats.
Discussion. We believe this to be the first re-ported case of tongue abscess due to P. multocida.We found no other reports when using a MED-LINE search.
A total of 207 tongue abscesses were reportedfrom 1861 to 1991,1 with most occurring before1910. Only 36 cases have been reported in the last33 years. With the advent of antibiotics, improveddental hygiene, and modern surgical techniques,tongue abscesses have become extremely rare.2
Oral infections are frequently encountered, butthe tongue appears resistant to infectious pro-cesses. Although the tongue faces an environmentladen with bacteria and endures occasional traumafrom unintentional biting or laceration, it resistsinfection secondary to its thick protective epithe-lium, continuous salivary flow, and excellent vas-cular and lymphatic supply.1,3,4 The cause of mosttongue abscesses are largely unknown.1 When acause of tongue abscess is discovered, the mostcommonly reported etiology is trauma. Examplesinclude penetration and/or retention of foreignbodies (such as retained sutures), unintentionalbiting, or as a complication of oral surgery.1–6 Lo-calized infections such as stomatitis, glossitis, ortonsillitis can spread to tongue abscess forma-tion.3,4 Almost exclusively, all infections are the re-sult of Staphylococcus, Streptococcus, and anaero-bic oral flora organisms, with the exception of onedocumented Hemophilus parainfluenzae4 tongueabscess.2,3,7–9 Several citations report negative cul-tures.1,5,10

942 CLINICAL PEARLS Ho, Bush • PAINFUL TONGUE SWELLING
Pasteurella multocida is commonly isolatedfrom infected cat bites, as well as some dog bites.Infection by P. multocida usually develops within24 hours after a cat bite, although the presentationin our patient was more indolent. As in this case,clindamycin is often used to empirically treat oralinfections. However, clindamycin does not cover P.multocida or some of the organisms in human oralflora (such as Eikenella corrodens). Penicillin G orampicillin is recommended for these organisms. Asalternatives, amoxicillin clavulanate, trimetho-prim-sulfamethoxazole, or fluoroquinolones mayprovide coverage. Cephalexin, penicillinase-resis-tant synthetic penicillins, and erythromycin aregenerally not effective against P. multocida or E.corrodens.11
Earlier reports suggest that more cases occuramong males and residents in rural areas, such asfarm workers.1–3 Tongue abscesses have been doc-umented as early as infancy7 and up to 70 years ofage, with most reported in the 30–50-year agerange.2,3,12 Typical symptoms include severe pain,unilateral tongue enlargement, dysphagia, anddrooling.3,5,9,13 Fever is usually absent on presen-tation, and the leukocyte count is variable.13 Pain-less presentations and chronic cases lasting up tosix months have been described.2,10 Most patientsseek medical attention within ten days of symptomonset.3
The differential diagnosis of tongue swelling in-cludes anaphylaxis, which is readily differentiatedfrom an abscess by the lack of pain and tenderness.Other diagnoses include Ludwig’s angina, lingualartery aneurysm, thyroglossal duct cyst, lingualthyroid goiters, tumor, lingual tonsillitis, syphiliticgumma, and actinomycosis. Fluctuance may helpdistinguish tongue abscess from other causes oftongue swelling.
Attention to airway is critical, and admission toan intensive care unit for close observation may benecessary. Airway obstruction within hours hasbeen reported.7,14 Incision and drainage success-fully treates most tongue abscesses, but dependingon the clinical situation, some tonuge abscesseshave been successfully treated with needle aspi-ration with adjunctive antibiotic therapy on anoutpatient basis.4,8,15 Antibiotic selection shouldcover oral flora, Staphylococcus, and Streptococ-cus. Amoxicillin clavulanate would cover P. mul-tocida as well as Staphylococcus amd Streptococ-cus more commonly encountered and wouldprobably be the best empiric choice for suspectedtongue abscess. Needle aspiration of pus confirmspresence of an abscess, but if the exam is equivo-cal, CT scan is an excellent diagnostic study.5 Al-ternatively, successful use of ultrasound examina-tion11,16 and magnetic resonance imaging (MRI)17
has been reported.
Clinical Pearls.
1. Tongue abscess is a rare condition predomi-nantly caused by Staphylococcus sp., Streptococcussp., and anaerobic organisms.2. Early airway management is important becausetongue abscesses can lead to rapid airway obstruc-tion. Airway obstruction and aspiration from ab-scess rupture are potential complications.3. Needle aspiration of purulent material confirmsthe diagnosis of tongue abscess; however, if indoubt, CT scan, ultrasound examination, or MRIaids in the diagnosis.4. Incision and drainage is usually required fortongue abscesses, although selected cases can betreated with needle aspiration and antibiotics. An-tibiotics, hydration, and airway managementshould be initiated in the emergency department.
Photographic Critique (by Michael A. Morris).
Intraoral photography is challenging. Teeth, lips,and mustaches make shooting images inside themouth difficult; even a healthy tongue can lookgrotesque on film. Oral retractors are frequentlyrequired to allow the camera an unobstructed viewof the mouth.
Good lighting technique and an extended depthof field are required to visualize the tongue ade-quately. Figures 1 and 2 illustrate both of theseconcepts well. The lighting in both illustrations isvirtually ‘‘shadowless.’’ There are no harsh shad-ows on the surface of the tongue that could hidedetail. The lighting technique used shows good tex-ture on the surface of the tongue and intense col-oration. The depth field (determined by the f/stopused when the image was made) is sufficient tokeep the entire tongue in acceptable focus. Figures1 and 2 are good clinical illustrations of the phys-ical findings.
Key words. tongue; Pasteurella multocida; abscess; airway;lingual.
References
1. Knight LC. Lingual abscess: a rarity. Br J Clin Pract. 1991;45:294–5.2. Tarachandra RD, Srivastava KN. Chronic lingual abscess.J Indian Med Assoc. 1973; 61:349–50.3. Pal J, Prakash J. Lingual abscess. J Indian Med Assoc.1976; 66:57–60.4. Roberge RJ, Fowler RM, Mayer NM. Glossal abscess. Am JEmerg Med. 1989; 7:406–8.5. Redleaf MI. Lingual abscess. Ann Otol Rhinol Laryngol.1994; 103:986–7.6. Jain HK, Bhatia PL. Lingual abscess. J Laryngol Otol.1970; 84:637–41.7. Sanders AD, Yeh S, Paige ML, et al. Lingual abscess pre-senting as airway obstruction in the infant. Otolaryngol HeadNeck Surg. 1988; 99:344–5.8. Jungell P, Asikainen S, Kuikka A, et al. Acute tongue ab-scess: report of two cases. Int J Oral Maxillofac Surg. 1996; 25:308–10.

ACADEMIC EMERGENCY MEDICINE • August 2000, Volume 7, Number 8 943
9. Sands M, Pepe J, Brown RB. Tongue abscess: case reportand review. Clin Infect Dis. 1993; 16:133–5.10. Luker J. A case of lingual abscess. Br Dent J. 1985; 159:300.11. Gilbert DN, Moellering RC Jr, Sande MA. The SanfordGuide to Antimicrobial Therapy, 29th edition, Hyde Park, VT:Antimicrobial Therapy, 1999.12. Hehar SS, Johnson IM, Jones NS. Glossal abscess pre-senting as unilateral tongue swelling. J Laryngol Otol. 1996;110:389–90.13. Kolb JC, Sanders DY. Lingual abscess mimicking epiglot-titis. Am J Emerg Med. 1998; 16:414–6.
14. Renehan A, Morton M. Acute enlargement of the tongue.Br J Oral Maxillofac Surg. 1993; 31:321–4.15. Agarwal KK, Changani DL, Bhattarcharya S. Lingualabscess—aetiopathogenesis. J Laryngol Otol. 1966; 80:1038–40.16. Osammor JY, Cherry JR, Daziel M. Lingual abscess: thevalue of ultrasound diagnosis. J Laryngol Otol. 1989; 103:950–1.17. A, Ballesteros AI, Bradariz Castelo JA. Primary˜Munozlingual abscess presenting as acute swelling of the tongue ob-structing the upper airway: diagnosis with MR. Am J Neuro-radiol. 1998; 19:496–8.
v
REFLECTIONS
Accepting Recommendation over Science
Those who retrieve data, analyze and offer reviewsSuggest intuition is increasingly difficult to defend.We’re exorted by these evidence canons to eschewDecision based on experience or what ‘‘experts’’contend.I’ve learned the credible skill to refute or support;I’m able to integrate several targeted annotationsInto my spectrum of practice and guidance of consorts.But beware, well-searched strategies have their limitations!
When advised by my spouse to start the vacuum machineIn the far corner of the bedroom, not the nearI asked, ‘‘How would my method fail to clean?’’‘‘Common sense, practiced routine suggests you’re a mutineer.’’To which I replied, ‘‘Hippocrates inferred that ScienceWas father of knowledge and Opinion bred no high tide.’’
Bringing the ‘‘office art’’ home can lead to abstinence.Evidenced-based issues may be hazardous at some bedsides.
JONATHAN SINGER, MDDepartment of Emergency MedicineWright State UniversityDayton, Ohio