CLINICAL ORTHOPAEDICS AND RELATED RESEARCH · CLINICAL ORTHOPAEDICS AND RELATED RESEARCH Number...
10
..~ "'"'I'! ", t I CLINICAL ORTHOPAEDICS AND RELATEDRESEARCH Number 396, pp. 142-151 @ 2002 Lippincott Williams & Wilkins, Inc. Intraoperative Monitoring for Safety of Bilateral Total Knee Replacement ; , Lawrence D. Dorr, MD*; Pacharapol Udomkiat, MD*,' Janos Szenohradszky, MD, PhD**,' Robin Chorn, BSc, MBChB*; and '~liQRayq, MD* Cardiopulmonary hemod~!~cs utive patients who had o~e:~~a~e para~eters of embolismbe done. knee replacements were moriitof~dprQsp~C;;C C ~:~=u:el:~ lar resistancewere measuredBefore sKlnclncl-; c' ,i ,i .. . 5 10 . f .i, ITiji :',c h fi st iuill!~mbolIslJl' f; ".d ,cardIopulmonary complIca- Slon, to minutes a ter Imp antmgct e r. ,ij".U'iijjiiU t" - I '. O C I "it ./ rt l ° ty 0 t1 t2 5 to " C'ii ccc IOQSf~"i' ;,;!" "s mo a 1 IS a eas 0 lffies :~ ~:;~a;:~::~m;:~ t~!i'b~lti(eral or bilateral two-stage total ment was cancelled in five patients be~ausectllb;,!i"i;~,f::f;,;feplacements.IO,I~ Ritter et alI6 reviewed pulmonary vascular resistance after the firstC~-"Healthcare Finance Administration reports of knee replacement was more than double the total knee replacements done between 1985 baseline, or above 200 dyne/second/cms. No and 19900 There were 62,730 bilateral total patient had clinical symptoms of fat embolism knee replacements and 12,922 were simulta- during the postoperative course.Patientpredic- neous,The 30-day mortality rate with simul- !ive f~ctors, or the u~,~ ~f pulse oxime~; read- ""taneous bi!atet:fil,total knee replacements was of pulmonary vascular resistanc~~::~f>r thIS~~a- :: ::...: d r1JiJ 1. .h 0 1 b"1 son the safety of this operation Itlitl~:f~t.el)t I!if~ari;j:;~i:r Ity rate WIt SI~U taneous 1 at- , ,:::' c,: "c:::c" ':, '~raltotatknee replacements ISmostly because F * Th Arthri . Ins . C . I H . taI M d of emboli of fat, blood, or bothoS,IO An in- rom e lIs I1tute at entme a OSP! e -.0' . ical Center, Inglewood, CA, and the**USC University creased fisk of fat embolIc complIcations was Hospital, Los Angeles, CA. reported by Jankiewicz et al,9Lane et aI,IO and This research was supported by funds from the Orthope- Dorr et aI,5 Jankiewicz et al9 reported no pa- dic Research Institute at Good Samaritan Hospital, Los tient deaths,but 8% of patients had mental sta- Angeles, CAo h ob ed f b 10 L . La DD MD Th Arthri tus c anges attri ut to at em 0 1. ane et Repnnt requests to wrence .OTT, ,e -10 h '" ai , d 29'" f th 0 tis Institute atCentine1a Hospital Medical Center, 501 E. al ad 1-/0 mort Ity an -/0 0 e patients Hardy Street, 3rd Floor, Inglewood, CA 903010 had mental status changes with simultaneous Received: November 3,2000. bilateral total knee replacements compared Revised: June 1, 2001; July 30, 2001. with no deaths and 7% of patients with mental Accepted: August 30, 2001. status changes with unilateral total knee re- 142 , """,,;
-
Upload
duongthien -
Category
Documents
-
view
217 -
download
0
Transcript of CLINICAL ORTHOPAEDICS AND RELATED RESEARCH · CLINICAL ORTHOPAEDICS AND RELATED RESEARCH Number...
..~ "'"'I'! ",
t I
CLINICAL ORTHOPAEDICS AND RELATED RESEARCHNumber 396, pp. 142-151@ 2002 Lippincott Williams & Wilkins, Inc.
Intraoperative Monitoring for Safety ofBilateral Total Knee Replacement
;,
Lawrence D. Dorr, MD*; Pacharapol Udomkiat, MD*,'Janos Szenohradszky, MD, PhD**,' Robin Chorn, BSc, MBChB*;
and '~liQRayq, MD*
Cardiopulmonary hemod~!~csutive patients who had o~e:~~a~e para~eters of embolism be done.knee replacements were moriitof~dprQsp~C;;C C
~:~=u:el:~lar resistance were measured Before sKlnclncl-; c' ,i ,i ... 5 10 . f .i, ITiji :',c h fi stiuill!~mbolIslJl'f;".d ,cardIopulmonary complIca- Slon, to minutes a ter Imp antmgct e r. ,ij".U'iijjiiUt" - I'.OC I"it ./ rt l °ty 0 t 1 t 2 5 to" C'ii ccc IOQSf~"i' ;,;!" "s mo a 1 IS a eas 0 lffies
:~ ~:;~a;:~::~m;:~ t~!i'b~lti(eral or bilateral two-stage totalment was cancelled in five patients be~ausectllb;,!i"i;~,f::f;,;feplacements.IO,I~ Ritter et alI6 reviewedpulmonary vascular resistance after the firstC~-"Healthcare Finance Administration reports ofknee replacement was more than double the total knee replacements done between 1985baseline, or above 200 dyne/second/cms. No and 19900 There were 62,730 bilateral totalpatient had clinical symptoms of fat embolism knee replacements and 12,922 were simulta-during the postoperative course. Patient predic- neous, The 30-day mortality rate with simul-!ive f~ctors, or the u~,~ ~f pulse oxime~; read- ""taneous bi!atet:fil,total knee replacements was
of pulmonary vascular resistanc~~::~f>r thIS ~~a- :: ::...: d r1JiJ 1. .h 0 1 b"1son the safety of this operation Itlitl~:f~t.el)t I!if~ari;j:;~i:r Ity rate WIt SI~U taneous 1 at-
, ,:::' c,: "c:::c" ':, '~raltotatknee replacements IS mostly because
F *Th Arthri . Ins . C . I H . taI M d of emboli of fat, blood, or bothoS,IO An in-rom e lIs I1tute at entme a OSP! e -.0' .
ical Center, Inglewood, CA, and the **USC University creased fisk of fat embolIc complIcations wasHospital, Los Angeles, CA. reported by Jankiewicz et al,9 Lane et aI,IO andThis research was supported by funds from the Orthope- Dorr et aI,5 Jankiewicz et al9 reported no pa-dic Research Institute at Good Samaritan Hospital, Los tient deaths, but 8% of patients had mental sta-Angeles, CAo h ob ed f b 10 L. La D D MD Th Arthri tus c anges attri ut to at em 0 1. ane etRepnnt requests to wrence .OTT, ,e -10 h '" ai, d 29'" f th 0tis Institute at Centine1a Hospital Medical Center, 501 E. al ad 1-/0 mort Ity an -/0 0 e patientsHardy Street, 3rd Floor, Inglewood, CA 903010 had mental status changes with simultaneousReceived: November 3, 2000. bilateral total knee replacements comparedRevised: June 1, 2001; July 30, 2001. with no deaths and 7% of patients with mentalAccepted: August 30, 2001. status changes with unilateral total knee re-
142
, """,,;

, ,
Number 396March,2002 Intraoperative Monitoring for Knee Replacement 143
-.
placements, Dorr et al5 reported one death in components at one time in all knees,3 Sixty-two64 patients with bilateral total knee replace- knees had the cruciate-retaining design and 91 kneesments and 12% with mental status changes had the posterior-stabilized design. Seventy-six pa-caused by fat emboli, Fahmy et aI7 observed tie~t.s had osteo~tis and ~?ad rheumatoid~-bone marrow contents and fat retrieval sam- thntis, PreoperatIve comorblditIes are shown mpies of blood in the right atrium during total T~ble 1; ~e comorbi~ities mos~y ar: assoc~atedkn I t d 'th " al ' WIth cardiovascular disease. Thirty-nme patIents
ee rep acemen one WI a lemor lD- .2 were men and 40 were women WIth a mean age oftramedullary rod. Berman et al measured 69.4 :t 6.9 years (range 50-82 years). The meanechogenic material in the right ,:entricle im- height was 168.7 :t 11.3'cm (range, 142-196 cm),aged by transesophageal echocardiogram. They and the mean weight was 83.7 :t 16.9 kg (range,sampled blood from one pulmonary arte~x",,""1~132 kg). This study was approved by the fustitu-catheter and 10 femoral vein catheters'and'.."G:uona:IReyiew Board at the authors' institution.
and mortalIty nsk of this Opt;i~tl~n coUld'belm-' ,,;.'~ " 'i'" ,,;'1, ',~I ..' Y .ry p.
Previous studies have focuS~'(jD th,e ben~Pts1j'(j~[;. I gt9YP a"d lli eYa~!~ti9h of patients who had the sec-
of epiduralpital stay,4.15 The scientific justifiCatio~l,uS'i',,'..'~g;..g'ml~pl ,~pesthesla Wl~ the epld~al catheterof this operation has been studied by"cOIl),i~~ 'j[i' jj{f}~ I~",£l~ce:" for postoperatIve analgesia. A Swan-
.th th . 1 t al kn I t ?'the """"""'"~"C,Ganz:pulmonary artery catheter (Baxter Healthcareson WI e urn a er ee rep acemen WI.. ...
I. .CorporatIon, Irvme, CA) was mserted via the fightcomp Icatlon rates, blood loss, deep venous internal jugular vein in every patient. Throughoutthrombosis, and pulmonary embolism.9,10.17 surgery, each patient's temperature was measuredThe current study showed that one-stage bilat -with an esophageal temperature probe. Patients'era! total knee replacements could be done temperatures were between 360 and 36.80 for the
~ay~~ inp=:~:~Vl ':b~~:~~ f' ~:~;:"
gg~:e~~~stored. Second, Medical, fuc~
~=~total knee replacements was justified. TABLE 1. Preoperative Medical
Conditions in the Current Study Group
MATERIALS AND METHODS Comorbidities Number of Cases
Seventy-nine consecutive patients were scheduled Smoking 20for one-stage bilateral primary total knee replace- Hypertension 17ments by one surgeon between September 1997 and Cardiopulmonary disease 13May 1999. Five patients had surgery for the second Diabetes mellitus. 9knee cancelled so that 153 knees were treated surgi- HYl:>ercholesteroleml~ 6
II Th A II Kn S te (S lz Orth edi Peripheral vascular disease 4ca y. e po 0 ee ys m u er op cs, C 3Austin, TX) was implanted by cementing all three ancer

1 ,
Clinical Orthopaedics144 Dorr et al and Related Research
The baseline hemodynamic parameters were guides were used. A tourniquet was used in all butmonitored before surgical incision and repeat mea- 13 patients who had a history of peripheral vascularsurements were done 5 to 10 minutes after comple- disease or diabetes mellitus, or both, or who had ra-tion of implantation of the first knee replacements, diographic evidence of atherosclerotic femoral orand 5 to 10 minutes after implantation of the second popliteal artery calcification, or both. The tourniquetknee replacement. These hemodynamic measure- was deflated before closure in all knees in which thements included systolic and diastolic blood pressure, tourniquet was inflated. If the pulmonary vascularmean pulmonary artery pressure, pulmonary artery resistance measurement indicated that the secondocclusion pressure, cardiac output, pulmonary vas- knee operation could be done safely, this was beguncular resistance, and systemic pulmonary vascular during the closure of the first knee.resistance. The oxygen saturation readings from the Patients were divided into three groups based onpulse oximeter also were recorded at the moment th~cccccc"fue length of intramedullary femoral alignment rodpulmonary vascular resistance was Group 1 was comprised of31 pa-
two patients were placed in t1ie~tt;!nsiv~::cai;~'ql1it:tt feJIilii-il1:rods, buttQt)t ~ tourniquet, were used. For
stabilized the cutting block instnib);en~uring"applp'r';"the pt;!~6.v~cular resistance changes if no rodcation of the cutting block to the and postoperative datalength rods, an external guide was"tls~~" ~hid;pC:!r ;!~Jte;d~~lJ1rlfnted for the anesthesia time, tourniquetpointed to two fingerbreadths medial to thea:nter~""C"C"t:tifne;"c6perative time, blood loss, fluid and bloodsuperior iliac spine of the pelvis. For tibial prepara- transfusion, intensive care unit and hospital stay time,tion, only the short 9-cm rod was used to stabilize the rehabilitation unit stay time, and complications.cutting jig in all 74 patients (143 knees) and an ex- At the most recent followup (average, 13.1 :t 5.9ternal rod was used to position the cutting block. For months) each patient completed a self-assessmenteach rod insertion, regardless of length, the insertion questionnaire (Orthographics, Salt Lake City, UT),drill hole was enlarged",to",!J:llow venting ~4,leduce c,which inclyde4" pwn and functional assessment,
:in five patients (10 knees) no rods Wl!!r"y~~dcforlfue ti:",,~e~;~ecl?,ati~!!rs satisfaction with having bilateralfemur or tibia. In these knees, onlyl,~*Trljn~,g.q~ 'Irrl:,~,plil~~~,rlP)cements at one operation.
TABLE 2. Six Specific Questions to Assess Patient's Satisfactionwith One-Stage Bilateral Total Knee Replacement
Specific Questions
1. Was having bilateral total knee replacements done at the same operation worth it?2. Would you have bilateral total knee replacements done at the same operation again?3. Would you rather do one knee at a time with two surgeries?4. Do both knees feel the same at this time?5. How long postoperatively before both knees felt the same?6. How long postoperatively before you felt completely recovered?
\ .
Number 396March,2002 Intraoperative Monitoring for Knee Replacement 145-
Statistical analysis was done using SPSS soft- Fluid loss during the series of total knee re-ware (S.tatistical Software In~, Chicago, IL). The placement surgeries using a tourniquet wascorrelation between cancellation of surgery of the limited to less than 250 mL of blood in allsecond knee replaceme~t to the length of fe~oral cases. The patients routinely received onlyrod and the use of tournIquet was analyzed usmg aLo .
t 1 1. al . A 1 . t ..crystalloId therapy durIng surgery, lImIted togl og mear an YSIS. OglS IC regressIon "
analysis was used to correlate preoperative medical 1200 ~ to ,1800 ~ m normal salIne or lac-comorbidities with surgery cancellation. Continu- tated Ringer s solut10n.ous variables including tourniquet and anesthesia Phenylephrine also was used routinely totime, amount of blood loss and transfusion, and ra- manage the acute changes of tourniquet re-diographic component position were compared us- lease. If a patient's heart rate was below 50ing an independent Student's t test. ",beats per minute after tourniquet release, 5 mg
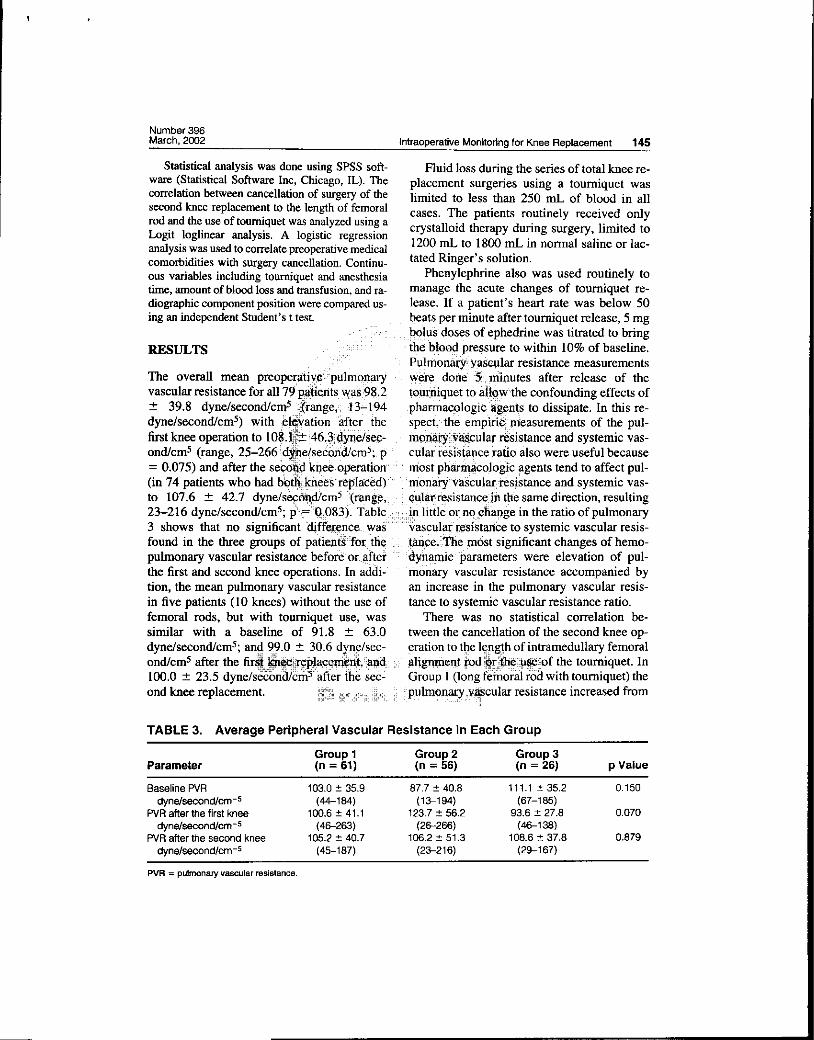
::t 39.8 dyne/second/cll}5;%!~t~geii!J: ~3r~9~::' :J:?l1a~~qg~oglc:~g~n~s to dissIpate. In thiS re-
dyne/second/cm5) with ;~.1.i¥aiion :'~fterJtlie::i!J spect~'tl1e: emp~ii!:~asurements of the pul-
first knee operation to and systemic vas-ond/cm5 (range, 25-266i!d~e(sec~r~cN5:. Pi!i!i!i!i!i! ql~ tfj~~&~~pce:r~!~~ ~lso were useful because
:~ds~s~:~ ~:~~to 107.6 ::t 42.7 dyne/sefOliI9l1:;ll}5 ':I~"gt;,;; fJ;:,q4)N~lJistal}cvi!i!jiJ1 tJ;l'e same direction, resulting
"';;" """""""""'."" "",," ""iF,,;. .23-216 dyne/second/cm5; p"\~':t08~). Table,:;l;;;ijl} lIttle o~;nq::lfia!j)ge m the ratIo of pulmonary3 shows that no significant to systemic vascular resis-found in the three groups of pati~rs';fOt, th~"i!i!,;i!:'i!~fewi!jfhe p16st significant changes of hemo-
.',," ",!";4\;""'4 .,,~iF .puhnonary vascular resistance before'oL,,~fte1i ;;: ;iy;nall}1c" parameters were elevatIon of pul-
~"""" ,-p"the first and second knee operations. In addi::P""monary vascular resistance accompanied bytion, the mean pulmonary vascular resistance an increase in the pulmonary vascular resis-in five patients (10 knees) without the use of tance to systemic vascular resistance ratio.femoral rods, but with tourniquet use, was There was no statistical correlation be-similar with a baseline of 91.8 ::t 63.0 tween the cancellation of the second knee op-dyne/second/cm5; an!g ~9.0 ::t 30.6 dXl}y/sec- ,fjration to t~e 17,P&,th of intramedullary femoralond/cm5 after the the tourniquet. In100.0 ::t 23.5 dyne/secona/cm5Pafter the sec:: P' 'GroupPl (long femorill rod with tourniquet) the
ond knee replacement. JP,V~~f!R;:¥!tcular resistance increased from" ;";';; Pp' ':;;;""PPP;
TABLE 3. Average Peripheral Vascular Resistance in Each Group
Group 1 Group 2 Group 3Parameter (n = 61) (n = 56) (n = 26) P Value
BaselinePVR 103.0:!:35.9 87.7:!:40.8 111.1:!:35.2 0.150dyne/second/cm-5 (44-184) (13-194) (67-185)
PVR afler the first knee 100.6:!:41.1 123.7:!:56.2 93.6:!:27.8 0.070dyne/second/cm-5 (46-263) (26-266) (46-138)
PVR aflerthe second knee 105.2:!:40.7 106.2:!:51.3 108.6:!:37.8 0.879dyne/second/cm-5 (45-187) (23-216) (29-167)
PVA = pulmonary vascular resistance.

I
Clinical Orthopaedics146 Dorr et al and Related Research
the baseline after the first knee surgery in 13 of as administered routinely for total joint surgery,31 patients (42%). In one patient, the surgery a high degree of sympathetic block is achieved.for the second knee was cancelled because the As a result, frequent reductions in the normalpulmonary vascular resistance increased to 263 systemic vascular resistance from approximatelydyne/second/cm5.1n the remaining 30 patients 1200 dyne/second/cm5 to approximately 800the pulmonary vascular resistance after the dyne/second/cm5 or lower are seen. To allevi-second knee surgery was higher than baseline ate the potentially deleterious effects of such ain 17 patients (57%), but none exceeded the low systemic vascular resistance (and, by ex-safety limits. tension, systemic arterial blood pressure), in-
In Group 2 (short femoral rod with tourni- termittent bolus doses of phenylephrine 20 toquet use), the pulmonary vascular resistanc~ccccc,,90 J.1g, or an infusion of phenylephrine at 5 toincreased after the first knee (0.1-1.0 J.1g/kg/minute) werec cc c"'"'"' cccccc", "",",ccc , c30 patients (70%). The second titrated to the patient's sys-
200 dyne/second/cm5 (21 ~ ,:i~~;an~29q~,~~~"' !S1s~~f1wt'ilnd\p'~~of1ary vascular resistance.in one patient because the p~lmonatYi vias~ular I The Isolated ele~~tiqn of pulmonary vascularresistance increased mor~ lli4~t ijredictive of mechanicalline (62 to 177 dyne/secQu'cm5):,!wentyiipa2'cc",! qp$.frpctJQ:ri! of itlJ[ ~ulmonary vasculature if
the second knee surgery 'ii~~ii ~o q~~ci~i~ITci i~i~,~~I!!}tIdh ",pr~~ute remaIned wIthIn normalmonary vascular resistancei,~t'W1eri,~1ian 20gJ~imits, ~picJjJ:Ih7f did in the operations in pa-dyne/second/cm5 (209 and (Tables 4,5). As seen intient had fat embolism in the pulmonary vascu-
In Group 3 (femoral rod without idun},igu~.t i!;Ji 41 ~~$istance to systemic vascular resistanceuse), no second knee surgeries were cancellea:c",", """Ciatlo after the first knee replacement in pa-Six patients (46%) had increased pulmonary tients whose second knee replacements werevascular resistance after the first knee re- cancelled increased from the baseline byplacement and seven patients (54%) after the 87.5% compared with an increase of 8.3% insecond knee surgery, but none reached 200 patients who received bilateral total knee re-
dyne/second/cm5. iiiii iiiii c'i iiii yjPlacemen~ (Piiii~iiiP.001).
compared with elevation of pullQary,¥ias;\iu,;; ;;c,Q~I:~~ti~~, ,'i£;lmorbidities. The five patientslar resistance alone to determiri"lf;~hi~iil1'al ii!lo~ese~tl knee replacements were can-surement might be more predictive of em- celled had a mean age of 70.8 :t 4.0 yearsbolism. During continuous epidural anesthesia compared with 69.3 :t 7.1 years in patients
TABLE 4. Blood Gas Analysis for the Entire Cohort of Patients
Parameter Baseline After First Knee After Second Knee
Pa02(mean) 257.1mmHg:t91.7 217.2mmHg:t82.2 222.6mmHg:t80.9O2 sat 99.4% 98.9% 99.3%pH 7.44 7.42 7.40PaC02 34.1 mm Hg:t 5.1 35.3 mm Hg :t 4.1 36.9 mm Hg :t 3.4

,
Number 396March, 2002 Intraoperative Monitoring for Knee Replacement 147-.
TABLE 5. Blood Gas Analysis of the Seven Patientswho had the Second Knee Procedure Cancelled
Parameter Baseline After First Knee
PaO2 291.0mmHg:t108 270.2mmHg:t117P aCO2 34.0 mm Hg :t 3.0 42.3 mm Hg :t 9.6
who had bilateral knee surgeries. Three pa- pulmonary vascular resistance above the safetients who had their second knee replacement limits.cancelled had no preoperative medical p~gb;"'"""""'""""Ihe tourniquet time of 148 knees which
=~~Fi~~cancelled had a history of titrie:!~QJ;Qilateral total knee replace-
cancellation of the seconp~ee rElf:l;Li\vEltnElni.::c: thElses:())UQsurge~was progressing.In one patien~, the f:l;ulmdr~ 9~atH1nced f:l;ostoperative con-tance at 10 mmutes after tpulplC!1uet ;ijat~g~,! "cfq~~ffi),())(!)~ncep}jalgpathy and there were nowas 266 dyne/second/cm$'~~fI!\the ::'$dJd~";fknee replacement was canc~~e~%cfOc};Ilinute~~~::'lents wh()):bf)~b!l~teral surgeries, but no otherlater it wa~ 314 was ~een. Deep .veinhours later It was 210 dyne/second/c!p~lth, c~mbos~~:In the calf occurred m three patIentsother patient, the pulmonary vasculiit"'resi~~::~np.,had"bilateral total knee replacements, buttance was 210 dyne/second/cm5 10 minutes""" no propagation of thrombi was identified and noafter tourniquet deflation and had dropped to treatment was given. No pulmonary embolism111 dyne/second/cm5 when measured again developed during the postoperative course.3.5 hours later. In the five patients who had Transient arrhythmia occurred in five patientstheir second surgery cancelled, the mean pre- who had bilateral surgeries and two patients
ings remained unchanged after the first total lateral surgeries, atrial fibrillation occurred inknee replacement despite an i'!t.rcj,,~;~, tachycardia in one, and
TABLE 6. Comparison of the Pulmonary Vascular Resistance and SystemicVascular Resistance Ratio Between Patients with Bilateral Surgeries andPatients with Cancelled Surgery after the First Knee Operation
Patients with Bilateral Patients With CanceledParameter. Surgeries Surgery
Baseline PVR/SVR ratio 0.12 :t 0.05 0.08 :t 0.04PVR/SVR ratio after the first knee 0.13 :t 0.05 0.15 :t 0.07Increase of PVR/SVR ratio (%) 8.3 87.5
.PVR = pulmonary vascular resistance; SVR = systemic vascular resistance.~

.
Clinical Orthopaedics148 Dorr et al and Related Research
transient ventricular tachycardia of 3 seconds in placed again at the same operation. Five pa-one. In the two patients with transient arrhyth- tients (7%) preferred that the knee replace-mias, who had only one knee replacement, atrial ments be done with two operations. Two offibrillation occurred in one and multifocal atrial these five were the previously mentioned pa-tachycardia occurred in one. For the patients tients who had postoperative complications.who had bilateral total knee replacements the One patient had limited motion of 80° on thestay in the intensive care unit averaged l.l:t left knee and 90° on the right knee with a 5° ex-0.3 days. The acute care hospital stay averaged tension lag, which precluded her from resum-5.1 :t 1.9 days. Sixty-four patients (86%) re- ing usual activities. One patient was not satis-quired a rehabilitation stay of 7.7 :t 5.8 days. fied with a one-stage operation despite rating
The patient self-assessment questionnair~"the surgical outcome as very good because hewas completed for 69 of 74 ileus and was uncomfort-
tients (11 %) had little, ilp~ov~I~~t. l;;WO"": 19~th§):~e aY~I~g~ time before patients had6.7:t 6.7
detected. Both of the ,!"
postoperatively. Forty-fivesumed their usual activities after"$iI~ry; 11;:f;;"";P~tielr;si:wJlo agree to simultaneous bilateral(20%) moderately resumed their 'acti~iiie$, 1'»' ,;j:toialkneereplacements do so for relief of painfive (7%) resumed their activities some~ar;~"""Candimproved function without two opera-and five (7%) resumed their activities only a tions. However, simultaneous bilateral totallittle. knee replacements should not be done unless
Forty patients (58%) rated the outcome of the patient can be assured that the operation issurgery as excellent, 18 (26%) as very good, as safe as two unilateral total knee replace-seven (10%) as goo~, 'i~nd two eachd'(~'i%) as !'ifllents. Thi¥ hYP~ifhesis of this study was that
One had.a quadri~eps rupt":e it"tJ1ijJ~'ti:fI~ :li~:~~f1e~~:j~"lihemodyn.amic parameters of em-after fallIng, requIred a repaIr atfd castlng~ and '!!'!'ilf)olIs'n{1:;;pft1s1'hypothesls was suggested by thehad an extension lag of 50°. This patient also findings of the study of Dorr et al5 who con-had suffered a recurrent dislocation of the cluded that a pulmonary vascular resistanceright posterior stabilized knee, which required elevation of 200 dyne/second!cm5 or morea revision to a constrained tibial insert. The was indicative of severe embolism and that aother patient experienced a partial peroneal second total knee replacement should not benerve palsy involving only the sensory func- done. In this study the criteria of the pul-tion in the left leg and depression developed monary vascular resistance doubling its base-postoperatively. line value was used as an indication of severe
Sixty-four patients (93%) thought the one- embolism. The use of the pulmonary vascularstage bilateral total knee replacements were resistance and the value of 200 dyne/second!worthwhile and would have both knees re- cm-5 was confirmed by Berman et aI2 who

,
Number 396March, 2002 Intraoperative Monitoring for Knee Replacement 149.~~~-r---" ---
observed that the pulmonary vascular resis- creased pulmonary vascular resistance. Oxy-tance increased to this level after tourniquet gen saturation readings would only decreaserelease only when venous emboli were as large below 90 mm Hg with massive pulmonaryas 0.5 cm or more. Furthermore, three of 55 pa- emboli.tients in their study had pulmonary embolism The use of a pulmonary artery catheter hasand this did not occur without a pulmonary vas- its own mortality rate if the pulmonary artery iscular resistance above 200 dyne/second/cm5. punctured. The mortality rate with the use of aThe 52 patients who did not have pulmonary pulmonary artery catheter was 0.016% in 6245embolism did not have a pulmonary vascular patients in one study20 and 0.07 % in 5306 pa-resistance above 200 dyne/second/cm5. tients in a second study.I4 The anesthesia task
Intraoperative measurement is necessary lorce on the use of pulmonary artery cathetersbecause the increased mortality the mortality and morbidity rates
Jankiewicz et al9 and La\1e~.r !fro ~,Q~l~ !:1~t;!;!'/ ~~q,U§J}?;!jlatet~l,,~pt~ knee replacements (450
identify any comorbiditi~s.;qt patieftt "fa~tQts';!;!;!;! j~ee§)fQftly one, ql~Nlication occurred with awhich would predict ip one patient the catheteret al2 observed that the e$bQliq rjg~fvpntricle and required re-
ter increased pulmonary va'1;cul~ r~sistance.fff'fji;!pulmonarY";~~tx;icatheter is the frequency ofParmet et alII-I3 also Anyanesthesiolo-greater risk of large venous \Cma,..!afge and current experience in thetourniquet was used. c"~';""~:!. i~s~"_Q,f,"'1he Swan-Ganz pulmonary artery
Safe intraoperative monitoring requires tne"'" "'"catheter can do this procedure with a very lowuse of a pulmonary artery catheter (Swan- incidence of complications. AnesthesiologistsGanz catheter). The use of pulse oximetry has who have a large volume of experience withnot been predictive of severe embolism of cardiac surgery have a large volume of expe-blood or fat. Dorr et al5 reported that the use of rience with a pulmonary artery catheter.blood pO2 was not ~"fl\\urate criteri~.;f~f safe !iii For adqi,tioj;!alsafety in decision-making,contin~ation to ~he to systemiccause III one patIent wno dIed, the pO2 dId not vascular resIstance ratIo can be used to aug-drop until the pulmonary artery ~,Yf;C;ii}1~,§, .J.JII~eift!~;¥",iw~pce of the pulmonary vascularabove 50 mm Hg and the pulmoft'aryhvaseuJ.hr" Jii,re§fstknce'measurement. The use of phenyl-resistance was above 800 dyne/second/cm5. ephrine to counter the sympathetic blockadeBerman et aI2 observed that pulse oximetry of continuous epidural anesthesia can cause awas not predictive of embolization dangerous concomitant rise in pulmonary vascular resis-to the patient. Barre et all studied bilateral to- tance independent of any embolic phenomena.tal hip replacements and reported that pulse Phenylephrine was used routinely to manageoximetry did not detect successive embolic the acute changes of hypotension withoutphenomena before pulmonary artery hyper- bradycardia secondary to tourniquet release. Iftension caused left heart changes that led to a patient's heart rate was below 50 beats perhemodynamic accidents. They recommended minute after tourniquet release, 5 mg bolusthe use of a Swan-Ganz catheter. In the current doses of ephedrine (which elevates bloodstudy, pulse oximetry was not sensitive to in- pressure and heart rate) were titrated to bring

..
Clinical Orthopaedics150 Dorr et al and Related Research
~ the blood pressure to within 10% of baseline. ready was experienced without intraoperative
Pulmonary vascular resistance measurements monitoring.5 Because no study has identifiedwere done 5 minutes after release of the patient predictive factors5.9.IO and Dorr et al5tourniquet to allow the confounding effects of described the occurrence of fat emboli as idio-the pharmacologic agents to dissipate. The syncratic, it would be unethical to randomizedifferentiation of the elevation of the pul- patients into those with or without pulmonarymonary vascular resistance from the pharma- vascular resistance measurements. Unilateralcologic therapy, and not embolic events, is total knee replacement and staged bilateral to-that the pharmacologic elevation is seen even tal knee replacements do not have the dangerbefore surgical incision in patients in whom of compounded emboli from two knee re-the vasoactive agent is given. To further dis;:cccc.cplacements, so these operations as a control dotinguish between pulmonary any additional information as to
elevated pulmonary to the patient self-
lar resIstanc.e Illcreased and r~ported a nationalvascular resIstance decreased patients wIth knee replace-nificant increase in in pain was reported insistan~e to systemic vasc~lar resistahce'!.~!~~:c:~i!~c487 patients (82.~%) an~ 415 of 487In patients whose surgenes were cancelled, patients (85.2%) were satisfied wIth the resultsthe pulmonary vascular resistance to systemic of the total knee replacement. In the currentvascular resistance ratio increased on average study, 64 of 69 patients (92%) reported that88%. The use of absolute values of pulmonary function was recovered for usual activities orvascular resistance and systemic vascular re- better. Hawker et al8 found 418 of 469 patientssistance and the ratio of these values allows (89.1 %) resumed their function after totalmore ~atio~al of the patientsoccumng III the pulmonary vascular bed dur- tliought that ohe knee liad a better result thaning surgery in which embolic PI;~~i~i i~i .I.II"i!r~ ~!~i~~' The time for full recovery fromnot uncommon. The authors recbm1fiefiaftliat fif.tlie 'tbtar Yee replacement was nearly 7an increase of more than 60% of baseline of months with many patients indicating that thethe pulmonary vascular resistance to systemic time for them to heal completely was 1 year.vascular resistance ratio after the first knee op- Stanley et a}22 also reported on a study oferation means that the second knee operation bilateral knee replacements that provided datashould be cancelled. on function. They studied 32 simultaneous bi-
A study conducted by using controls would lateral total knee replacements and 18 stagedprove the safety of the use of the pulmonary bilateral total knee replacements. The func-vascular resistance. However, any control tional data reported was that 11 % of themust be safe for the patient and this type of patients were household ambulators and onlycontrolled study would require death of a pa- 21 % of the patients thought they could do a fulltient for confirmation of a technique. This al- range of housework. This functional data seem
-

..
Number 396March, 2002 Intraoperative Monitoring for Knee Replacement 151, ~._. , ,.-.,. .-.
to be worse than the data of the current pa- anesthesia in surgical mortality. JAMA 178:261-268.
tients and those of Hawker et al.87 Fl~: NR Ch d1 HP D I huk K .B.
I I I kn I ."'llllY , an er , any c , et al.
latera tota ee rep acements can be Blood-gas and circulatory changes during total knee
done with protection against severe emboli replacement: ~ole of the intramedullary alignment
when an experienced team of anesthesiolo- rod. J Bone Jo~t Surg 72A:19-26, 1990.
..8. Hawker G, Wnght J, Coyle P, et al: Health-relatedgIsts and orthopaedIc total knee replacement quality of life after knee replacement. J Bone Joint
surgeons work together. Intraoperative moni- Surg.80~:163-173, 1998.
toring with a pulmonary artery catheter will 9. Jank;iewIcz JJ, Sculco TP, Ranawat CS, ~ehr C. Tar-
rentIno S: One-stage versus 2-stage bilateral totalindIcate whIch patIents are at Increased risk knee arthroplasty. Clin Orthop 309:94-101,1994.
for pulmonary vascular compromise after one 10. Lane GJ, Hozack WI, Shah S, et al: Simultaneous bi-
total knee replacement and therefore are not lateral vers~ unil~teral total knee arthroplasty: Out-
..c,c",CCC"""CCC"'C~9flle analysIs. Clrn Orthop 345:106-112, 1997.
be prepared with extrametlutfary tOO:].$j'\thichff'" c 4£' ~~~astY\,'~W9U~ pneumauc tournIquet use.
." cAA!,! AA, '!A, 'A, ,!,,!Ac AA,AA," ~2~!"'~1Analg,8!(t!lg9;,-444, 1998.may Include a short (9-cJn)I?ll~taphyseal.rod'A ;;13; Pafhtet'L, Ho!t:1"OW!JC, Pharo G, et al: The incidence
for stabilization of the tJhi!i
long tibial intramedullaJ!y,A)fOd win"'))P.rodu,c~',A,",)!! ')c~eelltt!~pl~:\t~)A~n~~th An.aIg ~1.757-762: 19:5..!" ill!, !" !A;l,. A "'!!,~ c '!"'!!!", 1'!i',AA~9c!l!i1Pfll1,'A!B, ~1~!~et1:;l1 G Miletti E, LattanzI W. A
more embolI than one use~ I~!,the;tl:}!lill!f. ~'Qyr-"' '" " ,;! ';review dfpultpq~ Ju1ery catheterization in 5,306
i~g patient selection cardiac surgery. Br
tlents who clearly manifest actnelancJ\:()I]1 ~:()Ir~!! AR~~ JD!MIJ) ~J C DD tal' Ct.
depressed ~rsonality2I 'son be,~.il~f;t s~~~eo~~ s~~s ~~~~~
do poorly wIth any surgery that)sltIgrie.,Qth:;!!!"i!"""'" e~t<1~~,PfiIt~plasty.JArthroplastyI3:172-179,
erwise, patient satisfaction was asi'gp~'[:1I;:;a~th'!irCO")); 6C!"'RiI9~A)AM'::'" c.4'amIi"" .LA M Iii CA t al . 0 t .
."', -', 4JJ "'f ,:!; M~ ,!M. n ,e .e .u come Im-
reported for unIlateral total knee repl.i:tcej 1£ il'1 i; plicatlons for the timing of bilateral total knee arthro-
ments,8 and the ratings of results by patie'nts""'""~""""""pl.asties. Clin ~op 345:~-105, ~997.
were not different from unilateral or sta g ed bi- 17. Ritter MA, Meding JB: Bilateral simultaneous total
knee arthroplasty. J Arthroplasty 2:185-189,1987.lateral total knee replacements.23 18. Roizen MF, Berger DL, Gabel RA, et al: Practice
guidelines for pulmonary artery catheterization: AReferences report by the American Society of Anesthesiologists
1. Barre J, Lepouse C, Segal P: Embolism and in- task force on pulmonary artery catheterization.
tramedullary femorai!,,; s\!l"gery. Rev Chjf ,prthop Co,,;' Anesthe!'~iol°¥IY !(t~:380-394, 1993.
2. proce-
observed with use of transesophagea)echocardiog- ~20.Shah KB. Rao TL, Laughlin S, El-Etr AA: A review
raphy immediately after tourniquet rl,Is.,:dl!J"i'lgl;IJ", ),IJJfj !i:ipfpq!~P!l. artery catheterization in 6,245 patients.
tal knee arthroplasty with cement. JBone',tJoiut!SiJirg: ::::lliij' AAA)iieSitheSiHgy 61:271-275,1984.
80A:389-396,1998. 21. Sharma L, Sinacore J. Daugherty C, et al: Proguos-
3. Bindelglass DF, Cohen JL, Dorr LD: The technique tic factors for function.al outcome of total knee ~e-
for total knee arthroplasty using simultaneous ce- placement: A prospectIve study. J Gerontol A BioI
mentingofcomponents. Tech Orthop 6:47-56, 1991. SciMedSci51:152-157,1996..
4. Brotherton SL, Roberson JR, de Andrade JR, FIem- 22. Stanley D, Stockley I, Getty CJ: SImultaneous or
ing LL: Staged versus simultaneous bilateral total s~ged bi~~teral total kn~ replacements in ~heurna-
knee replacement. J Arthroplasty 1:221-228, 1986. told arthrius: A prospectIve study. J Bone Jornt Surg
5. Dorr LD, Merkel C, Mellman MF, Klein I: Fat em- 72B:772-774, 1990. .
boll in bilateral total knee arthroplasty: Predictive 23. Udo~at p, Meng ~, Dorr .LD, Wan.Z: Funcuo~
factors for neurologic manifestations. Clin Orthop compansonofpostenorcruclateretenUonandsubstI-
248:112-118,1989. tution knee replacement. Clin Orthop 378:192-201,
6. Dripps RD, Lamont A, Eckenhoff JE: The role of 2000.
--