Clinical Infectious Diseases Society -...
7
Clinical Infectious Diseases Society Newsletter : July 2018 Website: www.cidsindia.org Volume 5, Issue 7, July 2018 Editor: Dr Ram Gopalakrishnan Associate Editors: Dr Neha Gupta, Dr Ashwini Tayade, Dr Vasant Nagvekar Editor's note Dear CIDS Members, CIDSCON 2018 will be from August 16th to 18th 2018 (Thursday to Saturday) in Vellore. Please block your dates and check out details at www.cidscon.in The society newsletter completes five years with this issue, hopefully we can take it to greater heights with your active contributions! Photoquiz A 40/M from Assam, a farmer with no known co-morbid conditions presented with lesions on the right forearm for 4 months. They started with single nodule and then other nodules started appearing with few of them ulcerating. He denied h/o trauma/animal bite. What is your diagnosis?
Transcript of Clinical Infectious Diseases Society -...
Clinical Infectious Diseases SocietyNewsletter : July 2018
Website: www.cidsindia.org Volume 5, Issue 7, July 2018
Editor: Dr Ram Gopalakrishnan Associate Editors: Dr Neha Gupta, Dr Ashwini Tayade, Dr Vasant Nagvekar
Editor's note
Dear CIDS Members, CIDSCON 2018 will be from August 16th to 18th 2018 (Thursday to Saturday) in Vellore. Please block your dates andcheck out details at www.cidscon.in
The society newsletter completes five years with this issue, hopefully we can take it to greater heights with youractive contributions!
Photoquiz
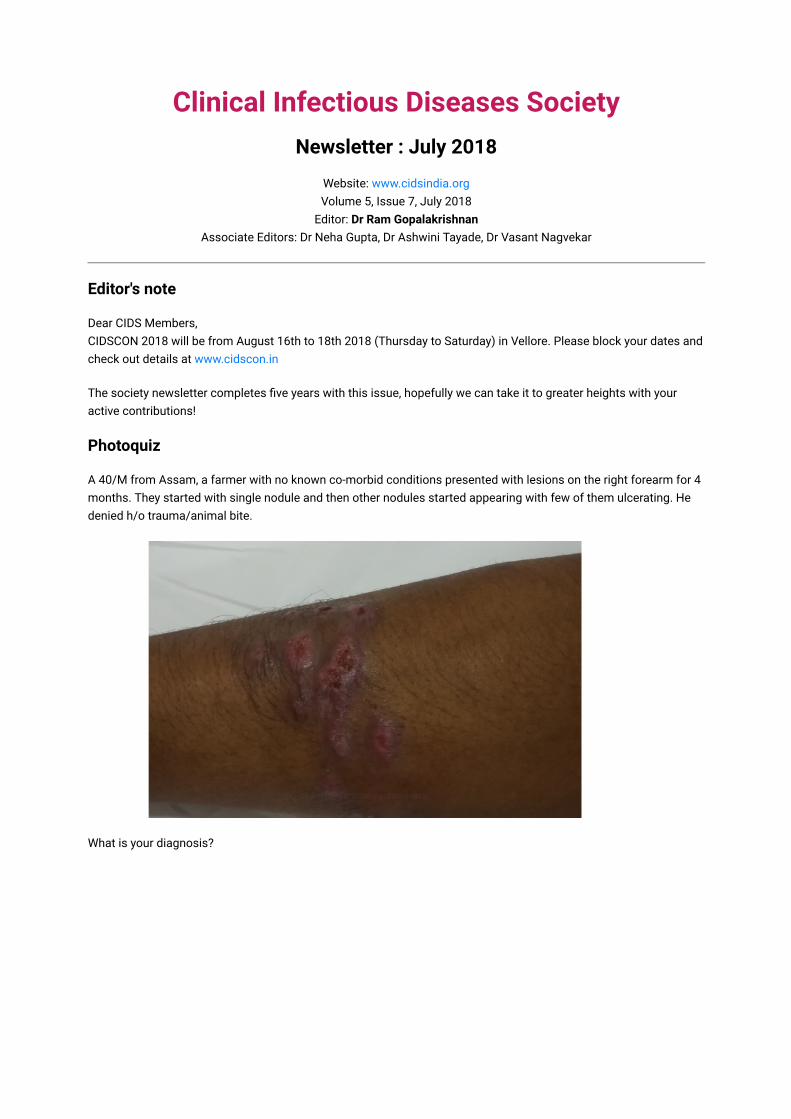
A 40/M from Assam, a farmer with no known co-morbid conditions presented with lesions on the right forearm for 4months. They started with single nodule and then other nodules started appearing with few of them ulcerating. Hedenied h/o trauma/animal bite.
What is your diagnosis?

ID NEWS
WHO recommends quadrivalent influenza vaccine for 2018-19
The quadrivalent influenza vaccine was licensed for use by the U.S. Food and Drug Administration (FDA) in 2013; it islicensed in 26 countries. Since the vast majority of influenza vaccines manufactured were trivalent till recently, theWorld Health Organisation (WHO) used to recommend two A subtypes and one B subtype, plus an optional fourthstrain (the other B virus strain). But this February 2018, for the first time, the WHO issued an official recommendationfor a quadrivalent vaccine. “It is recommended that quadrivalent vaccines for use in the 2018-2019 northernhemisphere influenza season,” the WHO noted. The quadrivalent vaccine will have two A virus strains — H1N1 andH3N2 — and two B virus strains — Victoria and Yamagata
The injectable influenza vaccine containing two A virus strains — H1N1 and H3N2 — and two B virus strains —Victoria and Yamagata — for active immunisation of adults of age 18 to 64 years was approved in May last year bythe Drug Controller General of India (DCGI). The application for the paediatric indication is under review by the DCGIand final approval is expected by the end of this month.
In the case of H1N1, there are two strains — California and Michigan — that cause influenza. In India, the Michiganstrain was earlier circulating and has been replaced by the California strain. For 2018, the WHO has recommendedthe Michigan strain for the southern hemisphere, including India.
Despite the high number of infections and mortality each year, India does not have in place a national policy forinfluenza immunisation.
JOURNAL REVIEW
Comparison of a Novel Human Rabies Monoclonal Antibody to Human RabiesImmunoglobulin for Postexposure Prophylaxis
Clin Infect Dis. 2018 Jan 18;66(3):387-395 Contributed by Dr Ashwini Tayade
Lack of access to rabies immunoglobulin (RIG) contributes to high rabies mortality. A recombinant humanmonoclonal antibody (SII RMAb) made in India was tested in Indian patients as a postexposure prophylaxis (PEP)regimen in comparison with a human RIG (HRIG)–containing PEP regimen.
This was a phase 2/3, randomized, single-blind, noninferiority study conducted in 200 participants with World HealthOrganization category III suspected rabies exposures. Participants received either SII RMAb or HRIG (1:1 ratio) inwounds and, if required, intramuscularly on day 0, along with 5 doses of rabies vaccine intramuscualarly on days 0, 3,7, 14 and 28. The primary endpoint was the ratio of the day 14 geometric mean concentration (GMC) of rabies virusneutralizing activity (RVNA) as measured by rapid fluorescent focus inhibition test for SII RMAb recipients relative toHRIG recipients.
One hundred ninety-nine participants received SII RMAb (n = 101) or HRIG (n = 98) and at least 1 dose of vaccine.The day 14 GMC ratio of RVNA for the SII RMAb group relative to the HRIG group was 4.23 (96.9018% confidenceinterval [CI], 2.59–6.94) with a GMC of of 24.90 IU/mL (95% CI, 18.94–32.74) for SII RMAb recipients and 5.88 IU/mL(95% CI, 4.11–8.41) for HRIG recipients. The majority of local injection site and systemic adverse reactions reportedfrom both groups were mild to moderate in severity.
A PEP regimen containing SII RMAb was safe and demonstrated noninferiority to HRIG PEP in RVNA production. Thenovel monoclonal potentially offers a safe and potent alternative for the passive component of PEP and couldsignificantly improve the management of bites from suspected rabid animals. The monoclonal antibody in made inIndia and is approved for this purpose by DCGI.

JOURNAL REVIEW
Does “latent” genital tuberculosis adversely affect the ovarian reserve in infertileIndian women?
Hum Reprod. 2018 Jul 1;33(7):1262-1269 Contributed by Dr Nitin Bansal
STUDY QUESTION: What is the effect of latent genital tuberculosis (GTB) on ovarian reserve in infertile women?
SUMMARY ANSWER: Women with latent GTB have lower ovarian reserves and yield lower numbers of oocytes in IVF.
WHAT IS KNOWN ALREADY: Limited evidence suggests that women with GTB may have a low ovarian reserve.Infertile women have a high incidence of latent GTB and treatment improves fertility outcomes.
STUDY DESIGN, SIZE, DURATION: This prospective study from February 2013 to January 2016 compared 431infertile women diagnosed with latent GTB (Group I) to 453 infertile women without latent GTB (Group II).
PARTICIPANTS/MATERIALS, SETTING, METHODS: The study was conducted at Shreyas Hospital, Kolhapur, India, atertiary referral centre for infertility. Women of both groups were 21–38 years of age. Group I consisted of infertilewomen with proven tubal patency but with latent GTB diagnosed by DNA PCR testing of an endometrial biopsy. Day2–4 anti-Mullerian hormone (AMH) and antral follicle count (AFC) were assessed in both groups. All women withlatent GTB took antituberculosis therapy (ATT). Gonadotropin dosages and oocyte and embryo details were noted inboth groups for those who underwent IVF.
MAIN RESULTS AND THE ROLE OF CHANCE: Women with latent GTB were younger (29.8 ± 4.4 years vs. 30.8 ± 4.5years; P = 0.003) and, following adjustment for age, had significantly lower AMH [Median (IQR): 2 (0.9, 4.1) ng/ml vs2.8 (1.3, 5) ng/ml; P = 0.01] and AFC [Median (IQR): 7 (5, 11) vs 8 (5, 14); P < 0.001]. Post ATT, women with latentGTB yielded fewer oocytes (9.3 ± 7.6 vs. 10.9 ± 8.1;P = 0.01), but had more grade I embryos transferred (1.1 ± 0.5 vs.0.89 ± 1.0; P = 0.001) and a better implantation rate (26.8% vs. 17.5%;P = 0.004) in IVF compared to women in GroupII. Group I had a higher pregnancy rate compared to Group II (51.6% vs. 40.5%; P = 0.001), through various treatmentmodalities. Considering the adequacy of the sample size and use of robust ovarian reserve markers, the role ofchance is minimal.
LIMITATIONS REASONS FOR CAUTION: The study is limited to an infertile population visiting a tertiary referralcentre. The mechanisms by which latent GTB infection would lead to ovarian damage are unclear.
WIDER IMPLICATIONS OF THE FINDINGS: It is believed that latent GTB is without any clinical significance. However,a low ovarian reserve in young women with latent GTB necessitates considering it as a cause of infertility, in womenwith prolonged infertility. These women may experience an accelerated decline in ovarian reserve with reducedsuccess in achieving biological parenthood. Clinicians must be aware of this condition and its consequences whilemanaging infertility.
There are multiple methodologic flaws in this study:
It is difficult to justify the term latent TB based on a positive PCR test, which by definition means active TB.Instead of using a WHO recommended PCR such as Xpert Mtb, the tissue was transported for a real timemultiplex DNA PCR (RT PCR) for M TB to a commercial lab in Mumbai, India which does a home brew PCR, atechnique known to give false positive results.No evidence of granulomatous inflammation or mycobacterial stain or culture positivity was demonstrated, asine qua non for TB diagnosis.
One hopes this will not lead to a wave of unnecessary and potentially toxic ATT prescriptions to young and healthyinfertile women, without any evidence of GTB.

JOURNAL REVIEW
Policy Recommendations From Transmission Modeling for the Elimination of VisceralLeishmaniasis in the Indian Subcontinent
Clin Infect Dis. 2018 Jun 1;66(suppl_4):S301-S308 Contributed by Dr Ashwini Tayade
Visceral leishmaniasis (VL) has been targeted by the World Health Organization (WHO) and 5 countries in the Indiansubcontinent for elimination as a public health problem. To achieve this target, the WHO has developed guidelinesconsisting of 4 phases of different levels of interventions, based on vector control through indoor residual sprayingof insecticide (IRS) and active case detection (ACD). Mathematical transmission models of VL are increasingly usedfor planning and assessing the efficacy of interventions and evaluating the intensity and timescale required toachieve the elimination target. This paper draws together the key policy-relevant conclusions from recenttransmission modeling of VL, and presents new predictions for VL incidence under the interventions recommendedby the WHO using the latest transmission models.
The model predictions suggest that the current WHO guidelines should be sufficient to reach the elimination targetin areas that had medium VL endemicities (up to 5 VL cases per 10000 population per year) prior to the start ofinterventions. However, additional interventions, such as extending the WHO attack phase (intensive IRS and ACD),may be required to bring forward elimination in regions with high precontrol endemicities, depending on the relativeinfectiousness of different disease stages.
The potential hurdle that asymptomatic and, in particular, post-kala-azar dermal leishmaniasis cases may pose toreaching and sustaining the target needs to be addressed. As VL incidence decreases, the pool of immunologicallynaive individuals will grow, creating the potential for new outbreaks.
JOURNAL REVIEW
Bone Marrow Is a Major Parasite Reservoir in Plasmodium vivax Infection
MBio. 2018 May 8;9(3). pii: e00625-18
Plasmodium vivax causes heavy burdens of disease across malarious regions worldwide. Mature P. vivax asexualand transmissive gametocyte stages occur in the blood circulation, and it is often assumed thataccumulation/sequestration in tissues is not an important phase in their development. Here, the authors present asystematic study of P. vivax stage distributions in infected tissues of nonhuman primate (NHP) malaria models aswell as in blood from human infections. In a comparative analysis of the transcriptomes of P. vivax and Plasmodiumfalciparum blood-stage parasites, we found a conserved cascade of stage-specific gene expression despite thegreatly different gametocyte maturity times of these two species. Using this knowledge, we validated a set ofconserved asexual- and gametocyte-stage markers both by quantitative real-time PCR and by antibody assays ofperipheral blood samples from infected patients and NHP (Aotus sp.). Histological analyses of P. vivax parasites inorgans of 13 infected NHP (Aotus and Saimiri species) demonstrated a major fraction of immature gametocytes inthe parenchyma of the bone marrow, while asexual schizont forms were enriched to a somewhat lesser extent in thisregion of the bone marrow as well as in sinusoids of the liver.
These findings suggest that the bone marrow is an important reservoir for gametocyte development andproliferation of malaria parasites.

JOURNAL REVIEW
LN34 pan-lyssavirus real-time RT-PCR assay for post-mortem rabies diagnostics
PLoS One. 2018 May 16;13(5):e0197074
The current gold standard for post-mortem diagnosis of human and animal rabies is the direct fluorescent antibody(DFA) test. While the DFA test has proven sensitive and reliable, it requires high quality antibody conjugates, a skilledtechnician, a fluorescence microscope and diagnostic specimen of sufficient quality. The LN34 pan-lyssavirus real-time RT-PCR assay represents a strong candidate for rabies post-mortem diagnostics due to its ability to detect RNAacross the diverse Lyssavirus genus, its high sensitivity, its potential for use with deteriorated tissues, and its simple,easy to implement design. Here, we present data from a multi-site evaluation of the LN34 assay in 14 laboratories. Atotal of 2,978 samples (1,049 DFA positive) from Africa, the Americas, Asia, Europe, and the Middle East were tested.The LN34 assay exhibited low variability in repeatability and reproducibility studies and was capable of detectingviral RNA in fresh, frozen, archived, deteriorated and formalin-fixed brain tissue. The LN34 assay displayed highdiagnostic specificity (99.68%) and sensitivity (99.90%) when compared to the DFA test, and no DFA positivesamples were negative by the LN34 assay. The LN34 assay produced definitive findings for 80 samples that wereinconclusive or untestable by DFA; 29 were positive. Five samples were inconclusive by the LN34 assay, and only onesample was inconclusive by both tests. Furthermore, use of the LN34 assay led to the identification of one falsenegative and 11 false positive DFA results. The new LN34 test is simpler and easier to use than current tests. Duringthe pilot study, it produced no false negatives, fewer false positive, and fewer inconclusive results. Together, theseresults demonstrate the reliability and robustness of the LN34 assay and support a role for the LN34 assay inimproving rabies diagnostics and surveillance.
JOURNAL REVIEW
Bedaquiline and delamanid for the treatment of patients with drug-resistanttuberculosis
Lancet Infect Dis. 2018 May;18(5):536-544 Contributed by Dr Nitin Bansal
The authors retrospectively analysed a cohort of all patients who received 6–12 months of oral bedaquiline anddelamanid in combination (400 mg bedaquiline once per day for 2 weeks, then 200 mg bedaquiline three times perweek and 100 mg delamanid twice per day). 28 patients (median age 32·5 years [IQR 28·5–40·5], 17 men) wereincluded in the analysis. 11 (39%) of 28 patients were HIV-positive. 24 patients (86%) had isolates resistant tofluoroquinolones; 14 patients (50%) had extensively drug-resistant tuberculosis. No patient had an increase of morethan 500 ms in their QTcF interval. Four patients (14%) had six instances of QTcF increase of more than 60 ms frombaseline but none permanently discontinued the drugs. 16 serious adverse events were reported in seven patients.Of 23 individuals with positive baseline cultures, 17 (74%) converted to negative by month 6 of treatment.
Use of the bedaquiline and delamanid combination appears to reveal no additive or synergistic QTcF-prolongingeffects. Access to bedaquiline and delamanid in combination should be expanded for people with few treatmentoptions while awaiting the results of formal clinical trials.
JOURNAL REVIEW
Association Between Bacteremia from Specific Microbes and Subsequent Diagnosisof Colorectal Cancer
Gastroenterology. 2018 May 2. pii: S0016-5085(18)30489-X
In a retrospective study in Hong Kong, investigators compared the incidence of CRC between over 13,000 patientswith bacteremia and age-, sex-, and comorbidity-matched controls without bacteremia. Bacterial species associatedwith CRC were Bacteroides fragilis (adjusted hazard ratio, 3.9), Fusobacterium nucleatum (HR, 6.9), Clostridiumsepticum (HR, 17.1), Clostridium perfringens (HR, 2.3), and Gemella morbillorum (HR, 15.2). Streptococcusgallolyticus, which belongs to the Streptococcus bovis group, was also significantly associated with CRC (HR, 5.7),but other S. bovis subspecies were not.
Clinicians should strongly consider colonoscopy for patients with bacteremia involving these species.
Upcoming Conferences
4th Transplant Infectious Diseases (TID) conference, Hyderabad, Aug 14-15.
Payment made by demand draft or wire transfer in advance. Interested participants may send in their names [email protected] and contact number - 0416-2282804
Guideline watch
BSAC: Treatment of infections caused by multidrug-resistant Gram-negative bacteria
J Antimicrob Chemother. 2018 Mar 1;73(suppl_3):iii2-iii78
IDSA/ASM: A Guide to Utilization of the Microbiology Laboratory
Clin Infect Dis. 2018 Jun 28
Answer to the photoquiz
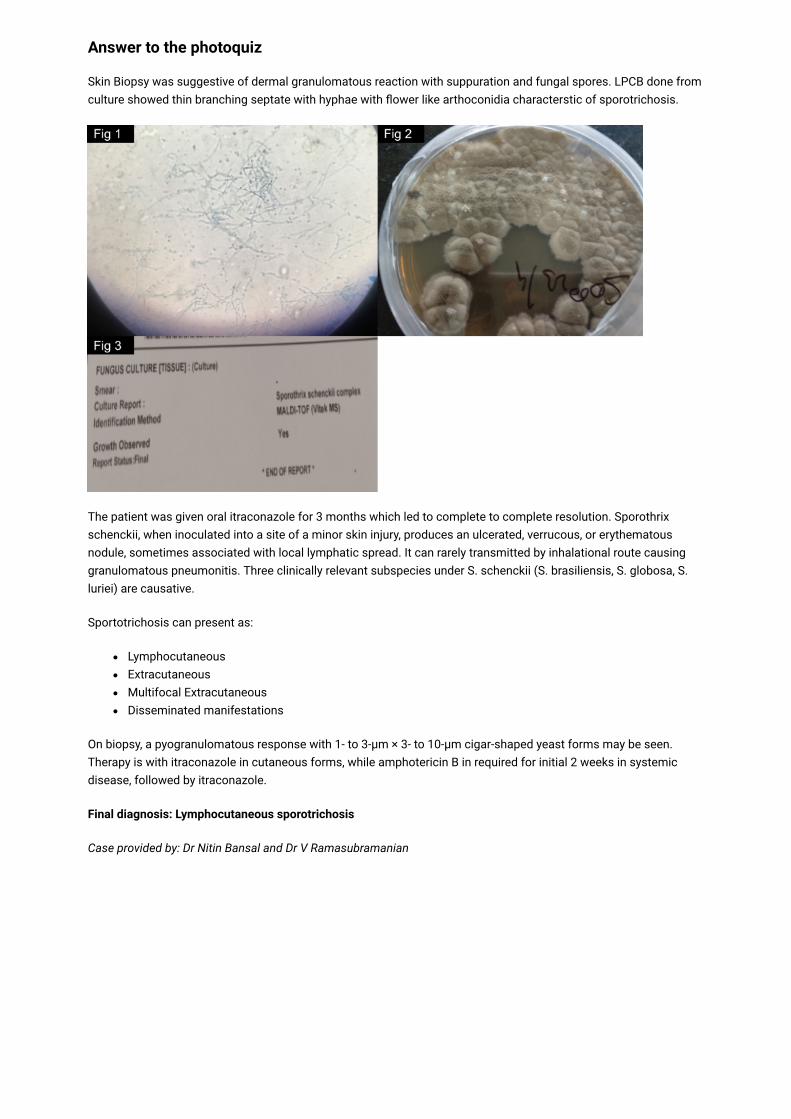
Skin Biopsy was suggestive of dermal granulomatous reaction with suppuration and fungal spores. LPCB done fromculture showed thin branching septate with hyphae with flower like arthoconidia characterstic of sporotrichosis.
The patient was given oral itraconazole for 3 months which led to complete to complete resolution. Sporothrixschenckii, when inoculated into a site of a minor skin injury, produces an ulcerated, verrucous, or erythematousnodule, sometimes associated with local lymphatic spread. It can rarely transmitted by inhalational route causinggranulomatous pneumonitis. Three clinically relevant subspecies under S. schenckii (S. brasiliensis, S. globosa, S.luriei) are causative.
Sportotrichosis can present as:
LymphocutaneousExtracutaneousMultifocal ExtracutaneousDisseminated manifestations
On biopsy, a pyogranulomatous response with 1- to 3-μm × 3- to 10-μm cigar-shaped yeast forms may be seen.Therapy is with itraconazole in cutaneous forms, while amphotericin B in required for initial 2 weeks in systemicdisease, followed by itraconazole.
Final diagnosis: Lymphocutaneous sporotrichosis
Case provided by: Dr Nitin Bansal and Dr V Ramasubramanian